

1. Introduction
The transition from late adolescence to adulthood is characterized by multiple role transitions as youth leave high school, seek employment, and change living situations. Substance use in the general population increases throughout this period until it peaks in young adulthood (Brown et al., 2008; Maggs & Schulenberg, 2004/2005; Schulenberg et al., 2005). Youth who are transitioning out of the foster care system may be particularly vulnerable to substance use problems during this period. These youth possess unique risk factors such as histories of maltreatment and placement changes that have been associated with increased risk for substance abuse (Aarons et al., 2008). In addition, these youth face unique transitions as they leave the foster care system, often moving to independent living situations without the support of a family system to provide a safety net (McCoy, McMillen, & Spitznagel, 2008). Little is currently known about the prevalence of and risk factors for substance use and substance use disorders as foster youth make this transition. This study aims to fill this gap by examining rates and predictors of substance use and substance use disorders (SUD) in a cohort of youth aging out of foster care in Missouri. We begin with a review of the literature on substance use among youth in child welfare, followed by a look at substance use disorders in this population. We then review literature on associated risk factors for all youth in child welfare and finally the unique risks for foster youth transitioning to adulthood.
1.1 Substance use among youth in child welfare
Alcohol and marijuana use in the general population increase throughout the period of late adolescence into adulthood (Johnston, O’Malley, Bachman, & Schulenberg, 2007; SAMSHA, 2006). There is mixed evidence, however, about how rates of substance use among youth in child welfare compare to youth in the general population. In a report from the National Survey of Child and Adolescent Well being (NSCAW), a national probability sample of maltreated children, rates of alcohol and marijuana use among 11–15 year olds were lower than in the general population (Wall & Kohl, 2007). In a study of foster care youth ages 15–18, Thompson & Auslander (2007) found rates of alcohol use similar to those reported in the general population - 40% of the sample reported alcohol use in the previous six months. Marijuana use was higher than in the general population, however, with 36% reporting use in the past 6 months (Thompson & Auslander, 2007). In previously published results from the first wave of this study of 17 year old foster youth in Missouri, 37% of youth had used alcohol in the last six months and 26% had used marijuana in the past six months (Vaughn, Ollie, McMillen, Scott, & Munson, 2007), rates similar to those reported in the general population (Johnston et al., 2007). No studies have yet reported on rates of alcohol and marijuana use among foster youth as they transition out of foster care.
1.2 Substance use disorders among youth in child welfare
Diagnosable substance use disorders (SUD) have been consistently found to be higher among youth in child welfare than in the general population (Aarons, Brown, Hough, Garland, & Wood, 2001; Aarons et al., 2008; Courtney, Terao, & Bost, 2004; Pilowsky & Wu, 2006; Vaughn et al., 2007; Wall & Kohl, 2007). In a study of adolescents in the child welfare system in San Diego, Aarons et al (2001) found that 11% had met criteria for a substance use disorder in the past year and 19.2% had met criteria for a substance use disorder in their lifetime. Vaughn et al (2007) found that 35% of the 17 year old Missouri sample had met criteria for a substance use disorder in their lifetime. In a report from the Midwest Evaluation of former foster youth study, 14% of 17 year old youth had met criteria for alcohol use disorder in their lifetime and 7.3% had met criteria for a substance use disorder (Courtney et al., 2004). Rates of alcohol and substance use disorders in the general population as reported in the National Epidemiological Survey of Alcohol and Related Disorders (NESARC) were 9.35% (Grant et al., 2004).
1.3 Risk factors for substance use and substance use disorders among youth in child welfare
Previous studies have identified demographic, psychosocial, and contextual risk factors for substance use for youth in child welfare. In a study of youth ages 13–18 in California, Aarons et al (2008) found that male gender, history of abuse, presence of internalizing or externalizing disorders, peer or sibling substance use, and older age at entry into child welfare were significantly related to increased risk for substance use and substance use disorders (Aarons et al., 2008). Analysis of data from 11–15 year olds from the National Survey of Child and Adolescent Well-being found that conduct disorder, history of physical abuse, and lower level of caregiver monitoring were associated with increased odds of substance use. African American youth in the sample reported significantly lower levels of substance use than their white and Hispanic peers (Wall & Kohl, 2007).
Two studies of older youth in foster care in Midwestern states provide information on risk factors for substance use specific to the older youth population. Vaughn et al. (2007) found that white race, history of physical neglect, history of conduct disorder or post traumatic stress disorder, and being in a more independent living situation were associated with increased odds of substance use and disorders in 17 year old foster youth. Having friends that used substances and skipping school were associated with increased odds of substance use in Thompson & Auslander’s (2007) study of 15–18 year old youth in care.
1.4 Unique risk factors as foster youth transition to adulthood
Older youth in foster care face the unique transition of leaving state custody as they age into adulthood, resulting in reduced support at a critical developmental period. While many young people face transitions to independence during this period, youth who age out of foster care often start out with a reduced support network, then face an additional reduction in support when they leave state custody. Many state policies allow youth to remain in care beyond age 18 under some circumstances (Dworsky & Havlicek, 2009), however, data from the Adoption and Foster Care Reporting System indicate that most youth leave care prior to age 19 (U. S. Department of Health and Human Services, 2008). In the Midwest Evaluation of former foster youth, young people who remained in foster care at age 19 had lower rates of substance use disorders (Courtney & Dworsky, 2006), though it is not clear whether this was the cause or effect of leaving care.
In addition to the transition in custody status during this period, many young people in foster care are also making transitions to less restrictive living situations. McCoy et al (2008) found that at age 17, many older youth in foster care resided in residential placements, however, by age 19 most had transitioned to less restrictive situations such as independent living programs or living with relatives. The steep transition out of highly structured environments may increase opportunities for substance use. Vaughn et al (2007) found that being in an independent living situation was associated with increased substance use in their sample of 17 year old foster youth.
1.5 The present study
Problem behavior theory provides a framework for understanding adolescent substance use as part of a developmental process, stressing the importance of environmental context as a whole in influencing an underlying pattern of problem behaviors (Donovan & Jessor, 1985). This study is guided by this theory in conceptualizing substance use in older foster youth as a result of underlying vulnerabilities and a changing environmental context. Youth transitioning out of foster care have increased vulnerabilities due to their abuse histories and unique risk factors as they leave the care of the state, often transitioning to independent situations with minimal supervision. Therefore, this study will address the following questions: How do rates of substance use and SUDs change as youth in child welfare transition to adulthood? How do rates of substance use differ by living situation? How do rates of substance use change as youth exit the foster care system? What factors, including transitions in living situation and custody status, are associated with getting drunk, marijuana use, and SUDs at ages 18 and 19? We anticipate that rates of substance use will increase for all youth over the transition period. We also expect that leaving the foster care system and transitioning to more independent situations will be associated with higher levels of substance use and SUDs.
2. Method
2.1 Participants
This study utilizes data from a larger study of older youth transitioning out of foster care in which youth were interviewed every 3 months. This paper utilizes data from interviews conducted at ages 17, 18 and 19 where youth were asked about their substance use. Participants were recruited from a pool of all youth turning age 17 in the foster care system in eight counties in Missouri between December 2001 and May 2003. Youth were screened by their Missouri Division of Family Services worker for inclusion criteria. Youth with IQ scores below 70 (n=31), those placed more than 100 miles from any of the eight counties (n=31), and youth who remained on runaway status up to 45 days past their 17th birthday (n=49), were excluded from the study. Ninety percent of the eligible youth were interviewed (n=404). This paper uses results from the 325 young adults who completed the study by participating in an interview at age 19, 80% of those who completed the first interview. Participants not retained were lost due to inability to locate (n=63), drop out (n=7), incarceration (n=7), overseas military service (n=2), and death (n=1). Twenty five participants who completed the final interview of the study did not complete an interview at age 18.
2.2 Procedures
Participants were interviewed by trained professional interviewers who used a structured interview protocol. Interviews were conducted in person at ages 17 and 19 and by phone when possible at age 18. Youth received $40 for the initial and final interviews and $20 for the phone interview. The study was approved by the University Human Subjects Committee and a federal certificate of confidentiality was obtained.
2.3 Measurement
2.3.1 Demographics
Race, gender, and geographic region were used as independent variables in this study. Race was recoded into Caucasian (0) and Youth of color (1) due to the small number of Latinos, Asians, and other minority groups in our sample. This racial distribution is typical of foster care populations in this region. Gender was dummy coded as 0=Female, 1=Male. Geographic region was originally measured by a variable that indicated the county in which the youth’s placement originated. For this analysis, counties with similar characteristics were grouped into 3 different regions. St. Louis City and the Southwest region of the state were dummy coded and the suburban counties outside St. Louis City were used as the reference group.
2.3.2 Maltreatment history/mental health history
Abuse history and mental health diagnosis were assessed at the initial interview and used as predictor variables. Physical abuse and physical neglect were measured using the Childhood Trauma Questionnaire (Bernstein & Fink, 1998) and dichotomous variables were created using cut off scores recommended by the author for severe or moderate maltreatment. Sexual abuse was measured using 3 items adapted from Russell (1986). Lifetime history of mental health diagnoses of conduct disorder, posttraumatic stress disorder, mania, attention deficit disorder, and major depression were assessed at the initial interview using the Diagnostic Interview Schedule, Version IV (Robins, Cottler, Bucholz, & Comptom, 1995). Indicators for lifetime history of each of these disorders were entered separately into multivariate models.
2.3.3 Past service use
Youth were asked at the initial interview whether they had ever been in a psychiatric hospital or ever stayed over night in a juvenile detention center using questions from the Service Assessment for Children and Adolescents (Stiffman, Horwitz, & Hoagwood, 2000). This instrument has demonstrated good to excellent test retest reliability for lifetime service use with children over age 10 (Horwitz et al., 2001). These variables were chosen as indicators of level of functional impairment for psychiatric and behavioral problems and used as control variables in multivariate analyses.
2.3.4 Peer substance use
Youth were asked to report on alcohol and marijuana in their peer group at each of the three time points with the following questions: “How many of your friends drink alcohol at least once a week?” and “How many of your friends use marijuana or other drugs?” Response categories for both questions included: None, a few, about half, most, and all. The variables were re-coded into three responses categories: none, a few, and half or more. Friends using alcohol was used to predict getting drunk; friends using marijuana or other drugs was used to predict marijuana use; and friends using either were used to predict substance use disorders.
2.3.5 Living situation
Living situation was assessed by the interviewer at each interview and coded into 20 categories which were then recoded into four for analysis (congregate care, living with kin, nonfamily foster home, and living more independently). For the 25 youth who were not contacted at age 18, living situation at age 18 was obtained utilizing a history calendar in the final interview. In order to look at the impact of changes in living situation, separate dichotomous variables were created to indicate whether there was a change to independent living from age 17 to 18 or from age 18 to 19. The same procedure was followed to create variables to indicate a change out of residential care from age 17 to 18 or from age 18 to 19.
2.3.6 Substance use and substance use disorders
Alcohol, marijuana and other substance use were measured with items modified from the Diagnostic Interview Schedule, Version IV (Robins et al., 1995). For this analysis, drinking was dichotomized by whether the respondent had been drunk within the time period. At the initial interview, respondents were asked whether they had been drunk in the past 6 months. At age 18 and 19, participants were asked whether they had been drunk in the previous year. Marijuana use was dichotomized by whether the respondent had smoked marijuana in the month prior to the interview. Other drug use was assessed with questions about whether the respondent had used amphetamines, opiates, cocaine, crack, hallucinogens, or inhalants. A dichotomous variable was created to indicate whether the respondent had used any of these drugs during the month prior to the interview. Questions from the Comprehensive Addiction Severity Index for Adolescents (Myers, 1994) were used to assess DSM-IV criteria for past year substance abuse and substance dependence at ages 18 and 19. Recent tests of reliability for the drug and alcohol addiction subscale of this instrument have found coefficient alpha of .86 and test-retest correlation of .95 (Myers et al., 2006). Participants who met criteria for either a substance abuse or substance dependence disorder in the past year were included in the substance use disorder category.
2.4 Analyses
Measures of substance use at age 18 were imputed for the 25 youth who did not complete that interview using IVEware (Raghunathan, Solenberger, & Van Hoewyk, 2002). The imputed values for each individual are fully conditional on all the values observed for that individual, with imputation conducted on a variable by variable basis using a sequence of regression models, varying the types of regression model by the type of variable being imputed (Raghunathan, Lepkowski, Van Hoewyk, & Solenberger, 2001). Five implicates of imputed variables were generated based on all of the available information.
Frequencies and percentages were calculated to describe sample characteristics as well as assess prevalence of getting drunk, using marijuana, using other substances, and substance use disorders at each time point. Chi square tests were used to test statistical significance of bi-variate relationships between the independent variables and each dependent variable. McNemar’s chi-square was used to test significance of changes in substance use and dependence from age 18 to age 19. Generalized estimating equations were used to test the significance of changes in rates of substance use over time. This approach was used due to its ability to produce less biased regression parameters with repeated measures longitudinal data (Ballinger, 2004). Multiple logistic regression analyses examined predictors of marijuana use, getting drunk, and a substance use disorder at ages 18 and 19. Proc MIanalyze was utilized in order to account for imputed data in the analysis. Models were built using backwards elimination. Variables were retained in the model if they remained significant at the p=.10 level.
3. Results
The sample used in this analysis contained 325 youth of whom 61% were female (n=197) and 59% were youth of color (n=192). A logistic regression analysis to predict retention was previously reported (McMillen & Raghavan, 2009). Being male, having a history of juvenile detention, having a history of post traumatic stress disorder, and being released from state custody prior to age 19 were all found to increase the odds of prematurely leaving the study.
3.1 Prevalence of substance use over time
The results in Table 1 show the prevalence of substance use at age 17, 18 and 19. The percentage of young people who reported getting drunk increased significantly from age 17 to age 18 (χ2=8.97, p<.001), however, at age 17 youth reported getting drunk in the last six months while at age 18, they reported getting drunk in the past year. The increase in the percentage getting drunk continued, however, from ages 18 and 19, when the reporting period was consistent. The percentage of youth who reported having been drunk in the past year increased significantly from 18% to 31% (χ2=19.60, p<.001). The percentage of youth who reported past month marijuana use also increased from age 17 to age 18 (χ2=2.86, p<.10), with a larger increase from 13% to 20% of the sample from age 18 to age 19 (χ2=8.00, p<.001). Self-reported use of other drugs increased from 2% at age 17 to 5% at age 18 (χ2=5.76, p<.05) but by only 1% from age 18 to age 19. The lifetime prevalence for substance use disorders were obtained at Age 17. As previously reported in an article by Vaughn et al (2007), 35% of the sample had met criteria for a SUD in their lifetime. The prevalence of substance abuse and substance dependence for the past 12 months were measured at ages 18 and 19. In spite of increases in the percentage of youth using substances from age 18 to 19, the changes in prevalence of substance abuse and substance dependence were not statistically significant.
Table 1.
Substance use by foster care youth from ages 17–19 (n=325)
| % prevalence/(change χ2) | |||
|---|---|---|---|
| Variable | Age 17 | Age 18 | Age 19 |
| Got drunk in past 6 months (age 17) or year (age 18 & 19) | 11 | 18 (8.97***) | 31 (19.60***) |
| Used marijuana in the previous month | 9 | 13 (2.86+) | 20 (8.00**) |
| Used other drugs in previous month | 2 | 5 (5.76*) | 6 (0.06) |
| Met criteria for substance abuse disorder in past year | — | 12 | 9 (1.38) |
| Met criteria for substance dependence in past year | — | 4 | 6 (1.65) |
+ p<.10,
p<.05,
p<.01,
p<.001
3.2.1 Rates of substance use by living situation
Tables 2 & 3 present the frequencies of getting drunk and marijuana use for each living situation across the three time points. Those living in independent living situations at age 17 reported higher rates of both getting drunk and marijuana use than youth in all other living situations, however at older ages, youth who lived in independent situations did not have higher self-reported rates of getting drunk or marijuana use. The percentage of youth who had used marijuana in the past month declined from 42% of those in independent situations at age 17 to 14% of those in independent situations at age 19. Those who were living in a biological or relative home at age 19 reported slightly higher rates of getting drunk than youth in independent situations and a rate of marijuana use 12% higher than those in independent situations, however, the differences were not statistically significant.
Table 2.
Got drunk in the past 6mo (age 17) or year (age 18 & 19) by living situation (n=325)
| n/% who reported use in each group | |||||
|---|---|---|---|---|---|
| Congregate Care | Non-kin foster home | Biological/Relative Home | Independent | Chi-square | |
| Age 17 | 16/136 (12%) | 10/91 (11%) | 6/86 (7%) | 4/12 (33%) | 7.57+ |
| Age 18 | 3/65 (5%) | 12/61 (20%) | 22/114 (19%) | 22/85 (22%) | 11.63*** |
| Age 19 | 5/29 (17%) | 8/31 (26%) | 40/73 (35%) | 48/152 (32%) | 4.00 |
+ p<.10,
p<.05,
p<.01,
p<.001
Table 3.
Used marijuana in the past month by living situation (n=325)
| n/% who reported use in each group | |||||
|---|---|---|---|---|---|
| Congregate Care | Non-kin foster home | Biological/Relative Home | Independent | Chi-square | |
| Age 17 | 9/136 (7%) | 7/91 (8%) | 8/86 (9%) | 5/12 (42%) | 16.91*** |
| Age 18 | 5/65 (8%) | 5/61 (8%) | 15/114 (13%) | 17/85 (20%) | 6.58+ |
| Age 19 | 4/29 (14%) | 4/31 (13%) | 29/113 (26%) | 29/152 (19%) | 3.96 |
+ p<.10,
p<.05,
p<.01,
p<.001
3.2.2 Rates of substance use by system exit
Figures 1 and 2 display the rates of getting drunk and marijuana use at age 17, 18, and 19 subdivided by the age at which youth left the formal foster care system. Though substance use increased for all groups across this time period, self-reported rates of use increased significantly more for youth who left foster care. At age 18, 28% of youth who had left care reported having gotten drunk compared to 16% of youth who stayed in the foster care system (χ2 =5.13, p<.05). At age 19, these differences were more pronounced, with 40% of youth who left reporting having been drunk compared to 21% of those who stayed (χ2 =13.02, p<.001). Thirty percent of youth who left care reported using marijuana at age 18 compared with 9% of those who stayed (χ2 =19.07, p<.0001). This difference diminished somewhat but was still significant at age 19 with 25% of those who left reporting use compared to 15% of those who stayed (χ2 =4.97, p<.05). At age 18, getting drunk and marijuana use were highest among those who had left care within the past year. The group that would leave care between age 18.6 and 19, looked very similar to youth who stayed in care at age 18 on both rates of drinking and marijuana use. At age 19, however, their rates increased sharply to surpass those who had left care between ages 17 and 18. The steepest increases in substance use can be seen in all groups in the year after the youth left care.
Figure 1.
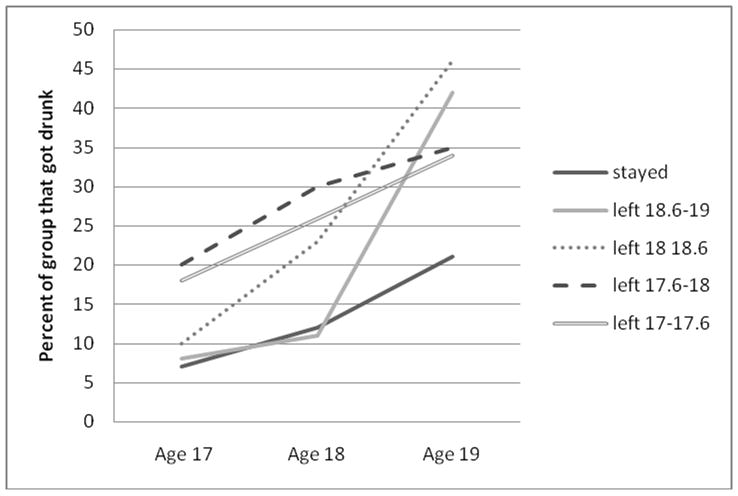
Got drunk by age of system exit (n=325)
Figure 2.
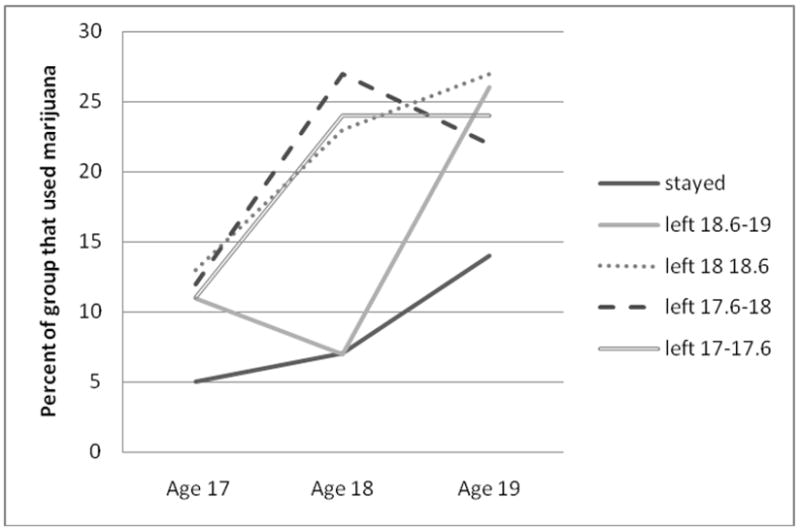
Used marijuana in the past month by age of system exit (n=325)
3.3 Predictors of Getting Drunk, Marijuana Use and Substance Use Disorders
3.3.1 Predictors at age 18
Results of the logistic regression models for getting drunk, marijuana use, and SUDs at age 18 are presented in Table 4. Peer substance use was a predictor for all three dependent variables. Youth who reported that half their peers used marijuana were more likely to have used marijuana (OR=3.00, p<.05), those who reported that half their peers used alcohol were more likely to have been drunk (OR=2.71, p<.05), and those who reported their peers used either substance were more likely to have met criteria for a substance use disorder in the past year compared to youth who had no friends who used (OR=4.10, p<.05). Conduct disorder at age 17 was a significant predictor of having a substance use disorder at age 18 (OR=3.33, p<.05). The transition out of custody was a risk factor for marijuana use with youth who had left custody in the previous year being significantly more likely to have used marijuana in the previous month (OR=3.41, p<.05). Some transitions in living situations were also associated with higher use. Youth who had left a congregate care setting in the past year were more likely to report being drunk compared to all other youth (OR=2.98, p<.05), while those who had moved to an independent living situation in the past year were more likely to report marijuana use compared to all other youth (OR=2.29, p<.05).
Table 4.
Logistic Regression for Got Drunk, Marijuana Use, and Substance Use Disorder at Age 18
| Variable | Got Drunk in past year | Used marijuana in the past month | Met criteria for substance use disorder – abuse or dependence | |||
|---|---|---|---|---|---|---|
| OR | CI | OR | CI | OR | CI | |
| Demographics | ||||||
| Youth of color | .34** | .17–.69 | ||||
| Maltreatment History | ||||||
| Sexual abuse | 1.94+ | .88–4.28 | ||||
| Mental Health Disorder | ||||||
| Conduct disorder | 3.33* | 1.34–8.30 | ||||
| Peer Substance Use | ||||||
| Half or more peers use | 2.71* | 1.13–6.51 | 3.00* | 1.13–7.99 | 4.10* | 1.19–14.13 |
| A few peers use | 1.59 | .72–3.50 | 1.08 | .39–2.99 | 1.34 | .43–4.11 |
| Transitions | ||||||
| Left custody of CD in past year | 3.41** | 1.54–7.58 | ||||
| Moved to independent living in past year | 2.29* | 1.02–5.13 | ||||
| Left congregate care in past year | 2.98* | 1.29–6.85 | ||||
| Model statistic | c=.72 | c=.73 | c=.75 | |||
+ p<.10,
p<.05,
p<.01,
p<.001
3.3.2 Predictors at age 19
Logistic regression models for getting drunk, marijuana use and SUDs at age 19 are shown in Table 5. Peer use of substances continued to be a significant predictor of getting drunk, marijuana use, and substance use disorders at age 19. At age 18, having half of peers using was a significant predictor while having few peers was not. At age 19, however, having a few friends who used substances was also significant. Several different predictors emerged as significant for getting drunk at age 19 compared to age 18. Male youth were substantially more likely to use alcohol compared to their female peers (OR=3.19, p<.001) and youth who had a history of sexual abuse were more likely to use alcohol compared to those who had not (OR=2.37, p<.01). Living in St. Louis was protective for getting drunk (OR=.51, p<.05) while leaving state custody was associated with greater odds of getting drunk (OR=2.12, p<.05). Transitions out of residential care and into independent living had been included in models at age 18, but were not significantly associated with substance use or SUDs at age 19.
Table 5.
Logistic Regression for Got Drunk, Marijuana Use, and Substance Use Disorder at Age 19
| Variable | Got drunk in past year | Used marijuana in the past month | Met criteria for substance use disorder – abuse or dependence | |||
|---|---|---|---|---|---|---|
| OR | CI | OR | CI | OR | CI | |
| Male gender | 3.19*** | 1.68–6.05 | ||||
| Geographic Region | ||||||
| St. Louis City | .51* | .27–.98 | .32+ | .10–1.02 | ||
| Southwest State | .87 | .40–1.91 | 1.96 | .63–6.11 | ||
| Maltreatment History | ||||||
| Physical abuse | .34* | .13–.92 | ||||
| Sexual abuse | 2.37** | 1.23–4.55 | 1.79+ | .96–3.35 | 2.74* | 1.05–7.11 |
| Mental Health Disorder | ||||||
| Conduct disorder | 3.76** | 1.80–7.88 | 2.80** | 1.43–5.45 | 3.21* | 1.24–8.31 |
| Post traumatic stress disorder | 2.04+ | .89–4.68 | ||||
| Peer Substance Use | ||||||
| A few friends use | 6.17*** | 2.54–15.02 | 5.70*** | 2.34–13.88 | 1.94 | .56–6.71 |
| Half or more use | 12.64*** | 5.13–31.16 | 20.09*** | 8.36–48.29 | 8.19*** | 2.40–28.05 |
| Transitions | ||||||
| Left custody of CD in past year | 2.12* | 1.11–4.05 | 2.70+ | .92–7.94 | ||
| Left CD custody between 17–18 | 2.22+ | .99–4.98 | 2.85+ | .83–9.69 | ||
| Model statistic | c=.83 | c=.81 | c=.82 | |||
+ p<.10,
p<.05,
p<.01,
p<.001
4. Discussion
This study is the first to examine both substance use and substance use disorders as foster youth age out of care. Three findings merit further comment. 1) Rates of substance use were generally lower than those found in the general population, while rates of SUDs were higher. 2) Leaving care was associated with steeper increases in substance use, with a time of increased vulnerability in the year after leaving care. 3) Different risk factors for getting drunk and marijuana use appear to exist at age 18 compared to age 19, while risk factors for substance use disorders were more stable.
As expected, substance use increased over the course of the study, regardless of living situation or custody status. Rates of having been drunk in the past year for our sample were lower at each time point than those reported for 10th and 12th graders in the 2003 Monitoring the Future Study (34.7% and 48%), however, the 13% increase observed in this sample is similar to the 13.3% increase between 10th and 12th graders in the MTF study (Johnston, O’Malley, Bachman, & Schulenberg, 2003). Rates of marijuana use in the past month at age 18 (13% in this sample) were lower than the MTF 10th graders (17%), however, rates at age 19 were similar to those of 12th graders (20% in this sample, 21.2% in MTF). Rates of all substance use disorders were compared to the Missouri data from the National Survey on Drugs and Health (SAMSHA, 2006). Rates in our sample were about 6% higher than those reported in this study. In our sample, youth that were involved with the foster care system used alcohol and marijuana at rates lower than or similar to the general population, however, rates of disorder were substantially higher than the general population. This parallels findings from the initial wave of data collection on lifetime substance use and SUDs (Vaughn et al, 2007). The persistence of high rates of substance use disorders among these youth highlight the need for screening youth at high risk for SUDs and providing treatment prior to their exit from care.
Our data also suggest that staying in state custody may have a protective effect against substance use as youth age into adulthood. No firm conclusion can be drawn from these results as youth in care may be less likely to report their true substance use than youth who have left the foster care system and youth who use substances may be less likely to remain in care. However, youth who remained in state custody consistently reported low rates of use, and while their use increased over time, the amount of these increases was much lower than those who left. Comparison of rates of use by when youth left care could indicate that the year after leaving care is a time of heightened vulnerability for substance use. Youth who had left before age 18 had higher rates at age 18 than at age 19, while youth who had left between 18 and 19 had the highest rates at age 19. More data is needed to further explore this relationship, however, it may be beneficial to consider education about substance use in discharge planning to discourage the initial surge in use following discharge.
Different sets of risk factors emerged for marijuana and alcohol at age 18 and age 19. Leaving congregate care was a predictor of getting drunk at age 18; however, it was not significant at age 19. Moving to an independent situation was a predictor of marijuana use at age 18 but not at age 19. Overall, transitions in living situation appear to have a greater impact on substance use at age 18 than at age 19. Substance abuse education and prevention efforts may be especially important for youth who are moving to less restrictive settings prior to age 18. The risk factors for substance use disorders, however, were relatively stable from ages 18 to 19. Having a history of conduct disorder, history of sexual abuse, or peers who used alcohol or marijuana were predictors of substance use disorders at both age 18 and 19. Screening for substance use disorders may be most efficiently targeted to youth who have these risk factors.
While this study provides important new information about substance use in this population, there are several limitations that should be considered in interpreting the results. Substance use was measured using youth self-report with no verification from collateral informants. Youth who are in state custody may be more likely to underreport their substance use compared to youth who are no longer in care. In addition, the report of getting drunk was for the past 6 months at age 17 and then the last year at ages 18 and 19. This limitation should be considered when comparing these rates over time. Generalizability to a wider geographic area may also be limited as these data were collected from youth in eight counties of one state. Finally, youth who were lost from the study differed from those who remained in the study. The youth who left the study shared some risk factors for substance use so the rates obtained may reflect an underreporting of substance use in this population.
This study provides data that can inform interventions directed at preventing substance use as young people transition out of custody. In addition, these findings highlight the need to provide substance abuse treatment as older youth in foster care are experiencing SUDs at higher rates than the general population. Intervening through the child welfare system before these young people leave care provides an opportunity to provide education and treatment that can promote positive transitions to adulthood.
This study also provides further support for the value of extending state custody for these young people beyond age 18. In a review of state policies to support young people transitioning out of care conducted in 2006, Dworsky and Havlicek (2009) found that all but 2 of the 45 states that responded had policies that allowed youth to remain in care under some circumstances. Only 14 of the states, however, specifically listed substance abuse or mental health treatment as one of the circumstances that could extend care (Dworsky & Havlicek, 2009). The Fostering Connections to Success and Increasing Adoptions Act of 2008 provides increased federal support for states that choose to extend care for foster youth to age 21. The high rates of substance use disorders among these youth and the association between SUDs and leaving state custody underscore the importance of developing policies that consider SUDs and the provision of substance abuse treatment in decisions to extend care.
Acknowledgments
This research was supported by NIMH R01-MH-6104, Curtis McMillen, principal investigator and NIMH T32-MH-19960 training grant. Thanks to Ed Spitznagel for statistical support.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Sarah Carter Narendorf, Washington University.
J. Curtis McMillen, Washington University.
References
- Aarons GA, Brown SA, Hough RL, Garland AF, Wood PA. Prevalence of adolescent substance use disorders across five sectors of care. Journal of the American Academy of Child and Adolescent Psychiatry. 2001;40(4) doi: 10.1097/00004583-200104000-00010. [DOI] [PubMed] [Google Scholar]
- Aarons GA, Hazen AL, Leslie LK, Hough RL, Monn AR, Connelly CD, et al. Substance involvement among youths in child welfare: The role of common and unique risk factors. American Journal of Orthopsychiatry. 2008;78(3):340–349. doi: 10.1037/a0014215. [DOI] [PubMed] [Google Scholar]
- Ballinger GA. Using generalized estimating equations for longitudinal data analysis. Organizational Research Methods. 2004;7(2):127–150. [Google Scholar]
- Bernstein DP, Fink L. The Childhood Trauma Questionnaire Manual. SanAntonio, TX: The Psychological Corporation; 1998. [Google Scholar]
- Brown SA, McGue M, Magge J, Schulenberg J, Hingson R, Swarzwelder S, et al. A developmental perspective on alcohol and youths 16 to 20 years of age. Pediatrics. 2008;121(Supplement 4):S290–310. doi: 10.1542/peds.2007-2243D. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courtney ME, Dworsky A. Early outcomes for young adults transitioning from out-of-home care in the USA. Child and Family Social Work. 2006;11:209–219. [Google Scholar]
- Courtney ME, Terao S, Bost N. Midwest evaluation of the adult functioning of former foster youth: conditions of preparing to leave state care [Electronic Version] 2004 Retrieved 3/19/2009, from http://www.chapinhall.org/sites/default/files/CS_97.pdf.
- Donovan JE, Jessor R. Structure of problem behavior in adolescence and young adulthood. Journal Of Consulting and Clinical Psychology. 1985;53(6):890–904. doi: 10.1037//0022-006x.53.6.890. [DOI] [PubMed] [Google Scholar]
- Dworsky A, Havlicek J. Review of state policies and programs to support young people transitioning out of foster care [Electronic Version] 2009 Retrieved 7/12/2009, from http://www.chapinhall.org/research/report/national-review-policies-and-programs-supporting-youth-transitioning-out-foster-care.
- Grant BF, Dawson DA, Stinson FS, Chou SP, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991–1992 and 2001–2002. Drug and Alcohol Dependence. 2004;74:223–234. doi: 10.1016/j.drugalcdep.2004.02.004. [DOI] [PubMed] [Google Scholar]
- Horwitz SM, Hoagwood K, Stiffman AR, Summerfeld T, Weisz JR, Costello EJ, et al. Reliability of the services assessment for children and adolescents. Psychiatric Services. 2001;52(8):1088–1094. doi: 10.1176/appi.ps.52.8.1088. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg J. Monitoring the future: National results on adolescent drug use. Overview of Key Findings, 2003. 2003 Retrieved March 12, 2009, from http://www.monitoringthefuture.org/pubs/monographs/overview2003.pdf.
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg J. Monitoring the future: National results on adolescent drug use. Overview of Key Findings 2007. 2007 Retrieved 3/12/2009, from http://www.monitoringthefuture.org/pubs/monographs/overview2007.pdf.
- Maggs J, Schulenberg J. Trajectories of alcohol use during the transition to adulthood. Alcohol Research & Health. 20042005;28(4):195–201. [Google Scholar]
- McCoy H, McMillen JC, Spitznagel EL. Older youth leaving the foster care system: Who, what, when, where, and why? Children and Youth Services Review. 2008;30:735–745. doi: 10.1016/j.childyouth.2007.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMillen JC, Raghavan R. Pediatric to adult mental health service use of young people leaving the foster care system. Journal of Adolescent Health. 2009;44:7–13. doi: 10.1016/j.jadohealth.2008.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myers K. Comprehensive addiction severity index for adolescents. In: McClellan T, Dembo R, editors. Screening and assessment of alcohol-and other drug-abusing adolescents. Rockville, MD: Substance Abuse and Mental Health Services Administration; 1994. [Google Scholar]
- Myers K, Hagan TA, McDermott P, Webb A, Randall M, Frantz J. Factor structure of the Comprehensive Adolescent Severity Inventory (CASI): Results of reliability, validity, and generalizability analyses. The American Journal of Drug and Alcohol Abuse. 2006;32:287–310. doi: 10.1080/00952990500479464. [DOI] [PubMed] [Google Scholar]
- Pilowsky DJ, Wu LT. Psychiatric symptoms and substance use disorders in a nationally representative sample fo American adolescents involved with foster care. Journal of Adolescent Health. 2006;38:351–358. doi: 10.1016/j.jadohealth.2005.06.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raghunathan TE, Lepkowski JM, Van Hoewyk J, Solenberger P. A multivariate technique for multiply imputing missing values using a sequence of regression models. Survey Methodology. 2001;27:85–95. [Google Scholar]
- Raghunathan TE, Solenberger PW, Van Hoewyk J. IVEware: Imputations and variance estimation software user guide. Ann Arbor, MI: Survey Research Center, Institute for Social Research; 2002. [Google Scholar]
- Robins L, Cottler L, Bucholz K, Comptom W. Diagnostic interview schedule for DSM-IV. St. Louis, MO: Washington University in St. Louis; 1995. [Google Scholar]
- Russell DEH. The secret trauma: Incest in the lives of girls and women. New York: Basic Books; 1986. [Google Scholar]
- SAMSHA. 2006 State Estimates of Substance Use & Mental Health. National Survey of Drug Use & Health. 2006 Retrieved 3/12/2009, from www.oas.samhsa.gov/2k6State/Missouri.htm.
- Schulenberg J, Merline AC, Johnston LD, O’Malley PM, Bachman JG, Laetz V. Trajectories of marijuana use during the transition to adulthood: The big picture based on national panel data. Journal Of Drug Issues, Spring. 2005:255–279. doi: 10.1177/002204260503500203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stiffman AR, Horwitz SM, Hoagwood K. The Service Assessment for Children and Adolescents (SACA): adult and child reports. Journal of American Academy of Child and Adolescent Psychiatry. 2000;39:1032–1039. doi: 10.1097/00004583-200008000-00019. [DOI] [PubMed] [Google Scholar]
- Thompson RG, Auslander WF. Risk factors for alcohol and marijuana use among adolescents in foster care. Journal of Substance Abuse Treatment. 2007;32:61–69. doi: 10.1016/j.jsat.2006.06.010. [DOI] [PubMed] [Google Scholar]
- U. S. Department of Health and Human Services. The AFCARS report: Preliminary FY 2006 estimates as of January 2008. 2008 Retrieved July 12, 2009 from http://www.acf.hhs.gov/programs/cb/stats_research/afcars/tar/report14.htm.
- Vaughn MG, Ollie MT, McMillen JC, Scott L, Munson M. Substance use and abuse among older youth in foster care. Addictive Behaviors. 2007;32:1929–1935. doi: 10.1016/j.addbeh.2006.12.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wall AE, Kohl PL. Substance use in maltreated youth: Findings from the National Survey of Child and Adolescent Well-Being. Child Maltreatment. 2007;12(1):20–30. doi: 10.1177/1077559506296316. [DOI] [PubMed] [Google Scholar]