

Abstract
Target population
This recommendation applies to adults with newly diagnosed brain metastases; however, the recommendation below does not apply to the exquisitely chemosensitive tumors, such as germinomas metastatic to the brain.
Recommendation
Should patients with brain metastases receive chemotherapy in addition to whole brain radiotherapy (WBRT)?
Level 1 Routine use of chemotherapy following WBRT for brain metastases has not been shown to increase survival and is not recommended. Four class I studies examined the role of carboplatin, chloroethylnitrosoureas, tegafur and temozolomide, and all resulted in no survival benefit. Two caveats are provided in order to allow the treating physician to individualize decision-making: First, the majority of the data are limited to non small cell lung (NSCLC) and breast cancer; therefore, in other tumor histologies, the possibility of clinical benefit cannot be absolutely ruled out. Second, the addition of chemotherapy to WBRT improved response rates in some, but not all trials; response rate was not the primary endpoint in most of these trials and end-point assessment was non-centralized, non-blinded, and post-hoc. Enrollment in chemotherapy-related clinical trials is encouraged.
Keywords: Brain metastases, Chemotherapy, Whole brain radiation therapy, Targeted agents, Systematic review, Practice guideline
Rationale
Brain metastases are a common complication of systemic cancer, occurring in 20–40% of patients [1]. The primary therapeutic approach for disseminated systemic disease remains chemotherapy, and therefore, one might expect this to be a logical choice for brain metastases as well. However, several issues have limited the application of chemotherapy in this context. One concern involves the ability of chemotherapeutic agents to cross the blood–brain barrier (BBB). Many chemotherapeutic agents are relatively excluded from the brain, and ones that do penetrate, may do so in insufficient concentrations. Although there is relative breakdown of the BBB in and around a metastatic lesion in the brain, some studies have demonstrated that there is still only very limited drug concentration within the lesion. Recent findings suggest that efflux pumps may play a major role in this phenomenon [2]. Some animal studies have shown that if metastatic tumors enhance strongly on computed tomography (CT) or magnetic resonance imaging (MRI), that the blood–brain barrier (BBB) is sufficiently impaired to allow entry of chemotherapeutic drugs. Newer agents which cross the BBB have and are being developed as well. New molecular based therapies directed against growth factor receptors and other protein kinases are being investigated, however their large size also raises concerns about penetrability. There is also the long-standing observation that intracranial response rates to chemotherapy are typically lower than in the extracranial compartment, and a common hypothesis for this finding is that patients are pre-exposed to cytotoxic therapies, and it is the chemoresistant clones that metastasize to the brain. However, data in newly diagnosed, previously untreated patients with small cell lung cancer (SCLC) suggest that intracranial response rates remain significantly lower than extracranial response rates, thereby suggesting that chemoresistant clones alone do not necessarily explain this dichotomy [3]. Some types of metastatic brain tumors may respond to chemotherapy to some degree, including breast cancer, germ cell cancer, and ovarian cancer in addition to SCLC.
The use of chemotherapy for brain metastases has been explored in four primary contexts:
WBRT vs. WBRT plus chemotherapy
Chemotherapy vs. chemotherapy plus WBRT
Chemotherapy plus concurrent WBRT vs. chemotherapy plus delayed WBRT
Chemotherapy first, followed by WBRT vs. WBRT first, followed by chemotherapy
Methods
To answer the above question and its subparts, a comprehensive systematic literature review was performed.
Search strategy
The following electronic databases were searched from 1990 to September 2008: MEDLINE®, Embase®, Cochrane Database of Systematic Reviews, Cochrane Controlled Trials Registry, and Cochrane Database of Abstracts of Reviews of Effects. A broad search strategy using a combination of subheadings and text words was employed. The search strategy is documented in the methodology paper for this guideline series by Robinson et al. [4] Reference lists of included studies were also reviewed.
For inclusion in this analysis, the following criteria had to be met:
Published in English with a publication date of 1990 forward.
Patients with newly diagnosed brain metastases.
Fully published peer-reviewed primary comparative studies (all comparative study designs for primary data collection included; e.g., RCT, non-randomized trials, cohort studies or case–control studies).
Any comparative studies evaluating chemotherapy alone or in combination with other treatment modalities for the treatment of newly diagnosed brain metastases.
Number of study participants with newly diagnosed brain metastases ≥5 per study arm for at least two of the study arms.
Baseline information on study participants is provided by treatment group in studies evaluating interventions exclusively in patients with newly diagnosed brain metastases. For studies with mixed populations (i.e., includes participants with conditions other than newly diagnosed brain metastases), baseline information is provided for the intervention sub-groups of participants with newly diagnosed brain metastases.
Study selection and quality assessment
Two independent reviewers evaluated citations using a priori criteria for relevance and documented decisions in standardized forms. Cases of disagreement were resolved by a third reviewer. The same methodology was used for full text screening of potentially relevant papers. Studies which met the eligibility criteria were data extracted by one reviewer and the extracted information was checked by a second reviewer. The PEDro scale [5, 6] was used to rate the quality of randomized trials. The quality of comparative studies using non-randomized designs was evaluated using eight items selected and modified from existing scales.
Evidence classification and recommendation levels
Both the quality of the evidence and the strength of the recommendations were graded according to the American Association of Neurological Surgeons (AANS)/Congress of Neurological Surgeons (CNS) criteria. These criteria are provided in the methodology paper for this guideline series.
Guideline development process
The AANS/CNS convened a multi-disciplinary panel of clinical experts to develop a series of practice guidelines on the management of brain metastases based on a systematic review of the literature conducted in collaboration with methodologists at the McMaster University Evidence-based Practice Center.
Scientific foundation
The literature search resulted in the identification of 16,966 citations of which 16,936 were eliminated at abstract review as not having relevance to the specific question. The remaining 30 studies were subject to full text screening, and 20 were excluded, seven because they lacked baseline patient data by treatment group, 10 because they lacked baseline patient subset data by treatment group, two because there was no treatment comparison of interest, and one because it was not a comparative study. Ten eligible studies [7–16] were therefore fully reviewed and form the basis of this report (see Table 1; Fig. 1).
Table 1.
Summary of primary studies
| First author (year) | Study design evidence class | Interventions | Population | Median survival | Tumor response | Median time to recurrence/progression |
|---|---|---|---|---|---|---|
| WBRT vs. WBRT + chemotherapy | ||||||
| Guerrieri (2004) [7] |
RCT Evidence class I |
G1: WBRT (n = 21) G2: WBRT + Carboplatin (n = 21) |
Pts with BM from NSCLC |
G1: 4.4 months G2: 3.7 months (survival curves: log-rank; P = NS) |
Response in brain: (Of evaluable pts) G1: OR 10% (of 11 pts assessed) G2: OR 29% (of 16 pts assessed) (P = NS) |
NR |
| Ushio (1991) [8] |
RCT Evidence class I |
G1: WBRT (n = 25) G2: WBRT + Chloroethylnitrosoureas (n = 34) G3: WBRT + Chloroethylnirosoureas + Tegafur (n = 29) |
Pts with BM from lung cancer |
G1: 27 weeks G2: 29 weeks G3: 30.5 weeks (survival curves: Wilcoxon; P = NS) |
Response rate in brain: (Of evaluable pts) G1: OR 36% (CR 4/14, PR 1/14) G2: OR 69% (CR 11/16, PR 0/16) G3: OR 74% (CR 12/19, PR 2/19) G1 vs. G2 (P = NS) G2 vs. G3 (P = NS) G1 vs. G3 (P < 0.05) |
NR |
| Antonadou (2002) [9] |
Randomized phase II trial Evidence class I |
G1: WBRT (n = 23) G2: WBRT + TMZ (n = 25) |
Pts with BM from lung, breast or unknown primary |
G1: 7.0 months G2: 8.6 months (survival curves: log-rank; P = NS) |
Response rate in brain: (Of evaluable pts) G1: OR 67% (CR 7/21, PR 7/21) G2: OR 96% (CR 9/24, PR 14/24) (P = 0.017) |
NR |
| Verger (2003) [10] |
Randomized phase II trial Evidence class I |
G1: WBRT (n = 41) G2: WBRT + TMZ (n = 41) |
Pts with BM |
G1: 3.1 months G2: 4.5 months (survival curves: log-rank; P = NS) |
Response in brain at 30 days: (by ITT) G1: OR 32% (CR 2/41, PR 11/41) G2: OR 32% (CR 2/41, PR 11/41) (P = NS) Response in brain at 90 days: G1: OR 2/41 (CR 0/41, PR 2/41) G2: OR 7/41 (CR 1/41, PR 6/41) (P = NS) |
Median: not reported % BM progression-free at 90 days: G1: 54% G2: 72% (P = 0.03) |
| Kim (2005) [11] |
Retrospective cohort study Evidence class II |
G1: WBRT (n = 32) G2: WBRT + platinum-based chemotherapy (n = 31) |
Pts with BM at diagnosis of NSCLC |
G1: 19.0 weeks G2: 58.1 weeks (survival curves: test not specified: P < 0.001) |
No comparison between groups | No comparison between groups |
| Chemotherapy vs. chemotherapy + WBRT | ||||||
| Mornex (2003) [12] |
RCT Evidence class I |
G1: Fotemustine (n = 39) G2: Fotemustine + WBRT (n = 37) |
Pts with BM from melanoma |
G1: 86 days G2: 105 days (survival curves: log-rank; P = NS) |
Response rate in brain at day 50 (by ITT) G1: OR 5.1% (CR 0/39, PR 2/39) G2: OR 8.1% (CR 0/37, PR 3/37) (P = NS) |
Median time to progression in brain: G1: 49 days G2: 80 days (BM progression-free curves; Wilcoxon: P = 0.03; log-rank: P = 0.069) |
| Postmus (2000) [13] |
RCT Evidence class I |
G1: Teniposide (n = 60) G2: Teniposide + WBRT (n = 60) |
Pts with BM from SCLC |
G1: 3.2 months G2: 3.5 months (survival curves: log-rank; P = NS) |
Response rate in brain: (by ITT) G1: OR 22% (CR 5/60, PR 8/60) G2: OR 57% (CR 18/60, PR 16/60) (P < 0.001) Response rate outside the brain: G1: OR 20% (CR 3/60, PR 9/60) G2: OR 33% (CR 6/60, PR 14/60) (P = NS) |
Median time to progression in brain: NR Significant difference in favor of G2 (BM progression-free curves: log-rank; P = 0.005) |
| Moscetti (2006) [14] |
Retrospective cohort study Evidence class II |
G1: Platinum-based chemotherapy (n = 110) G2: WBRT + chemotherapy (n = 46) |
Pts with BM at diagnosis of NSCLC |
G1: 10 months G2: 14 months (survival curves: test not specified; P = 0.07; NS) |
Response rate in brain: (OR by ITT) G1: OR 27.3% (CR 15/107, PR 15/107) G2: OR 34.8% (CR 2/46, PR 14/46) (P = NS) Extra-cranial response rate: G1: OR 34.5% (CR 0/107, PR 38/107) G2: OR 41.3% (CR 0/46, PR 19/46) (P = NS) |
Median progression-free survival: G1: 6 months G2: 6 months (Progression-free curves: test not specified; P = NS) |
| Chemotherapy + concurrent WBRT vs. chemotherapy + delayed WBRT | ||||||
| Robinet (1998) [15] |
RCT Evidence class I |
G1: Cisplatin + vinorelbine + delayed WBRT (n = 86) G2: Cisplatin + vinorelbine + concurrent WBRT (n = 85) |
Pts with BM from NSCLC |
G1: 24 weeks G2: 21 weeks (survival curves: log-rank; P = NS) |
Response rate in brain: (by ITT) G1: OR 27% (CR 1/76, PR 22/76) G2: OR 33% (CR 7/73, PR 21/73) (P = NS) Extra-cranial rate response: G1: OR 35% (CR 2/76, PR 28/76) G2: OR 25% (CR 2/73, PR 19/73) (P = NS) |
Median time to progression in brain: G1: 13 weeks G2: 11 weeks (BM progression-free curves: log-rank; P = NS) |
| WBRT + delayed chemotherapy vs. chemotherapy + delayed WBRT | ||||||
| Lee (2008) [16] |
RCT Evidence class I |
G1: Chemotherapy followed by WBRT (n = 25) G2: WBRT followed by chemotherapy (n = 23) |
Pts with BM from NSCLC |
G1: 9.1 months G2: 9.9 months (survival curves; log-rank: P = NS) |
Overall response in brain: G1: PR 7/25, SD 10/25, PD 8/25 G2: PR 9/23, SD 4/23, PD 6/23 (P = NS) |
Progression free survival: G1: 3.6 months G2: 4.4 months (P = NS) |
BM brain metastases, BR brain recurrence (local + distant), CR complete response, G1 group 1, G2 group 2, G3 group 3, G4 group 4, ITT intention-to-treat, NR not reported, NS not significant, NSCLC non-small cell lung cancer, OR objective response, PD progressive disease, PR partial response, Pts patients, RCT randomized control trial, SCLC small-cell lung cancer, SD stable disease, TMZ temozolomide; WBRT whole-brain radiation therapy
Fig. 1.
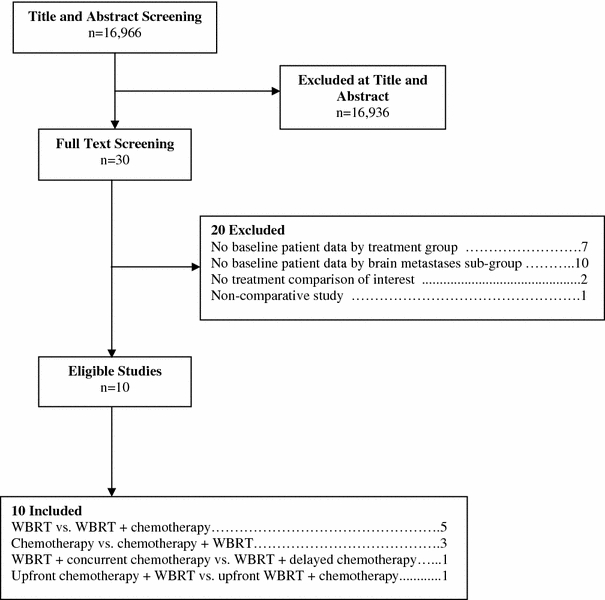
Flow of studies to final number of eligible studies
These 10 studies were assigned to the four sub-questions above as follows:
Chemotherapy vs. chemotherapy + WBRT: 3 studies [12, 13, 17].
Chemotherapy + concurrent WBRT vs. chemotherapy + delayed WBRT: 1 study [15].
Chemotherapy first, followed by WBRT vs. WBRT first, followed by chemotherapy: 1 study [16].
Clearly, the role of chemotherapy in the management of brain metastases has been explored in a very limited number of controlled comparative trials, and therefore the class of evidence and hence the level of recommendations have limited applicability. In addition, outcome parameters vary between the studies, further complicating direct comparisons; nonetheless, these studies do provide important information regarding the endpoints of survival, tumor response to therapy, and time to progression for specific clinical scenarios. Further, we must also acknowledge that these recommendations do not apply to the exquisitely chemosensitive tumors, such as germinomas metastatic to the brain. Finally, although many targeted agents hold some promise in the management of metastatic disease to the brain, controlled comparative trials are just beginning to be conducted, and the data are not sufficiently mature to be included in this analysis. Refer to Table 1 for details of the included studies.
WBRT vs. WBRT plus chemotherapy
Five studies [7–11] met the inclusion criteria for this sub-question. Four of five studies provide class I evidence (two are phase III randomized trials, and two are randomized phase II trials) and the fifth is a retrospective cohort study, providing, at best, class II evidence.
In 2004 Guerrieri et al. [7] published a multi-institutional, randomized controlled trial (RCT) of palliative radiation with concomitant carboplatin for patients with brain metastases from NSCLC, with overall survival as the primary endpoint. Patients with histologically or cytologically proven NSCLC, with ≥1 brain metastases identified by CT or MRI, deemed either inoperable or who refused surgery, with a WHO performance status of 0, 1 or 2, and who had adequate laboratory parameters were included. Prior chemotherapy or brain radiotherapy were exclusion criteria. Patients were stratified by institution. Forty-two patients were randomized to two groups, G1: WBRT (n = 21) G2: WBRT + Carboplatin (n = 21). The radiotherapy dose was 20 Gy in 5 fractions in both arms and the Carboplatin dose was 70 mg/m2 IV/day × 5 days. The detailed demographic breakdown is presented in the tabular summary. Patients were well-balanced between the two arms by age, gender, histology, and number of brain lesions; the status of extra-cranial disease was not reported. There was a mismatch in terms of WHO performance status between the two groups; there were 33% vs. 67% PS 1 patients in G1 vs. G2, and 52% vs. 19% PS 2 patients in G1 vs. G2. Additionally, in G1, 24% of patients had a neurologic function status of 3, compared to 5% in G2. Median follow-up was not reported. The degree of steroid usage in each of the two groups was not reported. The trial was terminated early due to low patient accrual, thus limiting the ability to draw statistically significant conclusions.
The median survival was comparable, 4.4 vs. 3.7 months for G1 vs. G2, which was statistically not significant. Overall response was reported in a subset of patients. Of 11 assessed patients in G1, the OR was 10%, compared to 29% in 16 patients in G2, which was statistically not significantly different; however, when patients were compared in terms of WHO performance status compared to pre-treatment, 14% in G1 were worse, and 57% in G2 were worse; similarly, in terms of neurological function status compared to pre-treatment, 10% were worse in G1, compared to 38% in G2. Although WHO performance and neurologic function deterioration were more common in G2, there were no significant differences in gastrointestinal or hematological toxicities between the groups.
This trial, with incomplete accrual, failed to meet the primary objective of demonstrating improved survival with the addition of carboplatin to WBRT in NSCLC patients with brain metastases. While designed as a class I study, the aforementioned concerns regarding this trial may further limit its impact when making treatment recommendations, as no statistically significant differences in survival were noted between the groups. However, the study does appear to support the use of chemotherapy when secondary endpoints such as response rate are analyzed.
The second major RCT, also designed as a class I study, was reported by Ushio et al. [8] in 1991. Patients with a diagnosis of brain metastases from lung cancer with the primary lesion and/or systemic lesions relatively well controlled, and a projected survival of >4 months, were enrolled. Previous chemotherapy with any of the drugs used in this study was an exclusion factor. Patients were randomized to three groups: G1: WBRT alone (n = 25), G2: WBRT + Chloroethylnitrosoureas (either methyl-CCNU or ACNU) (n = 34), G3: WBRT + Tegafur + Chloroethylnitrosoureas (n = 29). In all three groups, surgery was permitted prior to WBRT, if the lesions could be removed without neurologic deficits. The WBRT dose was 40 Gy in 1.5–2 Gy fractions; the methyl-CCNU dose was 100–120 mg/m2 orally every 6–8 weeks (at midpoint in the study, methyl-CCNU became unavailable and was replaced with ACNU 80–100 mg/m2 IV every 6–8 weeks) and the Tegafur dose was 300 mg/m2/day given orally. Patients were well balanced in all three groups by gender, age, histology, and number of brain metastases. The status of extra-cranial disease, the degree of corticosteroid use, and baseline functional performance score was not reported, and median follow-up of patients was not available.
The primary endpoint was tumor control, but median survival was also analyzed. There was no statistically significant difference in survival between the three arms (27, 29, and 30.5 weeks for G1, G2 and G3 respectively). Intracranial response analysis revealed an overall response rate of 36, 69, and 74% for groups 1–3, respectively. When the response rate for group 1 was statistically compared to that of group 3, it reached statistical significance, with a P < 0.05 (overall response rate: 36 vs. 74%; the comparable complete response rates for the two groups were four of 14 patients vs. 12 of 19 patients). Functional performance outcome was not reported nor was the time to intracranial recurrence/progression. The causes of death were ascertained, and the rate of neurologic death was 3/25 in G1, 0/32 in G2 and 4/28 in G3. Adverse events were not reported in detail in the study; however two patients were thought to have died from the effects of chemotherapy (one from pancytopenia and one from cardiac failure).
In summary, this RCT of 88 patients did not show a survival improvement with the addition of chemotherapy, but showed a statistically significant improvement in response rates, especially the rates of complete response, with the addition of Tegafur and a nitrosourea to WBRT in patients with NSCLC.
In 2002, Antonadou et al. [9] reported on a phase II RCT in which patients with brain metastases were randomized to WBRT alone or WBRT plus temozolomide. Adult patients aged 18 or older, with brain metastases from histologically proven cancer of the lung, breast, or unknown primary, with a performance status ≤2, life expectancy ≥3 months, and adequate hematologic, renal, hepatic function, were included. Exclusion factors were previous chemotherapy or radiotherapy for brain metastases, or any uncontrollable, life-threatening systemic disease, or pregnant or lactating women. Patients (n = 23) in group 1 received 40 Gy of WBRT in 20 fractions of 2 Gy each. In group 2, (n = 25) patients received the same dose of WBRT with 75 mg/m2/day of temozolomide orally during WBRT and continued temozolomide therapy (200 mg/m2/day for 5 days every 28 days for an additional 6 cycles after WBRT. The median follow-up time was 4 months. The groups were well-balanced with respect to gender, age, baseline performance status, neurologic functional level, and tumor type, with 65% of patients having NSCLC, as well as number of brain metastases and presence of extracranial disease.
The primary study endpoints were radiologic response and neurologic symptom evaluation. Survival was also analyzed. The median survival was 7 vs. 8.6 months for G1 vs. G2 (not statistically significant). The overall response rate was 67% vs. 96% for G1 vs.G2, with a P = 0.017 which was statistically significant. The time to recurrence or progression of disease in the brain, and also the cause of death were not reported. There was neurologic improvement in the group receiving temozolomide, and fewer patients required corticosteroids after treatment in the temozolomide group compared with radiotherapy alone. The temozolomide was generally well tolerated with some toxicities statistically more common in that group, including nausea, and vomiting. Hematologic toxicity was reversible.
In summary, this RCT of 48 patients did not show a survival improvement with the addition of temozolomide chemotherapy, but showed a statistically significant improvement in response rates and an improvement in neurologic function with the addition of temozolomide to WBRT, which constitutes class I evidence. We are aware of a subsequent larger randomized trial performed by the same group, but this has never been published in manuscript form and is therefore not available as a peer-reviewed literature item.
In 2003, Verger et al. [10] reported on a phase II RCT in patients with brain metastases randomized to WBRT alone or WBRT plus temozolomide. Adult patients aged 18 or older, with brain metastases from histologically proven cancer, unsuitable for surgery or SRS, with a Karnofsky performance score (KPS) ≥50, and adequate hematologic, renal, and hepatic function, were included. Exclusion factors included previous chemotherapy within the previous 3 weeks, prior cranial radiotherapy, leptomeningeal involvement, intratumoral hemorrhage, and clinical or psychiatric conditions that would interfere with completion or required evaluations.
Stratification variables included age, KPS and type of primary tumor. Patients (n = 41) in G1 received 30 Gy WBRT in 10 fractions of 3 Gy. In G2, 41 patients received the same dose of WBRT with 75 mg/m2/day of temozolomide orally during WBRT and continued temozolomide therapy (150–200 mg/m2/day for 5 days every 28 days for an additional 2 cycles after WBRT.) The median follow-up time was not reported. The groups were well-balanced with respect to gender, age, baseline performance status, tumor type (with 53 and 49% of patients having NSCLC), number of brain metastases and presence of extracranial disease.
Unlike in the other studies mentioned above, the primary outcome in this trial was an analysis of neurologic toxicity. Radiologic response and progression free survival were also analyzed secondarily. The trial was stopped prematurely due to low patient accrual. The median survival was 3.1 vs. 4.5 months for G1 vs. G2 and was not statistically significant. The overall response at day 30 was 32% for both G1 and G2. At 90 days, the radiologic response could only be assessed in 35 patients and was similar in the two groups. Freedom from intracranial progression at 90 days was 54 vs. 72% (P = 0.03) in favor of the WBRT plus temozolomide group. Functional performance change was not reported. There was a statistically significant difference in cause of death between the two groups, with neurologic death occurring in 69% in G1 compared to 41% in G2 (P = 0.029) again favoring the WBRT plus temozolomide group. No acute neurologic toxicity developed in the WBRT plus temozolomide arm and temozolomide did not interfere with delivery of WBRT.
In summary, this prematurely terminated RCT of 82 patients, which was designed as a class I study, did not show either a survival improvement with the addition of temozolomide chemotherapy, or statistically significant improvement in response rates, with the addition of temozolomide to WBRT. Although insufficient to support a level 1 recommendation, the evidence in this study did show an improvement with the addition of chemotherapy in the secondary endpoints of intracranial progression and neurologic death.
Finally, in 2005, Kim et al. [11] published a retrospective cohort study which included NSCLC patients with synchronous brain metastases who received WBRT for intracranial lesions found during evaluation of neurologic symptoms. The exclusion criteria were patients who did not receive WBRT, leptomeningeal carcinomatosis, Eastern Cooperative Oncology Group (ECOG) performance status of grade 3 or 4, surgical resection or radiotherapy for thoracic lesions, or open surgical removal of intracranial metastatic lesions. The interventions included G1: WBRT (n = 32) and G2: WBRT + platinum-based chemotherapy (n = 31). The WBRT dose was 30 to 40 Gy, and several platinum doublets were employed.
The median follow-up was not reported. The groups were well balanced in terms of gender, age, tumor type (100% NSCLC), number of brain metastases, presence of extracranial disease, and baseline performance score. The primary outcome was not specified, but there was a marked difference in median survival, G1: 19.0 weeks vs. G2: 58.1 weeks (P < 0.001). No data were presented regarding tumor control, time to intracranial recurrence, or cause of death. The neurologic response was not significantly different between the two groups.
In summary, this non-randomized cohort study of 63 patients showed a survival improvement with the addition of various platinum-based doublet chemotherapies in addition to WBRT. This constitutes class II evidence. There was no improvement in secondary endpoints.
Chemotherapy vs. chemotherapy plus WBRT
In 2003, Mornex et al. [12] published results of a prospective randomized phase III trial of fotemustine plus WBRT (n = 37) versus fotemustine alone (n = 39) in patients with cerebral metastases from malignant melanoma. The main objectives were objective response and time to cerebral progression. Patients with histologically confirmed malignant melanoma with at least one non-resectable metastasis and who fit other parameters were included. Patients were required to have received no chemotherapy in the prior 4 weeks, no previous nitrosourea-based chemotherapy and no previous cerebral radiotherapy. Both arms were well balanced with respect to the number of cerebral metastases, extent of visceral disease and age. Patients in the fotemustine alone arm had worse baseline performance status (ECOG 2–3 54% compared to 30% in the fotemustine plus WBRT group) and had been treated with more chemoimmunotherapy (59 versus 32% respectively). Additionally, the median time interval between the primary diagnosis and the onset of brain metastases was different between the two groups (550 days for the fotemustine alone group and 1131 days for the fotemustine + WBRT group). The dose of WBRT was 37.5 Gy in 15 fractions over 3 weeks. Fotemustine was given intravenously at 100 mg/m2 on days 1, 8 and 15, followed by a 5 week rest period and then every 3 weeks in non-progressing patients. Although the fotemustine alone patients had worse prognostic factors, there was no difference in cerebral response or control or in overall survival (86 days in the fotemustine group vs. 105 days in the combined treatment group). There was a statistically significant difference in time to cerebral progression favoring the WBRT + fotemustine group (P = 0.028) with that group having a median time to objective cerebral progression of 56 days compared to 49 days in the chemotherapy alone group. This constitutes class I evidence.
A phase III randomized study comparing teniposide (G1) versus teniposide with WBRT (G2) in patients with brain metastases from SCLC was reported by Postmus et al. [13] in 2000. Their stated goal was to evaluate the role of WBRT in SCLC patients with brain metastases. The primary end point was survival. Teniposide was administered intravenously at 120 mg/m2 on days 1, 3, and 5 every 3 weeks up to a maximum of 12 courses or until disease progression either inside or outside the brain. WBRT, dosed at 30 Gy in 10 fractions over 2 weeks, had to be started within 3 weeks of the start of treatment with teniposide. Dexamethasone dosing parameters were outlined. Of the 134 patients randomized, 120 were eligible (60 in each group). The groups were well matched for age, ECOG performance status, neurologic function and number of brain metastases. Although the response rate in the combined modality group (G2) was significantly higher (57%) than in the teniposide alone group (G1) (22%), this did not result in a prolongation of overall survival, thought to be due to progression of disease outside the brain (3.2 months in G1 and 3.5 months in G2). Time to progression in the brain was assessed by CT scan rather than MRI in this European study and was significantly longer in the combined modality group. This RCT constitutes class I evidence.
In a retrospective cohort study, Moscetti et al. [14] analyzed 110 patients (G1) with newly diagnosed NSCLC with brain metastases who had received up-front platinum-based chemotherapy and 46 patients who had received WBRT followed by chemotherapy (G2). The authors sought to analyze the process by which six oncologic centers guided the pattern of care. In this survey of unselected patients, choice of treatment appeared guided by presence of neurologic symptoms from the brain metastases. The response rate in the brain was 27.3% in G1 and 34.8% in G2 with no significant difference in median time to progression in the brain (6 months in both groups). With regard to the first treatment option, the median survival was 10 months for G1 and 14 months for G2. While this study does show that some patients with brain metastases from NSCLC will respond initially to platinum-based chemotherapy, there are too many variables in the patient cohorts and reasons for treatment choice to derive any meaningful data for recommendation. This retrospective study constitutes class II evidence.
Chemotherapy with concomitant WBRT vs. chemotherapy with delayed WBRT
Robinet et al. [15] published a randomized trial in 1998 evaluating the use of systemic chemotherapy for the treatment of inoperable brain metastases from NSCLC with early WBRT versus WBRT delayed until progression. They treated 85 patients with cisplatin and vinorelbine used concurrently with WBRT and 86 treated with the same chemotherapy, but with WBRT delayed for at least 2 cycles. No WBRT-alone group was included. Patients had histologically verified NSCLC and at least one brain metastasis >10 mm in diameter. Patients had an acceptable performance status and good end-organ function. Patients were treated with cisplatin 100 mg/m2 on day 1, vinorelbine 30 mg/m2 on days 1, 8, 15 and 22, with cycles repeated every 4 weeks. In one group, chemotherapy was started concurrent with WBRT, administered as 30 Gy in 10 fractions of 3 Gy given over 2 weeks. In the other group, radiation was deferred.
Median follow-up was not reported, but 171 patients were accrued and the two treatment groups were balanced with regard to age, sex, tumor type and single vs. multiple brain metastases. Extracranial disease and baseline performance status were also balanced between the treatment groups. The primary outcome reported was overall survival. There was no significant difference between the groups with regard to overall survival. The secondary outcome of overall response was also similar at approximately 20% in both groups. This was a combined assessment of brain and extracranial disease response. Functional performance was not reported. Neurologic cause of death was reported as 88% in the group with delayed WBRT as opposed to 81% in the group treated with concurrent WBRT and chemotherapy. Adverse events included toxic deaths in both groups in approximately 8%, and similar instances of myelosuppression, neuro- and renal toxicity and infection. These were equally distributed in both groups.
As a randomized trial of 171 patients, this study provides class I evidence for the similarity in outcome in the treatment of brain metastases from NSCLC with chemotherapy with concurrent vs. delayed WBRT. The initial response rates reported are similar with chemotherapy with or without concurrent WBRT, but overall survival is not significantly different. This study does not address the role of concurrent vs. delayed chemotherapy, but rather concurrent vs. delayed WBRT with chemotherapy, and remains the one and only study to have attempted to answer the question, without any confirmatory trials.
Chemotherapy first followed by WBRT vs. WBRT first followed by Chemotherapy
Lee et al. [16] published a randomized trial in 2008 testing the use of systemic chemotherapy first followed by WBRT vs. WBRT first followed by systemic chemotherapy for the treatment of advanced NSCLC with synchronous brain metastases. They treated 25 patients with gemicitabine and vinorelbine (up to 6 cycles) used prior to WBRT and 23 treated with upfront WBRT followed by the same chemotherapy. No WBRT-alone group was included. Patients had histologically verified NSCLC and clinically silent brain metastasis, not amenable to resection. Patients were 18–75 years of age, with an ECOG performance status of 0–2, measurable disease in both intracranial and extracranial sites, and adequate renal, hepatic and marrow function. The dose of gemcitabine was 900 mg/m2 on day 1, and vinorelbine was 25 mg/m2 on days 1 and 8, every 3 weeks, with a maximum of 6 cycles or disease progression. WBRT was administered as 30 Gy in 10 fractions of 3 Gy given over 2 weeks. In the WBRT-first arm, chemotherapy was initiated after at least a 2 week rest period.
In the primary chemotherapy arm, all patients received WBRT after systemic disease progression or 6 cycles, and no patient had progressive neurologic symptoms or signs by the time WBRT was started. In the WBRT-first arm, four patients deteriorated or died prior to receiving chemotherapy. There was no difference in overall response rates between the two arms (39 vs. 28%, WBRT first vs. chemo first); intracranial response was closely related to extracranial response (k = 0.82). With a median follow-up of 40 months, there was no difference in progression-free survival (PFS) or overall survival. Of note, this study was conducted in Korea, and the proportion of adenocarcinoma histology was 23/25 in the primary chemotherapy arm, and 17/23 in the WBRT first arm. Quality of life (QOL) parameters were evaluated in 33 patients using the European Organisation for Research and Treatment of Cancer (EORTC) questionnaires C30 and L13. Global health status was significantly impaired at baseline, but equally so in both arms. After WBRT, global health status was found to be significantly impaired, with a decreased mean score of 48 from 65. In the chemotherapy-first arm, cognitive function became more impaired as chemotherapy proceeded, whereas in the WBRT-first arm, cognitive function declined for a short period after WBRT, but improved slightly, thereafter. Grade 3 or 4 neutropenia occurred more frequently in the WBRT-first arm (79 vs. 40%, P = 0.014). Other toxicities were comparable.
As a randomized trial of 48 patients, this study provides class I evidence for the similarity in outcome in the treatment of brain metastases from NSCLC with either chemotherapy with delayed WBRT or WBRT followed by chemotherapy, with the caveat that all patients were asymptomatic at study entry, and patient ethnicity may also need to be factored in, given the known variability in clinical behavior and response between Caucasian and Far-Eastern patients.
Conclusions and discussion
The role of chemotherapy in the management of brain metastases has been explored in a very limited number of controlled comparative trials, and therefore the class of evidence and hence the level of recommendations have limited applicability. Further, it has to be acknowledged that these recommendations do not apply to the exquisitely chemosensitive tumors, such as germinomas metastatic to the brain. Additionally, these studies have been conducted mostly in patients with NSCLC and extrapolating to other histologic types would be considered inadequately supported by the data. Further confounding the conclusions is the recognition that some of these patients were pre-treated with chemotherapy, whereas others were chemotherapy-naive, and the differences in outcomes might reflect prior exposure to systemic therapy, which has essentially been inadequately accounted for in most of these trials. Primary endpoints also varied between the trials, with some studies unable to reach a statistically significant conclusion with regard to a primary endpoint, such as overall survival, while reporting significant differences in other secondary endpoints, such as tumor response rates. The variability in these endpoints contributes to the difficulty in making definitive treatment decisions, but the caveats are presented so that clinicians can make informed, individualized clinical decisions for their patients. Lastly, the inclusion in some trials of only asymptomatic patients also warrants consideration, because results from such trials cannot be extrapolated to symptomatic patients.
Major conclusions that emerge from these studies include:
The lack of clear and robust survival benefit with the addition of chemotherapy to WBRT.
Enhanced response rates, specifically in NSCLC with the addition of chemotherapy to WBRT.
In terms of secondary endpoints such as time to neurologic progression, steroid dose, etc., the data and results are mixed and do not permit robust conclusions.
In at least one trial, time to progression was improved by the addition of WBRT to chemotherapy as compared to chemotherapy alone; however, the evidence to corroborate this study is sparse.
A single trial provides evidence that outcome is similar whether WBRT is delivered upfront with chemotherapy or delayed by up to 2 cycles, but the data remains too limited to support definitive recommendations for the delay of radiation therapy, especially given the lack of any known survival advantage with chemotherapy.
Similarly, the sequencing question (does it matter if chemotherapy precedes WBRT or vice versa?) has been inadequately addressed and the data are too sparse to make definitive conclusions.
Key issues for future investigation
Although many targeted agents hold some promise in the management of metastatic disease to the brain, controlled comparative trials are just beginning to be conducted, and the data are not sufficiently mature to be included in this analysis. This remains a major future area of investigation.
Neurocognitive function remains poorly addressed in the majority of these trials and clearly should be accounted for in future trials.
The following is a list of major ongoing or recently closed randomized trials pertaining to the use of chemotherapy that evaluate treatment comparisons addressed by this guideline paper for the management of newly diagnosed brain metastases:
1. Temozolomide for Treatment of Brain Metastases From Non-Small Cell Lung Cancer (Study P03247AM3) (COMPLETED)
Official title A Randomized, Open-Label Phase 2 Study of Temozolomide Added to Whole Brain Radiation Therapy Versus Whole Brain Radiation Therapy Alone for the Treatment of Brain Metastasis From Non-Small Cell Lung Cancer
Status Completed
Clinicaltrials.gov Identifier NCT00076856
Principal Investigator Not provided
Location Not provided
Sponsors and Collaborators Schering-Plough
2. Study of Temozolomide in the Treatment of Brain Metastasis From Non-Small-Cell Lung Cancer (Study P02143) (COMPLETED)
Official title A Phase II Study of Temozolomide (SCH 52365) in Subjects With Brain Metastasis From Non-Small-Cell Lung Cancer
Status Completed
Clinicaltrials.gov Identifier NCT00034697
Principal Investigator Not provided
Location Not provided
Sponsors and Collaborators Schering-Plough
3. Safety and Tolerability of Low-Dose Temozolomide During Whole Brain Radiation in Patients With Cerebral Metastases From Non-Small-Cell Lung Cancer (Study P04071) (TERMINATED)
Official title Randomized Phase II Study: Temozolomide (TMZ) Concomitant to Radiotherapy Followed by Sequential TMZ in Advanced NSCLC Patients With CNS Metastasis Versus Radiotherapy Alone
Status Terminated (Phase II)
Clinicaltrials.gov Identifier NCT00266812
Principal Investigator Not provided
Location Not provided
Sponsors and Collaborators
Schering-Plough
AESCA Pharma GmbH
4. Radiation Therapy With or Without Temozolomide in Treating Patients With Non-Small Cell Lung Cancer That is Metastatic to the Brain
Official title A Phase II Study Of Temozolomide (SCH 52365) In Subjects With Brain Metastasis From Nonsmall Cell Lung Cancer
Status Active, not recruiting (Phase II)
Clinicaltrials.gov Identifier NCT00030836
Principal Investigator Lauren E. Abrey, MD, Memorial Sloan-Kettering Cancer Center
Location United States
Sponsors and Collaborators
Memorial Sloan-Kettering Cancer Center
National Cancer Institute (NCI)
5. Temozolomide With or Without Radiation Therapy to the Brain in Treating Patients With Stage IV Melanoma That Is Metastatic to the Brain
Official title Temozolomide Versus Temozolomide + Whole Brain Radiation In Stage IV Melanoma Patients With Asymptomatic Brain Metastases
Status Active, not recruiting (Phase III)
Clinicaltrials.gov Identifier NCT00020839
Principal Investigator Juergen C. Becker, MD, PhD Universitaets-Hautklinik Wuerzburg
Location Europe (33 locations)
Sponsors and Collaborators
European Organization for Research and Treatment of Cancer
6. Radiation Therapy Combined With Either Gefitinib or Temozolomide in Treating Patients With Non-Small Cell Lung Cancer and Brain Metastases
Official title Whole Brain Radiotherapy in Combination With Gefitinib (Iressa) or Temozolomide (Temodal) for Brain Metastases From Non-Small Lung Cancer (NSCLC) A Randomized Phase II Trial
Status Recruiting (Phase II)
Clinicaltrials.gov Identifier NCT00238251
Principal Investigators
Study Chair: Gianfranco Pesce, MD Oncology Institute of Southern Switzerland
Investigator: Roger Stupp, MD Centre Hospitalier Universitaire Vaudois
Location Switzerland
Sponsors and Collaborators Swiss Group for Clinical Cancer Research
7. Radiation Therapy and Stereotactic Radiosurgery With or Without Temozolomide or Erlotinib in Treating Patients With Brain Metastases Secondary to Non-Small Cell Lung Cancer
Official title A Phase III Trial Comparing Whole Brain Radiation And Stereotactic Radiosurgery Alone Versus With Temozolomide Or Erlotinib In Patients With Non-Small Cell Lung Cancer And 1-3 Brain Metastases
Status Recruiting (Phase III)
Clinicaltrials.gov Identifier NCT00096265
Principal Investigators
Paul Sperduto, MD, MAPP Park Nicollet Cancer Center
Minesh P. Mehta, MD University of Wisconsin, Madison
H. I. Robins, MD, PhD University of Wisconsin, Madison
Location United States and Canada (56 locations)
Sponsors and Collaborators
Radiation Therapy Oncology Group
National Cancer Institute (NCI)
8. Comparison Study of WBRT and SRS Alone Versus With Temozolomide or Erlotinib in Patients With Brain Metastases of NSCLC
Official title A Phase III Trial Comparing Whole Brain Radiation (WBRT) and Stereotactic Radiosurgery (SRS) Alone Versus With Temozolomide or Erlotinib in Patients With Non-Small Cell Lung Cancer and 1-3 Brain Metastases
Status Recruiting (Phase III)
Clinicaltrials.gov Identifier NCT00268684
Principal Investigator Felix Bokstein, M.D. Tel-Aviv Sourasky Medical Center
Location Israel
Sponsors and Collaborators
Tel-Aviv Sourasky Medical Center
RTOG
Acknowledgement
We would like to acknowledge the contributions of the McMaster Evidence-based Practice Center (EPC), Dr. Parminder Raina, (Director). Dr. Lina Santaguida (Co-Associate Director, Senior Scientist) led the EPC staff, which was responsible for managing the systematic review process, searching for and retrieving, reviewing, data abstraction of all articles, preparation of the tables and the formatting and editing of the final manuscripts.
Disclaimer of liability
The information in these guidelines reflects the current state of knowledge at the time of completion. The presentations are designed to provide an accurate review of the subject matter covered. These guidelines are disseminated with the understanding that the recommendations by the authors and consultants who have collaborated in their development are not meant to replace the individualized care and treatment advice from a patient’s physician(s). If medical advice or assistance is required, the services of a competent physician should be sought. The proposals contained in these guidelines may not be suitable for use in all circumstances. The choice to implement any particular recommendation contained in these guidelines must be made by a managing physician in light of the situation in each particular patient and on the basis of existing resources.
Disclosures
All panel members provided full disclosure of conflicts of interest, if any, prior to establishing the recommendations contained within these guidelines.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
References
- 1.Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol. 2005;75(1):5–14. doi: 10.1007/s11060-004-8093-6. [DOI] [PubMed] [Google Scholar]
- 2.Gerstner ER, Fine RL. Increased permeability of the blood-brain barrier to chemotherapy in metastatic brain tumors: establishing a treatment paradigm. J Clin Oncol. 2007;25(16):2306–2312. doi: 10.1200/JCO.2006.10.0677. [DOI] [PubMed] [Google Scholar]
- 3.Seute T, Leffers P, Wilmink JT, ten Velde GP, Twijnstra A. Response of asymptomatic brain metastases from small-cell lung cancer to systemic first-line chemotherapy. J Clin Oncol. 2006;24(13):2079–2083. doi: 10.1200/JCO.2005.03.2946. [DOI] [PubMed] [Google Scholar]
- 4.Robinson PD, Kalkanis SN, Linskey ME, Santaguida PL (2009) Methodology used to develop the AANS/CNS management of brain metastases evidence-based clinical practice parameter guidelines. J Neurooncol. doi:10.1007/s11060-009-0059-2 [DOI] [PMC free article] [PubMed]
- 5.Centre for Evidence-Based Physiotherapy (2009) Physiotherapy evidence database (PEDro). http://www.pedro.org.au/. Accessed Jan 2009
- 6.Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. [PubMed] [Google Scholar]
- 7.Guerrieri M, Wong K, Ryan G, Millward M, Quong G, Ball DL. A randomised phase III study of palliative radiation with concomitant carboplatin for brain metastases from non-small cell carcinoma of the lung. Lung Cancer. 2004;46(1):107–111. doi: 10.1016/j.lungcan.2004.02.019. [DOI] [PubMed] [Google Scholar]
- 8.Ushio Y, Arita N, Hayakawa T, Mogami H, Hasegawa H, Bitoh S, et al. Chemotherapy of brain metastases from lung carcinoma: a controlled randomized study. Neurosurgery. 1991;28(2):201–205. doi: 10.1097/00006123-199102000-00005. [DOI] [PubMed] [Google Scholar]
- 9.Antonadou D, Paraskevaidis M, Sarris G, Coliarakis N, Economou I, Karageorgis P, et al. Phase II randomized trial of temozolomide and concurrent radiotherapy in patients with brain metastases. J Clin Oncol. 2002;20(17):3644–3650. doi: 10.1200/JCO.2002.04.140. [DOI] [PubMed] [Google Scholar]
- 10.Verger E, Gil M, Yaya R, Vinolas N, Villa S, Pujol T, et al. Temozolomide and concomitant whole brain radiotherapy in patients with brain metastases: a phase II randomized trial. Int J Radiat Oncol Biol Phys. 2005;61(1):185–191. doi: 10.1016/j.ijrobp.2004.04.061. [DOI] [PubMed] [Google Scholar]
- 11.Kim DY, Lee KW, Yun T, Kim DW, Kim TY, Heo DS, et al. Efficacy of platinum-based chemotherapy after cranial radiation in patients with brain metastasis from non-small cell lung cancer. Oncol Rep. 2005;14(1):207–211. [PubMed] [Google Scholar]
- 12.Mornex F, Thomas L, Mohr P, Hauschild A, Delaunay MM, Lesimple T, et al. A prospective randomized multicentre phase III trial of fotemustine plus whole brain irradiation versus fotemustine alone in cerebral metastases of malignant melanoma. Melanoma Res. 2003;13(1):97–103. doi: 10.1097/00008390-200302000-00016. [DOI] [PubMed] [Google Scholar]
- 13.Postmus PE, Haaxma-Reiche H, Smit EF, Groen HJ, Karnicka H, Lewinski T, et al. Treatment of brain metastases of small-cell lung cancer: comparing teniposide and teniposide with whole-brain radiotherapy—a phase III study of the European Organization for the Research and Treatment of Cancer Lung Cancer Cooperative Group. J Clin Oncol. 2000;18(19):3400–3408. doi: 10.1200/JCO.2000.18.19.3400. [DOI] [PubMed] [Google Scholar]
- 14.Moscetti L, Nelli F, Felici A, Rinaldi M, De Santis S, D’Auria G, et al. Up-front chemotherapy and radiation treatment in newly diagnosed nonsmall cell lung cancer with brain metastases: survey by Outcome Research Network for Evaluation of Treatment Results in Oncology. Cancer. 2007;109(2):274–281. doi: 10.1002/cncr.22399. [DOI] [PubMed] [Google Scholar]
- 15.Robinet G, Thomas P, Breton JL, Lena H, Gouva S, Dabouis G, et al. Results of a phase III study of early versus delayed whole brain radiotherapy with concurrent cisplatin and vinorelbine combination in inoperable brain metastasis of non-small-cell lung cancer: Groupe Francais de Pneumo-Cancerologie (GFPC) Protocol 95–1. Ann Oncol. 2001;12(1):59–67. doi: 10.1023/A:1008338312647. [DOI] [PubMed] [Google Scholar]
- 16.Lee DH, Han JY, Kim HT, Yoon SJ, Pyo HR, Cho KH, et al. Primary chemotherapy for newly diagnosed nonsmall cell lung cancer patients with synchronous brain metastases compared with whole-brain radiotherapy administered first: result of a randomized pilot study. Cancer. 2008;113(1):143–149. doi: 10.1002/cncr.23526. [DOI] [PubMed] [Google Scholar]
- 17.Schwer AL, Gaspar LE. Update in the treatment of brain metastases from lung cancer. Clin Lung Cancer. 2006;8(3):180–186. doi: 10.3816/CLC.2006.n.045. [DOI] [PubMed] [Google Scholar]