

Abstract
Introduction
Hypovolemia and hypovolemic shock are life-threatening conditions that occur in numerous clinical scenarios. Near-infrared spectroscopy (NIRS) has been widely explored, successfully and unsuccessfully, in an attempt to use it as an early detector of hypovolemia by measuring tissue oxygen saturation (StO2). In order to investigate the measurement site dependence and probe dependence of NIRS in response to hemodynamic changes, such as hypovolemia, we applied a simple cardiovascular challenge: a posture change from supine to upright, causing a decrease in stroke volume (as in hypovolemia) and a heart rate increase in combination with peripheral vasoconstriction to maintain adequate blood pressure.
Methods
Multi-depth NIRS was used in nine healthy volunteers to assess changes in StO2 in the thenar and forearm in response to the hemodynamic changes associated with a posture change from supine to upright.
Results
A posture change from supine to upright resulted in a significant increase (P < 0.001) in heart rate. Thenar StO2 did not respond to the hemodynamic changes following the posture change, whereas forearm StO2 did. Forearm StO2 was significantly lower (P < 0.001) in the upright position compared to supine for all probing depths.
Conclusions
The primary findings in this study were that forearm StO2 is a more sensitive parameter to hemodynamic changes than thenar StO2 and that the depth at which StO2 is measured is of minor influence. Our data support the use of forearm StO2 as a sensitive parameter for the detection of central hypovolemia and hypovolemic shock in (trauma) patients.
Introduction
Hypovolemia and hypovolemic shock are life-threatening conditions that occur in numerous clinical scenarios such as in the emergency room, during surgery, and in intensive care patients [1-4]. Compensatory mechanisms that protect against alterations in blood pressure make standard hemodynamic measurements poor indicators for early assessment of hypovolemia and shock. One of these compensatory mechanisms is extreme peripheral vasoconstriction, and therefore measurement of alterations in the peripheral circulation could aid in the early detection of hypovolemia.
To this end, near-infrared spectroscopy (NIRS) - an optical technique for measuring tissue oxygen saturation - has been widely explored, successfully and unsuccessfully, in attempts to identify the severity of hypovolemia [5-8], to monitor blood loss [9-11] and guide resuscitation [12-14], and to predict patient outcome [15-17]. The main problem with the interpretation of tissue oxygen saturation (StO2) data from these studies, however, is the diversity of methodologies used for assessing StO2. Two major aspects regarding the inconsistent methodology are the application site and the probing depth. The application site is important because differences may exist in the sensitivity of underlying muscle groups and other anatomical structures to cardiovascular challenges such as central hypovolemia. The probing depth, additionally, determines the relative contribution of muscular and (sub)dermal tissue to the StO2 measurement.
Although it is often discussed that these aspects affect the assessment of StO2, no studies have simultaneously measured StO2 in the thenar and forearm at multiple depths. In order to investigate the actual measurement site dependence and probe dependence of NIRS in response to hemodynamic changes, such as hypovolemia, we applied a simple cardiovascular challenge: a posture change from supine to upright, causing a decrease in stroke volume (as in hypovolemia) and a heart rate increase in combination with peripheral vasoconstriction to maintain adequate blood pressure [18-22]. Multi-depth NIRS was used to assess changes in StO2 in the thenar and forearm in response to the hemodynamic changes associated with the described cardiovascular challenge.
Materials and methods
Subjects
The study protocol was approved by the Medical Ethics Committee of University College London. Nine healthy, normotensive volunteers who were not receiving any vaso-active medication were requested to refrain from consuming caffeine-containing beverages prior to the measurements. The room temperature was maintained at 20 ± 1°C.
Hemodynamic monitoring
Prior to the experimental protocol, systolic and diastolic blood pressures were measured in the supine position using an automatic blood pressure cuff around the upper arm (type M5-I, Omron Matsusaka Co. Ltd, Japan). The heart rate was continuously monitored during the entire experimental protocol, using a fingertip pulse oximeter (Defibron, Groningen, the Netherlands).
Near-infrared spectroscopy
StO2 was non-invasively and simultaneously measured in the thenar and forearm by applying one multi-depth NIRS probe on the skin of the thenar eminence and one multi-depth NIRS probe on the lateral side of the anterior surface of the forearm brachioradialis muscle, both placed in parallel to the orientation of the respective target muscle groups (Hutchinson Technology, Hutchinson, MN, USA). The NIRS devices employ reflectance mode probes that have one 1.5 mm optical fiber to illuminate the tissue and two optical fibers to detect the backscattered light from the tissue. The spatial separation between the illumination fiber and the two detection fibers is 15 mm and 25 mm, respectively. As described by Cui and colleagues, the NIRS measurement depth increases with increasing distance between the illuminating and detecting fibers [23]. The 25 mm separated fiber therefore measures a greater and deeper tissue volume than the 15 mm separated fiber. By subtracting the spectral absorbance measured by the 15 mm fiber from that measured by the 25 mm fiber, similar to the NIRS device used by the group of Torella and colleagues [9,10], the spectral absorbance between these two probing depths was determined and used to calculate StO2 in this isolated layer of tissue.
The relative optical attenuation of the backscattered light at four wavelengths (680 nm, 720 nm, 760 nm, and 800 nm) was measured for each probing depth to calculate two second-derivative attenuation values, one centered at 720 nm and the other at 760 nm [24]. A ratio of the 720 nm to 760 nm second-derivative values is directly related to StO2, defined as [HbO2]/([Hb] + [HbO2]), via a calibration table that is permanently stored within the device [25].
Experimental protocol
Subjects started the experiment in a supine position. After stable baseline traces were obtained for the heart rate and NIRS measurements, the subjects changed posture to an upright position. Fifteen minutes later, the subjects changed posture back to supine. The heart rate and StO2 data were obtained during the supine position, then upright for 5 and 15 minutes, and again in the supine position. The hand and forearm were kept at heart level during the entire experimental protocol using a sling.
Statistical analysis
Statistical analysis was performed in GraphPad Prism software (GraphPad Software, San Diego, CA, USA). Normal distribution of the data was confirmed for each StO2 parameter (15 mm, 25 mm, and 25 - 15 mm) using the D'Agostino and Pearson omnibus normality test. Comparative analysis between groups was performed using analysis of variance (ANOVA) with a Bonferroni post-hoc test. All data are presented as the mean ± standard deviation. Differences between groups with P < 0.05 were considered statistically significant.
Results
Subject demographics
The subject population consisted of six females and three males (all Caucasian) with a mean ± standard deviation age of 39 ± 14 years, height of 171 ± 6 cm, and weight of 70 ± 8 kg. Systolic and diastolic blood pressures were 110 ± 8 and 69 ± 7 mmHg, respectively.
Heart rate and StO2
No differences in heart rate and StO2 values between the first and second supine time points (beginning and the end of the experimental protocol, respectively) and between the first and second upright time points (after 5 and 15 minutes upright, respectively) were observed. The data were therefore categorized into supine and upright.
Repeated-measures ANOVA showed that a posture change from supine to upright resulted in a significant increase in heart rate (Figure 1). Furthermore, thenar StO2 did not respond to the hemodynamic changes following the posture change (Figure 2, left), whereas forearm StO2 did (Figure 2, right). In the forearm, StO2 was significantly lower (P < 0.001) in the upright position with respect to the supine position. StO2 measured in the supine position was significantly higher in the thenar than in the forearm (P < 0.05 for the 15 mm and 25 mm probing depths and P < 0.001 for the 25 - 15 mm probing depth). In the forearm, the mean ± standard deviation change in StO2 was 7.1 ± 4.0 for 15 mm, 8.6 ± 4.5 for 25 mm, and 10.9 ± 6.0 for 25 - 15 mm probing depth, respectively.
Figure 1.
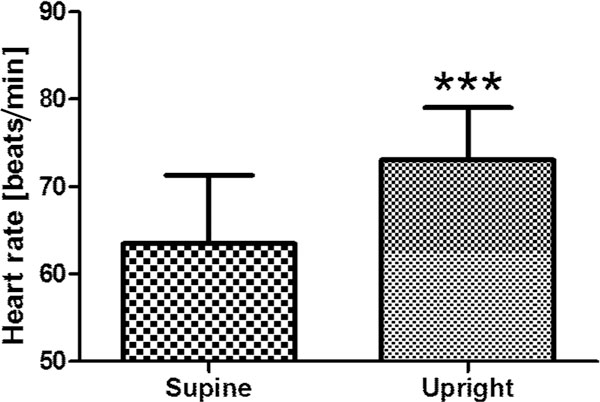
Heart rate in the supine and upright positions. ***P < 0.001 for upright versus supine position.
Figure 2.

Thenar and forearm tissue oxygen saturation using different probe spacings. Thenar tissue oxygen saturation (StO2) (left), and forearm StO2 (right) in the supine and upright positions as measured using different probe spacings. ***P < 0.001 for upright versus supine position. monitoring the effects of hemodynamic changes on peripheral tissue oxygenation.
Regular ANOVA (not repeated measures) revealed no significant differences between supine and upright positions for either the thenar or the forearm for all probing depths, indicating that the change in StO2 during the posture change from supine to upright (analyzed using repeated-measures ANOVA) is more important than the absolute StO2 values for monitoring the effects of hemodynamic changes on peripheral tissue oxygenation.
StO2 values in the thenar during both supine and upright positions were similar in females and males, but in the forearm StO2 values tended to be lower in females than in males (number too small for statistical analysis). The StO2 decrease caused by a posture change from supine to upright, however, was of a similar extent in females and males for both the thenar and the forearm for all probing depths.
Discussion and conclusion
The present study investigated the application site dependence and probing depth dependence of NIRS measurements for the detection of changes in StO2 following a simple cardiovascular challenge. The main findings were that forearm StO2 is a more sensitive parameter to hemodynamic changes than thenar StO2 and that the depth at which StO2 is measured is of minor influence. In addition, our data indicated that the change in StO2 during a cardiovascular challenge is more important than the absolute StO2 values for monitoring the effects of hemodynamic changes on peripheral tissue oxygenation.
In the present study, a simple cardiovascular challenge was created by a posture change from supine to upright. This challenge is associated with a decrease in stroke volume, an increase in heart rate, and an increase in peripheral vascular tone in order to maintain adequate blood pressure. Since we did not measure the stroke volume and cardiac output we could not assess the extent of this cardiovascular challenge further than its effect on the heart rate. The observed increases in heart rate, however, indicate that the applied posture change did induce significant alterations at the macrocirculatory level. This is supported by several studies investigating hemodynamic responses in healthy subjects undergoing passive upright tilt [18-22]. Furthermore, the focus of the present study was to investigate the capability of NIRS to detect alterations in StO2 following macrocirculatory changes and, especially, the role of NIRS application site and probing depth. This capability we have evidently shown.
We have shown that forearm StO2 is more responsive to hemodynamic changes than thenar StO2. This is surprising given that the employed NIRS device is promoted for use on the thenar and not the forearm. Many researchers using NIRS technology claim that the contribution of (sub)dermal tissue to the NIRS signal is deleterious for its interpretation, and many optical and algorithmic solutions are explored to minimize this effect. Indeed, the present study shows that the standard deviation in distribution of StO2 values obtained in the forearm is much larger compared with that in the thenar and, in addition, StO2 values in the forearm tended to be lower in females than in males. Both these observations could be attributed to interindividual variability in the contribution of subdermal adipose tissue to the NIRS signal. The variance in forearm StO2 appeared to be independent of probing depth, however, as the 15 mm, 25 mm, and 25 - 15 mm signals all provided very similar StO2 values. Furthermore, the StO2 change in response to the posture change was of similar extent for all probing depths. Taken together, these results suggest that the (micro)vascular response to a cardiovascular challenge might be similar in (sub)dermal tissue and in the muscle, and it is the forearm tissue as a whole that is more sensitive to hemodynamic changes compared to the thenar.
In a recent study by Soller and colleagues, where central hypovolemia was induced by lower body negative pressure (LBNP) [6], forearm StO2 was measured using a device developed by the authors (equipped with a 30 mm probe) and was shown to be a sensitive parameter to the stroke volume decrease associated with application of LBNP. The stroke volume and forearm StO2 decreased immediately at onset of simulated hypovolemia (LBNP = -15 mmHg), while the heart rate remained unresponsive until an LBNP of -45 mmHg and increased significantly at an LBNP of -60 mmHg. These data support our finding that forearm is a sensitive measure to detect alterations in StO2 cardiovascular autonomic tone associated with central hypovolemia.
In a subsequent LBNP study by the same group [7], thenar StO2 was measured with a device similar to the device used in the present study (HT device, 15 mm probe) and forearm StO2 was measured using the device developed by the authors (30 mm probe). The authors found that their device on the forearm was more sensitive to hypovolemia than the HT device on the thenar, and concluded that their device had superior sensitivity to detect acute hypovolemia. The authors furthermore hypothesize that the 15 mm probe spacing of the HT device is probably too small to collect light from a sufficiently deep layer of muscular tissue to detect hypovolemia and, additionally, it was suggested that the relatively large contribution of (sub)dermal tissue (due to the smaller probing depth) might affect the StO2 measurements. The present study, however, where thenar and forearm StO2 were measured at multiple depths simultaneously, clearly shows that forearm StO2 is a more sensitive parameter to detect changes in cardiovascular autonomic tone than thenar StO2 (both measured with the HT device), and that the sensitivity of these measurements was independent of probing depth.
Crookes and colleagues showed in a study in trauma patients that thenar StO2 could be used to identify severe hypovolemic shock, but that it was unable to detect mild and moderate hypovolemic shock [5]. The patient population in that study was categorized into mild, moderate, and severe hypovolemic shock, where maximum heart rates were 108 ± 26 beats/minute, 118 ± 23 beats/minute, and 130 ± 35 beats/minute, respectively. Their finding that thenar StO2 is insensitive to mild and moderate hypovolemic shock is supported by our data and, in addition, our data support the use of forearm StO2 as a more sensitive parameter for the detection of central hypovolemia and hypovolemic shock in (trauma) patients.
In conclusion, the present study has shown that forearm StO2 is more responsive to hemodynamic changes compared with thenar StO2 and that the response is similar for the applied probing depths. In addition, our results indicate that the change in StO2 during a cardiovascular challenge is more important than the absolute StO2 values for monitoring the effects of hemodynamic changes on peripheral tissue oxygenation. Our data furthermore suggest that the (micro)vascular response to a cardiovascular challenge might be similar in (sub)dermal tissue and in the muscle, and that it is the forearm tissue as a whole that is more sensitive to hemodynamic changes compared to the thenar tissue. This hypothesis, however, warrants further investigation.
Abbreviations
ANOVA: analysis of variance; LBNP: lower body negative pressure; NIRS: near-infrared spectroscopy; StO2: tissue oxygen saturation.
Competing interests
Multi-depth NIRS devices were provided by Hutchinson Technologies.
Acknowledgements
The present research is supported by the Landsteiner Foundation for Blood Transfusion Research.
This article is part of Critical Care Volume 13 Supplement 5: Tissue oxygenation (StO2) in healthy volunteers and critically-ill patients. The full contents of the supplement are available online at http://ccforum.com/supplements/13/S5. Publication of the supplement has been supported with funding from Hutchinson Technology Inc.
References
- Wo CC, Shoemaker WC, Appel PL, Bishop MH, Kram HB, Hardin E. Unreliability of blood pressure and heart rate to evaluate cardiac output in emergency resuscitation and critical illness. Crit Care Med. 1993;21:218–223. doi: 10.1097/00003246-199302000-00012. [DOI] [PubMed] [Google Scholar]
- Orlinsky M, Shoemaker W, Reis ED, Kerstein MD. Current controversies in shock and resuscitation. Surg Clin North Am. 2001;81:1217–1262. doi: 10.1016/s0039-6109(01)80006-2. [DOI] [PubMed] [Google Scholar]
- Porter JM, Ivatury RR. In search of the optimal end points of resuscitation in trauma patients: a review. J Trauma. 1998;44:908–914. doi: 10.1097/00005373-199805000-00028. [DOI] [PubMed] [Google Scholar]
- Wilson M, Davis DP, Coimbra R. Diagnosis and monitoring of hemorrhagic shock during the initial resuscitation of multiple trauma patients: a review. J Emerg Med. 2003;24:413–422. doi: 10.1016/s0736-4679(03)00042-8. [DOI] [PubMed] [Google Scholar]
- Crookes BA, Cohn SM, Bloch S, Amortegui J, Manning R, Li P, Proctor MS, Hallal A, Blackbourne LH, Benjamin R, Soffer D, Habib F, Schulman CI, Duncan R, Proctor KG. Can near-infrared spectroscopy identify the severity of shock in trauma patients? J Trauma. 2005;58:806–813. doi: 10.1097/01.ta.0000158269.68409.1c. [DOI] [PubMed] [Google Scholar]
- Soller BR, Yang Y, Soyemi OO, Ryan KL, Rickards CA, Walz JM, Heard SO, Convertino VA. Noninvasively determined muscle oxygen saturation is an early indicator of central hypovolemia in humans. J Appl Physiol. 2008;104:475–481. doi: 10.1152/japplphysiol.00600.2007. [DOI] [PubMed] [Google Scholar]
- Soller BR, Ryan KL, Rickards CA, Cooke WH, Yang Y, Soyemi OO, Crookes BA, Heard SO, Convertino VA. Oxygen saturation determined from deep muscle, not thenar tissue, is an early indicator of central hypovolemia in humans. Crit Care Med. 2008;36:176–182. doi: 10.1097/01.CCM.0000295586.83787.7E. [DOI] [PubMed] [Google Scholar]
- Soller BR, Yang Y, Soyemi OO, Heard SO, Ryan KL, Rickards CA, Convertino VA, Cooke WH, Crookes BA. Near infrared spectroscopy. Crit Care Med. 2009;37:385. doi: 10.1097/CCM.0b013e3181932d1b. [DOI] [PubMed] [Google Scholar]
- Torella F, Cowley RD, Thorniley MS, McCollum CN. Regional tissue oxygenation during hemorrhage: can near infrared spectroscopy be used to monitor blood loss? Shock. 2002;18:440–444. doi: 10.1097/00024382-200211000-00009. [DOI] [PubMed] [Google Scholar]
- Torella F, Haynes SL, McCollum CN. Cerebral and peripheral near-infrared spectroscopy: an alternative transfusion trigger? Vox Sang. 2002;83:254–257. doi: 10.1046/j.1423-0410.2002.00223.x. [DOI] [PubMed] [Google Scholar]
- Beilman GJ, Groehler KE, Lazaron V, Ortner JP. Near-infrared spectroscopy measurement of regional tissue oxyhemoglobin saturation during hemorrhagic shock. Shock. 1999;12:196–200. doi: 10.1097/00024382-199909000-00005. [DOI] [PubMed] [Google Scholar]
- Crookes BA, Cohn SM, Burton EA, Nelson J, Proctor KG. Nonin-vasive muscle oxygenation to guide fluid resuscitation after traumatic shock. Surgery. 2004;135:662–670. doi: 10.1016/j.surg.2003.11.017. [DOI] [PubMed] [Google Scholar]
- Cohn SM, Crookes BA, Proctor KG. Near-infrared spectroscopy in resuscitation. J Trauma. 2003;54(5 Suppl):S199–S202. doi: 10.1097/01.TA.0000047225.53051.7C. [DOI] [PubMed] [Google Scholar]
- McKinley BA, Marvin RG, Cocanour CS, Moore FA. Tissue hemoglobin O2 saturation during resuscitation of traumatic shock monitored using near infrared spectrometry. J Trauma. 2000;48:637–642. doi: 10.1097/00005373-200004000-00009. [DOI] [PubMed] [Google Scholar]
- Ikossi DG, Knudson MM, Morabito DJ, Cohen MJ, Wan JJ, Khaw L, Stewart CJ, Hemphill C, Manley GT. Continuous muscle tissue oxygenation in critically injured patients: a prospective observational study. J Trauma. 2006;61:780–788. doi: 10.1097/01.ta.0000239500.71419.58. [DOI] [PubMed] [Google Scholar]
- Moore FA, Nelson T, McKinley BA, Moore EE, Nathens AB, Rhee P, Puyana JC, Beilman GJ, Cohn SM. StO2 Study Group. Massive transfusion in trauma patients: tissue hemoglobin oxygen saturation predicts poor outcome. J Trauma. 2008;64:1010–1023. doi: 10.1097/TA.0b013e31816a2417. [DOI] [PubMed] [Google Scholar]
- Cohn SM, Nathens AB, Moore FA, Rhee P, Puyana JC, Moore EE, Beilman GJ. StO2 in Trauma Patients Trial Investigators. Tissue oxygen saturation predicts the development of organ dysfunction during traumatic shock resuscitation. J Trauma. 2007;62:44–54. doi: 10.1097/TA.0b013e31802eb817. [DOI] [PubMed] [Google Scholar]
- Sprangers RL, Veerman DP, Karemaker JM, Wieling W. Initial circulatory responses to changes in posture: influence of the angle and speed of tilt. Clin Physiol. 1991;11:211–220. doi: 10.1111/j.1475-097x.1991.tb00452.x. [DOI] [PubMed] [Google Scholar]
- Chan GS, Middleton PM, Celler BG, Wang L, Lovell NH. Change in pulse transit time and pre-ejection period during upright tilt-induced progressive central hypovolaemia. J Clin Monit Comput. 2007;21:283–293. doi: 10.1007/s10877-007-9086-8. [DOI] [PubMed] [Google Scholar]
- Zaidi A, Benitez D, Gaydecki PA, Vohra A, Fitzpatrick AP. Haemodynamic effects of increasing angle of head up tilt. Heart. 2000;83:181–184. doi: 10.1136/heart.83.2.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wieling W, Van Lieshout JJ, Ten Harkel AD. Dynamics of circulatory adjustments to upright tilt and tilt-back in healthy and sympathetically denervated subjects. Clin Sci (Lond) 1998;94:347–352. doi: 10.1042/cs0940347. [DOI] [PubMed] [Google Scholar]
- Smith JJ, Porth CM, Erickson M. Hemodynamic response to the upright posture. J Clin Pharmacol. 1994;34:375–386. doi: 10.1002/j.1552-4604.1994.tb04977.x. [DOI] [PubMed] [Google Scholar]
- Cui W, Kumar C, Chance B. Experimental study of migration depth for the photons measured at sample surface. Proc SPIE. 1991;1431:180–191. [Google Scholar]
- Myers DE, Cooper CE, Beilman GJ, Mowlem JD, Anderson LD, Seifert RP, Ortner JP. A wide gap second derivative NIR spectroscopic method for measuring tissue hemoglobin oxygen saturation. Adv Exp Med Biol. 2006;578:217–222. doi: 10.1007/0-387-29540-2_35. [DOI] [PubMed] [Google Scholar]
- Myers DE, Anderson LD, Seifert RP, Ortner JP, Cooper CE, Beilman GJ, Mowlem JD. Noninvasive method for measuring local hemoglobin oxygen saturation in tissue using wide gap second derivative near-infrared spectroscopy. J Biomed Opt. 2005;10:034017. doi: 10.1117/1.1925250. [DOI] [PubMed] [Google Scholar]