

Abstract
Objectives
This study investigated predictors of mental health service utilization from age 5 through age 16.
Methods
Data were collected on a community sample of 399 children, including 338 European Americans and 61 African Americans. Internalizing and externalizing behaviors were assessed by maternal and teacher reports in kindergarten. History of mental health service utilization was assessed by maternal reports when participants were 16 years old.
Results
On average, the probability of first-time mental health service utilization increased in early to middle childhood, stabilized, then increased in early adolescence. Mother-reports of internalizing behaviors (independent of teacher-reports of externalizing behaviors) predicted an increased likelihood of service use among European-American children but a decreased likelihood of service use among African-American children. Externalizing behaviors (independent of internalizing behaviors) predicted a higher likelihood of first-time service use in middle childhood. The combination of elevated internalizing and externalizing behaviors predicted a higher likelihood of first-time service use in adolescence, mainly among European-American children.
Conclusions
The present study provides evidence that elevated mother-reported internalizing behaviors are less likely to forecast mental health service utilization among African-American children, compared to European-American children. To meet the mental health service needs of all children, it is critical to further examine reasons for service utilization and underutilization among children with internalizing problems.
Key terms: mental health service utilization, ethnicity, internalizing, externalizing
INTRODUCTION
Approximately one in five children and adolescents experience symptoms of a mental disorder and about five percent experience “extreme functional impairment” in a given year.1 Yet, in its first-ever report on mental health, the Surgeon General estimated that 75 to 80% of children in need of mental health services fail to receive them.1 Mental health service underutilization is particularly unfortunate given the mounting evidence that intervention can ameliorate the most common behavioral and emotional problems of childhood and adolescence.2 Understanding factors that predict service utilization would allow us to capitalize on advances in evidence-based intervention.
Ethnicity is a robust predictor of mental health service utilization. Compared to European-American children, ethnic minority children are less likely to utilize mental health services when they have a psychiatric diagnosis or an elevated overall problem score (i.e., internalizing plus externalizing) on a behavior-problem assessment.3–12 Service underutilization among ethnic minorities is evident even after controlling for potential confounds such as socioeconomic status and parenting factors (e.g., parental attitudes about mental health care).5–8 On the basis of this evidence, the Surgeon General concluded: (1) minorities have less access to, and availability of, mental health services, and (2) minorities are less likely to receive needed mental health services.1 Potential explanations for service disparities range from ethnic differences in treatment-seeking and stigma associated with mental illness, to societal failures to provide equal access and quality of care across children of different ethnicities.1
To date, however, very few studies have considered whether overall ethnic disparities in service utilization can be illuminated, in part, by ethnic differences in service use for internalizing versus externalizing behaviors. That is, prior studies have not examined both internalizing behaviors and externalizing behaviors as independent predictors of mental health service utilization; therefore, it has not been possible to gauge whether children of different ethnicities tend to utilize services for different types of problems. An answer to this question would shed new light on disparities in mental health care, by indicating whether type of problem may be used to predict, understand, and reduce ethnic differences in service utilization.
The present study investigated whether mother-reported internalizing behaviors, teacher-reported externalizing behaviors, and ethnicity (European American or African American) would predict mental health service utilization from age 5 through age 16. We also examined interactions between ethnicity and both internalizing and externalizing behaviors. Mother-reported internalizing behaviors and teacher-reported externalizing behaviors were assessed in kindergarten and spanned the full continuum in this community sample (i.e., from low to high levels). When participants were 16 years-old, mothers also provided a detailed developmental history of mental health service utilization, including participants’ use of services for emotional, behavioral, or substance use problems.
We examined whether the association between mother-reported internalizing behaviors and service utilization would be higher among European-American children, compared to African-American children, and whether the association between teacher-reported externalizing behaviors and service utilization would be higher among African-American children, compared to European-American children. We proposed these ethnic differences based on evidence from cross-informant studies which suggests that parents and teachers tend to be less vigilant about internalizing behaviors and more vigilant about externalizing behaviors of African-American children, compared to European-American children.13–18 We also tested main and interactive effects of gender on service utilization, but did not make specific predictions due to inconsistencies in the literature.4,19
The timing of mental health service utilization is critical because maladaptive developmental trajectories may become more entrenched over time without appropriate intervention.20–22 Differences in the time (i.e., age) at which services are utilized might possibly exist among European Americans compared to African Americans. However, the design of most studies is cross-sectional or short-term longitudinal, which limits the opportunity to identify potentially important developmental differences. Information about service use that spanned childhood through adolescence allowed us to investigate developmental fluctuations in the likelihood of first-time service utilization via discrete-time survival analysis. We also examined whether gender, ethnicity, and reports of internalizing and externalizing behaviors interacted with time to predict mental health service utilization.
METHOD
Participants
The families in the present investigation were participants in the Child Development Project.23 Participants were originally recruited during kindergarten pre-registration, in two cohorts (1987 and 1988), from three sites: Nashville and Knoxville, TN and Bloomington, IN. Approximately 75% of families consented to participate in the project. Data collection began the summer before participants entered kindergarten, and follow-up assessments were conducted annually. The initial sample of 585 participants was diverse in terms of gender (52% male), ethnicity (81% European American, 17% African American, 2% other ethnic groups), family composition (26% lived with single mothers), and socioeconomic status (Hollingshead index, M = 40, SD = 14). The Institutional Review Board at each site approved the project.
Sixty-eight percent of the original 585 families provided complete data for the present study (n = 399). Participants included 197 boys and 202 girls; 338 children were European American and 61 were African American. Three participants of other ethnic groups were excluded from analyses due to insufficient sample size. The percentage of African-American children was lower among participants with complete data as compared to participants without complete data, χ2(1) = 8.15, p < .01. In addition, participants with complete data had higher socio-economic status, t(568) = −2.93, p < .01, higher mother-reported internalizing behaviors, t(565) = −3.21, p < .01, and lower teacher-reported externalizing behaviors, t(572) = 3.38, p < .01, compared to participants without complete data. Children with and without complete data did not differ on gender or mental health service utilization.
Measures
SES was measured by Hollingshead (1979) scores based on parental education and occupational status during the child’s kindergarten year.24 SES levels spanned a wide range from unskilled laborers with little formal education to major business people and professionals with high levels of formal education, M = 40.63, SD = 14.30.
Mothers and teachers completed respective versions of the 113-item Child Behavior Checklist (CBCL and CBCL-TRF)25 during the kindergarten year to assess internalizing behaviors (i.e., withdrawn, anxious, and depressive behaviors) and externalizing behaviors (i.e., aggressive and disruptive behaviors). For each item, mothers or teachers indicated whether the statement was not true regarding the target participant (0), somewhat or sometimes true (1), or very or often true (2). In the present study, we used mother reports on the internalizing subscale (M = 6.94, SD = 5.08) and teacher reports on the externalizing subscale (M = 4.96, SD = 7.67). Teacher reports of externalizing behaviors were log-transformed for analyses to correct the skewed distribution. Seventeen percent (17%) and 4% of children were in the borderline and clinical range, respectively, for mother-reports of internalizing behaviors. Thirteen percent (13%) and 2% of children were in the borderline and clinical range, respectively, for teacher-reports of externalizing behaviors.
Similar ratings of conduct problems in kindergarten have been validated as predictors of future involvement with mental health and juvenile justice systems;26 likewise, internalizing and externalizing behaviors in kindergarten predict social, behavioral, and academic outcomes throughout childhood.27–29 We used maternal and teacher reports of children’s behavior because these adults refer and seek treatment for children in the vast majority of cases (rather than children themselves).30 We chose different informants of internalizing and externalizing behaviors because using the same informant of both behavior problems may have introduced problems with multicollinearity. Teachers are viewed as valid informants of children’s externalizing behaviors throughout childhood; and, compared to teachers, mothers may be more accurate informants of children’s internalizing behaviors during early childhood, before children themselves provide reliable reports.31–32
A modified version of the Services Assessment for Children and Adolescents (SACA)34 was used to assess lifetime mental health service utilization. Mothers (n = 399) completed the SACA interview when participants were 16 years old. The SACA includes items that assess whether participants “ever” utilized several overarching types of mental health service (i.e., inpatient/residential, outpatient counseling, or school-based services) for behavioral, emotional, or drug or alcohol problems. Affirmative responses to these items were followed by questions about the age at which the services were first received. In addition, respondents indicated which specific services were used within each overarching service type. In the present study, we considered the following specific types of mental health service: psychiatric hospital or medical unit (n = 15); overnight drug or alcohol treatment unit (n = 2); residential treatment center (n = 7); therapy or counseling (n = 102); drug or alcohol clinic (n = 6); priest, minister, or rabbi (n = 14); and counseling or therapy at school (n = 45). These types of service were grouped together because (1) reports of service use at the general level are more reliable than reports of service use at the specific level33–35 and (2) the rate of each specific type of service was relatively low in the present study. Fathers also completed the SACA interview for 143 of the 399 participants, allowing an assessment of cross-informant agreement. Mothers and fathers agreed on whether services were utilized in 85% of the cases for which both parents completed the SACA interview, χ2(1, n = 143) = 54.07, p < .001.
Data Analysis
Logistic regression and discrete-time survival analyses were used to test the proposed models. The outcome variable in the logistic regression analysis was participants’ use of any mental health services from age 5 through age 16, as reported by mothers. This analysis has the advantage of using SACA data in the most general form, for which reliability is strongest.33–34 We also conducted discrete-time survival analysis to examine developmental fluctuations in first-time service use and to test possible interactions between age of first-time service use and gender, ethnicity, internalizing behaviors, or externalizing behaviors. In both analyses, predictors were entered in the following order: mother-reported internalizing behaviors and teacher-reported externalizing behaviors, the product of internalizing and externalizing behaviors to represent their interaction, ethnicity, the products of ethnicity and both internalizing and externalizing behaviors, SES and gender, and the products of gender and both internalizing and externalizing behaviors. The survival analysis also included time variables on the first step (time, time squared, time cubed, time to the fourth power) and interactions among time and other study variables on the last step. In addition, separate logistic and survival analyses were conducted with mother-reported externalizing behaviors and teacher-reported internalizing behaviors. Survival analyses were also fit with time interactions on the first step to control for violation of the proportionality assumption.
RESULTS
According to maternal reports, 124 participants (31%) received first-time mental health services between age 5 and age 16 (54 boys, 70 girls; 110 European Americans, 14 African Americans). As shown in Table 1, correlation analyses revealed that teacher reports of externalizing behaviors were associated with male gender and lower SES. European-American ethnicity and SES were positively correlated. Among participants who used mental health services, males and children with relatively high externalizing behaviors in kindergarten were more likely to use mental health services at younger ages, rs = .27 and −.35, ps < .01, respectively). African-American children were less likely than European-American children to utilize outpatient therapy or counseling, χ2(1) = 9.36, p < .01, but there were no other ethnic differences in type of service use.
Table 1.
Correlations among Study Variables (N = 399)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. Gender | - | ||||||
| 2. Ethnicity | −.02 | - | |||||
| 3. Socioeconomic status | −.04 | .48*** | - | ||||
| 4. Internalizing (Mother) | .02 | .04 | −.06 | - | |||
| 5. Internalizing (Teacher) | .03 | −.06 | −.16** | .10* | - | ||
| 6. Externalizing (Teacher) | −.15** | −.06 | −.23*** | .01 | .21*** | - | |
| 7. Externalizing (Mother) | −.04 | .01 | −.16** | .57*** | −.00 | .25*** | - |
| Mean | - | - | 40.76 | 6.90 | 4.42 | 4.89 | 11.47 |
| Standard deviation | - | - | 14.31 | 5.06 | 5.38 | 7.62 | 7.05 |
Note: For gender, boys were coded as “0” and girls were coded as “1.” For ethnicity, African Americans were coded as “0” and European Americans were coded as “1.”
p < .001.
p < .01.
A logistic regression was conducted on mental health service utilization as the outcome variable. As shown in Table 2, children with higher teacher-reported externalizing behaviors in kindergarten were more likely to use mental health services through age 16. Gender also predicted service use, such that females were more likely to utilize services than males. In addition, European-American ethnicity and mother-reported internalizing behaviors predicted service utilization; however, these main effects were qualified by a significant ethnicity × internalizing interaction. Specifically, at the mean level of externalizing behaviors and two standard deviations above the mean level of internalizing behaviors, which is near the clinical threshold for internalizing behaviors on the CBCL, the predicted probability of mental health service use was .43 for European-American children and .04 for African-American children. The main and interactive effects of ethnicity held even after controlling for SES (and all other study variables). The test of the final model against a constant-only model was statistically significant, χ2 (10, N = 399) = 32.33, p < .001, −2 log likelihood = 462.21.
Table 2.
Logistic Regression Predicting Mental Health Service Utilization from Age 5 through Age 16 (N = 399)
| Step of entry | Final step | |||||
|---|---|---|---|---|---|---|
| Predictors | b (SE) | Odds ratio (CI) | χ2 change | b (SE) | Odds ratio (CI) | |
| Externalizing behaviors (TR) | .77 (.22)** | 2.16 (1.40 – 3.34) | 12.06** | 1.98 (.77)* | 7.21 (1.60–32.38) | |
| Internalizing behaviors (MR) | .03 (.02) | 1.03 (.99 – 1.07) | 1.78 | −.19 (.10)* | .82 (.68 – .99) | |
| Externalizing × internalizing | .03 (.04) | 1.03 (.95 – 1.12) | .48 | .06 (.05) | 1.07 (.97 – 1.17) | |
| Ethnicity (European-American) | .56 (.33) | 1.75 (.91 – 3.36) | 3.00 | .89 (.45)* | 2.44 (1.01 – 5.89) | |
| Ethnicity × externalizing | −.65 (.72) | .52 (.13 – 2.14) | .85 | −.93 (.77) | .39 (.09 – 1.77) | |
| Ethnicity × internalizing | .23 (.09)* | 1.25 (1.05 – 1.51) | 7.79** | .24 (.10)* | 1.27 (1.05 – 1.54) | |
| Gender (female) | .51 (.23)* | 1.66 (1.05 – 2.61) | 4.85* | .54 (.24)* | 1.71 (1.08 – 2.72) | |
| Socioeconomic status | −.00 (.01) | 1.00 (.98 – 1.02) | .03 | −.00 (.01) | 1.00 (.98 – 1.02) | |
| Gender × externalizing | −.57 (.47) | .56 (.22 – 1.43) | 1.49 | −.57 (.47) | .56 (.22 – 1.43) | |
| Gender × internalizing | −.01 (.05) | .99 (.91 – 1.09) | - | −.01 (.05) | .99 (.91 – 1.09) | |
Note: Final Model χ2 (10, N = 399) = 32.33, p < .001, −2 log likelihood = 462.21. CI = 95% confidence interval. TR = teacher-report. MR = mother report. For gender, boys were coded as “0” and girls were coded as “1.” For ethnicity, African Americans were coded as “0” and European Americans were coded as “1.”
p < .01;
p < .05.
To examine the timing of first mental health service utilization, a series of nested discrete-time survival models that were similar in nature to the logistic regression models were fit to the same data (see Table 3). The unconditional baseline model illustrates the estimated conditional probabilities of service use prior to adding predictors (see Figure 1). As shown in Figure 1, the likelihood of first-time service use increased in early to middle childhood (ages 5 to 6), leveled until early adolescence (age 11–12), then increased again until the age of 15, when the likelihood of first-time service use declined. Overall, the conditional probabilities were low, ranging from less than 2% in early childhood to about 6% at age 15. However, the cumulative survival function indicated that about 31% of all children utilized mental health services by age 16.
Table 3.
Fit of discrete-time survival analysis models predicting first-time mental health service utilization (n = 395a)
| Model | AIC | Deviance | DF | Delta Deviance (Δdf) |
|---|---|---|---|---|
| 1. Baseline | ||||
| Time, Time2, Time3, Time4 | 1070 | 1060 | 4 | |
| 2. Externalizing behaviors (Teacher report) | ||||
| Internalizing behaviors (Mother report) | ||||
| Externalizing × internalizing | 1058 | 1042 | 7 | 18*** (3)b |
| 3. Ethnicity (European-American) | 1057 | 1038 | 8 | 4* (1)b |
| 4. Ethnicity × internalizing | 1051 | 1031 | 9 | 7*** (1)b |
| 5. Time × externalizing | 1049 | 1020 | 13 | 11** (4)b |
Note: Gender, SES, and interactions among gender and other study variables were tested but non-significant; therefore, these variables were not included in the Table.
Age of first service was missing for 4 participants; therefore, they were not used in the survival analysis.
Testing the null hypothesis, predictor is significant.
p< .05;
p<.01;
p<.001
Figure 1.
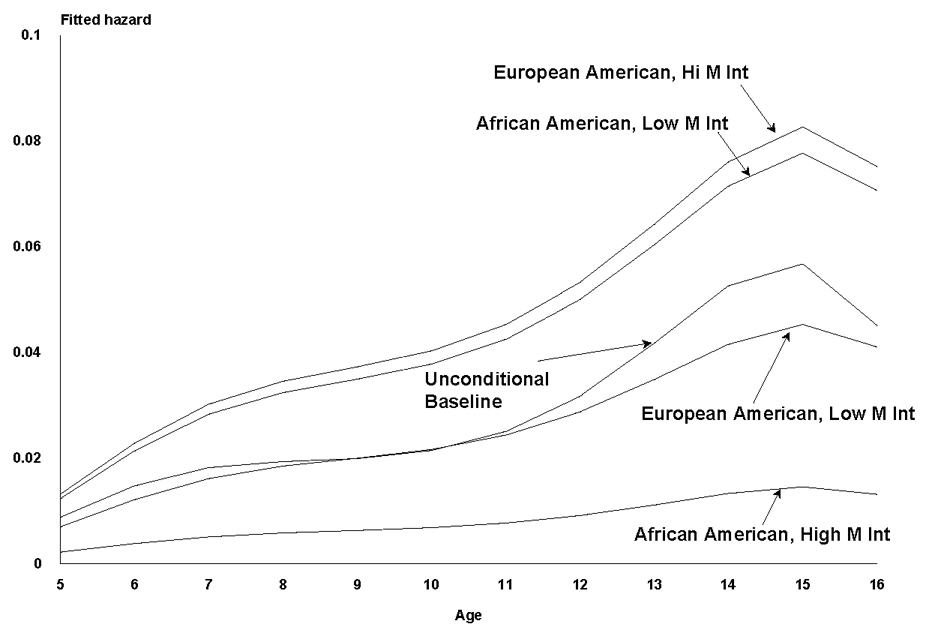
Fitted hazard plot for African Americans and European Americans for the final model showing the effects of the interaction of mother's internalizing scores with ethnicity, holding all else at the mean (N = 395).
Fitted conditional discrete-time survival models tested the effects of predictors on time to first mental health service utilization. As shown in Table 3, mother-reported internalizing behaviors, teacher-reported externalizing behaviors, and European-American ethnicity predicted service utilization. These main effects were qualified by interactions among externalizing behaviors and time, externalizing and internalizing behaviors, and ethnicity and internalizing behaviors.
Teacher-reported externalizing behaviors interacted with time and mother-reported internalizing behaviors to predict service utilization. Specifically, among children who exhibited high externalizing behavior in kindergarten, the likelihood of first-time service use was elevated from age 5 to age 12. Externalizing behaviors had a continuing effect on the likelihood of first-time service use in early adolescence, but mainly among European-American children with high internalizing and high externalizing behaviors in kindergarten.
Consistent with logistic regression results, discrete-time survival analysis revealed that European-American children were more likely to use mental health services compared to African-American children. In addition, there was an interaction between ethnicity and mother-reported internalizing behaviors, indicating that the effect of internalizing behaviors on likelihood of first-time service utilization differed significantly between European-American and African-American children. Figure 1 shows the profiles of likelihood of service utilization among European-American and African-American children at substantively interesting values of predictors (i.e., 1.5 SDs above and below the mean for internalizing behaviors, and 0, 1 for ethnicity).36 At high levels of internalizing behaviors, European Americans had a higher likelihood of first-time service use at each age (highest: 8.3%), compared to African Americans (highest: 1.5%). In contrast, at low levels of internalizing behaviors, African Americans had a higher likelihood of first-time service use in adolescence (highest: 7.8%), compared to European Americans (highest: 4.5%).
We also fit the discrete-time survival model with interactions among time and both internalizing and externalizing behaviors entered on the first step to control for violation of the proportionality of hazards assumption; significant effects were identical to the original model described above. In addition, we tested logistic and discrete-time survival models in which mother and teacher reports of both internalizing behaviors and externalizing behaviors were included as predictors. Mother-reported externalizing behaviors and teacher-reported internalizing behaviors did not predict mental health service utilization as main effects or as part of interactions with other study variables.
DISCUSSION
We investigated reports of childhood internalizing and externalizing behaviors as predictors of mental health service utilization in childhood and adolescence, and tested for gender, ethnic, and developmental differences in these associations. Consistent with prior research,4,19 teacher-reported externalizing behaviors predicted mental health service utilization in both logistic and discrete-time survival models, and the association between externalizing behaviors and service use did not vary by gender or ethnicity. Children who exhibit high levels of aggressive and disruptive behaviors may be referred for mental health treatment due, in part, to the burden these behaviors place on others (e.g., parents, teachers, peers). Although we cannot be certain about why children received mental health services, it is plausible that the offensive nature of externalizing behaviors overrides ethnic-related factors (e.g., inaccessibility of services) that otherwise limit service utilization among African-American children.
Logistic and discrete-time survival analyses also revealed that mother-reported internalizing behaviors differentially predicted mental health service utilization depending on child ethnicity. European-American children with higher internalizing behaviors were more likely to use mental health services than European-American children with lower internalizing behaviors; in contrast, African-American children with higher internalizing behaviors were less likely to use mental health services than African-American children with lower internalizing behaviors, controlling for externalizing behaviors. More specifically, as shown in Figure 1, the likelihood of service use among European-American children with elevated internalizing behaviors was greater than the likelihood of service use among African-American children with elevated internalizing behaviors and European-American children with lower internalizing behaviors. It should be noted, however, that even among European-American children with elevated internalizing behaviors, the likelihood of service utilization was not high in absolute terms, reflecting the possibility of unmet needs among these children. Most notably, African-American children with elevated internalizing behaviors were especially unlikely to utilize mental health services (particularly outpatient therapy or counseling), even as compared to European-American and African-American children with lower internalizing behaviors.
To our knowledge, this is the first study to provide evidence that internalizing behaviors (independent of externalizing behaviors) may partially account for ethnic disparities in childhood mental health service utilization. It is important to emphasize, however, that this ethnic difference is based on a relatively small subsample of African Americans (n = 61). The finding awaits replication with a larger sample before strong conclusions can be drawn. If replicated, the finding is troubling from a public health standpoint. Internalizing problems in childhood can have severe and long-lasting negative consequences,37–38 and African-American and European-American children report similar levels of internalizing problems.1 It may be necessary to raise adults’ awareness of children’s internalizing symptoms as well as effective mental health services for children’s internalizing symptoms.
There are several plausible explanations for ethnic differences in the association between internalizing behaviors and mental health treatment. Potential explanations include ethnic differences in the availability and accessibility of high quality mental health care,1 ethnic differences in parental beliefs about the causes of mental health problems or appropriate forms of treatment,39 and ethnic differences in adults’ responses to certain child behaviors depending on the child’s ethnicity.40–41 For example, parents’ beliefs that racial prejudice contributed to their children’s mental health problems were associated with a lower likelihood of mental health service use, in contrast to attributions involving relationships or trauma.39 In addition, compared to European-American children, parents or teachers may be hypervigilant about African-American children's externalizing behaviors,13–14,17–18 but underreport their internalizing behaviors, 16–17, 30 though evidence for such biases is not always found.42 Investigators have suggested that such ethnic-related biases may be due to adults’ differential attention to or distress thresholds for certain problems depending on child ethnicity, or due to prevailing ethnic stereotypes about what constitutes a problem behavior among African-American youths.30,40,43 These potential biases and inequities could exacerbate African-American children’s overall service underutilization. Future research that examines ethnic differences in views about certain mental health problems, as well as ethnic differences in views about appropriate and accessible solutions, would help reduce ethnic disparities in mental health treatment.
The longitudinal design of the present study also yielded new information about the timing of mental health service utilization. Discrete-time survival models showed that teacher-reported externalizing behaviors were differentially predictive of first-time service use across developmental periods. Externalizing behaviors (independent of mother-reported internalizing behaviors) predicted a higher likelihood of first-time service use in middle childhood. Externalizing behaviors may become increasingly evident or problematic as demands for children’s attentive and compliant participation in elementary school exceed the demands experienced in the home or preschool setting. Indeed, externalizing disorders, such as Oppositional Defiant Disorder and Attention Deficit/Hyperactivity Disorder, are often diagnosed in middle childhood.44 Mental health intervention by middle childhood (or sooner) may limit the extent to which emerging behavior problems become amplified and entrenched through negative exchanges among children and other individuals, which can accumulate across time and settings.20–21 In early adolescence, elevated internalizing behaviors in combination with elevated externalizing behaviors increased the likelihood of first-time service use, mostly for European Americans. It is possible that internalizing behaviors augment the effect of externalizing behaviors on service utilization as children develop the cognitive and emotional capacities to communicate anxious or depressed feelings to adults.
The present study provided evidence that rates of first-time mental health service utilization increase around significant transitional periods. This finding parallels evidence that rates of psychological diagnoses increase in early elementary school and early adolescence.45 Formal school entry is a significant developmental transition during which many children and families experience new demands and challenges and corresponding stress. To an even greater degree, emotional distress is well-documented around the transitions to middle school and junior high school, when early adolescents may experience “role strain” associated with concurrent biological, social, and school changes.46 Indeed, on average, academic performance, school liking, and self esteem decline, whereas loneliness, parent-child conflict, and antisocial behavior increase from fifth to seventh grade.47–48 Rates of psychiatric disorders also begin to increase around age 12.49 We cannot be certain that elevations in mental health service utilization were linked to school transitions; other biological (e.g., pubertal onset) and social (e.g., decreased adult monitoring and increased peer contact) changes occur around the same periods. Results of the present study suggest that children are more likely to begin mental health treatment during developmental periods that generally involve transitions, when rates of emotional and behavioral problems are known to increase.45 An important point is that children and families may be particularly receptive to intervention at these times, in part, because of the inherent change and reorganization associated with such transitions, and due to the increased awareness of stress around such transitions.20
Gender was a predictor of service utilization in the logistic regression analysis but not the survival analysis. In contrast, the interaction between mother-reported internalizing behaviors and teacher-reported externalizing behaviors was a significant predictor of first-time service use in the survival analysis but not the logistic analysis. It is possible that boys are more likely than girls to begin mental health services at younger ages, as a result of higher adult-reported externalizing behaviors. Girls may be more likely than boys to begin services at later ages, when service use becomes more common overall.4,19 Indeed, some research suggests that rates of psychological diagnoses spike in early elementary school among boys and in early adolescence among girls.45 Models that do not account for age of service utilization may detect gender effects that are not stable across time. As suggested by Singer and Willett (2003)50, dichotomization of all individual event histories often results in arbitrary conclusions by eliminating meaningful variation in the actual timing of events.
It is important to note several limitations of the present study and corresponding directions for future research. Data describing children’s mental health service utilization in the past 11 years were drawn from retrospective reports provided by mothers. It is possible that errors in parents’ recollection of their children’s treatment influenced results of the present study. Testing hypotheses based on prospectively collected annual or monthly assessments of behavior problems and service utilization would help limit errors in parents’ recall of their children’s treatment. Furthermore, although internalizing and externalizing behaviors that prompt service use tend to be relatively stable, these behaviors change over the course of childhood and adolescence; thus, we cannot be certain that kindergarten levels of internalizing and externalizing behaviors reflect the behaviors that prompted service use in later childhood or adolescence. Annual assessments of service utilization would also allow investigators to establish more proximal and precise links between annual assessments of internalizing and externalizing problems and service utilization for those behavior problems. Our reliance on maternal reports of service utilization is an additional limitation that could be overcome by including more objective measures of service utilization (e.g., service records). In the present study, we were able to examine only the occurrence and timing of first-time mental health service use. It is important for future research to investigate other dimensions of service use, such as the type, quality, duration, and outcomes of services. Finally, the composition of our sample precluded important questions about ethnicities other than European American and African American.
Despite these limitations, the present study provides new evidence that rates of mental health service utilization increase in early elementary school and early adolescence, and that elevated mother-reported internalizing behaviors are less likely to forecast service utilization among African-American children, compared to European-American children. To meet the mental health service needs of all children, it is critical to further examine reasons for service utilization and underutilization among children with internalizing problems. It appears warranted to direct additional attention to the internalizing problems of African-American children as potential indicators of mental health service needs.
Acknowledgments
The Child Development Project has been supported by grants from the National Institute of Mental Health (MH 42498, MH 56961, MH 57024, MH 57095), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (HD 30572), and the National Institute on Drug Abuse (DA 16903).
Contributor Information
Stephen A. Erath, Department of Human Development and Family Studies, Auburn University, Auburn, AL
Margaret K. Keiley, Department of Human Development and Family Studies, Auburn University, Auburn, AL
Gregory S. Pettit, Department of Human Development and Family Studies, Auburn University, Auburn, AL
Jennifer E. Lansford, Center for Child and Family Policy, Duke University, Durham, NC
Kenneth A. Dodge, Center for Child and Family Policy, Duke University, Durham, NC
John E. Bates, Department of Psychological and Brain Sciences, Indiana University, Bloomington, IN
REFERENCES
- 1.United States Department of Health and Human Services. Mental health: Culture, race, and ethnicity: A report of the Surgeon General. Rockville, MD: 2001
- 2.Kazdin AE, Weisz JR. Evidence-based psychotherapies for children and adolescents. New York: Guilford Press; 2003. [Google Scholar]
- 3.Angold A, et al. Psychiatric disorder, impairment, and service use in rural African American and White youth. Arch Gen Psychiatry. 2002;59:893–901. doi: 10.1001/archpsyc.59.10.893. [DOI] [PubMed] [Google Scholar]
- 4.Mowbray CT, Lewandowski L, Bybee D, Oyserman D. Children of mothers diagnosed with serious mental illness: patterns and predictors of service use. Mental Health Services Research. 2004;6:167–183. doi: 10.1023/b:mhsr.0000036490.10086.95. [DOI] [PubMed] [Google Scholar]
- 5.Garland AF, Lau AS, Yeh M, McCabe KM, Hough RL, Landsverk JA. Racial and ethnic differences in utilization of mental health services among high-risk youths. Am J Psychiatry. 2005;162:1336–1343. doi: 10.1176/appi.ajp.162.7.1336. [DOI] [PubMed] [Google Scholar]
- 6.Hurlburt MS, et al. Contextual predictors of mental health service use among children open to child welfare. Arch Gen Psychiatry. 2004;61:1217–1224. doi: 10.1001/archpsyc.61.12.1217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yeh M, McCabe K, Hough RL, Dupuis D, Hazen A. Racial/ethnic differences in parental endorsement of barriers to mental health services for youth. Mental Health Services. 2003;5:65–77. doi: 10.1023/a:1023286210205. [DOI] [PubMed] [Google Scholar]
- 8.Zahner GEP, Daskalakis C. Factors associated with mental health, general health, and school-based service use for child psychopathology. Am J Public Health. 1997;87:1440–1448. doi: 10.2105/ajph.87.9.1440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kataoka SH, Zhang L, Wells KB. Unmet needs for mental health care among US children: Variation by ethnicity and insurance status. Am J Psychiatry. 2002;159:1548–1555. doi: 10.1176/appi.ajp.159.9.1548. [DOI] [PubMed] [Google Scholar]
- 10.Kodjo CM, Auinger P. Predictors for emotionally distressed adolescents to receive mental health care. J Adolesc Health. 2004;35:368–373. doi: 10.1016/j.jadohealth.2003.12.005. [DOI] [PubMed] [Google Scholar]
- 11.Lavigne JV, et al. Mental health service use among young children receiving pediatric primary care. J Am Acad Child Psychiatry. 1998;37:1175–1183. doi: 10.1097/00004583-199811000-00017. [DOI] [PubMed] [Google Scholar]
- 12.Leslie LK, Hurlburt MS, Landsverk J, Barth R, Slymen DJ. Outpatient mental health services for children in foster care: A national perspective. Child Abuse Negl. 2004;28:697–712. doi: 10.1016/j.chiabu.2004.01.004. [DOI] [PubMed] [Google Scholar]
- 13.Fabrega H, Ulrich R, Loeber R. Adoelscent psychopathology as a function of informant and risk status. J Nerv Ment Dis. 1996;184:27–34. doi: 10.1097/00005053-199601000-00006. [DOI] [PubMed] [Google Scholar]
- 14.Puig M, Lambert MC, Rowan GT, Winfrey T, Lyubansky M, Hannah SD, Hill MF. Behavioral and emotional problems among Jamaican and African American children, ages 6 to 11: Teacher reports versus direct observations. J Emot Behav Disord. 1999;7:240–250. [Google Scholar]
- 15.Wachtel J, Rodrigue J, Geffken G, et al. Children awaiting invasive medical procedures: Do children and their mothers agree on child’s level of anxiety? J Pediatr Psychol. 1994;19:723–735. doi: 10.1093/jpepsy/19.6.723. [DOI] [PubMed] [Google Scholar]
- 16.Walton JW, Johnson SB, Algina J. Mother and child pereceptions of child anxiety: Effects of race, health status, and stress. J Pediatr Psychol. 1999;24:29–39. [Google Scholar]
- 17.Youngstrom E, Loeber R, Stouthamer-Loeber M. Patterns and correlates of agreement between parent, teacher, and male adolescent ratings of externalizing and internalizing problems. J Consult Clin Psychol. 2000;68:1038–1050. doi: 10.1037//0022-006x.68.6.1038. [DOI] [PubMed] [Google Scholar]
- 18.Zimmerman RS, Khoury E, Vega W, Gil A, Warheit G. Teacher and parent perceptions of behavior problems among a sample of African American, Hispanic, and Non-Hispanic White students. Am J Community Psychol. 1995;23:181–197. doi: 10.1007/BF02506935. [DOI] [PubMed] [Google Scholar]
- 19.Sayal K. Annotation: Pathways to care for children with mental health problems. J Child Psychol Psychiatry. 2006;47:649–659. doi: 10.1111/j.1469-7610.2005.01543.x. [DOI] [PubMed] [Google Scholar]
- 20.Conduct Problems Prevention Research Group (CPPRG) A developmental and clinical model for the prevention of conduct disorder: The Fast Track Program. Dev Psychopathol. 1992;4:509–527. [Google Scholar]
- 21.Dodge KA, Pettit GS. A biopsychosocial model of the development of chronic conduct problems in adolescence. Devel Psychol. 2003;39:349–371. doi: 10.1037//0012-1649.39.2.349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Greenberg MT, Domitrovich CE, Bumbarger B. The prevention of mental disorders in school-aged children: Current state of the field. Prevention and Treatment. 2001:4. [Google Scholar]
- 23.Dodge KA, Bates JE, Pettit GS. Mechanisms in the cycle of violence. Science. 1990;250:1678–1683. doi: 10.1126/science.2270481. [DOI] [PubMed] [Google Scholar]
- 24.Hollingshead AB. Four factor index of social status. 1975 Unpublished manuscript. [Google Scholar]
- 25.Achenbach TM. Integrative guide for the 1991 CBCL/4-18, YSR, and CBCL-TRF profiles. Burlington, VT: University of Vermont Department of Psychiatry; 1991. [Google Scholar]
- 26.Jones D, Dodge KA, Foster EM, Nix R Conduct Problems Research Group. Early identification of children at risk for costly mental health service use. Prev Sci. 2002;3:247–256. doi: 10.1023/a:1020896607298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Alexander KL, Entwisle DR. Achievement in the first two years of school : Patterns and processes. Monogr Soc Res Child Dev. 1988;53 (2, Serial No. 218) [PubMed] [Google Scholar]
- 28.Gagnon C, Craig WM, Tremblay RE, Zhou RM. Kindergarten predictors of boys’ stable behavior problems at the end of elementary school. J Abnorm Child Psychol. 1995;23:751–766. doi: 10.1007/BF01447475. [DOI] [PubMed] [Google Scholar]
- 29.Keiley MK, Bates JE, Dodge KA, Pettit GS. A cross-domain analysis : Externalizing and internalizing behaviors during 8 years of childhood. J Abnorm Child Psychol. 2000;28:161–179. doi: 10.1023/a:1005122814723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Roberts RE, Alegria M, Roberts CR, Ger Chen I. Mental health problems of adolescents as reported by their caregivers: A comparison of European, African, and Latino Americans. J Behav Health Ser R. 2005;32:1–13. [PubMed] [Google Scholar]
- 31.Loeber R, Green SM, Lahey BB. Mental health professionals’ perception of the utility of children, mothers, and teachers as informants on childhood psychopathology. J Clin Child Psychol. 1990;19:136–143. [Google Scholar]
- 32.Hinshaw SP, Han SS, Erhardt D, Huber A. Internalizing and externalizing behavior problems in preschool children: Correspondence among parent and teacher ratings and behavior observations. J Clin Child Psychol. 1992;21:143–150. [Google Scholar]
- 33.Horwitz SM, et al. Reliability of the services assessment for children and adolescents. Psychiatr Ser. 2001;52:1088–1094. doi: 10.1176/appi.ps.52.8.1088. [DOI] [PubMed] [Google Scholar]
- 34.Hoagwood K, et al. Concorfance between parent reports of children’s mental health services and service records: The services assessment for children and adolescents (SACA) J Child Fam Stud. 2000;9:315–331. [Google Scholar]
- 35.Bean DL, et al. False-negative reporting and mental health services utilization: Parents’ reports about child and adolescent services. Mental Health Services Research. 2000;2:239–249. [Google Scholar]
- 36.Willett JB, Sayer AG. Using covariance structure analysis to detect correlates and predictors of individual change over time. Psychol Bull. 1994;116:363–381. [Google Scholar]
- 37.Beidel DC, Turner SM. Shy children, phobic adults: Nature and treatment of social phobia. Washington, D.C: American Psychological Association; 2007. [Google Scholar]
- 38.Caspi A, Elder GH, Bem DJ. Moving away from the world: Life-course patterns of shy children. Dev Psychol. 1989;24:824–831. [Google Scholar]
- 39.Yeh M, McCabe K, Hough R, Lau A, Fakhry F, Garland A. Why bother with beliefs? Examining relationships between race/ethnicity, parental beliefs about causes of child problems, and mental health service use. J Consult Clin Psychol. 2005;73:800–807. doi: 10.1037/0022-006X.73.5.800. [DOI] [PubMed] [Google Scholar]
- 40.Lau AS, Garland AF, Yeh M, McCabe KM, Wood PA, Hough RL. Race/ethnicity and inter-informant agreement in assessing adolescent psychopathology. J Emot Behav Disord. 2004;12:145–156. [Google Scholar]
- 41.Weisz JR, Suwanlert S, Chaiyasit W, Weiss B, Achenbach TM, Eastman KL. Behavioral and emotional problems among Thai and American adolescents: Parent reports for ages 12–16. J Abnorm Psychol. 1993;102:395–403. doi: 10.1037//0021-843x.102.3.395. [DOI] [PubMed] [Google Scholar]
- 42.Chang DF, Sue S. The effects of race and problem type on teachers’ assessments of student behavior. J Consult Clin Psychol. 2003;71:235–242. doi: 10.1037/0022-006x.71.2.235. [DOI] [PubMed] [Google Scholar]
- 43.Lambert MC, Weisz JR, Knight F, Derosiers M-F, Overly K, Thesiger C. Jamaican and American adult perspectives of child psychopathology: Further exploration of the threshold model. J Consult Clin Psychol. 1992;60:146–149. doi: 10.1037//0022-006x.60.1.146. [DOI] [PubMed] [Google Scholar]
- 44.Maughan B, Rowe R, Messer J, Goodman R, Meltzer H. Conduct disorder and oppositional defiant disorder in a national sample: developmental epidemiology. J Child Psychol Psyc. 2004;45:609–621. doi: 10.1111/j.1469-7610.2004.00250.x. [DOI] [PubMed] [Google Scholar]
- 45.Schor EL. Use of health care services by children and diagnoses received during presumably stressful life transitions. Pediatrics. 1986;77:834–841. [PubMed] [Google Scholar]
- 46.Fenzel ML. Role strain in early adolescence: A model for investigating school transition stress. J Early Adolescence. 1989;9:13–33. [Google Scholar]
- 47.Barber BK, Olson JA. Assessing the transitions to middle and high school. J Adolescent Res. 2004;19:3–30. [Google Scholar]
- 48.Eccles JS, Midgley C, Wigfield A. Development during adolescence: The impact of stage-environment fit on you adolescents’ experiences in schools and in families [Special issue] Am Psychol. 1993;48:90–101. doi: 10.1037//0003-066x.48.2.90. [DOI] [PubMed] [Google Scholar]
- 49.Costello EJ, et al. Prevalence and Development of Psychiatric Disorders in Childhood and Adolescence. Arch Gen Psychiatry. 2003;60:837–844. doi: 10.1001/archpsyc.60.8.837. [DOI] [PubMed] [Google Scholar]
- 50.Singer JD, Willett JB. Applied longitudinal data analysis: Modeling change and event occurrence. New York: Oxford University Press; 2003. [Google Scholar]