

Abstract
Purpose
To investigate the pathways from level of education to low back pain (LBP) in the adult population, especially concerning the role of physical working constraints, and personal factors (overweight, tobacco consumption, and tallness).
Methods
The study population consisted of 15 534 subjects from the National Health Survey, with data on LBP, level of education, personal factors, and physical working constraints. Logistic models for LBP (pain more than 30 days during the previous 12 months) were compared in order to check the consistency of the data with specific causal pathways.
Results
LBP was strongly associated with level of education. This association was almost completely explained if present or past exposure to tiring work postures and handling of heavy loads were taken into account. For men, the OR for “no diploma”, adjusted only for age, was 1.75; it was 1.02 after additional adjustment on physical work factors. Personal factors played also a role, especially overweight for women. Among them, the OR associated with a Body Mass Index equal to 27 or more was 1.58 after adjustment on all the other factors.
Conclusions
In this national population the main pathways from education to LBP were through occupational exposure and lifestyle factors.
Keywords: Adult, Age Factors, Aged, Demography, Educational Status, Employment, Female, France, epidemiology, Humans, Life Style, Low Back Pain, epidemiology, etiology, psychology, Male, Middle Aged, Occupational Diseases, epidemiology, etiology, psychology, Occupational Exposure, adverse effects, Prevalence, Risk Factors
Keywords: low back pain, education, occupational exposure, lifestyle
A low level of education is associated with various diseases and conditions, including musculoskeletal disorders and more specifically low back pain (LBP) (Dionne et al. 2001; Aittomäki et al. 2007; Hagen et al. 2005; Schmidt et al. 2007). Associations between LBP and occupation have been much studied, since physical demands at work play a role in incidence and prevalence of LBP (Lund et al. 2006; Hoogendoorn et al. 1999). A study in Finland found that physical work factors explain most of the occupational class gradient in musculoskeletal disorders (Aittomäki et al 2007). A study of injury rates among Massachusetts hospital workers reached similar conclusions (d’Errico et al 2007).
The causal processes linking education and health are not well known (Blane 2003). This is the situation also for LBP in adulthood. Access to and quality of care are probably relatively unimportant, since most patients recover quickly from episodes of common LBP (Andersson 1999). Causal mechanisms that may play a role in the consequences of back pain, such as sick leave, probably differ from those related to its incidence and recurrence (Dionne et al. 2001; Andersson 1999; Hagen et al. 2006). Generally speaking, the outcome of LBP is likely to affect the magnitude of and explanations for the associations between LBP and socioeconomic status (Dionne et al. 2001; Hagen et al. 2006). Similarly, the magnitude of the associations between LBP and most of its risk factors will depend on the specific definition and outcome measures chosen (Griffith et al. 2007; Ozguler et al. 2000).
Education may affect the incidence and duration of LBP through lifestyle factors such as smoking or obesity (Goldberg et al. 2000; Lake et al. 2000; Power et al. 2001). While height (tallness) is reported to be a risk factor for LBP in some studies (Kopek et al. 2004; Leino-Arjas et al. 1998) it should not explain the higher frequency of LBP among the less educated, since being tall is associated with a higher educational level (Cavelaars et al. 2000).
Other potential intermediate factors are general stress and occupational psychosocial factors (Kopek, 2004), and sociocultural factors such as beliefs about back pain, which have an important role in disability associated with LBP, and might also play a role for duration of pain and self-assessment of back pain (Buckbinder, 2001, Skovron, 1994; van Tulder, 2002). Occupational exposure might be an intermediate factor. Most studies of the role of occupational risk factors have emphasized occupation more than education, partly because the proximal factor (occupation) is expected to be a stronger determinant than the more distant factor. Another reason is that occupational risk factors are a clear target for prevention (Schneider et al. 2005).
This study of more than 15 000 members of the French general population aged 30 to 69 years describes the associations between LBP and education for a specific outcome — LBP for more than 30 days during the previous 12 months, a definition similar to “long-lasting or frequent LBP” (Griffith et al. 2007). Our objective was to describe the frequency of LBP and associated factors and to help improve our understanding of pathways from education to LBP.
Methods
Subjects
The data come from the EDS (Enquête Décennale Santé), a national survey conducted in 2002–2003 by INSEE, the agency responsible for censuses and compulsory surveys (Lanoe and Makdessi-Raynaud, 2005).
A trained interviewer visited each subject at home three times. In addition to providing oral information to the interviewer, participants were asked to complete a self-administered questionnaire. Our study sample is composed of the 18 002 subjects aged 30 to 69 years who were visited three times. Weighting based on this sample enabled us to calculate figures for the entire population of France.
Low back pain
The self-administered questionnaire included a French version of the Nordic Questionnaire for the analysis of musculoskeletal symptoms (Kuorinka et al. 1987). The main definition used here for LBP was pain in the previous year for at least 30 days (at least 30 days but not daily, or pain everyday).
The interviewer considered that 210 of the 18 002 subjects in the target population (1 %) were unable to complete a questionnaire. Another subgroup of 114 subjects (0.6 %) had to be excluded because of missing data for several LBP questions. A final group (n=2144, 12 %) did not complete the LBP questionnaire at all. Hence the study population consisted of 15 534 subjects: 7292 men and 8242 women.
Study variables
Personal factors in this study were those considered to be potential risk factors for LBP: gender, age (in four categories), height (two categories), body mass index (BMI) (three categories), and tobacco consumption (three categories). For height, the cutoff between the categories was 180 cm for men and 170 for women.
Three variables described socioeconomic status: level of education, present or past occupation, and household income. Education had five categories: none or did not complete elementary school; elementary level or other low level general diploma; low level vocational diploma, medium-high level general diploma (“baccalaureate”), higher education (at least two years after baccalaureate).
Occupation was coded according to the French nomenclature, for the present occupation or (for those not in the labor force at the time of the survey) for the longest job held in the past. Only nine men and 321 women had missing data for occupation.
Household income was classified in four categories.
Two variables describing physical working constraints were based on the self-administered questionnaire: tiring work posture and handling heavy loads. The subjects were asked to indicate the duration of exposure (never, less than 10 years, 10 to 20 years, more than 20 years) in the present job, or in the longest job held in the past for those not in the labor force at the time of the survey.
In addition, employment status and income source was used for descriptive purposes only, with six mutually exclusive categories: employed; unemployed looking for a job; retired; housewife; receiving permanent disability benefits; other unemployed. These categories have previously been used for the study of chronic back problems in France (Leclerc et al. 2006). Of the three variables describing socioeconomic status, educational level was the only one taken into account in the models, since our objective was to study the respective roles of education and physical constraints at work in the causal pathway leading to LBP. Income level may be a consequence of chronic LBP (Stronks et al. 1997). Occupation may be considered an intermediate variable for it is both a consequence of education and a determinant of work-related risk factors.
Analyses
In a preliminary stage, we compared the study and target populations. Population employment status and income source (weighted results) were also described according to LBP.
The frequency of LBP in the population was described separately for men and women, according to the variables mentioned above. Confidence intervals were calculated with the SAS Proc Surveymeans procedure.
The main part of the analyses focused on education and the personal and occupational factors that might explain the associations between education and LBP. For bivariate analyses in the study population, chi-square tests were used. Logistic models were also used, with LBP as the variable of interest. Unweighted models were used, since previous results indicated that weighted and unweighted results were very similar.
Four models were compared, separately for men and women:
Model 1, education and age as explanatory variables.
Model 2A, education, age, and personal factors.
Model 2B, education, age, and physical constraints at work.
Model 3, education, age, personal factors, and physical constraints at work.
In models 2A and 2B, the variables in the initial models were those associated with LBP at a p-level of 20% (unadjusted) for men or women, except occupation and income, which were not included. The variables in final models 2A and 2B were education, age, and those associated with LBP in the model at a p-level of 10% or less.
Model 3 included education, age, and all the variables in final models 2A and 2B.
Since duration of exposure to physical occupational risk factors is closely associated with age, the two occupational risk factors were considered in the models with two categories, never or ever exposed, irrespective of duration.
All the models were based on a sample without any missing values (6811 men and 7013 women).
The third part of the analyses (tables not given) consisted of additional analyses aimed at a better understanding of complementary aspects: relations between education, lifestyle risk factors and height; role of occupation as an intermediate risk factor (associations with education, and physical work exposure), links between education and physical work exposure, and the sensitivity of the results to the “LBP” and “no LBP” definitions used.
Results
The 210 subjects unable to complete a questionnaire were older (28% were 60 years or older), and 76% were in the lowest educational category. The 114 with missing data for LBP were also older and less educated. The 2144 who did not complete the LBP questionnaire did not differ much from the rest of the sample, except that they were less educated.
The population estimates for LBP at least one day in the previous 12 months were 53.4% for men and 57.4% for women. LBP for 30 days or more in the previous year was reported by 15.6% of the men and 19% of the women, which corresponds to estimates of 15.8% and 19.3%, respectively, in the overall French population. As Table 1 shows, 67% of the men in the population reporting LBP were working (compared with 75% for those reporting no LBP or shorter duration). Among those unemployed, retirement was the most frequent situation. Among those in the LBP group, 3.1% were classified in “permanent disability benefits” (1.3% in the rest of the sample). For women the situation was rather similar; 3.2% of women with LBP were receiving permanent disability benefits.
Table 1.
Subjects with and without LBP according to employment status and source of income Number of subjects, and distribution (weighted results) in the target population.
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| LBP more than 30 days | No LBP or shorter duration | LBP more than 30 days | No LBP or shorter duration | |||||
| N= | Percentages (weighted results) | N= | Percentages (weighted results) | N= | Percentages (weighted results) | N= | Percentages (weighted results) | |
| Employed | 762 | 66.8 | 4624 | 74.7 | 855 | 53.0 | 4096 | 60.1 |
| Unemployed, looking for a job | 47 | 4.2 | 264 | 4.3 | 72 | 4.7 | 315 | 4.8 |
| Retired | 250 | 22.1 | 1081 | 17.6 | 297 | 19.4 | 941 | 14.5 |
| Housewife | 229 | 14.5 | 1056 | 16.2 | ||||
| Permanent disability benefits | 36 | 3.1 | 73 | 1.3 | 44 | 3.2 | 54 | 1.0 |
| Other unemployed | 43 | 3.8 | 112 | 2.0 | 72 | 5.1 | 211 | 3.3 |
| Total | 1138 | 100 | 6154 | 100 | 1569 | 100 | 6673 | 100 |
LBP according to personal, socioeconomic and occupational factors (Table 2)
Table 2.
Frequency of LBP more than 30 days according to personal, socioeconomic, and occupational factors
| Men | Women | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N (1) | Prevalence (2) | 95 % CI (2) | P (3) | N (1) | Prevalence (2) | 95 % CI (2) | P (3) | ||
| Age | 30–39 | 1997 | 12.42 | [10.83 – 14.02] | <0.0001 | 2379 | 14.74 | [13.18 – 16.30] | <0.0001 |
| 40–49 | 2139 | 14.43 | [12.80 – 16.07] | 2407 | 19,57 | [17.82 – 21.32] | |||
| 50–59 | 1918 | 18.63 | [16.68 – 20.59] | 2049 | 22,03 | [20.06 – 24.01] | |||
| 60–69 | 1238 | 19.42 | [16.99 – 21.85] | 1407 | 22,79 | [20.40 – 25.17] | |||
| Tallness (4) | No | 5976 | 15.65 | [14.63 – 16.67] | 0.42 | 7575 | 19.02 | [18.05 – 19.99] | 0.04 |
| Yes | 1316 | 16.27 | [14.06 – 18.49] | 667 | 23.14 | [19.60 – 26.69] | |||
| Tobacco consumption | Non smoker | 3151 | 13.91 | [12.57 – 15.24] | 0.003 | 5284 | 18.88 | [17.72 – 20.04] | 0.07 |
| Ex-smoker | 1764 | 18.17 | [16.17 – 20.17] | 970 | 21.71 | [18.86 – 24.55] | |||
| Smoker | 2377 | 16.45 | [14.81 – 18.09] | 1988 | 19.39 | [17.48 – 21.29] | |||
| BMI | Less than 24 | 2399 | 12.99 | [11.53 – 14.45] | <0.0001 | 4576 | 16.40 | [15.23 – 17.58] | <0.0001 |
| 24 to 27 | 2558 | 16.27 | [14.67 – 17.88] | 1803 | 19.83 | [17.82 – 21.85] | |||
| 27 and more | 2335 | 18.05 | [16.33 – 19.78] | 1863 | 25.77 | [23.58 – 27.97] | |||
| Education | high | 1844 | 12.42 | [10.80 – 14.04] | <0.0001 | 2077 | 15.34 | [13.69 – 16.99] | <0.0001 |
| Medium-high, general | 948 | 12.38 | [10.11 – 14.64] | 1184 | 15.52 | [13.33 – 17.71] | |||
| Lower vocational | 2292 | 16.35 | [14.71 – 17.98] | 1947 | 21.34 | [19.36 – 23.31] | |||
| Primary | 1176 | 17.01 | [14.60 – 19.41] | 1758 | 21.43 | [19.34 – 23.52] | |||
| No diploma | 1032 | 20.03 | [17.37 – 22.69] | 1275 | 21.43 | [18.96 – 23.90] | |||
| Occupation (5) | Farmer | 315 | 16.54 | [11.72 – 21.36] | 0.0003 | 234 | 21.63 | [15.78 – 27.49] | 0.008 |
| Self-employed | 580 | 15.08 | [11.75 – 18.41] | 326 | 15.36 | [11.13 – 19.59] | |||
| Professional | 1514 | 14.27 | [12.29 – 16.25] | 932 | 15.62 | [13.17 – 18.08] | |||
| Intermediate | 1799 | 13.91 | [12.17 – 15.66] | 1816 | 18.53 | [16.55 – 20.50] | |||
| Employee | 769 | 15.52 | [12.72 – 18.32] | 3584 | 20.49 | [19.04 – 21.93] | |||
| Blue-collar worker | 2306 | 17.98 | [16.28 – 19.67] | 1029 | 20.66 | [18.01 – 23.32] | |||
| Annual household income (€ per unit) | More than 21 000 | 2003 | 13.56 | [11.89 – 15.23] | 0.01 | 2083 | 18.07 | [16.23 – 19.91] | 0.01 |
| 15 000 to 21 000 | 1766 | 16.15 | [14.28 – 18.03] | 1936 | 17.83 | [15.98 – 19.68] | |||
| 10 000 to 15 000 | 1984 | 16.68 | [14.87 – 18.49] | 2245 | 21.11 | [19.27 – 22.95] | |||
| Less than 10 000 | 1539 | 16.63 | [14.56 – 18.69] | 1978 | 19.78 | [17.85 – 21.70] | |||
| Tiring postures at work (years) | Never | 4078 | 11.29 | [10.23 – 12.35] | <0.0001 | 4538 | 15.95 | [14.79 – 17.11] | <0.0001 |
| Less than 10 | 802 | 15.93 | [13.18 – 18.69] | 995 | 24.05 | [21.17 – 26.93] | |||
| 10 to less than 20 | 751 | 21.06 | [17.90 – 24.23] | 690 | 24.03 | [20.55 – 27.51] | |||
| More than 20 | 868 | 26.30 | [23.07 – 29.54] | 485 | 30.03 | [25.53 – 34.52] | |||
| Yes, unknown duration | 350 | 17.55 | [13.14 – 21.66] | 369 | 22.07 | [17.52 – 26.63] | |||
| Missing value | 443 | 21.63 | [17.39 – 25.87] | 1165 | 19.31 | [16.77 – 21.84] | |||
| handling heavy loads (years) | Never | 3949 | 10.53 | [9.50 – 11.56] | <0.0001 | 5215 | 16.01 | [14.93 – 17.09] | <0.0001 |
| Less than 10 | 979 | 17.61 | [15.01 – 20.21] | 760 | 25.13 | [21.75 – 28.50] | |||
| 10 to less than 20 | 774 | 20.66 | [17.54 – 23.78] | 543 | 29.98 | [25.83 – 34.13] | |||
| More than 20 | 777 | 28.04 | [24.55 – 31.52] | 283 | 35.13 | [28.93 – 41.33] | |||
| Yes, unknown duration | 386 | 18.13 | [13.95 – 22.32] | 276 | 26.80 | [21.21 – 32.29] | |||
| Missing value | 427 | 20.72 | [16.45 – 25.00] | 1165 | 18.68 | [16.19 – 21.17] | |||
Number of subjects in the study population
Prevalence and confidence interval in the target population (weighted).
p-value, test comparing prevalences in the study population, Chi-square test.
More than 180 cm for men, more than 170 cm for women.
nine men and 321 women with missing data for occupation.
Prevalence of LBP increased with age for men and women. Taller women had a higher risk, whereas the association with height was not significant for men. The risk was higher among ex-smokers of both sexes and was strongly associated with high BMI. LBP was associated with education, occupation, and income; however, the strongest association for both sexes was with education.
A dose-response relation was observed with duration of exposure to tiring postures and handling of heavy loads.
Generally speaking, the weighted and unweighted prevalences were very close.
Contribution of personal factors and physical working constraints to the association between LBP and education
For men (Table 3) both age and education were associated with LBP in model 1. The association with education was not modified when tobacco consumption, height and BMI were taken into account (model 2A). These three personal risk factors were significantly associated with LBP at a p-level of 10%. When tiring postures and handling heavy loads were taken into account (model 2B), the association with education was no longer significant at a p-level of 10%. The strongest association with LBP in this model was for “ handling heavy loads ”. The associations between LBP and physical working constraints were similar in model 3, which took into account both personal and occupational factors.
Table 3.
LBP and level of education, role of personal and occupational factors; logistic models for men
| Model 1 | Model 2A | Model 2B | Model 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | ||
| Age | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |||||||||
| 30–39 | 1 | 1 | 1 | 1 | |||||||||
| 40–49 | 1.19 | [0.98 – 1.43] | 1.19 | [0.98 – 1.43] | 1.27 | [1.05 – 1.54] | 1.27 | [1.05 – 1.54] | |||||
| 50–59 | 1.62 | [1.34 – 1.95] | 1.60 | [1.32 – 1.94] | 1.74 | [1.44 – 2.10] | 1.73 | [1.43 – 2.10] | |||||
| 60–69 | 1.71 | [1.38 – 2.11] | 1.75 | [1.40 – 2.18] | 1.82 | [1.47 – 2.26] | 1.87 | [1.49 – 2.33] | |||||
| Education | <0.0001 | <0.0001 | 0.11 | 0.08 | |||||||||
| high | 1 | 1 | 1 | 1 | |||||||||
| Medium-high | 1.09 | [0.86 – 1.38] | 1.06 | [0.84 – 1.35] | 0.90 | [0.71 – 1.15] | 0.89 | [0.70 – 1.13] | |||||
| Low vocational | 1.39 | [1.16 – 1.67] | 1.35 | [1.12 – 1.62] | 0.89 | [0.73 – 1.09] | 0.87 | [0.71 – 1.07] | |||||
| Primary | 1.17 | [0.94 – 1.47] | 1.13 | [0.90 – 1.42] | 0.77 | [0.60 – 0.97] | 0.75 | [0.59 – 0.95] | |||||
| No diploma | 1.75 | [1.41 – 2.18] | 1.70 | [1.36 – 2.12] | 1.02 | [0.81 – 1.30] | 1.01 | [0.79 – 1.28] | |||||
| Tobacco consumption | 0.004 | 0.02 | |||||||||||
| Non-smoker | (1) | 1 | (1) | 1 | |||||||||
| Ex-smoker | 1.21 | [1.02 – 1.43] | 1.19 | [1.00 – 1.41] | |||||||||
| Smoker | 1.28 | [1.10 – 1.51] | 1.24 | [1.06 – 1.46] | |||||||||
| Height, more than 180 cm | 0.04 | 0.04 | |||||||||||
| No | (1) | 1 | (1) | 1 | |||||||||
| Yes | 1.19 | [1.01 – 1.42] | 1.20 | [1.01 – 1.43] | |||||||||
| BMI | 0.06 | 0.12 | |||||||||||
| Less than 24 | (1) | 1 | (1) | 1 | |||||||||
| 24 to 27 | 1.15 | [0.97 – 1.37] | 1.15 | [0.97 – 1.36] | |||||||||
| 27 and more | 1.22 | [1.03 – 1.45] | 1.19 | [1.00 – 1.41] | |||||||||
| Tiring postures | <0.0001 | <0.0001 | |||||||||||
| Never | (1) | (1) | 1 | 1 | |||||||||
| Ever | 1.49 | [1.26 – 1.76] | 1.49 | [1.26 – 1.76] | |||||||||
| handling heavy loads | <0.0001 | <0.0001 | |||||||||||
| Never | (1) | (1) | 1 | 1 | |||||||||
| Ever | 1.83 | [1.54 – 2.17] | 1.81 | [1.52 – 2.15] | |||||||||
Not in the model
For women (table 4) the association with the lowest educational level in model 1 was smaller than for men. The association with education was weaker when personal factors were taken into account (model 2A). Overweight and height were more closely associated with LBP in women than men. Model 2B indicated that physical working constraints played an important role; controlling for them, the only educational category with a significantly elevated OR was “low vocational”. No significant association with education remained in model 3.
Table 4.
LBP and level of education, role of personal and occupational factors; logistic models for women
| Model 1 | Model 2A | Model 2B | Model 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | ||
| Age | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |||||||||
| 30–39 | 1 | 1 | 1 | 1 | |||||||||
| 40–49 | 1.33 | [1.13 – 1.56] | 1.34 | [1.13 – 1.57] | 1.39 | [1.18 – 1.64] | 1.40 | [1.19 – 1.65] | |||||
| 50–59 | 1.52 | [1.28 – 1.80] | 1.52 | [1.28 – 1.81] | 1.63 | [1.37 – 1.93] | 1.62 | [1.36 – 1.94] | |||||
| 60–69 | 1.67 | [1.37 – 2.03] | 1.69 | [1.38 – 2.08] | 1.80 | [1.48 – 2.20] | 1.82 | [1.48 – 2.24] | |||||
| Education | <0.0001 | 0.004 | 0.06 | 0.11 | |||||||||
| high | 1 | 1 | 1 | 1 | |||||||||
| Medium-high | 1.00 | [0.81 – 1.22] | 0.99 | [0.80 – 1.21] | 0.98 | [0.80 – 1.21] | 0.98 | [0.80 – 1.20] | |||||
| Low vocational | 1.42 | [1.20 – 1.68] | 1.34 | [1.13 – 1.59] | 1.23 | [1.03 – 1.46] | 1.18 | [0.99 – 1.40] | |||||
| Primary | 1.36 | [1.13 – 1.62] | 1.26 | [1.05 – 1.52] | 1.12 | [0.93 – 1.35] | 1.06 | [0.88 – 1.28] | |||||
| No diploma | 1.27 | [1.03 – 1.57] | 1.17 | [0.94 – 1.44] | 0.97 | [0.79 – 1.21] | 0.92 | [0.74 – 1.14] | |||||
| Tobacco consumption | 0.002 | 0.006 | |||||||||||
| Non smoker | (1) | 1 | (1) | 1 | |||||||||
| Ex-smoker | 1.35 | [1.13 – 1.62] | 1.33 | [1.11 – 1.60] | |||||||||
| Smoker | 1.19 | [1.02 – 1.38] | 1.14 | [0.98 – 1.32] | |||||||||
| Height, more than 170 cm | 0.006 | 0.005 | |||||||||||
| No | (1) | 1 | (1) | 1 | |||||||||
| Yes | 1.34 | [1.09 – 1.65] | 1.35 | [1.09 – 1.66] | |||||||||
| BMI | <0.0001 | <0.0001 | |||||||||||
| Less than 24 | (1) | 1 | (1) | 1 | |||||||||
| 24 to 27 | 1.15 | [0.98 – 1.34] | 1.12 | [0.96 – 1.31] | |||||||||
| 27 and more | 1.67 | [1.44 – 1.94] | 1.58 | [1.36 – 1.83] | |||||||||
| Tiring postures | 0.0004 | 0.0006 | |||||||||||
| Never | (1) | (1) | 1 | 1 | |||||||||
| Ever | 1.32 | [1.13 – 1.54] | 1.31 | [1.12 – 1.52] | |||||||||
| handling heavy loads | <0.0001 | <0.0001 | |||||||||||
| Never | (1) | (1) | 1 | 1 | |||||||||
| Ever | 1.75 | [1.49 – 2.05] | 1.70 | [1.45 – 2.00] | |||||||||
Not in the model
Additional analyses
Relationship between education and lifestyle risk factors and height
Men with low educational levels were more often smokers, while those with more education were relatively frequently ex-smokers. Strong associations between education and BMI were observed, especially among women. Among them the frequency of a BMI of 27 or more was 35.1% in the lowest educational category and 11.4% in the highest.
Tallness was more frequent among those most educated. The percentage of men taller than 180 cm ranged from 12.7% in the group with the least education to 24.1% for those with the most; the corresponding figures for women taller than 170 cm were 4.4% and 11.9%.
Occupation, education, and physical work exposure
Our first hypothesis was that a part of the pathway from education to LBP was through occupation. The links between education and occupation were not very strong, however. Logistic models conducted separately for men and women (figures not given) indicated that education remained a risk factor of LBP for men when occupation was taken into account and that having the lowest educational level had a stronger effect than being a blue-collar worker. LBP in women was also more strongly associated with education than with occupation.
The level of exposure to physical work factors was associated not only with occupation but also education. This held true especially for men and women classified as farmers and self-employed. Similar results were observed among women in intermediate occupations, a category that includes health care workers.
Education (alone) was a strong predictor for physical work exposure. For men, the frequency of tiring postures was highest (63%) among those with the least education and 53% for those with a vocational diploma; the lowest frequencies were for the highest (15%) and next highest (28%) educational levels. Results were similar for handling of heavy loads: in ascending order of educational levels, frequency of exposure was 65%, 53%, 56%, 32% and 13%. A strong contrast between educational categories was also observed among women. The highest percentages were observed for the lowest educational levels: 55% for tiring postures and 41% for handling of heavy loads. The lowest frequencies, conversely, were for those with the highest level: 22% and 15%, respectively.
Sensitivity of the results to the definition used for LBP, and to the reference group
With a broader definition for the outcome - LBP at least one day in the previous 12 months - the associations were much weaker. Among women, no significant association was observed with education; among men the relation to education was borderline for significance (p=0.051), and the trends were similar to those for LBP for more than 30 days.
If LBO for at least 30 days was compared to a reference group comprising only those without LBP, the link between LBP and level of education was slightly stronger for men, and slightly les strong for women. For men the OR for “no diploma” in model 1 was 1.79 instead of 1.75, for women it was 1.21 instead of 1.27. As in the models presented in tables 3 and 4, the excess of LBP in the lowest educational levels disappeared if physical work exposure variables were included in the models.
Discussion
This study suggest that the main pathways from education to LBP are through occupational exposure and lifestyle factors. Height had a special position, for it is both a risk factor for LBP and associated with a higher educational level. Figure 1 is intended to illustrate the results, rather than provide a general overview of mechanisms leading to LBP. It would not necessarily apply to LBP at all ages or to all dimensions of LBP (Mustard et al. 2005).
Figure 1.
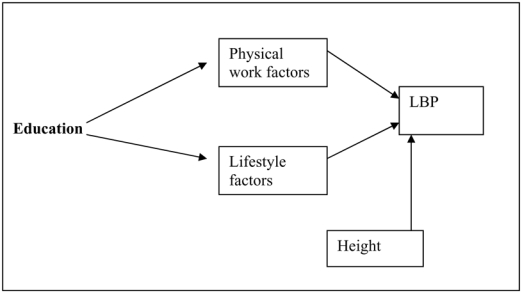
Illustration of the results, pathways between education and low back pain (LBP)
A national population-based survey offers the advantage of yielding estimates for the entire population, taking into account weights derived from the sample design (Leclerc et al. 2006). The study includes self–employed workers as well as those not in the labor force, which is not the case for other surveys of LBP. Information on past occupational exposure was more accurate than in most comparable population surveys, and LBP was assessed with a rather detailed questionnaire.
Risk indicators and risk factors for LBP, comparisons with other studies
Most but not all cross-sectional and longitudinal studies have observed a relationship between education and LBP prevalence (Dionne et al. 2001). In this study, associations with LBP were due mainly to two categories — those with the lowest educational level and those with vocational training, which are sometimes grouped with other categories. This might explain results from other studies in which an association with education was not found (Kopek et al. 2004) or observed only for women (Croft and Rigby 1994).
The associations with occupational factors were expected. Concerning the role of those factors, a German study concluded that they did not explain the relation between education and severe back pain (Latza et al. 2000). However, these results were based on a rather small sample of subjects with past history of back pain. Other authors have suggested that a lifetime perspective is important in understanding the mechanisms leading to musculoskeletal disorders (Khatun et al. 2004; Sainio et al. 2007).
Tobacco consumption and BMI were associated with LBP in this study. Some previous studies found these associations only for men or only for women (Leboeuf-Yde 1999; Goldberg et al. 2000; Lake et al. 2000; Leino-Arjas et al. 1998; Mustard et al. 2005; Power et al. 2001).
In the logistic models, LBP was associated with height, especially for women. A more detailed analysis of the frequency of LBP according to height also indicated that the association was stronger for women. Some studies have observed such an association only for men (Kopek et al. 2004) or only for women (Leino-Arjas et al. 1998).
Potential limitations of the study
The principal limitation of this survey was its cross-sectional design. However, most large population surveys comparable to the EDS are also cross-sectional (Kopek et al. 2004). Subjects with missing data for LBP were less educated, and the weights that we used for estimating prevalence in the general population did not correct for the completeness of specific questionnaires such as the LBP questionnaire. For that reason the prevalence of LBP 30 days or more in the population could be slightly underestimated. However, consequences for associations between LBP and various factors are expected to be negligible.
Exposure to risk factors was self-assessed. For educational level, height, BMI, or tobacco consumption, self-assessed measures may be imprecise or over- or underestimated. Differential misclassification (distribution of errors depends on presence of LBP) is unlikely however.
Those with LBP may overestimate their past occupational exposure (Stock et al. 2005). Here differential recall bias for past exposure was probably limited, since the survey did not focus on LBP but on health in general.
Another potential problem with a cross-sectional design is reverse causation or selection. Suffering from LBP might lead to a reduction of occupational exposure. Past exposure, however, includes exposure before LBP onset. There is no such problem for education, since LBP at school age is not expected to have consequences on education.
Psychosocial factors at work, which are potential risk factors for LBP, were not taken into account (Hoogendoorn et al. 2000). Since these variables were available only for those who held a job at the time of the survey. Additional analyses limited to this subsample indicated that associations between LBP and both education and physical work factors were unchanged when psychosocial factors were also taken into account.
We did not take into account the presence of psychological problems. Associations between LBP and psychological problems would have been difficult to interpret, since the presence of psychological problems is both a potential risk factor, and a consequence of chronic LBP (Andersson 1999; Linton 2000; Hurwitz et al. 2003; Dersh et al. 2007).
The role of two possible pathways from socioeconomic position to LBP could not be studied in this study: the first one is chronic stress in general (Kopek et al. 2004), which could be associated to LBP and also related to report of physical work exposure, especially since physical work exposure was self-assessed. The second one is sociocultural factors such as beliefs about back pain (Buchbinder, 2001, Skovron et al. 1994; van Tulder et al. 2002). How people understand and interpret back pain is expected to be related to education. However, the effects on LBP in general (rather than chronic or disabling LBP) has not been much studied. It would be interesting to study the role of these factors as an explanation to social differences in prevalence of LBP in the general population.
Mechanisms, role of occupation and education
In studies of LBP, occupation is often taken as a proxy for occupational exposure. An explanation for the limited role of occupation in our study may well be that occupation was not known very precisely, especially for self-employed workers. On the other hand, occupation may be less informative than education about LBP if the objective is to assess socioeconomic status or structural determinants of health, and less informative than occupational factors if the objective is to study the role of proximal factors.
Education is often considered first as a proxy for socioeconomic status in childhood or early adulthood and then as a determinant of occupation. Our results suggest that the role of education remains important in adulthood. A low educational level seems to predict career-long exposure to occupational factors, even within occupations often considered homogeneous for physical exposure. The effects might be slightly different for men and women, both for the level of exposure and for the number of years of exposure. In manual occupations, a low educational level may also limit the possibility of upward mobility or transfer to less physically demanding tasks.
Conclusion
These results from a large population survey suggest that physical work factors and lifestyle factors play an important role in social inequalities in LBP. In addition to reducing physical exposure and promoting healthy lifestyles, improving adults’ educational level and skills may be an important means of prevention.
Acknowledgments
Funding: Mission de la Recherche, French ministry of health.
Footnotes
Ethical standards: This study has been conducted in accordance with the French and European legislation concerning ethical standards and protection of confidentiality.
References
- Aittomäki A, Lahelma E, Rahkonen O, Leino-Arjas P, Martikainen P. The contribution of musculoskeletal disorders and physical workload to socioeconomic inequalities in health. The European Journal of Public Health. 2007;17(2):145–150. doi: 10.1093/eurpub/ckl121. [DOI] [PubMed] [Google Scholar]
- Andersson GBJ. Epidemiological features of chronic low-back pain. The Lancet. 1999;354:581–585. doi: 10.1016/S0140-6736(99)01312-4. [DOI] [PubMed] [Google Scholar]
- Blane D. Commentary: explanations of the difference in mortality risk between different educational groups. Int J of Epidemiol. 2003;32:355–356. doi: 10.1093/ije/dyg078. [DOI] [PubMed] [Google Scholar]
- Buchbinder R, Jolley D, Wyatt M. Population based interventions to change back pain beliefs and disability: three part evaluation. BMJ. 2001;322:1516–1520. doi: 10.1136/bmj.322.7301.1516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cavelaars AE, Kunst AE, Geurts JJ, Crialesi R, Grötvedt L, Helmert U, et al. Persistent variations in average height between countries and between socioeconomic groups: an overview of 10 European countries. Ann Hum Biol. 2000;27(4):407–421. doi: 10.1080/03014460050044883. [DOI] [PubMed] [Google Scholar]
- Croft PR, Rigby AS. Socioeconomic influences on back problems in the community in Britain. J Epidemiol Community Health. 1994;48:166–170. doi: 10.1136/jech.48.2.166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dersh J, Mayer T, Theodore BR, Polatin P, Gatchel RJ. Do psychiatric disorders first appear preinjury or postinjury in chronic disabling occupational spinal disorders? Spine. 2007;32:1045–1051. doi: 10.1097/01.brs.0000261027.28779.52. [DOI] [PubMed] [Google Scholar]
- Dionne CE, Von Korff M, Koepsell TD, Deyo RA, Barlow WE, Checkoway H. Formal education and back pain: a review. J Epidemiol Community Health. 2001;55:455–468. doi: 10.1136/jech.55.7.455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- d’Errico A, Punnett L, Cifuentes M, Boyer J, Tessler J, Gore R, Scollin P Promoting Healthy and Safe Employment in Healthcare Research Team. Hospital injury rates in relation to socioeconomic status and working conditions. Occup Environ Med. 2007;64:325–333. doi: 10.1136/oem.2006.027839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldberg MS, Scott SC, Mayo NE. A review of the association between cigarette smoking and the development of nonspecific back pain and related outcomes. Spine. 2000;25:995–1014. doi: 10.1097/00007632-200004150-00016. [DOI] [PubMed] [Google Scholar]
- Griffith LA, Hogg-Johnson S, Cole DC, Krause N, Hayden J, Burdorf A, Leclerc, Coggon D, Bongers P, Walter SD, Shannon HS. Low-back pain definitions in occupational studies were categorized for a meta-analysis using Delphi concensus methods. Journal of Clinical Epidemiology. 2007;60:625–633. doi: 10.1016/j.jclinepi.2006.09.005. [DOI] [PubMed] [Google Scholar]
- Hagen K, Zwart JA, Svebak S, Bovim G, Jacob Stovner L. Low socioeconomic status is associated with chronic musculoskeletal complains among 46, 901 adults in Norway. Scand J Public Health. 2005;33 (4):268–375. doi: 10.1080/14034940510005699. [DOI] [PubMed] [Google Scholar]
- Hagen KB, Tambs K, Bjerkedal T. What mediates the inverse association between education and occupational disability from back pain? – A prospective cohort study from the North-Trondelag health study in Norway. Social Science and Medicine. 2006;36:1267–1275. doi: 10.1016/j.socscimed.2006.03.041. [DOI] [PubMed] [Google Scholar]
- Hoogendoorn WE, van Poppel MN, Bongers PM, Koes BW, Bouter LM. Physical load during work and leisure time as risk factors for back pain. Scand J Work Environ Health. 1999;25:387–403. doi: 10.5271/sjweh.451. [DOI] [PubMed] [Google Scholar]
- Hoogendoorn WE, van Poppel MN, Bongers PM, Koes BW, Bouter LM. Systematic review of psychosocial factors at work and private life as risk factors for back pain. Spine. 2000;25(16):2114–2125. doi: 10.1097/00007632-200008150-00017. [DOI] [PubMed] [Google Scholar]
- Hurwitz EL, Morgenstern H, Yu F. Cross-sectional and longitudinal associations of low back pain and related disability with psychological distress among patients enrolled in the UCLA low-back study. Journal of clinical Epidemiology. 2003;56:463–471. doi: 10.1016/s0895-4356(03)00010-6. [DOI] [PubMed] [Google Scholar]
- Jacobsson L, Lindgarde F, manthorpe R, Ohlsson K. Effect of education, occupation and some lifestyle factors on common rheumatic complains in a Swedish group aged 50–70 years. Ann Rheum Dis. 1992;51 (7):835–843. doi: 10.1136/ard.51.7.835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khatun M, Ahlgren C, Hammarstrom A. The influence of factors identified in adolescence and early adulthood on social class inequities of musculoskeletal disorders at age 30: a prospective population-based cohort study. Int J Epidemiol. 2004;33(6):1353–1360. doi: 10.1093/ije/dyh237. [DOI] [PubMed] [Google Scholar]
- Kopek JA, Sayre EC, Esdaile JM. Predictors of back pain in a general population cohort. Spine. 2004;29(1):70–77. doi: 10.1097/01.BRS.0000103942.81227.7F. [DOI] [PubMed] [Google Scholar]
- Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sorensen F, Andersson G, et al. Standardised Nordic questionnaire for the analysis of musculoskeletal symptoms. Applied Ergonomics. 1987;18(3):233–237. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- Lake JK, Power C, Cole TJ. Back pain and obesity in the 1958 british birth cohort: cause or effect? Journal of clinical Epidemiology. 2000;53:245–250. doi: 10.1016/s0895-4356(99)00155-9. [DOI] [PubMed] [Google Scholar]
- Lanoë JL, Makdessi-Raynaud Y. L’état de santé en France en 2003: santé perçue, morbidité déclarée et recours aux soins à travers l’enquête décennale santé. Etudes et résultats. 2005:1–12. [Google Scholar]
- Latza U, Kohlmann T, Deck R, Raspe H. Influence of occupational factors on the relation between socioeconomic status and self-reported back pain in a population-based sample of German adults with back pain. Spine. 2000;25(11):1390–1397. doi: 10.1097/00007632-200006010-00011. [DOI] [PubMed] [Google Scholar]
- Leclerc A, Chastang JF, Ozguler A, Ravaud JF. Chronic back problems among persons 30 to 64 years old in France. Spine. 2006;31:479–484. doi: 10.1097/01.brs.0000199939.53256.e0. [DOI] [PubMed] [Google Scholar]
- Leboeuf-Yde C. Smoking and low back pain: a systematic literature review of 41 journal articles reporting 47 epidemiologic studies. Spine. 1999;24:1463–1470. doi: 10.1097/00007632-199907150-00012. [DOI] [PubMed] [Google Scholar]
- Leino-Arjas P, Hanninen K, Puska P. Socioeconomic variation in back and joint pain in Finland. Eur J Epidemiol. 1998;14(1):79–87. doi: 10.1023/a:1007448402954. [DOI] [PubMed] [Google Scholar]
- Liira JP, Shannon HS, Chambers LW, Haines TA. Long-term back problems and physical work exposures in the 1990 Ontario Health Survey. Am J Public Health. 1996;86(3):382–387. doi: 10.2105/ajph.86.3.382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25:1148–1156. doi: 10.1097/00007632-200005010-00017. [DOI] [PubMed] [Google Scholar]
- Lund T, Labriola M, Christensen KB, Bultmann U, Villadsen E. Physical work environment risk factors for long term sickness absence: prospective findings among a cohort of 5357 employees in Denmark. BMJ. 2006;332(7539):449–452. doi: 10.1136/bmj.38731.622975.3A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mustard CA, Kalcevich C, Frank JW, Boyle M. Childhood and early adult predictors of risk of incident back pain: Ontario Child Health Study 2001 follow-up. Am J Epidemiol. 2005;162 (8):779–786. doi: 10.1093/aje/kwi271. [DOI] [PubMed] [Google Scholar]
- Ozguler A, Leclerc A, Landre MF, Pietri-Taleb F, Niedhammer I. Individual and occupational determinants of low back pain according to various definitions of low back pain. Journal of Epidemiology and Community Health. 2000;54:215–220. doi: 10.1136/jech.54.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Power C, Frank J, Hertzman C, Schierhout G, Li L. Predictors of low back pain onset in a prospective British study. Am J Public Health. 2001;91(10):1671–1678. doi: 10.2105/ajph.91.10.1671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sainio P, Martelin T, Koskinen S, Heliövaara M. Educational differences in mobility: the contribution of physical workload, obesity, smoking and chronic conditions. Journal of Epidemiology and Community Health. 2007;61:401–408. doi: 10.1136/jech.2006.048306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt CO, Raspe H, Pfingsten M, Hasenbring M, Basler HD, Eich W, Kohlmann T. Back pain in the German adult population: prevalence, severity, and sociodemographic correlates in a multiregional survey. Spine. 2007;32(18):2005–2011. doi: 10.1097/BRS.0b013e318133fad8. [DOI] [PubMed] [Google Scholar]
- Schneider S, Schmitt H, Zoller S, Schiltenwolf M. Workplace stress, lifestyle and social factors as correlates of back pain: a representative study of the German working population. Int Arch Occup Environ Health. 2005;78(4):253–269. doi: 10.1007/s00420-004-0576-4. [DOI] [PubMed] [Google Scholar]
- Skovron ML, Szpalski M, Nordin M, Melot C, Cukier D. Sociocultural factors and back pain. A population-based study in Belgian adults. Spine. 1994;19(2):129–137. doi: 10.1097/00007632-199401001-00002. [DOI] [PubMed] [Google Scholar]
- Stock SR, Fernandes R, Delisle A, Vézina N. Reproducibility and validity of worker’s self-reports of physical work demands. Scand J Work Environ Health. 2005;31:409–437. doi: 10.5271/sjweh.947. [DOI] [PubMed] [Google Scholar]
- Stronks K, Van De Mheen H, Van Den Bos J, Mackenbach JP. The interrelationship between income, health and employment status. Int j Epidemiol. 1997;26:592–600. doi: 10.1093/ije/26.3.592. [DOI] [PubMed] [Google Scholar]
- van Tulder M, Kovacs F, Muller G, et al. European guidelines for the management of low back pain. Acta Orthop Scand (suppl 305) 2002;73:20–25. doi: 10.1080/000164702760379503. [DOI] [PubMed] [Google Scholar]