

Abstract
This article highlights the latest findings regarding the cognitive–behavioral syndromes of neglect and anosognosia for hemiplegia that occur following right hemisphere stroke. We review papers published in the past 2 years pertaining to neurophysiology, assessment, and intervention for these two syndromes.
Introduction
Stroke results in a variety of neurobehavioral impairments [1]; among the most common after right hemisphere stroke are hemispatial neglect and anosognosia [2,3]. Although these two syndromes are distinguishable and dissociable, they frequently co-occur [2]. Both lead to significant disability and may have a negative impact on recovery from hemiplegia [4], immobility [5], and overall functional deficits [6]. This effect on recovery may be secondary to the negative influence of neglect and anosognosia on engagement in the rehabilitation process. Recent investigations focus on understanding the impaired cognitive mechanisms and neural circuitry underlying these two syndromes, with the goal of improving intervention. In this article, we review recently published literature on neglect and anosognosia following right hemisphere stroke.
Neglect
Neglect has been defined as an impairment in attention or response to stimuli in the hemispace contralateral to the lesion, not attributable to a primary sensory or motor deficit [7]. However, this definition does not capture the heterogeneity of neglect. Varieties of neglect can be distinguished on the basis of regions of space affected, reference frame, or mode of output as well as the sensory modality [8]. Research over the past year reflects the recognition of diversity of neglect, with studies focused on better characterization of the presentation, pathophysiology, assessment, and intervention.
Cognitive and neural mechanisms of neglect
Recent research has evaluated how the heterogeneous forms of neglect constrain models of the normal cognitive representations underlying spatial attention. One model posits that attention is distributed across representations with distinct frames of reference. A spatial map with a viewer-centered frame of reference, defined according to the midline of the body, head, or retina, is required for gait direction, reaching movements, or eye movements toward targets. Neglect affecting the contralesional side of space defined by the viewer may be characterized as “egocentric” [9]. In contrast, a spatial representation with a stimulus-centered frame of reference is required for recognizing visual stimuli irrespective of their location relative to the viewer (eg, recognizing a printed word irrespective of its location on the page). A more abstract spatial representation with an object-centered frame of reference is required to recognize objects irrespective of their orientation (eg, to recognize a clock or a word presented upside down) or modality of input (eg, a word spelled aloud). Neglect of the contralesional side of the physical stimulus, regardless of the location of the stimulus with respect to the viewer (stimulus-centered neglect), or neglect of the contralesional side of the abstract representations of the object (irrespective of its orientation or modality) may be categorized as “allocentric” [10]. See Figure 1 for the distinction between egocentric and allocentric neglect.
Figure 1.
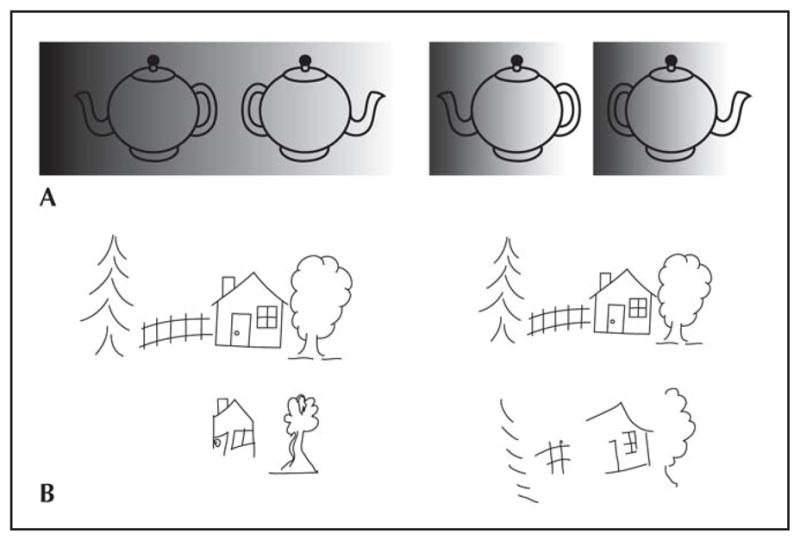
Egocentric and allocentric neglect. A, Schematic representation of egocentric neglect (left), in which the patient neglects the leftmost side of the view (the left teapot), and allocentric neglect (right), in which the patient neglects the left side of each teapot in the picture (the spout of the left teapot and the handle of the right one). B, Copy of the same scene by a patient with egocentric neglect (left) and a patient with allocentric neglect (right).
Using this model, neglect in different reference frames (egocentric neglect vs allocentric neglect) was investigated after right and left hemisphere stroke to determine whether there were differences in the frequency or character of neglect [11]. Left hemisphere damage was more frequently associated with allocentric neglect than egocentric neglect, whereas the opposite was found after right hemisphere stroke. The frequency of the two types of neglect combined was very similar after right and left hemisphere stroke. Earlier reports that neglect is more frequent and severe after right than after left hemisphere stroke may reflect their disproportionate reliance on tests of egocentric neglect. The authors also found that left or right parietal and posterior frontal lesions resulted in egocentric neglect, whereas temporal lesions resulted in more allocentric neglect [11].
Similar results were found in two recent studies of the neural substrates of egocentric versus allocentric neglect [12•,13]. In the first study, egocentric impairments were associated with damage in the premotor cortex involving the frontal eye fields, whereas allocentric impairments were associated with lesions in more ventral regions near the parahippocampal gyrus [12•]. In the second study, egocentric neglect was associated with infarct or hypoperfusion in the right dorsal visual stream including the right supramarginal gyrus, whereas infarct or hypoperfusion in the ventral visual stream including posterior inferior temporal gyrus was associated with allocentric neglect. Results were consistent with the hypothesis that the dorsal stream is essential for guiding movements toward an object (which would require an egocentric spatial representation), whereas the ventral stream is essential for recognizing objects (which would require an orientation- and location-independent allocentric representation).
There also have been advances in our understanding of the role of cortical versus white matter functioning in the manifestation of neglect. Older studies indicate that neglect results from damage to the cerebral cortex or subcortical gray matter, not from white matter damage per se [14]. However, more recently there has been focus on damage to white matter bundles, revitalizing Geschwind’s [15] model of the role of interhemispheric disconnection in neglect. Doricchi et al. [16•] reviewed evidence from animal and human literature that functional disruption of different white matter/gray matter networks may be associated with different neglect presentations. They call for further research on the role of white matter/gray matter networks underlying distinct neglect syndromes.
Another hypothesis regarding the neural mechanisms underlying neglect that has recently resurfaced is that of hemispheric rivalry. Following a functional connections model, Koch et al. [17] postulate that right hemisphere suppression by the intact left hemisphere can explain, at least in part, the preferential processing of stimuli on the ipsilateral (right) side. They found that transcranial magnetic stimulation to suppress the intact left posterior parietal cortex of patients with neglect after right hemisphere stroke resulted in amelioration of visual neglect, supporting potential avenues for intervention.
Factors that influence neglect severity
A recent study provided evidence that older stroke patients have more severe allocentric or egocentric neglect than younger patients, independent of the size of the stroke [18]. However, men and women showed very similar prevalence and severity of neglect [19].
Assessment of neglect
It is well recognized that neglect significantly impedes recovery from stroke [3]. It is associated with falls [20], longer lengths of hospital stay, and less likelihood of being discharged home [21]. To address the significant impact on daily functioning, investigators have sought to determine thorough assessment techniques that can capture the impact on functioning.
Most traditional tests of neglect are paper-and-pencil tasks that evaluate processing stimuli in the contralesional space or contralesional side of the visual stimuli. More recently, investigators have turned to more technologically advanced and possibly more ecologically valid tasks. For example, a recent study assessed the diagnostic sensitivity of computerized tasks of feature and conjunction visual search compared with traditional paper-and-pencil measures of neglect [22]. The computerized tasks differentiated between individuals with right or left hemisphere stroke and healthy controls just as well as traditional neglect tasks. Such computerized tasks may have the advantage of being less susceptible to test–retest bias, making them suitable for recovery tracking.
Other tests have focused on making assessment measures more functional by asking patients to perform tasks with which they show difficulty in daily life. Patients with neglect tend to deviate from a straight path when ambulating/moving in a wheelchair, sometimes leading to collisions and injuries. Several recent studies have sought to better characterize these behaviors and how they affect daily functioning. Turton et al. [23] investigated the navigational trajectory of 15 patients with right hemisphere damage who used a wheelchair or ambulated without assistive devices. Wheelchair users deviated to the left of center of the corridor, whereas independent ambulators deviated to the right of center of the corridor, indicating that the direction of deviation is task dependent.
In another recent study, Punt et al. [24] proposed functional tasks of neglect to better understand the errors in neglect patients. Seven individuals with neglect were asked to perform two tasks in a power wheelchair: negotiate an obstacle course and steer a central path between gaps (doorways) of different sizes. As expected, the subjects demonstrated contralesional errors on the obstacle course. However, they deviated to the ipsilesional side of larger doorways and tended more toward the contralesional side of smaller doorways, similar to the crossover effect seen in paper-and-pencil tasks.
Another attempt to recreate a naturalistic environment to determine the functional implications of neglect has led to the use of virtual reality. A recent study by Jannink et al. [25] assessed acute stroke patients with orientation and exploration tasks when immersed in a three-dimensional, virtual environment. Individuals with neglect could be differentiated from healthy controls with regard to total time spent on the test, mean response time left field of vision, mean response time in the left field of vision/environment, and scanning search pattern. Based on a recent review of the use of virtual reality for assessment and intervention of neglect, it appears that virtual reality can enhance current methods of diagnosis of neglect, given its ability to provide additional information about eye movements, postural changes, and limb kinematics [26••]. Additionally, virtual reality has the advantage of being able to place individuals in potentially unsafe situations to assess and intervene without truly putting the individual at risk. Although this new technology is intriguing, limitations include high cost and weight of the equipment to be worn by patients with impaired movement.
Interventions for neglect
A variety of intervention techniques have been developed in attempts to remediate the behavioral disturbance of neglect. Top-down mechanistic interventions for neglect, such as scanning treatments, which focus on training patients to orient to the neglected side, have sometimes been effective [27]. However, they rely on the patient learning a technique to compensate for neglect, which is not always possible. Furthermore, scanning treatments may be effective for visual neglect but not for other modalities of neglect. These limitations have spurred researchers to investigate bottom-up mechanistic interventions for neglect further.
Bottom-up mechanistic interventions use sensory stimulation to enhance perception of the contralesional space. Prism adaptation through the use of rightward prism glasses has received the most attention. It is hypothesized that the optical deviation of the visual field to the ipsilesional side produced by the prism results in a systematic contralesional deviation of visuomotor responses. Recent studies have evaluated augmentation of prism adaptation with other techniques. Nijboer et al. [28] investigated the influence of prism adaptation treatment on attention orienting under conditions of exogenous and endogenous cueing in two patients. There was a leftward reorienting of attention for the endogenous-cue trials but not for the exogenous-cue trials. The authors conclude that prism adaptation may improve neglect by improving compensatory processes of leftward voluntary orienting, rather than by a fundamental change in attentional bias [28]. However, larger-scale studies are needed to confirm these results.
Keller et al. [29] used pursuit eye movement training and arm movements to augment the effect of prism adaptation on neglect. Each of 10 patients received four different single-session treatments: scanning treatment, pursuit eye movement training alone, pursuit eye movement training with prism adaptation, and pursuit eye movement training with arm movements. Pursuit eye movement training alone led to significant improvements in a variety of neglect tasks with only one treatment session, but the combination of pursuit eye movement training and prism adaptation led to no additional improvement. However, it has been widely demonstrated that prism training requires a longer duration of treatment than just one session, so further research is essential.
Finally, Saevarsson et al. [30] investigated the effects of time restrictions and visual and auditory feedback for task completion on the effects of prism adaptation for neglect. Restrictions on visual search time with feedback for correct and incorrect responses rendered prism adaptation non-effective. When the time restrictions and feedback were removed, prism adaptation resulted in improvements on standard neglect measures. However, in another study, a time-pressure component showed a positive effect on a spatial cancellation task [31]. Specifically, in this study the participants were asked to complete a spatial cancellation task with and without instructions regarding a time limit. The authors concluded that the time pressure provided an increased subjective arousal and possibly increased alertness, resulting in improvements in overall brain functioning. These two studies may represent two separate endogenous means for positively affecting spatial neglect.
Anosognosia
Several anosognostic syndromes following right hemisphere stroke have been identified, including unawareness of cognitive, emotional, and physical sequelae. However, anosognosia for hemiplegia (AHP) has received the most attention and scientific scrutiny [32••]. Individuals with AHP have motor impairments leading to gait and self-care deficits but are unaware of the impairments and the deficits in functioning. Because these individuals believe there is nothing wrong with their motor functioning, they do not follow appropriate precautions, resulting in safety risks. Additionally, they do not understand the need for therapeutic interventions, leading to refusals to participate in rehabilitation [33]. Overall, AHP has been found to be associated with longer rehabilitation stays [6] and poorer functional outcomes following stroke [33,34].
Approximately one third of stroke patients present with AHP throughout the acute and subacute rehabilitation phases [2,34,35]. Given the prevalence of AHP after stroke and its impact on recovery and rehabilitation, research has focused on better understanding the pathophysiology as well as appropriate assessment and intervention techniques. Research over the past year has focused particularly on testing a cognitive model of AHP.
Cognitive model and pathophysiology of AHP
A variety of neuropathologic theories have been proposed to explain AHP. An early hypothesis proposed by Geschwind [15] was that AHP represented a disconnection between the sensory processing hemisphere (right) and the verbal expression hemisphere (left). However, it has been demonstrated that even when the left hemisphere is provided information regarding the hemiplegia, the level of awareness does not necessarily change [36]. Other contributory mechanisms also have been proposed. AHP can co-occur with neglect, impaired somatosensory processing, impaired cognitive functioning, and poor psychological adjustment after right hemisphere stroke, but these are not necessary for and do not explain AHP [34–36]. Their co-occurrence may in part be a product of anatomic rather than functional contiguity [35]. Nevertheless, these concomitant impairments may contribute to the persistence of AHP [36].
Historically, research on AHP has led to mixed and sometimes conflicting findings, for several reasons. The timing of the assessment of AHP varied between studies and some used retrospective data for the diagnosis of AHP. Additionally, assessment of AHP was not always completed during the same time period as the ascertainment of neuropathologic data (neuroradiologic study or postmortem analysis). There is evidence that by weeks to months post-stroke, some reorganization of structure–function relationships may have already occurred [37,38]. Furthermore, in the weeks to months post-stroke, coping strategies (maladaptive or adaptive) may have already been implemented and led to a different clinical presentation. Thus, the typically transient behavioral presentation is most likely a reflection not only of infarcted tissue, but also of surrounding, hypoperfused tissue. Furthermore, the severity of AHP likely depends on the degree of cerebral reorganization that has occurred, comorbid factors, and time after the stroke. Therefore, accurate delineation of the timing of assessment of AHP and the neuropathology is needed to determine the relationships between AHP and its neuropathologic underpinnings. Additionally, there needs to be incorporation of other factors, including physical and psychological factors that might contribute to the behavioral presentation of unawareness.
Although several studies have identified lesion locations associated with AHP [39], AHP likely does not result from damage to just one structure or region. Awareness of motor functioning most likely is a complex process that requires integration of sensory, motor, and emotional information involving several brain circuits. Berti and Pia [40] applied the “forward” model of healthy motor control and awareness [41], which specifies that discrepancy between the predicted sensory consequences of intended movement and the actual sensory feedback from the impaired movement leads to normal awareness when detected and anosognosia when not detected. Berti and Pia [40] proposed that the ability to predict the expected sensory consequences of movement is preserved in AHP, but there is a failure to detect when these predictions are incongruent with actual sensory feedback. Recent research has aimed to test various aspects of this model.
Fotopoulou et al. [42••] investigated the role of motor intention in the observed awareness of action in AHP. They evaluated whether hemiplegic individuals with and without AHP could accurately detect movement of the paretic limb when provided false visual feedback, at times using a prosthetic rubber hand. They found that individuals with AHP, more often than those without, ignored the visual feedback of a motionless limb and claimed they had moved the limb when they had attempted a self-generated movement. The authors concluded that motor intention plays a critical role in awareness of action over sensory feedback information.
In another test of the forward theory, Jenkinson et al. [43] presented individuals with AHP, hemiplegic controls, and healthy volunteers with a nonmotor reality-monitoring task and action reality-monitoring task. They found that individuals with AHP exhibit a reality-monitoring impairment for visual information and for motor movement, whereas hemiplegic controls and healthy volunteers do not. The authors concluded that these findings provide preliminary support for the forward model in AHP, proposing that impaired monitoring in AHP is the result of failure to discriminate between internally generated information about intended movements and externally generated sensory information concerning actual movement.
Assessment of AHP
Orfei et al. [44••] recently suggested that a more holistic, wider definition of anosognosia in stroke be considered to facilitate appropriate evaluation and therefore better understanding of anosognosia following stroke. They argue that investigators should incorporate the “causal attribution of the deficit, evaluation of functional implication in activities of daily living, expectations of recovery, changes in various ability domains, and adherence to the treatment” (p 281) along with the basic awareness of the deficit itself in the assessment process. Additionally, they suggest that evaluation of anosognosia include concurrent dimensions of the general level of cognitive impairment, memory functioning, language functioning, executive functioning, and psychopathology. Finally, incorporation of both conventional and nonconventional (eg, diffusion tensor imaging) neuroimaging is recommended to provide relevant information about the neural circuitry underlying dimensions of awareness impairments. The goal of this more holistic approach is to develop a reliable assessment procedure for anosognosia that considers the neuropathologic, cognitive, emotional, and behavioral factors playing a role in its presentation and course. Behavioral syndromes, such as impaired self-awareness, are quite complex; the interplay between neuropathology and the experience and reaction of the individual to the resulting impairments cannot be teased apart easily. Consideration of a more holistic model of unawareness will lay the groundwork for developing appropriate interventions.
Intervention for AHP
No single method of treatment or rehabilitation has emerged for AHP [45]. During the very acute stages of recovery following stroke, patients typically present with a myriad of cognitive, behavioral, and physical disturbances that require intervention. Structuring the environment and providing greater levels of supervision to reduce the risk of falls and other safety risks appear important. However, little is known about interventions that have a direct impact on awareness level. In the mid-1980s, research demonstrated that temporary remission of AHP symptoms can be initiated by vestibular stimulation [46]. However, since that time, few advances have been made in treatment approaches. Very recently, Fotopoulou et al. [47•] provided preliminary evidence that using video feedback of the motor impairment may lead to permanent recovery of the AHP. Specifically, they presented the case of a 67-year-old individual with a left-sided hemiplegia and AHP that persisted 3 weeks after onset. They provided her with video feedback of herself performing the awareness assessment, which included questions and execution of motor movements. This feedback intervention reportedly resulted in spontaneous recovery of the AHP, with persistence of the awareness through the next day. Although these results are intriguing and in line with findings from other studies focusing on the effectiveness of video feedback in rehabilitation [48,49], further research is needed to validate this singular finding and to determine whether such interventions are effective in the acute stage of recovery.
Conclusions
Stroke investigators have continued in their pursuit to understand how stroke affects behavior and how better to assess and intervene to address dysfunction. As this review of the recent research suggests, neglect and AHP have continued to draw much attention given their significant impacts on the recovery process and daily life functioning, particularly in the acute stages of recovery. Although these two syndromes frequently co-occur, more recent research has focused on understanding them better as separate entities in terms of their neurophysiology, assessment, and intervention.
Recent research has demonstrated that distinct lesions are associated with different types of hemispatial neglect (eg, egocentric vs allocentric), the severity of which are influenced by age but not gender. However, new treatments (eg, prism adaptation and scanning treatments) have focused on treating egocentric neglect, likely because of the functional implications of egocentric impairments on functional tasks such as reaching and mobility. However, identifying the reference frame of space, mode of output, and sensory modality affected is essential for developing appropriate treatments to address neglect in its various forms.
The evidence is mounting that lesions anywhere in the complex circuitry underlying awareness of deficits may lead to the complex syndrome of AHP. However, further research using diffusion tensor imaging and other imaging methods at the time of AHP assessment is required to delineate these circuits. Improving awareness of the mismatch between the intended movement and the actual movement through visual feedback might ameliorate AHP. Future research should determine the optimal timing and other factors that influence the effectiveness of intervention.
Acknowledgments
This work was supported in part by grant K23 HD052774-02 from the National Institutes of Health, National Institute of Child Health and Human Development/National Center for Medical Rehabilitation Research, and by grant RO1NS047691 from the National Institute of Neurological Disorders and Stroke.
Footnotes
Disclosure: No potential conflicts of interest relevant to this article were reported.
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as:
• Of importance
•• Of major importance
- 1.Barker-Collo S, Feigin V. The impact of neuropsychological deficits on functional stroke outcomes. Neuropsych Rev. 2006;16:53–64. doi: 10.1007/s11065-006-9007-5. [DOI] [PubMed] [Google Scholar]
- 2.Appelros P, Karlsson G, Seiger A, Nydevik I. Neglect and anosognosia after first-ever stroke: incidence and relationship to disability. J Rehab Med. 2002;34:215–220. doi: 10.1080/165019702760279206. [DOI] [PubMed] [Google Scholar]
- 3.Jehkonen M, Laihosalo M, Kettunen J. Anosognosia after stroke: assessment, occurrence, subtypes and impact on functional outcome reviewed. Acta Neurol Scand. 2006;114:293–306. doi: 10.1111/j.1600-0404.2006.00723.x. [DOI] [PubMed] [Google Scholar]
- 4.Gialanella B, Mattioli F. Anosognosia and extrapersonal neglect as predictors of functional recovery following right hemisphere stroke. Neuropsych Rehab. 1992;2:169–178. [Google Scholar]
- 5.Paolucci S, Antonucci G, Guariglia C, et al. Facilitatory effect of neglect rehabilitation on the recovery of left hemiplegic stroke patients: a cross-over study. J Neurol. 1996;243:308–314. doi: 10.1007/BF00868403. [DOI] [PubMed] [Google Scholar]
- 6.Gialanella B, Monguzzi V, Santoro R, Rocchi S. Functional recovery after hemiplegia in patients with neglect: the rehabilitative role of anosognosia. Stroke. 2005;36:2687–2690. doi: 10.1161/01.STR.0000189627.27562.c0. [DOI] [PubMed] [Google Scholar]
- 7.Heilman K, Watson R, Valenstein E. Localization of lesions in neglect and related disorders. In: Kertesz A, editor. Localization and Neuroimaging in Neuropsychology. San Diego: Academic Press; 1994. pp. 495–524. [Google Scholar]
- 8.Hillis A, Caramazza A. A framework for interpreting distinct patterns of hemispatial neglect. Neurocase. 1995;1:189–207. [Google Scholar]
- 9.Hillis A, Rapp B, Benzing L, Carmazza A. Dissociable coordinate frames of unilateral spatial neglect: viewer-centered neglect. Brain Cogn. 1998;37:491–526. doi: 10.1006/brcg.1998.1010. [DOI] [PubMed] [Google Scholar]
- 10.Ota H, Fujii T, Suzuki K, et al. Dissociation of body-centered and stimulus-centered representations in unilateral neglect. Neurology. 2001;57:2064–2069. doi: 10.1212/wnl.57.11.2064. [DOI] [PubMed] [Google Scholar]
- 11.Kleinman J, Newhart M, Davis C, et al. Right hemispatial neglect: frequency and characterization following acute left hemisphere stroke. Brain Cogn. 2007;64:50–59. doi: 10.1016/j.bandc.2006.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12•.Grimsen C, Hildebrandt H, Fahle M. Dissociation of egocentric and allocentric coding of space in visual search after right middle cerebral artery stroke. Neuropsychologia. 2008;46:902–914. doi: 10.1016/j.neuropsychologia.2007.11.028. This article provides confirmatory evidence of two dissociable types of neglect after stroke. [DOI] [PubMed] [Google Scholar]
- 13.Medina J, Kannan V, Pawlak M, et al. Neural substrates of visuospatial processing in distinct reference frames: evidence from unilateral spatial neglect. J Cogn Neurosci. 2008 Nov 18; doi: 10.1162/jocn.2008.21160. (Epub ahead of print) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vallar G, Perani D. The anatomy of unilateral neglect after right-hemisphere stroke lesions. A clinical/CT scan correlation study in man. Neuropsychologia. 1986;24:609–622. doi: 10.1016/0028-3932(86)90001-1. [DOI] [PubMed] [Google Scholar]
- 15.Geschwind N. Disconnexion syndromes in animals and man. Brain. 1965;88:237–294. doi: 10.1093/brain/88.2.237. [DOI] [PubMed] [Google Scholar]
- 16•.Doricchi F, de Schotten M, Tomaiuolo F, Bartolomeo P. White matter (dis)connections and gray matter (dys)functions in visual neglect: gaining insights into the brain networks of spatial awareness. Cortex. 2008;44:983–995. doi: 10.1016/j.cortex.2008.03.006. The authors present new evidence regarding the anatomy of neglect. [DOI] [PubMed] [Google Scholar]
- 17.Koch G, Oliveri M, Cheeran B, et al. Hyperexcitability of parietal-motor functional connections in the intact left-hemisphere of patients with neglect. Brain. 2008;131:3147–3155. doi: 10.1093/brain/awn273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gottesman R, Kleinman J, Davis C, et al. Unilateral neglect is more severe and common in older patients with right hemisphere strokes. Neurology. 2008;71:1439–1444. doi: 10.1212/01.wnl.0000327888.48230.d2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kleinman J, Gottesman R, Davis C, et al. Gender differences in unilateral spatial neglect within 24 hours of ischemic stroke. Brain Cogn. 2008;68:49–52. doi: 10.1016/j.bandc.2008.02.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Czernuszenko A, Czlonkowska A. Risk factors in falls in stroke patients during inpatient rehabilitation. Clin Rehab. 2008;23:176–188. doi: 10.1177/0269215508098894. [DOI] [PubMed] [Google Scholar]
- 21.Wee J, Hopman W. Comparing consequences of right and left unilateral neglect in a stroke rehabilitation population. Am J Phys Med Rehab. 2008;87:910–920. doi: 10.1097/PHM.0b013e31818a58bd. [DOI] [PubMed] [Google Scholar]
- 22.Erez A, Katz N, Ring H, Soroker N. Assessment of spatial neglect using computerized feature and conjunction visual search tasks. Neuropsych Rehab. 2009;2:1–19. doi: 10.1080/09602010802711160. [DOI] [PubMed] [Google Scholar]
- 23.Turton A, Dewar S, Lievesley A, et al. Walking and wheelchair navigation in patients with left visual neglect. Neuropsych Rehab. 2009;19:274–290. doi: 10.1080/09602010802106478. [DOI] [PubMed] [Google Scholar]
- 24.Punt T, Kitadono K, Hulleman J, et al. From both sides now: crossover effects influence navigation in patients with unilateral neglect. J Neurol Neurosurg Psychiatry. 2008;79:464–466. doi: 10.1136/jnnp.2007.129205. [DOI] [PubMed] [Google Scholar]
- 25.Jannink M, Aznar M, de Kort A, et al. Assessment of visuospatial neglect in stroke patients using virtual reality: a pilot study. Int J Rehabil Res. 2008 Aug 7; doi: 10.1097/MRR.0b013e3283013b1c. (Epub ahead of print) [DOI] [PubMed] [Google Scholar]
- 26••.Tsirlin I, Dupierrix E, Chokron S, et al. Uses of virtual reality for diagnosis, rehabilitation, and study of unilateral spatial neglect: review and analysis. Cyberpsychol Behav. 2009;12:175–181. doi: 10.1089/cpb.2008.0208. This is an excellent review of the potential uses of virtual reality as well as the limitations to be considered. [DOI] [PubMed] [Google Scholar]
- 27.Mazer B, Sofer S, Korner-Bitensky N, Gelinas I. Use of the UFOV to evaluate and retrain visual attention skills in clients with stroke: a pilot study. Am J Occup Ther. 2001;55:552–557. doi: 10.5014/ajot.55.5.552. [DOI] [PubMed] [Google Scholar]
- 28.Nijboer T, McIntosh R, Nys G, et al. Prism adaptation improves voluntary but not automatic orienting in neglect. Neuroreport. 2008;19:293–298. doi: 10.1097/WNR.0b013e3282f4cb67. [DOI] [PubMed] [Google Scholar]
- 29.Keller I, Lefin-Rank G, Losch J, Kerkhoff G. Combination of pursuit eye movement training with prism adaptation and arm movements in neglect therapy: a pilot study. Neurorehabil Neural Repair. 2009;23:58–66. doi: 10.1177/1545968308317438. [DOI] [PubMed] [Google Scholar]
- 30.Saevarsson S, Kristjansson A, Hildebrandt H, Halsband U. Prism adaptation improves visual search in hemispatial neglect. Neuropsychologia. 2009;47:717–725. doi: 10.1016/j.neuropsychologia.2008.11.026. [DOI] [PubMed] [Google Scholar]
- 31.George M, Mercer J, Walker R, Manly T. A demonstration of endogenous modulation of unilateral spatial neglect: the impact of apparent time-pressure on spatial bias. J Int Neuropsychol Soc. 2008;14:33–41. doi: 10.1017/S135561770808003X. [DOI] [PubMed] [Google Scholar]
- 32••.Orfei M, Robinson R, Prigatano G, et al. Anosognosia for hemiplegia after stroke is a multifaceted phenomenon: a systemic review of the literature. Brain. 2007;130:3075–3090. doi: 10.1093/brain/awm106. This is an up-to-date review of AHP based on a consensus conference. [DOI] [PubMed] [Google Scholar]
- 33.Hartman-Maeir A, Soroker N, Katz N. Anosognosia for hemiplegia in stroke rehabilitation. Neurorehabil Neural Repair. 2001;15:213–222. doi: 10.1177/154596830101500309. [DOI] [PubMed] [Google Scholar]
- 34.Maeshima S, Dohi N, Funahashi K, et al. Rehabilitation of patients with anosognosia for hemiplegia due to intracerebral haemorrhage. Brain Inj. 1997;11:691–697. doi: 10.1080/026990597123232. [DOI] [PubMed] [Google Scholar]
- 35.Bisiach E, Vallar G, Perani D, et al. Unawareness of disease following lesions of the right hemisphere: anosognosia for hemiplegia and anosognosia for hemianopia. Neuropsychologia. 1986;24:471–482. doi: 10.1016/0028-3932(86)90092-8. [DOI] [PubMed] [Google Scholar]
- 36.Heilman K, Barrett A, Adair J. Possible mechanisms of anosognosia: a defect in self-awareness. Philos Trans R Soc Lond B Biol Sci. 1998;353:1903–1909. doi: 10.1098/rstb.1998.0342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Marshall J. Brain function: neural adaptations and recovery from injury. Annu Rev Psychol. 1984;35:377–408. doi: 10.1146/annurev.ps.35.020184.001425. [DOI] [PubMed] [Google Scholar]
- 38.Wall J. Variable reorganization in cortical maps of the skin as an indication of the lifelong adaptive capacities of circuits in the mammalian brain. Trends Neurosci. 1988;11:549–557. doi: 10.1016/0166-2236(88)90184-1. [DOI] [PubMed] [Google Scholar]
- 39.Pia L, Neppi-Modona M, Ricci R, Berti A. The anatomy of anosognosia for hemiplegia: a meta-analysis. Cortex. 2004;40:367–377. doi: 10.1016/s0010-9452(08)70131-x. [DOI] [PubMed] [Google Scholar]
- 40.Berti A, Pia L. Understanding motor awareness through normal and pathological behavior. Curr Direct Psychol Sci. 2006;15:245–250. [Google Scholar]
- 41.Wolpert D. Computational models of motor control. Trends Cogn Sci. 1997;1:209–216. doi: 10.1016/S1364-6613(97)01070-X. [DOI] [PubMed] [Google Scholar]
- 42••.Fotopoulou A, Tsakiris M, Haggard P, et al. The role of motor intention in motor awareness: an experimental study on anosognosia for hemiplegia. Brain. 2008;131:3432–3442. doi: 10.1093/brain/awn225. The authors present a cleverly designed study suggesting the role of motor intention in awareness. [DOI] [PubMed] [Google Scholar]
- 43.Jenkinson P, Edelstyn N, Drakeford J, Ellis S. Reality monitoring in anosognosia for hemiplegia. Conscious Cogn. 2009;18:458–470. doi: 10.1016/j.concog.2008.12.005. [DOI] [PubMed] [Google Scholar]
- 44••.Orfei M, Caltogirone C, Spalletta G. The evaluation of anosognosia in stroke patients. Cerebrovasc Dis. 2009;27:280–289. doi: 10.1159/000199466. The authors propose a holistic model of anosognosia for research and clinical assessment. [DOI] [PubMed] [Google Scholar]
- 45.Prigatano G. The assessment and rehabilitation of anosognosia and syndromes of impaired awareness. In: Halligan P, Kischka U, Marshall JC, editors. Oxford Handbook of Clinical Neuropsychology (OHCN) Oxford: Oxford University Press; 2003. pp. 387–397. [Google Scholar]
- 46.Cappa S, Sterzi R, Vallar G, Bisiach E. Remission of hemineglect and anosognosia during vestibular stimulation. Neuropsychologia. 1987;25:775–782. doi: 10.1016/0028-3932(87)90115-1. [DOI] [PubMed] [Google Scholar]
- 47•.Fotopoulou A, Rudd A, Holmes P, Kopelman M. Self-observation reinstates motor awareness in anosognosia for hemiplegia. Neuropsychologia. 2009;47:1256–1260. doi: 10.1016/j.neuropsychologia.2009.01.018. This article provides data indicating that motor awareness may improve with treatment. [DOI] [PubMed] [Google Scholar]
- 48.McGraw-Hunter M, Faw G, Davis P. The use of video self-modeling and feedback to teach cooking skills to individuals with traumatic brain injury: a pilot study. Brain Inj. 2006;20:1061–1068. doi: 10.1080/02699050600912163. [DOI] [PubMed] [Google Scholar]
- 49.van Vliet P, Wulf G. Extrinsic feedback for motor learning after stroke: what is the evidence? Disabil Rehabil. 2006;28:831–840. doi: 10.1080/09638280500534937. [DOI] [PubMed] [Google Scholar]