

Abstract
Previously depressed and never-depressed individuals identified personal characteristics (self-guides) defining their ideal, ought, and feared selves. One week later they completed the autobiographical memory test (AMT). For each participant the number of AMT cues that reflected self-guide content was determined to produce an index of AMT cue self-relevance. Individuals who had never been depressed showed no significant relationship between cue self-relevance and specificity. In contrast, in previously depressed participants there was a highly significant negative correlation between cue self-relevance and specificity—the greater the number of AMT cues that reflected self-guide content, the fewer specific memories participants recalled. It is suggested that in individuals with a history of depression, cues reflecting self-guide content are more likely to prompt a shift to processing of information within the long-term self (Conway, Singer, & Tagini, 2004), increasing the likelihood that self-related semantic information will be provided in response to cues on the autobiographical memory test.
Research has consistently demonstrated that the autobiographical memory of depressed individuals lacks specific detail. Most studies examining this phenomenon have used the Autobiographical Memory Test (AMT) in which participants are presented with a series of cue words (e.g., “Happy”) and asked to come up with a memory of a specific event that each word reminds them of. When tested in this way, depressed individuals tend to retrieve generic summaries of past experience (e.g., “birthdays”) rather than memories of specific events (e.g., “going swimming with my friends on my birthday last year”). This deficit has been demonstrated across a range of populations including individuals with major depression, suicidal patients, mothers with postnatal depression, and dysphoric students (see Williams et al., 2007). Over-general memory (OGM) is linked to the persistence of affective disturbance in depressed populations (e.g., Brittlebank, Scott, Williams, & Ferrier, 1993; Dalgleish, Spinks, Yiend, & Kuyken, 2001; Peeters, Wessel, Merckelbach, & Boom-Vermeeren, 2002; cf. Brewin, Reynolds, & Tata, 1999) and is also observed in clinical groups following recovery from depression (e.g., Brittlebank, Scott, Williams, & Ferrier, 1993; Mackinger, Pachinger, Leibetseder, & Fartacek, 2000; Nadrino, Pezard, Poste, Reveillere, & Beaune, 2002; Spinhoven et al., 2006), suggesting that it may represent a relatively stable marker of vulnerability to depressive episodes.
In order to understand the mechanisms that contribute to OGM in depression, it is helpful to consider the phenomenon in the context of models of normative memory functioning and the relationship between autobiographical memory and the self. One contemporary model, shown in Figure 1, is the “Self Memory System” of Conway and Pleydell-Pearce (2000; see also Conway, Singer, & Tagini, 2004, for an elaboration). According to this model, autobiographical memories are the “transitory mental constructions” of a self memory system (SMS), comprising the working self, the episodic memory system, and the long-term self. The function of the working self is to initiate and monitor ongoing goal-directed activity, and to control the storage and retrieval of autobiographical memories. The long-term self represents self-related autobiographical knowledge in an abstract form, having two elements: the “conceptual self” (self-guides, schemata, attitudes and beliefs etc.) and the “autobiographical knowledge base” (representations of an individual's life story schema, distinct lifetime periods, e.g., “when I lived in London”, and general events, e.g., “travelling to work by tube in the mornings”). Finally, the episodic memory system encodes sensory perceptual representations of discrete events (e.g., the sights, sounds, and smells of a particular subway journey), often in the form of visual imagery.
Figure 1.
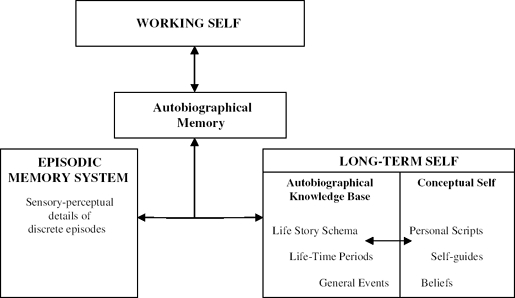
A summary of the self-memory system (SMS) as described by Conway et al. (2004).
Within this model, specific autobiographical memories are conceptualised as the product of coordinated retrieval of sensory-perceptual information from the episodic memory system and contextualising information from the long-term self. Over-general memories, in contrast, appear to be dominated by information from the long-term self. Indeed, while general event memories (or “categoric memories” e.g., Williams & Dritschel, 1988) are the most common “error” seen on the autobiographical memory test, responses that may be better thought of as output of life story schema information or information from the conceptual self are also observed.
Why might depressed individuals, and other clinical groups who display over-general memory, tend to respond with information from the long-term self? One possibility relates to the suggestion that autobiographical knowledge and autobiographical memories stored in the self memory system are of primary importance to an individual's ability to evaluate progress towards goals (e.g., Conway & Pleydell-Pearce, 2000). According to the Self Memory System model, information signalling challenges to goal progress (such as the awareness of discrepancies between one's current circumstances and desired goals) will prompt a shift of self memory system processing priorities from the encoding and retrieval of information in the episodic memory system (“adaptive correspondence”) towards the long-term self, with an increased emphasis on the maintenance of self-coherence, such that “knowledge based in the long-term self is likely to dominate attention” (Conway et al., 2004, p. 495).
A considerable body of research has indicated that depressive states and other forms of negative affect are closely linked to the perception of discrepancy from approach goals (often referred to as “ideal or ought self-guides”) and proximity to avoidance goals (“feared self-guides”; e.g., Carver, Lawrence, & Scheier, 1999; Carver & Scheier, 1998; Higgins, 1987; Higgins, Bond, Klein, & Strauman, 1986; Strauman, 1989). Rumination, which can also be regarded as a form of discrepancy-based processing in which an attempt is made to reduce the gap between a current state and desired state by mental analysis (e.g., Martin & Tesser, 1989, 1996; Matthews & Wells, 2004; Watkins, Teasdale, & Williams, 2000), is also common during depressive episodes. If the Self Memory System model is correct then depressive episodes will be associated with the increased salience of abstract autobiographical information stored in the long-term self, more extensive processing and elaboration of this information, and an increased likelihood that individuals will respond with such information when asked to retrieve memories to cue words.
The observation that the induction of rumination (discrepancy-based processing) maintains over-general memory in depressed patients, whereas distraction reduces it (e.g., Watkins et al., 2000), is supportive of this suggestion, as are the findings of other studies demonstrating a link between rumination and over-general memory in clinical samples (Park, Goodyer, & Teasdale, 2004; Raes et al., 2005). Further, Dalgleish et al. (2003) hypothesised that over-general memory may be particularly likely to occur if cues forming the basis of a memory search actually map on to, and hence directly prime, concepts in the long-term self. These data suggest that over-general memory may be observed when an individual is prompted to shift to a mode of processing that favours self-coherence (and facilitation of information in the long-term self) over adaptive correspondence. This is most likely following exposure to salient self-relevant information, information related to important goals, or to stimuli that promote rumination.
In what circumstances might we expect to see the effects of priming of self-relevant concepts on autobiographical memory? The most obvious context is during episodes of depression. At such times, the predominance of rumination, negative self-referent thinking, and perceived discrepancies from goals or ideals are likely to ensure that the self memory system is focused on the processing of information within the long-term self, elaborating this content and producing high levels of over-general memory. However, a second context in which we might expect to see effects of self-relevant priming is in previously depressed individuals. The increased rehearsal of abstract autobiographical knowledge during prior periods of depressive rumination and the potential for self-referent cues to prime latent negative self-schemas are suggested to increase the likelihood that previously depressed individuals, relative to never-depressed controls, will experience a shift to processing information in the long-term self when exposed to self-referent material. Given the relative absence in recovery of other factors (such as deficits in motivation and executive capacity) that may contribute to over-general memory during depressive episodes, over-general memory in previously depressed groups may be particularly related on the extent to which cues are salient and self-relevant, for example, relating to an individual's long-term goals or ideals.
The study reported here examines the effects of exposure to self-relevant material on autobiographical memory specificity in individuals with a history of depression and never-depressed controls. Participants were asked to complete a “self-guides” questionnaire (see Carver et al., 1999) in which they listed personal characteristics defining their ideal, ought, and feared selves (e.g., the characteristics they felt they ought to have, would ideally like to have, and most feared having). One week after completing the questionnaire, participants completed a standard version of the AMT. It was hypothesised that increased exposure to self-relevant material on the AMT would be associated with a general reduction in memory specificity in previously depressed individuals, but that this relationship would be attenuated or absent in never-depressed controls. It was unclear whether exposure to self-relevant information would act to influence retrieval on a cue-by-cue basis or would have a more pervasive impact on retrieval. Therefore the specificity of responses to self-relevant and non-self-relevant cues was compared, but no firm hypotheses were developed a priori.
Method
Recruitment
Advertisements in community buildings, in the local newspaper, and on a community internet site requested volunteers who had been depressed in the past but were currently well, and individuals who had never been depressed. Individuals who were interested in taking part were invited to attend two experimental sessions at the University Department of Psychiatry. Participants were paid £20 for participating in the study, which was approved by University of Oxford, Central Research Ethics Committee.
Participants
A total of 21 individuals without a history of major depression and 23 individuals with a history of major depression participated in the study. A further six individuals who reported significant past depressive symptoms but did not meet full criteria for past major depression (see later) were interviewed but excluded. Additionally, one individual was excluded due to current mania (which manifested itself in the week between psychiatric interview and cognitive testing) and two individuals were excluded as a result of equipment failure.
All previously depressed participants were recovered at the time of participation in the study, having had noor only minimal symptoms for at least 8 weeks (Frank et al., 1991; Keller, Shapiro, Lavori, & Wolfe, 1982). More detailed assessment of recovery as well as details of other psychiatric disorders were established when participants attended the Department of Psychiatry, using the Structured Clinical Interview for DSM-IV (SCID: First, Spitzer, Gibbon & Williams, 1996). All interviews were conducted by a post-doctoral clinical or research psychologist.
Other psychiatric diagnoses. The SCID interview identified current psychiatric diagnoses in two of the 21 individuals who had never been depressed, with one case of current alcohol dependence and one of current substance abuse. In contrast, current psychiatric diagnoses were identified in 12 of the 23 individuals with a history of major depression.1 Two individuals had specific phobias and one individual had panic and specific phobia in partial remission. One individual had social phobia, one had agoraphobia, one panic disorder, one panic disorder with agoraphobia in partial remission, one alcohol abuse with PTSD, and two PTSD in partial remission. Finally, one individual had generalised anxiety disorder and one individual had bulimia. These disorders were of mild to moderate severity in all cases.
Procedure
Session 1 began with a discussion of the study and the gathering of written informed consent. This was followed by the clinical interview and the completion of several questionnaires (those of relevance to the current study are described below). A second appointment was scheduled for approximately 1 week later. During this session, individuals completed the autobiographical memory test, followed by the Mill-Hill Vocabulary Test and Raven's Advanced Progressive Matrices, to assess current cognitive functioning. Following these tasks, participants were fully debriefed.
Questionnaires
Beck Depression Inventory. The Beck Depression Inventory (BDI-II; Beck, Steer, & Brown, 1996) is a well-established measure of depressive symptomatology that contains 21 groups of statements, referring to the presence of symptoms of depression over the preceding 2 weeks.
Self-Description Questionnaire (Carver et al., 1999). Participants completed a questionnaire in which they were asked to describe three different “self-concepts”: their “ought self”, “ideal self”, and “feared self” (see Appendix for definition). Participants first identified and listed seven characteristics that described their “ought”, “ideal”, and “feared” self-concepts. They then copied each of the characteristics onto a second page and first rated their current similarity to each characteristic on a scale ranging from 1 (“presently I am the opposite of this characteristic”) to 7 (“presently I am just like this characteristic”). In an addition to the questionnaire of Carver et al., they then rated the likelihood that they would possess each characteristic in the future, and the importance of each characteristic, again on scales ranging from 1 (“it is very unlikely that I will have this characteristic in the future”/ “this characteristic is not important to my xxxx self”) to 7 (“it is very likely that I will have this characteristic in the future”/“this characteristic is very important to my xxxx self”).
Autobiographical memory test (AMT)
Participants were presented one at a time with a series of cue words, which were read aloud by the experimenter and also presented on a computer screen. For each cue word, participants were asked to report an event that had happened to them of which the word reminded them—a specific event, defined as an event that had lasted less than a day and occurred at a particular time and place. Three practice words were given to participants, with practice continuing until specific memories had been recalled for at least two of these three words. In the test phase, participants were given 30 seconds to respond to each cue word. To ensure that all individuals received the same instructions, no prompts were given when a first response was not specific and participants were informed that they would not receive feedback on the specificity of their memories once the test phase had begun. After 18 cues had been presented (i.e., halfway through the task), the instructions were briefly reiterated to all participants. Participants’ responses to each cue word were recorded verbatim by the experimenter and were also recorded on audio tape for later rating.
For the current study, 36 words were used as cues. Of these, 12 cue words related to interpersonal issues (affectionate, friendly, loved, sensitive, caring, loyal, lonely, needy, rejected, heartless, isolated, disliked), 12 related to achievement issues (efficient, thorough, successful, ambitious, able, determined, incompetent, unproductive, inept, inefficient, failure, useless), and 12 described emotional states (lively, happy, calm, excited, glorious, lucky, upset, tired, bad, awful, sad, bored), with 6 positive and 6 negative words in each category. These words were selected to increase the likelihood that cues would overlap to some extent with participants’ self-guides. Words were identified from a larger pool, with positive and negative words matched for emotionality, frequency, and imageability on the basis of ratings made by 25 individuals blind to the research hypotheses. Words were presented in one of two pseudo-random orders, counter-balanced across participants.
Following previous studies, responses were rated by the experimenter as specific (events lasting less than a day), categoric (repeated events), extended (events lasting longer than one day), semantic associates of the cue word, and omissions (no response; details of scoring procedures for the AMT are available from the authors).
Other cognitive tasks
In order to ensure that general cognitive performance was matched between previously depressed and never-depressed controls, two cognitive tasks were administered.
Mill Hill Vocabulary Test. This test (Raven, Raven, & Court, 1998) assesses a participant's ability to reproduce previously acquired knowledge (crystallised intelligence), in this case word meanings. A total of 66 target words requiring definition were presented. For each target, participants were required to select from six alternative words one that was most similar in meaning to the target. The test was untimed, with the total number of target words correctly defined (out of a possible 66) recorded.
Ravens Advanced Progressive Matrices — Set 1. The progressive matrices (Raven, 1976) provide a culture-fair test of fluid intelligence—the ability to adapt reasoning skills to novel problems. Participants were presented with 12 problems to complete in 10 minutes. Each problem consisted of a visual pattern in which one “piece” was missing. Participants were required to select from eight options the piece that correctly completed the pattern. The total number of matrices correctly completed (out of 12) was recorded.
Deriving indices of AMT cue self-relevance
Two indices of AMT cue self-relevance were derived. First, we determined for each participant the number of self-guides that were represented by one or more AMT cue or AMT cue synonym. To do this, a document was created that contained each AMT cue (e.g., “affectionate”) and each cue's synonyms (e.g., “loving”, “demonstrative”, “warm”, “friendly”, “kind”), based on the synonyms provided by the Thesaurus in Microsoft Office Word 2003. This document was searched electronically for each self-guide to identify exact matches, and the total number of matches was recorded. From time to time an individual reported the same attribute as both an “ideal” and an “ought” self-guide. Where these attributes matched an AMT cue, they were counted twice, as it was considered that the attribute was more important to the individual's sense of self.
Second, we identified the AMT cues that had represented matches to self-guides. Although some self-guides matched AMT cues exactly, others matched synonyms of the cues. If a self-guide had matched an AMT cue synonym, the “originating” cue was identified. The number of originating cues was counted for each individual to create an index of the number of AMT cues that were self-relevant. This index differs from the index corresponding to the number of self-guides whose content was represented in the AMT, because it was possible for two self-guides to be synonyms of a single AMT cue (e.g., “kind” and “loving” are both synonyms of the AMT cue “caring”). Identifying the originating cues also allowed for a comparison of specificity of responses to self-relevant cues and non-relevant cues on the AMT (see below).
RESULTS
Demographics
The mean age of the participants was 32.95 (SD = 12.66, range 18-62) years. Individuals with a past history of depression (M = 36.13, SD = 13.92) were somewhat older than those without such a history (M = 29.48, SD = 10.35). However, there was no significant difference between the groups in mean age (U = 186.00, Z= −1.31, p= .19). There were nine male participants in each group.
Past depressive symptoms
Among those individuals with a history of depression, mean age of onset of depressive symptoms was 21.65 (SD = 8.79) years. The median number of past episodes of depression was 3 (M = 6.83, SD = 9.71, range 1–40). Of the 23 individuals, 14 had experienced thoughts of death or suicide during their worst episode of depression.
Current depression
Mean BDI score was 3.90 (SD = 4.01) in the never-depressed group and 6.26 (SD = 7.05) in the previously depressed group, with no significant difference between the groups in current depressive symptoms, F(1, 42) = 1.81, MSE = 33.72, p > .18.
Cognitive tasks
Never-depressed and previously depressed participants did not differ in their performance on the Raven's Matrices (Never Depressed: M= 10.90, SD = 0.94; Previously Depressed: 10.81, SD = 1.22), F(1, 41) = 0.07, MSE = 1.20, p > .70. Nor did they differ from one another on the Mill Hill Vocabulary Test (Never Depressed: M = 42.62, SD = 10.14; Previously Depressed: M = 43.26, SD = 11.39) F(1, 42) = 0.04, MSE = 116.84, p> .80, indicating that the two groups were well matched in general cognitive abilities.
Self-description questionnaire
Similarity, likelihood, and importance ratings for ideal, ought, and feared self-guides were compared between groups. There was a trend towards previously depressed participants reporting less similarity to ought self-guides than never-depressed controls, F(1, 39) = 3.62, MSE = 65.32, p = .06. There were no significant differences between groups in similarity ratings for ideal or feared self-guides (ps > .10), although mean differences were in the expected direction (i.e., less similarity to ideal self-guides and more similarity to feared self guides in the previously depressed group). Future likelihood ratings also did not differ between groups (all ps >.12), although again mean differences were in the expected direction. Previously depressed participants tended to rate ideal, ought, and feared self-guides as more important than never-depressed controls. However these differences did not reach statistical significance in any case (ps > .15). Descriptive statistics for the self-description questionnaire are shown in Table 1.
TABLE 1.
Descriptive statistics for self-discrepancy questionnaire
|
Never depressed |
Previously depressed |
|||
| Self-guide | M | SD | M | SD |
| Ideal | ||||
| Similarity | 32.11 | 6.55 | 30.05 | 5.39 |
| Likelihood | 37.83 | 5.25 | 35.05 | 5.63 |
| Importance | 41.56 | 3.36 | 43.05 | 3.69 |
| Ought | ||||
| Similarity | 33.90 | 7.73 | 29.10 | 8.40 |
| Likelihood | 36.60 | 8.05 | 33.71 | 7.50 |
| Importance | 39.35 | 7.80 | 42.29 | 4.70 |
| Feared | ||||
| Similarity | 20.95 | 7.00 | 24.81 | 9.12 |
| Likelihood | 20.57 | 7.24 | 24.04 | 10.06 |
| Importance | 39.71 | 5.31 | 41.83 | 6.86 |
Scores on each variable could range from 0 (lowest similarity, importance, likelihood) to 49 (highest similarity, importance, likelihood). For feared self-guides higher ratings are more negative (i.e., more similarity to a feared self-concept).
Autobiographical memory test (AMT)
Descriptive statistics for participants’ performance on the AMT (number of responses that were specific, extended, categoric, associates, and omissions) are shown in Table 2. Visual inspection of the data indicates that specific memories were by far the most common response, but that in cases where participants failed to retrieve a specific memory, the most common response was an omission. Univariate analysis of variance revealed no significant difference between groups in number of specific memories: F(1, 42) = 1.07, MSE = 54.35, p > .30; extended memories: F(1, 42) = 0.00, MSE = 6.66, p > .99; categoric memories: F(1, 42) = 0.53, MSE = 7.45, p > .40; semantic associates: F(1, 42) = 1.53, MSE = 7.55, p > .20; or omissions: F(1, 42) = 0.23, MSE = 25.46, p > .60. Given the relatively small number of responses that fell into each category of nonspecific memory, number of specific memories was used as the primary outcome variable in subsequent analyses.2
TABLE 2.
Number of AMT responses falling into each category (36 items in total)
|
Never depressed |
Previously depressed |
|||
| Type of response | M (%) | SD | M (%) | SD |
| Specific | 24.48 (68%) | 6.05 | 22.17 (61.6%) | 8.39 |
| Extended | 3.05 (8.5%) | 2.82 | 3.04 (8.4%) | 2.34 |
| Categoric | 2.10 (5.8%) | 1.87 | 2.70 (7.5%) | 3.32 |
| Associate | 1.19 (3.3%) | 1.72 | 2.22 (6.2%) | 3.42 |
| Omission | 5.14 (14.3%) | 3.82 | 5.87 (16.3%) | 5.94 |
Number of self-guides represented
The mean number of self-guides that were represented by an AMT cue or cue synonym was M = 6.29 (SD = 3.16) for never-depressed individuals and M = 6.09 (SD = 2.54) for previously depressed individuals. ANOVA indicated no significant difference between groups in this index of self-relevance, F(1, 42) = 0.05, MSE = 8.15, p > .80. When this index was considered separately for ideal, ought, and feared self-guides, there were also no significant differences between groups (all ps = .50).
Number of self-relevant AMT cues
The mean number of AMT cues that matched a self-guide or had a synonym that matched a self-guide was M = 5.57 (SD = 2.48) for never-depressed individuals and M = 5.09 (SD = 1.98) for previously depressed individuals. ANOVA indicated no significant difference between the groups in the number of self-relevant cues presented on the AMT, F(1, 42) = 0.52, MSE = 4.98, p > .40.
Relationship between indices of cue self-relevance
As expected, the two indices of cue-self relevance, although distinct, were found to be highly correlated (r= .84, p < .001). For clarity, further analyses focus on the index corresponding to the number of AMT cues that were self-relevant, since this index is not influenced by repetition of attributes across two self-guide domains.
Cue self-relevance and memory specificity
A regression analysis was conducted to examine the impact of previous MDD, cue self-relevance (number of AMT cues that matched self-guides), and the interaction between cue self-relevance and previous MDD on the number of specific memories retrieved by participants. Depression status (never depressed, previously depressed) was entered at Step 1. The index of cue self-relevance was entered at Step 2 and the interaction at Step 3 (see Table 3 for summary of regression model). At Step 1, the regression model was non-significant. At Step 2, there was a significant improvement in the model, ΔF(1, 41) = 5.22, p=.03, with the model becoming significant at trend level, R2 =. 14, F(2, 41) = 3.20, p = .051, and cue self-relevance entering as a significant predictor of number of specific memories (p < .05). With the addition of the interaction between past history of depression and AMT cue self-relevance at Step 3, there was a significant improvement in the model, ΔR2= .21, ΔF(1, 40) = 12.69, p = .001, and the overall regression model became highly significant, R2 = .34, F(3, 40) = 6.97, p = .001. The interaction between cue self-relevance and past MDD entered as a significant predictor of specificity (p = .001), with the final model accounting for 34% of the variance in number of specific memories retrieved.
TABLE 3.
Regression model examining the contribution of past history of MDD and cue self-relevance to the prediction of number of specific memories retrieved on the AMT
| Variable | B | SE B | β | t | p | |
| Model 1 | Past MDD | −2.30 | 2.23 | .16 | −1.03 | .31 |
| Model 2 | Past MDD | −2.84 | 2.13 | −.20 | −1.33 | .19 |
| Cue Self-Relevance | −1.11 | .49 | −.33 | −2.28 | .03 | |
| Model 3 | Past MDD | 13.57 | 4.98 | .93 | 2.73 | .009 |
| Cue Self-Relevance | .17 | .56 | .05 | .30 | .77 | |
| Past MDD* Cue Self-Relevance | −3.11 | .87 | −1.23 | −3.56 | .001 |
Model 1: R2 −.03, F(1, 42) =1.07, p = .31.
Model 2: R2 = .14, F(2, 41) = 3.20, ρ= .051, ΔR2 = .11, ΔF(1, 41) = 5.22, Sig ΔF p = .03.
Model 3: R2 = .34, F(3, 40) = 6.97, p = .001, ΔR2 = .21, ΔF(1, 40) = 12.69, Sig ΔF p = .001.
To examine the nature of the interaction between cue self-relevance and specificity, Pearson's correlation coefficients were calculated for the relationship between number of specific memories retrieved and number of self-relevant cues presented, separately for individuals with and without a history of major depression. These indicated that while there was no significant correlation between cue self-relevance and specificity in the never-depressed group (r = .07, p > .70), there was a highly significant correlation in the previously depressed group (r = −.69, p < .001). Thus, increased exposure to self-relevant cues was associated with reduced retrieval of specific memories, but only in individuals with a history of major depression. Scatter plots depicting these relationships are shown in Figure 2.
Figure 2.
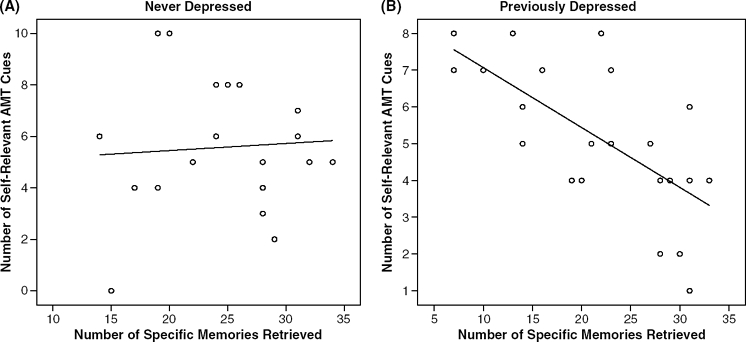
Relationship between the number of self-relevant AMT cues and number of specific memories recalled in never-depressed (A) and previously depressed (B) participants.
Specificity of responses to self-relevant and non-self-relevant cues
In order to examine whether the presence of self-relevant cues influenced only retrieval of specific memories to those cues, or had a broader impact on retrieval, the proportion of specific responses given to self-relevant cues and non self-relevant cues was calculated for each individual. Repeated measures analysis of variance was used to compare these two scores in individuals with and without a history of major depression. This analysis revealed no significant effect of cue type, F(1, 41) = 1.38, p = .25 and no significant interaction between cue type and past MDD, F(1, 41) = 1.08, p = .30. Because the mean number of self-relevant cues was relatively low compared to the total number of cues presented, in some cases proportions were based on the very few responses to self-relevant cues. An alternative way of examining the pervasiveness of the effect of cue self-relevance is to examine the effect of number of self-relevant cues on specificity of responses to cues that were not matches to self-guides. Pearson's correlation coefficients revealed that in the previously depressed group, the greater the number of self-relevant cues presented, the less specific participants were in response to other, non-self-relevant cues, r = −.76, p < .001. In contrast, in the never-depressed group, the presence of self-relevant cues had no impact on specificity to non-self-relevant cues, r= −.18, p > .40.
Discussion
The aim of this study was to examine whether the ability to retrieve specific autobiographical memories varies as a function of the self-relevance of memory cues. Results indicated that in never-depressed participants there was no systematic relationship between cue self-relevance and specificity. In contrast, previously depressed participants showed a highly significant negative correlation between the number of self-relevant cues presented on the AMT and the ability to retrieve specific autobiographical memories—the greater the number of self-relevant cues presented, the fewer specific memories participants recalled. Regression analysis confirmed that history of major depression moderated the association between cue self-relevance and specificity, with the variance in specificity explained by the regression model containing the interaction term rising to approximately 30%. Subsequent analyses indicated that the effect of exposure to self-relevant cues had a general deleterious effect in the previously depressed group, with specificity of retrieval to non-self relevant cues also being affected.
The current study examined the effects on retrieval specificity of AMT cues whose content reflected a participant's self-guides (desired or feared characteristics or attributes). The Self Memory System model suggests that when information that signals a challenge to goal progress is presented, the processing of information stored in the long-term self (e.g., general event memories, lifetime period, life story schema, and conceptual self-knowledge) will be prioritised, with an emphasis on the maintenance of self-coherence. Because, during depressive episodes, individuals report marked discrepancies from self-guides and spend significant amounts of time engaged in depressive rumination (a form of discrepancy-based processing), it was hypothesised that presentation of cues relating to an individual's self-guides would be more likely to produce a shift towards processing for self-coherence in the previously depressed group, reinstating a form of processing that has been over-rehearsed in the past. In addition, information relating to goals and self-guides stored within the long-term self may be more elaborated in individuals with a history of depression as a consequence of increased processing during prior episodes, making such a shift towards long-term self-processing more difficult to override. Although speculative at present, such a suggestion would be consistent with other studies showing that in recovered individuals with a history of depression, negative cognitive biases remain latent and can be easily reactivated, for example when individuals process self-referent material in the context of mood challenge or cognitive load (e.g., Scher, Ingram, & Segal, 2005; Wenzlaff & Bates, 1998).
The fact that increased cue self-relevance influenced specificity of retrieval to all cues in previously depressed participants, not just those that were identified as matching self-guides, is interesting. One possibility is that because the cues on the AMT were selected to relate to interpersonal issues, achievement issues, and emotional states, the overlap in meaning between cues was too great for distinct effects to be observed for cues identified as matching or not matching self-guides. However, it is also possible that exposure to some self-relevant content may have been sufficient to have a more persistent effect on specificity. For example, previous research has indicated that brief rumination inductions maintain over-generality and brief distraction inductions reduce over-generality during subsequent AMT testing (e.g., Watkins et al., 2000), and it also appears that over-general memory increases across repeated trials in individuals with low self-esteem relative to those with high self-esteem (Roberts & Carlos, 2006). These findings may reflect the cumulative effects of activation of self-related content on retrieval in vulnerable groups. Further research incorporating distinct neutral cues would be required to clarify the scope of any effect of cue self-relevance on specificity.
A number of limitations should be borne in mind when interpreting the current results. First, although individuals with a history of depression did not differ significantly from never-depressed controls in ratings of self-discrepancy, in all cases mean differences were in the expected direction, suggesting that self-guide cues may have been more salient for those with a history of MDD. Additionally we measured self-guides 1 week before completion of the AMT, in order to reduce the likelihood that participants would see a link between the two tasks. However, it is possible that individuals with a history of depression show more stability in their ratings of self-guides (for example due to prolonged periods of rumination on these issues in the past). If this was the case, it is plausible that the measure of self-relevance of AMT cues would be more accurate for the previously depressed than the never-depressed group. Further research is required to address this possibility as well as to examine the extent to which the effect of self-relevance on specificity is restricted to discrepant self-relevant information.
Second, in the current study there was no significant effect of history of depression on memory specificity. While several studies have identified persisting over-generality in previously depressed patients (e.g., Brittlebank et al., 1993; Spinhoven et al., 2006), others have failed to find such an effect (e.g., Kuyken & Dalgleish, 1995; Wessel, Meeren, Peeters, Arntz, & Merckelbach, 2001; Williams, Barnhofer, Crane, & Beck, 2005). It is possible that differences between studies may relate to the extent to which different samples had residual symptoms, or had experienced past trauma, the proximity of the most recent depressive episode, or the number of depressive episodes an individual has experienced (e.g., Nandrino et al., 2002). Additionally, given the current findings, it is possible that studies have differed by chance in the extent to which AMT cues primed previously depressed participants’ core concerns.
Third, many of the previously depressed participants were experiencing other psychiatric symptoms at the time of testing. In most cases these were anxiety disorders, which do not usually appear to be associated with over-general memory (e.g., Burke & Matthews, 1992; Wenzel, Jackson, & Holt, 2002). However, the presence of these disorders may have acted to increase the likelihood that self-relevant cues would activate information stored in the long-term self, and it would therefore be premature to assume that the effect of self-relevance on memory specificity is a feature related specifically to a history of depression. Finally, while there was no difference between the groups in the extent to which AMT cues were self-relevant, it remains possible that some third factor may have contributed to the association between self-relevance and specificity seen in the previously depressed participants in this study.
There has been little previous research examining the impact of cue self-relevance on the ability to retrieve specific autobiographical memories (though see Spinhoven et al., 2007, this issue). Although preliminary, this study provides evidence to suggest that the presence of self-relevant memory cues may contribute to over-general retrieval in previously depressed individuals, as a result of the increased tendency of conceptual self-relevant information to capture attention. It has been demonstrated that both brief experimental manipulations (e.g., Watkins et al., 2000) and clinical interventions (e.g., Williams, Teasdale, Segal, & Soulsby, 2000) that facilitate disengagement from analytical self-focused thinking produce decreases in over-general autobiographical memory. The current findings further emphasise the importance of self-related processing in the manifestation of over-generality in depression and, although in need of replication, suggest that the integration of research examining self-related processing with research examining autobiographical memory retrieval (e.g., Conway et al., 2004; Williams et al., 2007) may provide valuable insights into how these aspects of cognitive functioning determine persisting vulnerability to depression.
Acknowledgments
The authors wish to thank everyone who gave their time to participate in this research. This research was supported by the Wellcome Trust GR067797.
Appendix
Definitions of ought, ideal, and feared selves
The “ought self” was described as “the kind of person you believe you have a duty or obligation to be, or that you believe people think you should be. It's defined by the personality characteristics you think you ought to possess, or feel obligated to possess. It's not necessary that you have these characteristics now, only that you believe you ought to have them.”
The “ideal self” was described as “The kind of person you'd really like to be. It's defined by the personality characteristics you would ideally like to have. It's not necessary that you have these characteristics now, only that you believe you want to have them.”
The “feared self” was described as “the kind of person that you fear being, worry about being, or dislike being. It's defined by the personality characteristics that you think you might have now or in the future, but that you would rather not have. It's not necessary that you have these characteristics now, only that you do not want to have them, or want to avoid having them.
Footnotes
1 Additional past psychiatric diagnoses were identified in 15 of the 23 individuals with a history of major depression. One individual had a past manic episode and a prior history of anorexia, three had a lifetime history of alcohol abuse, four had past dysthymia (one with a prior history of OCD), one had a prior history of bulimia, one non-alcohol substance abuse and dependence (cannabis), two alcohol dependence in sustained full remission (one with panic in full remission), two alcohol dependence in early full remission (one with lifetime alcohol dependence and non-alcohol substance dependence in full remission (cannabis, amphetamine), one non-alcohol substance abuse (cannabis) in early full remission.
2 We examined number of specific memories rather than proportion of specific memories (number of specific memories controlling for omissions), because during debriefing most participants reported that when they had made an omission they actually had in mind non-specific content (for example, semantic associates, or self-related thoughts), which they withheld in order not to violate task instructions. It is possible that when in recovery, improvements in cognitive control reduce output of over-general memories—individuals are better able to retain task instructions and withhold incorrect responses. As such, omissions are likely to represent a mixture of different types of over-general response as well as true memory absences.
References
- Beck A. T., Steer R. A., Brown G. K. Manual for the BDI-II. San Antonio, TX: Psychological Corporation; 1996. [Google Scholar]
- Brewin C, Reynolds M., Tata P. Autobiographical memory processes and the course of depression. Journal of Abnormal Psychology. 1999;108:511–517. doi: 10.1037//0021-843x.108.3.511. [DOI] [PubMed] [Google Scholar]
- Brittlebank A. D., Scott J., Williams J. M. G., Ferrier I. N. Autobiographical memory in depression: State or trait marker. British Journal of Psychiatry. 1993;162:118–121. doi: 10.1192/bjp.162.1.118. [DOI] [PubMed] [Google Scholar]
- Burke M., Mathews A. Autobiographical memory and clinical anxiety. Cognition & Emotion. 1992;6:23–35. [Google Scholar]
- Carver C. S., Lawrence J. W., Scheier M. F. Self-discrepancies and affect: incorporating the role of feared selves. Personality and Social Psychology Bulletin. 1999;25:783–792. [Google Scholar]
- Carver C. S., Scheier M. F. On the self-regulation of behaviour. Cambridge, UK: Cambridge University Press; 1998. [Google Scholar]
- Conway M. A., Pleydell-Pearce C. W. The construction of autobiographical memories in the self-memory system. Psychological Review. 2000;107:261–288. doi: 10.1037/0033-295x.107.2.261. [DOI] [PubMed] [Google Scholar]
- Conway M. A., Singer J. A., Tagini A. The self and autobiographical memory: Correspondence and coherence. Social Cognition. 2004;22:491–529. [Google Scholar]
- Dalgleish T., Spinks H., Yiend J., Kuyken W. Autobiographical memory style in seasonal affective disorder and its relationship to future symptom remission. Journal of Abnormal Psychology. 2001;110:335–340. doi: 10.1037//0021-843x.110.2.335. [DOI] [PubMed] [Google Scholar]
- Dalgleish T, Tchanturia K., Serpell L., Herns S., Yiend J., de Silva P., et al. Self-reported abuse relates to autobiographical memory in patients with eating disorders. Emotion. 2003;3:211–222. doi: 10.1037/1528-3542.3.3.211. [DOI] [PubMed] [Google Scholar]
- First M. B., Spitzer R. L., Gibbon M., Williams J. B. Users guide for the Structured Clinical Interview for DSM-IVAxis I Disorders. Washington, DC: American Psychiatric Press; 1996. [Google Scholar]
- Frank E., Prien R. F, Jarrett R. B., Keller M. B., Kupfer D. J., Lavor P. W., et al. Conceptualisation and rational for consensus definitions of terms in major depressive disorder: response, remission, recovery, relapse, and recurrence. Archives of General Psychiatry. 1991;48:851–855. doi: 10.1001/archpsyc.1991.01810330075011. [DOI] [PubMed] [Google Scholar]
- Higgins E. T, Bond R. N., Klein R., Strauman T. Self-discrepancies and emotional vulnerability: How magnitude, accessibility and type of discrepancy influence affect. Journal of Personality and Social Psychology. 1986;5:5–15. doi: 10.1037/0022-3514.51.1.5. [DOI] [PubMed] [Google Scholar]
- Higgins T. E. Self-discrepancy: A theory relating self and affect. Psychological Review. 1987;94:319–340. [PubMed] [Google Scholar]
- Keller M. B., Shapiro R. W., Lavori P. W., Wolfe N. Recovery in major depressive disorder: Analysis with Life Table and regression models. Archives of General Psychiatry. 1982;39:905–910. doi: 10.1001/archpsyc.1982.04290080025004. [DOI] [PubMed] [Google Scholar]
- Kuyken W, Dalgleish T. Autobiographical memory and depression. British Journal of Clinical Psychology. 1995;34:89–92. doi: 10.1111/j.2044-8260.1995.tb01441.x. [DOI] [PubMed] [Google Scholar]
- Mackinger H. F, Pachinger M. M., Leibetseder M. M., Fartacek R. R. Autobiographical memories in women remitted from major depression. Journal of Abnormal Psychology. 2000;109:331–334. [PubMed] [Google Scholar]
- Martin L. M., Tesser A. Towards and motivational and structural model of ruminative thought. In: Uleman J. S., editor; Baragh J. A., editor. Unintended thought: Limits of awareness, intention and control. New York: Guilford Press; 1989. pp. 306–326. [Google Scholar]
- Martin L. M., Tesser A. Some ruminative thoughts. In: Wyer R. S. Jr., editor. Advances in social cognition. Vol. 9. Mahwah. NJ: Lawrence Erlbaum Associates, Inc; 1996. pp. 1–47. [Google Scholar]
- Matthews G., Wells A. Rumination, depression and metacognition: The S-REF model. In: Papageorgiou C., editor; Wells A., editor. Depressive rumination: Nature, theory & treatment. Chichester, UK: Wiley; 2004. [Google Scholar]
- Nandrino J., Pezard L., Poste A., Reveillere C, Beaune D. Autobiographical memory in major depression: A comparison between first-episode and recurrent patients. Psychopathology. 2002;35:335–340. doi: 10.1159/000068591. [DOI] [PubMed] [Google Scholar]
- Park R. J., Goodyer I. M., Teasdale J. D. Effects of induced rumination and distraction on mood and overgeneral memory in adolescent major depressive disorder and controls. Journal of Child Psychology and Psychiatry. 2004;45:996–1006. doi: 10.1111/j.1469-7610.2004.t01-1-00291.x. [DOI] [PubMed] [Google Scholar]
- Peeters F., Wessel I., Merckelbach H., Boom-Vermeeren M. Autobiographical memory specificity and the course of major depressive disorder. Comprehensive Psychiatry. 2002;43:344–350. doi: 10.1053/comp.2002.34635. [DOI] [PubMed] [Google Scholar]
- Raes F., Hermans D., Williams J. M. G., Demytte-naere K., Sabbe B., Pieters G., et al. Reduced specificity of autobiographical memory: A mediator between rumination and ineffective problem solving in major depression? Journal of Affective Disorders. 2005;87:331–335. doi: 10.1016/j.jad.2005.05.004. [DOI] [PubMed] [Google Scholar]
- Raven J., Raven J. C., Court J. H. Manual for the Mill Hill Vocabulary Scale. Oxford, UK: Oxford Psychologist Press; 1998. [Google Scholar]
- Raven J. C. Manual for the Advanced Progressive Matrices: Set 1. Oxford, UK: Oxford Psychologist Press; 1976. [Google Scholar]
- Roberts J. E., Carlos E. L. Impact of depressive symptoms, self-esteem and neuroticism on trajectories of overgeneral autobiographical memories over repeated trials. Cognition and Emotion. 2006;20:383–401. doi: 10.1080/02699930500341367. [DOI] [PubMed] [Google Scholar]
- Scher C. D., Ingram R. E., Segal Z. V. Cognitive reactivity and vulnerability: Empirical evaluation of construct activation and cognitive diathesis in unipolar depression. Clinical Psychology Review. 2005;25:487–510. doi: 10.1016/j.cpr.2005.01.005. [DOI] [PubMed] [Google Scholar]
- Spinhoven P., Bockting C. L. H., Kremers I. P., Schene A. H., Williams J. M. G. The endorsement of dysfunctional attitudes is associated with an impaired retrieval of specific autobiographical memories in response to matching cues. Memory. 2007;15:324–338. doi: 10.1080/09658210701256555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spinhoven P., Bockting C. L. H., Schene A. H., Koeter M. W J., Wekking E. M., Williams J. M. G, et al. Autobiographical memory in the euthymic phase of recurrent depression. Journal of Abnormal Psychology. 2006;115:590–600. doi: 10.1037/0021-843X.115.3.590. [DOI] [PubMed] [Google Scholar]
- Strauman T. J. Self-discrepancies in clinical depression and social phobia: cognitive structures that underlie emotional disorders? Journal of Abnormal Psychology. 1989;98:14–22. doi: 10.1037//0021-843x.98.1.14. [DOI] [PubMed] [Google Scholar]
- Watkins E., Teasdale J. D., Williams R. M. Decentring and distraction reduce overgeneral autobiographical memory in depression. Psychological Medicine. 2000;30:911–920. doi: 10.1017/s0033291799002263. [DOI] [PubMed] [Google Scholar]
- Wenzel A., Jackson L. C, Holt C. S. Social phobia and the recall of autobiographical memories. Depression and Anxiety. 2002;15:186–189. doi: 10.1002/da.10053. [DOI] [PubMed] [Google Scholar]
- Wenzlaff R. M., Bates D. E. Unmasking a cognitive vulnerability to depression: How lapses in mental control reveal depressive thinking. Journal of Personality and Social Psychology. 1998;75:1559–1571. doi: 10.1037//0022-3514.75.6.1559. [DOI] [PubMed] [Google Scholar]
- Wessel I., Meeren M., Peeters F., Arntz A., Merckelbach H. Correlates of autobiographical memory specificity: The role of depression, anxiety and childhood trauma. Behaviour Research & Therapy. 2001;39:409–421. doi: 10.1016/s0005-7967(00)00011-5. [DOI] [PubMed] [Google Scholar]
- Williams J. M. G, Barnhofer T, Crane C, Beck A. T. Problem solving deteriorates following mood challenge in formerly depressed patients with a history of suicidal ideation. Journal of Abnormal Psychology. 2005;114:421–431. doi: 10.1037/0021-843X.114.3.421. [DOI] [PubMed] [Google Scholar]
- Williams J. M. G, Barnhofer T, Crane C, Hermans D., Raes F., Watkins E., et al. Autobiographical memory specificity and emotional disorder. Psychological Bulletin. 2007;133:122–148. doi: 10.1037/0033-2909.133.1.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams J. M.G, Teasdale J. D., Segal Z. V., Soulsby J. Mindfulness-based cognitive therapy reduces over-general autobiographical memory in formerly depressed patients. Journal of Abnormal Psychology. 2000;109:150–155. doi: 10.1037//0021-843x.109.1.150. [DOI] [PubMed] [Google Scholar]