

Abstract
The 20th century in the United States (U.S.) has experienced a dramatic increase in life expectancy among adult men and women, an increase unprecedented in the history of this country. As a result, the pattern of disease and conditions most responsible for death in the U.S. shifted during the past century from infectious diseases and unintentional injuries to the current array of the leading causes of mortality dominated by the chronic diseases. During this same period, daily lifestyle dramatically shifted from a life full of active living to one of inactivity. The argument has been made that in the case of human beings, there has been little or no change in our genotype within the past 50 years. However, there have been major changes documented in the living environment among economically developed societies during this same time period. Through the collection of epidemiologic, clinical, and experimental findings, evidence exists to suggest that physical inactivity is associated with the onset of chronic diseases of our day. Trends in physical inactivity evident through the monitoring of transport, recreational, sport, and purposeful activity have demonstrated that the current lifestyle of the 21st century has contributed substantially to the chronic disease burden in the U.S. and elsewhere. By addressing the domains that influence physical activity behaviors including the environment (both physical and social/cultural), health systems access, and behavioral correlates of physical activity and inactivity, the current chronic disease crisis can potentially be addressed.
Keywords: exercise, inactivity, mortality, trends, community health
Achievements in Public Health in the 20th Century
The 20th century in the United States (U.S.) has experienced a dramatic increase in life expectancy among adult men and women, an increase unprecedented in the history of this country. This major health improvement was primarily due to the control of infectious diseases, improved sanitation (i.e., better water delivery and sewage disposal) and improvements in the general living and working environments of people. As a result, the pattern of disease and conditions most responsible for death in the U.S. shifted during the past century from infectious diseases and unintentional injuries to the current array of the leading causes of mortality in the 21st century: coronary heart disease (CHD); cancers; stroke; chronic obstructive pulmonary disease (COPD).1 These so-called leading causes of death have been clearly linked to what some have referred to as the Actual Causes of Death; that is, those factors that through epidemiologic, clinical, and experimental study have demonstrated an association through biological mechanisms with the occurrence of these leading causes of death.2 Recent investigators have identified the following factors as the actual causes of death in the order of effect: tobacco use, physical inactivity/poor diet; alcohol (chronic and acute use), all of which are modifiable lifestyle factors; and infectious agents.2
During this same period, daily lifestyle dramatically shifted from a life full of active living to one of inactivity.3 The extent to which the chronic diseases have emerged as the leading causes of death has paralleled the increased pattern of inactivity.4 Insights into the possible correlates of these changes in active living are the subject of the following sections of this paper.
Evolution of physical inactivity
Historically, at least from around 10,000 years ago, human beings established themselves as primary hunters and gatherers in order to sustain themselves.3 This type of lifestyle required a very high level of physical activity in association with the hunting of animals for food and the gathering of other foodstuffs such as berries, roots, nuts, etc. in order to maintain life.5 As human beings further adapted to their environment and created implements and simple machines to assist them in the cultivation of foodstuffs, this agrarian lifestyle was still supported by a high to moderate level of physical activity up until the middle of the 18th century. From the late 18th century and through the 19th century, industrialization took place in most of Western Europe, North America, Asia, and North Africa/Mediterranean.4 With the advent of greater mechanization, which generally required lower levels of daily physical activity, came increasingly greater levels of inactivity or sedentary behavior, particularly among people living in more urban areas.5 Finally, during the 20th century, and particularly following World War II, most of the economically developed world shifted to what is now a highly mechanized, commuter/computer-driven world where daily living is comprised of low levels of physical activity and high levels of physical inactivity, supplemented by occasional bouts of recreational, sport, and leisure activities.5
Defining the Chronic Disease Epidemic: Changing Environment acting upon Pre-existing Genes
In the study of genetics the phenotype is an expression of the interaction of the genotype of an organism and its physical environment.6 The argument has been made that in the case of human beings, there has been little or no change in our genotype within the past 50 years.7 However, there have been major changes documented in the living environment among economically developed societies during this same time period.7 Thus, evidence supports that it is the environmental factors leading to a more physically inactive lifestyle among human beings which has brought about an unhealthy gene expression that leads to the common health disorders currently encountered by human beings in these emergent inactive cultures.7 Through a recent systematic review, these include: coronary heart disease, osteo-arthritis pain, lower health-related quality of life, cardiac arrhythmias, menopausal symptoms, breast cancer, obesity, colon cancer, osteoporosis, congestive heart failure, peripheral vascular disease, depression, physical frailty, digestive problems, gallbladder disease, respiratory problems, hypertriglyceridemia, sarcopenia, hypercholesterolemia, sleep apnea, hypertension, stroke, low blood high density lipoprotein cholesterol (HDLc), and type 2 diabetes mellitus (Type II DM).8
Evidence that Environmental (physical inactivity)-Gene interaction produces chronic disease
A continuing evidence-base has grown demonstrating the powerful effect that physical inactivity has on genetic predispositions and the onset of chronic disease.7 Significant associations have been shown between physical activity and the prevention of type II DM. Hu, 1999 has demonstrated among siblings with a parental history of type 2 DM that their risk of this disease can be reduced by as much as 40% by being in the top 20% for physical activity.9 This powerful metabolic effect of regular physical activity has repeatedly been shown in controlled studies. One such seminal study among masters athletes showed that these athletes manifested a deterioration of glucose tolerance in response to just 10 days of doing no exercise, with a rebound to near baseline levels of glucose tolerance and insulin response following just one bout of exercise.10 Others have demonstrated that physical inactivity rapidly produces insulin insensitivity.11 Regular physical activity has also been demonstrated to improve lipid metabolism with powerful adjustments coming from just one exercise bout.12 For example Zhang, et al.12 showed that engaging in a moderate- to-vigorous intensity exercise bout prior to a fatty meal raised blood HDLc and HDL2c by 10%. In addition, a concomitant improvement in triglycerides clearance from the blood was demonstrated among subjects who engaged in a single exercise bout prior to a fatty meal.12 These studies employed a rather vigorous bout of activity to bring about these changes. However more recent studies, such as those carried out by Olsen, et al., 200813 in Denmark, examined the effects of rather light- to-moderate intensity physical activity on metabolic measures and have found rather striking changes. Using pedometers to assess the number of steps per day, the study investigators recruited young adults to wear a pedometer for two weeks at baseline and undergo metabolic testing (i.e., fasting blood glucose, insulin levels) as well as a magnetic resonance imaging (MRI) assessment of their intra-abdominal fat density. Median steps at baseline were 10,053 steps per day. The subjects were then asked to reduce their daily steps for the next two (2) weeks to a median of 1381 steps per day. Intra-abdominal fat mass went from a mean volume of 693 mL at baseline to 740 mL following the two week restriction in daily steps (p< .05). These findings suggest that even subtle changes in activity have a rather profound short term effect on body composition and the metabolic pathways that support mobilization and utilization of energy stores.13
Recently a body of evidence has emerged that suggest that daily sitting for transport, television (TV) watching, computer-based work, sedentary entertainment, and other sedentary activities are associated with total mortality, CHD, Type II DM, risk for metabolic syndrome, and obesity.14 Furthermore experimental studies examining the physiologic and biochemical responses to inactivity have shown significant perturbations in the metabolic pathways associated with the above disease outcomes.14 This collection of epidemiologic, clinical, and experimental findings have provided evidence that the onset of chronic diseases has increased due to negative lifestyle behaviors without an appreciable change in the human genome during the same time period.7
The Transitions in Physical Activity to Physical Inactivity
When attempting to explain why current levels of physical activity are so low across the population and levels of inactivity so high, one needs to consider the possibility that the social and physical environments have changed dramatically. Data from the National Transportation Surveys conducted in the U.S. in 1969 and 200115 demonstrate that the percent of trips made from home by automobile have increased 10 fold from 1969 through 2001.15 Conversely, from the same data source, the percent of trips made from home by walking have decreased dramatically over the same period.16 Other data that supports the notion that we are becoming a more sedentary population is derived from the national Youth Risk Behavior Surveillance System (YRBSS).17 Figure 1 illustrates that the percentage of high school students who attended physical education classes daily from 1991 to 2007 decreased or remained stable among select subgroups of the high school population in the United States.17 From these same data, the percentage of students enrolled in physical education class drops precipitously with each increasing grade level throughout high school. This inverse trend exists in all youth, with girls, particularly African-Americans and Latinas, showing the steepest declines. Absent from communities is walking to school as well as other physically active routines of daily life such as home maintenance, transport activities, and active recreation that collectively contribute to the decline in physical activity levels.17, 18
Figure 1.
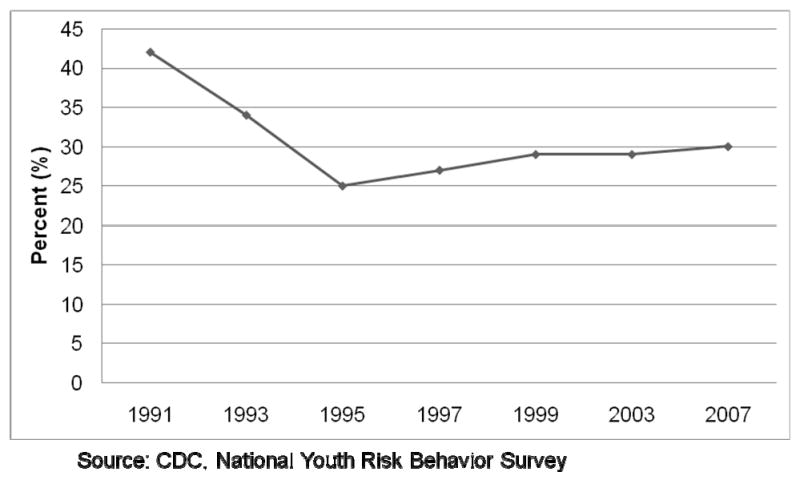
Trends in daily attendance in physical education classes among U.S. high school students- 1991-2007. (Source: Youth Risk Behavior Surveillance System, see Reference #17)
Essentially, opportunities for physical activity have been systematically engineered out of our daily lives. Consider the case of the old order Amish compared to their culturally main-stream neighbors. Using highly technical pedometers (accelerometers), Bassett and colleagues19 measured the daily activity of men and women living in an Amish community in Canada (North America). The International Physical Activity Questionnaire (IPAQ), a standard physical activity questionnaire, was used to comment respondents about all physical activities including household, occupational, transport, recreational, sport, and exercise. The IPAQ scores (MET-min wk-1 × 1000) were 10 fold higher among the Amish compared to mainstream respondents in Colorado.19 The accelerometer data yielded even more dramatic differences with the Amish men and women achieving an average of 16,000 steps per day vs. 6,000 steps per day for mainstream North American men and women.
The benefits of regular physical activity translate into both health and fitness benefits. Many of the health benefits have already been mentioned including the prevention of CHD, stroke, hypertension, adverse blood lipid levels, Type 2DM, colon and breast cancer, weight gain, depression, and improved cognitive function and bone health.8 The fitness benefits that extend to children, youth, and adults include improved cardiorespiratory and muscular fitness, flexibility, balance, and favorable body composition.8
Trends in the Prevalence of Physical Inactivity and Recommended Levels of Physical Activity
Figure 2 illustrates that starting in approximately 1996, there appears to have been a slight downturn in prevalence of physical inactivity among adults aged 18 and older.20 This positive finding is evident among both men and women but does not appear to transcend all race/ethnic and socioeconomic (SES) groups in the U.S., suggesting continuing disparities among these groups relative to physical inactivity and activity. It is rather curious that this reduction in self-reported physical inactivity among the majority of Americans started during the year that the first Surgeon General's Report on Physical Activity and Health was released.21 This perhaps can be explained by an actual increase in the number of Americans who actually became more active in response to the promotion of the Surgeon General's recommendations, or perhaps respondents were simply more aware of the social pressure of not reporting themselves as ‘couch potatoes’.
Figure 2.
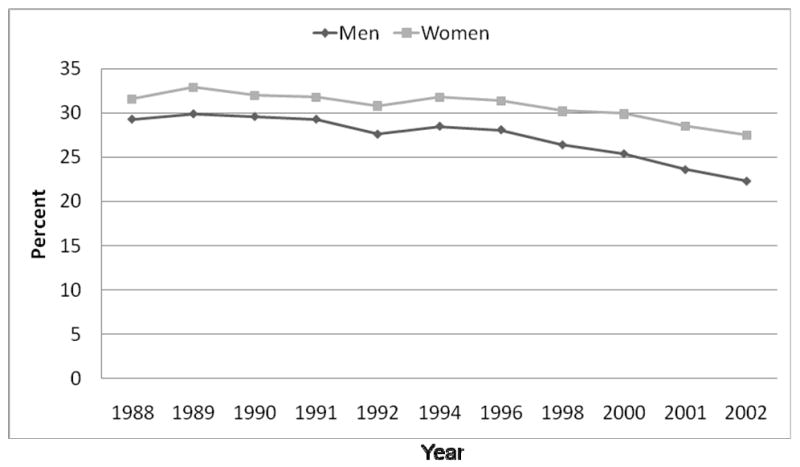
Trends in leisure-time physical inactivity among adults, United States, 1994-2002. (Source: Behavioral Risk Factor Surveillance System, see reference # 20).
The most recent estimates of physical activity levels seen among U.S. adults and youth are abstracted from data collected in 2007.22, 17 Among adults, using the recommendations established by the American College of Sports Medicine and the American Heart Association,23 49% of adults met physical activity recommendations, while those engaging in insufficient physical activity is 27%, with 24% for those who report being inactive (See Figure 3).24
Figure 3.

Physical activity patterns among adults, United States, 2005, 2007. (Source: Behavioral Risk Factor Surveillance System, see reference # 23).
Investigators have successfully identified a number of key correlates or determinants of physical activity, the factors that are associated with persons being more likely to adopt regular physical activity. These moderators and mediators of physical activity can be classified into at least three domains: 1). environmental, both physical and social/cultural; 2). health system including issues around access, quality of service, and safety; and 3). intra-individual factors such as self-efficacy, cognition, and social support.25 Evidence suggests that when these three domains are accounted for in the development and delivery of physical activity interventions, there exists a greater likelihood that people will become more physically active.26, 27
Indicators of a Healthy Community
Academicians and practitioners in community health have sought to identify the indicators of a healthy community. Among these indicators has emerged an understanding that a community is healthier if children and youth are engaged in active trips to school and active play outdoors, and older adults have increased outdoor interaction and mobility through active transport and active recreation.28 These types of indicators have been shown to be successfully implemented in communities where there is strong advocacy for active living environments. These advocacy efforts often result in environments that: 1) provide safe sidewalks and bikeways; 2) support attractive and safe public places; 3) foster the presence of people; 4) provide facilities linked to neighborhoods; 5) provide support for neighborhood schools and parks; 6) support preservation of green space; and 7) create a sense of community, permanence, and PLACE.29
Summary
Despite little or no change in the human genome within the past 100 years, there has been an unprecedented shift in morbidity and mortality among the world's economically developed populations from primarily infectious conditions to chronic diseases. Likewise, lifestyles and living environments have shifted from physical activity-dependent to inactivity-dependent patterns, particularly among peoples in countries like the U.S. These lifestyle transitions from physical activity to inactivity have been accelerated by the systematic reordering of community structures, changes in land-use, commuting behaviors, and greater dependence on technology for living. Patterns of physical inactivity and activity have shown little improvement since the release of the Surgeon General's Report on Physical Activity and Health in 1996. Evidence exists that the physiologic and metabolic consequences of inactivity and low physical activity continue to drive our current chronic disease epidemic. An increasing evidence-base points to successful methods that can alter the way 21st Century people live by introducing more opportunities for active living through improved urban design and land use and by providing effective methods of physical activity promotion through improved policy and environmental efforts at the level of structures, agencies, and institutions.
Acknowledgments
This paper represents material that was presented at the Lifestyle Conference held at Arizona State University, Mesa, AZ on February 28-29, 2008.
References
- 1.Granados JAT. Increasing mortality during expansions of the U.S. economy, 1900-1996. International Journal of Epidemiology. 2005;34:1194–1202. doi: 10.1093/ije/dyi141. [DOI] [PubMed] [Google Scholar]
- 2.Mokdad AH, Marks JS, Stroup DF, Gerbering JL. Actual causes of death in the United States, 2000. JAMA. 2004;261(10):1238–1245. doi: 10.1001/jama.291.10.1238. [DOI] [PubMed] [Google Scholar]
- 3.Walker AR, Walker BF, Adam F. Nutrition, diet, physical activity, smoking, and longevity: from primitive hunter-gatherer to present passive consumer, how far can we go? Nutrition. 2003;19:169–173. doi: 10.1016/s0899-9007(02)00948-6. [DOI] [PubMed] [Google Scholar]
- 4.Gage TB. Are modern environments really bad for us?: revisiting the demographic and epidemiologic transitions. American Journal of Physical Anthropology. 2005;41(Suppl):96–117. doi: 10.1002/ajpa.20353. [DOI] [PubMed] [Google Scholar]
- 5.Cordain L, Gotshall RW, Eaton SB, Eaton SB., III Physical activity, energy expenditure and fitness: an evolutionary perspective. International Journal of Sports Medicine. 1998;19:328–335. doi: 10.1055/s-2007-971926. [DOI] [PubMed] [Google Scholar]
- 6.Beaudet AL, Scriver CR, Sly WS, Valle D. Genetics, biochemistry, and molecular basis of variant human phenotypes. In: Scriver CR, Beaudet AL, Sly WS, Valle D, Stanbury JB, Wyngaarden JB, Fredrickson DS, editors. The Metabolic and Molecular Bases of Inherited Disease. 7th. Vol. 1. New York: McGraw-Hill; 1995. p. 79. [Google Scholar]
- 7.Chakravarthy MV, Booth FW. Eating, exercise, and “thrifty” genotypes: connecting the dots toward and evolutionary understanding of modern chronic diseases. JAppl Physiol. 2004;96:3–10. doi: 10.1152/japplphysiol.00757.2003. [DOI] [PubMed] [Google Scholar]
- 8.Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008. Washington, DC: U.S. Department of Health and Human Services; 2008. [DOI] [PubMed] [Google Scholar]
- 9.Hu FB, Sigal RJ, Rich-Edwards JW, Colditz GA, Solomon CG, Willett WC, Speizer FE, Manson JE. Walking compared with vigorous physical activity and risk of type 2 diabetes mellitus risk in women: a prospective study. JAMA. 1999;282:1433–1439. doi: 10.1001/jama.282.15.1433. [DOI] [PubMed] [Google Scholar]
- 10.Rogers MA, King DS, Hagberg JM, Ehsani AA, Holloszy JO. Effect of 10 days of physical inactivity on glucose tolerance in master athletes. J Appl Physiol. 1990 May;68(5):1833–7. doi: 10.1152/jappl.1990.68.5.1833. [DOI] [PubMed] [Google Scholar]
- 11.Heath GW, Gavin JR, Ponser JM, Hagberg JM, Bloomfield SA, Holloszy JO. Effects of exercise and lack of exercise on glucose tolerance and insulin sensitivity. Journal of Applied Physiology. 1983;55(2):512–517. doi: 10.1152/jappl.1983.55.2.512. [DOI] [PubMed] [Google Scholar]
- 12.Zhang JQ, Thomas TR, Ball SD. Effect of exercise timing on postprandial lipemia and HDL cholesterol subfractions. J Appl Physiol. 85(4):1516–1522. doi: 10.1152/jappl.1998.85.4.1516. [DOI] [PubMed] [Google Scholar]
- 13.Olsen RH, Krogh-Madsen R, Thomsen C, Booth FW, Pedersen BK. Metabolic responses to reduced daily steps in healthy nonexercising men. JAMA. 2008;299(11):1261–1263. doi: 10.1001/jama.299.11.1259. [DOI] [PubMed] [Google Scholar]
- 14.Hamilton MT, Hamilton DG, Zderic TW. Role of low energy expenditure and sitting in obesity, metabolic syndrome, Type 2 diabetes, and cardiovascular disease. Diabetes. 2007;56:2655–2667. doi: 10.2337/db07-0882. [DOI] [PubMed] [Google Scholar]
- 15.Pucher J, Renne JL. Socioeconomics of urban travel: evidence from 2001 NHTS. Transportation Quarterly. 2003;57:49–77. [Google Scholar]
- 16.Ham SA, Macera CA, Lindley C. Trends in walking for transportation in the United States, 1995 and 2001. [February 5, 2008];Prev Chronic Dis. 2005 Oct; serial online. Available from: URL: http://www.cdc.gov/pcd/issues/2005/oct/04_0138.htm. [PMC free article] [PubMed]
- 17.Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, et al. Youth risk surveillance – United States, 2007. MMWR. 2008;57(SS04):1–131. [PubMed] [Google Scholar]
- 18.Ham SA, Martin S, Kohl HW., 3rd Changes in the percentage of students who walk or bike to school- United States, 1969 and 2001. J Phys Act Health. 2008;5(2):205–215. doi: 10.1123/jpah.5.2.205. [DOI] [PubMed] [Google Scholar]
- 19.Bassett DR, Schneider PL, Huntington GE. Physical activity in an Old Order Amish community. Med Sci Sports Exerc. 2004;36:79–85. doi: 10.1249/01.MSS.0000106184.71258.32. [DOI] [PubMed] [Google Scholar]
- 20.CDC. Trends in leisure-time physical inactivity by age, sex, and race/ethnicity – United States, 1994-2004. MMWR. 2005;54:991–4. [PubMed] [Google Scholar]
- 21.US Department of Health and Human Services. Physical Activity and Health: A Report of he Surgeon General. Atlanta, GA: U.S. Dept of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996. [Google Scholar]
- 22.CDC. Prevalence of self-reported physically active adults – United States, 2007. MMWR. 2008;57(48):1297–1300. [PubMed] [Google Scholar]
- 23.CDC. Prevalence of regular physical activity among adults—United States, 2001 and 2005. MMWR. 2007;56(46):1209–1212. [PubMed] [Google Scholar]
- 24.Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, Macera CA, Heath GW, Thompson PD, Bauman A. Physical Activity and Public Health: Updated Recommendation for Adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:01–13. doi: 10.1161/CIRCULATIONAHA.107.185649. [DOI] [PubMed] [Google Scholar]
- 25.Sallis JF, Kraft K, Linton LS. How the environment shapes physical activity: a transdisciplinary research agenda. Am J Prev Med. 2002;22(3):208–210. doi: 10.1016/s0749-3797(01)00435-4. [DOI] [PubMed] [Google Scholar]
- 26.Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, Stone EJ, Rajab MW, Corso P. The effectiveness of interventions to increase physical activity: A systematic review. American Journal of Preventive Medicine. 2002;22(4S):73–107. doi: 10.1016/s0749-3797(02)00434-8. [DOI] [PubMed] [Google Scholar]
- 27.Heath GW, Brownson RC, Kruger J, Miles R, Powell KE, Ramsey LT. The Effectiveness of Urban Design and Land Use and Transport Policies and Practices to Increase Physical Activity: A Systematic Review. Journal of Physical Activity and Health. 2006;1:S55–S71. doi: 10.1123/jpah.3.s1.s55. [DOI] [PubMed] [Google Scholar]
- 28.Metzler M, Kanarek N, Highsmith K, Bialek R, Straw R, Auston I, et al. Community Health Status Indicators Project: the development of a national approach to community health. Prev Chronic Dis. 2008;5(3) www.cdc.gov/pcd/issues/2008/jul/07_0225.htm. [PMC free article] [PubMed]
- 29.Pickett KE, Pearl M. Multilevel analyses of neighborhood socioeconomic context and health outcomes: A critical review. Journal of Epidemiology and Community Health. 2001;55:111–122. doi: 10.1136/jech.55.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]