

Abstract
BACKGROUND
The purpose of our study was to perform a large cross-sectional study aimed at determining the postnatal growth pattern of the clavicle from birth to 18 years of age.
METHODS
We analyzed digital chest radiographs of a convenience sample of 961 individuals between birth and 18 years of age. Malrotated radiographs were excluded. Right and left clavicle lengths were measured in millimeters from the most lateral ossified border to the most medial ossified border of each clavicle. Study subjects were divided into 19 subgroups with the first group being labeled “birth to 11 months of age” followed by 1 year olds, 2 year olds, etc. Subjects were also grouped by gender. There was a minimum of 25 subjects in each group.
RESULTS
At 18 years of age the mean±SD clavicle length for females was 149±12 mm and for males it was 161±11 mm. Although a statistically significant difference (p=0.049) was noted between the length of right and left clavicles it was not clinically significant (0.036 mm). A steady growth rate was noted for both genders from birth to age 12 years (8.4 mm per yr). Above age 12 there were significant differences in the growth of the clavicles of girls (2.6 mm per yr) versus boys (5.4 mm per yr) (p<0.001). Our data suggest that females achieve 80% of their clavicle length by 9 years of age and boys by 12 years of age.
CONCLUSION
This cross-sectional study establishes that relatively little clavicle growth (20%) remains for girls beyond age 9 years and for boys beyond 12 years. The length of one clavicle may be properly judged by comparing it to the contralateral clavicle.
CLINICAL RELEVANCE
Remodeling of clavicle shaft fractures is currently believed to be proportional to growth remaining. Our study questions the capacity of the clavicle to re-establish normal length beyond the age thresholds we have identified.
INTRODUCTION
The clavicle is the most commonly fractured bone about the shoulder in children.1,2 The treatment standard for virtually all clavicle fractures has been nonoperative in nature, often consisting of a simple sling.3,4 The success of such nonoperative treatment has been attributed to the remarkable remodeling potential of growing children.5-7 In fact the following has been said of clavicle fractures in children: “If the two ends of the clavicle are in the same room they will heal and remodel adequately.”6
In sharp contrast to the abundant confidence in clavicle fracture remodeling, remarkably little data actually exist regarding the growth of the clavicle. Ernest Gardner outlined the pre-natal growth of the clavicle, pointing out that intramembranous ossification of the clavicle begins at 5 ½ weeks gestation and at 8 weeks it has assumed the typical S-shaped configuration spanning the distance between acromion and sternum.8 Age specific delineation of bone growth, commonly used for the spine and extremities, has simply not been performed for the clavicle.9-13 The purpose of our study was to determine the postnatal growth pattern of the clavicle from birth to eighteen years of age.
MATERIALS & METHODS
A convenience sample of individuals from birth to eighteen years of age was selected from roentgenograms in our institution’s digital radiographic database. Approval for this cross-sectional, observational study was obtained from our institutional review board. Patients were included in the study if they were younger than nineteen years of age and had an available chest radiograph that clearly displayed both clavicles. Patients were excluded if they had any musculoskeletal deformity (i.e. scoliosis), chest trauma, clavicle fracture or previous spine surgery evident by surgical hardware, along with congenital or acquired growth conditions noted in the radiographic report.
All available radiographic records for each subject were screened to identify any exclusion not readily present on the image being measured. Further exclusion occurred using the method described by Lazarides and Zafiropoulos to identify roentgenograms with excessive chest rotation that could alter the appearance of the clavicle giving false measurements.14 At our institution, the standardized technique followed by our radiology technicians is to perform AP chest radiographs of children less than four years of age in a supine position with the beam forty inches away. Children four years of age and older are positioned upright with the beam seventy-two inches away. Specific radiographic parameters are also adjusted for age and these technique standards are presented in Table 1.
Table 1.
Pediatric Chest X-Ray Standards
| Patient Age | Patient Position | Distance | mAs | kVp |
|---|---|---|---|---|
| Neonate | Supine | 40″ | 1 | 65 |
| Infant (0-2) | Supine | 40″ | 1.25 | 65 |
| Toddler (2-4) | Supine | 40″ | 1.25/1.6 | 65 |
| Child (4-6) | Upright | 72″ | 5 | 65 |
| Pre-Teen (6-12) | Upright | 72″ | 6.4 | 65 |
| Teen/Adult | Upright | 72″ | 8 | 65 |
The subjects were divided into nineteen groups based upon chronological age, the first comprised of infants from newborn through eleven months of age. The following eighteen groups were separated by each chronological year, one-year-olds, two-year-olds, etc. The nineteen groups were also subdivided by gender with a minimum of 25 males and 25 females in each subgroup. The minimum of 25 subjects in each subgroup was chosen based upon previous large cross-sectional orthopaedic studies.15-17
The clavicle lengths were measured in millimeters using the ruler application in the Centricity Enterprise Web V2.1 PACS viewing system (GE Healthcare, Chalfont St. Giles, Buckinghamshire, United Kingdom). As demonstrated in Figures 1 & 2, the starting point was the most lateral border of the clavicle present at the intersection of the clavicle and the acromioclavicular joint with the ending point the most medial border identifiable on the roentgenogram at the intersection of the clavicle and the sternoclavicular joint.
Figure 1.

Posteroanterior chest radiograph of a normal patient demonstrating the measured length (mm) of a nearly straight clavicle.
Figure 2.

Posteroanterior chest radiographs of a normal patient demonstrating the measured length (mm) the commonly seen S-shaped clavicle.
One researcher screened and measured all subjects to omit inter-examiner variability. Thirty radiographs (60 clavicles) were measured by three researchers to estimate inter-examiner variability. Intra-observer reliability was also assessed by one researcher measuring the same set of thirty roentgenograms on three separate occasions over a two-week period.
Statistical Methods
Means and standard deviations are used to describe the data. Paired-sample t-tests with probability values (p-values) of less than or equal to 0.05 defined as significant were used to compare left and right clavicles. Linear mixed models were used to estimate the growth of the clavicle over time, taking into account the repeated measures structure of the data. Age group specific growth rates were compared both within and between the gender groups.
Inter-observer and intra-observer reliability were evaluated using intraclass correlation coefficients (ICC), a test for concordance or agreement for continuous data. Measurements greater than 0.75 are considered to represent excellent agreement.18, 19 Paired t-tests were used to determine whether systematic bias existed. Limits of agreement were computed to estimate the amount of variation that might be expected from one reader to the next. Data were managed in Microsoft Excel and Microsoft Access (Microsoft Corporation, Redmond, WA). Statistical analyses were conducted in SPSS v 15.0 (SPSS Inc., Chicago, IL).
RESULTS
Nine hundred sixty-one individuals were included in this study. Several individuals were measured more than once at different ages: 850 were measured once, 94 measured twice, 12 measured three times, 3 measured four times, and 2 measured five times. Both right and left clavicle of each subject was measured, resulting in 2,192 measurements, with 1,078 being female and 1,114 male. The rate of change of clavicle length over time is shown graphically in Figure 3 and anatomically in Figure 4.
Figure 3.
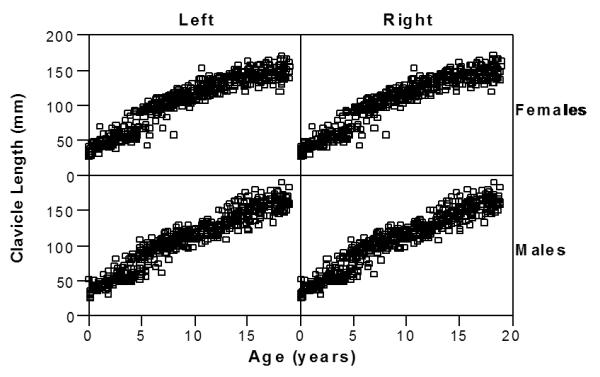
Clavicle Length for females and males (rows) for both left and right clavicles (columns).
Figure 4.

Comparing growth of the clavicle in females and males from <1 to 18 years of age.
The mean ± SD clavicle length at age eighteen, genders combined was 155.2 ± 12.9mm (range, 119.45 to 190.44mm). When examining the genders separately the mean clavicle length at age eighteen was 161.3 ± 10.8mm (range, 145.75 to 190.44mm) for males and 149.2 ± 12.3mm (range, 119.45 to 171.52mm) for females. The difference between the left and right clavicles was statistically significant (p=0.049) due to the large sample size. However, as shown in Table 2 the difference was not clinically significant with a mean difference of 0.036mm (CI95 0.00 to 0.07mm).
Table 2.
Mean, standard deviation, and range of clavicle lengths (mm) separated by side, age and gender.
| Age (years) | Female | Male | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Left Clavicle | Right Clavicle | Left Clavicle | Right Clavicle | |||||||||||||||||
| N | Mean | SD | Min | Max | N | Mean | SD | Min | Max | N | Mean | SD | Min | Max | N | Mean | SD | Min | Max | |
| 0 | 27 | 37.8 | (6.5) | 26.9 | 48.4 | 27 | 37.8 | (6.3) | 27.1 | 48.2 | 26 | 37.6 | (7.6) | 25.3 | 52.3 | 26 | 37.6 | (7.6) | 25.1 | 52.4 |
| 1 | 27 | 48.0 | (6.7) | 39.7 | 69.8 | 27 | 48.1 | (6.6) | 39.8 | 69.8 | 33 | 44.8 | (7.3) | 30.8 | 63.6 | 33 | 44.9 | (7.3) | 30.6 | 64.0 |
| 2 | 30 | 53.9 | (7.9) | 39.3 | 72.1 | 30 | 53.9 | (7.9) | 39.1 | 72.0 | 26 | 55.5 | (8.3) | 43.5 | 80.7 | 26 | 55.5 | (8.3) | 43.1 | 80.7 |
| 3 | 29 | 58.8 | (10.9) | 46.4 | 89.0 | 29 | 58.8 | (10.9) | 47.0 | 89.1 | 31 | 57.9 | (11.2) | 47.1 | 85.3 | 31 | 58.0 | (11.3) | 47.2 | 85.3 |
| 4 | 29 | 67.2 | (15.0) | 46.5 | 93.8 | 29 | 67.3 | (15.1) | 46.4 | 94.3 | 33 | 69.6 | (15.9) | 47.5 | 108.6 | 33 | 69.4 | (15.8) | 47.2 | 108.6 |
| 5 | 26 | 86.0 | (15.7) | 43.0 | 106.3 | 26 | 86.1 | (16.0) | 42.0 | 106.9 | 30 | 85.8 | (12.3) | 55.3 | 104.4 | 30 | 85.7 | (12.3) | 55.3 | 104.5 |
| 6 | 32 | 98.7 | (9.8) | 67.4 | 111.7 | 32 | 98.7 | (9.9) | 67.1 | 111.0 | 32 | 96.4 | (11.3) | 59.2 | 111.3 | 32 | 96.4 | (11.1) | 60.3 | 111.3 |
| 7 | 30 | 102.8 | (7.5) | 82.5 | 115.6 | 30 | 102.7 | (7.5) | 82.9 | 115.6 | 34 | 103.1 | (8.9) | 79.1 | 120.7 | 34 | 102.9 | (8.9) | 79.2 | 120.2 |
| 8 | 31 | 110.7 | (12.1) | 58.0 | 124.1 | 31 | 110.6 | (12.1) | 57.8 | 124.1 | 32 | 110.8 | (8.7) | 93.5 | 129.2 | 32 | 110.7 | (8.8) | 92.9 | 129.3 |
| 9 | 31 | 113.8 | (7.8) | 96.6 | 130.6 | 31 | 113.8 | (7.8) | 96.7 | 130.9 | 36 | 112.8 | (8.6) | 95.9 | 129.0 | 36 | 112.4 | (8.3) | 95.9 | 129.3 |
| 10 | 27 | 122.8 | (10.4) | 106.7 | 153.1 | 27 | 122.8 | (10.4) | 107.0 | 153.4 | 28 | 120.0 | (8.2) | 103.1 | 135.4 | 28 | 119.9 | (8.1) | 103.7 | 135.1 |
| 11 | 27 | 125.2 | (8.9) | 106.3 | 143.5 | 27 | 125.2 | (8.8) | 107.0 | 143.6 | 25 | 123.4 | (8.8) | 105.5 | 137.9 | 25 | 123.3 | (8.8) | 105.2 | 137.8 |
| 12 | 25 | 130.4 | (8.1) | 114.6 | 143.5 | 25 | 130.4 | (8.0) | 114.9 | 143.0 | 27 | 127.4 | (10.4) | 107.8 | 151.1 | 27 | 127.3 | (10.3) | 108.4 | 150.7 |
| 13 | 26 | 139.3 | (8.3) | 119.8 | 150.3 | 26 | 139.3 | (8.4) | 119.8 | 151.4 | 26 | 141.2 | (10.8) | 124.0 | 164.2 | 26 | 141.3 | (11.1) | 123.9 | 164.1 |
| 14 | 27 | 139.4 | (9.4) | 119.2 | 162.2 | 27 | 139.4 | (9.6) | 120.1 | 162.8 | 29 | 145.2 | (12.9) | 121.1 | 175.7 | 29 | 145.2 | (12.9) | 121.3 | 175.3 |
| 15 | 29 | 143.4 | (6.9) | 129.8 | 157.6 | 29 | 143.3 | (7.0) | 129.2 | 157.9 | 28 | 150.5 | (13.5) | 121.1 | 179.7 | 28 | 150.6 | (13.5) | 121.5 | 179.8 |
| 16 | 27 | 143.6 | (10.5) | 123.7 | 164.1 | 27 | 143.7 | (10.7) | 123.7 | 164.2 | 29 | 155.1 | (10.6) | 129.3 | 176.6 | 29 | 155.1 | (10.6) | 129.0 | 176.1 |
| 17 | 29 | 145.6 | (8.7) | 130.0 | 162.7 | 29 | 145.5 | (8.9) | 129.1 | 162.3 | 26 | 161.0 | (11.7) | 132.8 | 179.7 | 26 | 161.0 | (11.8) | 132.7 | 179.3 |
| 18 | 30 | 149.2 | (12.4) | 119.5 | 171.5 | 30 | 149.1 | (12.2) | 120.2 | 171.1 | 26 | 161.2 | (10.7) | 145.4 | 190.4 | 26 | 161.4 | (10.9) | 145.8 | 190.8 |
The rate of growth was similar between the genders from birth through age twelve (p = 0.601). The growth rate averaged 8.4mm per year for males and females. Above age twelve, the growth rate was lower for females than males averaging 5.4mm per year for males and 2.6mm per year for females. This effect of gender on growth rate was statistically significant (p<0.000). The models are displayed in Figure 5.
Figure 5.

Clavicle lengths (mm) for males and females estimated from the linear mixed model.
Table 3 demonstrates that mean clavicle lengths at age eighteen in this study are comparable to other published studies that measured clavicle lengths in the adult population.14, 20-23 Multiple clavicle measurement validation studies have determined posteroanterior (PA) thorax radiographs, the radiograph type most commonly measured in this study, have the highest agreement with their control, computed tomography (CT) scan measurements and insignificant intra or inter-observer variations.20, 24 Smekal et al did point out the small distance between the clavicles and the x-ray film allowed for minor amplification effects and errors due to rotation and posture.20
TABLE 3.
Variabilities in measurement determined in present and past studies demonstrated by clavicle length (mm) means and standard deviations.
| Mean Clavicle Length (mm) | |||||
|---|---|---|---|---|---|
| Sample Size |
Study Location/ Specimen Source |
Genders Combined |
Female | Male | |
| Present Study | |||||
| Radiographs | 1096 | Cincinnati, OH, USA | 154.79 ± 12.98 | 149.16 ± 12.2 | 161.29 ± 10.69 |
| Previous Studies | |||||
| Smekal et al. | |||||
| Thorax PA Radiographs | 30 | Innsbruck, Austria | 169.7 ± 12.3 | N/A | N/A |
| Lazarides & Zafriopoulos | |||||
| PA Radiographs | 132 | Merthyr Tidfil, Wales | N/A | 140.3 ± 25.5 | 190.5 ± 34.5 |
| Rios et al. | |||||
| Fresh Anatomic Cadaver | 19 | Farmington, CT, USA | 147 ± 14 | N/A | N/A |
| Rios et al. | |||||
| Dry Osteology Cadaver | 60 | Cleveland Museum of Natural History, Cleveland, OH, USA |
149 ± 9.1 | 136 ± 8.5 | 152 ± 6.1 |
| Huang et al. | |||||
| Cadaver | 100 | Cleveland Museum of Natural History, Cleveland, OH, USA |
145 ± 12.7 | 137.3 ± 10.2 | 152.6 ± 10.2 |
| McCormick et al. | |||||
| Cadaver | 724 | North American autopsy population |
N/A | (R) 140 ± 7.9 (L) 141 ± 7.7 |
(R) 157 ± 9.5 (L) 159 ± 9.1 |
Inter-observer reliability statistics are shown in Table 4. Observer 1 tended to measure a little shorter (<2mm) than Observer 2 and 3, while Observer 2 tended to measure a little longer (about 1 mm) than Observer 3. Although the differences were statistically significant the correlations were very high suggesting all observers rated the same cases relatively high and relatively low. Limits of agreement suggest expected differences between repeated measures by different observers are unlikely to exceed ± 8 or 9 mm. Pearson’s correlation coefficients for intra-rater reliability were very high (R2>0.99), as displayed in Table 5. Thus, both our inter-rater and intra-rater reliability measurements were in the excellent range according to the intraclass correlation coefficient (ICC) criteria of Fleiss, as referenced in Table 6.18
Table 4.
Inter-observer Reliability
| Mean difference (mm) |
Std. Deviation of the difference |
Lower limit of agreement |
Upper limit of agreement |
95% Confidence Interval of the Difference |
−value for paired samples t- test |
Pearsons correlation coefficient |
p-value for correlation |
|||
|---|---|---|---|---|---|---|---|---|---|---|
| Right clavicle |
Observer 1 v observer 2, n=31 | −1.5 | 2.7 | −6.8 | 3.7 | −2.5 | −0.6 | 0.0032 | 0.997 | <0.0001 |
| Observer 1 v observer 3, n=50 | −1.7 | 3.6 | −8.7 | 5.3 | −2.7 | −0.7 | 0.0016 | 0.996 | <0.0001 | |
| Observer 3 v observer 2, n=30 | −1.1 | 3.1 | −7.1 | 5.0 | −2.2 | 0.1 | 0.0713 | 0.996 | <0.0001 | |
| Left clavicle |
Observer 1 v observer 2, n=31 | −2.4 | 2.8 | −7.8 | 3.1 | −3.4 | −1.3 | 0.0000 | 0.997 | <0.0001 |
| Observer 1 v observer 3, n=50 | −2.0 | 2.4 | −6.8 | 2.8 | −2.7 | −1.3 | 0.0000 | 0.998 | <0.0001 | |
| Observer 3 v observer 2, n=30 | 0.2 | 2.9 | −5.4 | 5.8 | −0.9 | 1.3 | 0.7062 | 0.996 | <0.0001 | |
Table 5.
Intra-observer Reliability
| Mean difference (mm) |
Std. Deviation of the difference |
Lower limit of agreement |
Upper limit of agreement |
95% Confidence Interval of the Difference |
−value for paired samples t- test |
Pearsons correlation coefficient |
p-value for correlation |
|||
|---|---|---|---|---|---|---|---|---|---|---|
| Right clavicle |
Observer 1 v observer 2, n=31 | 0.0 | 0.6 | −1.1 | 1.1 | −0.2 | 0.2 | 0.8014 | 1.000 | <0.0001 |
| Observer 1 v observer 3, n=50 | −0.4 | 1.4 | −3.1 | 2.3 | −0.9 | 0.1 | 0.1452 | 0.999 | <0.0001 | |
| Observer 3 v observer 2, n=30 | −0.4 | 1.2 | −2.8 | 2.0 | −0.8 | 0.1 | 0.0848 | 0.999 | <0.0001 | |
| Left clavicle |
Observer 1 v observer 2, n=31 | −0.1 | 0.6 | −1.2 | 1.0 | −0.3 | 0.1 | 0.4172 | 1.000 | <0.0001 |
| Observer 1 v observer 3, n=50 | −0.3 | 1.3 | −2.9 | 2.2 | −0.8 | 0.1 | 0.1645 | 0.999 | <0.0001 | |
| Observer 3 v observer 2, n=30 | −0.3 | 1.1 | −2.5 | 1.9 | −0.7 | 0.1 | 0.1885 | 1.000 | <0.0001 | |
Table 6.
Fleiss Criteria
| R | Reliability |
|---|---|
| >0.75 | Excellent |
| 0.4 – 0.75 | Fair to Good |
| <0.4 | Poor |
R = correlation coefficient
DISCUSSION
The clavicle has the honor of being the first bone to start the ossification process and the last to finish it.8, 25-27 It has also been described as the most frequently injured bone in children less than 10 years of age.26 Overall clavicle fractures account for 10-15% of all fractures in children.1 Since the clavicle contributes significantly to the proper motion and function of the upper extremity, appropriate fracture healing is essential.3 Our cross-sectional study has established that relatively little longitudinal growth remains for girls beyond nine years of age and for boys beyond 12 years of age. It is interesting to contrast the findings from our study with those related to thoracic growth. Whereas a 10 year old child has achieved only 55% of their three-dimensional thoracic growth, a similarly aged child has completed 80% of their clavicle growth.28
Until recently, conservative treatment for clavicle fractures has been accepted as the standard of care for all ages without complete knowledge of the clavicle’s longitudinal growth over time. In 1955 Walter Putnam Blount stated: “The prognosis is uniformly good. The bump of callus and alarming deformity frequently seen in the roentgenogram will be obliterated by the molding incident to further growth. There is no justification for open reduction.”5 Over a decade later Rowe et al. offered similar sentiments, “Fortunately for children, the clavicle heals rapidly and remodels so completely that very little treatment is needed other than instruction to parents to lift the child by the waist rather than by the arms or the shoulders.”29 These and similar statements were made without specific knowledge of postnatal growth of the clavicle.
Our findings show an almost identical pattern of growth between the genders until puberty. After age twelve we found a statistically significant change in clavicle growth between the two genders. On average, males, between the ages of thirteen and eighteen, achieved twice as much clavicle length as females (20.02mm vs. 9.87mm), whereas the female subjects in our sample reached the 80% milestone of clavicle length almost three years prior to males. Although factors affecting growth of the physes are not completely understood, a likely contributing factor is the hormonal differences present at puberty. Androgens tend to augment skeletal growth while estrogen’s role is principally one of inhibition.30
Kubiak et al. documented their results of surgical treatment of clavicle fractures in older children.1 In their study, the median age for surgical treatment was 13.1 years with a range from 9.3 to 15.6 years. Ogden also hinted at the difference between younger children and adolescents when he stated, “In adolescents, anatomic realignment assumes more importance, since remodeling is less active and may not correct major malalignment,” although no specific age cut-off was defined.31 Our findings agree with Lazarides et al. that the right and left clavicles are similar in length in normal individuals, with the mean difference observed in this study of 0.036mm.14 This permits the uninjured clavicle to serve as a control in determining the amount of shortening caused by a fracture.
Our findings must be interpreted within the context of the study design. One limitation is that our data collection terminated at age eighteen. Ideally we would have continued to measure clavicle length until the closure of the secondary ossification center, noted in the literature to be between the ages of 24-26,17 although individual’s receiving chest radiographs at our children’s hospital beyond age eighteen regularly fell into our exclusion criteria due to a medical or musculoskeletal condition. While including ages 19-25 would make the results more complete, they would not make our representation of clavicle growth over time more compelling. Our large sample size and comparability to other published studies that have measured clavicle lengths in subjects aged 18 and beyond support the validity of our findings.
Possible variations between the different races were not examined in this study due to lack of complete demographic data. A previous cohort study of 503 patients at this medical center noted a racial distribution of 83% Caucasian and 17% African-American.32 Rios et al. also noted no significant difference in clavicle measurements when samples were compared according to race in a dry osteology study.21
Our study results question the remodeling capability of the clavicle to re-establish normal growth and length beyond the years mentioned for each gender when the majority of its length has been obtained. Figures 6A and 6B demonstrate a fourteen year old male who did not regain any of his initial 20mm clavicle shortening at one year follow-up after a displaced clavicle fracture. Now that the normal growth of the clavicle has been established, future age-related indications for clavicle fracture treatment by open reduction-internal fixation may be based more upon the percentage of clavicle length shortening. Further research should delineate the age-related ability of the child’s clavicle to heal and remodel, as well as the potential that a shortened clavicle secondary to fracture is able to re-establish length. Special consideration should be focused on the ages our study identified as growth milestones for the clavicle.
Figure 6-A.

Serial radiographs of a 14-year-old male who sustained a completely displaced clavicle fracture. Injury radiograph illustrating initial 20mm shortening.
Figure 6-B.

Serial radiographs of a 14-year-old male who sustained a completely displaced clavicle fracture. One year follow-up radiograph of now 15-year old male still demonstrates 20mm shortening of the injured clavicle.
Acknowledgments
This research was supported in part by the University of Cincinnati Orthopaedic Research and Education Fund and the division of Pediatric Orthopaedic Surgery at Cincinnati Children’s Hospital Medical Center. Support for statistical analysis was provided in part through the Institutional Clinical and Translational Science Award, NIH/NCRR Grant Number UL1RR026314, awarded to Cincinnati Children’s Hospital Medical Center.
Contributor Information
Molly A McGraw, Medical Student, Ohio University College of Osteopathic Medicine Musculoskeletal Outcomes Research Fellow Division of Pediatric Orthopaedic Surgery Cincinnati Children’s Hospital Medical Center 8750 Arborcrest Drive, Cincinnati, Ohio 45236 (513) 253-6517 mm118207@ohio.edu.
Charles T Mehlman, Professor Pediatric Orthopaedic Surgery Director Musculoskeletal Outcomes Research Division of Pediatric Orthopaedic Surgery Cincinnati Children’s Hospital Medical Center 3333 Burnet Avenue, ML 2017, Cincinnati, Ohio 45229-3039.
Christopher J. Lindsell, Associate Professor Department of Emergency Medicine University of Cincinnati College of Medicine 231 Albert Sabin way, Cincinnati, Ohio 45267 Office: (513) 558-6937 Fax: (513) 558-5791 Christopher.Lindsell@uc.edu.
Cassie L. Kirby, Clinical Research Coordinator III Division of Pediatric Orthopaedic Surgery Cincinnati Children’s Hospital Medical Center 3333 Burnet Avenue, ML 2017, Cincinnati, Ohio 45229-3039 Office: (513) 803-6133 Fax: (513) 636-3928 Cassie.Kirby@cchmc.org.
REFERENCES
- 1.Kubiak R, Slongo T. Operative treatment of clavicle fractures in children: a review of 21 years. J Pediatr Orthop. 2002;22:736–739. [PubMed] [Google Scholar]
- 2.Curtis RJ. Operative management of children’s fractures of the shoulder region. Orthop Clin North Am. 1990;21:315–324. [PubMed] [Google Scholar]
- 3.Sarwark JF, King EC, Luhmann SJ. Proximal humerus scapula and clavicle. Chapter 17. In: Beaty JH, Kasser JR, editors. Rockwood & Wilkins Fractures in Children. 6th edition Lippincott Williams & Wilkins; Philadelphia: 2006. pp. 727–729. [Google Scholar]
- 4.Mooney JF. Shoulder Upper Arm and Elbow Trauma: Pediatrics. Chapter 54. In: Fischgrund JS, editor. Orthopaedic Knowledge Update 9. American Academy of Orthopaedic Surgeons; Rosemont, Illinois: 2008. p. 660. [Google Scholar]
- 5.Blount WP. Fractures in Children. Williams & Wilkins; Baltimore: 1955. Injuries of the shoulder region. Chapter 2; pp. 9–11. [Google Scholar]
- 6.Pring M, Wenger DR. Clavicle. Chapter 6. In: Rang M, Wenger DR, Pring ME, editors. Rang’s Children’s Fractures. 3rd edition Lippincott Williams & Wilkins; Philadelphia: 2005. pp. 79–83. [Google Scholar]
- 7.Waters PM. Injuries of the shoulder elbow and forearm. Chapter 24. In: Abel MF, editor. Orthopaedic Knowledge Update Pediatrics 3. American Academy of Orthopaedic Surgeons; Rosemont, Illinois: 2006. p. 303. [Google Scholar]
- 8.Gardner E. The embryology of the clavicle. Clin Orthop. 1968;58:9–16. [PubMed] [Google Scholar]
- 9.Dimeglio A. Growth of the spine before age 5 years. J Pediatr Orthop (Part B) 1993;1:102–107. [Google Scholar]
- 10.Shapiro F. Epiphyseal disorders. N Engl J Med. 1987;317:1702–1710. doi: 10.1056/NEJM198712313172705. [DOI] [PubMed] [Google Scholar]
- 11.Pritchett JW. Growth and predictions of growth in the upper extremity. J Bone Joint Surg-AM. 1988;70-A:520–525. [PubMed] [Google Scholar]
- 12.Pritchett JW. Growth plate activity in the upper extremity. Clin Orthop Rel Res. 1991;268:235–242. [PubMed] [Google Scholar]
- 13.Anderson M, Green WT, Messner MB. Growth and prediction of growth in the lower extremities. J Bone Joint Surg-AM. 1963;45-A:1–14. [PubMed] [Google Scholar]
- 14.Lazarides S, Zafiropoulos G. Conservative treatment of fractures at the middle third of the clavicle: The relevance of shortening and clinical outcome. J Shoulder Elbow Surg. 2006;15(2):191–194. doi: 10.1016/j.jse.2005.08.007. [DOI] [PubMed] [Google Scholar]
- 15.Staheli LT, Chew DE, Corbett M. The Longitudinal Arch. J Bone Joint Surg. 1987;69A(3):426–428. [PubMed] [Google Scholar]
- 16.Staheli LT, Corbett M, Wyss C, King H. Lower-Extremity Rotational Problems in Children. J Bone Joint Surg. 1985;67A(1):39–47. [PubMed] [Google Scholar]
- 17.Jit I, Kulkarni M. Times of Appearance and Fusion of Epiphysis at the Medial End of the Clavicle. Indian J Med Res. 1976;64(5):773–782. [PubMed] [Google Scholar]; Neer CS. Nonunion of the clavicle. JAMA. 1960;172(10):1006–11. doi: 10.1001/jama.1960.03020100014003. [DOI] [PubMed] [Google Scholar]
- 18.Fleis JL. The Design and Analysis of Clinical Experiments. Wiley Interscience; New York: 1986. pp. 1–31. [Google Scholar]
- 19.Feinstein AR. Principles of Medical Statistics. Chapman & Hall/CRC; 2002. pp. 430–431. [Google Scholar]
- 20.Smekal V, Deml C, Irenberger A, Niederwanger C, Lutz M, Blauth M, Krappinger K. Length Determination in Midshaft Clavicle Fractures: Validation of Measurement. J Orthop Trauma. 2008;22(7):458–462. doi: 10.1097/BOT.0b013e318178d97d. [DOI] [PubMed] [Google Scholar]
- 21.Rios CG, Arciero RB, Mazzocca AD. Anatomy of the clavicle and coracoid process for reconstruction of the coracoclavicular ligaments. Amer J Sports Med. 2007;35(5):811–817. doi: 10.1177/0363546506297536. [DOI] [PubMed] [Google Scholar]
- 22.Huang JI, Toogood P, Chen MR, Wilber JH, Cooperman DR. Clavicular Anatomy and the Applicability of Precontoured Plates. J Bone Joint Surg Am. 2007;89(10):2260–5. doi: 10.2106/JBJS.G.00111. [DOI] [PubMed] [Google Scholar]
- 23.McCormick WF, Stewart JH, Greene H. Sexing of Human Clavicles Using Length and Circumference Measurements. Am J Forensic Med Pathol. 1991;12(2):176–181. doi: 10.1097/00000433-199106000-00017. [DOI] [PubMed] [Google Scholar]; Ogden JA, Conlogue GJ, Bronson ML. Radiology of postnatal skeletal development. Skel Radiol. 1979;4:196–203. doi: 10.1007/BF00347213. [DOI] [PubMed] [Google Scholar]
- 24.Bhattacharya R, Lazarides S, Finn P, Campbell R, Rangan A. Clavicular length measurement following trauma. Injury Extra. 2004;35(2):22. [Google Scholar]
- 25.Neer CS. Nonunion of the clavicle. JAMA. 1960;172(10):1006–11. doi: 10.1001/jama.1960.03020100014003. [DOI] [PubMed] [Google Scholar]
- 26.Ogden JA, Conlogue GJ, Bronson ML. Radiology of postnatal skeletal development. Skel Radiol. 1979;4:196–203. doi: 10.1007/BF00347213. [DOI] [PubMed] [Google Scholar]
- 27.Mehlman CT. Injuries to the lateral end of the clavicle and AC joint: a pediatric perspective. J Am Osteo Acad Orthop. 1996;33:82–83. 90. [Google Scholar]
- 28.Charles YP, Dimeglio A, Marcoul M, Bourgin JF, Marcoul A, Bozonnat MC. Influence of Idiopathic Scoliosis on Three-Dimensional Thoracic Growth. Spine. 2008;33(11):1209–1218. doi: 10.1097/BRS.0b013e3181715272. [DOI] [PubMed] [Google Scholar]
- 29.Rowe CR. An Atlas of Anatomy and Treatment of Midclavicular Fractures. Clin. Orthop. 1968;58:29–42. [PubMed] [Google Scholar]
- 30.Trippel SB. Bone Formation and Repair. American Academy of Orthopaedic Surgeons; 1994. Biologic Regulation of Bone Growth. Chapter 4; p. 45. [Google Scholar]
- 31.Ogden JA. Skeletal Injury in the Child. Lea & Febiger; Philadelphia: 1982. Chest and Pectoral Girdle. Chapter 2 & 9; pp. 16–17.pp. 202–203. [Google Scholar]
- 32.VanderBeek BL, Mehlman CT, Foad SL, Wall EJ, Crawford AH. The Use of Conscious Sedation for Pain Control During Forearm Fracture Reduction in Children. Does Race Matter? J Pediatr Orthop. 2006;26(1):53–57. doi: 10.1097/01.bpo.0000187993.17387.09. [DOI] [PubMed] [Google Scholar]