

Abstract
The melphalan-prednisone regimen has been considered as standard therapy for patients with multiple myeloma (MM) for many years. Recently, high-dose chemotherapy with stem-cell support has extended progression-free survival and increased overall survival, and it is now considered conventional therapy in younger patients. However, most patients relapse and the salvage treatment is not very effective. New active drugs, including immunomodulatory agents, thalidomide (Thal) and lenalidomide, and the proteasome inhibitor bortezomib, have shown promising anti-myeloma activity. These novel treatments are aimed at overcoming resistance of tumour cells to conventional chemotherapy, acting both directly on myeloma cells and indirectly by blocking the interactions of myeloma cells with their local microenvironment and suppressing growth and survival signals induced by autocrine and paracrine loops in the bone marrow. Thal has been widely studied, mostly in combination regimens in patients with relapsed MM and, more recently, in front-line therapy, showing efficacy in terms of response rate and event-free survival. Bortezomib has been found to possess remarkable activity, especially in combination with other chemotherapeutic agents, in relapsed/refractory and newly diagnosed MM, as well as in patients presenting adverse prognostic factors. Lenalidomide, in combination with dexamethasone, is showing high overall response rates in relapsed and refractory MM and promising results also in first-line therapy. In this paper, the results of the most significant trials with Thal, bortezomib and lenalidomide are reported. Several ongoing clinical studies will hopefully allow the identification of the most active combinations capable of improving survival in patients with MM.
Key words: Multiple myeloma, Therapy, Thalidomide, Lenalidomide, Bortezomib
Introduction
Multiple myeloma (MM) is an aggressive and incurable haematological neoplasia, characterised by expansion of malignant plasma cells, which accounts for an estimated 14,000 new cases per year in the USA [1]. For many years, the combination treatment with melphalan-prednisone (MP) has been its conventional chemotherapy, resulting in a median survival of about 3 years.
The frequency of remission, the disease-free survival (DFS) and overall survival (OS) have been improved in patients ≤65 years with the use of first-line high-dose chemotherapy, followed by autologous stem-cell transplantation (ASCT) [2, 3]. Indeed, two large randomised trials have compared this procedure with standard chemotherapy and the overall 5-year survival improved from 12% to 52% in one trial (P=0.03), while the median survival increased from 42 to 54 months in the second trial (P=0.04) [4, 5]. Even so, most patients relapse and further therapies are largely ineffective.
In the past 10 years, new advances have been gained into the understanding of the biologic and molecular mechanisms of MM pathogenesis. Several studies have indeed shown a critical role of the bone marrow microenvironment in the development of this tumour. The interactions of MM cells with stromal cells and extracellular matrix trigger paracrine and autocrine loops of many cytokines involved in MM progression and activate intracellular signal pathways that promote bone destruction as well as survival, proliferation, drug resistance and genomic instability of myeloma cells [6–9].
The identification of these mechanisms has led to the development of novel therapeutic options to target specific pathways involved in the pathogenesis of disease in order to disrupt functional interactions between MM cells with bone marrow microenvironment and to block autocrine self-supporting circuits. These agents include the immunomodulatory drug thalidomide (Thal), the proteasome inhibitor bortezomib, and the Thal derivative lenalidomide. Clinical studies have shown encouraging results first in patients with relapsed/refractory MM, then in newly diagnosed patients. These drugs, alone and in combination, are now all approved treatment options for symptomatic MM.
Thalidomide
Mechanism of action
Thal was introduced in the treatment of advanced MM in the late 1990s, because of its antiangiogenic properties. These were first described by D'Amato et al. [10], who showed that Thal and its metabolites inhibit basic fibroblast growth factor (bFGF)-induced angiogenesis in a rabbit cornea micropocket assay. The antiangiogenic activity of Thal metabolites was further confirmed by other Authors [11–13]. More recently, a significant decrease in bone marrow microvessel density was demonstrated in patients who responded to Thal [14] without reduction in the plasma level of angiogenic cytokines [15], thus suggesting that different mechanism(s) are involved in the antitumour effect of the drug.
Subsequently, these mechanisms have been progressively disclosed. Thal has been shown to: (a) induce in vitro growth arrest during the G1 phase and apoptosis by either triggering activation of caspase-8 and/or increasing the MM cell sensitivity to Fas-induced apoptosis [16, 17]; (b) block the increased secretion of tumour necrosis factor alpha (TNF-α) by either enhancing TNF-α mRNA degradation or neutralising α1-acid glycoprotein, a stimulator of TNF-α secretion [18–20]; (c) modulate myeloma/stromal cell interaction by either decreasing the expression of adhesion molecules (ICAM-1, VCAM-1, E-selectin and L-selectin) or inhibiting the paracrine loops of cytokine secretion (particularly vascular endothelial growth factor (VEGF) and interleukin (IL)-6) [21, 22]; (d) enhance host immune response against MM, by the ability to increase anti-CD3+ T-cell-induced proliferation and cytokine secretion [IL-2 and interferon (IFN)-γ] in normal donors [23] and/or by increasing in vivo CD56+ NK cell proliferation [24]; and (e) interfere with intracellular growth signalling by down-regulating the constitutive activity of nuclear factor kappa B (NFkB) (i.e., through the block of insulin-like growth factor-1) [25, 26] as well as the expression of cellular inhibitor of apoptosis protein-2 (cIAP-2) and FLICE inhibitory protein (FLIP), two well known inhibitors of apoptosis [17] (Fig. 1).
Fig. 1.
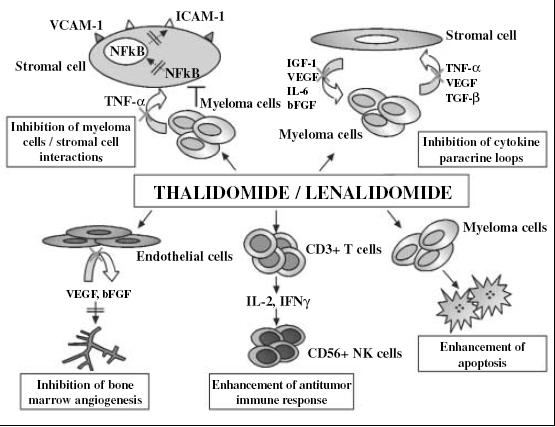
Schematic representation of the effects of Thal and lenalidomide on myeloma cells, tumor microenvironment, and host immunity. VCAM-1= vascular cell adhesion molecule 1; ICAM-1= intercellular adhesion molecule 1; TNF-α= tumor necrosis factor alpha; NFkB= nuclear factor kappa B; bFGF= basic fibroblast growth factor; VEGF= vascular endothelial growth factor; IGF= insulin growth factor; IL-6= interleukin 6; TGF-β= transforming growth factor beta; IL-2= interleukin 2; IFN-γ= interferon gamma
The role of TNF-α is crucial, as indicated by Thompson et al. [27] and Neben et al [28]. The former investigators showed a poorer progression-free survival (PFS) of Thal-treated MM patients if their pretreatment serum TNF-α levels were elevated, while the second group demonstrated a correlation between TNF-α gene polymorphism and response to Thal.
Clinical studies
Relapsed/refractory myeloma
The efficacy of Thal as a single agent or in combination in the treatment of relapsed/refractory MM is described in Table 1 [29–36]. Singhal et al. were the first to demonstrate that Thal is effective in MM treatment [29]. In this phase II study and its update on 169 patients (most of whom had failed high-dose therapy) [30], a 30% partial response (PR) and a 14% near complete response (nCR) were observed. A 2-year follow-up showed 20% and 48% event-free survival (EFS) and OS rates respectively. Cytogenetic abnormalities were associated with a poor prognosis.
Table 1.
Response and survival of refractory/relapsed myeloma patients following thalidomide-based therapy
| Patients (no.) | Schedule | Response (%) | Survival (%/evaluationyear) | Reference | |||||
|---|---|---|---|---|---|---|---|---|---|
| Drugs | Dose | Time | PR | CR+nCR | OR | EFS | OS | ||
| 84 | Thal | 200–800 mg/day | Continuous | – | – | 32 | 22±5/1 | 58±5/1 | [29] |
| 169 | Thal | 200–800 mg/day | Continuous | 30 | 14 | 44 | 20±6/2 | 48±6/2 | [30] |
| 83 | Thal | 400 mg/day | Continuous | 35 | 13 | 48 | 78/1a | 87/1a | [31] |
| 77 | Thal | 100 mg/day | Continuous | 23 | 18 | 41 | 1b | – | [32] |
| Dex | 40 mg/day | Days 1–4/month | |||||||
| 44 | Thal | 200–400 mg/day | Continuous | 55 | – | 55 | – | 1.05c | [33] |
| Dex | 20 mg/m2 | Days 1–4,9–12,17–20,then1–4 | |||||||
| 71 | Thal | 200–800 mg/day | Continuous | 55 | 2 | 57 | 57/2b | 66/2 | [34] |
| Cy | 50 mg/day | Continuous | |||||||
| Dex | 40 mg/day | Days 1–4 every 3 weeks | |||||||
| 52 | Thal | 100–300 mg/day | Continuous | 62 | 17 | 79 | 34/2 | 73/2 | [35] |
| Cy | 300 mg/m2 | 1 every week | |||||||
| Dex | 40 mg/day | Days 1–4 every 4 weeks | |||||||
| 50 | Thal | 00 mg/day | Continuous | 44 | 32 | 92 | 61/1 | 79/1 | [36] |
| Doxil | 40 mg/m2 | Days 1 | |||||||
| Dex | 40 mg/day | Days 1–4,9–12 | |||||||
aPatients with favourable prognostic markers; bprogression-free survival (PFS); cmedian OS in years
PR, partial response; CR, complete response; nCR, near complete response; OR, overall response; EFS, event-free survival; OS, overall survival ; Thal, thalidomide; Dex, dexamethasone; Doxil, pegylated liposomal doxorubicin; Cy, cyclophosphamide
Many other studies have demonstrated the efficacy of Thal as a single agent in advanced MM with response rates ranging from 25% to 64% [37–39].
Thal-Dexamethasone (Dex)
Preclinical studies have suggested synergistic activity of Thal-Dex and clinical results have confirmed major efficacy of this combination as compared with Thal alone [40, 41]. Dimopoulos et al. treated 44 patients with Thal (schedule is shown in Table 1) [33]. Twenty-four patients (55%) achieved a PR with a median time to response of 1.3 months. The median time to progression for responding patients was 10 months and the median survival for all patients was 12.6 months. Similar encouraging results have also been reported in another phase II study (Table 1) [32]. After 3 months of treatment, 41% of patients reported objective response rates (18% complete response (CR) and nCR). After a median follow-up of 8 months, median PFS was 12 months.
Thal-Dex-pegylated liposomal doxorubicin (Doxil) or Thal-Dex-cyclophosphamide (Cy)
The addition of Doxil to Thal-Dex increased the rate of objective responses up to over 70% [42]. In a recent prospective multicentre phase II study, 50 patients received Thal-Dex and Doxil (40 mg/m2) (Table 1). The overall response (OR) rate was 92%, with 26% CR, 6% nCR and 44% PR [36]. The median PFS, EFS and OS were 22 months, 17 months and not reached, respectively.
A regimen that included cyclophosphamide (Cy) with Thal-Dex showed objective responses in 79% of the 52 patients (17% of them reaching a CR) [35]. This combination can induce a stable plateau phase and prolong stable disease.
Newly diagnosed MM
The efficacy of Thal as salvage treatment has led to the use of this agent in newly diagnosed MM patients and to its proposal as front-line therapy in preparation for subsequent ASCT [43, 44].
For many years, vincristine, doxorubicin and Dex (VAD) has been used as standard pretransplantation induction therapy [45]. However, VAD has some disadvantages, including the risk of catheter-related infection with related thrombosis and toxicity (particularly, cardiac and neuropathic), which limit the subsequent use of Thal or bortezomib in advanced phases of the disease. In a comparative case-control study of 200 patients, the superiority of Thal-Dex over VAD was reported with a significantly higher response rate (76% vs. 52%; P<0.001) [46] (Table 2) [46–52]. In each of the 2 treatment groups, 91% of patients proceeded to peripheral blood stem-cell mobilisation.
Table 2.
Response and survival of newly diagnosed myeloma patients following Thal-based therapy in comparative trials
| Patients (no.) | Schedule | Response (%; P) | Survival (%; p/evaluation-year) | Reference | |||||
|---|---|---|---|---|---|---|---|---|---|
| Drugs | Dose | Time | PR | CR+nCR | OR | EFS | OS | ||
| 200 | Thal | 100–200 mg/day | Continuous | 63 vs. 39; NAb | 13 vs. 13; NA | 76 vs. 52; <0.001 | – | – | [46] |
| Dexa | 40 mg | Days 1–4, 9–12, 17–20 then 1–4 | |||||||
| 668 | Thal high-dose therapyc | 100–400 mg/day | Continuous | – | 62 vs. 43; <0.001 | 62 vs. 43; <0.001 | 56 vs. 44; =0.01/5 | 65 vs. 65; =0.09/5 | [47] |
| 207 | Thal | 200 mg/day | Continuous | – | 4 | 63 vs. 41; =0.0017 | – | – | [48] |
| Dexd | 40 mg | Days 1–4, 9–12, 17–20 | |||||||
| 255 | Thal | 100 mg/day | Continuous | 60.4 vs. 45.2; <0.0001 | 27.9 vs. 7.2; <0.0001 | 76 vs. 47.6; <0.0001 | 54 vs. 27; =0.0006/2 | 80 vs. 64; =0.19/3 | [49] |
| Melphalan | 4 mg/m2 | Days 1–7 | |||||||
| Prednisone (MPT)e | 40 mg/m2 | Days 1–7 | |||||||
| 50 | Thal | 300 mg/day | Days 1–4, 17–20 | 62 | 10 | 72 | – | – | [50] |
| Melphalan | 8 mg/m2 | Days 1–4 | |||||||
| Dex | 20 mg/m2 | Days 1–4, 17–20 | |||||||
| 597 | Thal | 100 mg/day | Continuous | 30 vs. 37 vs. 37; =0.001 | 67 vs. 57 vs. 55; =0.001 | 97 vs. 97 vs. 92; =0.001 | 52 vs. 37 vs. 36; <0.009/3 | 87 vs. 74 vs. 77; <0.04/4 | [51] |
| Pamidronatef | 90 mg/m2 | Day 1 every 4 weeks | |||||||
| 112 | Thalg | 200 mg/day | Continuous | – | – | – | – | 5.4 vs 3.8; =0.09b | [52] |
avs. VAD; bNA, not applicable; cvs. no Thal; dvs. Dex; evs. MP; fvs. pamidronate vs. no maintenance; gmaintenance in post-transplantation; hmedian OS
Recently, in a phase 3 randomised study, Thal-Dex combination therapy has been compared to Dex alone in 207 patients eligible for ASCT [48]. The OR was significantly higher with Thal-Dex than Dex alone (63% vs. 41% respectively, P=0.0017), with CR in 4% of patients. Disease progression was noted in 2% of patients with Thal-Dex and 5% of patients with Dex alone. Stem-cell harvest was successful in 90% of patients in each arm. However, combination therapy was associated with more severe nonhaematologic toxicity ≥ grade 3 (67% vs. 43%). Thromboembolic events, especially deep venous thrombosis (DVT), occurred more frequently in the Thal-Dex arm (17% vs. 3%, P<0.001). The evaluation of OS was not an endpoint in this study, because the trial was intended to assess the efficacy of pretransplantation induction therapy.
The capacity to further prolong survival and to improve the outcome of patients with MM has been evaluated in a randomised phase III study. Patients (668) were enrolled to receive two cycles of high-dose melphalan supported by ASCT either with Thal (400 mg daily during induction chemotherapy, 100 mg daily between transplantations, 200 mg daily with consolidation therapy, 100 mg daily during the first year of maintenance therapy and 50 mg on alternate days) or not [47]. After a median follow-up of 42 months, the CR rate in the Thal group was 62% vs. 43% in the control group (P<0.001), and the 5-year EFS was 56% vs. 44% (P=0.01). Even so, the five-year OS did not statistically differ between the two groups (65% in both groups, P=0.90) and the median survival after relapse was lower in the Thal group (1.1 years) than in the control group (2.7 years) (P<0.001).
The occurrence of adverse events (DVT and pulmonary embolism) was higher in the Thal group (30% vs. 17% of the control group). The addition of low-molecular-weight heparin given prophylactically, starting after three years from the beginning of the study, did not reduce the risk. Moreover, the incidence of debilitating peripheral neuropathy (>grade 2) was more frequent in the Thal group than in the control group (27% vs. 17%, P<0.001). These results indicate that: (a) Thal failed to improve OS; (b) it was associated to severe toxic effects; and (c) CR was not necessarily correlated to a longer survival. When the relapsed patients received salvage therapies, the response rate was higher and the survival longer in the patients who did not receive Thal, suggesting that the drug may also induce resistance to following treatments in relapsed patients.
However, some studies showed encouraging results with the use of Thal as maintenance therapy following high-dose chemotherapy/ASCT [53, 54]. In a randomised phase III study, conducted by the InterGroupe Francophone du Myélome, 597 patients were assigned to receive maintenance therapy with Thal (100 mg daily) plus pamidronate (PAM), maintenance with PAM alone or no maintenance [51]. A CR or very good partial response (VGPR) was achieved by 67% of patients in the group receiving Thal-PAM, 57% in the group of PAM alone and 55% in the group with no maintenance. Thal-PAM increased 3-year EFS compared to the other two groups (52% vs. 37% and 36%, respectively; P<0.009) as well as the probability of 4-year OS (87% vs. 74% and 77%; P<0.04).
In a recent retrospective study on 112 patients undergoing ASCT, it has been demonstrated that patients receiving Thal-based maintenance treatment had a higher median survival (65.5 months) as compared with patients (44.5 months) who did not receive Thal (P=0.09) [52]. Based on these results, the post-transplant use of low-dose (50–100 mg) Thal as maintenance treatment appears to be promising, because of the lower incidence of adverse events (thromboembolic risk and peripheral neuropathy) and of developing drug resistance.
MP and Thal (MPT)
In patients over 60, who are not eligible for bone-marrow transplantation, the results of a phase III randomised trial conducted by Palumbo et al. showed that the addition of Thal to MP in elderly patients is more active than standard MP [49]. One hundred and twenty-nine out of 255 enrolled patients received Thal (100 mg daily until progression or relapse) and oral MP for six 4-week cycles. These patients had higher response rates and longer EFS than patients treated with MP alone. Combined CR and PR rates were 76% for MPT and 47.6% for MP alone, and the nCR or CR rates were 27.9% and 7.2%, respectively. Two-year EFS was 54% for MPT and 27% for MP (P=0.0006). Threeyear survival rates were 80% for MPT and 64% for MP (P=0.19). The grade 3 or 4 adverse events of MPT compared with those of MP were 48% vs. 25%. The addition of enoxaparin prophylaxis reduced the rate of thromboembolism from 20% to 3% (P=0.005).
Thus, therapy with Thal is effective, even if not curative, in the patients with symptomatic MM and can offer the advantage of oral administration.
Bortezomib
Mechanism of action
Bortezomib is representative of a class of peptide boronate proteasome inhibitors, which target the 26S proteasome, a multicatalytic proteinase complex involved in intracellular protein degradation [55].
A variety of proteins that regulate cell-cycle progression, signal transduction, gene expression, apoptosis, immune response and angiogenesis are tagged for degradation by polyubiquitin chains. The ubiquitin-tagged proteins entering the proteasome are stripped of their ubiquitin and cleaved. Bortezomib has high affinity, specificity and selectivity for catalytic activity of the proteasome. It ultimately inhibits the activation of the transcription factor NF-kB by protecting its inhibitor (IkB) from degradation by the proteasome complex (Fig. 2).
Fig. 2.
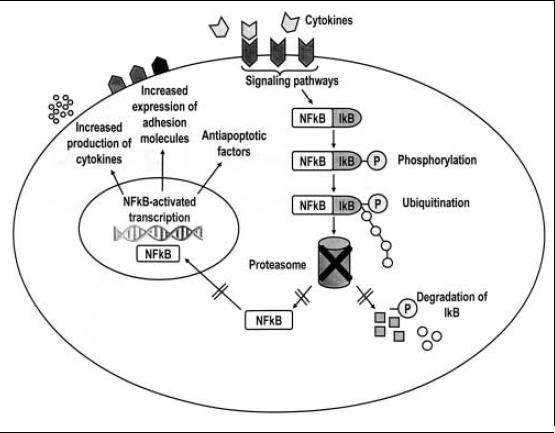
Mechanism of action of bortezomib. P, phosphorylated protein; IkB, nuclear factor kB inhibitory protein
NF-kB is a transcription factor constitutively active in MM and, when it is bound to its inhibitor IkB, it is retained in the cytoplasm [8, 56, 57]. Degradation of IkB by proteasome activates NF-kB, which moves to the nucleus and up-regulates transcription of proteins that promote cell survival and growth, reduce susceptibility to apoptosis, influence the expression of adhesion molecules and induce drug resistance in myeloma cells. Bortezomib can also directly induce apoptosis of primary and drug-resistant myeloma cell lines by interfering with the caspase-dependent pathway, by down-regulating IL-6 and up-regulating p53 and the cell-cycle inhibitor p27 [58, 59].
Furthermore, bortezomib acts in the bone marrow microenvironment by inhibiting the binding of MM cells to bone marrow stromal cells, bone marrow-triggered angiogenesis and/or cytokine (particularly IL-6) transcription/secretion involved in the growth, survival and migration of myeloma cells and in the bone marrow angiogenesis [58, 60].
The results of recent studies suggest that bortezomib inhibits osteoclastic bone resorption and increases osteoblastic function [61–64], thus counteracting the lytic processes triggered by myeloma cells.
Clinical studies
Relapsed/refractory myeloma
Bortezomib has been approved for the treatment of relapsed/refractory MM in the USA and Europe on the basis of results of two phase 2 clinical trials, namely SUMMIT and CREST, and of the multicentre randomised phase 3 APEX study [65–67]. This trial, conducted on 669 patients who relapsed after the first-, second- or third-line therapies, compared bortezomib with standard high-dose Dex and demonstrated a higher efficacy of bortezomib than Dex in terms of response rate, time to progression (primary endpoint) and OS. The results of these trials are summarised in Table 3 [65–69]. An APEX subgroup analysis demonstrated the efficacy of bortezomib also in elderly high-risk patients (β2-microglobulin level >2.5 mg/l, >65 years of age, refractory to previous therapy and >1 previous line of therapy). Furthermore, bortezomib was more effective in patients who received the drug as second- than as third- and fourth-line treatment (45% vs. 26% P=0.004). At 8.3-months median follow-up, the median duration of response was significantly longer in first relapsed patients treated with bortezomib than in those with Dex (8.1 vs. 6.2 months, respectively).
More recently, an updated analysis of the APEX trial confirmed significant benefits of bortezomib after a longer follow-up (median 22 months) as far as time to progression and duration of response were concerned. The OR (CR and PR) improved from 38% to 43% and the CR and nCR rate increased to 16% [70]. In this trial, the most prominent bortezomib-dependent adverse events were grade 3–4 (8% of patients) and grade 1–2 (28% of patients) peripheral neuropathy. Gastrointestinal disorders were: grade 1–2 diarrhoea (50%), vomiting (35%), nausea (57%), constipation (42%) and grade 1–2 fatigue (37% of patients). Herpes zoster infection was common during the treatment (13% vs. 5% of patients of the Dex group; P<0.001). Grade 3–4 thrombocytopenia was also more frequent (30% vs. 6% of Dex group), but reversible in a short time.
Bortezomib-Dex
Of the 256 patients enrolled in the SUMMIT (n=202) and CREST (n=54) studies, 106 patients (41%) who had a suboptimal response, in addition to bortezomib, received Dex at the third or fourth cycle (20 mg on the day of and the day after each dose of bortezomib) [71]. Thirteen (18%) patients from SUMMIT and 9 (33%) from CREST had improved responses to the combined treatment, including the 8 patients (6 out of 13 and 2 out of 9 from SUMMIT and CREST study respectively) who had been refractory to previous Dex regimen alone. Nevertheless, the median time to progression in this subset of patients was shorter than in the whole population of patients both in SUMMIT and CREST studies (5.3 vs. 6.9 months and 6.8 vs. 10.6 months, respectively).
Bortezomib-melphalan
To improve survival of patients with relapsed or refractory MM and overcome chemotherapy resistance, additional combinations have been considered.
In a phase I/II trial on 35 patients, which included the association of bortezomib plus low doses of oral melphalan, CR and PR were achieved in 47% of them (6% of CR and 9% of nCR) [68]. Median PFS was 8 months (Table 3). The addition of Dex to this combined therapy improved response rates up to 80% [72].
Table 3.
Response and survival of refractory/relapsed myeloma patients following bortezomib-based therapy
| Patients (no.) | Schedule | Response (%; P) | Survival (median in months) | Reference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drugs | Dose | Time (days) | Cycles (no.) | PR | CR+nCR | OR | PFS | OS | ||
| 202 | Bortezomib | 1.3 mg/m2 | 1,4,8,11 every 3 weeks; on day and day after bortezomib | 8 | 18 | 10 | 28 | 12b | 16 | [65] |
| Dexa | 20 mg | |||||||||
| 54 | Bortezomib | 1 or 1.3 mg/m2 | 1,4,8,11 every 3 weeks; on day and day after bortezomib | 8 | – | – | 30 | – | – | [66] |
| 38 | ||||||||||
| 50c | ||||||||||
| 669 | Bortezomibd | 1.3 mg/m2 | 1,4,8,11e | 8 | 25 vs 16; <0.001 | 13 vs2; <0.001 | 38 vs 18; <0.001 | 6.22b | 80g | [67] |
| 1,8,15,22f | 3 | |||||||||
| 35 | Bortezomib | 0.7–1 mg/m2 | 1,4,8,11 | 8 | 32 | 15 | 47 | 8 | – | [68] |
| then 1–4 | ||||||||||
| Melphalan | 0.025–0.25 mg/kg | every 4 weeks | ||||||||
| 30 | Bortezomib | 1–1.6 mg/m2 | 1,4,15,22 | 6 | 50 | 17 | 67 | 61g | 84g | [69] |
| Melphalan | 6 mg/m2 | 1–5 | ||||||||
| Prednisone | 60 mg/m2 | 1–5 | ||||||||
| Thal | 50 mg | 1–35 | ||||||||
| (VMPT) | ||||||||||
aAdministered in patients with suboptimal response (progressive disease or stable disease after two or four cycles respectively); btime to progression in months; ccresults with both doses of bortezomib; dvs. high-dose Dex; einduction; fmaintenance; g% at 1 year
Bortezomib-Cy and bortezomib-Doxil
The combination bortezomib, Dex and Cy was shown to be significantly more effective than bortezomib alone or bortezomib and Dex (OR rates were 64% vs. 30% and 47% in 42 evaluable patients) [73].
In a phase 1 study on 22 evaluable patients, the association of bortezomib and Doxil demonstrated significant antitumour activity in advanced MM, with an OR rate of 73%, including 36% of CR or nCR [74]. An additional follow-up on all patients revealed a median time to progression of 9.3 months, and a median OS of 38.3 months [75]. These findings have suggested the possibility that this combination treatment may be very effective in relapsed/refractory MM. Actually, a multicentre randomised phase 3 study on 646 patients comparing the combination of Doxil and bortezomib vs. bortezomib alone has confirmed these encouraging results [76].
Bortezomib-MP-Thal (VMPT)
Among the bortezomib-based combinations, the addition of immunomodulatory drugs is also being investigated. In a recent multicentre phase I/II study, Palumbo et al. evaluated the efficacy and tolerability of VMPT on 30 patients to identify the most appropriate and effective dose of bortezomib in the MPT regimen [69] (Table 3). The maximum tolerated dose of bortezomib was 1.3 mg/m2. Sixty-seven percent of patients achieved a PR and 43% of these had a VGPR. A CR was observed in the subset of patients who received this regimen as second-line treatment (36%). The 1-year PFS and 1-year OS were 61% and 84%, respectively.
Other bortezomib-based combination regimens
Many other combination regimens including Thal and lenalidomide have been considered, such as bortezomib-Doxil-Thal or bortezomib-Thal-Dex or bortezomib-lenalidomide [77–79]. Most phase I or II studies reported response rates of about 60%, with improvement of median PFS and OS compared to standard regimens of chemotherapy. These results are promising and raise the suggestion that bortezomib, in association with either conventional or novel active agents, may offer a valid treatment option in relapsed and refractory patients presenting adverse prognostic factors such as increased β2-microglobulin, cytogenetic abnormalities (chromosome 13 deletion) and/or renal failure.
Newly diagnosed MM
Bortezomib is currently being evaluated as a first-line treatment in previously untreated patients either ineligible or candidates for ASCT in ongoing clinical trials. In the front-line setting, bortezomib was studied as a single agent in a multicentre phase 2 study in 63 patients (46 of them evaluable for response) with a median age of 60 years [80]. Eleven, 20 and 28% of patients obtained a complete, partial and minimal response respectively, giving an OR rate of 59%. The most common adverse events were peripheral neuropathy (55% treatment-related) of mild to moderate severity, and fatigue, rash, nausea, constipation and infection by Varicella zoster virus.
Bortezomib-MP
Mateos et al. performed a phase 1–2 study involving 60 untreated patients aged ≥65 (median age 74 years) with the aim of determining efficacy and safety of bortezomib plus standard MP [81]. The administration schedule and response rates are indicated in Table 4 [81, 82]. Responses were not conditioned by cytogenetic abnormalities, such as retinoblastoma gene deletion, IgH translocations and t(11; 14), t(4; 14), t(14; 16). Principal adverse effects ≥grade 3 were haematologic (thrombocytopenia 46% and neutropenia 39%), gastrointestinal (23%), peripheral neuropathy (15%) and infections (14%). The results seem to be superior to those of historical data with MP, suggesting this combination as a valid option to standard MP in elderly patients who are not eligible to transplantation.
Table 4.
Response and survival of newly diagnosed myeloma patients following bortezomib-based therapy
| Patients (no.) | Schedule | Response (%) | Survival (%/evaluation months) | Reference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drugs | Dose | Time (days) | Cycles (no.) | PR | CR+nCR | OR | EFS | OS | ||
| 60 | Bortezomib | 1.3 mg/m2 | 1,4,8,11,22, 25,29,32 | 4 | 46 | 43 | 89 | 83/16 | 90/16 | [81] |
| 1,8,15,22 | 5 | |||||||||
| Melphalan | 9 mg/m2 | 1–4 | 9 | |||||||
| Prednisone | 60 mg/m2 | 1–4 | 9 | |||||||
| 52 | Bortezomib | 1.3 mg/m2 | 1,4,8,11 | 4 | 45 | 21 | 66 | – | – | [82] |
| Dex | 40 mg | 1–4, 9–12 | 2 | |||||||
| then 1–4 | 2 | |||||||||
Presently, an international phase 3 randomised trial (VISTA) comparing VMP with standard MP is ongoing to determine if this combined therapy could be a standard of care in replacing MP.
Bortezomib and ASCT
The rationale behind the use of bortezomib as part of induction therapy stems from the observation that the drug does not have meaningful toxic effects on haematopoietic stem cells and that a successful mobilisation and quality of the haematopoietic graft could be obtained following its administration. Indeed, the combination of bortezomib-Dex has been shown to be a very effective induction therapy. In a phase II trial, when dexamethasone was added to bortezomib in 36 of 48 patients who had achieved less than a PR after 2 cycles of treatment with bortezomib as monotherapy or less than a CR after 4 cycles, the response to bortezomib improved in 64% of patients [83]. At the end of treatment, the OR rate was 88% (CR and nCR 25% and minimal response 8%). After a median follow-up of 24 months, the median time to alternative therapy for patients not undergoing high-dose therapy was 22 months and 1-year survival rate was 80%. Post-transplantation 1-year survival rate was 90%. A very similar rate of CR (21%) was obtained in another multicentre open-label phase II trial with 52 patients, when Dex was administered from the beginning of the study (schedule is shown in Table 4) [82]. The stem cell collection was successful in most patients (88%) and the toxicity was manageable.
Although it has not been shown that achieving a better response is associated with overall improved survival after transplantation, these results provide the rationale for the ongoing phase III randomised trial planning to enrol 480 patients to compare bortezomib plus Dex regimen with standard induction treatment VAD [84]. The results from the interim analysis, presented at the American Society of Hematology meeting in 2006, are promising (response rate of bortezomib-Dex vs. VAD: 20% vs. 10%), though not conclusive.
Bortezomib-doxorubicin-Dex (PAD)
In an initial trial, the PAD regimen induced overall CR rates after 4 cycles of therapy of 29% and CR and VGPR rates of 62% [85]. More recently, this combination has been studied to determine if it can improve the quality of response in patients who obtained a plateau PR after induction therapy [86]. The association is able to break this plateau and to induce further cytoreduction, also achieving a cytogenetic CR in 3/8 patients with chromosome 13 deletion. The efficacy of doxorubicin in a steroid-free regimen is being evaluated by Orlowski et al. in 63 patients who are candidates for ASCT [87]. Preliminary response data available for 57 patients and presented at the American Society of Hematology meeting in 2006 showed 16% CR or nCR and 58% PR. Among 29 patients who completed the therapeutic programme, the CR and nCR were 28%, with an OR rate of 79%. Furthermore, this therapeutic regimen allowed an adequate collection of stem cells and was well tolerated.
Additional trials including bortezomib alone or in combination are ongoing to evaluate its efficacy as front-line therapy and the results seem promising, but many more studies are required to provide clinical guidance, to define how to use this agent and, finally, to establish if initial efficacy can be translated into a real prolonged survival.
Lenalidomide
Mechanism of action
Lenalidomide is a Thal derivative, which has been developed to overcome the toxic nonhaematologic profile of Thal, including its teratogenicity. It differs from Thal for an amino group and is a more powerful inhibitor of TNF-α activity. Similarly to Thal, lenalidomide is an anti-angiogenic agent, inhibits the adhesion of myeloma cells to bone marrow stromal cells, reduces the secretion of growth and survival factors, induces direct apoptosis of myeloma cells and promotes the cytotoxic activity of natural killer and T-cells against human myeloma cells by stimulating their proliferation and the secretion of IL-2 and IFN-γ [17, 88, 89] (Fig. 1). It also down-regulates the activity of NFkB. These observations prompted the introduction of lenalidomide for MM treatment.
Clinical studies
Relapsed/refractory MM
In phase I studies of patients with relapsed/refractory MM, 25 mg of lenalidomide daily was fixed as the maximum tolerated dose [90]. The major dose-limiting toxic effect was myelosuppression. Lenalidomide was evaluated in a multicentre, open-label, randomised phase II trial of 70 patients by Richardson et al. [91]. The different schedules of administration are shown in Table 5 [81–94]. Treatment with lenalidomide alone resulted in OR, including CR and PR or minor response, of 25%; median OS in the two groups was similar (28 and 27 months, respectively), while median PFS was higher in the first high-dose group (7.7 months vs. 3.9 months). Among 68 patients who received Dex, response occurred in 29% of them. Myelosuppression of grade 3 or 4 (thrombocytopenia and neutropenia) occurred more frequently in patients who received 15 mg twice daily (41% vs. 13%); peripheral neuropathy and DVT were observed in 3% of the patients.
Table 5.
Response and survival of refractory/relapsed and newly diagnosed myeloma patients following lenalidomide-based therapy
| Patients (no.) | Schedule | Response (%; P) | Survival (median in months; P) | Reference | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drugs | Dose | Time (days) | Cycles (no.) | PR | CR+nCR | OR | PFS | OS | ||
| 70 | Lenalidomide | 30 or 15·2 mg | 1–21 every 4 weeks | 12 vs. 14b; NRc | 6 vs. 0b; NR | 24 vs. 29b; NR | 7.7 vs. 3.9b; =0.2 | 28 vs. 27b; NR | [91] | |
| Dexa | 40 mg | 1–4 | ||||||||
| 62 | Lenalidomide | 25 mg | 1–21 every 4 weeks | 46 | 29 | 75 | 12 | – | [92] | |
| Doxil | 40 mg/m2 | 1 | ||||||||
| Vincristine | 2 mg | 1 | ||||||||
| Dex | 40 mg | 1–4 | ||||||||
| 21 | Lenalidomide | 25 mg | 1–21 | 9 | – | – | 65 | – | – | [93] |
| Cy | 500 mg | 1,8,15,21 | ||||||||
| Dex | 40 mg | 1–4, 12–15 | ||||||||
| every 4 weeks | ||||||||||
| 34 | Lenalidomide | 25 mg | 1–21 | 4 | 53 | 38 | 91 | – | – | [94] |
| Dex | 40 mg | 124, 9–12, 17–20 | ||||||||
| every 4 weeks | ||||||||||
aAdministered in patients with progressive or stable disease after two cycles; bonce-daily vs. twice-daily cohort; cNR, non-reported
Two randomised phase 3 trials (MM-009 and MM-010) have compared the combination lenalidomide plus highdose Dex vs. high-dose Dex alone, achieving similar response rates in patients treated with the combination [95, 96]. In both studies, the group receiving lenalidomide and Dex therapy reported remarkably higher OR rates (CR and PR) than the Dex group (MM-009 61% vs. 20.5%, P<0.001; MM-010 59.1% vs. 24%, P<0.001, respectively), time to progression was better for combination therapy than for Dex alone (MM-009: 11.1 vs. 4.7 months, P<0.001; MM-010: 11.3 vs. 4.7 months, P<0.001, respectively) and the same applied for OS (MM-009 29.6 vs. 20.5 months, P<0.001). The most common adverse event was myelosuppression with thrombocytopenia and neutropenia of grade 3 or 4, but the risk of venous thromboembolism was much higher when lenalidomide was associated to Dex. Differently from Thal, the incidence of peripheral neuropathy, sedation and constipation was very low.
Lenalidomide-Doxil and lenalidomide-Cy
Lenalidomide has also been studied in combination with other chemotherapeutic agents. Recently, the efficacy and safety of a regimen comprising Doxil was studied in a phase I/II trial of 62 patients with a median age of 62 years (Table 5) [92]. After a median follow-up of 7.5 months, the OR rate was 75%, and the rate of CR and nCR was 29%, with a maximum tolerated dose of lenalidomide of 10 mg. The median PFS was 12 months.
Also, the addition of an alkylating agent such as Cy has been demonstrated to increase the response rate. In a retrospective analysis, 21 patients of median age 59 years, pretreated with various lines of chemotherapy (comprising Thal, high-dose melphalan, bortezomib and allogeneic bone marrow transplantation) were included [93]. The observed OR rate was 65% (CR and PR), with a toxicity profile especially characterised by neutropenia (38%) and DVT (14%).
Newly diagnosed MM
Lenalidomide-Dex
A phase 2 study evaluated a lenalidomide-Dex regimen as induction therapy in 34 patients of median age 64 years [94]. The treatment schedule is shown in Table 5. An objective response was obtained in 91% of patients, and 6% of them achieved a CR, 53% a PR and 32% a VGPR. Forty-four percent of patients proceeded to ASCT with an adequate collection of stem cells. In 47% of patients, nonhaematologic toxicity of grade 3 or 4 was observed, including fatigue (15%), muscle weakness (6%), pneumonitis (6%), anxiety (6%) and rash (6%). The incidence of thromboembolic events was very low (3%), probably because all patients initiated aspirin prophylaxis from the very beginning.
Lenalidomide-MP
In patients ineligible for transplantation, lenalidomide-MP has been evaluated in 54 patients aged ≥65 years [97]. The OR rate was up to 85% with 23.8% of CR. Toxicity mainly included myelosuppression, with neutropenia and thrombocytopenia of grade 3–4 (66% and 34%, respectively). Thromboembolic events were observed in 3 patients, though all patients received prophylaxis with aspirin.
These combination regimens are promising and may represent a valid alternative to Thal-based treatment, mainly because there are fewer non-haematologic adverse events observed with lenalidomide.
Adverse events
Thalidomide
Besides the advantages of oral treatment for Thal and lenalidomide, generally these drugs are well tolerated and show a predictable and manageable toxicity profile. Nevertheless, several side effects are related to their administration, though with different severity.
Most of the adverse events correlate with dose and duration of treatment. With doses lower than 400 mg daily, their severity is mild to moderate. In addition to known teratogenicity, frequently observed adverse events are: sedation, somnolence, constipation, nausea, fatigue, cutaneous rash, bradycardia, hypothyroidism and oedema. The most serious complications are peripheral neuropathy and venous thromboembolism [98–101]. The incidence of the former is very high (up to 50%) and seems to be related to long-term use (generally over 6 months) and to a pretreatment neuropathy [102]. The most frequent neuropathyrelated symptoms were numbness, paraesthesia or burning sensation with involvement of hands and feet. Its definite correlation with daily/cumulative dose [103] or with duration of treatment [104] has been confirmed. Thus, before receiving Thal, patients should undergo neurological evaluation to identify those at higher risk for peripheral neuropathy. In the initial phases of neuropathy, drug withdrawal can increase the probability of recovery.
The incidence of thromboembolic events, especially DVT and less commonly pulmonary embolism, seems to be higher in patients with either newly diagnosed MM (30% vs. 17% of control group) [47] and/or in Thalsteroids combination regimens (17% vs. 3% of control group) [48, 105]. On the basis of this evidence, the Authors recommend routine prophylaxis with low-molecularweight heparin or warfarin or, in the patients with high bleeding risk, aspirin. However, the efficacy of low-molecular-weight heparin is an open question, because some, but not all, Authors reported a considerable reduction in the risk of DVT. Nevertheless, the generally held opinion is that prophylaxis is recommended.
Lenalidomide
Lenalidomide has a better safety profile than Thal and the most common adverse event is myelosuppression, particularly neutropenia and thrombocytopenia ≥3 grade. But lenalidomide is also associated with a high risk of DVT when it is used with other agents, especially high-dose Dex [106]. Dimopoulos et al. and Weber et al. reported high rates of thromboses (9% and 17.5% respectively) in patients receiving this combination therapy and the rate was higher among patients who received concomitant erythropoietic growth factors [107]. However, administration of aspirin or salicylates seems to reduce the risk of DVT [94, 108]. Therefore, aspirin or other antithrombotic drugs should regularly be used in patients receiving this combination therapy and the concomitant use of erythropoietic agents should be considered with caution.
Bortezomib
The toxicity profile of bortezomib is mainly characterised by peripheral neuropathy and thrombocytopenia. Clinical manifestations include paraesthesias, numbness and pain affecting especially the lower extremities. Overall, the investigators reported that 37% of patients had developed a dose-related peripheral neuropathy of any grade, and 14% of grade ≥3 within the first five cycles of treatment [109]. The baseline neuropathy and previous therapies with other neurotoxic agents, Thal, vincristine or platinum, did not appear to affect the incidence of peripheral neuropathy. Complete resolution or improvement of neuropathic symptoms was observed in 71% of patients during treatment by reducing the dose without compromising the efficacy of therapy or completion of treatment.
In the APEX study, bortezomib was associated with thrombocytopenia of grade ≥3 in 30% of patients, but this effect was transient and the platelet count returned to normal values between cycles with short time of recovery and without cumulative effect. The cause and kinetics of bortezomibinduced thrombocytopenia were different from those seen with standard cytotoxic agents, given that bortezomib does not induce cytotoxic effects on marrow megakaryocytes [110]. Generally, thrombocytopenia is characterised by a mean reduction in platelet counts from a baseline of approximately 60%. Therefore, the most important predictor of severe thrombocytopenia is the initial platelet count. Grade 3 or 4 thrombocytopenia occurs in patients who have low platelet counts at baseline. Approximately 15% of patients treated with bortezomib in the APEX study required transfusions of platelets and this requirement peaked during the first 2 cycles and decreased with increasing cycles of treatment. Moreover, the incidence of serious bleeding episodes associated with grade 3 thrombocytopenia was very low.
Conclusions
The use of targeted therapies exhibiting efficacy in MM is certainly opening a new scenario in this tumour and is showing promise to improve the outcome of these patients, even though many randomised phase 3 studies are still required. Despite impressive advances, the most important challenge remains a better understanding of the disease biology, and to identify additional and more specific targets either within molecular genetics, especially gene expression profile, involved in myelomagenesis or within bidirectional interactions between myeloma cells and their microenvironment, which promote not only growth and survival of malignant cells, but also bone resorption and drug resistance.
Acknowledgement
This work was supported by grants from Associazione Italiana per la Ricerca sul Cancro (AIRC), Milan, Italy.
References
- 1.Riedel DA, Pottern LM (1992) The epidemiology of multiple myeloma. Hematol Oncol Clin North Am 6:225 [PubMed]
- 2.Kyle RA, Rajkumar SV (2004) Multiple myeloma. N Engl J Med 351:1860–1873 [DOI] [PubMed]
- 3.Dammacco F, Perosa F, Procaccio P et al (2001) Mieloma multiplo e gammapatie monoclonali: quadri clinici, acquisizioni eziopatogenetiche e progressi terapeutici. Atti 102° Congr Naz Soc Ital Med Int. Annali Italiani di Medicina Interna 16:5s–40s
- 4.Attal M, Harousseau JL, Facon T et al (2003) Single versus double autologous stem-cell transplantation for multiple myeloma. N Engl J Med 349:2495–2502 [DOI] [PubMed]
- 5.Child JA, Morgan GJ, Davies FE et al (2003) High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med 348:1875–1883 [DOI] [PubMed]
- 6.Chauhan D, Uchiyama H, Akbarali Y et al (1996) Multiple myeloma cell adhesion-induced interleukin-6 expression in bone marrow stromal cells involves activation of NF-kappa B. Blood 87:1104–1112 [PubMed]
- 7.Podar K, Tai YT, Davies FE et al (2001) Vascular endothelial growth factor triggers signaling cascades mediating multiple myeloma cell growth and migration. Blood 98:428–435 [DOI] [PubMed]
- 8.Hideshima T, Chauhan D, Richardson P et al (2002) NF-kappa B as a therapeutic target in multiple myeloma. J Biol Chem 277:16639–16647 [DOI] [PubMed]
- 9.Yaccoby S, Pearse RN, Johnson CL et al (2002) Myeloma interacts with the bone marrow microenvironment to induce osteoclastogenesis and is dependent on osteoclast activity. Br J Haematol 116:278–290 [DOI] [PubMed]
- 10.D’Amato RJ, Loughnan MS, Flynn E, Folkman J (1994) Thalidomide is an inhibitor of angiogenesis. Proc Natl Acad Sci U S A 91:4082–4085 [DOI] [PMC free article] [PubMed]
- 11.Kenyon BM, Browne F, D’Amato RJ (1997) Effects of thalidomide and related metabolites in a mouse corneal model of neovascularization. Exp Eye Res 64:971–978 [DOI] [PubMed]
- 12.Vacca A, Scavelli C, Montefusco V et al (2005) Thalidomide downregulates angiogenic genes in bone marrow endothelial cells of patients with active multiple myeloma. J Clin Oncol 23:5334–5346 [DOI] [PubMed]
- 13.Lentzsch S, LeBlanc R, Podar K et al (2003) Immunomodulatory analogs of thalidomide inhibit growth of Hs Sultan cells and angiogenesis in vivo. Leukemia 17:41–44 [DOI] [PubMed]
- 14.Kumar S, Witzig TE, Dispenzieri A et al (2004) Effect of thalidomide therapy on bone marrow angiogenesis in multiple myeloma. Leukemia 18:624–627 [DOI] [PubMed]
- 15.Neben K, Moehler T, Kraemer A et al (2001) Response to thalidomide in progressive multiple myeloma is not mediated by inhibition of angiogenic cytokine secretion. Br J Haematol 115:605–608 [DOI] [PubMed]
- 16.Hideshima T, Chauhan D, Shima Y et al (2000) Thalidomide and its analogs overcome drug resistance of human multiple myeloma cells to conventional therapy. Blood 96:2943–2950 [PubMed]
- 17.Mitsiades N, Mitsiades CS, Poulaki V et al (2002) Apoptotic signaling induced by immunomodulatory thalidomide analogs in human multiple myeloma cells: therapeutic implications. Blood 99:4525–4530 [DOI] [PubMed]
- 18.Hideshima T, Chauhan D, Schlossman R et al (2001) The role of tumor necrosis factor alpha in the pathophysiology of human multiple myeloma: therapeutic applications. Oncogene 20:4519–4527 [DOI] [PubMed]
- 19.Moreira AL, Sampaio EP, Zmuidzinas A et al (1993) Thalidomide exerts its inhibitory action on tumor necrosis factor alpha by enhancing mRNA degradation. J Exp Med 177:1675–1680 [DOI] [PMC free article] [PubMed]
- 20.Turk BE, Jiang H, Liu JO (1996) Binding of thalidomide to alpha1-acid glycoprotein may be involved in its inhibition of tumor necrosis factor alpha production. Proc Natl Acad Sci U S A 93:7552–7556 [DOI] [PMC free article] [PubMed]
- 21.Geitz H, Handt S, Zwingenberger K (1996) Thalidomide selectively modulates the density of cell surface molecules involved in the adhesion cascade. Immunopharmacology 31:213–221 [DOI] [PubMed]
- 22.Gupta D, Treon SP, Shima Y et al (2001) Adherence of multiple myeloma cells to bone marrow stromal cells upregulates vascular endothelial growth factor secretion: therapeutic applications. Leukemia 15:1950–1961 [DOI] [PubMed]
- 23.Haslett PA, Corral LG, Albert M, Kaplan G (1998) Thalidomide costimulates primary human T lymphocytes, preferentially inducing proliferation, cytokine production, and cytotoxic responses in the CD8+ subset. J Exp Med 187:1885–1892 [DOI] [PMC free article] [PubMed]
- 24.Davies FE, Raje N, Hideshima T et al (2001) Thalidomide and immunomodulatory derivatives augment natural killer cell cytotoxicity in multiple myeloma. Blood 98:210–216 [DOI] [PubMed]
- 25.Mitsiades CS, Mitsiades N, Poulaki V et al (2002) Activation of NF-kappaB and upregulation of intracellular anti-apoptotic proteins via the IGF-1/Akt signaling in human multiple myeloma cells: therapeutic implications. Oncogene 21:5673–5683 [DOI] [PubMed]
- 26.Keifer JA, Guttridge DC, Ashburner BP, Baldwin AS Jr (2001) Inhibition of NF-kappa B activity by thalidomide through suppression of IkappaB kinase activity. J Biol Chem 276:22382–22387 [DOI] [PubMed]
- 27.Thompson MA, Witzig TE, Kumar S et al (2003) Plasma levels of tumour necrosis factor alpha and interleukin-6 predict progression-free survival following thalidomide therapy in patients with previously untreated multiple myeloma. Br J Haematol 123:305–308 [DOI] [PubMed]
- 28.Neben K, Mytilineos J, Moehler TM et al (2002) Polymorphisms of the tumor necrosis factor-alpha gene promoter predict for outcome after thalidomide therapy in relapsed and refractory multiple myeloma. Blood 100:2263–2265 [PubMed]
- 29.Singhal S, Mehta J, Desikan R et al (1999) Antitumor activity of thalidomide in refractory multiple myeloma. N Engl J Med 341:1565–1571 [DOI] [PubMed]
- 30.Barlogie B, Desikan R, Eddlemon P et al (2001) Extended survival in advanced and refractory multiple myeloma after single-agent thalidomide: identification of prognostic factors in a phase 2 study of 169 patients. Blood 98:492–494 [DOI] [PubMed]
- 31.Yakoub-Agha I, Attal M, Dumontet C et al (2002) Thalidomide in patients with advanced multiple myeloma: a study of 83 patients - report of the Intergroupe Francophone du Myelome (IFM). Hematol J 3:185–192 [DOI] [PubMed]
- 32.Palumbo A, Giaccone L, Bertola A et al (2001) Low-dose thalidomide plus dexamethasone is an effective salvage therapy for advanced myeloma. Haematologica 86:399–403 [PubMed]
- 33.Dimopoulos MA, Zervas K, Kouvatseas G et al (2001) Thalidomide and dexamethasone combination for refractory multiple myeloma. Ann Oncol 12:991–995 [DOI] [PubMed]
- 34.Garcia-Sanz R, Gonzalez-Porras JR, Hernandez JM et al (2004) The oral combination of thalidomide, cyclophosphamide and dexamethasone (ThaCyDex) is effective in relapsed/refractory multiple myeloma. Leukemia 18:856–863 [DOI] [PubMed]
- 35.Kyriakou C, Thomson K, D’sa S et al (2005) Low-dose thalidomide in combination with oral weekly cyclophosphamide and pulsed dexamethasone is a well tolerated and effective regimen in patients with relapsed and refractory multiple myeloma. Br J Haematol 129:763–770 [DOI] [PubMed]
- 36.Offidani M, Corvatta L, Marconi M et al (2006) Low-dose thalidomide with pegylated liposomal doxorubicin and high-dose dexamethasone for relapsed/refractory multiple myeloma: a prospective, multicenter, phase II study. Haematologica 91:133–136 [PubMed]
- 37.Tosi P, Zamagni E, Cellini C et al (2002) Salvage therapy with thalidomide in patients with advanced relapsed/refractory multiple myeloma. Haematologica 87:408–414 [PubMed]
- 38.Richardson P, Schlossman R, Jagannath S et al (2004) Thalidomide for patients with relapsed multiple myeloma after high-dose chemotherapy and stem cell transplantation: results of an open-label multicenter phase 2 study of efficacy, toxicity, and biological activity. Mayo Clin Proc 79:875–882 [DOI] [PubMed]
- 39.Wu KL, Helgason HH, van der Holt B et al (2005) Analysis of efficacy and toxicity of thalidomide in 122 patients with multiple myeloma: response of soft-tissue plasmacytomas. Leukemia 19:143–145 [DOI] [PubMed]
- 40.Anagnostopoulos A, Weber D, Rankin K et al (2003) Thalidomide and dexamethasone for resistant multiple myeloma. Br J Haematol 121:768–771 [DOI] [PubMed]
- 41.Alexanian R, Weber D, Anagnostopoulos A et al (2003) Thalidomide with or without dexamethasone for refractory or relapsing multiple myeloma. Semin Hematol 40:3–7 [DOI] [PubMed]
- 42.Hussein MA, Baz R, Srkalovic G et al (2006) Phase 2 study of pegylated liposomal doxorubicin, vincristine, decreased-frequency dexamethasone, and thalidomide in newly diagnosed and relapsed-refractory multiple myeloma. Mayo Clin Proc 81:889–895 [DOI] [PubMed]
- 43.Rajkumar SV, Hayman S, Gertz MA et al (2002) Combination therapy with thalidomide plus dexamethasone for newly diagnosed myeloma. J Clin Oncol 20:4319–4323 [DOI] [PubMed]
- 44.Cavo M, Zamagni E, Tosi P et al (2004) First-line therapy with thalidomide and dexamethasone in preparation for autologous stem cell transplantation for multiple myeloma. Haematologica 89:826–831 [PubMed]
- 45.Alexanian R, Barlogie B, Tucker S (1990) VAD-based regimens as primary treatment for multiple myeloma. Am J Hematol 33:86–89 [DOI] [PubMed]
- 46.Cavo M, Zamagni E, Tosi P et al (2005) Superiority of thalidomide and dexamethasone over vincristine-doxorubicin-dexamethasone (VAD) as primary therapy in preparation for autologous transplantation for multiple myeloma. Blood 106:35–39 [DOI] [PubMed]
- 47.Barlogie B, Tricot G, Anaissie E et al (2006) Thalidomide and hematopoietic-cell transplantation for multiple myeloma. N Engl J Med 354:1021–1030 [DOI] [PubMed]
- 48.Rajkumar SV, Blood E, Vesole D et al (2006) Phase III clinical trial of thalidomide plus dexamethasone compared with dexamethasone alone in newly diagnosed multiple myeloma: a clinical trial coordinated by the Eastern Cooperative Oncology Group. J Clin Oncol 24:431–436 [DOI] [PubMed]
- 49.Palumbo A, Bringhen S, Caravita T et al (2006) Oral melphalan and prednisone chemotherapy plus thalidomide compared with melphalan and prednisone alone in elderly patients with multiple myeloma: randomised controlled trial. Lancet 367:825–831 [DOI] [PubMed]
- 50.Dimopoulos MA, Anagnostopoulos A, Terpos E et al (2006) Primary treatment with pulsed melphalan, dexamethasone and thalidomide for elderly symptomatic patients with multiple myeloma. Haematologica 91:252–254 [PubMed]
- 51.Attal M, Harousseau JL, Leyvraz S et al (2006) Maintenance therapy with thalidomide improves survival in patients with multiple myeloma. Blood 108:3289–3294 [DOI] [PubMed]
- 52.Brinker BT, Waller EK, Leong T et al (2006) Maintenance therapy with thalidomide improves overall survival after autologous hematopoietic progenitor cell transplantation for multiple myeloma. Cancer 106:2171–2180 [DOI] [PubMed]
- 53.Alexanian R, Weber D, Giralt S, Delasalle K (2002) Consolidation therapy of multiple myeloma with thalidomidedexamethasone after intensive chemotherapy. Ann Oncol 13:1116–1119 [DOI] [PubMed]
- 54.Stewart AK, Chen CI, Howson-Jan K et al (2004) Results of a multicenter randomized phase II trial of thalidomide and prednisone maintenance therapy for multiple myeloma after autologous stem cell transplant. Clin Cancer Res 10:8170–8176 [DOI] [PubMed]
- 55.Adams J, Palombella VJ, Sausville EA et al (1999) Proteasome inhibitors: a novel class of potent and effective antitumor agents. Cancer Res 59:2615–2622 [PubMed]
- 56.Hideshima T, Mitsiades C, Akiyama M et al (2003) Molecular mechanisms mediating antimyeloma activity of proteasome inhibitor PS-341. Blood 101:1530–1534 [DOI] [PubMed]
- 57.Rajkumar SV, Richardson PG, Hideshima T, Anderson KC (2005) Proteasome inhibition as a novel therapeutic target in human cancer. J Clin Oncol 23:630–639 [DOI] [PubMed]
- 58.Hideshima T, Richardson P, Chauhan D et al (2001) The proteasome inhibitor PS-341 inhibits growth, induces apoptosis, and overcomes drug resistance in human multiple myeloma cells. Cancer Res 61:3071–3076 [PubMed]
- 59.Hideshima T, Chauhan D, Hayashi T et al (2003) Proteasome inhibitor PS-341 abrogates IL-6 triggered signaling cascades via caspase-dependent downregulation of gp130 in multiple myeloma. Oncogene 22:8386–8393 [DOI] [PubMed]
- 60.Roccaro AM, Hideshima T, Raje N et al (2006) Bortezomib mediates antiangiogenesis in multiple myeloma via direct and indirect effects on endothelial cells. Cancer Res 66:184–191 [DOI] [PubMed]
- 61.Shimazaki C, Uchida R, Nakano S et al (2005) High serum bone-specific alkaline phosphatase level after bortezomibcombined therapy in refractory multiple myeloma: possible role of bortezomib on osteoblast differentiation. Leukemia 19:1102–1103 [DOI] [PubMed]
- 62.Heider U, Kaiser M, Muller C et al (2006) Bortezomib increases osteoblast activity in myeloma patients irrespective of response to treatment. Eur J Haematol 77:233–238 [DOI] [PubMed]
- 63.Zangari M, Yaccoby S, Cavallo F et al (2006) Response to bortezomib and activation of osteoblasts in multiple myeloma. Clin Lymphoma Myeloma 7:109–114 [DOI] [PubMed]
- 64.Giuliani N, Morandi F, Tagliaferri S et al (2007) The proteasome inhibitor bortezomib affects osteoblast differentiation in vitro and in vivo in multiple myeloma patients. Blood 110:334–338 [DOI] [PubMed]
- 65.Richardson PG, Barlogie B, Berenson J et al (2003) A phase 2 study of bortezomib in relapsed, refractory myeloma. N Engl J Med 348:2609–2617 [DOI] [PubMed]
- 66.Jagannath S, Barlogie B, Berenson J et al (2004) A phase 2 study of two doses of bortezomib in relapsed or refractory myeloma. Br J Haematol 127:165–172 [DOI] [PubMed]
- 67.Richardson PG, Sonneveld P, Schuster MW et al (2005) Bortezomib or high-dose dexamethasone for relapsed multiple myeloma. N Engl J Med 352:2487–2498 [DOI] [PubMed]
- 68.Berenson JR, Yang HH, Sadler K et al (2006) Phase I/II trial assessing bortezomib and melphalan combination therapy for the treatment of patients with relapsed or refractory multiple myeloma. J Clin Oncol 24:937–944 [DOI] [PubMed]
- 69.Palumbo A, Ambrosini MT, Benevolo G et al (2007) Bortezomib, melphalan, prednisone, and thalidomide for relapsed multiple myeloma. Blood 109:2767–2772 [DOI] [PubMed]
- 70.Richardson PG, Sonneveld P, Schuster MW et al (2005) Bortezomib continues to demonstrate superior efficacy compared with high-dose dexamethasone in relapsed multiple myeloma: updated results of the APEX trial. Blood (ASH Annual Meeting Abstracts) 106:2547
- 71.Jagannath S, Richardson PG, Barlogie B et al (2006) Bortezomib in combination with dexamethasone for the treatment of patients with relapsed and/or refractory multiple myeloma with less than optimal response to bortezomib alone. Haematologica 91:929–934 [PubMed]
- 72.Popat R, Oakervee HE, Foot N et al (2005) A phase I/II study of bortezomib and low dose intravenous melphalan (BM) for relapsed multiple myeloma. Blood (ASH Annual Meeting Abstracts) 106:2555
- 73.Davies FE, Wu P, Srikanth M et al (2006) The combination of Cyclophosphamide, Velcade and Dexamethasone (CVD) induces high response rates with minimal toxicity compared to Velcade alone (V) and Velcade plus Dexamethasone. Blood (ASH Annual Meeting Abstracts) 108:3537
- 74.Orlowski RZ, Voorhees PM, Garcia RA et al (2005) Phase I trial of the proteasome inhibitor bortezomib and pegylated liposomal doxorubicin in patients with advanced hematologic malignancies. Blood 105:3058–3065 [DOI] [PubMed]
- 75.Biehn SE, Moore DT, Voorhees PM et al (2007) Extended follow-up of outcome measures in multiple myeloma patients treated on a phase I study with bortezomib and pegylated liposomal doxorubicin. Ann Hematol 86:211–216 [DOI] [PubMed]
- 76.Orlowski RZ, Zhuang SH, Parekh T et al, the DOXIL-MMY-3001 Study Investigators (2006) The combination of pegylated liposomal doxorubicin and bortezomib significantly improves time to progression of patients with relapsed/refractory multiple myeloma compared with bortezomib alone: results from a planned interim analysis of a randomized phase III study. Blood (ASH Annual Meeting Abstracts) 108:404
- 77.Chanan-khan AA, Padmanabhan S, Miller KC et al (2006) Final results of a phase II study of bortezomib (Velcade) in combination with liposomal doxorubicin (Doxi) and thalidomide (VDT) demonstrate a sustained high response rates in patients (pts) with relapsed (rel) or refractory (ref) multiple myeloma. Blood (ASH Annual Meeting Abstracts) 108:3539
- 78.Zangari M, Barlogie B, Burns MJ et al (2006) Velcade (V)-Thalidomide (T)-Dexamethasone (D) for advanced and refractory multiple myeloma (MM): long term follow-up of phase I/II trial UARK 2001–37: superior outcome in patients with normal cytogenetics and no prior T. Blood (ASH Annual Meeting Abstracts) 106:2552
- 79.Richardson PG, Jagannath S, Avigan DE et al (2006) Lenalidomide plus bortezomib (Rev-Vel) in relapsed and/or refractory multiple myeloma (MM): final results of a multicenter phase 1 trial. Blood (ASH Annual Meeting Abstracts) 108:405
- 80.Richardson PG, Chanan-khan AA, Schlossman R et al (2005) A multicenter phase II trial of bortezomib in patients with previously untreated multiple myeloma: efficacy with manageable toxicity in patients with unexpectedly high rates of baseline peripheral neuropathy. Blood (ASH Annual Meeting Abstracts) 106:2548
- 81.Mateos MV, Hernandez JM, Hernandez MT et al (2006) Bortezomib plus melphalan and prednisone in elderly untreated patients with multiple myeloma: results of a multicenter phase 1/2 study. Blood 108:2165–2172 [DOI] [PubMed]
- 82.Harousseau JL, Attal M, Leleu X et al (2006) Bortezomib plus dexamethasone as induction treatment prior to autologous stem cell transplantation in patients with newly diagnosed multiple myeloma: results of an IFM phase II study. Haematologica 91:1498–1505 [PubMed]
- 83.Jagannath S, Durie BG, Wolf J et al (2005) Bortezomib therapy alone and in combination with dexamethasone for previously untreated symptomatic multiple myeloma. Br J Haematol 129:776–783 [DOI] [PubMed]
- 84.Harousseau JL, Marit G, Caillot D et al (2006) VEL-CADE/Dexamethasone (Vel/Dex) versus VAD as induction treatment prior to autologous stem cell transplantation (ASCT) in newly diagnosed multiple myeloma (MM): an interim analysis of the IFM 2005–01 randomized multicenter phase III trial. Blood (ASH Annual Meeting Abstracts) 108:56
- 85.Oakervee HE, Popat R, Curry N et al (2005) PAD combination therapy (PS-341/bortezomib, doxorubicin and dexamethasone) for previously untreated patients with multiple myeloma. Br J Haematol 129:755–762 [DOI] [PubMed]
- 86.Di Carlo BA, Stern JL, Schuster M et al (2006) Breaking the plateau response in myeloma: preliminary results of a phase II pilot study of sequential bortezomib in combination with dexamethasone and pegylated liposomal doxorubicin (DoVeD) in patients no longer responsive to standard induction regimens. Blood (ASH Annual Meeting Abstracts) 108:3538
- 87.Orlowski RZ, Peterson BL, Sanford B et al; the Cancer and Leukemia Group B (2006) Bortezomib and pegylated liposomal doxorubicin as induction therapy for adult patients with symptomatic multiple myeloma: Cancer and Leukemia Group B Study 10301. Blood (ASH Annual Meeting Abstracts) 108:797
- 88.Hideshima T, Chauhan D, Podar K et al (2001) Novel therapies targeting the myeloma cell and its bone marrow microenvironment. Semin Oncol 28:607–612 [DOI] [PubMed]
- 89.Dredge K, Marriott JB, Macdonald CD et al (2002) Novel thalidomide analogues display anti-angiogenic activity independently of immunomodulatory effects. Br J Cancer 87:1166–1172 [DOI] [PMC free article] [PubMed]
- 90.Richardson PG, Schlossman RL, Weller E et al (2002) Immunomodulatory drug CC-5013 overcomes drug resistance and is well tolerated in patients with relapsed multiple myeloma. Blood 100:3063–3067 [DOI] [PubMed]
- 91.Richardson PG, Blood E, Mitsiades CS et al (2006) A randomized phase 2 study of lenalidomide therapy for patients with relapsed or relapsed and refractory multiple myeloma. Blood 108:3458–3464 [DOI] [PMC free article] [PubMed]
- 92.Baz R, Walker E, Karam MA et al (2006) Lenalidomide and pegylated liposomal doxorubicin-based chemotherapy for relapsed or refractory multiple myeloma: safety and efficacy. Ann Oncol 17:1766–1771 [DOI] [PubMed]
- 93.Morgan GJ, Schey SA, Wu P et al (2007) Lenalidomide (Revlimid), in combination with cyclophosphamide and dexamethasone (RCD), is an effective and tolerated regimen for myeloma patients. Br J Haematol 137:268–269 [DOI] [PubMed]
- 94.Rajkumar SV, Hayman SR, Lacy MQ et al (2005) Combination therapy with lenalidomide plus dexamethasone (Rev/Dex) for newly diagnosed myeloma. Blood 106:4050–4053 [DOI] [PMC free article] [PubMed]
- 95.Dimopoulos MA, Spencer T, Attal M et al (2005) Study of lenalidomide plus dexamethasone versus dexamethasone alone in relapsed or refractory multiple myeloma (MM): results of a phase 3 study (MM-010). Blood (ASH Annual Meeting Abstracts) 106:6
- 96.Weber D, Wang M, Chen CI et al (2006) Lenalidomide plus high dose dexamethasone provides improved overall survival compared to high-dose dexamethasone alone for relapsed or refractory multiple myeloma (MM): results of 2 phase III studies (MM-009, MM-010) and subgroup analysis of patients with impaired renal function. Blood (ASH Annual Meeting Abstracts) 108:3547
- 97.Palumbo A, Falco P, Falcone A et al (2006) Oral Revlimid® plus Melphalan and Prednisone (R-MP) for newly diagnosed multiple myeloma: results of a multicenter phase I/II study. Blood (ASH Annual Meeting Abstracts) 108:800
- 98.Chaudhry V, Cornblath DR, Corse A et al (2002) Thalidomide-induce neuropathy. Neurology 59:1872–1875 [DOI] [PubMed]
- 99.Bennett CL, Schumock GT, Desai AA et al (2002) Thalidomide-associated deep vein thrombosis and pulmonary embolism. Am J Med 113:603–606 [DOI] [PubMed]
- 100.Cavo M, Zamagni E, Cellini C et al (2002) Deep-vein thrombosis in patients with multiple myeloma receiving first-line thalidomide-dexamethasone therapy. Blood 100:2272–2273 [DOI] [PubMed]
- 101.Osman K, Comenzo R, Rajkumar SV (2001) Deep venous thrombosis and thalidomide therapy for multiple myeloma. N Engl J Med 344:1951–1952 [DOI] [PubMed]
- 102.Mileshkin L, Stark R, Day B et al (2006) Development of neuropathy in patients with myeloma treated with thalidomide: patterns of occurrence and the role of electrophysiologic monitoring. J Clin Oncol 24:4507–4514 [DOI] [PubMed]
- 103.Cavaletti G, Beronio A, Reni L et al (2004) Thalidomide sensory neurotoxicity: a clinical and neurophysiologic study. Neurology 62:2291–2293 [DOI] [PubMed]
- 104.Tosi P, Zamagni E, Cellini C et al (2005) Neurological toxicity of long-term (>1 yr) thalidomide therapy in patients with multiple myeloma. Eur J Haematol 74:212–216 [DOI] [PubMed]
- 105.Rajkumar SV (2005) Thalidomide therapy and deep venous thrombosis in multiple myeloma. Mayo Clin Proc 80:1549–1551 [DOI] [PubMed]
- 106.Rajkumar SV, Blood E (2006) Lenalidomide and venous thrombosis in multiple myeloma. N Engl J Med 354:2079–2080 [PubMed]
- 107.Dimopoulos MA, Weber D, Chen CI (2005) Evaluating oral lenalidomide (Revlimid) and dexamethasone versus placebo and dexamethasone in patients with relapsed or refractory multiple myeloma. Haematologica 90[Suppl 2]:160
- 108.Palumbo A, Rus C, Zeldis JB et al (2006) Enoxaparin or aspirin for the prevention of recurrent thromboembolism in newly diagnosed myeloma patients treated with melphalan and prednisone plus thalidomide or lenalidomide. J Thromb Haemost 4:1842–1845 [DOI] [PubMed]
- 109.Richardson PG, Briemberg H, Jagannath S et al (2006) Frequency, characteristics, and reversibility of peripheral neuropathy during treatment of advanced multiple myeloma with bortezomib. J Clin Oncol 24:3113–3120 [DOI] [PubMed]
- 110.Lonial S, Waller EK, Richardson PG et al (2005) Risk factors and kinetics of thrombocytopenia associated with bortezomib for relapsed, refractory multiple myeloma. Blood 106:3777–3784 [DOI] [PMC free article] [PubMed]