

Abstract
A total of 13 to 14% of European and North American workers are involved in shift work. The present aim is to explore the relationships between coping strategies adopted by shift workers and their leisure-time energy expenditure. Twenty-four female and 71 male shift workers (mean ± SD age: 37 ± 9 years) completed an adapted version of the Standard Shift-work Index (SSI), together with a leisure-time physical activity questionnaire. Predictors of age, time spent in shift work, gender, marital status and the various shift-work coping indices were explored with step-wise multiple regression. Leisure-time energy expenditure over a 14-d period was entered as the outcome variable. Gender (β = 7168.9 kJ/week, p = 0.023) and time spent in shift work (β = 26.36 kJ/week, p = 0.051) were found to be predictors of energy expenditure, with the most experienced, male shift workers expending the most energy during leisure-time. Overall ‘disengagement’ coping scores from the SSI were positively related to leisure-time energy expenditure (β = 956.27 kJ/week, p = 0.054). In males disengagement of sleep problems (β = −1078.1 kJ/week, p = 0.086) was found to be negatively correlated to energy expenditure, whereas disengagement of domestic-related problems was found to be positively related to energy expenditure (β = 1961.92 kJ/week, p = 0.001). These relations were not found in female shift workers (p = 0.762). These data suggest that experienced male shift workers participate in the most leisure-time physical activity. These people ‘disengage’ more from their domestic-related problems, but less from their sleep-related problems. It is recommended that physical activity interventions for shift workers should be designed with careful consideration of individual domestic responsibilities and perceived disruption to sleep.
Keywords: domestic work, exercise, nocturnal work, sleep-wake cycles
1. Introduction
For many years, shift work has been required to provide emergency cover and essential services at all hours of the day and night, as well as for maintaining long-term industrial processes. Nevertheless, shift work is no longer restricted to these types of occupations, but is increasingly found in modern ‘call centres’, where employees deliver financial and retail services around the clock to meet the demands of a ’24-h’ society, in shops, and so on. It is not surprising, therefore, that approximately 13–14% of the European and North American workforce is now involved in a shift-work schedule that includes some time spent working at night (Spelten et al. 1999, Harrington 2001, Rajaratnam and Arendt 2001, Costa 2003). Many employees can also be found working ‘unusual hours’; outside of the ‘normal’ 09.00 – 17.00 hours period, but not necessarily involving night work, e.g. the permanent early morning shifts worked by postal delivery personnel or the shorter morning and evening ‘split-shifts’ worked by public transport staff or office cleaners (Taylor et al. 1997).
Shift-work schedules differ markedly in terms of organisation, timing and duration of each shift, as well as in the speed of shift rotation of the shifts. Whilst there might be benefits of working ‘unusual hours’ and shifts, such as increased wages, shift work, and in particular that including night work, has been associated with greater health problems in comparison to ‘normal’ day work (Waterhouse et al. 1992, Harrington 2001). The health effects of shift work can include a reduction in quality and quantity of sleep, insomnia, chronic fatigue, anxiety and depression, adverse cardiovascular and gastrointestinal effects and reproductive effects in women. More recently, links between shift work and an increased risk of obesity have been proposed (Lasfargues et al. 1996, Karlsson et al. 2001, Di Lorenzo et al. 2003). The accumulative sleep deprivation that is associated with shift work is also thought to have long-term effects in the form of ‘allostatic load’, which refers to the cumulative wear and tear on body systems (McEwen 2007). Such loading has been forwarded as a contributory factor to hypertension, reduced parasympathetic tone, increased pro-inflammatory cytokines, increased oxidative stress, increased evening cortisol and insulin, as well as an overall increased risk of obesity (McEwen 2007). The exact explanation for the detrimental effects of shift work on health is complicated. Nevertheless, most general reviews have suggested that the health inequalities associated with shift work are biological and behavioural in nature (Waterhouse et al. 1992, Harrington 2001, Costa 2004, Knutsson 2004). Harrington (2001) identified improvements in recreational facilities as a factor that could potentially ameliorate shift-work problems in the short term. Furthermore, Harrington (2001) and Harma et al. (1982, 1988a) highlighted the importance of physical fitness and activity in helping workers reduce the problems associated with shift work. Whilst various studies have highlighted the problems associated with shift work and have sought to develop recreational/leisure/physical activity recommendations to help alleviate such problems, few have addressed the implementation of practical coping strategies within an ‘actual’ working environment.
The extent to which individuals cope with shift work is very heterogeneous (Lasfargues et al. 1996, Karlsson et al. 2001, Di Lorenzo et al. 2003). As such, most researchers would agree that it is imperative to consider how individuals cope with working shifts and how they deal with the possible health problems that they might experience. Whilst a number of reviews, booklets and guides on how to cope with irregular working hours have been produced (Monk and Folkard 1992, Harrington 2001, Costa 2003), little attention has focused on how individuals actually cope with shift work and examining how effective are the strategies they employ at sustaining health and wellbeing. A more systematic approach to exploring individual coping strategies may help to understand why some individuals seem to be more successful than others (Spelten et al. 1993).
Coping refers to individuals’ behavioural and cognitive efforts to manage situations that are viewed as taxing personal resources (Carver et al. 1989, Soderstrom et al. 2000). Generally, researchers distinguish between two broad types of coping strategy: approach/engagement-oriented strategies (involving active attempts to confront and resolve the problem) and avoidance/disengagement strategies (reducing the associated emotional distress or evading the problem) (Tobin et al. 1989, Klag and Bradley 2004). Some study findings indicate that engaging or approaching problems is more beneficial and will prevent burnout as opposed to avoiding or disengaging from the problem (Ceslowitz 1989, Chang et al. 2006). Nevertheless, Lazarus (1993) suggested that there are no universally good or bad coping processes, merely those that might often be better or worse than others in a particular individual. Indeed, it has been suggested that individuals use both disengagement and engagement strategies to deal with shift work-related problems, regardless of shift schedule or job type (Spelten et al. 1999). Since coping is a dynamic process, the strategies employed may also evolve with time and experience. For example, Spelten et al. (1999) found that, regardless of the shift schedule, shift-working nurses with inflexible sleeping habits tended to avoid or disengage from the problems whilst permanent night-working nurses utilised both engagement and disengagement strategies when dealing with sleep and social/family disturbances. It should be noted that the vast majority of participants were female; coping is thought to show gender differences (Tamres et al. 2002).
Shift workers may become desynchronised from their family’s habits and routines and, therefore, become dissatisfied with the amount of time spent with them. It is feasible that participation in leisure-time physical activity (LTPA) may not only have stress-reducing effects but also increase time spent with the family if leisure activities can be pursued as a group (Beermann and Nachreiner 1995, Presser 2000, Nomaguchi and Bianchi 2004). Mechanisms for the stress-reducing effects of physical activity may involve increases in self-esteem, self-efficacy and energy (Wijndaele et al. 2007). These states might evoke feelings of competence, through which individuals may be able to appraise or perceive a stressor as less harmful or threatening. An increase in self-efficacy, energy levels and social support through increased LTPA and, therefore, a decrease in stress and an increase in the ability to cope would seem to be beneficial to shift workers in theory. Yet, no previous research work has established that the degree of shift-work coping is even related to participation in physical activity.
2. Method
2.1. Participants
From a sampling frame of approximately 200, 95 participants (24 females and 71 males) volunteered to complete a modified version of the Standard Shift-work Index (SSI), together with the LTPA questionnaire validated by Lamb and Brodie (1990). Some characteristics of the sample are shown in Table 1.
Table 1.
Characteristics of shift-workers studied
| Characteristics | |
|---|---|
| Number studied | 95 |
| Number of females | 24 |
| Number of males | 71 |
| Mean (SD) Age | 37.2 (8.9) years |
| Age range | 22–59 years |
| Mean (SD) Experience working shift patterns | 120.62 (103.66) months |
| Mean height (SD) | 1.75 (0.08) m |
| Mean female height (SD) | 1.68 (0.07) m |
| Mean male height (SD) | 1.78 (0.003) m |
| Mean weight (SD) | 81.0 (11.29) kg |
| Mean female weight (SD) | 73.74 (13.30) kg |
| Mean male weight (SD) | 79.78 (1.087) kg |
| Mean BMI (SD) | 26.2 (3.42)% |
| Mean female BMI (SD) | 25.84 (3.87)% |
| Mean male BMI (SD) | 26.27 (3.21)% |
| Shift rotation (direction and speed) | Forward/Backward, Fast/Slow, All incorporated a period of nights |
| Marital status | |
| Married/Living with partner | 76% |
| Single | 14% |
| Divorced | 10% |
| Percentage of participants with dependants | 40.85% (1–3 dependants age range 0–70 + years) |
| Marital status of those with dependants: | |
| Married/Living with partner | 39.85% |
| Single parent | 1% |
| Job type/title and number of participants: | |
| Police Service | Group 1–22 |
| Firefighters/Watch managers/Control operators/Station officer | Group 2–66 |
| Bus drivers/Bus engineers | Group 3–6 |
| Flight attendant | Group 4–1 |
2.2. Research design
Copies of an adapted version of the SSI were distributed by the research team to the various organisations that participated in the study, along with pre-paid envelopes in which the SSIs were to be returned to the research team. This distribution process ensured that participants were allowed enough time to complete the questionnaire as well as maintaining anonymity. The SSI represents a well-established and validated (Barton et al. 1990) battery of questions that have been used frequently on shift workers to measure perceived problems and issues. The SSI covers items referring to: biographical and demographic information; chronotype; major difficulties caused by working shifts (adaptation to shift work, fitness to undertake job content, social life, fatigue, daytime sleepiness, shift system advantages, psychological well-being) and problems associated with each shift (sleep disturbance, alertness on the job, workload and items specific to the night-shift); health and well-being; the ability to cope with night work (Takahashi et al. 2005). Likert scales are used throughout the SSI.
To date, the SSI has not included sections designated to explore diet and physical activity during leisure time. Therefore, a LTPA questionnaire was added to the SSI. The LTPA questionnaire was an adapted version of Lamb and Brodie’s (1990) LTPA questionnaire, which allows recording of physical activities that are participated in during leisure time over a 14-d period. The LTPA questionnaire was complemented with additional questions regarding time spent watching television, transportation, adherence to exercise regimens, availability/accessibility to exercise facilities and barriers to participating in LTPA. Whilst combining the LTPA questionnaire with the social and domestic component of the SSI helped shorten the questionnaire, it was felt that, at 40 pages, the questionnaire was too long to expect a reasonable response rate. Therefore, modified versions of specific sections in the original SSI were used. The original Composite Morning Questionnaire (CS) within the SSI was changed for the validated shortened version of the Preference Scale Questionnaire (PS). Diaz-Morales and Sanchez-Lopez (2004) found that the relationship between the CS and the PS is high (r = 0.76), which indicates adequate convergent validity. Smith et al. (2002) suggested that whilst both CS and PS are quite adequate psychometrically, the PS is preferable as it is simpler to use and is not influenced by the respondent’s sleep-wake schedule.
2.3. Data analysis
According to previous research on factors that influence shift-work tolerance, the most important predictors were delimited to be age, time spent in shift work (experience), gender, marital status and the overall shift work engagement and disengagement coping scores. These were entered into an initial exploratory step-wise multiple regression model, with leisure-time energy expenditure over a 14-d period entered as the dependent (outcome) variable. Following this initial analysis, a second exploratory step-wise multiple regression model was implemented to consider the predictive value of the various subscales for individual coping indices. There were four individual subscales of coping mechanisms related to social, domestic, sleep and work-dependent problems, which were entered into the step-wise multiple regression model, with leisure-time energy expenditure over a 14-d period entered as the dependent variable.
3. Results
The distribution of the outcome variable of energy expenditure in leisure-time was found to be slightly skewed. Therefore, these data were analysed before and after logarithmic transformation. Results of the multivariate regression analyses did not differ substantially between logged and non-logged data. Therefore, the beta coefficients and associated p-values presented below are for the non-logged data.
Time spent in shift work (β = 26.36 kJ/week, p = 0.051; Figure 1) and gender (β = 7168.9 kJ/week, p = 0.023; Figure 2) were found to be predictors of leisure-time energy expenditure, with the most experienced male shift workers expending the most energy during leisure-time activities. The overall ‘disengagement’ coping score (the overall score is the sum of all four subscales related to sleep, domestic life, work performance and social life) was found to be a positive predictor of leisure-time energy expenditure (β = 956.27 kJ/week, p = 0.054; Figure 3); whilst there was no relationship between physical activity and overall ‘engagement’ coping scores (p = 0.756).
Figure 1.
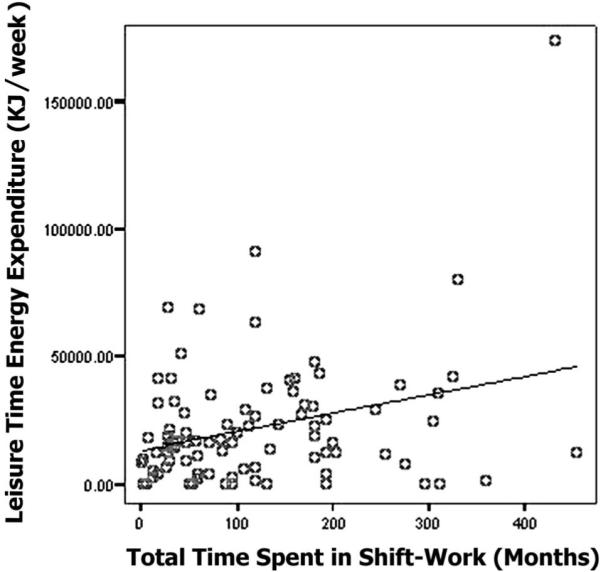
Relationship between energy expenditure (kJ/week) and time spent in shift work. Data are total energy expenditure for 14 d (kJ/week), with time spent in shift work being total number of months an individual had spent in shift work. This relationship remained when the outlier was not included in the analysis.
Figure 2.
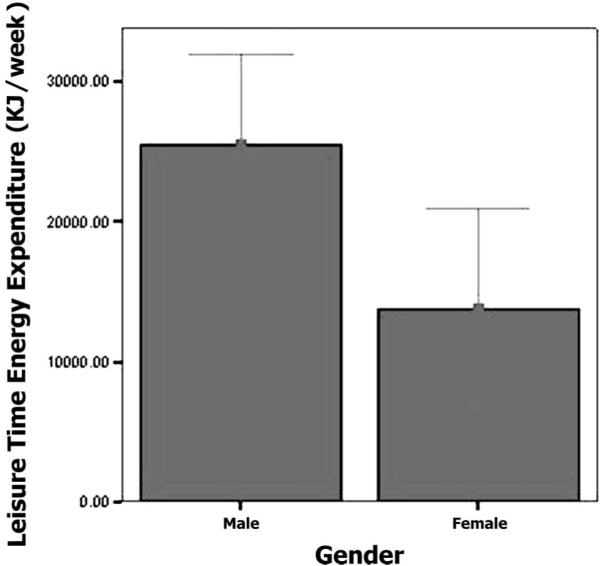
Relationship between energy expenditure and gender. Data are mean ± SE.
Figure 3.
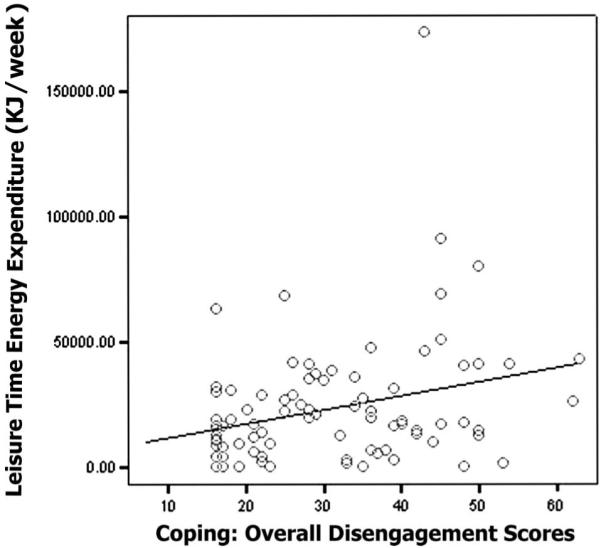
Relationship between energy expenditure (kJ/week) and overall coping disengagement scores. Data are total energy expenditure for 14 d (kJ/week) with coping disengagement scores being individual total scores from the four subscales of the Standard Shift-work Index. This relationship remained when the outlier was not included in the analysis.
In males, the individual disengagement subscale of sleep disturbances (β = −1078.1 kJ/week, p = 0.086) was found to be negatively correlated to energy expenditure, whereas disengagement of domestic-related disturbances was found to be positively related to leisure-time energy expenditure (β = 1961.92 kJ/week, p = 0.001). Nevertheless, the r-squared statistic for both these predictors in combination was quite low (14%). These disengagement indices were not found to relate to the energy expenditure of female shift workers (p = 0.762).
4. Discussion
These data suggest that experienced male shift workers participate in the most LTPA. Some indices related to an individuals’ coping strategy were also found to correlate with leisure-time energy expenditure; the male shift workers with higher levels of physical activity in leisure-time ‘disengaged’ more from their domestic-related problems, but less from their sleep-related problems. These findings have important implications for the design of physical activity interventions, especially in targeting the least active shift workers who cope less well with certain stressors related to working at unusual hours.
The most experienced shift workers were found to participate in more LTPA. Obviously, an individual’s experience of shift work will increase with age (Baker et al. 2004). Whilst a number of researchers have suggested that older shift workers have more pronounced difficulties and health issues in comparison with younger shift workers (Harma 1996, Nachreiner 1998, Furnham and Hughes 1999, Seo et al. 2000, Pati et al. 2001, Baker et al. 2004, Rouch et al. 2005), an alternative view is that time spent doing shift work could be a moderating factor and promote adaptation (Oginska et al. 1993, Bohle and Tiley 1989, Baker et al. 2004, Bonnefond et al. 2006). Rutenfranz et al. (1985) suggested that a number of phases are lived through if an individual remains in shift work. The first 1–5 years of shift work (the first phase) comprise an adaptation phase, whereby workers attempt to adapt and adjust to new working schedules and to deal with social, family, domestic and leisure activities and obligations. Kundi et al. (1979) indicated that the first 5 years of shift work also have the strongest effect on subjective health and well-being, highlighting the process of self-selection, which can also hamper interpretation of study findings. That is, those with a greater tolerance and ability to cope with shift work opt to stay on a shift schedule but those who are unable to tolerate or cope with shift work leave. Therefore, those individuals who continue to work a shift schedule (i.e. who have a greater experience of working shifts) have been able to adapt their lifestyles; they accept the various forms of disruption and desynchronisation associated with shift work as opposed to ‘newcomers’, who must go through the adaptive process and find suitable strategies to help them tolerate and cope with shift work. Shift workers have been shown to value time similarly to day workers (Herbert 1983, Hornberger and Knauth 1993, Knutsson 2003, Baker et al. 2004, Lipovcan et al. 2004); therefore, their attempts and ability to adhere to societal norms and diurnal activities such as LTPA may influence the amount of work and life satisfaction they experience. Since the more experienced shift worker is thought to have adapted to a ‘non-diurnal’ existence, and deals better with the problems associated with ‘free/spare’ time and time/activity/obligation management in comparison with a less experienced worker, his/her ability to participate in LTPA and to schedule it may be somewhat easier. Therefore, promotion of an active lifestyle may be particularly important within the first 5 years of a shift worker’s career.
Higher levels of LTPA were found to be associated with a disengagement style of coping strategy. It is clear that the very nature of shift work requires individuals to have a dynamic and flexible adaptation/coping process, which allows for the variable circumstances that a rotating shift system brings. Such coping could be related to the relatively new personality construct associated with shift-work tolerance - ‘hardiness’. Hardiness has been described as an amalgamation of attitudes that enhance health and mood despite stressful circumstances (Maddi et al. 2006). This attitude construct consists of commitment, control and challenge. Since the shift worker often lacks ‘control’ over his/her shift pattern, both commitment and challenge would seem to be the primary factors influencing shift workers’ hardiness and therefore the ability to cope with shift systems. Challenge may refer to the requirements of the job and these might contribute to a shift worker’s tolerance to shift work due to shifts being part of the job they enjoy. Commitment is highly individualised, especially in relation to shift work. However, this commitment could relate to issues such as higher rates of pay and the fact that shift work might allow for second jobs. Workers who are ‘hardy’ may in fact be able to adapt more favourably to shift work, allowing for domestic, social and leisure time activities, such as physical activity, to be scheduled within their day. This begs the question as to whether experienced shift workers are better able to adapt and therefore more able to schedule activities such as physical activity into their time; ‘hardier’ shift workers are better able to cope with shift work, due to their commitment to their work schedule (for whatever reason) and, therefore, more willing/able to schedule physical activity within their day; or experienced shift workers exhibit both ‘hardiness’ and ‘adaptive’ coping strategies, so allowing for participation in leisure activities and the fulfilment of social and domestic tasks. Such theories and questions are relatively new and require further research but may be a useful tool in understanding the differences between those who can and cannot tolerate or cope with shift schedules (Wedderburn and Scholarios 1993, Harma, 1996, Nachreiner 1998, Maddi et al. 2006).
Females were found to be less active than males. Gender has been found to influence the ability to cope with the pressures of shift work, with women showing more signs and symptoms of intolerance than men, until the age of about 50 years (Oginska et al. 1993, Spelten et al. 1993, Nachreiner 1998, Winwood et al. 2006). The divergence in coping with shift schedules can be attributed mainly to social rather than biological factors. The roles and activities that female workers engage in tend to differ from those of their male counterparts. Female shift workers generally engage more in domestic and household obligations.
Furthermore, those with children or dependents experience an increase in such obligations and often feel as though they work a ‘double-shift’ (working their shift at work and coming home to fulfil domestic duties). Female shift workers often cite ‘a lack of time’ or their ‘shift system’ as a factor affecting their participation in LTPA. There could also be gender differences in the quality of leisure-time activity as well as the quantity. Males are less likely to combine their leisure-time activities with other activities such as housework or childcare or time spent with family and friends. All of these variables are affected by working shift schedules and so this increases the likelihood of female workers having to combine their ‘spare/leisure’ time with domestic and social obligations. Clearly, this influences female shift workers’ participation in LTPA (Bird and Fremont 1991, Nomaguchi and Bianchi 2004, Baker et al. 2004, Demerouti et al. 2004, Lipovcan et al. 2004, Karlsen et al. 2006). The combination of effects of gender and experience clearly highlights some key areas that require further study, particularly with regard to why more experienced male shift workers appear to be able to expend more energy in LTPA.
In support of the above points, male shift workers with higher levels of LTPA ‘disengaged’ more from their domestic-related problems, but less from their sleep-related problems, in comparison with their female counterparts. Coping mechanisms are, at best, complex with no definitive ‘right’ or ‘wrong’ strategy as to which shift workers should employ. There may well be more advantageous general methods of coping, ones that are often cited as more favourable than others for those working shifts. However, the effects of shift schedules on workers are individual in nature; therefore, the coping strategy employed must be individually chosen by the person concerned. Moreover, the transient nature of coping strategies must be appreciated, i.e. as people grow and evolve, or as the situation changes, the coping strategy also will evolve to meet the varying needs of the individuals and their environment (Lazarus 1993). Many perceive disengagement or avoidance as a negative form of coping with regard to shift work, with some studies suggesting that increased use of disengagement strategies by the shift worker actually increased the number of problems experienced (Spelten et al. 1993). However, the results of the present study, in conjunction with previous research, have highlighted the need to employ a mixed copying strategy. This will allow an individual to construct a method that matched the changing difficulties of shift work and the shift worker. This study suggests that males who expend more energy through LTPA tend to disengage more from domestic problems. It appears plausible to suggest that physical activity is used by male shift workers as a strategy to disengage from domestic issues or problems.
Avoidance/disengagement has often been cited as a more favourable coping strategy than approach/engagement in situations that cannot be controlled by the individual (Roth and Cohen 1986, Lazarus 1993, Spelten et al. 1999, Karlsen et al. 2006, Winwood et al. 2006). For example, a shift worker’s ability to control for domestic problems is somewhat hampered by the shift system and the ‘non-diurnal’ lifestyle. Since the shift system is to a certain extent ‘out’ of their control, it is reasonable to assume that approach/engagement strategies (trying to change or solve the problem) are not feasible (unless a worker chooses to change his/her job). Therefore, avoidance/disengagement strategies (avoiding/distancing from/escaping from the problems) may be the only workable option. Clearly, it is possible that male shift workers in this study used LTPA as a tool to distance themselves from domestic issues that they were unable to influence due to the shift work. Conversely, the same male shift workers disengaged far less from their sleep problems. Sleep and sleep hygiene may be issues that can be controlled more by the individual. Whilst there is little a shift worker can do to prevent sleep at undesirable times of the day (as this is dictated by the shift roster), there are certain activities and routines that can aid sleep. However, the male shift workers appeared to use instead a more engaging strategy via the medium of LTPA. Whilst such a statement is highly presumptuous, it is reasonable after all that those male shift workers utilised other disengaging strategies and mechanisms or indeed used a combination of engaging and disengaging strategies in an attempt to deal with issues surrounding sleep. Nonetheless, physical activity has been linked with increased sleep quality, but the links between physical activity, sleep and shift work are unclear and further investigation is needed. It is also plausible that male shift workers may have been more aware of the links between physical activity and sleep in general and therefore more inclined to participate in greater levels of LTPA in comparison to females.
The question remains as to whether being more physically active allows a shift worker to cope better with shift patterns or whether coping better with shift patterns allows more time for a worker to participate in physical activity. It is feasible that LTPA, whether it be used as an engaging or disengaging strategy, is a tool that can be utilised to increase a shift workers’ tolerance and therefore their ability to cope with unusual working hours (Roth and Cohen 1986, Lazarus 1993, Spelten et al. 1993, 1999, Karlsen et al. 2006, Winwood et al. 2006. This view is in agreement with previous research conducted by Winwood et al. (2007) and Eriksen and Bruusgaard (2003), who reported that individuals with more active leisure pursuits reported significantly better sleep, recovery between periods of work and were less likely to develop persistent fatigue. These authors attributed their findings to the down-regulation of stress-induced brain arousal and stimulation of the pleasure-reward brain neurophysiology associated with physical leisure-time activities (Eriksen and Bruusgaard 2003, Winwood et al. 2007). To allow for a thorough exploration of coping mechanism, shift work and physical activity, it would appear that a new more extensive measurement tool needs to be designed. The present authors recommend that physical activity interventions for shift workers should be designed with careful consideration of individual domestic responsibilities and perceived disruption to sleep.
References
- Baker A, et al. Shift-work experience and the value of time. Ergonomics. 2004;47(3):307–317. doi: 10.1080/0014013032000157896. [DOI] [PubMed] [Google Scholar]
- Barton J, et al. Standard Shift-work Index Manual. Social and Applied Psychology Unit, Department of Psychology, University of Sheffield; 1990. SAPU Memo No: 1159 MRC/ESRC. [Google Scholar]
- Beermann B, Nachreiner F. Working shifts - different effects for women and men? Work and Stress. 1995;9(2–3):289–297. [Google Scholar]
- Bird CE, Fremont AM. Gender, time use, and health. Journal of Health and Social Behaviour. 1991;32(2):114–129. [PubMed] [Google Scholar]
- Bohle P, Tiley A. The impact of night work on psychological well-being. Ergonomics. 1989;32(9):1089–1099. doi: 10.1080/00140138908966876. [DOI] [PubMed] [Google Scholar]
- Bonnefond A, et al. Interaction of age with shift-related sleep-wakefulness, sleepiness, performance, and social life. Experimental Aging Research. 2006;32(2):185–208. doi: 10.1080/03610730600553968. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology. 1989;56(2):267–283. doi: 10.1037//0022-3514.56.2.267. [DOI] [PubMed] [Google Scholar]
- Ceslowitz S. Burnout and coping strategies among hospital staff nurses. Journal of Advanced Nursing. 1989;14(7):553–558. doi: 10.1111/j.1365-2648.1989.tb01590.x. [DOI] [PubMed] [Google Scholar]
- Chang EM, et al. The relationships among workplace stressors, coping methods, demographic characteristics, and health in Australian nurses. Journal of Professional Nursing. 2006;22(1):30–38. doi: 10.1016/j.profnurs.2005.12.002. [DOI] [PubMed] [Google Scholar]
- Costa G. Shift-work and occupational medicine: an overview. Occupational Medicine - Oxford. 2003;53(2):83–88. doi: 10.1093/occmed/kqg045. [DOI] [PubMed] [Google Scholar]
- Costa G. Multidimensional aspects related to shift-workers health and well being. Rev Saude Publica. 2004;38(Supplement):86–91. doi: 10.1590/s0034-89102004000700013. [DOI] [PubMed] [Google Scholar]
- Demerouti E, et al. The impact of shift-work on work-home conflict, job attitudes and health. Ergonomics. 2004;47(9):987–1002. doi: 10.1080/00140130410001670408. [DOI] [PubMed] [Google Scholar]
- Diaz-Morales J, Sanchez-Lopez M. Composite and preference scales of mornings and reliability and factor invariance in an adult university sample. Spanish Journal of Psychology. 2004;7(2):93–100. doi: 10.1017/s1138741600004790. [DOI] [PubMed] [Google Scholar]
- Di Lorenzo L, et al. Effect of shift-work on body mass index: results of a study performed in 319 glucose-tolerant men working in a Southern Italian industry. International Journal of Obesity. 2003;27(11):1353–1358. doi: 10.1038/sj.ijo.0802419. [DOI] [PubMed] [Google Scholar]
- Eriksen W, Bruusgaard D. Do physical leisure time activities prevent fatigue? A 15 month prospective study of nurses’ aides. British Journal of Sports Medicine. 2003;38(4):331–336. doi: 10.1136/bjsm.2002.004390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furnham A, Hughes K. Individual difference correlates of night work and shift-work rotation. Personality and Individual Differences. 1999;26(5):941–959. [Google Scholar]
- Härmä M. Ageing, physical fitness and shift-work tolerance. Applied Ergonomics. 1996;27(1):25–29. doi: 10.1016/0003-6870(95)00046-1. [DOI] [PubMed] [Google Scholar]
- Harma MI, et al. Physical training intervention in shift-workers. 1. The effects of intervention on fitness, fatigue, sleep, and psychomotor symptoms. Ergonomics. 1988a;31(1):39–50. doi: 10.1080/00140138808966647. [DOI] [PubMed] [Google Scholar]
- Harma MI, et al. Physical-training intervention in female shift-workers. 2. The effects of intervention on the circadian-rhythms of alertness, short-term-memory, and body-temperature. Ergonomics. 1988b;31(1):51–63. doi: 10.1080/00140138808966648. [DOI] [PubMed] [Google Scholar]
- Harrington JM. Health effects of shift-work and extended hours of work. Occupational and Environmental Medicine. 2001;58(1):68–72. [Google Scholar]
- Herbert A. The influence of shift-work on leisure activities. A study with repeated measurement. Ergonomics. 1983;26(6):565–574. doi: 10.1080/00140138308963375. [DOI] [PubMed] [Google Scholar]
- Hornberger S, Knauth P. Interindividual differences in the subjective valuation of leisure time utility. Ergonomics. 1993;36(3):255–264. [Google Scholar]
- Karlsen E, Dybdahl R, Vitterso J. The possible benefits of difficulty: How stress can increase and decrease subjective well-being. Scandinavian Journal of Psychology. 2006;47(5):411–417. doi: 10.1111/j.1467-9450.2006.00549.x. [DOI] [PubMed] [Google Scholar]
- Karlsson B, Knutsson A, Lindahl B. Is there an association between shift-work and having a metabolic syndrome? Results from a population based study of 27,485 people. Journal of Occupation and Environmental Medicine. 2001;58(11):747–752. doi: 10.1136/oem.58.11.747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klag S, Bradley G. The role of hardiness in stress and illness: An exploration of the negative affectivity and gender. British Journal of Health Psychology. 2004;9(2):137–161. doi: 10.1348/135910704773891014. [DOI] [PubMed] [Google Scholar]
- Knutsson A. Health disorders of shift-workers. Occupational Medicine. 2003;53(2):103–108. doi: 10.1093/occmed/kqg048. [DOI] [PubMed] [Google Scholar]
- Knutsson A. Methodological aspects of shift-work research. Chronobiology International. 2004;21(6):1037–1047. doi: 10.1081/cbi-200038525. [DOI] [PubMed] [Google Scholar]
- Kundi M, et al. Consequences of shiftwork as a function of age and years on shift. Chronobiologia. 1979;6(2):123. [Google Scholar]
- Lamb KL, Brodie DA. The assessment of physical activity by leisure-time physical activity questionnaires. Sports Medicine. 1990;10(3):159–180. doi: 10.2165/00007256-199010030-00003. [DOI] [PubMed] [Google Scholar]
- Lasfargues G, et al. Relations among night work, dietary habits, biological measures, and health status. International Journal of Behavioural Medicine. 1996;3(2):123–134. doi: 10.1207/s15327558ijbm0302_3. [DOI] [PubMed] [Google Scholar]
- Lazarus RS. Coping theory & research: past, present, and future. Psychosomatic Medicine. 1993;55(3):234–247. doi: 10.1097/00006842-199305000-00002. [DOI] [PubMed] [Google Scholar]
- Lipovcan K, Larsen P, Zganec P. Quality of life, life satisfaction and happiness in shift and non-shift-workers. Revista De Saude Publica. 2004;38(1):3–10. doi: 10.1590/s0034-89102004000700002. [DOI] [PubMed] [Google Scholar]
- McEwen BS. Sleep deprivation as a neurobiologic and physiologic stressor: allostasis and allostatic load. Metabolism Clinical and Experimental. 2007;55(suppl. 2):S20–S23. doi: 10.1016/j.metabol.2006.07.008. [DOI] [PubMed] [Google Scholar]
- Maddi SR, et al. The personality construct of hardiness, III: Relationships with repression, innovativeness, authoritarianism, and performance. Journal of Personality. 2006;72(2):575–598. doi: 10.1111/j.1467-6494.2006.00385.x. [DOI] [PubMed] [Google Scholar]
- Monk TH, Folkard S. Making shift-work tolerable. Taylor and Francis; Basingstoke: 1992. [Google Scholar]
- Nachreiner F. Individual and social determinants of shift-work tolerance. Scandinavian Journal of Work and Environmental Health. 1998;24(3):35–42. [PubMed] [Google Scholar]
- Nomaguchi KM, Bianchi SM. Exercise time: Gender differences in the effects of marriage, parenthood, and employment. Journal of Marriage and Family. 2004;66(2):413–429. [Google Scholar]
- Oginska H, Pokorski J, Oginski A. Gender, aging and shift-work intolerance. Ergonomics. 1993;36(1–3):161–168. doi: 10.1080/00140139308967868. [DOI] [PubMed] [Google Scholar]
- Pati AK, Chandrawanshi A, Reinberg A. Shift-work: consequences and management. Current Science. 2001;81(1):32–52. [Google Scholar]
- Presser HB. Nonstandard work schedules and marital instability. Journal of Marriage and Family. 2000;62(1):93–110. [Google Scholar]
- Rajaratnam SMW, Arendt J. Health in a 24-hr society. Lancet. 2001;358(9286):999–1005. doi: 10.1016/S0140-6736(01)06108-6. [DOI] [PubMed] [Google Scholar]
- Roth S, Cohen LJ. Approach, avoidance, and coping with stress. American Psychologist. 1986;41(7):813–819. doi: 10.1037//0003-066x.41.7.813. [DOI] [PubMed] [Google Scholar]
- Rouch I, et al. Shift-work experience, age and cognitive performance. Ergonomics. 2005;48(10):1282–1293. doi: 10.1080/00140130500241670. [DOI] [PubMed] [Google Scholar]
- Rutenfranz J, Haider M, Koller M. Occupational health measures for night workers and shiftworkers. In: Folkard S, Monk T, editors. Hours of work: Temporal factors in work scheduling. Wiley; New York: 1985. [Google Scholar]
- Seo YJ, et al. The relationship between sleep and shift system, age and chronotype in shift-workers. Biological Rhythm Research. 2000;31(5):559–579. [Google Scholar]
- Smith CS, et al. Investigation of morning-evening orientation in six countries using the preferences scale. Personality and Individual Differences. 2002;32:949–968. [Google Scholar]
- Soderstrom M, et al. The relationship of hardiness, coping strategies, and perceived stress to symptoms of illness. Journal of Behavioural Medicine. 2000;23(3):311–327. doi: 10.1023/a:1005514310142. [DOI] [PubMed] [Google Scholar]
- Spelten E, et al. The relationship between coping strategies and GH scores in nurses. Ergonomics. 1993;36(1–3):227–232. doi: 10.1080/00140139308967876. [DOI] [PubMed] [Google Scholar]
- Spelten E, Totterdell P, Costa G. A process model of shiftwork and health. Journal of Occupational Health Psychology. 1999;4(3):207–218. doi: 10.1037//1076-8998.4.3.207. [DOI] [PubMed] [Google Scholar]
- Takahashi M, et al. Modifying effects of perceived adaptation to shift work on health, wellbeing, and alertness on the job among nuclear power plant operators. Industrial Health. 2005;43(1):171–178. doi: 10.2486/indhealth.43.171. [DOI] [PubMed] [Google Scholar]
- Tamres LK, Janicki D, Helgeson VS. Sex differences in coping behaviour: A meta-analytic review and an examination of relative coping. Personality and Social Psychology Review. 2002;6(1):2–30. [Google Scholar]
- Taylor E, Briner RB, Folkard S. Models of shift-work and health: An examination of the influence of stress on shift-work theory. Human Factors. 1997;39(1):67–82. doi: 10.1518/001872097778940713. [DOI] [PubMed] [Google Scholar]
- Tobin DL, et al. The hierarchical factor structure of the coping strategies inventory. Cognitive Therapy and Research. 1989;13(4):343–361. [Google Scholar]
- Waterhouse J, Folkard S, Minors D. Shift-work, health and safety. An overview of the scientific literature 1978–1990. HMSO; London: 1992. HSE contract research report. [Google Scholar]
- Wedderburn A, Scholarios D. Guidelines for shift-workers: trials and errors? Ergonomics. 1993;36(3):211–218. [Google Scholar]
- Wijndaele K, et al. Association between leisure time physical activity and stress, social support and coping: A cluster-analytical approach. Psychology of Sport and Exercise. 2007;8(4):425–440. [Google Scholar]
- Winwood CP, Bakker AB, Winefield AH. An investigation of the role of non-work-time behavior in buffering the effects of work strain. Journal of Occupational and Environmental Medicine. 2007;49(8):862–871. doi: 10.1097/JOM.0b013e318124a8dc. [DOI] [PubMed] [Google Scholar]
- Winwood PC, Winefield AH, Lushington K. Work-related fatigue and recovery: the contribution of age, domestic responsibilities and shift-work. Journal of Advanced Nursing. 2006;56(4):438–449. doi: 10.1111/j.1365-2648.2006.04011.x. [DOI] [PubMed] [Google Scholar]