

Introduction
The Institute of Medicine is calling for nursing homes to implement and use clinical information systems to support clinical practice 1. Thus, it was suggested, by 2007, nursing homes should have integrated electronic medical records to clinically manage residents and computerized cross checking for drug-dose, drug-lab, and drug-diet verification. To date there is limited evidence that nursing homes are reaching these levels of sophistication, with 1% or less of skilled nursing facilities, for example, incorporating electronic health records into clinical processes 2, 3. In most cases, nursing home technology has been limited to business applications related to billing/claims, eligibility processing, and the minimum data set 4-6. However, innovation does exist and nursing homes using highly sophisticated computerized systems to manage care have been identified7, 8. Through these innovators much has been learned about the ways in which sophisticated technologies can facilitate the exchange of information to thereby improve client safety and quality of care 9-11. The current paper presents an initial evaluation of the concept of IT sophistication in nursing homes using qualitative analytics including field notes collected during interviews and focus groups and axial coding to derive common themes.
IT sophistication is the level of diversity in technological tools and software used to support patient care, clinical support, and administration 12. Greater IT sophistication has been shown to have a positive effect on the ability to provide improved quality of care in acute care settings 13; however, there is limited understanding of the level of IT sophistication present and its effects in nursing homes. Consequently, the purpose of this study was to develop a matrix of nursing home IT sophistication from interviews and focus groups with knowledgeable IT staff using highly sophisticated IT systems. Common themes derived from the interviews and focus groups resulted in a matrix of the attributes describing the dimensions of IT sophistication (functional, technological, integration) in three domains of healthcare (resident care, clinical support, administration). The matrix of nursing home IT sophistication will be used as a framework to measure IT sophistication in future studies.
IT Sophistication in Nursing Homes
IT sophistication was derived from Nolan’s Stage Theory, which has been used to evaluate computer activity and the degree of IT maturation over time 14. Nolan identified four stages that organizations move through on the way to a fully integrated information system. Nolan’s stages include initiation, expansion, formalization, and maturity. These stages represent growth from technology meeting basic isolated organizational needs to a fully integrated system that meets general organizational needs15. For example, a basic isolated system would report employees’ work schedules on a nursing unit; in contrast, a fully integrated system would use employee schedules, financial data, resident census and acuity to support administrative decision making about staffing needs for a clinical unit or facility. The range of integration from isolated to fully integrated information systems creates diversity between facility operations, influences interoperability between internal and external stakeholders and can provide a unique measure for a facility’s level of IT sophistication.
An example illustrating the importance of interoperability of integrated information systems is demonstrated during a transition of care from a nursing home to another healthcare facility. Figure 1 provides a diagram depicting stakeholders (patient, clinician, receiving facility, and transferring facility) involved in the transition of care for a patient between two healthcare facilities16. The range of integration of sophisticated information systems such as electronic health records (EHR) affects the presentation and types of patient care data transferred between facilities. Diverse information can lead to conflicts and consensus about the need for transfer between stakeholders involved in the care of the patient as a result of varied interpretations of the acuity or severity of the health problem17. National efforts are currently underway to standardized clinical information, determine necessary patient data, and to structure information about the intended care to be provided by the consulting clinician or receiving care setting when transitions of care occur18.
Figure 1.
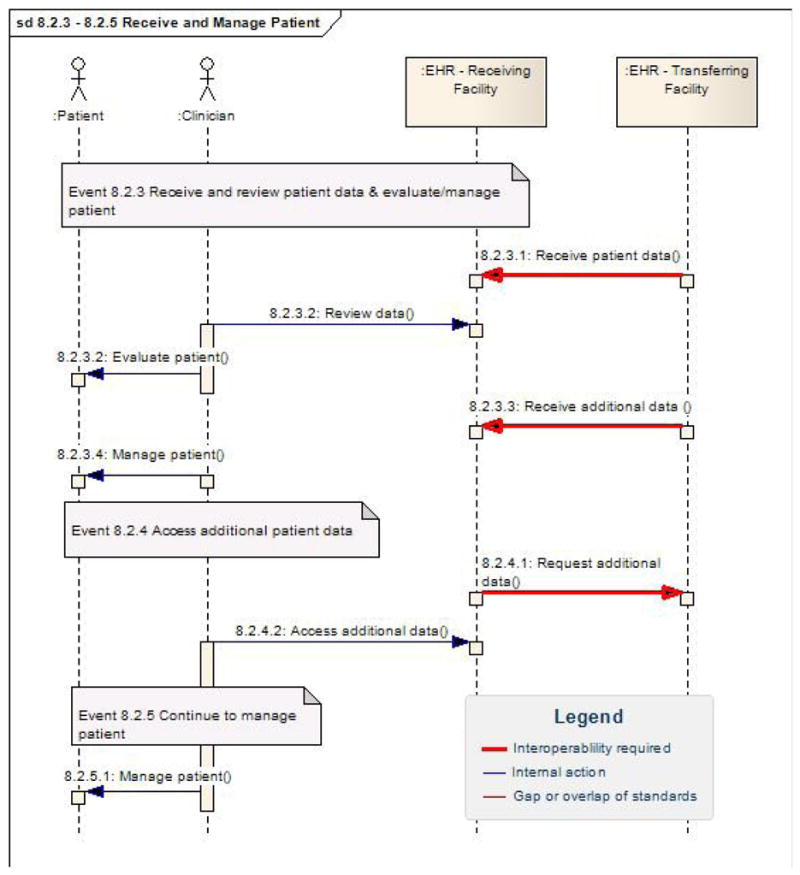
Transfer of Care Interoperability Specification © 2008 ANSI
Measures of IT sophistication developed from early applications in business firms 19, 20. Recently, IT sophistication has been used to describe measures of diversity among technological tools and software used to support patient care, clinical support, and administration in healthcare 12, 21, 22. Three types of sophistication have been defined through these early applications. The types of IT sophistication include: functional sophistication (types of processes or activities that are computerized); technological sophistication (degree in which technology is used in each clinical area); and integration sophistication (level of integration among internal and external departments and clinical settings) 12, 19, 21, 23.
The potential for IT sophistication in nursing home settings is great. IT solutions can assist in the delivery, support, and management of resident care, provides opportunity for interoperable clinical support networks and facilitates administrative oversight1. For instance, nursing homes with high IT sophistication could collect appropriate clinical data about residents with congestive heart failure with edema (vital signs, weight, fluid intake/output, appetite, medications) and be able to transfer the data to all relevant healthcare team members; such as primary care providers to alert for change in condition, dietary and licensed staff to reassess resident, and nurse assistants to monitor water and fluid intake. In contrast, facilities that use paper and pen based applications or checklists would be considered to have a lower level of sophistication in regard to their IT system; hence treatment plans for residents with congestive heart failure with edema may be implemented slower resulting in more negative resident outcomes. Results from this study of nursing home IT sophistication will be used to develop and investigate performance measures between facilities that have varying degrees of functionality, technological instruments and integration. These measures can then be used to benchmark best practices in IT use to guide development, new implementations and quality improvement initiatives among early adopters of information systems in nursing homes.
Methods
Research design
This qualitative study is based on interviews with key stakeholders from four technologically sophisticated nursing homes that self-identified as using significant amounts of IT. In particular, a combination of key informant interviews and focus groups were used to explicate the dimensions of IT sophistication among the three clinical domains. The Computerized Physician Order Entry & IT Infrastructure survey 24, previously used as a measure of IT sophistication in acute care settings, was used in this study to develop a guide for the nursing home interviews and focus groups. Examples of the questions in the guide that was used for focus groups and key informant interviews are included in Table 1. Respondents’ responses from the nursing home interviews and focus groups were then used to adapt the original survey for nursing home facilities.
Table 1.
Examples of Focus Group and Key Informant Interview Guide Questions
|
While the original survey has been rigorously tested and validated in acute care settings12, 21, further analysis of the concepts for the nursing home were required to determine how critical attributes of IT sophistication were different and/or similar in the nursing home setting. All research methods and procedures were approved by the university’s Institutional Review Board.
Sample
Participants were selected from a purposive sample of four nursing homes that had highly sophisticated IT systems. There was not attempt to recruit different homes based upon size, regional location, or proprietary status. Advanced IT sophisticated nursing homes were defined by the investigators as having diverse and integrated clinical information systems incorporating advanced technological devices and software. In the context of this study, a nursing home was considered to have advanced IT sophistication if they had implemented the following: electronic medical record with clinical decision support capabilities, automated alerting mechanisms, wireless electronic data capture, point of care documentation, real time minimum data set functionality, and/or electronic medication administration.
Initial contact with selected nursing homes was completed with the administrator who then facilitated the identification of key IT stakeholders. Recruitment of IT stakeholders focused on those playing leadership and implementation roles vis-à-vis different clinical and administrative information technologies. Participation was voluntary, and included individual interviews, and guided focus groups composed of one to four participants. This method of using multiple nursing homes and key stakeholders in facilities considered to have highly sophisticated IT systems allowed researchers to draw more credible conclusions about the many different dimensions of IT sophistication in the particular nursing homes studied25, 26. They also allowed the authors to acquire an in-depth understanding that would have been available through use of a larger sample.
Data collection
Four key informant interviews and three focus groups were conducted across the four facilities. Key informant interviews were conducted with 1-2 people; focus groups were conducted with 3 or more people. Subjects participated in either a focus group or key informant interview but not both.
A predetermined interview guide was used to help interviewers capture insights into the attitudes, perceptions, and opinions of informants solicited through open-ended questions. The use of the interview guide questions (Table 1) provided a consistent approach to obtaining information from the key informants and focus group participants. Participants were asked to explain how technology was integrated into administrative functions in their facility, describe the extent of use of different technologies in resident management activities, and to share what types of technologies were needed for the nursing home to be considered highly sophisticated.
Both key informant interviews and focus groups were recorded by tape recorder and by field notes taken by a research assistant. During the discussions, pause and probe methods were used to solicit additional information from the participants until saturation of each topic was reached. No identifying information was collected from any participant. A short debriefing session was held following each encounter to capture first impressions and highlight and contrast findings.
Analysis
A transcript based approach was used to analyze field notes. Transcribed tapes were coupled with field notes and debriefing information. The analysis process included identifying phenomenon that emerged and reappeared across all focus groups and interviews. The conclusions extracted from these initial interviews were used to adapt, to nursing homes, the dimensions of IT sophistication across three clinical domains previously used in acute care. An axial coding process 27 was used to fracture and reassemble the data in new ways. A matrix of the attributes was created using overriding common themes found in nursing home IT sophistication (functional, technological, and integration) as one axis and the domains of health care (resident care, clinical support, and administrative activities) as the other axis (see Table 2). This resulted in a total of nine dimensions of IT sophistication in nursing homes.
Table 2.
Dimensions of IT Sophistication in Three Domains of Nursing Home Care
| Attributes of IT Sophistication | Resident Care | Clinical Support | Administrative Activities |
|---|---|---|---|
| Functional | Admissions | Staff scheduling | Tracking IT system issues |
| Discharges | Vital signs recording | IT requests | |
| Transfers | Medication admin. | IT “Help Desk” | |
| Waiting list management | Staff workload mgmt. | Backup Power Source | |
| Bed availability estimation | Physician orders transcription | Biotechnology | |
| Discharge summary | Care planning/RAPS | Resident ID | |
| Order entry | Historical records | Electronic wand | |
| Physician order sheet | Resident acuity | ||
| Progress notes | Quality assurance | ||
| Results reporting | Nursing flowsheet | ||
| Face sheet (abstracts) | Incident reporting | ||
| Real time MDS/RAI | |||
| Clinical reporting | |||
| Label generation | |||
| Specimen archiving | |||
| Recurring tests management | |||
| Technological | Electronic Tracking | PCs at nursing station | Databases |
| Medical records | PCs in the hallway | Networks | |
| Resident ID | PCs on the med cart | Operating Systems | |
| Scanning medical records | PCs at the bedside | Fax machines | |
| Centralized scheduling | Portable computing devices | Fiber optics | |
| Dictation systems | Laptops | Wide area network | |
| Voice recognition systems | Handheld (PDA) | Satellite connections | |
| Connection to external databases | Wireless | Microwave connections | |
| Expert System | Touch screens | Local area network | |
| Telemedicine | Integrated Service Delivery Network (ISDN) | ||
| Access to radiological images | Wireless network | ||
| Modems | |||
| Infrared connections | |||
| Integration | Resident management systems | Electronic and automatic transfer of information between IT systems | Environmental systems in place |
| Admissions | Nursing IT integration | Fire protection systems | |
| Scheduling | Pharmacy | Security access | |
| Resources availability | Dietary | Centralized systems | |
| Laboratory | PT/OT | Disaster recovery plan | |
| Pharmacy | Laboratory | Nursing home website | |
| Human resources | IT Department | External email | |
| Finance | Electronic bulletin boards | ||
| Medical/resident records | Intranet applications | ||
| Extranet applications | |||
| Enterprise Resource Planning | |||
Results
Twelve key IT stakeholders from four nursing homes participated in the three focus groups and four key informant interviews. As noted in Table 3, nursing homes varied in size and profit status. All homes were located in or near Midwestern metropolitan cities in the USA. Two different electronic health record (EHR) systems and numerous software programs were used in the four nursing homes to manage resident care activities, provide clinical support for direct care providers, and conduct administrative activities within each facility.
Table 3.
General Overview of Participating Nursing Home Facilities
| Nursing Home Facility | ||||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| Number of focus groups/participants | 2/4 | 1/4 | 0/0 | 0/0 |
| Number of key informant interviews/participants | 1/1 | 0/0 | 2/2 | 1/1 |
| Title of IT oversight person | Supervisor, IT Dept. | Chief Financial Officer | Owner Administrator | Administrator |
| Number of IT employees | 4 Serves all corporate facilities |
2 |
1 Serves 4-5 related facilities |
0 |
| Bed Size | 240 | 120 | 112 | 132 |
| Ownership | Non Profit Church related | For profit Partnership | For Profit Partnership | Non Profit Corporation |
The interviews provided a rich set of information describing IT applications in real-world nursing home settings that were analyzed within dimensions of IT sophistication previously used in acute care settings 12. Table 2 illustrates how IT sophistication is represented in the four nursing homes across the three domains of healthcare.
Resident Care
Functional sophistication
In resident care, functional sophistication refers to the types of resident care activities that are supported by technological devices (e.g. physician, nursing, dietary, and restorative documentation/reporting). Each of the facilities in this study was considered to have advanced IT sophistication because they had implemented an EHR with decision support capabilities, electronic data capture of clinical information, and other automated features. However, there were differences in the degree of functional sophistication even within this group of highly sophisticated homes. Key IT stakeholders emphasized different components of the EHR systems available for resident care.
The administrator in one facility noted the variety of IT components and uses: including “… nursing documentation, there’s bookkeeping, of course, the Minimum Data Set (MDS) system, our activities, and social service. I haven’t done dietary …”. In contrast, an Assistant Director in charge of education at another facility emphasized the following components of the IT system, “We do our medication administration, and it’s all electronic. All of our physical assessments and all of our risk assessments are done on computer. All nurses notes, physician orders.” He went on to say, “the dietary department, I’m not sure whether she processes her diet orders through the computer or not, but all of our weight management is pulled to run QA [Quality Assurance] reports. Her dietary assessments and nutrition notes are all entered into the system and then are reflected on the record, and the team can pull those up.”
For our purposes, functional sophistication is the degree of diversity supported by technology directed toward the care of residents. An example of this diversity is the use of digital photos in resident care. All but one facility declined to use digital photos for the purposes of documenting wound status. One administrator stated, “No, I haven’t done wounds for a number of years, because you get into a liability situation with the picture, they just blow them up and use them against you in court. We do not take pictures of anything.” The nursing and medical records supervisors from another facility explained, “We maintain a photo album for medication delivery, matching the person receiving the medication with their photo in the album…this can present a problem as people change and sometimes people look alike. We haven’t started taking and storing digital photos for computer storage. We may occasionally keep wound pictures on a computer, but it is not standard practice.” Another nursing home only took pictures of residents’ faces, uploading them into the clinical information system solely for identification purposes.
Technological sophistication
Statements regarding technological sophistication reflect the degree in which technology is used in resident care. An example of increased technological sophistication was discussed by the administrator of the same nursing home noted above, he described a homegrown wireless call light system he developed and added to the facilities technology, “The call light system is attached to the computerized nursing system which has a series of four incremental pages occurring every four minutes to alert staff. The first level pages the aide on the hall; the second level pages exactly the same; the third level pages the medication aide, the float, the regular hall; and the fourth level pages the nurse. Four minutes later it goes to the next level; it pages everybody until it’s answered.” There are added revenues for facilities that have high technological sophistication, the administrator explained, “We sell almost everything that we do with technology. We’re a reseller for the wireless nurse call system.”
Integration sophistication
Integration sophistication represents the level of internal and external connectivity among departments and clinical settings 12. Goals for system integration are to link processes across different applications and ensure that information is kept consistent within systems. Most facilities in this study had higher levels of internal integration, as opposed to external integration. However, a wide range of internal integration was noted among facilities. Three nursing homes appeared to have taken steps to integrate internal charting mechanisms. For example, three nursing homes had integrated electronic charting for nurse assistants, while the other nursing home did not allow nurse assistants access to the EHR.
Internal electronic messaging systems, called task lists, were available and being used by three nursing homes to transmit preformatted messages from nurses to nurse assistants about clinical care to be performed. Use of these systems might increase technological and functional sophistication to support clinical communication; however, the level of integration across the system can fluctuate between facilities. For example, a nursing home using the task lists might provide each user (nurse aide and registered nurse) the capability to post messages to other users accounts indicating a higher level of communication capabilities, thus greater integration. In contrast, another home may only allow registered nurses to post messages to a nurse aide account, with nurse aides only being able to visualize but not manipulate the information displayed resulting in poorer system integration. This example illustrates a different level of integration for the same system between two different facilities.
Clinical Support
Functional sophistication
Functional sophistication in the area of clinical support (e.g. laboratory, pharmacy, and radiology) again varied. Three nursing homes had clinical decision support systems with clinical alerts for potential resident problems such as hydration status and skin integrity. Although these alerts were available in three of the four nursing homes, these alerts were used inconsistently28. For example, one facility had the alerts turned on but ignored them, “We don’t use them [alerts] because we don’t input everybody’s intake. We just have a set group of people [residents] we do intake on.” Another nursing home had the alerts turned on to alert staff of impending resident problems; systems administrators in one facility indicated they used them to make decisions about toileting and nutritional status, and yet other administrators had elected to turn the alerts in the system off. The decision to deactivate the clinical alerts appeared to be related to perceived accuracy and trustworthiness of the alerts29.
Technological sophistication
Technical sophistication relies heavily on external connections and adaptable IT systems. All nursing homes had Internet access; however, in most cases Internet access was limited to management. The exception was one nursing home that allowed Internet access to all staff except nurse assistants via a staff breakroom PC. Few external electronic connections existed in these nursing homes.
There also was little external adaptability with clinical support networks in these highly advanced IT homes. In these homes, interfaces which allow interactions between IT users, creating the ability for users to accept commands and display the results generated by other portions of the computer system were not available with clinical support networks. However, there was some evidence that nursing home administrators were beta testing electronic interfaces with external laboratories to enhance clinical support networks.
Integration sophistication
Another important aspect of achieving a high level of IT integration is the level of available IT staff to support clinical operations. Only one nursing home had an IT department. The IT department provided a 24/7 help desk for clinical staff. The help desk assisted in troubleshooting, upgrading IT systems, and performing general maintenance. The other nursing homes relied heavily on their administrators, who carried pagers to support IT help and maintenance. There were also varying degrees of IT management experience which typically consisted of “on the job” training. One nursing home appeared to have an extremely competent administrator who had compiled significant knowledge of IT systems and networks. He was outsourcing technology he had developed.
As mentioned, all nursing homes had a rudimentary level of integration sophistication with external clinical support entities such as labs, pharmacy and radiology. However, there were some indications that external integration was becoming more developed. For example, one administrator described current beta testing for a lab request and reporting system, “…which would automatically notify the lab when they would have to come and pick up a lab [specimen] at the facility on a monthly basis.” Conversely, the other nursing homes relied on paper based requisitions, fax reports, and telephone communications to facilitate transfer of information from external sources. This is evidence that some clinical support activities were being re-engineered in order to take advantage of what IT can do.
Specific areas of IT support that proved to be helpful for internal IT integration and function included an implementation team to perform upgrades to the clinical information system, to build clinical libraries or knowledge databases, a maintenance staff to fix and track broken equipment, and a centralized point of integration staffed with knowledgeable people who could provide effective troubleshooting and networking.
Administrative Support
Functional sophistication
Functional sophistication is needed to maintain an operable IT system that will perform clinical processes and activities associated with administrative oversight in nursing homes. Specifically, the use of consultants and outsourcing was found to be especially helpful in cases where an IT department didn’t exist. In one nursing home where no IT personnel were employed, the administrator used an intern who was getting a Master’s in information technology to develop the wireless network and user defined assessments. The administrator described how the intern helped develop user defined assessments to enhance reporting capabilities, “the first year we chose the hardware, and then the second year I had them do a lot of work entering user defined assessments. We have a specialized assessment when we put in intake and supplements at meals. So the questions, kind of feedback and kind of answers you get are dependent on how you set up your input and then develop your report.”
There was evidence administrators who were knowledgeable of IT systems were becoming savvier because of types of sophistication analyzed. Some administrators were developing their own technological solutions such as a “bio-time” clock system for quality improvement. For example, IT systems were being used to validate the timeliness of answering call lights, “Using the bio time clock system, [nurse] aids can punch in by putting their finger on it [scanner], it reads their fingerprint, and if it matches, they go on. Our future plan is to take that technology on the time clock system, integrate that with the nurse call system, and know who answered every call light on every call. It can be used as a base to improve services.”
Finally, administrators who are implementing sophisticated technologies want more sophistication. This was evident in comments regarding magnetic scanning devices used for resident identification “ We are hoping for an update to the use of wand which is less intrusive to the resident as it does not require physical touching to scan. This would be especially helpful at night to keep from disturbing the resident.”
Technological sophistication
An important aspect of maintaining technological sophistication for administrative activities is having remote access. All nursing homes had some form of remote access. For example, two nursing homes used an application service provider (ASP) model allowing capital expenditures to be folded into monthly operating fees with individual vendors to support internal IT systems. Other nursing homes used remote access as a function of the nursing home being part of a system that owned/operated the systems centrally. For example, two nursing homes used remote access to assist in troubleshooting network problems, perform training, or evaluate system security with sister facilities. One administrator explained their networking capabilities, “The server is tied in virtually with a private network between all the sites, and then we’re the controller that controls all of that in and out of the Internet. One facility has all the main data as to who can log in and all their other rights and all that…we can pull my documents up at any remote site.” The other two nursing homes used remote access to allow vendors to log onto their network to assist with network problems.
All forms of IT sophistication in terms of administrative activities were observed through the administrators’ daily use. In every nursing home there was technology being used to manage accounting, billing, and payroll, and regulatory functions such as the MDS. There was more technological diversity in applications for supplies management than in other ones. One administrator described the current use of technology for these purposes, “We have a scanning system for supplies, with its own set of palms, which is automatically linked to billing but not purchasing [a supply chain management application]. These supplies are used by individual residents and patients. We do have an inventory maintenance program but are not using it currently, due to warehouse space issues.”
Integration sophistication
Every administrator identified that IT systems were either fiscally or clinically strong in their individual products, however no system had been created with a strong integrated product linking clinical, fiscal, and regulatory needs; creating less integration sophistication for some facilities. This has lead to consistent problems with fiscal and clinical interfaces and the development of separate silo systems to facilitate financial and clinical functions. One administrator explained, “The [clinical program] implemented by our facility doesn’t talk to the [financial program] and that is the biggest weakness. Another major weakness is that the [clinical program] has no financial capabilities. At this time we have to double enter information into both the [financial program] and the [clinical program] systems.” The administrator also indicated that a new version of the clinical program was forthcoming that would create a more effective interface.
Administrative integration is represented by the level of internal and external integration of administrative functions among departments and clinical settings inside and outside a facility. Higher levels of integration were evidenced by improved administrative reporting capabilities across the system. All administrators reported technological enhancements enabled them to manage human resources more effectively, allowed them to perform audits of clinical areas from anywhere within the network, and provided them with critical clinical information to identify high risk residents within the system. One informant described how reporting capabilities have been improved because of the technology,
“…we are utilizing weekly reports for each nursing home unit, [to monitor] antibiotic therapy, residents who have had an incident, new resident admissions, new medication orders, who is Medicare part A and getting therapy. So it really helps to talk about the high risk patients so we can all be on top of the same thing.”
Descriptions of the usefulness of technology portray how computerization in these settings is moving away from a focus on billing applications and MDS completion to more advanced integrated IT systems that enhance administrative oversight.
Discussion
The promises for improved care quality, safety and value for residents are the primary drivers of future investment in IT by nursing homes. Investigators are attempting to understand the types of IT currently being implemented, how IT functions to support clinical processes, and to what extent IT integration has occurred or is possible between various clinical and administrative IT solutions. Administrators implementing sophisticated IT systems are beginning to see how IT can enhance the quality improvement efforts in their facilities. Administrators who are slow to adopt can learn from the experiences of early adopters discussed in this manuscript. While nursing home IT adoption is in early stages, early adopters are beginning to realize benefits across all three clinical domains (resident care, clinical support, and administrative activities). In an effort to understand nursing home IT sophistication, this study explored the concept of IT sophistication across these three domains.
The interviews with early adopters of IT systems in nursing homes provided justification to adapt the original IT sophistication survey used in acute care settings to nursing homes. Following the interviews, modifications were made to the language of the original survey to fit the mold of nursing homes; for example, patients were identified as residents, hospital was replaced with nursing home. Other changes included deleting some sections of the survey instrument that pertained to computerization used in operating rooms and emergency services. This was necessary because these types of services are not located in nursing homes. Additional items were added related to specialized services performed in nursing homes such as minimum data set assessments and resident assessment protocols.
In regards to content and structure, most of the items in the original survey were left intact. This is most likely due to hospitals adopting IT earlier and having more advanced information systems; therefore, much of the original survey was complete with respect to identification of types of systems being used.
The most important thread of information about IT sophistication emerging from these discussions was the need for further interface development between IT systems in order to enhance integration and connectivity. Of critical importance is the need for interfaces that allow different IT applications to communicate with each other in order to build common data repositories and data warehouses. Interface operability was recognized as an important issue in every clinical domain.
Interfaces are important because they allow for the exchange of vital clinical information between internal and external entities. Interfaces contribute to the formation of relational databases that can combine distinct datasets into powerful reporting tools fostering a seamless clinical environment. Additionally, the adaptation of interfaces to connect stand alone IT systems reduces the duplicative work required to keep separate IT systems current. Adaptation of interface links also facilitates a safer environment through more consistent data entry, faster retrieval of information, and improved reliability of data sources.
An important aspect of IT sophistication which is related to interface development is the usability of IT systems. Functional sophistication and integration of clinical decision support can be positively or negatively affected by the users’ perceptions, accuracy of information input into the system, and the specificity of information guiding users’ decisions. Increased levels of IT support and training personnel can improve usability, contribute to the design of sophisticated systems, keep the technology up and running smoothly, and are important for maintaining connections with users of IT.
Limitations
Limitations of this study include the small sample size of respondents interviewed during the focus groups and interviews. Additionally, all of the interviews were conducted in urban or metropolitan regions; therefore, some of the results may not reflect issues that more rurally located nursing homes have implementing sophisticated IT systems. Furthermore, differences in the types of technologies being considered in diverse regional settings may not be reflected in our results and therefore could lessen generalizability to other settings.
Future Work
Several studies are underway using the results of this study including the development of a state profile of IT sophistication for nursing homes in Missouri30, 31. The state profile includes a description of the different types and levels of IT sophistication described in the matrix (see Table 2) in a sample of nursing homes. Additional studies are underway to investigate best practices of IT use in nursing homes with diverse levels of IT sophistication. Specifically, investigators are researching the implementation of recommended evidence based prevention measures for pressure ulcer management in nursing homes with high levels of IT sophistication versus nursing homes with low levels of IT sophistication. In these studies nursing home quality measures pertinent to pressure ulcer residents will be compared to the level of IT sophistication to determine if a relationship exists between these two variables.
Conclusion
The study shows how some early nursing home adopters of more advanced IT applications are achieving added benefit for resident care, clinical support, and administrative functions. These early adopters are anxious for more technological advancements; some are even beginning to develop their own entrepreneurial status as a result of visionary IT leadership. Nursing home IT is beginning to advance beyond business applications and the required minimum data set as illustrated in the matrix. There is a belief among nursing home administrators that IT systems do improve the quality of care given to their residents. However, there is still room for a higher level of IT sophistication as the development of interfaces and more advanced and complex resident care and information technologies change the nature of work.
Acknowledgments
This study was funded by University of Missouri, Research Council Grant URC-O6-039, IT Sophistication in Nursing Homes. PI: Alexander, G.L.
This project was supported by grant K08HS016862 from the Agency for Healthcare Research and Quality (PI: Gregory Alexander). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality, the U.S. Administration on Aging, or the National Science Foundation.
We wish to thank Jill Scott-Cawiezell PhD, RN, FAAN and Professor at the University of Iowa College of Nursing, for her research support and assistance editing this manuscript. We also wish to thank Stephanie Herrick, Research Associate, University of Missouri, Sinclair School of Nursing for her tireless assistance with data management and transcription services.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Gregory L. Alexander, Assistant Professor, University of Missouri, Sinclair School of Nursing.
Douglas S. Wakefield, Professor, Director, Center for Health Care Quality, University of Missouri.
Reference List
- 1.Committee on Data Standards for Patient Safety. Key capabilities of an electronic heatlh record system. Washington DC: Institute of Medicine National Academies Press; 2003. [PubMed] [Google Scholar]
- 2.Martin RD, Brantley D, Dangler D. Report to the National Commission for Quality Long Term Care Essential but not sufficient: Information Technology in Long Term Care as an enabler of consumer independence and quality improvement. McLean VA: BearingPoint Inc. Management & Technology Consultants; 2007. Sep, 24, [Google Scholar]
- 3.Ferris N. Long-term care lags in health IT. Government health IT: A guide to public policy and its applications in health IT. Retrieved from http://govhealthitcom/article90387-08-24-05-Web 2005;Available at: URL: http://govhealthit.com/article90387-08-24-05-Web.
- 4.Abbott PA, Brocht D. Challenges for Data Management in Long-Term Care. In: Saba VK, McCormick KA, editors. Essentials of Computers for Nurses. 3. New York: McGraw-Hill; 2001. pp. 357–64. [Google Scholar]
- 5.Ossip-Klein DJ, Karuza J, Tweet A, et al. Benchmarking implementation of a computerized system for long term care. American Journal of Medical Quality. 2002;17(3):94–102. doi: 10.1177/106286060201700304. [DOI] [PubMed] [Google Scholar]
- 6.Martin RD, Brantley D, Dangler D. Report to the National Commission for Quality Long Term Care Essential but not sufficient: Information Technology in Long Term Care as an enabler of consumer independence and quality improvement. McLean VA: BearingPoint Inc. Management & Technology Consultants; 2007. Sep 24, [Google Scholar]
- 7.Pulliam L, Valentine J, Raymond J, Racine D. Implementation of a computerized information system in a longterm care facility. Computers in Nursing. 1992;10(5):201–7. [PubMed] [Google Scholar]
- 8.Alexander GL. Issues of trust and ethics in computerized clinical decision support systems. Nursing Administration Quarterly. 2005 doi: 10.1097/00006216-200601000-00005. In press. [DOI] [PubMed] [Google Scholar]
- 9.Scott-Cawiezell J, Vogelsmeier A. Nursing home safety: A review of the literature. In: Fitzpatrick JJ, Stone PW, Walker PH, editors. Annual Review of Nursing Research. Vol. 24. NY: Springer Publishing; 2005. [PubMed] [Google Scholar]
- 10.Rantz MJ, Connolly RP. Measuring nursing care quality and using large data sets in nonacute care settings: state of the science. Nursing Outlook. 2004;52(1):23–37. doi: 10.1016/j.outlook.2003.11.002. [DOI] [PubMed] [Google Scholar]
- 11.Vogelsmeier A, Scott-Cawiezell J, Zellmer D. Barriers to safe medication administration in the nursing home. Journal of Gerontological Nursing. 2006 doi: 10.3928/00989134-20070401-02. In press. [DOI] [PubMed] [Google Scholar]
- 12.Pare G, Sicotte C. Information technology sophistication in health care: An instrument validation study among Canadian hospitals. International Journal of Medical Informatics. 2001;63:205–23. doi: 10.1016/s1386-5056(01)00178-2. [DOI] [PubMed] [Google Scholar]
- 13.Breslin S, Greskovich W, Turisco F. Wireless technology improves nursing workflow and communications. CIN: Computers, Informatics, Nursing. 2004;22(5):275–81. doi: 10.1097/00024665-200409000-00007. [DOI] [PubMed] [Google Scholar]
- 14.Nolan RL. Managing the computer resource: A stage hypothesis. Communications of the ACM. 1973;16(7):399–405. [Google Scholar]
- 15.ten Hoopen AJ, van der Maas AAF, Helder JC. Modeling of health care for information system development. In: van Bemmel JH, Musen MA, editors. Handbook of Medical Informatics. Bohn: Springer; 1997. pp. 309–30. [Google Scholar]
- 16.HITSP Provider Perspective Technical Committee. HITSP Consultations and Transfers of Care Interoperability Specification. Washington Publishing Company; 2008. Sep 26, Report No.: Version 0.0.1. [Google Scholar]
- 17.Jablonski RA, Utz SW, Steeves R, Gray PD. Decisions about transfer from nursing home to emergency department. Journal of Nursing Scholarship. 2008;39(3):266–72. doi: 10.1111/j.1547-5069.2007.00179.x. [DOI] [PubMed] [Google Scholar]
- 18.American National Standards Institute. [AccessedOctober 16, 2008];HITSP Enabling Healthcare Interoperability. http://wwwhitsporg/ 2008;Available at: URL: http://www.hitsp.org/
- 19.Cheney PH, Dickson GW. Organizational characteristics and information systems: An exploratory investigation. Academy of Management Journal. 1982;25(1):170–84. [Google Scholar]
- 20.Raymond L, Pare G. Measurement of IT sophistication in small manufacturing businesses. Journal of Information Resources Management. 1992;5(2):4–16. [Google Scholar]
- 21.Jaana M, Ward MM, Pare G, Wakefield DS. Clinical information technology in hospitals: A comparison between the state of Iowa and two provinces in Canada. International Journal of Medical Informatics. 2005;74:719–31. doi: 10.1016/j.ijmedinf.2005.05.009. [DOI] [PubMed] [Google Scholar]
- 22.Culler S, Atherly A, Walczak S, et al. Urban-Rural Differences in the availability of hospital information technology applications: A survey of Georgia hospitals. Journal of Rural Health. 2006;22(3):242–7. doi: 10.1111/j.1748-0361.2006.00039.x. [DOI] [PubMed] [Google Scholar]
- 23.Jaana M, Ward MM, Pare G, Sicotte C. Antecedents of clinical information technology sophistication in hospitals. Health Care Management Review. 2006;31(4):289–99. doi: 10.1097/00004010-200610000-00004. [DOI] [PubMed] [Google Scholar]
- 24.Ohsfeldt R, Ward M, Schneider J, et al. Implementation of hospitalized computerized physician order entry systems in a rural state: Feasibility and financial impact. Journal of the American Medical Informatics Association. 2005;12(1) doi: 10.1197/jamia.M1553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park, CA: Sage; 1985. [Google Scholar]
- 26.Polit DF, Hungler BP. Nursing Research: Principles and Methods. 6. Philadelphia: Lippincott; 1995. Assessing data quality; pp. 407–36. [Google Scholar]
- 27.Krueger RA. Focus Groups: A Practical Guide for Applied Research. 2. Thousand Oaks, CA: Sage; 1994. [Google Scholar]
- 28.Alexander GL. An analysis of an integrated clinical decision support system in nursing home clinical information systems. Journal of Gerontological Nursing. 2007 doi: 10.3928/00989134-20080201-01. In press. [DOI] [PubMed] [Google Scholar]
- 29.Alexander GL, Rantz MJ, Flesner M, Diekemper M, Siem C. Clinical Information Systems in Nursing Homes: An Evaluation of Initial Implementation Strategies. Computers Informatics Nursing. 2007;25(4):189–97. doi: 10.1097/01.NCN.0000280589.28067.18. [DOI] [PubMed] [Google Scholar]
- 30.Alexander GL, Madsen D, Herrick S, Russell B. Measuring IT sophistication in nursing homes. Rockville Maryland: AHRQ; 2008. Report No.: AHRQ Publication No. 08-0034-CD. [PubMed] [Google Scholar]
- 31.Alexander GL. A state profile of IT sophistication in nursing homes. Washington DC: American Medical Informatics Association; 2008. [PMC free article] [PubMed] [Google Scholar]