

Abstract
An adaptation of the Family Stress Model (FSM) with hypothesized linkages between family contextual factors, custodial grandmothers' psychological distress, parenting practices, and grandchildren's adjustment was tested with structural equation modeling. Interview data from 733 custodial grandmothers of grandchildren between ages 4-17 revealed that the effect of grandmothers' distress on grandchildren's adjustment was mediated by dysfunctional parenting, especially regarding externalizing problems. The effects of contextual factors on grandchildren's adjustment were also indirect. The model's measurement and structural components were largely invariant across grandmothers' race and age, as well as grandchildren's gender and age. Group differences were more prevalent regarding the magnitude of latent means for model constructs. We conclude that parenting models like the FSM are useful for investigating custodial grandfamilies.
Introduction
Grandparents are increasingly serving as surrogate parents to grandchildren on a long-term basis. There were over 2.4 million “grandparent caregivers” in the United States with primary responsibility for a co-resident grandchild under age 18 in 2000, and 39% were in this role 5 or more years (Simmons & Dye, 2003). This study focuses on the 34% of these caregivers, known as “custodial” grandparents, who live with a grandchild in absence of the child's parents. Although psychological distress among custodial grandmothers (Minkler, Fuller-Thomson, Miller, & Driver, 1997; Strawbridge, Wallhagen, Shema, & Kaplan, 1997; Szinovacz, DeViney, & Atkinson, 1999) and adjustment problems in their grandchildren (Smith & Palmieri, 2007) are common, research is scant on links between grandmothers' mental health and grandchildren's well-being. Yet, as Daly and Glenwick (2000) note, “a grandmother's adjustment difficulties could influence the way in which she interacts with her grandchild, which, in turn, might contribute to the development and maintenance of her grandchild's behavior problem” (p. 116).
Models of family stress and resilience typically maintain that stressors either cause, sustain, or amplify mental health difficulties in family members (Kwok, Haine, Sandler, Ayers, Wolchik, & Tein, 2005; Webster-Stratton, 1990). McLoyd (1990) reviewed abundant research showing that family stress in the form of socioeconomic hardship heightens anxiety, depression, and irritability within parents, and that such distress increases the “tendency of parents to be punitive, erratic, unilateral, and generally nonsupportive of their children” (p. 330). In turn, this type of dysfunctional parenting is widely viewed as an antecedent of adjustment difficulties in children of all ages (Goodman & Gotlib, 1999; Johnson & Mash, 2001; Rothbaum & Weisz, 1994; Smith, Sprengelmeyer, & Moore, 2004).
Specific causal links between socioeconomic stressors, parental psychological distress, dysfunctional parenting, and children's outcomes are well delineated in the Family Stress Model (FSM) (Conger, Rueter, & Conger, 2000; Conger, Wallace, Sun, Simons, McLoyd, & Brody, 2002). First, the stress associated with socioeconomic hardship increases the depressed mood of primary and secondary caregivers alike. This heightened negative affect in caregivers then diminishes parental warmth and involvement directly, as well as indirectly by disrupting the relationship between the child's caregivers. The final causal sequence is that diminished parenting increases the child's adjustment problems. Thus, a major assumption is that dysfunctional parenting mediates relationships between all prior constructs in the FSM and children's outcomes (Conger et al., 2002).
The FSM is germane to custodial grandfamilies for two main reasons. First, these families often face the types of socioeconomic hardship emphasized by the FSM. Custodial grandchildren are more likely than children at-large to be poor, without health insurance, and in households on public assistance (Bryson & Casper, 1999). Caregiving grandparents in one national sample had significantly lower mean and median incomes than non-caregiving grandparents and were 60% more likely to have incomes below the poverty line (Fuller-Thomson, Minkler, & Driver, 1997). New financial strains may also emerge as grandparents assume child-rearing costs, curtail employment, or exhaust personal savings.
Second, there is compelling evidence that custodial grandparenting yields new stressors that add to psychological distress in an already vulnerable population (Minkler et al., 1997; Strawbridge et al., 1997; Szinovacz et al., 1999). In addition, custodial grandchildren are predisposed to psychological troubles due to their birth parents' difficulties. Such predispositions may stem from prenatal impacts (e.g., drug addiction, fetal alcohol syndrome, HIV/AIDS), and from the emotional trauma of abuse and neglect (Hayslip, Shore, Henderson, & Lambert, 1998). In turn, diminished parenting among custodial grandparents caused by stressful circumstances can become a risk factor that interacts with a grandchild's predispositions to facilitate, maintain, or exacerbate adjustment difficulties (Johnson & Mash, 2001).
Despite the possibility that psychological problems of custodial grandchildren may be exacerbated or maintained by diminished parenting due to the caregiver's distress, scant research exists on the parenting practices of custodial grandparents. A rare exception is a study by Rodgers-Farmer (1999) who found that parenting stress among custodial grandmothers was significantly related to their depression, and that higher depression was associated with greater use of inconsistent discipline. Although Rodgers-Farmer (1999) concluded that custodial grandmothers' depression mediates the relationship between stress and dysfunctional parenting, as would be predicted by the FSM, she did not examine if these constructs were related to grandchildren's adjustment.
We shed new light on these issues by testing an adaptation of the FSM that hypothesizes key linkages between family stressors, custodial grandmothers' psychological distress, parenting practices, and grandchildren's adjustment problems (Figure 1). Although the FSM has been verified across diverse family contexts (Conger, Ge, Elder, Lorenz, & Simons, 1994; Conger et al., 2002; Forgath, Patterson, & Ray, 1995; Kwok et al., 2005; Mistry, Vandewater, Huston, & McLoyd, 2002), our study is the first to examine its relevance to custodial grandfamilies.
Figure 1.
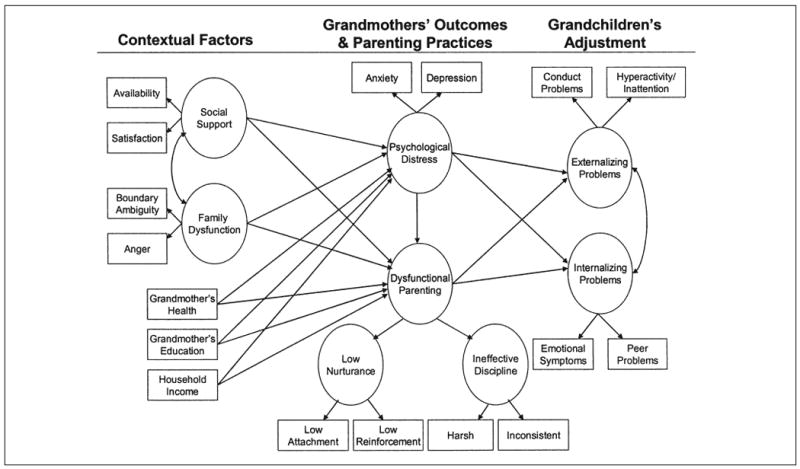
Expanded version of the Family Stress Model as applied to custodial grandfamilies.
Our model differs from the original FSM in three important ways. First, we expand the range of family contextual factors presumed to have indirect effects on children's adjustment beyond a core focus on socioeconomic concerns. Not only is our approach consistent with the view that the influence of diverse family-related contextual factors on children's outcomes is mediated by parenting practices (Cummings & Davies, 1994; Smith et al., 2004), it also provides a fuller account of contextual influences faced by custodial grandfamilies. Thus, in addition to the socioeconomic influences of income and education (McLoyd, 1990), we recognize grandmothers' physical health as a relevant variable in light of past evidence that custodial grandparents are a high health risk population (Musil & Amhad, 2002). Based on prior aging research (George, 1995), we hypothesize that better health will have an inverse effect on grandmothers'psychological distress. In view of concerns that the physical challenges and health problems experienced by custodial grandmothers may compromise their ability to parent effectively (Solomon & Marx, 1999), we further hypothesize that grandmothers in better health will report less dysfunctional parenting.
Family dysfunction is another stressor in our adapted version of the FSM that is widely found in the parenting literature to exert adverse indirect effects on children's adjustment (Campbell, 1995). We contend that custodial grandfamilies are especially prone to family dysfunction in the form of boundary ambiguity and grandparent's anger toward the grandchild's birth parent. These caregivers must negotiate boundaries across three generations, while often feeling animosity toward an offspring whose possibly irresponsible behavior has forced them to care for a needy grandchild (Bartram, 1996). Because there is neither a distinct absence or presence of the child's parent, boundaries regarding family roles, norms, and the allocation of family resources are ambiguous and anger toward that parent escalates (Brown-Standridge & Floyd, 2000; Hirshorn, Van Meter, & Brown, 2000). We hypothesize that family dysfunction of this sort will affect dysfunctional parenting both directly and indirectly by increasing custodial grandmother's psychological distress.
Social support is a final contextual factor in our model. Surprisingly, this construct was not in the original FSM even though abundant research has shown social support to have a direct positive effect on the psychological well-being of parents, and to mediate the effect of stressful life situations on parenting behaviors (Conley, Caldwell, Flynn, Dupre, & Rudolph, 2004; Rubin & Burgess, 2002). Given past studies where perceived support from others was related inversely to custodial grandparents' stress (Musil & Amhad, 2002; Sands & Goldberg-Glen, 2000), we hypothesize that social support will lessen dysfunctional parenting both directly and indirectly by reducing grandmother's distress.
A second major difference between our model and the original FSM is that our definitions for both caregivers' psychological distress and grandchildren's adjustment are dissimilar to those traditionally used in SEM studies of the FSM. Rather than conceptualizing psychological distress in terms of depressed mood alone, we define this construct to encompass both depression and anxiety. This is consistent with the consensus that negative affectivity in general rather than depression per se leads to dysfunctional parenting (Conley et al., 2004; Lovejoy, Graczyk, O'Hare, & Neuman, 2000). Our model is also unique in postulating grandchildren's internalizing and externalizing disorders as distinct, yet related, indices of children's adjustment. This distinction is meaningful given that children of distressed caregivers are at risk for diverse adjustment problems, including both internalizing and externalizing problems (Cummings & Davies, 1994; Rubin & Burgess, 2002).
A third major way in which the two models differ is that we propose a more complex delineation of dysfunctional parenting in our SEM analyses than has occurred in past research on the FSM (e.g., Conger et al., 2002). Instead of conceptualizing dysfunctional parenting as a first-order latent construct assessed by multiple indicators (e.g., harshness, lack of warmth, poor child management), we model this construct as a higher-order factor encompassing two first-order factors labeled ineffective discipline and low nurturance. This approach is consistent with the widespread view that ineffective discipline and low nurturance are distinct, yet highly correlated constructs, which comprise the most influential parenting mechanisms known to affect the development of adjustment problems in children (Cummings & Davies, 1994; Locke & Prinz, 2002; Lovejoy et al., 2000; Rubin & Burgess, 2002). Although it has been argued that highly correlated constructs may be combined meaningfully into a composite measure of parenting practice (Rothbaum & Weisz, 1994; Rubin & Burgess, 2002), recent findings suggest that ineffective discipline and low parental nurturance can exert differential effects on children's adjustment (Pfiffner, McBurnett, Rathouz, & Judice, 2005). Thus, an additional aim is to examine both the measurement and structural aspects of the proposed higher-order dysfunctional parenting construct.
Another key contribution of our study is that we examine if the measurement model, the structural model, and the latent means of key model constructs are invariant by grandmothers' race and age and by grandchildren's age and gender. Determining if the measurement model is invariant across these groupings is important because if factor loadings for model constructs differ by group, then the inferred meanings of those constructs may also differ. Moreover, even if the measurement model is equivalent between groups, it is possible that group invariance does not exist in terms of the structural model (i.e., pathways connecting the latent constructs may differ across groups). Finally, even if both the measurement and structural models are equivalent across groups, one or more groups might differ on the latent means of the model's key constructs (Byrne, 2006).
Given the dearth of past research on the parenting practices of custodial grandparents, we frame these group comparisons as research questions rather than as specific hypotheses. This absence of hypotheses is further justified by the inconsistent evidence and competing hypotheses found in the parenting literature with respect to the potential moderating effects of race, gender, and age. For example, two opposing views exist regarding race as a potential moderator (Rowe, Vasonyi, & Flannery, 1994). The no group differences hypothesis holds that culturally specific environmental factors do not alter associations among developmental variables because most families in a society are exposed to developmental processes that transcend all groups. Nevertheless, this hypothesis acknowledges that main effect differences between racial or ethnic groups are possible. In contrast, the group differences hypothesis is synonymous with culturally relative models of socialization and thus assumes that correlations among variables do differ between racial and ethnic groups.
Competing hypotheses similarly exist with respect to the possible moderating effects of the grandchild's age on the association between parenting and child outcomes. Whereas one view predicts greater effects for young children when there are fewer competing socialization influences (e.g., teachers, peers), the alternative view predicts greater effects for older children due to cumulative reciprocal influences that increase dyadic dysfunction over time (see Lovejoy et al., 2000; Rothbaum & Weisz, 1994). To date, however, the extent to which family stressors and parenting practices influence the development and maintenance of adjustment problems in children of different ages is largely unknown (Cummings & Davies, 1994; Rubin & Burgess, 2002). The role of children's gender as a potential moderator in models like the FSM is also unknown (Cummings & Davies, 1994; Rubin & Burgess, 2002). Finally, although one might suspect custodial grandmothers'age to be an important moderator in the proposed model, the scarcity of research on the parenting behaviors of these caregivers precludes any specific hypotheses.
Methods
Participants
The participants were 733 custodial grandmothers (M age = 56 years, SD = 8.1) who had provided full-time care to a grandchild in absence of the child's parents for at least 3 months (M = 6.4 years, SD = 4.0, range = 3 months to 16 years). Grandmothers were recruited across the 48 contiguous states for an NIMH-funded study of stress and coping among custodial grandparents through a combination of convenience (e.g., social service agencies, Internet, radio, and newspaper ads) and population-based methods. Population-based sampling involved recruitment letters sent to randomly generated lists of, purchased from Survey Sampling, Inc., of the approximately 38 million households containing children under age 18.
Quota sampling was used to obtain a sample of grandmothers that was half Black and half White. The purchased population-based lists varied in terms of racial density within geographical areas and attempts were made in convenience sampling to focus on sources with high concentration and appeal to Black families. Blacks were over sampled because the probability of custodial care is much higher for Black families than for Whites (Bryson & Casper, 1999). Grandmothers' self-reported race was chosen as the analytical variable because all measures of constructs in the proposed model were obtained directly from them. Thus, any potential racial differences observed in the present study may be ascribed to grandmothers. Other racial and ethnic populations were not sampled because they comprise a much smaller percentage of the population of custodial grandparents than do non-Hispanic Whites and Blacks (Bryson & Casper, 1999). Otherwise, the sample was diverse in terms of marital status, education, residential locale, work status, and income. Grandmothers were excluded if they were providing care due to the death of their own child. Key demographic information regarding the sample, including reasons for providing care, is shown in Table 1.
Table 1.
Descriptive Demographic Statistics of Grandmothers and Target Grandchildren (N = 733)
| Variable | n | % | Variable | n | % |
|---|---|---|---|---|---|
| Marital Status | Target Grandchild Age | ||||
| Married | 352 | 48.0 | 4-7 years | 235 | 32.1 |
| Divorced | 159 | 21.7 | 8-10 years | 194 | 26.5 |
| Widowed | 102 | 13.9 | 11-14 years | 206 | 28.1 |
| Single, never married | 66 | 9.0 | 15-17 years | 98 | 13.4 |
| Separated | 49 | 6.7 | |||
| Living with partner (not married) | 5 | 0.7 | Formal Legal Arrangements | ||
| Formal custody | 271 | 37.0 | |||
| Education | Foster parent status | 16 | 2.2 | ||
| Less than 5 years | 5 | 0.7 | Adoption | 90 | 12.3 |
| 5-8 years | 19 | 2.6 | Guardianship | 215 | 29.3 |
| Some high school | 99 | 13.5 | Currently seeking legal custody | 69 | 9.4 |
| High school graduate | 205 | 28.0 | None | 72 | 9.8 |
| Some college | 260 | 35.5 | |||
| College graduate | 95 | 13.0 | Relationship of Target Grandchild's | ||
| Graduate/professional training | 50 | 6.8 | Parent to Grandmother | ||
| Son | 227 | 31.0 | |||
| Residential Locale | Step-son | 7 | 1.0 | ||
| Urban | 350 | 47.7 | Daughter | 482 | 65.8 |
| Rural | 238 | 32.5 | Step-daughter | 16 | 2.2 |
| Suburban | 141 | 19.2 | Missing data | 1 | 0.1 |
| Other | 4 | 0.5 | |||
| Work Status | Reasons for Careb | ||||
| Not working | 202 | 27.6 | Child abandonment | 205 | 28.0 |
| Retired | 144 | 19.6 | Physical or emotional abuse | 201 | 27.4 |
| Working full- or part-time | 329 | 44.9 | Removed from parental custody | 225 | 30.7 |
| Full-time homemaker | 41 | 5.6 | Parents' mental health problems | 218 | 29.7 |
| Seeking employment | 17 | 2.3 | Parents' teen pregnancy | 133 | 18.1 |
| Parental substance abuse | 406 | 55.4 | |||
| lncomea | Parents' incarceration | 312 | 42.6 | ||
| Under 10,000 | 123 | 16.8 | Parents' HIV-AIDS | 11 | 1.5 |
| $10,000-$15,000 | 109 | 14.9 | Other (not AIDS) health problems | 114 | 15.6 |
| $16,000-$20,000 | 85 | 11.6 | One of the parents deceased | 47 | 6.4 |
| $21,000-$25,000 | 90 | 12.3 | |||
| $26,000-$35,000 | 112 | 15.3 | |||
| $36,000-$50,000 | 99 | 13.5 | |||
| $51,000-$75.000 | 59 | 8.0 | |||
| $76,000-$100,000 | 19 | 2.6 | |||
| $101,000-$125,000 | 4 | 0.7 | |||
| More than $125,000 | 5 | 0.7 | |||
| Missinga | 28 | 3.8 |
Missing data were less than 10% and mean substitution was used for imputation in the data analyses.
Respondents were asked to report any and all reasons for assuming care of the target grandchild that applied to their situation. Grandmothers were excluded if the deceased parent was their own child.
If a grandmother was caring for multiple grandchildren, then a target grandchild (TG) was selected using the most recent birthday technique. The TG were 391 girls and 342 boys (M age = 9.8 years, SD = 3.7, Range = 4 to 17 years). The majority of grandmothers (65.8%) provided care to a TG who was born to a daughter. Most reported multiple reasons for providing full-time care to the target grandchild, and the majority of reasons concerned crisis or tragedy within the parent generation (e.g., parental substance abuse: 55.4%; parental incarceration: 42.6%). For the multigroup comparisons involving grandchildren's age, the age groupings of 4-7, 8-11, and 12-17 were selected. These groupings respectively correspond to early childhood, middle childhood, and adolescence.
Measures
Grandmothers completed the following self-report measures as part of a comprehensive telephone interview conducted by professionally trained interviewers at a public research university in Ohio.
Grandchildren's Adjustment
Four subscales from the parent-informant version of the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 2001) were used. The SDQ has shown good psychometric properties in diverse populations and correlates highly with other indices of childhood maladjustment (Goodman, 2001). Externalizing problems were assessed by the Hyperactivity-Inattention (α = .82) and Conduct Problems (α = .74) scales, while Internalizing problems were assessed by the Emotional Symptoms (α = .73) and Peer Problems (α = .62) scales. Each scale contained five items that were rated by grandmothers regarding the target grandchild's behavior on a 3-point scale from 0 (not true) to 2 (certainly true). Scores for each scale were computed by summing items on that scale for a potential range of 0-10, with higher scores indicating greater levels of the measured behavior.
Psychological Distress
This construct encompassed self-reported indicators of depression and anxiety. Depression was assessed by the Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff, 1977), a 20-item measure of depressive symptoms. For each item, participants endorsed the response that best described how often they had felt a particular way in the past week on a 4-point Likert-type scale from 0 (rarely or none of the time—less than 1 day) to 3 (most or all of the time—5 to 7 days). Potential CES-D scores ranged from 0 to 60, (α = .90). Anxiety was assessed by the three-item anxiety scale from the Mental Health Inventory II (Stewart, Ware, Sherbourne, & Wells, 1992). Respondents rated how often during the past month they had been either very nervous, tense, or restless from 1 (all of the time) to 6 (none of the time). A total score was computed by averaging the three items, with a possible range of 1 to 6. Higher scores indicated greater anxiety (α = .84).
Low Nurturance
Two subscales from the Parenting Stress Index (Abidin, 1995) were indicators of the low nurturance construct. The Reinforces Parent scale contains six items measuring the extent to which a caregiver projects negative responses onto the child. The Attachment scale contains seven items assessing the caregiver's emotional closeness to the child and the real or perceived inability to observe and understand the child's needs and feelings. Items on both scales are rated from 5 (strongly disagree) to 1 (strongly agree) with several items reverse-scored so that the higher the summed score, the more problematic the parent-child relationship. The potential range of scores and Cronbach's alphas, respectively, were 6-29 and .69 for Reinforces Parent and 7-35 and .60 for Attachment.
Ineffective Discipline
Scales measuring grandmothers'use of harsh and inconsistent discipline, respectively, served as indicators of the ineffective discipline construct. Each scale contained three items adapted from the Parenting Practices Interview (PPI). The latter was derived from the Oregon Social Learning Center's discipline questionnaire by Webster-Stratton, Reid, and Hammond (2001). Grandmothers rated each item (e.g., “Raise your voice, scold, or yell,” “Threaten to punish your grandchild but not really punish him/her”) on a 5-point Likert-type scale ranging from 1 (never) to 5 (very often) in response to the query “In general, how often do you do each of the following when your grandchild misbehaves?” Items were summed to yield scores for each type of discipline (possible range = 3-15), with higher scores indicating greater use. Alphas were low (.66 for harsh; .54 for inconsistent).
Social Support
This construct was measured in terms of both perceived availability and satisfaction with support from friends and family. Availability was assessed by the eight-item Expressive Support Scale (Pearlin, Mullan, Semple, & Skaff, 1990). Each item was rated from 1 (strongly disagree) to 5 (strongly agree), with potential scores ranging from 8-40 (α = .89). Satisfaction was measured by one item developed for this study: “Overall, how satisfied are you with the emotional support and understanding that you receive from your friends and neighbors?” that was rated from 0 (not at all satisfied) to 5 (extremely satisfied).
Family Dysfunction
This construct was assessed by two scales developed specifically for this research that were pilot tested with a sample of 44 custodial grandparents. Boundary Ambiguity was measured by a four-item adaptation of an 11-item instrument used by Caron, Boss, and Mortimer (1999) to measure this construct in dementia caregivers. Each item was rated in regards to the target grandchild's absent parent (e.g., “There is confusion in my family right now about who should be playing what roles”) from 4 (strongly agree) to 1 (strongly disagree). Potential scores range from 4-16 (α = .71). Anger toward the grandchild's birth parent was assessed by five items (e.g., “I feel angry about the way________has behaved as a parent”) rated from 4 (strongly agree) to 1 (strongly disagree). Potential scores range from 5-20 (α = .88).
Contextual Demographic Variables
Household income was measured by asking grandmothers “What is your approximate total yearly household income after taxes?” Response alternatives ranged from 1 (under $10,000) to 10 (more than $125,000). Education was self-reported by grandmothers with response alternatives ranging from 1 (less than 5 years of school) to 7 (graduate/professional training). Grandmother's health was assessed by a single item that was self-rated from 1 (poor) to 5 (excellent).
Although some of the measures described above were found to have low alphas, all had reliability estimates that exceeded .50 which is considered acceptable for group comparisons and correlational analyses (Stewart et al., 1992). Also, the use of SEM corrected for measurement error (Byrne, 2006).
Analytic Plan
We followed Byrne's (2006) recommended procedures for examining multi-group invariance using EQS 6.0 software. Baseline models were first established separately for each group to identify the best fitting model in terms of both parsimony and substantive meaningfulness. The robust maximum likelihood (ML) procedure was used because it provides standard model fit indices as well as statistics adjusting for non-normality via the Satorra-Bentler (S-B) correction (Curran, West, & Finch, 1996). This correction is critical because unadjusted non-normality can contribute to distorted factor analytic results, and non-normality is typical of mental health measures like those used in this study.
After determining the baseline model separately for each group, we then tested for group invariance in a logically ordered and increasingly restrictive sequence (Byrne, 2006). We first tested for configural invariance of the model across each grouping under investigation. In these tests, the same parameters estimated in the baseline model for each group separately were estimated again within a multigroup representation of the baseline model. The fit of the resulting configural models provided the baseline values against which subsequently specified invariance models were compared.
Next, group invariance of the measurement model was tested by computing model fit for a pooled sample of groups (e.g., Whites and Blacks) with the hypothesized factor loadings for all latent constructs constrained to be equal across groups. Fit indices from the fully constrained measurement model were then compared to those of the configural model, and a nonsignificant difference in the Satorra-Bentler chi-square values was indicative of invariance. If the resulting was significant, the Lagrange Multiplier (LM) test was used to identify which factor loadings differed significantly between groups and equality constraints were then released for the identified parameters.
To test for structural invariance, we used a procedure that was analogous to that used to examine measurement invariance. With all of the same constraints that were imposed in the final model of the test for measurement invariance left in place, all hypothesized causal paths (Figure 1) were then constrained to be equal across groups. A difference test was then computed and interpreted in the same manner as for the tests of measurement invariance.
The approach used to test for group invariance regarding the latent factor means involved several steps. First, all constraints that were imposed in the final model of the test for structural invariance were left in place. Then, additional tests for the equivalence of intercepts and latent factor means were conducted following the procedures described by Byrne (2006). One group within each comparison was selected as the reference group and its latent mean parameter was fixed to zero, while those for other groups were estimated, thereby indicating the group difference in latent means. Because models containing higher-order factors are generally not identified, we followed Byrne's (2006) strategy whereby the two latent factor intercepts associated with the second-order dysfunctional parenting construct were fixed to zero for all groups within each multi-group comparison conducted. As such, it was hypothesized that the single second-order factor mean was sufficient to account for mean differences across all indicators of the ineffective discipline and low nurturance single-order factors and that the latent means of these two factors would be approximately equal in magnitude. The resulting fit indices were examined and LM tests were used to identify indicators whose intercepts were not invariant. If any intercepts were not invariant, their equality constraints were then relaxed and the model was re-fit. Finally, standardized effect sizes were calculated by dividing the relevant factor intercept value by the standard deviation of the pooled variance estimate for each group contrast.
Results
Because 52.8% of the sample was recruited through convenience, we first explored if both the measurement and structural aspects of the proposed model were invariant by recruitment method. Data (available upon request) from both the convenience and population-based samples fit the baseline model extremely well, and subsequent analyses revealed complete measurement and structural invariance.
Test of Baseline Model for Each Group
Indices of model fit suggested that data from all groups under investigation fit the baseline model well. The range of values for the indices across all groups were: Comparative Fit Index (CFI) = .95-.99; Root Mean Square Error of Approximation (RMSEA) = .020-.045; Standardized Root Mean Square Residual (SRMR) = .032-.050; S-B χ2(94 df) = 108.02-158.76, p = .15-.00003. No alterations to the baseline model were indicated by the ML tests for any groups under investigation.
Tests of Measurement Invariance
Full measurement invariance was found for each group comparison. The corresponding fit indices for the configural model, fit indices for the constrained measurement model, and corrected chi square difference tests for each respective group comparison are as follows: Grandchildren's Gender configural model (CFI = .98; RMSEA = .023; SRMR = .037; S-B χ2(188) = 263.72, p = .0002), constrained model (CFI = .98; RMSEA = .023; SRMR = .038; S-B χ2(196) = 274.46, p = .0002), and , p = .22); Grandchildren's Age configural model (CFI = .96; RMSEA = .024; SRMR = .047; S-B χ2(282) = 402.22, p = .00000), constrained model (CFI = .96; RMSEA = .024; SRMR = .052; S-B χ2(298) = 424.33, p = .00000), and , p = .14). Grandmothers' Race configural model (CFI = .98; RMSEA = .023; SRMR = .035; S-B χ2(188) = 260.42, p = .0004), constrained model (CFI = .98; RMSEA = .023; SRMR = .037; S-B χ2(196) = 269.57, p = .0004), and , p = .33); Grandmothers' Age configural model (CFI = .97; RMSEA = .026; SRMR = .039; S-B χ2(188) = 283.55, p = .00001), constrained model (CFI = .97; RMSEA = .025; SRMR = .039; S-B χ2(196) = 287.77, p = .00002), and , p = .84). Table 2 shows the standardized and unstandardized factor loadings on model latent constructs for all groups as derived from the final tests of the measurement model. All hypothesized factor loadings were statistically significant for all groups and there were no cross-loadings.
Table 2.
Estimated Standardized/Unstandardized Factor Loadings
| Grandchild gender | Grandchild age | Grandmother race | Grandmother age | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Latent factors indicators | Boys (n = 342) |
Girls (n = 391) |
4-7 (n = 235) |
8-11 (n = 247) |
12-17 (n = 251) |
White (n = 367) |
Black (n = 366) |
≤ 55 (n = 342) |
> 55 (n = 391) |
| Grandchild Internalizing Problems | |||||||||
| Emotional symptoms | .83/1.00 | .71/1.00 | .73/1.00 | .70/1.00 | .86/1.00 | .75/1.00 | .78/1.00 | .73/1.00 | .79/1.00 |
| Peer problems | .68/.76 | .68/.76 | .63/.76 | .61/.76 | .77/.76 | .68/.77 | .68/.77 | .67/.78 | .70/.78 |
| Grandchild Externalizing Problems | |||||||||
| Conduct disorder | .82/1.00 | .81/1.00 | .81/1.00 | .83/1.00 | .79/1.00 | .82/1.00 | .81/1.00 | .79/1.00 | .84/1.00 |
| Hyperactive/inattentive | .73/1.17 | .78/1.17 | .76/1.19 | .77/1.19 | .74/1.19 | .76/1.17 | .75/1.17 | .76/1.18 | .75/1.18 |
| Grandmother Psychological Distress | |||||||||
| Anxiety | .80/.10 | .76/.10 | .78/.10 | .76/.10 | .78/.10 | .75/.10 | .80/.10 | .80/.10 | .72/.10 |
| Depression | .84/1.00 | .83/1.00 | .83/1.00 | .82/1.00 | .86/1.00 | .80/1.00 | .88/1.00 | .89/1.00 | .80/1.00 |
| Dysfunctional Parenting | |||||||||
| Ineffective disciplinea | .73/.44 | .67/.45 | .76/.45 | .71/.45 | .68/.45 | .64/.44 | .75/.44 | .69/.45 | .73/.45 |
| Harsh | .62/1.00 | .64/1.00 | .59/1.00 | .61/1.00 | .70/1.00 | .68/1.00 | .59/1.00 | .65/1.00 | .63/1.00 |
| Inconsistent | .59/.97 | .76/1.00 | .56/.94 | .60/.94 | .66/.94 | .64/.99 | .65/.99 | .61/.94 | .62/.94 |
| Low Nurturancea | .83/1.00 | .76/1.00 | .86/1.00 | .77/1.00 | .84/1.00 | .80/1.00 | .80/1.00 | .77/1.00 | .84/1.00 |
| Attachment | .83/1.06 | .86/1.06 | .85/1.05 | .81/1.05 | .83/1.05 | .86/1.09 | .86/1.09 | .84/1.06 | .84/1.06 |
| Reinforcement | .77/1.00 | .83/1.00 | .77/1.00 | .85/1.00 | .80/1.00 | .76/1.00 | .82/1.00 | .81/1.00 | .79/1.00 |
| Social Support | |||||||||
| Expressive support | .68/3.20 | .68/3.19 | .70/3.27 | .69/3.27 | .68/3.27 | .69/3.26 | .69/3.26 | .68/3.30 | .71/3.30 |
| Family/friends | .76/1.00 | .71/1.00 | .77/1.00 | .72/1.00 | .68/1.00 | .76/1.00 | .68/1.00 | .73/1.00 | .71/1.00 |
| Family Dysfunction | |||||||||
| Boundary ambiguity | .81/.70 | .78/.70 | .82/.70 | .76/70 | .82/.70 | .82/.79 | .86/.79 | .80/.74 | .84/.74 |
| Anger | .81/1.00 | .80/1.00 | .79/1.00 | .81/1.00 | .81/1.00 | .74/1.00 | .79/1.00 | .82/1.00 | .75/1.00 |
Note: All factor loadings were statistically significant (p < .05). One indicator per factor had its loading fixed at 1.00 to establish the factor scale.
Value in this row represent loadings on the second order Dysfunction Parenting factor.
Tests of Structural Invariance
Evidence of full structural invariance was found for those group comparisons involving grandchildren's gender, grandmothers'race, and grandmothers'age. The corresponding indices of fit for the structural invariance model and the between this model and the preceding model for measurement invariance for each of the respective comparisons were as follows: Grandchildren's Gender (CFI = .97; RMSEA = .023; SRMR = .048; S-B χ2(222) = 307.39, p = .0001); , p = .16); Grandmothers' Race (CFI = .98; RMSEA = .021; SRMR = .047; S-B χ2(222) = 296.55, p = .0006; , p = .41); Grandmothers' Age (CFI = .97; RMSEA = .025; SRMR = .050; S-B χ2(222) = 321.67, p = .00001; , p = .14).
Although model fit indices for the test of structural invariance by grandchildren's age were good (CFI = .95; RMSEA = .025; SRMR = .060; S-B χ2(324) = 472.43, p = .00000), the comparison to the measurement invariance model was significant , and the LM test suggested releasing constraints involving three paths (education to dysfunctional parenting; family dysfunction to grandmothers'distress; social support to dysfunctional parenting) and three involving covariances of exogenous variables (education—family dysfunction; grandmothers' health—family dysfunction; education—social support). These six constraints were released and model fit (CFI = .96; RMSEA = .022; SRMR = .060; S-B χ2(338) = 459.69, p = .00001) improved significantly .
Given that far more similarities than differences were found between groups regarding the structural model, Figure 2, presents the range of standardized and unstandardized coefficients observed across groups for the hypothesized paths derived from the final tests of the structural model. The following paths were statistically significant for all groups: dysfunctional parenting to both internalizing and externalizing problems; grandmothers' distress to internalizing problems; grandmothers' distress to dysfunctional parenting; social support to both grandmothers' distress and dysfunctional parenting; family dysfunction to both grandmothers' distress and dysfunctional parenting; grandmothers' health to grandmothers' distress; and education to grandmothers' distress. The path from income to dysfunctional parenting was insignificant except for the group comparison involving grandchildren's gender (where this path barely reached significance). In contrast, the following paths (deleted from Figure 2) were not significant for any groups: grandmothers' distress to externalizing problems; grandmothers' health to dysfunctional parenting; and income to grandmother's distress. The path from education to dysfunctional parenting was significant for grandmothers of children age 8-11 only.
Figure 2.
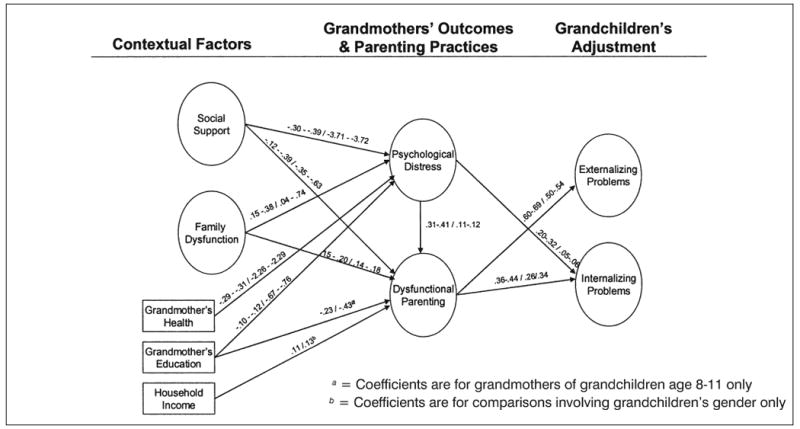
Ranges of statistically significant standardized/unstandardized path coefficients for final structural model.
Note: Non-significant pathways are deleted from Figure. All path coefficients are statistically significant (p < .05).
See text for description of group differences.
Grandchildren's age was the only category where between group differences were observed—the inverse path from social support to dysfunctional parenting was significantly lower for grandmothers of children age 4-7 compared to children age 12-17 (–.12/–.35 vs. –.39/–1.43, p < .05); the path from family dysfunction to grandmothers' distress was significantly lower among grandmothers of children age 8-11 relative to children 4-7 (.15/.42 vs. 38/1.04, p < .05); and the inverse path from education to dysfunctional parenting was significantly higher for grandmothers of children age 8-11 compared to age 4-7 (–.22/–.43 vs. .00/.01, p < .05). The pathways from social support to dysfunctional parenting and from family dysfunction to grandmother distress, however, were statistically significant for all age groups. In contrast, the pathway from education to dysfunctional parenting was significant only for grandmothers of children 8-11.
Covariances (available upon request) between the exogenous variables were largely invariant across all groupings except for two that differed by grandchildren's age (social support—education and family dysfunction—education).
Analyses of Total Effects
To further evaluate the structural model, we examined the total effects of each latent construct on the respective outcomes of grandchildren's internalizing and externalizing problems (Table 3). The total effects associated with grandmothers' distress and dysfunctional parenting on both types of problems were statistically significant and of moderate to high magnitude for all groups. This, along with the above finding that the direct path from grandmothers' distress to externalizing problems was insignificant across all groups, supports the basic FSM tenet that dysfunctional parenting mediates the effect of caregiver distress on children's adjustment. In contrast, our finding that the direct path from grandmothers' psychological distress to internalizing problems was significant for all groups suggests that dysfunctional parenting may only partially mediate the relationship between caregiver distress and children's adjustment in terms of internalizing problems. Table 3 further reveals that social support and family dysfunction tend to exert significant though modest total effects on both indices of grandchildren's adjustment, whereas education and household income generally do not. Finally, although grandmothers' health had a significant total effect on internalizing problems for all groups except grandmothers of older children, the total effects of this variable on externalizing problems were significant in only three groups (Black grandmothers, grandmothers of girls, and grandmothers of children age 4-7).
Table 3.
Standardized/Unstandardized Total Effects of Antecedent Constructs on Grandchildren's Internalizing and Externalizing Problems, by Group
| Grandchild gender | Grandchild age | Grandmother race | Grandmother age | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Antecedent construct | Boys | Girls | 4-7 | 8-11 | 12-17 | White | Black | ≤ 55 | > 55 |
| Internalizing Problems | |||||||||
| Grandmother psychological distress | .41/.10* | .47/.11* | .53/.11* | .39/.09* | .37/.09* | .41/.11* | .37/.07* | .47/.09* | .35/.09* |
| Dysfunctional parenting | .21/.17* | .64/.45* | .29/.20* | .38/.29* | .36/.28* | .27/.21* | .55/.39* | .38/.28* | .41/.31* |
| Family dysfunction | .16/.11* | .22/.14* | .19/.10* | .14/.09* | .15/.11* | .14/.10* | .22/.14* | .19/.11* | .14/.10* |
| Social support | −.21/−.51* | −.17/−.40* | −.18/−.36* | −.31/−.68* | −.23/−.68* | −.19/−.45* | −.25/−.57* | −.21/−.49* | −.22/−.52* |
| Grandmother health | −.08/−.15* | −.13/−.21* | −.17/−.27* | −.03/−.05 | −.07/−.14 | −.09/−.16* | −.12/−.19* | −.13/−.20* | −.08/−.14* |
| Education | −.05/−.09 | −.07/−.10 | −.06/−.09 | −.20/−.27* | .03/.06 | −.06/−.09 | −.04/−.06 | −.07/−.12* | −.07/−.07 |
| Household income | .01/.00 | −.05/−.04 | .03/.02 | .03/.03 | −.04/−.04 | .02/.02 | −.05/−.04 | −.01/−.01 | −.02/−.02 |
| Externalizing Problems | |||||||||
| Grandmother psychological distress | .32/.08* | .42/.10* | .49/.12* | .25/.06* | .29/.09* | .37/.10* | .28/.06* | .37/.08* | .31/.08* |
| Dysfunctional parenting | .57/.45* | .76/.60* | .49/.38* | .68/.56* | .71/.50* | .64/.53* | .66/.49* | .53/.42* | .83/.63* |
| Family dysfunction | .19/12* | .24/.16* | .16/.10* | .19/.13* | .19/.13* | .17/.13* | .23/.16* | .19/.13* | .20/.14* |
| Social support | −.32/−.73* | −.15/−.36* | −.18/−.42* | −.34/−.81* | −.33/−.86* | −.24/−.58* | −.24/−.58* | −.20/−.50* | −.28/−.66* |
| Grandmother health | −.02/−.04 | −.10/−.18* | −.15/−.28* | .04/.07 | −.01/−.02 | −.03/−.06 | −.10/−.16* | −.09/−.15 | −.04/−.07 |
| Education | −.06/−.09 | −.07/−.11 | −.05/−.08 | −.25/−.38* | .06/.10 | −.08/−.14 | −.04/−.06 | −.07/−.13 | −.05/−.07 |
| Household income | −.04/−.04 | −.07/−.06 | −.01/−.00 | .03/.02 | −.08/−.07 | −.01−.01 | −.06/−.06 | −.02/−.02 | −.06/−.05 |
Note: Total effects were estimated in the final version of the measurement model for each grouping.
p < .05.
Tests for Invariance of Latent Means
Results of the group invariance tests regarding the latent means for model constructs are summarized in Table 4. Factor intercept values showing statistically significant group differences and corresponding standardized effect sizes controlling for exogenous variables are presented.
Table 4.
Summary of Latent Means Analyses: Unstandardized Factor Means and Standardized Effect Sizes, by Group
| Grandchild gender | Grandchild age | Grandmother race | Grandmother age | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys vs. Girlsa | 4-7 vs. 8-11a | 4-7 vs. 12-17a | 8-11 vs. 12-17a | White | Black | ≤ 55 | > 55 | |||||
| Factor mean | Effect size | Factor mean | Effect size | Factor mean | Effect size | Factor mean | Effect size | Factor mean | Effect size | Factor mean | Effect size | |
| Grandchild externalizing problems | .49/.54 | .26/.29 | .81 | .42 | .73 | .38 | .46/.60 | .24/.31 | .40 | .21 | ||
| Grandchild internalizing problems | .43/.46 | .23/.24 | -.41 | .24 | .56 | .30 | .70/.79 | .38/.42 | ||||
| Grandmother psychological distress | 1.26 | .46 | ||||||||||
| −.290 | 1.13 | 2.13 | .80 | −.53/−.76 | .22/.32 | −.98 | .12 | |||||
| Dysfunctional parenting | ||||||||||||
| Social support | ||||||||||||
| Family dysfunction | 1.03/.52 | .35/.19 | ||||||||||
Note: Entries are shown for statistically significant (p < .05) group differences only. Effects were computed with adjustments for the measured and/or latent antecedents as per the structural model. For comparisons of White and Black grandmothers, entries to the left of the slash are for the original model, and entries to the right of the slash are for the revised model as suggested by Lagrange Multiplier test results (p < .05).
Entered as the reference group in the analysis.
Although model fit indices for the initial test of latent means by grandchild's gender were good (CFI = .97; RMSEA = .026; SRMR = .045; S-B χ2(230) = 338.72, p = .000000), the LM test suggested releasing one constraint (the factor intercept involving anger). The retested model yielded a significant improvement in model fit . Two statistically significant latent mean differences were observed: grandmothers of boys reported higher levels on both the internalizing and externalizing constructs than did grandmothers of girls.
Model fit indices for the initial test of invariance for the latent means by grandchildren's age were good (CFI = .96; RMSEA = .023; SRMR = .061; S-B χ2(354) = 492.28, p = .00000), and the LM test did not suggest the release of any constraints. Several statistically significant group differences were observed with respect to the latent means. Grandmothers of children age 12-17 had significantly lower means on the externalizing construct in comparison to grandmothers of children in the two younger age groups, whereas grandmothers of children age 8-11 had significantly higher mean scores on the internalizing constructs than did grandmothers of children in the oldest and youngest age groups. Grandmothers of children age 8-11 also had significantly higher means on the dysfunctional parenting construct than did grandmothers of children in the two other age groups.
Although model fit indices for the initial test of invariance for the latent means by race were good (CFI = .97; RMSEA = .028; SRMR = .046; S-B χ2(230) = 359.39, p < .00000), the LM test suggested releasing the equality constraints associated with three factor intercepts (anger, expressive support, and inconsistent discipline). The revised model yielded a significant improvement in model fit . Four statistically significant differences were found regarding the latent means comparisons (Table 4). Compared to Blacks, White grandmothers reported more externalizing problems, more internalizing problems, less dysfunctional parenting, and more family dysfunction.
Model fit indices for the initial test of invariance for the latent means by grandmothers'age were good (CFI = .96; RMSEA = .026; SRMR = .050; S-B χ2(230) = 344.46, p =.00000) and no constraints were suggested for release by the LM test. Significant age differences were found on three latent constructs. Younger grandmothers reported greater externalizing problems, more psychological distress, and less dysfunctional parenting than did older grandmothers.
Discussion
We tested via SEM an expanded version of the FSM that includes contextual factors likely to affect the psychological outcomes of both custodial grandmothers and the grandchildren to whom they provide care. Multigroup comparisons were made to determine if the measurement, structural, and latent means components of the model were invariant in terms of grandmothers' race and age, as well as grandchildren's gender and age. No significant group differences emerged regarding the model's measurement components, and only a few group differences were found regarding its structural components. Between-group differences in the latent means of model constructs, however, were more prevalent. Thus, group differences mainly involved dissimilarities in the magnitude of the latent constructs rather than in the pattern or degree of correlation among them.
Consistent with past studies of the FSM involving diverse types of families and parenting circumstances (Conger et al., 1994, 2002; Forgath et al., 1995; Kwok et al., 2005; Mistry et al., 2002), our findings with custodial grandfamilies reinforce the overall generalizability and robustness of the FSM. In particular, like past investigators, we found strong support for the basic principle that dysfunctional parenting mediates the relationship between caregivers' psychological distress and children's adjustment. However, since our adaptation of the FSM recognizes key family characteristics beyond socioeconomic circumstances, the present findings shed important new light on the interrelationships between diverse family contextual factors, grandmothers' distress, dysfunctional parenting practices, and grandchildren's adjustment.
One unique finding is that the extent to which dysfunctional parenting mediates the relationship between grandmothers' distress and grandchildren's adjustment was greater for externalizing problems than for internalizing problems. This difference is particularly informative given that little is known about the effects of parenting and children's socialization experiences on internalizing disorders (Rubin & Burgess, 2002). Although there is abundant evidence that the impact of caregivers' distress on children's externalizing problems is largely indirect through inept discipline and a disruption in the parent-child relationship (Johnson & Mash, 2001), our findings suggest that distress in caregivers exerts both direct and indirect effects on grandchildren's internalizing problems. Possible mechanisms discussed in the parenting literature whereby a caregiver's distress might exert direct effects on a child's internalizing difficulties include: disengaging from the child; being critical of the child; modeling one's own fears and insecurities; discouraging the child's self-expression; reducing the child's experience of positive reinforcement; and expressing burden to the child (Conley et al., 2004; Cummings & Davies, 1994; Joiner & Katz, 1999). There may also be a direct genetic link between a grandchild's internalizing problems and a grandparent's psychological distress (Joiner & Katz, 1999). These conclusions are speculative, however, and research is needed to clarify how psychological distress among those in the parenting role is related to the onset, maintenance, or exacerbation of children's internalizing difficulties.
Our results also point to the conclusion that a custodial grandmother's distress does not bear an increased risk for her grandchild's psychological difficulties independent of the family's psychosocial circumstances as a whole. This was evidenced, for example, by our finding that family dysfunction, social support, and grandmother's health concurrently exerted statistically significant total effects on grandchildren's internalizing and externalizing problems. However, as expected, the effects of these factors on grandchildren's adjustment were indirect through grandmother's distress and dysfunctional parenting. Not only are these findings consistent with the consensus in the parenting literature that the impact of parental distress on children is best considered within a larger family context of interdependent elements and processes (Cummings & Davies, 1994), they also reinforce the view that variables such as social support and family stress are largely distal influences on child behavior (Rubin & Burgess, 2002).
Apart from a few exceptions, neither education nor household income exerted statistically significant direct, indirect, or total effects on grandchildren's adjustment within our expanded version of the FSM. This is despite the fact that indices of socioeconomic hardship are regarded as the primary source of family stress in the original FSM (Conger, Conger, Elder, Lorenz, Simons, & Whitbeck, 1992). Instead, our findings support the view that several psychosocial risk factors in combination are more damaging to children's well-being than any single factor in isolation (Cumming & Davies, 1994). A caveat, however, is that we used very objective indicators (i.e., education and household income) instead of the more subjective measures of socioeconomic hardship typically used in studies of the FSM.
Presence and Absence of Group Invariance
The generalizability of an expanded FSM across various types of custodial grandfamilies is evidenced by the overall results of our group invariance tests. As noted earlier, no between-group differences whatsoever emerged regarding the model's measurement components, suggesting that all latent constructs had equivalent meaning irrespective of grandmother's race and age or grandchildren's age and gender. For each subgroup under investigation, every hypothesized factor loading was statistically significant and there were no cross loadings.
The structural components of the proposed model were also largely invariant across subgroups, and the few statistically significant between group differences that did emerge were limited to grandchildren's age. For example, the inverse path from grandmother's education to dysfunctional parenting was significant only for grandmothers of children age 8-11. It may be that parenting children in this age range involves certain challenges (e.g., greater need for consistent discipline; expressing warmth via verbal communication; assisting with homework and other school issues; help with establishing peer relationships) that require higher levels of educational attainment than in parenting younger children or adolescents (see Collins, Madsen, & Susman-Stillman, 2002). Although group differences involving grandchildren's age were also found for two other paths (social support to dysfunctional parenting, and family dysfunction to grandmother distress), these differences involved magnitude only while both paths were statistically significant across all three age groups. Overall, our findings support the conclusion reached by Cummings and Davies (1994) in their literature review of research on children of psychologically distressed caregivers that “no one age group seems either particularly protected or particularly at risk” (p. 91).
After controlling for the effects of grandmother's education, income, and health, we also found several significant between-group differences on the latent means of the key constructs in our model. That the latent means associated with both the externalizing and internalizing constructs were higher among grandmothers caring for boys versus girls, is consistent with national findings where a higher percentage of boys than girls were reported by caregivers to have the kinds of difficulties assessed by the Strengths and Difficulties Questionnaire (SDQ) that was used in the present study (Simpson, Bloom, Cohen, & Blumberg, 2005). Likewise, our finding that latent means on the externalizing construct were higher for the two younger age groups compared to grandchildren age 12-17, is consistent with past research showing that aggressive behavior decreases as children develop and their emotion regulation skills and alternative conflict-resolution strategies emerge (Campbell, Spieker, Burchinal, & Poe, 2006). This trajectory of decreased aggressiveness as children grow older might similarly explain why younger grandmothers reported higher levels of externalizing problems than their older counterparts who were more likely to care for the oldest target grandchildren. In fact, the zero order correlation between grandmothers'age and target grandchild's age was statistically significant and positive (r = .34, p < .001, N = 733).
In contrast, our finding that the latent means on the internalizing construct were significantly higher for grandchildren in the 8-11 age group compared to the other two age groups is at odds with the fact that prevalence of internalizing disorders such as depression increases with age in the general population. However, this discrepancy may be due to the fact that the rate of internalizing disorders is often higher in children with comorbid externalizing disorders (e.g., ADHD and conduct disorder). It should be noted, however, that the techniques we used to measure grandchildren's internalizing and externalizing problems are not equivalent to a psychiatric diagnosis. Also, because it is difficult for lay informants like custodial grandmothers to observe internalizing symptoms (Simpson et al., 2005), our findings regarding grandchildren's internalizing problems should be viewed cautiously.
That White grandmothers in our sample reported higher levels of both internalizing and externalizing problems than Blacks is at odds with past findings that externalizing disorders are slightly more prevalent among Black children (Staller, 2006) and that race differences disappear when SES is controlled (Dodge, Pettit, & Bates, 1994). However, Pruchno (1999) found statistically significant differences between White and Black custodial grandmothers'reports of specific behavior problems. While White grandmothers in her sample were more likely to say that their grandchild was argumentative, impulsive, unhappy, withdrawn, and too dependent on others, felt worthless, or acted too young for his or her age, Black grandmothers were more likely to report that their grandchild lied, cheated, disobeyed at school, destroyed things, or got into fights. Future research is needed to decipher why Black and White custodial grandmothers report different patterns of behavior problems in grandchildren.
Differences also were found between White and Black custodial grandmothers on the latent means of the family dysfunction and dysfunctional parenting constructs. That Black grandmothers reported greater dysfunctional parenting than Whites is in line with past research showing that harsh (but not abusive) discipline is more normative among Blacks than Whites even though the deleterious effects of harsh discipline are similar in children from both races (Dodge, 2000). Because this style of discipline is more normative in Black families, it may be that it is not experienced as deviant or unusual parenting by Black custodial grandchildren and thus exerts no remarkable adverse impact on them. Similarly, our finding that Blacks reported significantly less family dysfunction than Whites may be explained by the fact that Blacks are more likely to live in extended family households that respond to family members' needs, less likely to embrace the traditional grandparental “norm of noninterference” in child-rearing, and have historically played much different roles in family maintenance than Whites (Brown & Mars, 1999). Thus, Black grandmothers may view the circumstances that encompass surrogate parenting as normative within the context of Black family life. That differences between Black and White grandmothers in this study were limited to dissimilarities in the latent constructs described above with no race differences at all found regarding the measurement and structural aspects of our model is supportive of the no group differences hypothesis described in the introduction (Rowe et al., 1994).
The only group difference observed regarding the means for the latent constructs of grandmothers' psychological distress and dysfunctional parenting involved the respective ages of grandmothers and grandchildren. Psychological distress was significantly higher for grandmothers under age 55, which is consistent with past research on custodial grandmothers (see Mills, Gomez-Smith, & De Leon, 2005) and with prior epidemiological studies showing that rate of mood disorders in females declines after menopause (Kornstein & Wojcik, 2002). In contrast, the latent means for dysfunctional parenting tended to be lower for younger grandmothers and for those who were caring for the youngest grandchildren. The latter findings suggest that older grandmothers may find it more difficult to parent effectively due to their own advancing age (Berrick, 1997) or that younger grandmothers may be more aware of current knowledge about effective parenting techniques. It may also be true that the physical demands of caring for younger children makes appropriate parenting strategies more obvious and straightforward to their carers.
Practice Implications
The strength of the relationship observed between grandmothers' psychological distress and dysfunctional parenting is meaningful given that a non-clinic sample of custodial grandfamilies was examined. In fact, only 24.3% of the entire sample had depression scores that met the clinical cutoff of 16 or higher on the CES-D. These findings suggest that ineffective parenting may occur even when stressful situations are encountered by custodial grandmothers who are without substantial mental health problems. Moreover, our use of self-reported depression and anxiety as a composite index of psychological distress reinforces the belief that negative affect, in general, rather than depressed mood per se, leads to poor parenting (Conley et al., 2004; Lovejoy et al., 2000). It is imperative for professionals to routinely screen and monitor custodial grandparents' levels of psychological distress, as well as to offer appropriate support, advice, and referral to reduce probable stressors.
The present findings also suggest that interventions designed to improve behavioral outcomes for custodial grandchildren should involve a combination of modalities that includes parent training, engaging grandparents in positive interactions with grandchildren, stress reduction, and counseling for grandparents' psychological distress (Conley et al., 2004). In some cases, it may be beneficial to target grandparents' psychological distress in addition to or instead of parenting deficits as their distress may be serving as the antecedent for parenting difficulties (Forehand & McCombs, 1988). Interventions geared toward building social supports and reducing family dysfunction appear to be especially critical in assisting custodial grandparents in dealing with stress. An important direction for future clinical research is to test whether improvement in positive parenting or reduction in grandparents' distress mediates the impact of an intervention on their grandchildren's adjustment, and whether these mediators operate independently or additively.
Study Limitations
Several limitations of the present study preclude drawing definitive conclusions from these findings. First, in the absence of longitudinal data, alternative causal paths among the constructs in the proposed model can not be ruled out. Some custodial grandparents may have psychological characteristics that predispose them to both family adversity and dysfunctional parenting (McLoyd, 1990), and custodial children's adjustment problems may act as stressors that heighten a grandmother's distress and trigger a breakdown in parenting (Johnson & Mash, 2001; Rothbaum & Weisz, 1994). Our cross-sectional data do not allow for examination of these alternatives, however. Nevertheless, the presumed causal sequence where the effect of grandmother's distress on the grandchild's adjustment is indirect through ineffective parenting is congruent with past longitudinal studies involving biological parents (Forehand & McCombs, 1988; Kwok et al., 2005) and custodial grandparents (Goodman & Hayslip, 2006) alike.
Another limitation is that our model is underspecified to the extent that several potentially relevant constructs were excluded. For example, the original FSM regards conflicted relations between the child's caregivers as an important antecedent of diminished parenting and the absence of this construct is a key shortcoming given past evidence that marital difficulties associated with parental distress can play an important role in the development or maintenance of childhood psychopathology (Cummings & Davies, 1994; Downey & Coyne, 1990). Future research is needed to determine the role of custodial grandfathers within the context of parenting models like the FSM. Other relevant constructs absent from our model include ideational factors such as grandparents' values and beliefs, cultural differences in socialization, socialization agents outside the family, grandchild characteristics other than age and gender (e.g., temperament, social-cognitive skills, duration of adjustment problems), and genetic influences (Goodman & Gotlib, 1999; Lovejoy et al. 2000; McLoyd, 1990; Rothbaum & Weisz, 1994). Preliminary analyses revealed that such variables as number of children cared for, other caregivers in the home, and time in the caregiver role did not add to the proposed model.
Additional limitations concern key measurement issues. Our use of grandmothers' self-report is problematic in that a caregiver's negative perceptions of a child's behavior, and of herself as a parent, may be determined more by subjective feelings of distress than by objective circumstances of the caregiver-child relationship (Goodman & Gotlib, 1999). Our reliance on questionnaires may have influenced the results given past evidence that their use in studies on the relationship between parental caregiving and child externalizing behavior yields smaller effect sizes than non-questionnaire techniques, and tends to mask differences associated with child gender and age (Rothbaum & Weisz, 1994). Finally, our indices of discipline and nurturance embody flaws typically associated with measures of this type, such as engendering a socially-desirable response set and wording items without tying them to specific parenting contexts (Locke & Prinz, 2002).
Despite these limitations, our findings with a large, national sample of custodial grandmothers shed important new light on how the psychological distress of custodial grandparents associated with adverse family circumstances can detrimentally affect the parenting behaviors of these caregivers. In turn, diminished ability to parent effectively may serve to generate, maintain, or exacerbate both the internalizing and externalizing problems present among custodial grandchildren (Smith & Palmieri, 2007). Moreover, this sequence appears to hold true regardless of the age and race of custodial grandmothers, and the age and gender of target grandchildren. Although the cross-sectional design of this study precludes conclusions regarding the direction of causality among model constructs, these findings clearly suggest that custodial grandmothers' psychological distress, dysfunctional parenting practices, and grandchildren's adjustment difficulties are highly intertwined and that each of these factors should be targeted in future interventions with these families. Not only do our findings support the claim by Hayslip et al. (1998) that a lack of parenting skills among grandparents “could contribute to the creation of new problems or the exacerbation of existing problems” (p. S172), they also suggest the value of exploring the unique circumstances of custodial grandfamilies by adapting extant parenting models like the FSM.
Acknowledgments
We wish to thank two anonymous reviewers and the editor for their helpful comments.
Footnotes
This research was supported by a grant from the National Institute of Mental Health awarded to the first author.
An earlier version of this article was presented at the 59th Annual Scientific Meeting of the Gerontological Society of America, Dallas, TX, November 2006.
Contributor Information
Gregory C. Smith, Kent State University
Patrick A. Palmieri, Summa Health System and Kent State University
Gregory R. Hancock, University of Maryland, College Park
Rhonda A. Richardson, Kent State University
References
- Abidin RR. Parenting stress index: Professional manual. 3rd. Lutz, FL: Psychological Assessment Resources, Inc; 1995. [Google Scholar]
- Bartram MH. Clarifying subsystem boundaries in grandfamilies. Contemporary Family Therapy. 1996;18:267–277. [Google Scholar]
- Berrick JD. Assessing quality of care in kinship and foster family care. Family Relations. 1997;46:273–280. [Google Scholar]
- Brown DR, Mars J. Profile of contemporary grandparenting in African-American Families. In: Cox CB, editor. To grandmother's house we go and stay: Perspectives on custodial grandparents. New York: Springer; 1999. pp. 203–217. [Google Scholar]
- Brown-Standridge MO, Floyd CW. Healing bittersweet legacies: Revisiting contextual family therapy for grandparents raising grandchildren in crisis. Journal of Marital and Family Therapy. 2000;26:185–197. doi: 10.1111/j.1752-0606.2000.tb00288.x. [DOI] [PubMed] [Google Scholar]
- Bryson K, Casper LM. Current Population Reports. Washington, DC: US Bureau of the Census; 1999. Coresident grandparents and grandchildren; pp. 23–198. [Google Scholar]
- Byrne BM. Structural equation modeling with EQS: Basic concepts, applications, and programming. 2nd. Mahwah, NJ: Lawrence Erlbaum Associates; 2006. [Google Scholar]
- Campbell SB. Behavior problems in preschool children: A review of recent research. Journal of Child Psychology and Psychiatry. 1995;36:113–149. doi: 10.1111/j.1469-7610.1995.tb01657.x. [DOI] [PubMed] [Google Scholar]
- Campbell SB, Spieker S, Burchinal M, Poe MD. Trajectories of aggression from toddlerhood to age 9 predict academic and social functioning through age 12. Journal of Child Psychology and Psychiatry. 2006;47:791–800. doi: 10.1111/j.1469-7610.2006.01636.x. [DOI] [PubMed] [Google Scholar]
- Caron W, Boss P, Mortimer J. Family boundary ambiguity predicts Alzheimer's outcomes. Psychiatry. 1999;62:347–356. doi: 10.1080/00332747.1999.11024882. [DOI] [PubMed] [Google Scholar]
- Collins WA, Madsen SD, Susman-Stillman A. Parenting during middle childhood. In: Bornstein MH, editor. Handbook of parenting. Vol. 1. Mahwah, NJ: Erlbaum; 2002. pp. 73–101. [Google Scholar]
- Conger KJ, Rueter MA, Conger RD. The role of economic pressure in the lives of parents and their adolescents: The Family Stress Model. In: Crockett LJ, Silbereisen RK, editors. Negotiating adolescence in times of social change. New York: Cambridge University Press; 2000. pp. 201–223. [Google Scholar]
- Conger RD, Conger KJ, Elder GH, Jr, Lorenz FO, Simons RL, Whitbeck LB. A family process model of economic hardship and adjustment of early adolescent boys. Child Development. 1992;63:526–541. doi: 10.1111/j.1467-8624.1992.tb01644.x. [DOI] [PubMed] [Google Scholar]
- Conger RD, Ge X, Elder GH, Lorenz FO, Simons RL. Economic stress, coercive family processes, and developmental problems of adolescents. Child Development. 1994;65:541–561. [PubMed] [Google Scholar]
- Conger RD, Wallace LE, Sun Y, Simons RL, McLoyd VC, Brody GH. Economic pressure in African American families: A replication and extension of the Family Stress Model. Developmental Psychology. 2002;38:179–193. [PubMed] [Google Scholar]
- Conley CS, Caldwell MS, Flynn M, Dupre AJ, Rudolph KD. Parenting and mental health. In: Hoghughi M, Long N, editors. Handbook of parenting: Theory and research for practice. Thousand Oaks, CA: Sage; 2004. pp. 276–285. [Google Scholar]
- Cummings EM, Davies PT. Maternal depression and child development. Journal of Child Psychology and Psychiatry. 1994;35:73–112. doi: 10.1111/j.1469-7610.1994.tb01133.x. [DOI] [PubMed] [Google Scholar]
- Curran PJ, West SG, Finch JF. The robustness of test statistics to non normality and specification error in confirmatory factor analysis. Psychological Methods. 1996;1:16–29. [Google Scholar]
- Daly SL, Glenwick DS. Personal adjustment and perceptions of grandchild behavior in custodial grandmothers. Journal of Clinical Child Psychology. 2000;29:108–118. doi: 10.1207/S15374424jccp2901_11. [DOI] [PubMed] [Google Scholar]
- Dodge KA. Conduct disorder. In: Sameroff AJ, Lewis M, Miller SM, editors. Handbook of developmental psychopathology. 2nd. New York: Plenum; 2000. pp. 447–463. [Google Scholar]
- Dodge KA, Pettit GS, Bates JE. Socialization mediators of the relation between socioeconomic status and child conduct problems. Child Development. 1994;65:649–665. [PubMed] [Google Scholar]
- Downey G, Coyne JC. Children of depressed parents: An integrative review. Psychological Bulletin. 1990;108:50–76. doi: 10.1037/0033-2909.108.1.50. [DOI] [PubMed] [Google Scholar]
- Forehand R, McCombs A. Unraveling the antecedent-consequence conditions in maternal depression and adolescent functioning. Behavior Research and Therapy. 1988;26:399–405. doi: 10.1016/0005-7967(88)90073-3. [DOI] [PubMed] [Google Scholar]
- Forgath MS, Patterson GR, Ray JA. Divorce and boys' adjustment problems: Two paths with a single model. In: Hetherington EM, Blechman EA, editors. Stress, coping, and resiliency in families. Mahwah, NJ: Erlbaum; 1995. pp. 67–105. [Google Scholar]
- Fuller-Thomson E, Minkler M, Driver D. A profile of grandparents raising grandchildren in the United States. The Gerontologist. 1997;37:406–411. doi: 10.1093/geront/37.3.406. [DOI] [PubMed] [Google Scholar]
- George LK. Social factors and illness. In: Binstock RH, George LK, editors. Handbook of aging and the social sciences. 4th. San Diego: Academic Press; 1995. pp. 229–252. [Google Scholar]
- Goodman CG, Hayslip B. Grandmothers raising grandchildren: Grandmother and grandchild well-being over time. 2006 Unpublished manuscript. [Google Scholar]
- Goodman R. Psychometric properties of the Strengths and Difficulties Questionnaire. Journal of the American Academy of Adolescent Psychiatry. 2001;40:1337–1345. doi: 10.1097/00004583-200111000-00015. [DOI] [PubMed] [Google Scholar]
- Goodman SH, Gotlib IH. Risk for psychopathology in children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review. 1999;106:458–490. doi: 10.1037/0033-295x.106.3.458. [DOI] [PubMed] [Google Scholar]
- Hayslip B, Shore RJ, Henderson CE, Lambert PL. Custodial grandparenting and the impact of grandchildren with problems on role satisfaction and role meaning. Journal of Gerontology: Social Sciences. 1998;53B:S164–S173. doi: 10.1093/geronb/53b.3.s164. [DOI] [PubMed] [Google Scholar]
- Hirshorn BA, Van Meter MJ, Brown DR. When grandparents raise grandchildren due to substance abuse: Responding to a uniquely destabilizing factor. In: Hayslip B, Goldberg-Glen R, editors. Grandparents raising grandchildren: Theoretical, empirical, and clinical perspectives. New York: Springer; 2000. pp. 269–287. [Google Scholar]
- Johnson C, Mash EJ. Families of children with attention-deficit/hyperactivity disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review. 2001;4:183–207. doi: 10.1023/a:1017592030434. [DOI] [PubMed] [Google Scholar]
- Joiner TE, Katz J. Contagion of depressive symptoms and mood: Meta-analytic review and explanations from cognitive, behavioral, and interpersonal viewpoints. Clinical Psychology: Science and Practice. 1999;6:149–164. [Google Scholar]
- Kornstein SG, Wojcik BA. Depression. In: Kornstein SG, Clayton AH, editors. Women's mental health: A comprehensive textbook. New York: Guilford; 2002. pp. 147–165. [Google Scholar]
- Kwok O, Haine RA, Sandler IN, Ayers TS, Wolchik SA, Tein J. Positive parenting as a mediator of the relations between parental psychological distress and mental health problems of parentally bereaved children. Journal of Clinical Child and Adolescent Psychology. 2005;34:260–271. doi: 10.1207/s15374424jccp3402_5. [DOI] [PubMed] [Google Scholar]
- Locke LM, Prinz RJ. Measurement of parental discipline and nurturance. Clinical Psychology Review. 2002;22:895–929. doi: 10.1016/s0272-7358(02)00133-2. [DOI] [PubMed] [Google Scholar]
- Lovejoy MC, Graczyk PA, O'Hare EO, Neuman G. Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology Review. 2000;20:561–592. doi: 10.1016/s0272-7358(98)00100-7. [DOI] [PubMed] [Google Scholar]
- McLoyd VC. The impact of economic hardship on Black families and children: Psychological distress, parenting, and socioemotional development. Child Development. 1990;61:311–346. doi: 10.1111/j.1467-8624.1990.tb02781.x. [DOI] [PubMed] [Google Scholar]
- Mills TM, Gomez-Smith Z, De Leon JM. Skipped generation families: Sources of psychological distress among grandmothers of grandchildren who live in homes where neither parent is present. Marriage and Family Review. 2005;37:191–212. [Google Scholar]
- Minkler M, Fuller-Thomson E, Miller D, Driver D. Depression in grandparents raising grandchildren: Results of a national longitudinal study. Archives of Family Medicine. 1997;6:445–452. doi: 10.1001/archfami.6.5.445. [DOI] [PubMed] [Google Scholar]
- Mistry RS, Vandewater EA, Huston AC, McLoyd VC. Economic well-being and children's social adjustment: The role of family process in an ethically diverse low-income sample. Child Development. 2002;73:935–951. doi: 10.1111/1467-8624.00448. [DOI] [PubMed] [Google Scholar]
- Musil CM, Amhad M. Health of grandmothers: A comparison by caregiver status. Journal of Aging and Health. 2002;14:96–121. doi: 10.1177/089826430201400106. [DOI] [PubMed] [Google Scholar]
- Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: An overview of concepts and their measures. The Gerontologist. 1990;30:583–594. doi: 10.1093/geront/30.5.583. [DOI] [PubMed] [Google Scholar]
- Pfiffner LJ, McBurnett K, Rathouz PJ, Judice S. Family correlates of oppositional and conduct disorders in children with Attention Deficit/Hyperactivity Disorder. Journal of Abnormal Child Psychology. 2005;33(5):551–563. doi: 10.1007/s10802-005-6737-4. [DOI] [PubMed] [Google Scholar]
- Pruchno RA. Raising grandchildren: The experience of Black and White grandmothers. The Gerontologist. 1999;39:209–221. doi: 10.1093/geront/39.2.209. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Rodgers-Farmer AY. Parenting stress, depression, and parenting in grandmothers raising their grandchildren. Children and Youth Services Review. 1999;21:377–388. [Google Scholar]
- Rothbaum F, Weisz JR. Parental caregiving and child externalizing behavior in nonclinical samples: A meta-analysis. Psychological Bulletin. 1994;116:55–74. doi: 10.1037/0033-2909.116.1.55. [DOI] [PubMed] [Google Scholar]
- Rowe DC, Vazsonyi AT, Flannery DJ. No more than skin deep: Ethnic and racial similarity in developmental process. Psychological Review. 1994;101:396–413. [Google Scholar]
- Rubin KH, Burgess K. Parents of aggressive and withdrawn children. In: Bornstein M, editor. Handbook of parenting. 2nd. Vol. 1. Hillsdale, NJ: Lawrence Erlbaum Associates; 2002. pp. 383–418. [Google Scholar]
- Sands RG, Goldberg-Glen RS. Factors associated with stress among grandparents raising their grandchildren. Family Relations. 2000;49:97–105. [Google Scholar]
- Simmons T, Dye JL. Grandparents living with grandchildren: 2000. 2003 Retrieved July 8, 2006, from www.census.gov/prod/2003pubs/c2kbr-31.pdf.
- Simpson GA, Bloom B, Cohen RA, Blumberg S. US children with emotional and behavioral difficulties: Data from the 2001, 2002, and 2003 National Health Interview Surveys Advance data from vital and health statistics; No 360. Hyattsville, MD: National Center for Health Statistics; 2005. [PubMed] [Google Scholar]
- Smith GC, Palmieri PA. Risk for psychological difficulties in children raised by custodial grandparents. Psychiatric Services. 2007;58:1303–1310. doi: 10.1176/appi.ps.58.10.1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith DK, Sprengelmeyer PG, Moore KJ. Parenting and antisocial behaviour. In: Hoghughi M, Long N, editors. Handbook of parenting: Theory and research for practice. Thousand Oaks, CA: Sage; 2004. pp. 237–255. [Google Scholar]
- Solomon JC, Marx J. Who cares? Grandparent/grandchild households. Journal of Women and Aging. 1999;11:3–25. doi: 10.1300/J074v11n01_02. [DOI] [PubMed] [Google Scholar]
- Staller JA. Diagnostic profiles in outpatient child psychiatry. American Journal of Orthopsychiatry. 2006;76:98–102. doi: 10.1037/0002-9432.76.1.98. [DOI] [PubMed] [Google Scholar]
- Stewart AL, Ware JE, Sherbourne CD, Wells KB. Psychological distress/well-being and cognitive functioning measures. In: Stewart AL, Ware JE, editors. Measuring functioning and well-being: The Medical Outcomes Study Approach. Durham, NC: Duke University Press; 1992. pp. 102–142. [Google Scholar]
- Strawbridge W, Wallhagen M, Shema S, Kaplan G. New burdens or more of the same? Comparing adult grandparent, spouse, and adult-child caregivers. The Gerontologist. 1997;17:505–510. doi: 10.1093/geront/37.4.505. [DOI] [PubMed] [Google Scholar]
- Szinovacz ME, DeViney S, Atkinson MP. Effects of surrogate parenting on grandparents' well-being. Journal of Gerontology: Social Sciences. 1999;54B:S376–S388. doi: 10.1093/geronb/54b.6.s376. [DOI] [PubMed] [Google Scholar]
- Webster-Stratton C. Stress: A potential disruptor of parent perceptions and family interactions. Journal of Clinical Child Psychology. 1990;19:302–312. [Google Scholar]
- Webster-Stratton C, Reid MJ, Hammond M. Preventing conduct problems, promoting social competence: A parent and teacher training partnership in Head Start. Journal of Clinical Child Psychology. 2001;30:283–302. doi: 10.1207/S15374424JCCP3003_2. [DOI] [PubMed] [Google Scholar]