

Dear Editor,
Spontaneous venous pulsation (SVP) is a result of the variation in the pressure gradient along the retinal vein as it traverses the lamina cribrosa.[1] When the intracranial pressure (ICP) rises, the intracranial pulse pressure also rises to equal the intraocular pulse pressure and the SVP ceases.
Optic disc edema can occur with or without a raised ICP. Cessation of the SVP is a sensitive marker of raised ICP. However, even in the presence of a normal ICP, optic disc edema has been considered to cause cessation of SVP.[2] We recently discovered pseudo-tumor cerebri in a 57-year-old female suffering from headache. Her vision was 20/40 in the right eye (RE), N8; counting fingers close to face in the left eye (LE) due to anisometropic amblyopia. SVP was seen on both edematous optic nerves in the erect posture and disappeared upon lying down (Figs 1–7). Magnetic resonance imaging revealed widened perioptic cerebrospinal fluid (CSF) spaces and empty sella. Her CSF opening pressure in lateral recumbent posture was 400 mm of H2O. She was not anemic and her systemic blood pressure was 140/90 mmHg.
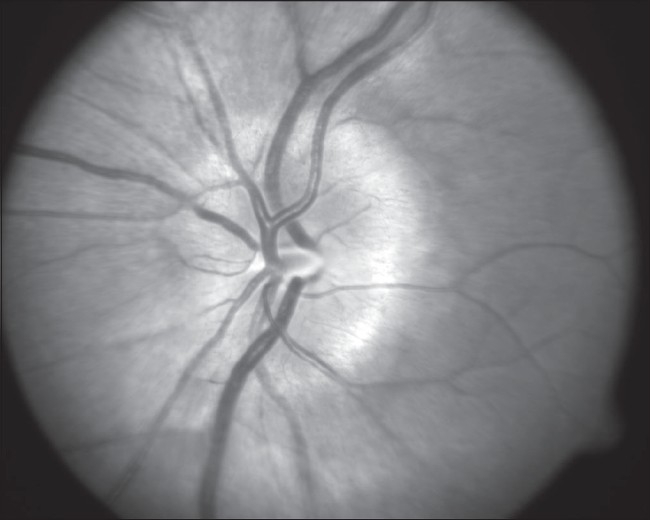
Figure 1.
Photograph of the Left optic disc showing disc edema
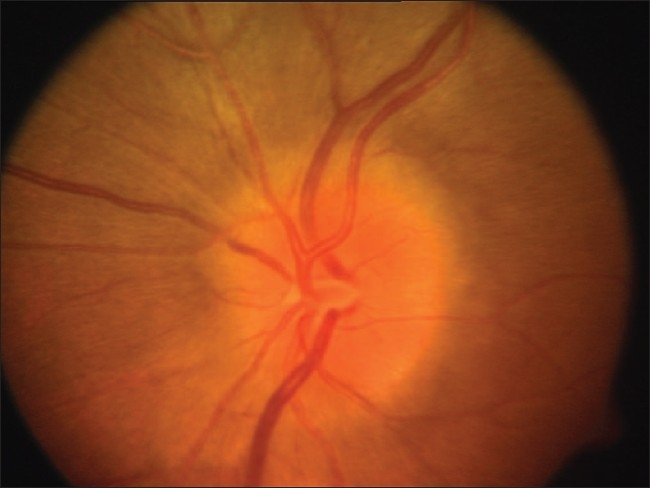
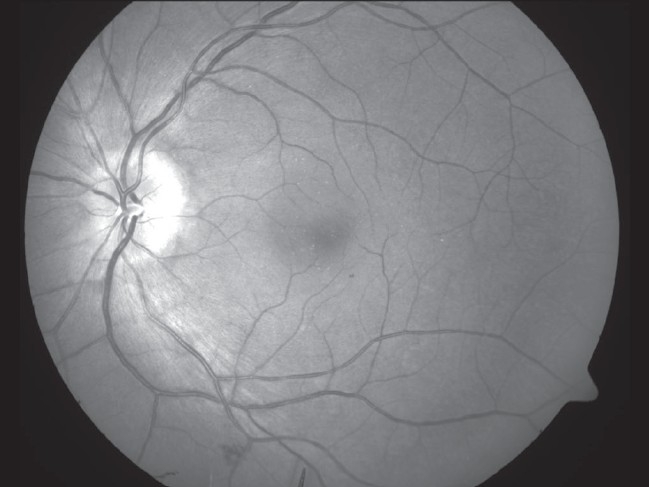
Figure 7.
Red free photograph of the edematous Right optic disc.A central corneal scar affected clarity of the images of the Right eye
Figure 2.
As she is one eyed and papilledema is an emergency, we obtained fundus photographs after she received treatment for raised intracranial pressure for 5 days. The visible optic disc edema is less than that was seen at her initial presentation
Figure 3.
OS (Left eye) fundus photograph
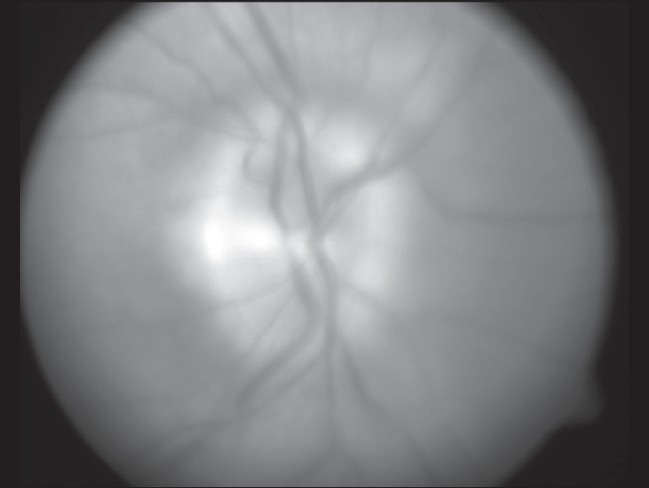
Figure 4.
OS (Left eye) red free fundus photograph
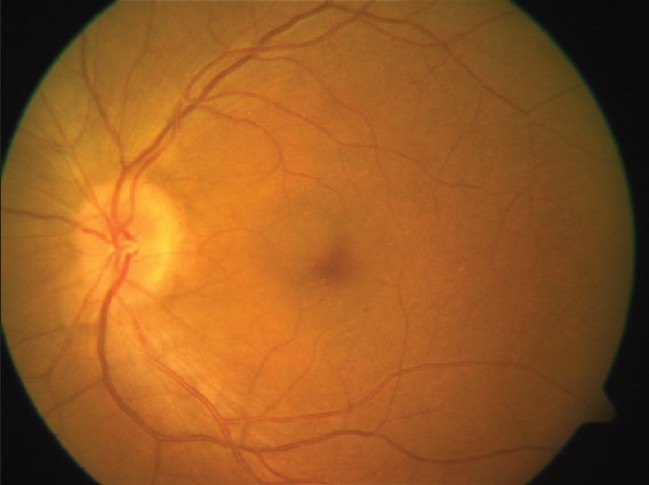
Figure 5.
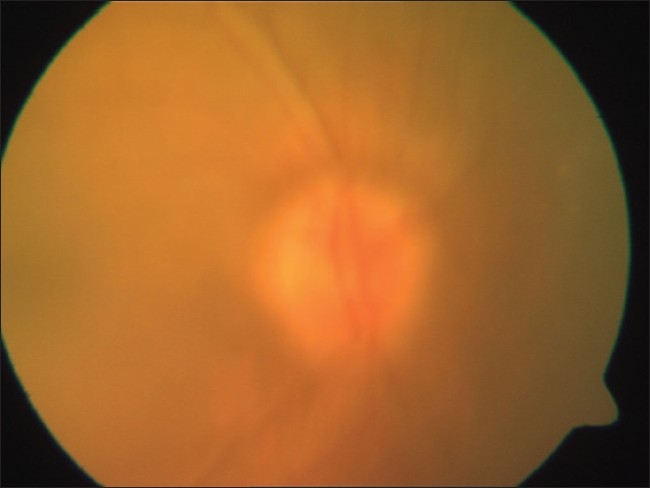
OD (Right eye) fundus photograph
Figure 6.
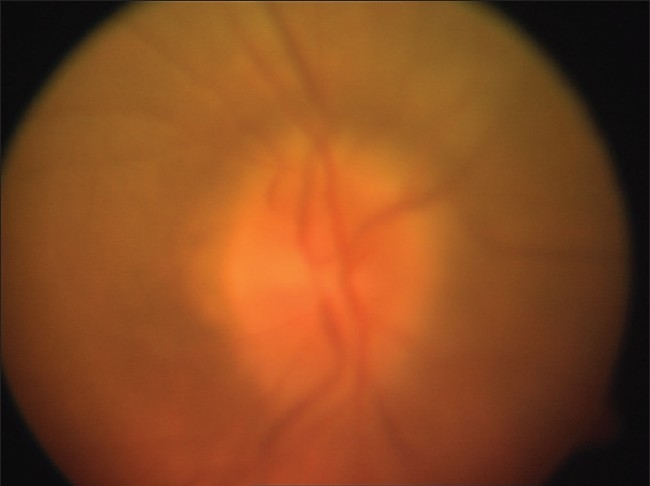
Photograph of the Right optic disc showing disc edema
SVP is seen in the majority of normal eyes in which the central retinal vein can be followed, unobscured by optic disc arteries or glial tissue, as it enters the cup.[3] However, the effect of optic disc size on the visibility of SVP has never been investigated. Logically, a large optic disc with a large physiologic cup would have more space to enable central vein to be seen entering the depth of the cup. In our case, optic discs were moderate to large (vertical diameter being 1.95 and 1.74 mm in RE and LE respectively) with a correspondingly larger physiological cup.
In pathological studies, a common pathway of axoplasmic stasis at the level of lamina cribrosa has been demonstrated to lead to optic disc edema of any etiology.[4] Moreover, in most individuals the amplitude of SVP is low and therefore the venous collapse spreads retrograde for a short distance from the exit point of the central retinal vein.[1] Therefore, when the ICP is normal, SVP may be obscured by the swollen axons but not necessarily diminished by them.
SVP is reported, albeit rarely, on a swollen optic disc in patients without elevated ICP.[2] On the other hand, McKee et al.[5] reported a case similar to ours. They could visualize SVP in the presence of a markedly elevated optic disc. The CSF opening pressure in their patient was 400 mm of H2O.[5] However, they have not commented on the size of the optic disc and the effect of posture on the visibility of SVP. A sudden lowering of the CSF pressure to normal does not produce immediate resolution of optic disc edema.[4] Owing to the effect of the spinal sac in CSF dynamics, a raised ICP is reduced in the erect posture. When such fluctuation in ICP touches normality, SVP may appear and be visible in a large edematous optic disc with a large physiologic cup as long as the optic cup is not completely obliterated by the swollen axons.
References
- 1.Levine DN. Spontaneous pulsation of the retinal veins. Microvasc Res. 1998;56:154–65. doi: 10.1006/mvre.1998.2098. [DOI] [PubMed] [Google Scholar]
- 2.McCulley TJ, Lam BL, Bose S, Feuer WJ. The effect of optic disk edema on spontaneous venous pulsations. Am J Ophthalmol. 2003;135:706–8. doi: 10.1016/s0002-9394(03)00122-3. [DOI] [PubMed] [Google Scholar]
- 3.Hedges TR, Jr, Baron EM, Hedges TR, 3rd, Sinclair SH. The retinal venous pulse. Its relation to optic disc characteristics and choroidal pulse. Ophthalmology. 1994;101:542–7. [PubMed] [Google Scholar]
- 4.Hayreh SS. Optic disc edema in raised intracranial pressure. V. Pathogenesis. Arch Ophthalmol. 1977;95:1553–65. doi: 10.1001/archopht.1977.04450090075006. [DOI] [PubMed] [Google Scholar]
- 5.McKee HD, Ahad MA. Spontaneous retinal venous pulsations can be present with a swollen optic disc. J Neurol Neurosurg Psychiatry. 2004;75:941. author reply 941. [PMC free article] [PubMed] [Google Scholar]