

Abstract
Objective To explain, through mediation analyses, the mechanisms by which ATHENA (Athletes Targeting Healthy Exercise and Nutrition Alternatives), a primary prevention and health promotion intervention designed to deter unhealthy body shaping behaviors among female high school athletes, produced immediate changes in intentions for unhealthy weight loss and steroid/creatine use, and to examine the link to long-term follow-up intentions and behaviors. Methods In a randomized trial of 1668 athletes, intervention participants completed coach-led peer-facilitated sessions during their sport season. Participants provided pre-test, immediate post-test, and 9-month follow-up assessments. Results ATHENA decreased intentions for steroid/creatine use and intentions for unhealthy weight loss behaviors at post-test. These effects were most strongly mediated by social norms and self-efficacy for healthy eating. Low post-test intentions were maintained 9 months later and predicted subsequent behavior. Conclusions ATHENA successfully modified mediators that in turn related to athletic-enhancing substance use and unhealthy weight loss practices. Mediation analyses aid in the understanding of health promotion interventions and inform program development.
Keywords: adolescents, educational interventions, health promotion and prevention, lLongitudinal research, peers, mediation analysis.
Female adolescent athletes encounter conflicting pressures as they strive to shape their bodies for success in competitive sports and simultaneously to comply with peer norms for thinness. To meet their goals, young female athletes may engage in both unhealthy weight control strategies and use of dangerous athletic-enhancing substances. ATHENA (Athletes Targeting Healthy Exercise and Nutrition Alternatives) is a primary prevention program targeting both health harming behaviors among high-school female athletes. Primary and delayed intervention findings have previously been reported (Elliot et al., 2004, 2006, 2008). This article reports, through mediation analyses, an examination of the mechanisms by which the intervention reduced intentions to engage in two types of unhealthy body-shaping behaviors.
Female athletes are at risk for disordered eating. Roberts, Glen, and Kreipe (2003) found that 8.4% of 7th–12th grade female athletes tested within the eating disorder range on a measure of disordered eating attitudes. Fully 10% of high-school female athletes employed at least two pathogenic strategies for weight control within a 28-day period, and in extreme cases exhibited the female athlete triad syndrome (Nichols, Rauh, Lawson, Ming, & Barkai, 2006).
Anabolic steroid use, once of more concern among male than among female athletes, is now becoming a serious problem among female athletes (Johnston, O’ Malley, Bachman, & Schulenberg, 2004). Negative effects of steroids include emotional imbalance, liver damage, development of masculine traits, heart attack and stroke, immune deficiency disease risk (e.g., HIV through shared needles), and death (National Institute on Drug Abuse, 2000).
Consistent with the goal of primary prevention, ATHENA aimed to lower intentions for risky weight loss strategies and athletic-enhancing substance use and thereby to prevent their initiation (Elliot et al., 2004, 2006). ATHENA is a sport team-based scripted curriculum which targeted modifiable risk and protective factors associated with disordered eating and body shaping drug use. Elliot et al. (2004, 2006) assessed the immediate impact of the ATHENA program in a randomized trial involving 928 female high school athletes and documented short-term reductions in intention for disordered eating, intention to use athletic-enhancing substances, and initiation of diet pill use. ATHENA also produced improved nutrition skills, greater knowledge of harmful effects of steroid use and disordered eating, improved ability to control mood, enhanced ability to resist unhealthy weight loss, decreased belief in advertisements, and improved norms from friends among ATHENA participants. Elliot et al. (2008) reported reduced drug and alcohol use but not disordered eating 1–3 years beyond high-school graduation.
Elliot et al. (2006) suggested but did not explore whether skills, knowledge, beliefs, and norms were the mechanisms by which intentions to avoid risky behavior in the future were reduced. This article expands on Elliot et al. (2006) by examining via mediation analyses, the mechanisms through which the ATHENA intervention produced changes in intentions that ultimately predict behavior. These hypothesized meditational chains were based on health behavior theory and closely related empirical studies. Additionally, this article expands on previous work by examining the extent to which immediate post-test intentions predict long-term follow-up intentions and behaviors. Analyses are conducted on data of the initial cohort of ATHENA participants (Elliot et al., 2006) plus heretofore unpublished data from two additional cohorts of ATHENA participants. Together, findings inform the design of effective interventions, especially for adolescent prevention and health promotion.
Mediation analysis provides an examination of the process through which an intervention impacts participants by (a) identifying intervention effects on the mediators, and (b) establishing links from changes on mediators to changes on outcomes. Using mediation analysis to uncover intervention mechanisms requires that distinct intervention components target specific mediators ([a], above), and also that the putative links from mediators to outcomes be specified (b above; MacKinnon, 2008; West & Aiken, 1997). The design of health promotion interventions assumes linkages between specific program content and change in targeted constructs. ATHENA targeted particular constructs under the assumption that those changes would lead to decreased intentions to initiate high risk behaviors. The targeted constructs, or hypothesized mediators, in ATHENA included control of negative moods, nutritional practices for athletes, risks of steroid use and unhealthy weight loss, resistance to media messages, pressure from coaches to be thin, and peer norms for eating disorders and steroid use.
Relationships among constructs that are tested in ATHENA appear within established models of health behavior: the theory of planned behavior (TPB; Ajzen, 1991), social cognitive theory (SCT; Bandura, 2001), and the information, motivation, behavior model (IMB; Fisher & Fisher, 1992). In the TPB, norms, attitudes (i.e., outcome expectancies for the effects of a behavior) and perceived behavioral control (self-efficacy) predict intentions to behave. These constructs were hypothesized to be central to the ATHENA program. Knowledge is included in both the IMB and SCT. ATHENA aimed to increase knowledge of harmful effects of steroids, diet pills, laxatives, diuretics, and vomiting. This knowledge, in turn, was expected to intensify negative outcome expectancies for risk behaviors. In SCT, knowledge acquired through observational and active learning predicts self-efficacy; in IMB, information predicts behavioral skills. ATHENA aimed to increase knowledge of nutrition in order to increase self-efficacy for eating to become a better athlete. Baranowski, Perry, and Parcel (2002) describe emotional arousal as inhibiting performance and recommend training for dealing with arousing situations in SCT. ATHENA taught participants ways to control their moods.
There is empirical support for the hypothesized relations among ATHENA constructs. The Adolescents Training and Learning to Avoid Steroids (ATLAS) program is a team-based primary prevention curriculum for high school male athletes. Knowledge of the harmful effects of steroids mediated the program's effect on intentions to use steroids (MacKinnon et al., 2001). Among male adolescents, negative outcome expectancies for steroids are associated with lower steroid use (Lovstakken, Peterson, & Homer, 1999). Interventions with young women support the efficacy of changing outcome expectancies to modify behavior (Whaley, 1999). College women at high risk for eating disorders have greater internalization of societal normative influences on attitudes about their appearance than do women at lower risk (Franko et al., 2005). Self-efficacy, knowledge, personal values, norms, and self-esteem relate to unhealthy weight loss behaviors (Franko et al., 2005). Depressed mood is associated with disordered eating among adolescents (Santos, Richards, & Bleckley, 2007). A strong association has been shown between intentions and subsequent behaviors of young women for physical activity (Everson, Daley, & Ussher, 2007), sun protection (Jackson & Aiken, 2006), and calcium intake (Schmiege, Aiken, Sander, & Gerend, 2007).
ATHENA is a primary prevention program; most participants had not yet engaged in the targeted risky behaviors, and reducing intentions was a principal intervention goal. The current analyses examine which constructs that were changed by the ATHENA intervention mediated the immediate effect of the intervention on two intention measures: intention to engage in unhealthy weight loss and intention to use athletic-enhancing substances. Our focus was to investigate, through mediation analysis, whether change on putative mediators led to change in intentions. Furthermore, we examined the relation between post-test intentions and long-term follow-up behaviors and intentions.
Method
Participants
The ATHENA program was conducted with female athletes in sport teams at 18 high schools in the Northwest. Over a 3-year period, 1668 athletes participated (928, 485, and 255 athletes in the year one, two, and three cohorts, respectively). The CONSORT diagram in Figure 1 includes all participants. The majority of participants were White (91%), and in 9th (46%) or 10th grade (25%) at pre-test. In all 70% of mothers and 68% of fathers had completed at least some college. Only 11% of participants received free or reduced price school lunch. Athletes participated in 11 different sports; 68% were in volleyball, soccer, or basketball. At pre-test, few participants had used diet pills (6%), diuretics (1%), vomiting (4%), laxatives (1%), anabolic steroids (< 1%), or creatine (2%) in the past 3 months; 14% had not eaten for a day or more to lose weight. Students and their parents or guardians provided written informed consent. The Institutional Review Board of the Oregon Health & Science University approved the study.
Figure 1.
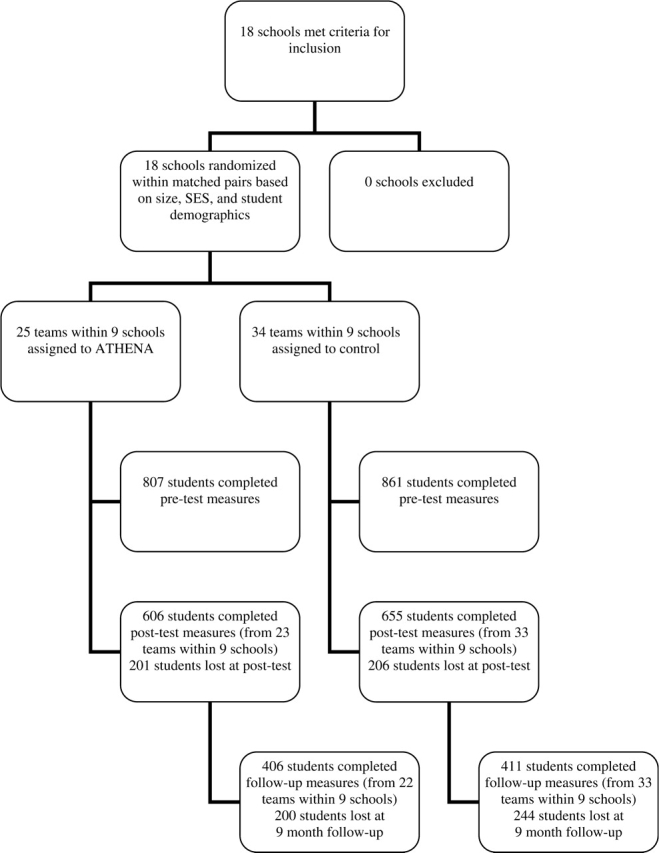
CONSORT diagram depicting participants’ assignment to condition and retention.
Procedure
Schools were matched in pairs based on size, average socioeconomic status, and student demographics. One school in each pair was randomly assigned to the experimental condition and the other to control. An offer to participate in ATHENA was extended to all girls’ sports teams at each experimental school. After a team agreed to participate, the same sport team at the paired control school was asked to complete the questionnaires and was given pamphlets on disordered eating, drug use, and sports nutrition. One to eight sport teams participated from each school.
There were three measurement points: (i) immediate pre-test, (ii) immediate post-test, and (iii) long-term follow-up. After participants completed pre-test measures, they began the ATHENA program. The immediate post-test measures were gathered within 2 weeks of the end of the 3–4-month sport season. Follow-up data were collected 9 months after post-test.
Immediate Post-test Retention
Only participants who completed the sport season were included in immediate post-test data collection. The number of participants declined from 1668 to 1261 (24% loss) between pre-test and immediate post-test data collection. Attrition (25%, 24%, in treatment vs. control, respectively) was mainly attributable to athletic program structure. Some participants were cut and others dropped out of the sport. Attrition was comparable to that of male high school athletes in the ATLAS study (Goldberg et al., 2000).
Long-term Follow-up Retention
Only participants who remained in their sport in the year after ATHENA were included in long-term (9 months) follow up. Data were collected from 817 (81%) of the 1006 participants from the first two cohorts. The final cohort of 255 participants had been enrolled in the study in its third year, not allowing for long-term follow-up.
The ATHENA Intervention
The ATHENA program was a sequenced intervention consisting of eight weekly 45 min sessions facilitated by the coach and integrated into usual team activities. Athletes were partitioned into six member groups with a designated squad leader; the squad leader and coach used scripted lesson plans for these meetings. The majority of activities were peer-led and involved group participation. Additional information on ATHENA is given at the following website: http://www.nrepp.samhsa.gov/programfulldetails.asp?PROGRAM_ID=111. The curriculum focused on the putative mediators shown in Table I. Participants learned proper nutrition for sport performance (sessions 1 and 2) to enhance self-efficacy for healthy eating through achievable weekly goals (session 4). They learned negative effects of use of body shaping substances (session 2) and disordered eating (session 3). These effects were then personalized to produce negative outcome expectancies (sessions 5 and 6). Participants deconstructed messages in advertisements of supplements and diet pills to reverse beliefs in deceptive norms portrayed in advertisements (session 4). Participants made their own ads that promoted healthy activities to establish healthy normative beliefs about drug and substance use and to reinforce negative outcome expectancies (sessions 5 and 6). Participants learned to recognize the linkage between their activities and feelings by keeping daily diaries and also acquired strategies to control their mood (session 3). Role playing taught skills to resist unhealthy weight loss behaviors (session 7). Intentions were targeted in session 8. Participating in the program with their coach and peers was designed to teach participants that their coach and peers endorse healthy norms.
Table I.
Construct Reliabilities and Means (Standard Deviations) at Pre-Test and Immediate Post-Test Measures
| aCoefficient α | Mean (SD) |
eCohen's d | ||||
|---|---|---|---|---|---|---|
| bTest–retest r | Pretest |
Post-test (3–4 months) |
||||
| ATHENA | Control | ATHENA | Control | |||
| Putative mediators | ||||||
| 1. Knowledge: harmful effects of steroids | .39b | 3.3 (1.6) | 2.8 (1.7) | 4.1 (1.6) | 2.9 (1.9) | .56 |
| 2. Knowledge: nutrition for sport performance | .38b | 5.9 (1.2) | 5.7 (1.4) | 5.9 (1.2) | 5.5 (1.4) | .24 |
| 3. Peer norm for steroid use | .79a | 1.9 (1.6) | 1.8 (1.5) | 1.9 (1.6) | 1.9 (1.5) | .00 |
| 4. Social Norms: coach and magazines | .51a | 2.2 (0.8) | 2.2 (0.8) | 2.0 (0.9) | 2.2 (.0.9) | .28 |
| 5. Peer norm for eating disorders | .86a | 3.6 (2.2) | 3.2 (2.1) | 3.3 (2.1) | 3.1 (2.1) | .03 |
| 6. Belief: ability to control mood | .30a | 5.5 (1.0) | 5.6 (1.1) | 5.6 (1.1) | 5.4 (1.2) | .20 |
| 7. Knowledge: effects of vomiting, diet pills, etc. | .29b | 3.2 (1.1) | 3.1 (1.2) | 3.4 (1.2) | 3.1 (1.4) | .22 |
| 8. Belief: ability to resist unhealthy weight loss | .21b | 5.8 (2.0) | 5.8 (2.0) | 6.0 (1.8) | 5.8 (1.9) | .11 |
| 9. Outcome expectancy: steroids | .22b | 6.4 (1.4) | 6.2 (1.5) | 6.3 (1.5) | 6.1 (1.5) | .13 |
| 10. Self-efficacy: eating to become better athlete | .37b | 5.7 (1.4) | 5.8 (1.3) | 6.1 (1.2) | 5.6 (1.4) | .41 |
| 11. Outcome Expectancy: diet pills | .35b | 6.0 (1.5) | 6.0 (1.5) | 6.3 (1.4) | 6.0 (1.5) | .19 |
| Intentions and behavior | ||||||
| 12. Intentions to use steroids/creatine | .47a | 1.5 (0.9) | 1.5 (0.9) | 1.4 (0.9) | 1.6 (1.0) | .15 |
| 13. Intention to engage in unhealthy weight loss | .85a | 1.7 (1.0) | 1.6 (1.0) | 1.7 (1.0) | 1.7 (1.1) | .19 |
| 14. Behavior: steroid/creatine use, past 3 monthsc | .27b | .02 (.13) | .02 (.13) | .01 (.09) | .00 (.06) | .10 |
| 15. Behavior: diet pills, etc., past 3 monthsd | .54b | .29 (.66) | .23 (.60) | .23 (.55) | .21 (.57) | .03 |
aCoefficient α for multiple continuous-item scales.
bTest–retest correlation in control group for single item scales and multiple binary-item scales; the 3–4-month interval between measurements, which included the sport season, may have resulted in construct instability.
cProportion of two behaviors (steroid use, creatine use) in which athlete engaged.
dProportion of five behaviors (not eating, vomiting, laxative use, diet pill use, diuretic use) in which athlete engaged.
eImmediate post-test effect size.
Measures
The 15 constructs included in analyses were assessed through the pre-test, post-test, and long-term follow-up questionnaires. All items are included in Appendix 1. With the exception of intentions for unhealthy weight loss from the EAT-26 (Garner, Olmsted, Bohr, & Garfinkel, 1982), and ability to control mood (Clarke et al., 2001), items were drawn from the ATLAS program (Goldberg et al., 2000). Internal consistency reliabilities (coefficient α) for multiple continuous-item scales are given in Table I. For the remaining scales, the correlation between pre-test and post-test scores in the control group appear in Table I; stability was not expected to be high because the control group had experienced a sport season between the two measurement points.
Mediational Models and Statistical Analyses
All analyses controlled for pre-test differences across groups by including pre-test measures as predictors of corresponding post-test and follow-up measures. Each of the 11 hypothesized mediators was tested in a single mediator analysis to determine whether (i) the intervention changed the mediator and (ii) the change on that mediator was associated with change on the outcome. A multiple mediator model was also tested (see Figure 2). Mediational chains were specified (e.g., intervention → knowledge → self-efficacy → intention) that followed the logic of the ATHENA intervention design and the specific sequence in which content related to the mediators was presented across sessions. The numerical value in the box for each mediator is the specific session in which content aimed at the mediator was presented; temporal ordering was followed for all chains. The models supported the role of each mediator in bringing about change in intentions. Models were estimated in MPlus (Muthén & Muthén, 2006).
Figure 2.

Multiple mediator model predicting intention to use steroids and creatine and intention to engage in unhealthy weight loss and subsequent behaviors. The number in the lower right hand corner of construct boxes indicates the session in which the corresponding intervention material was introduced. Each construct measure in the model is a post-test score with the corresponding pre-test score partialed out. All pre-test measures were allowed to correlate with each other and with the ATHENA treatment variable. Post-test mediator measures within each step were allowed to correlate (i.e., the three knowledge measures, social norms and mood; the two outcome expectancies and self-efficacy; the two intention measures; the two follow-up behavior measures; the two follow-up intention measures). All direct effects of ATHENA were included in the model but only significant paths are depicted. Unstandardized path coefficients are reported. *p < .05, **p < .01, ***p < .001.
Full-information maximum likelihood (FIML) estimation (the Type = missing command) was employed to include all available data. Models were estimated at the individual level with 1668 participants. The hierarchical clustering of students within schools was controlled (the Type = complex command) to yield accurate tests of inference (Raudenbush & Bryk, 2002). Asymmetric confidence limits, which yield tests of significance of the mediated effect with maximum power and accurate Type I error rates, were calculated for each mediated effect using the program PRODCLIN (MacKinnon, Fritz, Williams, & Lockwood, 2007).
Single-mediator analyses were conducted following MacKinnon (2008). For each mediator, four values (c, a, b, c′) characterized the relationships among the intervention (X), mediator (M), and outcome (Y). The c path is the total effect of the intervention X on outcome Y. The a path is the effect of the intervention X on the mediator M. The b path is the relationship of mediator M to outcome Y. The product of the a and b paths, ab, is the mediated effect, the part of the total program effect transmitted through the mediator. Statistical significance of the ab estimate is evidence of mediation. The c′ path (c′ = c − ab) is the direct effect of the intervention X on outcome Y not transmitted through the mediator. Finally, meditational analysis of the multiple mediator model permitted tests of unique contributions of mediators and estimates of the proportion of the total effect transmitted through each meditational chain.
ATHENA aimed to lower behavioral intentions to prevent future harmful behaviors. Immediate post-test intentions served as primary outcomes. The multiple mediator model examined prediction of intentions over time and long-term follow-up behaviors.
Results
Equivalence of ATHENA and Control Groups at Pre-test and Attrition Analyses
Table I gives means and standard deviations on all constructs at pre-test and immediate post-test. Pre-test equivalence was tested in models in which the treatment variable alone predicted each pre-test score. The intervention and control groups did not differ for 13 of the 15 measures. Intervention participants had more knowledge of steroids (β = .51, z = 2.70, d = .30) and engaged in fewer unhealthy weight loss behaviors (β = .065, z = 1.96, d = .10) than control participants. Pre-test scores of those retained versus lost to follow up were examined to test for differential attrition across condition (Jurs & Glass, 1971). Of the thirty models tested (15 constructs for two retention times), there was only one significant condition by retention interaction, as expected by chance. Girls with lower steroid outcome expectancies were more likely to be retained in ATHENA than in the control condition (β = −0.037, z = −2.54, p < .05).
Total effects
Immediate Post-test Intentions
Based on c paths (the total effects of treatment on intentions), reported in Table II, ATHENA produced small effect size decreases in immediate post-test intentions to use steroids (β = −0.123, z = −3.09, p < .01, Cohen's d = .15) and to engage in unhealthy weight loss (β = −0.148, z = −2.77, p < .01, d = .19) relative to control participants.
Table II.
Estimates from the Single Mediator Models on Both Immediate Post-test Intention Measures
| 95% CL of mediated effect |
||||||
|---|---|---|---|---|---|---|
| Mediators | a | b | c′ | ab | Lower | Upper |
| Outcome: Post-test intention to use steroids/creatine | ||||||
| Knowledge: harmful effects of steroids | .949* | −.059* | −.055 | −.056* | −.089 | −.027 |
| Knowledge: nutrition for sport performance | .308* | −.089* | −.089* | −.027* | −.051 | −.010 |
| Peer norm for steroid use | −.017 | .053* | −.124* | −.001 | −.008 | .006 |
| Social norms: coach and magazines | −.223* | .337* | −.053 | −.075* | −.120 | −.035 |
| Mood management | .203* | −.169* | −.090* | −.034* | −.059 | −.013 |
| Outcome expectancy: steroids | .192 | −.163* | −.090* | −.031 | −.075 | .010 |
| Self-efficacy: eating to become better athlete | .497* | −.145* | −.054 | −.072* | −.118 | −.034 |
| Outcome: Intention to engage in unhealthy weight loss practices | ||||||
| Knowledge: nutrition for sport performance | .309* | −.071* | −.122* | −.022* | −.044 | −.005 |
| Social norms: coach and magazines | −.224* | .301* | −.075 | −.067* | −.106 | −.032 |
| Peer norm for eating disorders | .038 | .034* | −.155* | .001 | −.008 | .011 |
| Mood management | .203* | −.133* | −.120* | −.027* | −.0461 | −.010 |
| Knowledge: harmful effects of vomiting, diet pills, etc. | .226* | −.071* | −.127* | −.016* | −.036 | −.006 |
| Belief: ability to resist unhealthy weight loss | .225 | −.064* | −.133* | −.014 | −.033 | .001 |
| Self-efficacy: eating to become better athlete | .498* | −.145* | −.079 | −.072* | −.117 | −.035 |
| Outcome expectancy: diet pills | 260* | −.155* | −.104* | −.040* | −.070 | −.015 |
Note. Unstandardized paths are reported. *p<.05. The total effect of ATHENA on intention to use steroids/creatine (c path) was –.123*. The total effect of ATHENA on intention for unhealthy weight loss (c path) was –.148*. CL: asymmetric confidence limits around ab mediated effect.
Long-term Follow up
ATHENA reduced long-term follow-up intentions to use steroids and creatine (β = −0.128, z = −2.16, p < .05, d = .11; ATHENA, M = 1.5, SD = 0.9; Control, M = 1.6, SD = 1.0) and tended to do so for intentions to engage in unhealthy weight loss (β = −0.130, z = −1.76, p = .08, d = .09; ATHENA, M = 1.7, SD = 1.2; Control, M = 1.8, SD = 1.1). At long-term follow-up, there was no effect of ATHENA on steroid and creatine use (β = .001, z = 0.11, ns; ATHENA, M = 0.02, SD = 0.2; Control, M = 0.02, SD = 0.2, d = 0) and unhealthy weight loss behaviors (β = −0.020, z = −0.55, ns; ATHENA, M = 0.3, SD = 0.7; Control, M = 0.3, SD = 0.6, d = 0).
Single Mediator Models
We estimated seven single mediator models for the outcome “intention to use steroids/creatine” and eight single mediator models for the outcome “intention to engage in unhealthy weight loss behaviors”; four mediators were common to both intention measures. Results are given in Table II. ATHENA had the intended effect on seven of the 11 putative mediators, as indicated by significant a paths. All mediators significantly related to the outcome (significant b paths). Significant ab paths supported mediation in 11 of 15 instances; in Table II asymmetric confidence limits (CL) that do not include zero indicate significance of an ab path. Finally, the c′ path shows the direct effect of the intervention on the outcome, not transmitted through the mediator; non-significant c′ paths indicated that the mediator completely mediated the effect of the intervention on the outcome.
We calculated the proportion mediated (ab/c) as an effect size measure for each mediator (MacKinnon, 2008), that is, the proportion of the total effect of the ATHENA intervention on an outcome (c) that is carried through a mediator (ab). Social norms, self-efficacy, and knowledge of steroid effects mediated the largest proportion of the effect of ATHENA on intention to use steroids/creatine, .61, .59, and .46, respectively. Social norms, self-efficacy, and outcome expectancies mediated the largest proportions of the effect of ATHENA on intention to engage in unhealthy weight loss practices, .49, .45, and .27, respectively. The sum of these measures exceeds one, since the mediators are correlated and the proportions are thus in part overlapping.
Multiple Mediator Model
The multiple mediator model contained all but three mediators; the omitted mediators (peer norms for steroids, peer norms for eating disorders, belief in ability to resist unhealthy weight loss) were not affected by ATHENA. Outcome expectancy for steroids was retained because it was predicted from steroid knowledge and not directly from ATHENA. The multiple mediator model assessed the contribution of each mediator in the presence of all other mediators and included a test of whether post-test intentions predicted behaviors and intentions at long-term follow-up. All constructs were predicted by corresponding pre-test measures to control for baseline levels; these paths are not shown. A path from ATHENA to each construct was estimated in the model; only significant paths are shown.
Model fit was adequate [χ2(209) = 706.474, p<.001, CFI = .911, RMSEA = .038, SRMR = .062]. The multiple mediator model explained a large proportion of variance in intention to use steroids/creatine (R2 = 0.317) and in intention to engage in unhealthy weight loss (R2 = 0.532). Hypothesized mediational chains were supported. These included the linkages from knowledge to outcome expectancies, from knowledge and norms to self-efficacy, and from outcome expectancies, norms, self-efficacy and mood management to intentions. The direct paths from ATHENA to both intention measures were non-significant, indicating that the set of mediators fully mediated the relation of ATHENA to immediate post-test intentions. Post-test intentions predicted corresponding behaviors at long-term follow-up. Long-term follow-up intentions were predicted by corresponding follow-up behaviors and post-test intentions.
Proportion-mediated measures in the multiple mediator model assessed the proportion of the difference between the ATHENA and control means (total effect of treatment) uniquely attributable to each mediated chain from ATHENA to intention (see Appendix 2 for an explanation of the computation, Appendix 3 for estimates for steroid/creatine use, and Appendix 4 for estimates for unhealthy weight loss). The strongest mediated effects were the same across the two intention measures. The mediated effect that accounted for the largest proportion of the total effect was the chain from ATHENA through social norms to intention (.45, .40 of the total effect for steroids/creatine and unhealthy weight loss, respectively). The second largest mediated effect was from ATHENA through self-efficacy to intention (an additional .17, .20 of the total effect for steroids/creatine and unhealthy weight loss, respectively).
Discussion
This article extends Elliot et al. (2004, 2006, 2008) by documenting the putative mechanisms through which ATHENA produced outcomes. The impact of ATHENA on knowledge, self-efficacy, social norms, mood management, and intentions was replicated in the full three cohorts of participants. Elliot et al. (2004, 2006) found immediate post-test effects of ATHENA on diet pill use and on a measure of amphetamine, anabolic steroid, and sport substance use. We found no effects on weight loss and athletic enhancing substances at 9-month follow-up (see Elliot et al., 2008 for post-high school follow up). Results support the focus of ATHENA as a primary prevention program that had a stronger effect on reducing intentions for new unhealthy behaviors than on reducing the rare unhealthy behaviors themselves.
We can clearly state that changes in knowledge, norms, mood management, outcome expectancies for risky behaviors, and self-efficacy were associated with salutary changes in intentions, which, in turn, were associated with behavior. The multiple mediator model provided a thorough examination of how the program impacted participants. Following the call for the development of hybrid models of health behavior (Baranowski, Cullen, & Baranowski, 1999), we drew from three well researched models of health behavior and the sequential eight-session design of ATHENA to specify an integrated model of the intervention. Strong support accrued for the hypothesized mediators within ATHENA, in that all constructs were related to one or both outcome intentions (b paths of Table II). Diminished intentions for high risk behaviors at immediate post-test were maintained over a 9-month period and were related to behavior at follow-up. The majority of intervention components led to changes on the mediators (a paths of Table II). The intervention did not change peer norms or reported ability to resist unhealthy weight loss practices; thus we cannot conclude whether a change in peer norms or resistance skills would lead to a change in targeted outcomes. These mediators did correlate with intentions; thus targeting these constructs effectively may strengthen interventions.
The strongest mediator of the ATHENA effects was the social norm construct which measured perceived injunctive norms from the coach and from magazine advertisements. Coach beliefs are important influences on female adolescent disordered eating (Fender-Scarr, 1999). Magazine ads relate to restricting calories and diet pill use among female adolescents (Thomsen, Weber, & Beth Brown, 2002). Results suggest that changing female adolescents’ distorted perceptions of normative behavior reduces their risk for unhealthy body shaping behaviors.
Self-efficacy for eating to become a better athlete was the second strongest mediator of the effect of ATHENA on both intention measures. Athletes learned how to include proper nutrients in their diet to improve their athletic performance while also learning about harmful side effects of steroids, diet pills, fasting, etc. Having a positive behavior to substitute for the risky behavior may have been important. Leventhal (1970) theorized that when people are threatened with negative health outcomes and given viable steps to protect themselves, they mitigate the threat through protective behavior. Given no path to protection, they deny the threat.
A third essential mediator of the effect of ATHENA on both intentions measures was knowledge of the harmful effects of the behaviors. This replicates findings from the ATLAS program for steroid use among male high school athletes (MacKinnon et al., 2001). Knowledge of risks is not typically an effective prevention strategy for adolescents. As MacKinnon et al. (2001) speculated, however, teaching of harmful effects of steroids and diet pills may have succeeded because participants acquired new information about behaviors that are less common than other typically studied risky behaviors such as alcohol use and smoking.
Mood management also mediated both intention measures. Negative affect has been shown to be associated with disordered eating among adolescents (Santos et al., 2007). Targeting mood management in ATHENA reduced intentions for high-risk behavior.
Several limitations exist. Data are self-reported and are thus vulnerable to biases (e.g., under-reporting of high risk behavior). One or two item scales may have limited the strength of observed relations (e.g., the low stability measure of ability to resist unhealthy weight loss, which apparently was not affected by ATHENA). Incomplete specification of mediators is a potential limitation of all models. Significant program effects were found, however, and effects were almost completely explained by included mediators.
Our findings may be restricted to athletes retained in a sport throughout a sport season. Most attrition was due to not completing the sport season. Those lost to follow-up had slightly higher intentions for unhealthy weight loss behaviors (d = .15) and unhealthy weight loss behaviors (d = .16). High-risk behavior among participants was low; ATHENA served as primary prevention and may not be as successful for girls well engaged in risky body-shaping behaviors.
Implications for Practitioners
The mediation analyses suggest important content for interventions. Given powerful media impact on dieting behaviors, deconstructing media content is a critical point of intervention. The component that paired information about nutrition and sport performance with concrete behavioral strategies can be used broadly in educational settings. The effective mood control strategy provides a model for helping adolescents maintain emotional equilibrium.
The strategies employed to deliver the intervention may provide useful approaches for practitioners. Peer-led group activities supported participant involvement. Lytle et al. (2004) argued for use of peer leaders in school-based diet interventions. Active participation in ongoing activities, keeping diaries of activities and mood states, as well as carrying out exercises related to nutrition stimulated involvement in the program. Participation of powerful adult figures (here the coach) who are part of the adolescents’ authority system rather than health promotion specialists from outside may be an important vehicle of intervention.
Conclusion
The ATHENA program found success through sport team implementation endorsed by the participants’ coach and led by their peers, targeting knowledge, outcome expectancies, mood management, norms, and self-efficacy. Similar mediational paths led to reduction in intentions to engage in unhealthy weight loss and steroids and creatine use. These relations among constructs were supported by past research, primarily within unhealthy weight loss behaviors; the research on steroid and creatine use among female adolescents is limited.
The number of female and male high school students engaged in sports has been on the rise for the past 19 years, and 55% participated in the 2007–08 school year (National Federation of State High School Associations, 2008). As such, sport team interventions have substantial reach and should be considered as settings for health promotion programs. Targeting social norms, self-efficacy for healthy eating, and harmful effects of risk behaviors were effective prevention strategies for unhealthy body shaping practices among female adolescent athletes. Mediation analyses aid in the understanding of ATHENA and inform program development.
Funding
National Institute on Drug Abuse [DA07356, DA09757].
Conflict of interest: ATHENA is a program on the Substance Abuse and Mental Health Services Administration's National Registry of Evidence-based Programs and Practices (http://www.nrepp.samhsa.gov/programfulldetails.asp?PROGRAM_ID=111), and it is distributed through the Center for Health Promotion Research at Oregon Health & Science University (OHSU). OHSU and Drs. Elliot and Goldberg have a financial interest from the commercial sale of technologies used in this research. This potential conflict of interest has been reviewed and managed by the OHSU Conflict of Interest in Research Committee.
Appendix 1. Items and Calculation of Each Construct
| Measure | Items | Responses | Computation |
|---|---|---|---|
| 1. Knowledge: harmful effects of steroids | Please mark whether or not you think these health problems can really be caused by anabolic steroids. A. Kidney disease B. Facial hair C. Deepened voice D. Severe acne E. Psychotic, “crazy” F. AIDS by sharing needles G. Hair loss | 1 = strongly disagree … 7 = strongly agree | Items were recoded as 0 = incorrect, 1 = correct and the sum of correct responses was calculated. |
| 2. Knowledge: nutrition for sport performance | What I eat is important for how I perform in sports. | 1 = strongly disagree … 7 = strongly agree | This item was used. |
| 3. Peer norm for steroid use | Out of every 100 girl students at your school who play sports, or are on the dance or rally squads, how many do you think have ever used anabolic steroids even once? Out of every 100 girl students at other schools who play sports, or are on the dance or rally squads, how many do you think have ever used anabolic steroids even once? | 0 = 0, 1 = 1–5, 2 = 6–10, 3 = 11–15, 4 = 16–20, 5 = 21–30, 6 = 31–40, 7 = 41–50, 8 = 51–70, 9 = 71–99, 10 = 100 Same for both items. | The mean of these two items was computed. |
| 4. Social norms: coach and magazines | Most products advertised in magazines do what they say they do. Ads in magazines are based on science and usually are true. My coach thinks that being thin is best. My coach keeps a close watch on team members’ weights. My coach has told me to lose weight. | 1 = strongly disagree … 7 = strongly agree Same for all 5 items. | The mean of these five items was computed. |
| 5. Peer norm for eating disorders | Out of every 100 girls at your school who play sports, or are on the dance or rally squads, how many do you think have ever had an eating disorder or used drugs to lose weight, even once? Out of every 100 girl students at other schools who play sports, or are on the dance or rally squads, how many do you think have ever had an eating disorder or used drugs to lose weight, even once? | 0 = 0, 1 = 1–5, 2 = 6–10, 3 = 11–15, 4 = 16–20, 5 = 21–30, 6 = 31–40, 7 = 41–50, 8 = 51–70, 9 = 71–99, 10 = 100 Same for both items. | The mean of these two items was computed. |
| 6. Belief: ability to control mood | I know how to control my moods or emotions. In general, when you do more fun things, your mood is better. | 1 = strongly disagree … 7 = strongly agree Same for both items. | The mean of these two items was computed. |
| 7. Knowledge: effects of vomiting, diet pills, etc. | Please mark whether or not you think that these health problems can really be caused by vomiting or using diet pills, laxatives, or diuretics to lose weight. A. Reduced female hormones B. Muscle weakness C. Dental problems D. Stomach ulcers E. Urinary infections F. Bone weakening G. Hair loss | 1 = strongly disagree … 7 = strongly agree Same for all 7 items. | Items were recoded as 0 = incorrect, 1 = correct. The scale was created as a sum of correct responses on these seven items. |
| 8. Belief: ability to resist unhealthy weight loss | I know how to turn down someone wanting me to skip meals or use drugs and other unhealthy behaviors to lose weight. | 1 = strongly disagree … 7 = strongly agree | This item was used. |
| 9. Outcome expectancy: steroids | If I were to use anabolic steroids, they probably wouldn’t have any bad effects. | 1 = strongly disagree … 7 = strongly agree | This item was reverse coded. |
| 10. Self-efficacy: eating to become better athlete | I know the basics of a good eating style to help become a better athlete. | 1 = strongly disagree … 7 = strongly agree | This item was used. |
| 11. Outcome expectancy: diet pills | If I were to use diet pills, they probably wouldn’t have any bad effects. | 1 = strongly disagree … 7 = strongly agree | This item was reverse coded. |
| 12. Intentions to use steroids/creatine | In the future, I would consider using muscle building supplements that you can buy at a health foods store (like creatine, DHEA, or Megabolics). In the future, I would consider using anabolic steroids. | 1 = strongly disagree … 7 = strongly agree Same for both items. | The mean of these two items was used. |
| 13. Intention to engage in unhealthy weight loss | In the future, I would consider using drugs to control my weight. I would use drugs to make myself vomit to lose weight, if that would help my team win or help me get a college athletic scholarship. In the future, I would consider using diet pills (such as Dexatrim) or energy pills (such as No Doz) to lose weight. I would use drugs to control my weight if more of my teammates used them. If I gained weight, I would make myself vomit or use drugs. In the future, I would vomit or use drugs to control my weight if more of my friends or teammates did this. | 1 = strongly disagree … 7 = strongly agree Same for all 6 items. | The mean of these six items was used. |
| 14. Behavior: steroid/creatine use in past 3 months | How many times (if any) have you used anabolic steroids in the last 3 months? How many times (if any) have you used muscle building supplements that you can buy at a health foods store (like creatine, DHEA, or Megabolics) in the last 3 months? | 0 = none, 1 = 1–2, 2 = 3–5, 3 = 6–9, 4 = 10–19, 5 = 20–39, 6 = 40+ Same for both items. | Recoded into binary variables and summed to create measure. |
| 15. Behavior: vomiting, diet pills, etc., in past 3 months | How many times (if any) have you not eaten for a day or more to lose weight in the last 3 months? Laxatives are sometimes used to lose weight. How many times (if any) have you used laxatives to lose weight in the last 3 months? Some people make themselves vomit (throw up) to lose weight. How many times (if any) have you made yourself vomit to lose weight in the last 3 months? Appetite suppressant pills, sometimes called diet pills, are used to lose weight. How many times (if any) have you used diet pills (such as Dexatrim) or energy pills (such as No Doz) to lose weight in the last 3 months? Diuretics are sometimes used to lose weight, especially “water weight.” How many times (if any) have you used diuretics to lose weight in the last 3 months? | 0 = none, 1 = 1–2, 2 = 3–5, 3 = 6–9, 4 = 10–19, 5 = 20–39, 6 = 40+ Same for all 5 items. | Recoded into binary variables and summed to create measure. |
Appendix 2
Computation of estimates of the proportion of the total effect that is uniquely attributable to each mediational chain is explained. These estimates are non-redundant because each path coefficient is estimated with all others held constant. Computation of the proportion mediated measures for the full model is shown below for intention to use steroids/creatine and in Appendix 3 for intention to engage in unhealthy weight loss. Each mediated effect is the product of the unstandardized path coefficients along a meditational chain, as shown in Figure 2. The sum of these mediated effects plus the direct effect (c′) equals the total effect. The product of path coefficients on a single meditational chain divided by the total effect equals the proportion mediated by that chain.
Appendix 3. Unstandardized Path Estimates of the Effects of ATHENA on Intentions to Use Steroids/Creatine and Proportion-Mediated Measures
| Mediators | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mediational Chain | Knowledge of steroids | Knowledge of nutrition | Social Norms | Mood Maintenance | Self-efficacy | Outcome Expectancies for steroids | Intention to use steroids/creatine | Estimate of effect | Proportion mediated |
| Session 2 | Session 1, 2 | Session 4 | Session 3 | Session 4 | Sessions 5, 6 | Session 8 | |||
| 1 | .976 | .059 | −.090 | −.005 | .0417 | ||||
| 2 | .305 | .258 | −.058 | −.010 | .0833 | ||||
| 3 | .335 | −.058 | −.020 | .1667 | |||||
| 4 | −.219 | −.508 | −.090 | −.005 | .0416 | ||||
| 5 | −.219 | –.270 | −.058 | −.003 | .0250 | ||||
| 6 | −.219 | .248 | −.054 | .4500 | |||||
| 7 | .197 | −.082 | −.016 | .1333 | |||||
| Direct effect | −.006 | −.006 | .0500 | ||||||
| Total effect | −.120 | 1 | |||||||
Note. The total effect (row 9) is the difference between the means of the Athena versus control group on intention to use steroids/creatine at immediate post-test adjusted for pre-test, as estimated in the full mediator model of Figure 2. Each of rows 1 through 7 represents a distinct mediational chain from the Athena intervention to intention to use steroid/creatine. Row 1 shows the unstandardized path coefficient from Athena to Knowledge of steroids (.976) to outcome expectancies for steroids (.059) to intention for steroids/creatine use (−.090). The product of these three paths [(.976)(.059)(−.090) = −.005] is the mediated effect for this path. Row 8 is the direct effect (unmediated) of Athena to intention. The sum of the 8 estimates of effects is the total effect of Athena on intention (−.120). For each path, the proportion mediated is the estimate of effect for that path divided by the total effect (e.g., −.005/−.120 = .0417 for row 1).
Appendix 4. Unstandardized Path Estimates of the Effects of ATHENA on Intentions to Engage in Unhealthy Weight Loss Behaviors and Proportion-Mediated Measures
| Mediators | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mediational chain | Knowledge of diet pills, laxatives, etc. | Knowledge of nutrition | Social norms | Mood Maintenance | Self-efficacy | Outcome expectancies for diet pills | Intention unhealthy weight loss | Estimate of effect | Proportion mediated |
| Session 2 | Session 1, 2 | Session 4 | Session 3 | Session 4 | Sessions 5, 6 | Session 8 | |||
| 1 | .267 | .072 | −.061 | −.001 | .0078 | ||||
| 2 | .197 | −.053 | −.010 | .0775 | |||||
| 3 | −.219 | .234 | −.051 | .3950 | |||||
| 4 | −.219 | −.270 | −.078 | −.005 | .0388 | ||||
| 5 | −.219 | −.555 | −.061 | −.008 | .0620 | ||||
| 6 | .335 | −.078 | −.026 | .2020 | |||||
| 7 | .309 | .258 | −.078 | −.006 | .0465 | ||||
| Direct effect | −.022 | −.022 | .1705 | ||||||
| Total effect | −.129 | −.129 | 1 | ||||||
Note. The total effect (row 9) is the difference between the means of the Athena versus control group on intention for unhealthy weight loss behaviors at immediate post-test adjusted for pre-test, as estimated in the full mediator model of Figure 2. Each of rows 1 through 7 represents a distinct mediational chain from the Athena intervention to intention for unhealthy weight loss behavior. Row 1 shows the unstandardized path coefficient from Athena to Knowledge of diet pills (.267) to outcome expectancies for diet pills (.072) to intention for unhealthy weight loss behavior (−.061). The product of these three paths [(.267)(.072)(−.061) = −.001] is the mediated effect for this path. Row 8 is the direct effect (unmediated) of Athena to intention. The sum of the 8 estimates of effects is the total effect of Athena on intention (−.129). For each path, the proportion mediated is the estimate of effect for that path divided by the total effect (e.g., −.001/−.129 = .0078 for row 1).
References
- Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991;50:179–211. [Google Scholar]
- Bandura A. Social cognitive theory: An agentic perspective. Annual Review of Psychology. 2001;52:1–26. doi: 10.1146/annurev.psych.52.1.1. [DOI] [PubMed] [Google Scholar]
- Baranowski T, Cullen KW, Baranowski J. Psychosocial correlates of dietary intake: Advancing dietary intervention. Annual Review of Nutrition. 1999;19:17–40. doi: 10.1146/annurev.nutr.19.1.17. [DOI] [PubMed] [Google Scholar]
- Baranowski T, Perry CL, Parcel GS. How individuals, environments, and health behavior interact. In: Glanz K, Rimer BK, Lewis FM, editors. Health behavior and health education: theory, research, and practice. 3rd. San Francisco: Jossey-Bass; 2002. pp. 165–182. [Google Scholar]
- Clarke GN, Hornbrook M, Lynch F, Polen M, Gale J, Beardslee W, et al. A randomized trial of a group cognitive intervention for preventing depression in adolescent offspring of depressed parents. Archives of General Psychiatry. 2001;58:1127–1134. doi: 10.1001/archpsyc.58.12.1127. [DOI] [PubMed] [Google Scholar]
- Elliot DL, Goldberg L, Moe EL, DeFrancesco CA, Durham MB, Hix-Small H. Preventing substance use and disordered eating: Initial outcomes of the ATHENA (Athletes Targeting Healthy Exercise and Nutrition Alternatives) Program. Archives of Pediatric and Adolescent Medicine. 2004;158:1043–1049. doi: 10.1001/archpedi.158.11.1043. [DOI] [PubMed] [Google Scholar]
- Elliot DL, Goldberg L, Moe EL, DeFrancesco CA, Durham MB, McGinnis W, et al. Long-term outcomes of the ATHENA (Athletes Targeting Health Exercise & Nutrition Alternatives) program for female high school athletes. Journal of Alcohol & Drug Education. 2008;52:73–92. [PMC free article] [PubMed] [Google Scholar]
- Elliot DL, Moe EL, Goldberg L, DeFrancesco CA, Durham MB, Hix-Small H. Definition and outcome of a curriculum to prevent disordered eating and body-shaping drug use. Journal of School Health. 2006;76:67–73. doi: 10.1111/j.1746-1561.2006.00070.x. [DOI] [PubMed] [Google Scholar]
- Everson ES, Daley AJ, Ussher M. The theory of planned behaviour applied to physical activity in young people who smoke. Journal of Adolescence. 2007;30:347–351. doi: 10.1016/j.adolescence.2006.11.001. [DOI] [PubMed] [Google Scholar]
- Fender-Scarr LK. An investigation of athlete, coach, and family variables in relationship to eating pathology in adolescent female gymnasts. DAI. 1999;59:3743. [Google Scholar]
- Fisher JD, Fisher WA. Changing AIDS risk behavior. Psychological Bulletin. 1992;111:455–474. doi: 10.1037/0033-2909.111.3.455. [DOI] [PubMed] [Google Scholar]
- Franko DL, Mintz LB, Villapiano M, Green TC, Mainelli D, Folensbee L, et al. Food, mood and attitude: Reducing risk for eating disorders in college women. Health Psychology. 2005;24:567–578. doi: 10.1037/0278-6133.24.6.567. [DOI] [PubMed] [Google Scholar]
- Garner DM, Olmsted MP, Bohr Y, Garfinkel PE. The eating attitudes test: Psychometric features and clinical correlates. Psychological Medicine. 1982;12:871–878. doi: 10.1017/s0033291700049163. [DOI] [PubMed] [Google Scholar]
- Goldberg L, MacKinnon DP, Elliot DL, Moe EL, Clarke G, Cheong J. The adolescents training and learning to avoid steroids program. Archives of Pediatrics & Adolescent Medicine. 2000;154:332–338. doi: 10.1001/archpedi.154.4.332. [DOI] [PubMed] [Google Scholar]
- Jackson KM, Aiken LS. Evaluation of a multicomponent appearance-based sun-protective intervention for young women: Uncovering the mechanisms of program efficacy. Health Psychology. 2006;25:34–46. doi: 10.1037/0278-6133.25.1.34. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Bethesda, MD: NIDA; 2004. Monitoring the future national survey results on drug use, 1975–2003. Volume I: Secondary school students. NIH Publication No. 04-5507. [Google Scholar]
- Jurs SG, Glass GV. The effect of experimental mortality on the internal and external validity of the randomized comparative experiment. Journal of Experimental Education. 1971;40:62–66. [Google Scholar]
- Leventhal H. Findings and theory in the study of fear communications. In: Berkowitz L, editor. Advances in experimental social psychology. Vol. 5. New York: Academic Press; 1970. pp. 119–186. [Google Scholar]
- Lovstakken K, Peterson L, Homer AL. Risk factors for anabolic steroid use in college students and the role of expectancy. Addictive Behaviors. 1999;24:425–430. doi: 10.1016/s0306-4603(98)00060-4. [DOI] [PubMed] [Google Scholar]
- Lytle LA, Murray DM, Perry CL, Story M, Birnbaum AS, Kubik MY, et al. School-based approaches to affect adolescents’ diets: Results from the TEENS study. Health Education and Behavior. 2004;31:270–287. doi: 10.1177/1090198103260635. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP. Introduction to statistical mediation analysis. Mahwah, NJ: Erlbaum; 2008. [Google Scholar]
- MacKinnon DP, Fritz MS, Williams J, Lockwood CM. Distribution of the product confidence limits for the indirect effect program PRODCLIN. Behavioral Research Methods. 2007;39:384–389. doi: 10.3758/bf03193007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Goldberg L, Clarke GN, Elliot DL, Cheong J, Lapin A, et al. Mediating mechanisms in a program to reduce intentions to use anabolic steroids and improve exercise self-efficacy and dietary behavior. Prevention Science. 2001;2:15–28. doi: 10.1023/a:1010082828000. [DOI] [PubMed] [Google Scholar]
- Muthén L, Muthén B. Mplus 4 User's Guide. Los Angeles, CA: Muthén & Muthén; 2006. [Google Scholar]
- National Federation of State High School Associations. High school sports participation increases again; boys, girls and overall participation reach all-time highs. 2008. Retrieved from www.nfhs.org/web/2008/09/high_school_sports_participation.aspx on October 7, 2008.
- National Institute on Drug Abuse. NIDA research report; Steroid abuse and addiction. Bethesda, MD: NIDA, NIH, DHHS; 2000. NIH Pub. No. 00-3721. [Google Scholar]
- Nichols JF, Rauh MJ, Lawson MJ, Ming J, Barkai H-S. Prevalence of the female athlete triad syndrome among high school athletes. Archives of Pediatric Adolescent Medicine. 2006;160:127–142. doi: 10.1001/archpedi.160.2.137. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical linear models: Applications and data analysis methods. 2nd. Thousand Oaks, CA: Sage; 2002. [Google Scholar]
- Roberts TA, Glen J, Kreipe RE. Disordered eating and menstrual dysfunction in adolescent female athletes participating in school-sponsored sports. Clinical Pediatrics. 2003;42:561–564. doi: 10.1177/000992280304200613. [DOI] [PubMed] [Google Scholar]
- Santos M, Richards CS, Bleckley MK. Comorbidity between depression and disordered eating in adolescents. Eating Behaviors. 2007;8:440–449. doi: 10.1016/j.eatbeh.2007.03.005. [DOI] [PubMed] [Google Scholar]
- Schmiege SJ, Aiken LS, Sander JL, Gerend MA. Osteoporosis prevention among young women: Psychosocial models of calcium consumption and weight-bearing exercise. Health Psychology. 2007;26:577–587. doi: 10.1037/0278-6133.26.5.577. [DOI] [PubMed] [Google Scholar]
- Thomson SR, Weber MM, Beth Brown L. The relationship between reading beauty and fashion magazines and the use of pathogenic dieting methods among adolescent females. Adolescence. 2002;37:1–18. [PubMed] [Google Scholar]
- West SG, Aiken LS. Towards understanding individual effects in multiple component prevention programs: Design and analysis strategies. In: Bryant K, Windle M, West S, editors. The science of prevention: Methodological advances from alcohol and substance abuse research. Washington, DC: APA; 1997. pp. 167–209. [Google Scholar]
- Whaley AL. Preventing the high-risk sexual behavior of adolescents: Focus on HIV/AIDS transmission, unintended pregnancy, or both? Journal of Adolescent Health. 1999;24:376–382. doi: 10.1016/s1054-139x(98)00153-0. [DOI] [PubMed] [Google Scholar]