

Abstract
In the last forty years, mechanical circulatory support devices have become an effective option for the treatment of end stage heart failure in adults. Few possibilities, however, are available for pediatric cardiopulmonary support. Ension Inc. (Pittsburgh, PA) is developing a pediatric cardiopulmonary assist system (pCAS) intended to address the limitations of existing devices used for this patient population. The pCAS device is an integrated unit containing an oxygenator and pump within a single casing, significantly reducing the size and blood-contacting surface area in comparison to current devices. Prototype pCAS devices produce appropriate flows and pressures while minimizing priming volume and preparation time. The pCAS was tested on a mock circulation designed to approximate the hemodynamic parameters of a small infant using a 10 Fr. ECMO inflow cannula and an 8 Fr. ECMO outflow cannula. Revision 4 of the device provided a flow rate of 0.42 L/min at 6500 RPM. Revision 5, featuring improved impeller and diffuser designs, provided a flow rate of 0.57 L/min at 5000 RPM. The performance tests indicate that for this cannulae combination, the pCAS pump is capable of delivering sufficient flows for patients less than 5 kg.
Keywords: Pediatric, Cardiopulmonary Support, pCAS, Performance Testing
Introduction
The early 1960s witnessed the first attempts to develop ventricular assist devices (VADs). Since that time both technology and medical management of VAD patients have progressed significantly. Mechanical assist devices have now been shown to be more effective than optimum medical management and are being used with more regularity every year1. Despite these advances, there have been relatively few devices made available in the past forty years for the treatment of children in need of cardiac or cardiopulmonary support.
Today there are nearly 40,000 children born with congenital heart disease every year in the United States. Of these 40,000 children, 25% will require invasive treatment to correct or palliate these defects, creating the need to provide cardiopulmonary bypass during surgery, as well as circulatory support in the pre or post operative periods2. The first attempts at pediatric mechanical circulatory support were undertaken in 1963 using a roller pump and small disk oxygenator to provide post-operative support to a six year old female3. Since that initial groundbreaking treatment there have been ongoing attempts to provide mechanical pediatric support.
Currently the most commonly used treatment option is extracorporeal membrane oxygenation (ECMO). ECMO systems include both pump and oxygenator and are most commonly used to provide cardiopulmonary support, although they are also used in situations where only cardiac support is needed. Though ECMO has a success rate of approximately 75% depending on the indication, the technique is plagued by complications including thrombosis and bleeding.4-10 ECMO requires a great deal of circuit assembly which prolongs set up time in an emergency situation and requires extensive training for its operators. ECMO circuits also require a large priming volume which may create challenges in relation to the small blood volumes of pediatric patients and increases the blood contact with foreign materials which can stimulate an inflammatory response.
In an effort to alleviate the morbidities associated with the existing ECMO systems and extend the use of mechanical support to a wider range of pediatric patients, the National Heart, Lung and Blood Institute issued five research contracts to develop five new pediatric cardiac assist systems11. Four of these systems are either pulsatile or continuous flow ventricular assist devices. Ension Inc. (Pittsburgh, PA), as one of the contractors, has developed an integrated pump oxygenator which is capable of providing both cardiac and pulmonary support to neonates and small children. This device, the pediatric cardiopulmonary assist system (pCAS), is intended for short term stabilization of pre-operative neonatal and infant patients or patients requiring post-operative support. The integrated pCAS design results in reduced priming volume and blood contacting surface area. A key feature of the pCAS is the Ension biologic coating intended to minimize the need for systemic heparin and to prevent plasma breakthrough. It is anticipated that once the initial version is finalized and proven adequate, a second, larger device will be developed with the capability of supporting children up to 25 kg.
Methods
The pCAS system employs a design which incorporates both oxygenator and pump into a single housing, providing a significant reduction in blood-contact surface area and priming volume as compared to currently employed systems (Figure 1). This reduction in tubing and equipment is expected to reduce inflammatory response as well as lower the necessary anticoagulation medication required. The minimal space required by the system creates the possibility of a greater interaction between the patient and parent during treatment and easier patient transport. Research has shown that parent/infant interaction in the neonatal period is essential in the bonding process and has a profound affect on the patient’s later social abilities12-14. It is anticipated that this new device will allow a newborn on cardiopulmonary support to be touched and held by the parents as well as the nurse.
Figure 1.
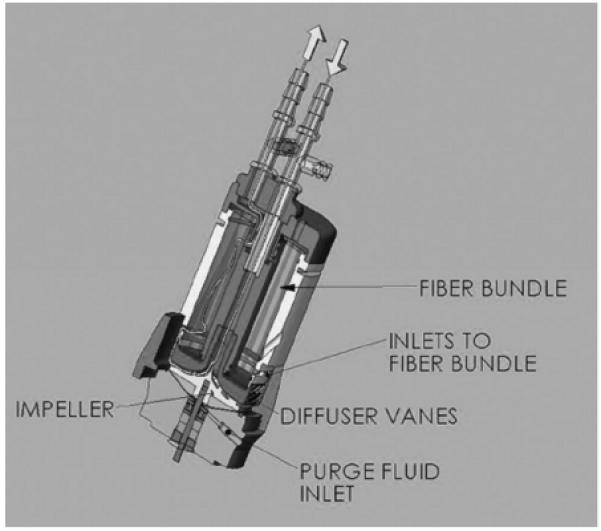
pCAS cross-section.
The pCAS system must be able to provide an adequate flow to restore the normal hemodynamic parameters while reducing volume, contact surface area, and hemolysis at the same time. The following design criterion has been laid down by the developers and is thought to be sufficient for the patient population described. The device must be capable of delivering flows of 1 L/min for children up to the weight of 10 kg, provide oxygen transfer ranging from 40-150 mL/min depending on the size of the patient (newborns require a calculated 22 mL/min and children a calculated 121 mL/min), and achieve a carbon-dioxide clearance of 32-120 mL/min (newborns require a removal of 17 mL/min and children a calculated 97 mL/min).
The entire unit consists of an integrated oxygenation fiber bundle and electrically driven pump. An inlet cannulae may be placed either into the right atrium if the chest is open or inserted into the jugular vein and advanced to the right atrium if a peripheral insertion is deemed appropriate by the surgeon. Similarly, the outlet cannulae may be placed directly into the aorta if the chest is opened or into a peripheral artery (i.e. the carotid). Once attached and primed the pump may be set to provide either pulsatile or continuous flow. This investigation is limited to the in vitro pumping performance testing of the pCAS when operated in continuous flow mode with inflow and outflow cannulae selection appropriate for a neonate.
In vitro pumping performance of Revision 4 of the pCAS was evaluated using a mock circulation loop that approximates the key anatomic features and hemodynamics of a small infant (Table 1). The mock loop system employs the use of two pneumatically driven, 10 cc VADs which simulate the native right and left ventricles. Atria are simulated through the use of 1 inch diameter bladder bags, and compliance is created through the use of 1/2” Penrose drain tubing in the pulmonary artery and descending aorta components of the loop. The remainder of the loop is a sequence of tubing which simulate the pulmonary and systemic circuits and incorporate adjustable pinch clamps to establish the needed vascular resistance in each region (Figure 2). Consistent with anticipated clinical use under conditions for neonatal support, the right atrium was cannulated with a 10 Fr. ECMO inflow cannula (Medtronic Bio-Medicus, Mineapolis MN); the aorta was cannulated with an 8 Fr. ECMO arterial cannula (Medtronic Bio-Medicus, Mineapolis MN) for the pump outflow. The cannulae were connected to the pCAS inlet and outlet using 60 cm of 1/2” I.D. bypass tubing. The total tip-to-tip priming volume of the cannulae, tubing and pump/oxygenator was 80 cc.
Table 1.
Mock loop parameters recorded during pCAS performance testing, TBD=To Be Determined.
| Parameter | Test Range |
|---|---|
| Mean AoP | 70-75 mmHg |
| Aortic Flow | 800-1000 mL/min |
| Left Atrial Pressure | 10-12 mmHg |
| Right Atrial Pressure | 8-10 mmHg |
| Pulmonary Art. Pressure | 18-22 mmHg |
| Coronary Flow | 45-55 mL/min |
| Carotid Flow | 90-110 mL/min |
| Left Driveline Pressure | 130-140 mmHg |
| Right Driveline Pressure | 40-45 mmHg |
| pCAS Flow | 0-6500(Rev. 4)/5000(Rev 5) |
| pCAS RPM | TBD |
| pCAS Inlet Pressure | TBD |
| pCAS Outlet Pressure | TBD |
Figure 2.
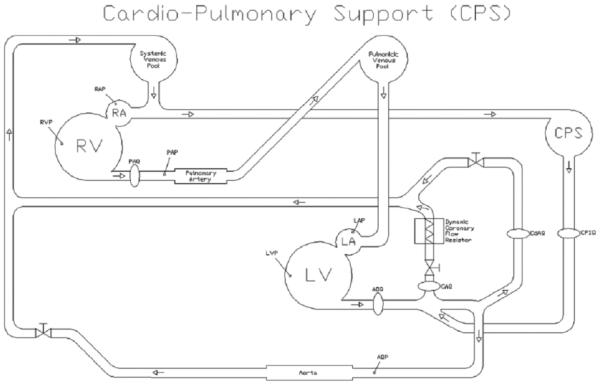
Schematic representation of the mock loop system during cardiopulmonary assist.
Right atrial pressure (RAP), left atrial pressure (LAP), pCAS inlet and outlet pressures, and aortic pressure (AoP) were measured with high fidelity pressure catheters (Millar Instruments, Houston, TX). The aortic flow (AOF), brachiocephalic flow (BCF), pulmonary artery flow (PAF), and the pCAS outflow were measured with ultrasonic, transit-time flow probes (Transonic Systems, Inc, Ithica, NY). All transducers were pre-calibrated against known standards to ensure measurement accuracy. Hemodynamic data was signal conditioned and analog-to-digitally converted at a sampling rate of 400 Hz and stored for digital data analysis using a Good Laboratory Practices compliant data acquisition system (DAQ)15.
The test fluid was a 40% glycerin/water, blood-analog fluid (μ = 3.7 cP @ 22°C @ 250 sec-1 comparable to a hematocrit of 45%). Each test run was initiated by establishing baseline hemodynamic conditions (heart rate = 120 bpm, cardiac output (CO) = 800 ml/min, mean AoP = 75 mm Hg, mean RAP = 4 to 8 mm Hg, and mean LAP = 8 to 12 mm Hg. These hemodynamic values were selected based on intra-operative data collected at Primary Children’s Hospital (Salt Lake City, UT) and Kosair Children’s Hospital (Louisville, KY) and ongoing animal experiments conducted in appropriately sized piglets 16-17. Pump-stop reverse flow was determined by unclamping the cannulae with the pump at 0 RPM. The RPM was initially increased until the zero-flow RPM, the setting at which no net flow passes through the pump, was identified. The RPM was then increased in 500 RPM increments with the systemic vascular resistance element of the mock circulation adjusted to maintain a mean AoP of 75 mm Hg for each RPM setting with the resulting pump outflow rate noted. The RPM increments were continued until the controller reached the maximum operating RPM. The test sequence was completed three times and the data at each test point averaged over the three runs.
The Revision 5 version of the pCAS resulted from a redesign of the pump impeller and diffuser that were anticipated to result in greater pCAS flow rates at lower RPM compared to the Revision 4 device. The controller for the new pump was connected and the Revision 5 pump primed in the same manner as the previous version. The tip-to-tip priming volume of the fifth revision was also 80 cc of the 40% glycerin solution. The same test protocol used for Revision 4 was used for Revision 5 using the same mock loop and DAQ system.
Results
At the maximum RPM of approximately 6500, an average flow rate of 0.42 L/min was delivered by the Revision 4 pCAS (Figure 3). As shown in Figure 3, as the RPM’s are increased, the change in pressure increases across the pump according to a second order equation, with a maximum difference of nearly 300 mmHg. Upon initial unclamping of the device a reverse flow equal to - 0.12 L/min was observed. The zero flow RPM setting was approximately 2700. The change in pressure across the cannulae was also measured. Inflow cannula pressure drop was defined as RAP-Inlet pressure and resulted in a maximum value of 47 mmHg at an inlet pressure of -41 mmHg. Outflow cannula drop was defined Outflow Pressure-AoP and was found to be 213 mmHg.
Figure 3.
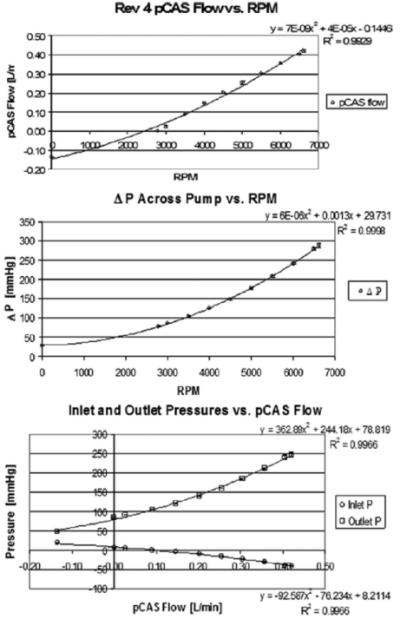
Results of the Revision 4 pCAS. Top: Flow rates produced by pump as RPMs are incrementally increased. Middle: Change in pressure drop (ΔP) across the pump as the RPMs are incrementally increased. Bottom: Change in inlet and outlet pressure as a function of pCAS flow.
The same inflow and outflow cannulas, mock loop and protocol were followed for the testing of the Revision 5 of the pCAS pump. As was anticipated, the larger, more efficient impeller produced higher flow rates at lower RPMs (Figures 4&5). Despite the improvement in impeller efficiency however, there still existed a large pressure difference between the pump inlet and outlet which was increased at the higher flow rates achieved with the newly revised pump (Figure 4). The reverse flow through the pump when the RPM was zero was -.15 L/min. The zero-flow speed of the revised pump was lowered to an average of 1870 RPM. At the maximum RPM setting of 5000, the flow rate was measured at 0.57 liters per minute, which is double that of the Revision 4 pCAS at the same RPM (Figure 5). The maximum pressure drop across the inflow cannula was seen to increase to 89 mmHg at an inlet pressure of -87mmHg. The maximum pressure drop across the outflow cannula was found to be 279 mmHg.
Figure 4.
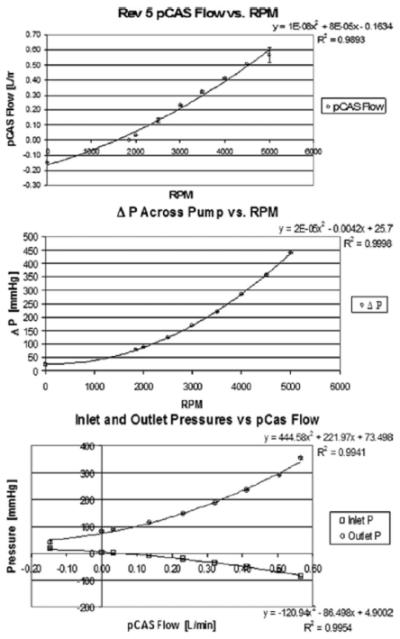
Results of Revision 5 pCAS. Top: Flow rates produced by pump as RPMs are incrementally increased. Middle: Change in pressure drop (ΔP) across the pump as the RPMs are incrementally increased. Bottom: Change in inlet and outlet pressure as a function of pCAS flow.
Figure 5.
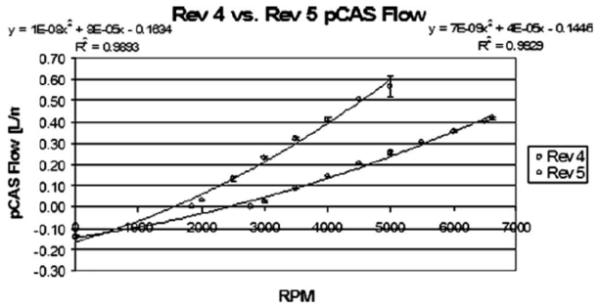
Comparison of flow rates between Revision 4 and Revision 5 as a function of RPM.
Discussion
The developing series of pCAS devices has demonstrated adequate pumping ability for neonates up to 5 kg. Modifications in the Revision 5 pCAS improved the pump performance at the same RPM compared to the Revision 4 pCAS. A major concern of pump operation for these tests is the lower inlet pressure at higher flow rates (Figures 3&4). This lower pressure is mostly do to the high resistance of the small cannulae used in this particular testing and the viscosity of the test fluid used. In previously published articles it has been shown that an extremely negative inflow pressure, one exceeding -20 mmHg, may result in high levels of hemolysis18.
Extreme or rapid changes in pressure can also be traumatic to blood cells and are therefore concerning as the blood moves from a very low inflow pressure to a very high outflow pressure. However, the mock circulation was created to represent a challenging clinical scenario, creating higher levels of resistance with the smallest cannula than may be seen during common use. In the animal testing of the Rev 4 pCAS, larger cannulae which would be more commonly used clinically in larger patients resulted in both higher flow rates (>1 L/min), and much smaller pressure gradients and inlet pressures than seen in the mock circulation experiments. This result would also be expected in a situation where the hematocrit was lower, such as neonates and infants with non-cyanotic heart disease. It is expected that during animal studies of the new revisions of the pCAS, similar performance improvements will be seen as well as definition of maximum acceptable flow rates and pump speeds permissible before creating unacceptable hemolysis as indicated by plasma free hemoglobin.
The new pCAS utilizes a small, versatile pump which is highly advantageous in a pediatric assist system. The ability to operate in both a continuous and pulsatile mode provides the ability to stabilize critically ill patients while still maintaining a reasonable level of systemic pulsatile flow that has been considered as a possible benefit19. It is the expectation that this device will offer access to life saving procedures to a wider range of pediatric patients or grant them a time period sufficient to recover diminished myocardial and pulmonary function while reducing the complications experienced with ECMO. The next revisions of the pCAS are already in early in vitro testing with initial chronic tests scheduled for the autumn of 2008. A pre-clinical readiness testing program is being planned for 2009 with initial clinical trials anticipated in 2010.
Conclusion
A small and portable cardiopulmonary assist device like the pCAS could provide a number of advantages in the treatment of pediatric patients. This device not only allows for stabilization of a failing heart or lungs, but may also provide adequate support for use during or after surgical procedures in which a pediatric patient needs to be placed on cardiopulmonary bypass. The Revision 4 and Revision 5 pCAS pump/oxygenator devices were tested in vitro under conditions comparable to a neonatal patient. Both devices delivered adequate flow rates for neonates up to 5 kg. The improved design of the Revision 5 pCAS was able to produce greater flow at a lower RPM which may reduce the hemolysis potential of the device in vivo. Final revisions of the pCAS are in progress as plans for pre-clinical testing are being considered.
Acknowledgement
Funding for this project was provided by the National Institutes of Health Heart, Lung and Blood Institute (Grant 2 R44 HL059810 and Contract No. HHSN268200449189C), the Jewish Hospital & St. Mary’s Foundation (Louisville, KY), and Kosair Charities.
Reference
- 1.Rose, et al. Long term use of Left Ventricular Assist Device for End Stage Heart Failure. New England Journal of Medicine. 2001;345(20):1435–1443. doi: 10.1056/NEJMoa012175. [DOI] [PubMed] [Google Scholar]
- 2.Baldwin JT, Borovetz HS, Duncan VW, Gartner MJ, Jarvik RK, Weiss WJ, Hoke TR. The National Heart Lung and Blood Institute Pediatric Ciruclatory Support Program. Circulation. 2006;113:147–155. doi: 10.1161/CIRCULATIONAHA.105.571422. [DOI] [PubMed] [Google Scholar]
- 3.Spencer FC, Eisemen B, Trinkle JK, Rossi NP. Assisted Circulation for Cardiac Failure Following Intracardiac Surgery with Cardiopulmonary Bypass. JThoracic.Cardiovasc.Surg. 1965;49:56–73. [PubMed] [Google Scholar]
- 4.Cooper DS, Jacobs JP, Moore L, Stock A, Gaynor JW, Chancy T, Parpard M, Griffin DA, Owens T, Checchia PA, Thiagarajan RR, Spray TL, Ravishankar C. Cardiac Extraorpreal Life Support: State of the Art in 2007. Cardiol Young. 2007;17:104–115. doi: 10.1017/S1047951107001217. [DOI] [PubMed] [Google Scholar]
- 5.Tamblyn J. 5-13-2003. Ref Type: Personal Communication.
- 6.Pennington DG. Commentary on Circulatory Support in Infants and Children. Semin.Thorac.Cardiovasc.Surg. 1994;6:154–60. [PubMed] [Google Scholar]
- 7.Karl TR. Extracorporeal Circulatory Support in Infants and Children. Semin.Thoracic.Cardiovasc.Surg. 1994;6:154–60. [PubMed] [Google Scholar]
- 8.Trento A, Thompson A, Siewers Rea. Extracorporeal Membrane Oxygenation in Children, New Trends. J Thorac.Cardvasc.Surg. 1986;96:542–47. [PubMed] [Google Scholar]
- 9.Fuhrman BP, Dalton HJ. Progress in Pediatric Extracorporeal Membrane Oxygenation. Crit Care Clin. 1992;8:191–202. [PubMed] [Google Scholar]
- 10.Hilt T, Grave DF, Chernin JM, Angel CA, Herndon DN, Zwischenberger JB. Successful Use of Extracorporeal Membrane Oxygenation to Treat Severe Respiratory Failure in a Pediatric Patient with a Scald Injury. Crit Care Nurse. 1998;18:63–72. [PubMed] [Google Scholar]
- 11.Baldwin JT, Borovetz HS, Duncan BW, Gartner MJ, Jarvik RK, Weiss WJ, Hoke TR. The National Heart, Lung and Blood Institue Pediatric Circulatory Support Program. Circulation. 2006;113:147–155. doi: 10.1161/CIRCULATIONAHA.105.571422. [DOI] [PubMed] [Google Scholar]
- 12.Stern D. The Intrapersonal World of the Infant. Basic Books; New York: 1985. [Google Scholar]
- 13.Siegel D, Hartzell M. Parenting from the Inside Out. Putnam; New York: 2003. [Google Scholar]
- 14.Siegel D. The Developing Mind. Guilford Press; New York: 1999. [Google Scholar]
- 15.Koenig SC, Woolard C, Drew SD, Unger L, Gillars KJ, Ewert DL, Gray LA, Pantalos GM. Integrated Data Acquisition System for Medical Device Testing and Physiology Research in Compliance with Good Laboratory Practices. Biomed Instr & Tech. 2004;38(3):229–240. doi: 10.2345/0899-8205(2004)38[229:IDASFM]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Pantalos GM, Giridharan G, Colyer J, Mitchell M, Speakman J, Lucci C, Johnson G, Gartner M, Koenig SC. Effect of Continous and Pulsatile Flow Left Ventricular Assist on Pulsatility in a Pediatric Animal Model of Left Ventricular Dysfunction: Pilot Observation. ASAIO Journal. 2007;53(3):385–391. doi: 10.1097/MAT.0b013e318050d210. [DOI] [PubMed] [Google Scholar]
- 17.Pantalos GM, Minich LL, Tani LY, McGough EC, Hawkins JA. Estimation of Timing Errors for the Intraaortic Balloon Pump Use in Pediatric Patients. ASAIO Journal. 1999;45(3):166–171. doi: 10.1097/00002480-199905000-00012. [DOI] [PubMed] [Google Scholar]
- 18.Thuys TA, Mullay RJ, Horton SB, O’Connor EB, Cochrane AD, Brizard CPR, Karl TR. Centrifugal Ventricular Assist in Children Under 6 kg. European journal of Cardiothoracic Surgery. 1998;13:130–134. doi: 10.1016/s1010-7940(97)00310-2. [DOI] [PubMed] [Google Scholar]
- 19.Undar A: Pulsatile versus nonpulsatile cardiopulmonary bypass procedures in neonates and small infants: from bench to clinical practice. ASSIO J. 2005;51:vi–x. doi: 10.1097/01.mat.0000178215.34588.98. [DOI] [PubMed] [Google Scholar]