

Abstract
Background:
Handwriting skills, which are crucial for success in school, communication, and building children’s self-esteem, have been observed to be poor in individuals with autism. Little information exists on the handwriting of children with autism, without delineation of specific features that can contribute to impairments. As a result, the specific aspects of handwriting in which individuals with autism demonstrate difficulty remain unknown.
Methods:
A case-control study of handwriting samples from children with and without autism spectrum disorders (ASD) was performed using the Minnesota Handwriting Assessment. Samples were scored on an individual letter basis in 5 categories: legibility, form, alignment, size, and spacing. Subjects were also tested on the Wechsler Intelligence Scale for Children–IV and the Physical and Neurological Examination for Subtle (Motor) Signs.
Results:
We found that children with ASD do indeed show overall worse performance on a handwriting task than do age- and intelligence-matched controls. More specifically, children with ASD show worse quality of forming letters but do not show differences in their ability to correctly size, align, and space their letters. Within the ASD group, motor skills were significantly predictive of handwriting performance, whereas age, gender, IQ, and visuospatial abilities were not.
Conclusions:
We addressed how different elements of handwriting contribute to impairments observed in children with autism. Our results suggest that training targeting letter formation, in combination with general training of fine motor control, may be the best direction for improving handwriting performance in children with autism.
GLOSSARY
- ADI-R
= Autism Diagnostic Interview–Revised;
- ADOS-G
= Autism Diagnostic Observation Schedule–Generic;
- ASD
= autism spectrum disorders;
- DICA-IV
= Diagnostic Interview for Children and Adolescents, 4th edition;
- DSM-IV
= Diagnostic and Statistical Manual of Mental Disorders, 4th edition;
- FSIQ
= full-scale IQ;
- PANESS
= Physical and Neurological Examination for Subtle (Motor) Signs;
- PRI
= Perceptual Reasoning Indices;
- WISC-IV
= Wechsler Intelligence Scale for Children–IV.
Good handwriting is crucial for academic progress, social and communicative development, and the building of self-esteem.1,2 Poor handwriting was noted in the original description of Asperger syndrome3 and it has since been demonstrated that individuals with autism spectrum disorders (ASD) have impairments within multiple domains that contribute to handwriting. For example, problems with fine and gross motor functions are consistently observed in individuals with ASD.4–7 Such problems could make precise manipulations of a writing tool difficult. In terms of sensory functioning, first-hand accounts from individuals with ASD reveal difficulties in sensing limb position,8 and experiments have indirectly suggested that children with autism have proprioceptive deficits.9,10 The inability to accurately sense where their limbs are in space could leave patients unable to develop fluid, automatic handwriting. Visual differences have also been observed between individuals with and without ASD: individuals with ASD demonstrate a visual bias to focus more on details, or local features, as opposed to the whole, or global features.11 In other words, while typically developing populations are said to see “the forest rather than the trees,” individuals with ASD are said to see “the trees at the expense of seeing the forest.” Differences in visual perception may affect how the shapes of letters are perceived and subsequently reproduced, a hypothesis that is supported by ASD subjects’ piecemeal strategy and configural violations when copying drawings.12
Previous studies have suggested that children with ASD have impaired handwriting abilities relative to controls, but these conclusions were inferred from tasks involving copying geometric figures (e.g., the Developmental Test of Visual-Motor Integration13) or tasks that additionally involve executive functioning and memory (e.g., the Coding subtest of the Wechsler Intelligence Scale for Children–IV [WISC-IV]14–16). One study assessed freely written handwriting samples from adults with and without ASD and found that the ASD group wrote significantly larger than the control group.17 Writing large letters does not in and of itself account for poor quality handwriting; thus we predict that handwriting impairments in individuals with autism go beyond size abnormalities. In this study we asked whether, consistent with common observations, children with ASD show overall handwriting impairments, and if so, whether these impairments are in specific qualitative categories.
METHODS
Subjects.
Twenty-eight subjects between 8 and 13 years of age participated in the study: 14 with ASD (3 female) and 14 typically developing controls (5 female). Based on performance on the WISC-IV,14 all children had full-scale IQs (FSIQ) greater than 80, with the exception of 2 children with ASD who had marked discrepancies between factor scores (subject A: Perceptual Reasoning Index 96, Working Memory Index 56, FSIQ 67; subject B: Perceptual Reasoning Index 83, Working Memory Index 68, FSIQ 71). All subjects had Perceptual Reasoning Indices (PRI) greater than 80. Research suggests that task-specific measures of intelligence provide more appropriate assessments of intellectual abilities in children with ASD than do general measures.18 Here the PRI was used as the primary intelligence measure since the study involved nonverbal, perceptually based motor tasks.
Children with ASD were recruited from outpatient clinics at the Kennedy Krieger Institute in Baltimore and from local Autism Society of America chapters, schools, social groups, and pediatricians’ offices. Children met DSM-IV criteria for ASD according to the Autism Diagnostic Observation Schedule–Generic (ADOS-G)19 and the Autism Diagnostic Interview–Revised (ADI-R).20 Children with identifiable causes of autism (e.g., fragile X syndrome) and known neurologic disorders were excluded.
Subjects in the control group were free of neurologic, developmental, or psychiatric disorders and had no immediate family member with a pervasive developmental disorder. Psychiatric diagnoses were ruled-out based on the Diagnostic Interview for Children and Adolescents, 4th edition (DICA-IV).21
Standard protocol approvals, registrations, and patient consents.
Written assent to participate was obtained from children, and written consent was obtained from a parent or guardian. Protocols were approved by the Johns Hopkins Institutional Review Board.
Procedure.
Subjects were administered the Minnesota Handwriting Assessment.22 The assessment presents a sample of the following words: “The brown jumped lazy fox quick dogs over” (figure 1). Presenting the words scrambled eliminates any speed advantage of more fluent readers.23 Subjects were instructed to copy the words on the provided solid lines (baselines) on the lower half of the test sheet, making their letters the same size as the sample and using their best handwriting.
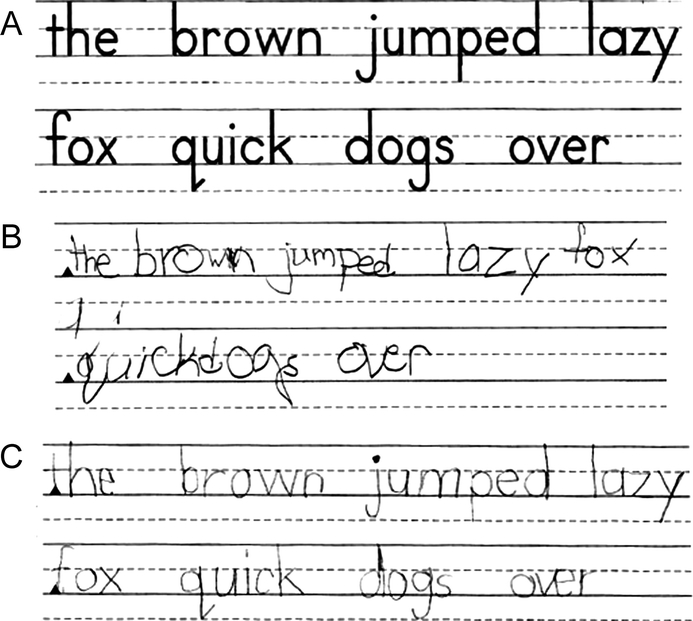
Figure 1 Handwriting samples from subjects with autism spectrum disorders (ASD)
Subjects copied the top sample (A). The ASD group consisted of children with a range of handwriting skills. Samples are from one of the lower scoring subjects with ASD (B) and from a higher scoring subject from the ASD group (C).
Subjects’ motor skills were assessed using the Revised Physical and Neurological Examination for Subtle (Motor) Signs (PANESS).24 The PANESS consists of several categories, including stressed gaits, balance, and timed movements. Stressed gait tasks include heel walking, toe walking, walking on the sides of the feet, and tandem walking. Balance tasks require standing and hopping on one foot. Timed movement tasks include repetitive movements (hand patting, finger tapping, foot tapping) and patterned movements (hand pronation-supination, finger apposition, heel-toe tapping). In previous studies, children with ASD have performed worse on the PANESS relative to controls.4,25,26
Subjects also underwent the Block Design test, a core subtest of the WISC-IV that assesses visuospatial abilities. For this test, subjects were timed as they reconstructed a series of complex designs by properly assembling a set of blocks whose surfaces are components of the larger patterns. Previous studies have demonstrated that subjects with ASD perform better (i.e., faster) than controls on this task. This is thought to be due to a local visuospatial bias in subjects with ASD, which gives them a superior ability to segment objects into components.27
Analysis.
Handwriting samples were scored according to the Minnesota Handwriting Assessment scoring protocol.22 Letters were scored on an individual basis in 5 categories:
Category 1: Legibility.
Letters must be present, recognizable out of context, have all parts complete, and be lowercase. If these criteria are not met, the letter is marked as an error in all 5 categories.
Category 2: Form.
Overall letter quality must be good. Letters must not have gaps or extensions greater than 1/16 of an inch. Curved segments cannot have sharp points, and pointed segments cannot be curved. Letters must not contain extra lines.
Category 3: Alignment.
Letters must rest within 1/16 of an inch above or below the baseline.
Category 4: Size.
The tops of letters with ascenders (e.g., k) must be within 1/16 of an inch of the top solid line. The tops of letters without ascenders (e.g., a) must be within 1/16 of an inch of the middle dotted line. The bottoms of letters with tails (e.g., g) must be within 1/16 of an inch of the bottom dotted line.
Category 5: Spacing.
Letters within words can be neither touching nor over ¼ of an inch apart. The distance between words must be at least ¼ of an inch.
In addition to the 5 qualitative categories, subjects also received a rate score, earning 1 point for each letter completed within the first 2.5 minutes of the assessment. Combining the 5 qualitative scores with the rate score, each of the 34 letters could earn up to 6 points, for a maximum total score of 204.
There are limitations to the assessment’s accuracy; imprecise measurements and inconsistencies with judgment of legibility and form quality are possible. To minimize these errors, 2 raters, both blind to group classifications, independently scored each sample, and the averages of these scores were used in the analyses. Scoring between our raters was reliable, with high intraclass correlation coefficients for total score (0.975) as well as form score (0.909), the most qualitative subscore in the assessment.
Mean total handwriting scores, as well as mean scores in the 5 qualitative categories and rate, were compared between ASD and control groups with Student t tests. Student t tests were also used to compare age, FSIQ, PRI, Block Design scores, and PANESS scores between the 2 groups. Within- and across-group stepwise multiple regressions were performed with handwriting scores as the dependent variable and age, gender, FSIQ, Block Design scores (i.e., visuospatial ability), and PANESS scores (i.e., motor function) as predictor variables.
RESULTS
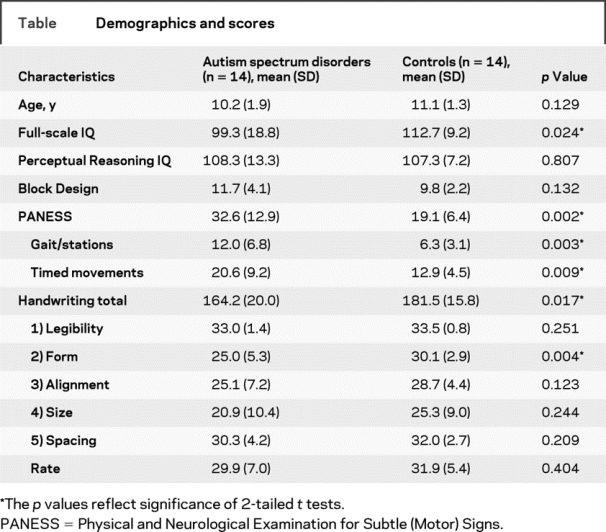
There was no significant difference between groups in age, PRI, or Block Design score. Consistent with previous studies, a significant difference was found for performance on the PANESS, with the control group performing better overall (i.e., earning lower scores) than the ASD group, as well as specifically performing better in the gait/stances and timed movements subcategories (table).
Table Demographics and scores
Children within the ASD group demonstrated a range of handwriting abilities; figure 1 shows one low-scoring ASD sample and one high-scoring sample. Overall, total handwriting scores were lower in the ASD group than the control group (p = 0.025, figure 2). Within the assessment’s subcategories, ASD subjects scored lower in form (p = 0.006, figure 2), but no group differences were found for any other category (table). Figure 3 shows examples of common ASD form errors, such as sharp points in sections that should be curved and large extensions, compared with performance from control subjects. The average form score for the ASD group was 24, which is below that previously reported for “somewhat below average” 6- to 8-year-old typically developing children.22
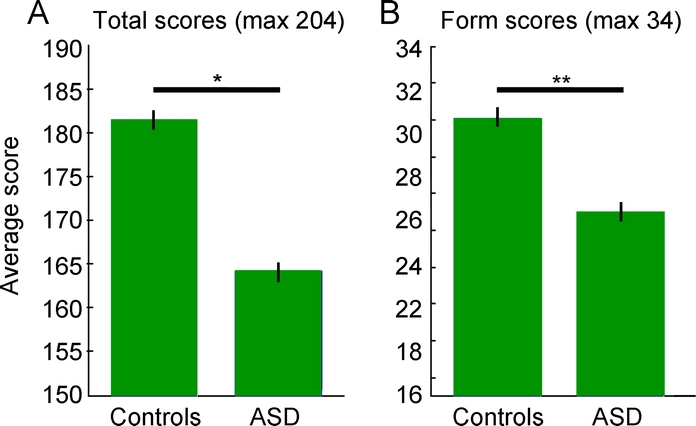
Figure 2 Average total and form handwriting scores across groups
The control group averaged significantly higher total (A) and form (B) handwriting scores than did the autism spectrum disorders (ASD) group. Error bars represent standard error (*p < 0.02, **p < 0.01).
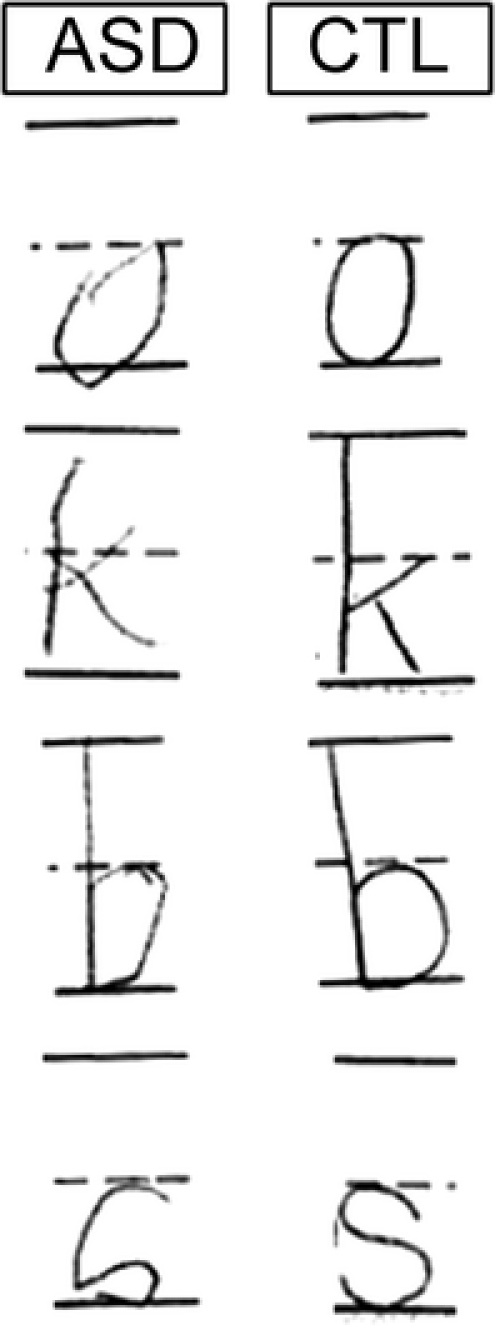
Figure 3 Examples of autism spectrum disorders (ASD) form errors
Examples of common form errors demonstrated by subjects with ASD and well-formed corresponding letters by control subjects (CTL). Some featured errors included sharp points in sections that should be curved (o and s), extensions greater than 1/16 of an inch (b), and generally poor quality (k).
Stepwise multiple regressions were performed with age, gender, FSIQ, Block Design score, and PANESS total score or PANESS timed movement score as predictors for handwriting scores. PANESS timed movement scores were the strongest predictors of handwriting performance within the ASD group (e.g., form: R2 = 0.52, p = 0.004; total: R2 = 0.56, p = 0.002). The PANESS total score was also significantly predictive of handwriting scores, though slightly less so than the timed movement component. Figure 4 shows the relationship between the PANESS timed movement score and total handwriting score for ASD subjects and controls. Controls had a truncated range, since they performed well on both tests, and therefore showed no significant relationship, whereas the ASD group showed a clear relationship between these parameters.
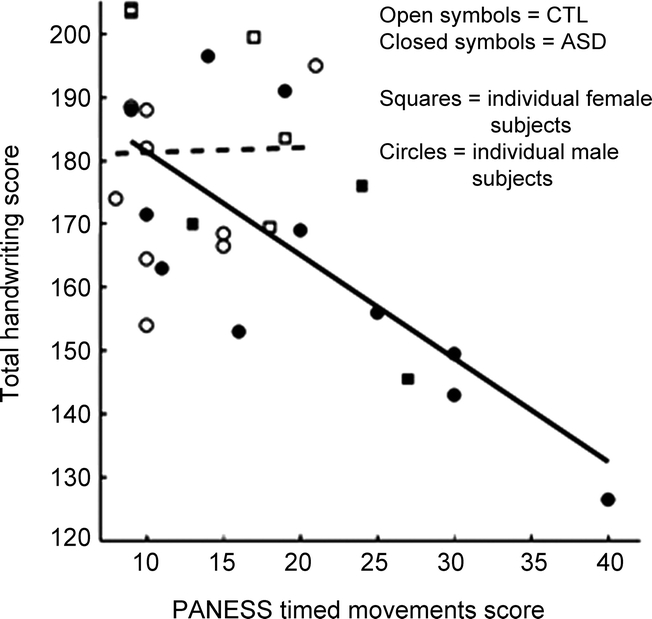
Figure 4 Physical and Neurological Examination for Subtle (Motor) Signs (PANESS) scores predict overall handwriting scores in subjects with autism spectrum disorders (ASD)
Only within the ASD group, PANESS timed movement scores predicted total handwriting scores (R2 = 0.56, p = 0.002). Higher handwriting scores represent better performance, while higher PANESS scores represent worse performance. Solid line represents ASD group’s least squares fit; dashed line represents control group’s fit. CTL = controls.
The only parameter to predict handwriting scores within the control group was gender, which predicted form and alignment performance (form: R2 = 0.32, p = 0.036; alignment: R2 = 0.31, p = 0.040). In these categories control girls performed better than boys (mean ± standard error of form: girls = 32.20 ± 0.68, boys = 28.89 ± 0.96, p = 0.036; alignment: girls = 31.90 ± 01.35, boys = 26.94 ± 1.40, p = 0.040). Within the ASD group, there was no significant difference in handwriting scores based on gender.
DISCUSSION
We show that children with ASD have lower overall quality of handwriting related to motor difficulties that may impede the proper formation of letters. While their overall quality is worse, children with ASD are able to align, size, and space their letters as well as control children.
Despite its inherent qualitative nature, the Minnesota Handwriting Assessment has been praised as a strong tool for evaluating handwriting. The test yields both high interrater and intrarater reliability.23 Furthermore, detailed training and practice scoring provided by the manual, as well as the use of ruler measurements to guide scoring, uniquely improve assessment. In a review of handwriting tests, the Minnesota Handwriting Assessment was described as a tool that “is easy to score and administer and yields a more quantitative result than most handwriting assessments.”28 The test also has strong construct validity, successfully predicting subjects who are subjectively labeled by their teachers as having “good” or “bad” handwriting.1
We found that individuals with ASD were not worse than control subjects at aligning their letters on the specified lines or sizing their letters to match the sample. These features are specified in the task directions and are the most dependent on attending to the task. The lack of difference in performance within these realms strongly suggests that the ASD group attended to the task’s directions as well as the control group.
Although there was no difference in rate scores between the ASD and control groups, we cannot conclude that children with ASD write at the same rate as control children. In line with the Minnesota Handwriting Assessment scoring, subjects only began to lose points for rate if they did not complete the test within 2.5 minutes. Almost all subjects (10/12 control, 9/12 ASD) completed the test within the time limit, so we cannot assess rate differences within these subjects (e.g., a subject who took 1 minute to complete the test received the same rate score as a subject who took 2 minutes). Rather than setting a predetermined time limit, future studies should look for group differences in average time for completion.
Previous studies have found that individuals with autism are perceptually biased toward local features, as opposed to control subjects, who are biased toward global features. The Block Design test is a classic task used to demonstrate this bias, as subjects with ASD reproduce the patterns more quickly than control subjects.27,29–32 It is hypothesized that this superior performance is linked to an improved ability to segment the patterns (i.e., see the local components) and in turn more easily construct the patterns from smaller pieces. We hypothesized that visuospatial biases may influence handwriting by affecting subjects’ visual representations of letters. We found, however, that visual biases, as determined by Block Design scores, did not predict handwriting performance. Since our methods only analyzed the completed handwriting sample, it is possible that visual biases for local features may have influenced the strategy of individuals with ASD. This possibility is supported by a study that showed that when boys with ASD copied drawings of objects they were more likely than controls to begin by drawing local features rather than the overall outline and they tended to continue drawing in a piecemeal fashion.12 Individuals with ASD may use a more local strategy for drawing letters, or it is possible that letters are so commonly viewed that they are visually processed more automatically, not requiring the build up of local features into a whole that more novel visual stimuli require. This seems likely given that our subjects were all fluent readers. Either way, within our sample the final quality of handwriting was not affected by visuospatial biases. Other senses, such as proprioception, were not examined; how other sensory issues contribute to handwriting in autism should be examined in future studies.
A number of studies have demonstrated that individuals with autism have problems with motor functions.4–7 The PANESS in particular has been used to demonstrate basic motor impairments in children with ASD relative to controls.4,25,26 Consistent with these results, our ASD group scored significantly worse on the PANESS than our control group, demonstrating general motor impairments.
Unlike visuospatial abilities, within the ASD group motor performance predicted overall handwriting quality, as well as performance within a number of the assessment’s subcategories, suggesting that general difficulties with motor control contribute to lower quality handwriting. These results suggest that without steady motor control one cannot accurately and fluidly control hand and arm movements. Asperger noted such a relationship when commenting on one of his original patients: “this motorically clumsy child had atrocious handwriting ... The pen did not obey him.”3 Within the PANESS, performance on timed movements—the movements requiring the greatest fine motor control—was specifically linked to handwriting performance, which corroborates findings suggesting a relationship between complex finger movement abilities and handwriting.33 No such relationship was found within the control group, likely due to the group’s lack of variability in scores. While within the control group girls performed better than boys in some categories, no gender difference was found within the ASD group, possibly due to motor impairments overshadowing gender effects.
Performance in form observed in our ASD group, which had an average age of 10.2 years, is below that previously reported in younger typically developing children: “somewhat below average” 6- to 7-year-olds scored between 25 and 29 and 7- to 8-year-olds between 28 and 30.22 Despite being older than these groups and being intelligence matched to our older control group, our subjects with ASD averaged a form score of only 24. This suggests that handwriting impairments in children with autism do not simply reflect a developmental delay. These results are only generalizable to individuals of average intelligence whose primary deficit is autism.
Our finding that subjects with ASD did not size their letters differently than controls is inconsistent with the previous result that adults with ASD demonstrate macrographia, sizing letters larger than controls.17 In our task, however, instructions specified that letter size match the sample, while in the previous study size was not specified. Furthermore, given that the previous study was performed in adults, subjects may have learned to draw letters larger to compensate for difficulties with fine motor control. Our younger subjects may not yet have adapted this strategy or could not use it given that the task instructions specified letter size. Even within the adults study, the authors commented that many handwriting samples from subjects with ASD were subjectively hard to read, and they speculated that this poorer quality and macrographia were related to motor coordination impairments.
While unable to use a compensatory sizing strategy, observations suggest that our ASD subjects exhibited other compensatory motor techniques. For example, 2 of the highest scoring subjects with ASD gripped their dominant forearms with their nondominant hands to help steady their movements, a strategy they were taught in school. These observations, in combination with the result that motor abilities strongly predict handwriting performance, suggest that therapies targeting motor control are the best approach to improving handwriting in individuals with autism.
ACKNOWLEDGMENT
The authors thank all participants in this research study, as well as Lauren Dowell and Jessica O’Brien for their assistance in subject recruitment and data collection.
DISCLOSURE
C.T. Fuentes reports no disclosures. Dr. Mostofsky served on a scientific advisory for Bristol-Myers Squibb; serves on the editorial board of Neurocase; has received speaker honorarium from The National Academy of Neuropsychology; and receives research support from the NIH [NINDS 5 R01 NS047781-04 (PI), NINDS R01 NS048527-04 (PI), NIMH 5 R01 MH078160-03 (PI), and NICHD P50 HD052121-03 (Co-I)] and from Autism Speaks. Dr. Bastian reports no disclosures.
Address correspondence and reprint requests to Dr. Amy Bastian, Kennedy Krieger Institute, 707 N Broadway–G05, Baltimore, MD 21205 bastian@kennedykrieger.org
Supported by an Autism Speaks Pre-Doctoral Fellowship (A.J.B. and C.T.F.) and NIH Grant R01 NS048527 (S.H.M.).
Disclosure: Author disclosures are provided at the end of the article.
Received April 24, 2009. Accepted in final form August 7, 2009.
REFERENCES
- 1.Cornhill H, Case-Smith J. Factors that relate to good and poor handwriting. Am J Occup Ther 1996;50:732–739. [DOI] [PubMed] [Google Scholar]
- 2.Feder KP, Majnemer A. Handwriting development, competency, and intervention. Dev Med Child Neurol 2007;49:312–317. [DOI] [PubMed] [Google Scholar]
- 3.Frith U. Translation and annotation of “autistic psychopathy” in childhood by H. Asperger. In: Autism and Asperger Syndrome. Cambridge, UK: Cambridge University Press; 1991:37–92. [Google Scholar]
- 4.Jansiewicz EM, Goldberg MC, Newschaffer CJ, Denckla MB, Landa R, Mostofsky SH. Motor signs distinguish children with high functioning autism and Asperger’s syndrome from controls. J Autism Dev Disord 2006;36:613–621. [DOI] [PubMed] [Google Scholar]
- 5.Manjiviona J, Prior M. Comparison of Asperger syndrome and high-functioning autistic children on a test of motor impairment. J Autism Dev Disord 1995;25:23–39. [DOI] [PubMed] [Google Scholar]
- 6.Ghaziuddin M, Butler F. Clumsiness in autism and Asperger syndrome: a further report. J Intellect Disabil Res 1998;42:43–48. [DOI] [PubMed] [Google Scholar]
- 7.Noterdaeme M, Mildenberger K, Minow F, Amorosa H. Evaluation of neuromotor deficits in children with autism and children with a specific speech and language disorder. Eur Child Adolesc Psychiatry 2002;11:219–225. [DOI] [PubMed] [Google Scholar]
- 8.Biklen D. Autism and the Myth of the Person Alone. New York: NYU Press; 2005. [Google Scholar]
- 9.Weimer AK, Schatz AM, Lincoln A, Ballantyne AO, Trauner DA. “Motor” impairment in Asperger syndrome: evidence for a deficit in proprioception. J Dev Behav Pediatr 2001;22:92–101. [DOI] [PubMed] [Google Scholar]
- 10.Molloy CA, Dietrich KN, Bhattacharya A. Postural stability in children with autism spectrum disorder. J Autism Dev Disord 2003;33:643–652. [DOI] [PubMed] [Google Scholar]
- 11.Dakin S, Frith U. Vagaries of visual perception in autism. Neuron 2005;48:497–507. [DOI] [PubMed] [Google Scholar]
- 12.Booth R, Charlton R, Hughes C, Happe F. Disentangling weak coherence and executive dysfunction: planning drawing in autism and attention-deficit/hyperactivity disorder. Philos Trans R Soc Lond B Biol Sci 2003;358:387–392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Beer KE. The Beery-Buktenica Developmental Test of Visual-motor Integration (VMI), 4th ed. Parsippany, NJ: Modern Curriculum Press; 1997. [Google Scholar]
- 14.Wechsler D. Wechsler Intelligence Scale for Children, 4th ed. San Antonio, TX: Psychological Corporation; 2003. [Google Scholar]
- 15.Mayes SD, Calhoun SL. Ability profiles in children with autism: influence of age and IQ. Autism 2003;7:65–80. [DOI] [PubMed] [Google Scholar]
- 16.Mayes SD, Calhoun SL. Learning, attention, writing, and processing speed in typical children and children with ADHD, autism, anxiety, depression, and oppositional-defiant disorder. Child Neuropsychol 2007;13:469–493. [DOI] [PubMed] [Google Scholar]
- 17.Beversdorf DQ, Anderson JM, Manning SE, et al. Brief report: macrographia in high-functioning adults with autism spectrum disorder. J Autism Dev Disord 2001;31:97–101. [DOI] [PubMed] [Google Scholar]
- 18.Mottron L. Matching strategies in cognitive research with individuals with high-functioning autism: current practices, instrument biases, and recommendations. J Autism Dev Disord 2004;34:19–27. [DOI] [PubMed] [Google Scholar]
- 19.Lord C, Risi S, Lambrecht L, et al. The autism diagnostic observation schedule–generic: a standard measure of social and communication deficits associated with the spectrum of autism. J Autism Dev Disord 2000;30:205–223. [PubMed] [Google Scholar]
- 20.Lord C, Rutter M, Le CA. Autism Diagnostic Interview–Revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord 1994;24:659–685. [DOI] [PubMed] [Google Scholar]
- 21.Reich W, Welner Z, Herjanic B. The Diagnostic Interview for Children and Adolescents–Revised. North Tonawanda, NY: Multi-Health Systems; 1997. [Google Scholar]
- 22.Reisman J. Minnesota Handwriting Assessment. San Antonio, TX: Psychological Corporation; 1999. [Google Scholar]
- 23.Reisman JE. Development and reliability of the research version of the Minnesota Handwriting Test. Phys Occup Ther Pediatr 1993;13:41–55. [Google Scholar]
- 24.Denckla MB. Revised Neurological Examination for Subtle Signs (1985). Psychopharmacol Bull 1985;21:773–800. [PubMed] [Google Scholar]
- 25.Mostofsky SH, Burgess MP, Gidley Larson JC. Increased motor cortex white matter volume predicts motor impairment in autism. Brain 2007;130:2117–2122. [DOI] [PubMed] [Google Scholar]
- 26.Mandelbaum DE, Stevens M, Rosenberg E, et al. Sensorimotor performance in school-age children with autism, developmental language disorder, or low IQ. Dev Med Child Neurol 2006;48:33–39. [DOI] [PubMed] [Google Scholar]
- 27.Shah A, Frith U. Why do autistic individuals show superior performance on the block design task? J Child Psychol Psychiatry 1993;34:1351–1364. [DOI] [PubMed] [Google Scholar]
- 28.Feder KP, Majnemer A. Children’s handwriting evaluation tools and their psychometric properties. Phys Occup Ther Pediatr 2003;23:65–84. [PubMed] [Google Scholar]
- 29.Shah A, Frith U. An islet of ability in autistic children: a research note. J Child Psychol Psychiatry 1983;24:613–620. [DOI] [PubMed] [Google Scholar]
- 30.Ropar D, Mitchell P. Susceptibility to illusions and performance on visuospatial tasks in individuals with autism. J Child Psychol Psychiatry 2001;42:539–549. [PubMed] [Google Scholar]
- 31.Caron MJ, Mottron L, Rainville C, Chouinard S. Do high functioning persons with autism present superior spatial abilities? Neuropsychologia 2004;42:467–481. [DOI] [PubMed] [Google Scholar]
- 32.Caron MJ, Mottron L, Berthiaume C, Dawson M. Cognitive mechanisms, specificity and neural underpinnings of visuospatial peaks in autism. Brain 2006;129:1789–1802. [DOI] [PubMed] [Google Scholar]
- 33.Berninger VW, Rutberg J. Relationship of finger function to beginning writing: application to diagnosis of writing disabilities. Dev Med Child Neurol 1992;34:198–215. [DOI] [PubMed] [Google Scholar]