

Abstract
Objectives
We test associations of frequency of performing three types of socially productive activities (voluntary work, informal help and caring for a person) with depressive symptoms in older people. Is well-being positively associated with frequency in all three types or rather in those activities that are characterized by a high degree of autonomy and perceived control?
Methods
Data on social activities and frequency of performance were collected in the frame of the annual follow-up of the French GAZEL cohort study in 2005. Depressive symptoms were measured by the CES-D scale. Perceived control was assessed by two items of a quality of life measure (CASP-19). 14477 respondents aged 52 to 66 years completed a standardized questionnaire. Linear regression models were calculated adjusting for important confounders including self-rated health the previous year.
Results
In activities characterized by high autonomy (voluntary work, informal help) a negative association of frequency with depressive symptoms was observed, whereas the reverse effect was found in the type of activity with low autonomy (caring). Perceived control attenuated this latter association to some extent.
Conclusion
Being often socially productive in early old age may contribute to well-being to the extent that autonomy and perceived control are given.
Keywords: Age Factors; Aged; psychology; Caregivers; psychology; Cohort Studies; Depression; diagnosis; psychology; Female; Follow-Up Studies; France; Helping Behavior; Humans; Internal-External Control; Male; Middle Aged; Models, Psychological; Personal Autonomy; Prospective Studies; Quality of Life; Questionnaires; Social Behavior; Social Isolation; Voluntary Workers; psychology
Keywords: social productivity, frequency of investment, depressive symptoms, perceived control
Introduction
Participation of older people in social activities was shown to promote healthy ageing (Bath & Deeg, 2005). In particular, this holds true for activities involving some element of social productivity, such as voluntary work or providing help to other people (Glass et al., 1999; Maier & Klumb, 2005; Menec, 2003). Social productivity can be defined as any agreed upon continued activity that generates goods or services that are socially or economically valued by the recipient (s), whether or not based upon a formal contract (Siegrist et al. 2004). Findings documenting an association of social productivity with healthy ageing are concordant with the activity theory of ageing which claims that activities including social contacts provide opportunities to experience role support. Role support in turn can confirm a positive self-concept (Lemon et al., 1972; Reitzes et al., 1995). In fact, Herzog and colleagues (1998) observed that social activities are positively associated with a sense of personal empowerment (‘agentic self’) that largely accounts for the observed association with well-being. Similarly, Krause et al. (1992) found that providing social support to others was indirectly related to reduced risks of depressive symptoms, as mediated by feelings of personal control.
Activity theory also claimed that the positive effect of a socially productive activity is contingent on its frequency as positive self experience may occur more frequently. Few studies examined this assumption explicitly, but several results seem to indicate a threshold effect of frequency on well-being (Morrow-Howell et al., 2003; Musick et al., 1999; van Willigen, 2000). However, well-being may not only depend on the frequency of an activity (up to a certain level), but equally so on nature or specific characteristics of the social activity under study. One such characteristic concerns the quality of social exchange inherent in productive activities. In a recent study we documented a strong association of quality of social exchange in terms of experienced reciprocity with well-being (Wahrendorf et al., 2006). Experience of non-reciprocity (high efforts in combination with low rewards; Siegrist, 1996) was related to reduced well-being and elevated levels of depressive symptoms. This was particularly the case in people who were caring for a sick person.
Degree of autonomy and perceived control in choosing and performing a socially productive activity may be a second characteristic with relevance to well-being, due to the fact that self-determination is considered a critical element of positive self experience (Haid & Rodin 1999).
In this report, we analyse relationships between frequency of investment in three types of socially productive activities and depressive symptoms: voluntary work, informal help and caring for a person. We hypothesise that frequency of productive activities with a high degree of autonomy and perceived control (voluntary work, informal help) is negatively associated with depressive symptoms, whereas the opposite is the case in activities with a low degree of autonomy, such as caring for a sick person. Furthermore, we expect that perceived control may attenuate this latter association to some extent.
Methods
Data
Our analyses are based on data from the French GAZEL cohort study. The GAZEL cohort was established in 1989 and is followed annually by a self-administered questionnaire. Data on socially productive activities were included in 2005. At study onset the sample included 20624 individuals aged 35–50 years working at the French National Electric and Gas Company (for detailed cohort profile see Goldberg M. et al., 2006). The response rate in 2005 was 75% (N=14477).
Measurement
Socially productive activities
three types of socially productive activities are considered in our analysis measured in 2005: 1. Done voluntary or charity work 2. Provided help to family, friends or neighbors 3. Cared for a sick or disabled adult. For each activity respondents were asked whether they engaged in one or more of these activities during the last month and, if so, how often. Response categories were “almost daily”, “almost every week”, “less often” and “never”. While most studies including levels of involvement used number of hours engaged during the last year, previous investigations showed that assessing frequency as mentioned above, appears to be more valid, specifically in elderly populations (Tourangeau, 2000).
Depressive symptoms
To measure depressive symptoms we applied the original form of the Center for Epidemiologic Studies Depression (CES-D) scale included in 2005. The CES-D scale is a well established instrument for measuring depressive symptoms in general population surveys (Radloff, 1977) reflecting reduced emotional well being. The total sum score of the 20 four-point Likert scale items ranges from 0 to 60, with higher scores indicating more depressive symptoms. Cronbach’s alpha was .89. While it does not meet the standard of a physician-based diagnosis of depression, this instrument was nevertheless shown to be a valid and a consistent indicator of elevated levels of depressive symptoms (Weismann et al., 1977).
Perceived Control
We use two items from the CASP-19 questionnaire (Hyde et al., 2003), a theory-based measurement of quality of life in older people, to measure perceived control that was part of the 2005 questionnaire. Respondents were asked to answer the following statements: (1) “I feel that what happens to me is out of my control.” and (2) “I can do the things that I want to do.” Response categories were: “Often”, “Sometimes”, “Rarely” or “Never”. If participants experienced “often” or “sometimes” (first statement) and/or “rarely” or “never” (second statement) they were categorised as having a low degree of perceived control.
Additional Measures
To control for a possible bias produced by the participants’ general health status we included self-report information on their health status that was collected in the year preceding this survey. The question was: “How do you rate your general health status?”. Response categories range from ‘very good’ (coded 1) to ‘very poor’ (coded 8). This item was previously shown to be strongly associated with physical disease in the GAZEL cohort (Goldberg, P. et al., 2001). Participants with answers ranging from 5 to 8 were considered to exhibit poor health. Additionally, we included information on age, gender, retirement status, marital status, and three indicators of social position, education, income and occupation. Income information was based on the total monthly household income assessed in the questionnaire in 2002. Occupational groups (managers, supervisory employees, operating employees) measured in 2005, were available from the EdF-GdF administrative department. Education was assessed by the highest educational degree declared in 1989.
Statistical Analysis
First, we describe the prevalence of socially productive activities in our study population according to relevant socio-demographic variables. Secondly, we analyze associations between measures of socially productive activities and depressive symptoms. Thirdly, multivariate regression modeling is applied to test significant associations of frequency of socially productive activities with depressive symptoms. In addition to the three activities, the regression model includes the socio-demographic and socioeconomic variables (age, gender, retirement status, marital status, number of household members, income, occupation and education) as well as self-rated health the previous year. In a final step, perceived control is introduced to examine the relative importance in explaining associations between activities and depressive symptoms. Traditional model diagnostics were done based on residual analysis. Calculations and figures were estimated with the statistical package STATA version 9.2 (Kohler & Kreuter, 2005).
Results
Concerning sample characteristics, 72.8 per cent of the participants are men. 80.5 per cent of the cohort are retired and the age range is 52 to 66 years with a mean age of 61 years for men and 58 years for women.
In Table 1 we observe that voluntary work and informal help show the highest overall prevalence, whereas only few people engage in care for a person. In view of frequency of involvement, more than half of the volunteers were engaged almost every week or more frequently, whereas those who cared for a person were comparatively less often involved. Considering retirement status, retired persons, with the exception of caring for a person, are socially more active compared to those who are still working. With respect to gender, differences for volunteering (more men) and caring for a person (more women) are observed. In addition, the prevalence of volunteering increases with age.
Table 1.
Prevalence of socially productive activities (%; N=14477)
| Frequency among participants (%) |
|||||
|---|---|---|---|---|---|
| Type of Activity | Participate (%) | Almost daily | Almost every week | Less often | |
| Voluntary work overall) | 54.3 | 22.0 | 38.3 | 39.7 | |
| Gender | Male | 58.8 | 23.5 | 37.9 | 38.6 |
| Female | 41.3 | 15.4 | 40.3 | 44.3 | |
| Age | 52–58 | 47.9 | 19.2 | 37.8 | 43.1 |
| 59–62 | 57.6 | 22.6 | 38.7 | 38.7 | |
| 63–66 | 57.3 | 23.8 | 38.3 | 37.9 | |
| Retired | Yes | 57.0 | 22.7 | 39.1 | 38.2 |
| No | 43.3 | 18.1 | 34.1 | 47.8 | |
| Informal help (overall) | 94.6 | 11.5 | 41.0 | 47.5 | |
| Gender | Male | 95.1 | 10.6 | 41.5 | 47.9 |
| Female | 93.3 | 14.0 | 39.6 | 46.4 | |
| Age | 52–58 | 93.3 | 10.8 | 40.5 | 48.8 |
| 59–62 | 95.6 | 12.0 | 40.9 | 47.1 | |
| 63–66 | 94.9 | 11.6 | 41.7 | 46.7 | |
| Retired | Yes | 95.6 | 12.1 | 41.7 | 46.3 |
| No | 90.9 | 8.7 | 38.2 | 53.1 | |
| Care for a person (overall) | 26.4 | 18.1 | 27.2 | 54.6 | |
| Gender | Male | 25.2 | 16.1 | 26.9 | 57.0 |
| Female | 30.0 | 23.1 | 28.0 | 49.0 | |
| Age | 52–58 | 25.7 | 19.5 | 25.0 | 55.4 |
| 59–62 | 26.8 | 16.6 | 28.4 | 54.9 | |
| 63–66 | 26.8 | 18.6 | 28.0 | 53.4 | |
| Retired | Yes | 26.4 | 18.3 | 27.9 | 53.8 |
| No | 26.5 | 17.6 | 24.5 | 57.9 | |
Figure 1 shows mean CES-D scores according to frequency of engagement. Voluntary work and informal help are negatively associated with depressive symptoms. In contrast, care for a person is positively related to depressive symptoms. The more people engage, the higher is their CES-D score. While associations are linear in case of volunteering (negative) and caring (positive) we observe a non-linear relation in case of informal health, with a higher CES-D score in those who are engaged on a daily basis.
Figure 1.
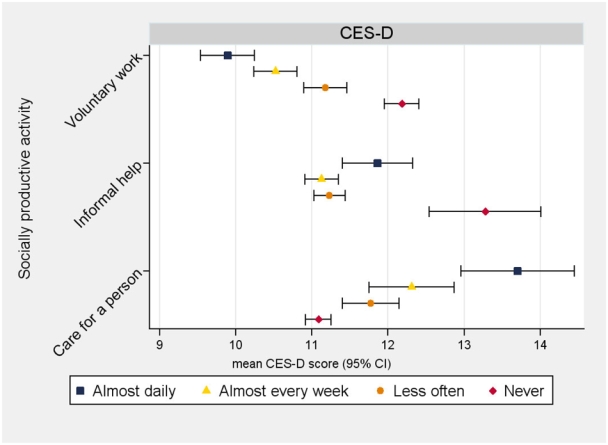
Well-being and socially productive activities: Mean scores and CI (95%; N=14477)
The first model of our multivariate analysis confirms bivariate results (table 2, model 1). Findings remain unchanged after controlling for important confounders including self-rated health the previous year. Again, we observe significantly higher scores of depressive symptoms for those who care for a person, whereas voluntary work and informal help is negatively associated with depressive symptoms.
Table 2.
Association of socially productive activities with depressive symptoms (unstand. regression coefficients; N=14477)
| Model |
|||||||
|---|---|---|---|---|---|---|---|
| Variables | Ia | IIb | |||||
| Coef. | CI 95% | P | Coef. | CI 95% | P | ||
| Voluntary work | Almost daily | −0.80 | (−1.29 to −0.30) | 0.002 | −0.58 | (−1.03 to −0.12) | 0.014 |
| Almost every week | −0.67 | (−1.07 to −0.27) | 0.001 | −0.45 | (−0.82 to −0.08) | 0.018 | |
| Less often | −0.30 | (−0.69 to 0.09) | 0.130 | −0.23 | (−0.59 to 0.13) | 0.217 | |
| Never | 0 | - | - | 0 | - | - | |
| Informal help | Almost daily | −1.22 | (−2.02 to −0.41) | 0.003 | −1.01 | (−1.76 to −0.26) | 0.008 |
| Almost every week | −1.30 | (−1.99 to −0.60) | 0.000 | −1.15 | (−1.79 to −0.50) | 0.001 | |
| Less often | −1.12 | (−1.79 to −0.44) | 0.001 | −0.95 | (−1.58 to −0.31) | 0.003 | |
| Never | 0 | - | - | 0 | - | - | |
| Care for a person | Almost daily | 1.72 | (0.98 to 2.46) | 0.000 | 1.02 | (0.33 to 1.70) | 0.004 |
| Almost every week | 1.02 | (0.42 to 1.62) | 0.001 | 0.52 | (−0.04 to 1.08) | 0.069 | |
| Less often | 0.77 | (0.34 to 1.20) | 0.000 | 0.46 | (0.06 to 0.86) | 0.025 | |
| Never | 0 | - | - | 0 | - | - | |
Adjusted for gender, age, retirement status, education, occupation, income, number of household members, marital status and self-rated health the previous year
Model I + perceived control
In the second model of table 2, the indicator of perceived control is additionally entered. Adjusting for perceived control attenuates the coefficients for all categories of the three activities, most markedly for caring (see also figure 2). In this latter case, the reduction is 41% for daily care, 49% for weekly care and 40% for caring less often. Less striking reductions are seen for voluntary work (28% for daily, 33% for weekly and 23% for less frequent volunteering) and for informal help (17% for daily, 11% for weekly and 15 % for less frequent informal help). Results are interpreted as moderate support of a mediation effect where a high level of personal control reduces the effect of frequency of engagement on depressive symptoms, particularly so in the type of activity with a low degree of autonomy.
Figure 2.
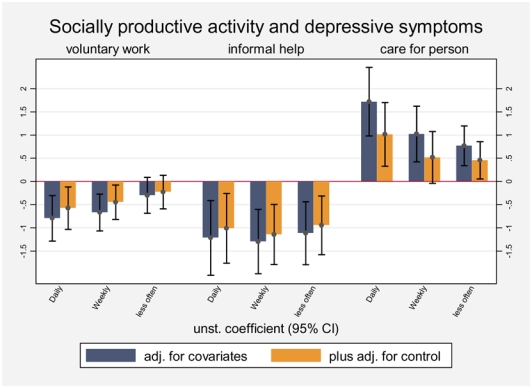
Association of socially productive activities with depressive symptoms (unstand. regression coefficients and 95% confidence intervals/based on table 2; N=14477)
Discussion
This study examined associations of frequency of investment in three socially productive activities (voluntary work, informal help, care for a person) and depressive symptoms in early old age people, based on the French GAZEL study.
Our central findings indicate that the frequency of an activity with a high degree of autonomy and perceived control is negatively related to depressive symptoms (in particular voluntary work), whereas a positive relation is observed in a productive activity that is characterized by a low degree of autonomy (caring for a sick person). This latter result is further substantiated by the fact that the amount of perceived control attenuates the effect of frequency of performance on severity of depressive symptoms.
Our findings are in line with the activity theory of ageing (Lemon et al., 1972), but add a new element to its predictions with regard to health and well-being. The beneficial effect of frequency of performing a socially productive activity on depressive symptoms seems to be contingent on its quality in terms of experiencing autonomy and perceived control. In contrast, if people are engaged in a socially productive activity with low degree of autonomy, a reverse effect is observed: the more frequent this activity is performed, the more depressive symptoms are experienced. Results underline the crucial role of sense of control for health and well-being that was documented both in midlife (Bosma, 2006; Lachman & Weaver, 1998; Marmot, 2004) and old age (Baltes & Baltes, 1986; Haidt & Rodin, 1999).
The benefits of social activities might not only depend on type of the activity but also on socio-demographic characteristics of the providers, such as retirement status. For instance, frequent informal help may not enhance feelings of control in providers who are still regularly employed as this cumulative burden threatens the providers’ autonomy. In fact, additional multivariate analyses of the two groups of retired versus non-retired participants confirmed that the beneficial effect of frequent engagement is restricted to the former group. A similar argument concerns women with multiple roles (Moen et al., 1992). This assumption was supported by further analyses where no benefits were observed for women involved in daily informal help.
The interpretation of the results of this study is restricted by several limitations. First, given the cross-sectional study design we cannot draw any conclusion concerning the causal direction of the observed association. It is possible, though unlikely, that people with depressive symptoms engage more often in caring activities and less often in voluntary work. Yet, we adjusted our analyses for level of self-reported health in the year preceding the data collection. Secondly, a selection bias of those participants who engage in any of the three types of activity is possible due to a well documented association between social activity and general health status (Menec, 2003). However, as indicated in table 1, a large majority of the total sample was engaged in at least one of the three activities to a moderate degree.
A third limitation concerns the measurement of social activities and of perceived control. Information was restricted to three main types of activities: volunteering, informal help, and caring for a sick person. Although these are activities with relatively highest prevalence at older age it is possible that inclusion of additional activities might have changed the results. Our measure of perceived control must be considered an unsatisfactory proxy of the notion of sense of control (Lachman & Weaver, 1998) which prevents a more substantial interpretation of results of the second model in Table 2. More specifically, we cannot distinguish to what extent the mediation effect is due to control in terms of perceived situational characteristics (Averill, 1973) or in terms of generalized control beliefs (Rotter, 1966). Finally, despite the fact that our measure of depressive symptoms is a well validated screening instrument at population level (Weisman et al., 1977), no clinical diagnoses could be included in this analysis. Therefore, it is not clear whether the strong positive association of frequency of caring for a sick person with depressive symptoms can be interpreted as further support of available evidence on a health-adverse effect of caring (Epel et al., 2004; Lee et al., 2003; Schulz & Beach, 1999).
Despite these restrictions the current report supports the general assumption of activity theory of ageing, but adds an important element by pointing to the role of specific characteristics of the socially productive activity under study, in particular the degree of autonomy and perceived control available to acting providers. According to our results, beneficial effects of frequently performed productive activities are bound to this latter condition. If further validated findings may have implications for recommendations, measures and opportunities of social productivity among older people that contribute to healthy ageing.
References
- AVERILL JR. Personal control over aversive stimuli and its relationship to stress. Psychological Bulletin. 1973;80:286–303. [Google Scholar]
- BALTES MM, BALTES PB. The Psychology of Control and Aging. Hillsdale, N.J: Erlbaum; 1986. [Google Scholar]
- BATH PA, DEEG D. Social engagement and health outcomes among older people: introduction to a special section. European Journal of Ageing. 2005;2:24–30. doi: 10.1007/s10433-005-0019-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BOSMA H. Socioeconomic differences in health: Are control beliefs fundamental mediators? In: SIEGRIST J, MARMOT M, editors. Social Inequalities in Health: New Evidence and Policy Implications. Oxford: Oxford University Press; 2006. pp. 153–166. [Google Scholar]
- EPEL ES, BLACKBURN EH, LIN J, DHABHAR FS, ADLER NE, MORROW JD, CAWTHON RM. Accelerated telomere shortening in response to life stress. Proceedings of the National Academy of Sciences. 2004;101:17312–17315. doi: 10.1073/pnas.0407162101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GLASS TA, MENDES DE LEON C, MAROTTOLI RA, BERKMAN LF. Population based study of social and productive activities as predictors of survival among elderly Americans. British Medical Journal. 1999;319:478–483. doi: 10.1136/bmj.319.7208.478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GOLDBERG M, LECLERC A, BONEFANT S, CHASTANG JF, SCHMAUS A, KANIESWSKI N, ZINS M. Cohort profile: the GAZEL Cohort Study. International Journal of Epidemiology. 2006 doi: 10.1093/ije/dyl247. published online on November 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GOLDBERG P, GUEGUEN A, SCHMAUS A, NAKACHE JP, GOLDBERG M. Longitudinal study of associations between perceived health status and self reported diseases in the French GAZEL cohort. Journal of Epidemiology and Community Health. 2001;55:233–238. doi: 10.1136/jech.55.4.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HAIDT J, RODIN J. Control and efficacy as interdisciplinary bridges. Review of General Psychology. 1999;3:317–337. [Google Scholar]
- HERZOG AR, FRANKS MM, MARKUS HR, HOLMBERG D. Activities and well-being in older age: effects of self-concept and educational attainment. Psychology & Aging. 1998;13:179–185. doi: 10.1037//0882-7974.13.2.179. [DOI] [PubMed] [Google Scholar]
- HYDE M, WIGGINS RD, HIGGS P, BLANE DB. A measure of quality of life in early old age: the theory, development and properties of a needs satisfaction model (CASP-19) Aging & Mental Health. 2003;7:186–194. doi: 10.1080/1360786031000101157. [DOI] [PubMed] [Google Scholar]
- IDLER EL, BENYAMINI Y. Self-rated health and mortality: A review of twenty-seven community studies. Journal of Health and Social Behavior. 1997;38:21–37. [PubMed] [Google Scholar]
- KOHLER U, KREUTER F. Data Analysis Using Stata. College Station: Stata Press; 2005. [Google Scholar]
- KRAUSE N, HERZOG AR, BAKER E. Providing support to others and well-being in later life. Journal of Gerontology. 1992;47:300–311. doi: 10.1093/geronj/47.5.p300. [DOI] [PubMed] [Google Scholar]
- LACHMAN ME, WEAVER SL. Sociodemographic variations in the sense of control by domain: findings from the MacArthur studies of midlife. Psychology and Aging. 1998;13:553–562. doi: 10.1037//0882-7974.13.4.553. [DOI] [PubMed] [Google Scholar]
- LEE S, COLDITZ GA, BERKMAN LF, KAWACHI I. Caregiving and risk of coronary heart disease in U.S. women: a prospective study. American Journal of Preventive Medicine. 2003;24:113–119. doi: 10.1016/s0749-3797(02)00582-2. [DOI] [PubMed] [Google Scholar]
- LEMON BW, BENGSTON VL, PETERSON JA. An exploration of the activity theory of aging: activity types and life-satisfaction among in-movers to a retirement community. Journal of Gerontology. 1972;27:511–523. doi: 10.1093/geronj/27.4.511. [DOI] [PubMed] [Google Scholar]
- MAIER H, KLUMB PL. Social participation and survival at older ages: is the effect driven by activity content or context? European Journal of Ageing. 2005;1:31–39. doi: 10.1007/s10433-005-0018-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MARMOT M. Status Syndrome. London: Bloomsbury; 2004. [Google Scholar]
- MENEC VH. The relation between everyday activities and successful aging: a 6-year longitudinal study. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2003;58:74–82. doi: 10.1093/geronb/58.2.s74. [DOI] [PubMed] [Google Scholar]
- MOEN P, DEMPSTER-MC CLAIN D, WILLIAMS RM., JR Successful aging: A life-course perspective on women’s multiples roles and resilience. American Journal of Sociology. 1992;97:1612–1638. [Google Scholar]
- MORROW-HOWELL N, HINTERLONG J, ROZARIO PA, TANG F. Effects of volunteering on the well-being of older adults. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2003;58:137–145. doi: 10.1093/geronb/58.3.s137. [DOI] [PubMed] [Google Scholar]
- MUSICK MA, HERZOG AR, HOUSE JS. Volunteering and mortality among older adults: findings from a national sample. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 1999;54:173–180. doi: 10.1093/geronb/54b.3.s173. [DOI] [PubMed] [Google Scholar]
- RADLOFF LS. The CES-D scale: A self report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- REITZES DC, MUTRAN EJ, VERRIL LA. Activities and self-esteem. Research on Aging. 1995;17:260–277. [Google Scholar]
- ROTTER JB. Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs. 1966;80:1–28. [PubMed] [Google Scholar]
- SCHULZ R, BEACH SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. Journal of the American Medical Association. 1999;282:2215–2219. doi: 10.1001/jama.282.23.2215. [DOI] [PubMed] [Google Scholar]
- SIEGRIST J. Adverse health effects of high-effort/low-reward conditions. Journal of Occupational Health Psychology. 1996;1:27–41. doi: 10.1037//1076-8998.1.1.27. [DOI] [PubMed] [Google Scholar]
- SIEGRIST JVD, KNESEBECK O, POLLACK CE. Social productivity and well-being of older people: A sociological exploration. Social Theory & Health. 2004;2:1–17. [Google Scholar]
- TOURANGEAU R, RIPS LJ, RASINSKI K. The Psychology of Survey Response. Cambridge: Cambridge University Press; 2000. [Google Scholar]
- VAN WILLIGEN M. Differential benefits of volunteering across the life course. Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2000;55:308–318. doi: 10.1093/geronb/55.5.s308. [DOI] [PubMed] [Google Scholar]
- WAHRENDORF SMVD, KNESEBECK O, SIEGRIST J. Social Productivity and well-being of older people: results from the SHARE study. European journal of Ageing. 2006;3:67–73. doi: 10.1007/s10433-006-0028-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WEISMANN MM, SHOLOMSKAS D, POTTENGER M, PRUSOFF BA, LOCKE BZ. Assessing depressive symptoms in five psychiatric populations: a validation study. American Journal of Epidemiology. 1977;106:203–214. doi: 10.1093/oxfordjournals.aje.a112455. [DOI] [PubMed] [Google Scholar]