

Abstract
Purpose
To evaluate the safety and period of hospitalization of the treatment of femoral shaft fractures with titanium elastic nails (TEN) in the age range 5 to 14 years. The hypothesis was that TEN might be a low-cost treatment, with good clinical results and short length of hospitalization.
Methods
Thirty children with femur fractures were surgically treated with TEN.
Results
The patients spent an average of 9.4 days in hospital. The average period for the healing process was 7.7 weeks. Partial weight bearing was permitted 3.3 weeks after surgery. The incidence of overgrowth was 60%, with an average of 0.40 cm.
Conclusions
The surgical method brings few complications and results in good limb alignment, with a short period of hospitalization and early return to daily activities and school.
Keywords: Femur, Bone nails, Orthotic devices
Introduction
Femur fracture is the most common orthopedic lesion found in the pediatric population, resulting from high-energy traumas. There are two peaks of incidence: one around the age of 2 years and the other around the age of 12 years. Regarding these lesions, 70% affect the femoral shaft and its treatment has been discussed thoroughly [1].
The conservative choice of treatment is based on skin or skeletal traction, followed by cast, which is a universally used and accepted method [2–4]. Concerning open fractures and multiple traumas in children over the age of 10 years, the surgical approach is the most often recommended. In this situation, intramedullary rods came into use, initially with the rigid Küntscher rods, followed by the semi-rigid Ender rods [5, 6]. More recently, elastic stable intramedullary nails (ESIN), or simply titanium elastic nails (TEN), were introduced, with great applicability in children over the age of 5 years [7, 8].
In addition to the age, the fracture aspects and the stability patterns also influence the choice of treatment. The TEN treatment is more appropriate for transverse and/or short oblique fractures than for long oblique or comminuted fractures, which respond better to external fixation or traction followed by spica cast [1]. Other variables, such as social, economic, and psychological factors, should be considered when choosing the treatment that best suits each patient [9, 10].
This study analyzes the efficacy, safety, and period of hospitalization of the treatment of femoral shaft fractures with ESIN made of titanium (TEN) in the age range 5 to 14 years. The hypothesis was that TEN might provide good clinical results requiring short length of hospitalization.
Methods
Setting
This study was carried out in a large university hospital with public funding. Therefore, the costs of treatment are held by the government, and access to intramedullary nails is narrowed by public budget. Since this study began when the use of TEN for this particular population was relatively new, it was difficult to obtain financial support for the acquisition of the nails. This is, thus, the first Brazilian study on TEN in the treatment of femoral shaft fractures in children by public funding.
Design and patients
All consecutive patients between the ages of 5 and 14 years with femur fractures and treated in our hospital between June 2001 and February 2004 were included in this retrospective observational study. The institutions’ Ethical Committee approved the project.
The criteria for inclusion were: the presence of femoral shaft fractures treated exclusively with ESIN, TEN, and with a follow-up of at least 24 months after fracture. Patients presenting osteometabolic diseases, bone dysplasias, and pathological fractures associated to neuromuscular syndromes were excluded. Patients treated with spica casts or with other surgical techniques (such as those with multiple traumas or at the risk of death, or with bone, skin, or soft tissue conditions that would not allow the insertion of TEN, were excluded). After exclusions, a total of 30 children were assessed.
Patient characteristics
The age range of the patients varied from 5.4 to 13.5 years (9.6 years on average, standard deviation of 2.16). There were 16 (53.3%) male patients.
In the majority of the cases (63.3%), the cause of the fracture was being run over by a vehicle (Table 1). All femur fractures were unilateral. Among the patients studied, 33.3% (10 patients) presented lesions other than fracture of the femur: 13.3% of them were leg fractures (50% ipsilateral and 50% contralateral). Much less frequent were fractures of the skull or the humerus, lesions of soft tissues, clavicle fracture, nose fracture, and fracture of the fifth metatarsal. The femur fractures were transverse in 60% of the cases, oblique in 26.7%, spiral in 6.7%, and 6.7% of the cases were comminuted. There were only two open fractures (Table 1).
Table 1.
Types of fractures and their causes among 30 operated children
| Variable | Frequency (n = 30) | Percentage |
|---|---|---|
| Mechanism of trauma | ||
| Pedestrian hit by vehicle | 19 | 63.3 |
| Car accident | 4 | 13.3 |
| Falls | 4 | 13.3 |
| Objects falling on the limb | 1 | 3.3 |
| Bicycle | 1 | 3.3 |
| Aggression | 1 | 3.3 |
| Associated lesions | ||
| Leg fractures | 4 | 13.3 |
| Skull fracture | 1 | 3.3 |
| Humerus fracture | 1 | 3.3 |
| Nose fracture | 1 | 3.3 |
| Jaw fracture | 1 | 3.3 |
| Fifth metatarsal fracture | 1 | 3.3 |
| Clavicle fracture | 1 | 3.3 |
| Soft tissues lesions | 1 | 3.3 |
| Fracture aspect | ||
| Transverse | 18 | 60.0 |
| Oblique | 8 | 26.7 |
| Spiral | 2 | 6.7 |
| Comminuted | 2 | 6.7 |
| Type of fracture | ||
| Closed | 28 | 93.3 |
| Open | 2 | 6.7 |
TEN insertion
All of the fractures were initially stabilized by skin or skeletal traction. The patients with indication for surgical treatment were then referred to the surgical center and operated on as soon as their clinical conditions were favorable.
They were placed on a radiotransparent table in the supine position. The diameter of the chosen nail (TEN) was roughly 40% of the respective medullary canal (isthmus). The nails were placed in a retrograde fashion, with the aid of an image intensifier, approximately two to three centimeters proximally from the femoral distal growth cartilage (Fig. 1). The reduction of the fractures were all closed. No casts for supplementary immobilization were used.
Fig. 1.
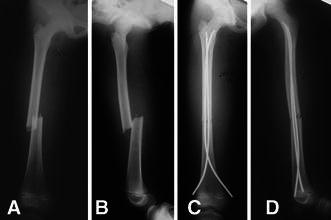
Radiographs of one case of femur fracture, a girl, 9 years and 1 month old, who was submitted to initial treatment with skeletal traction during 1 day, and definitive treatment with titanium flexible nails. a Pre-operation, anteroposterior (AP) view. b Side view. c Post-operation AP view. d Post-operation side view
Post-operative care and follow-up
Depending on the fracture aspects and its reduction, early weight bearing and joint movement were allowed, especially of the knee, and the patient was encouraged to do so soon after the operation.
Anteroposterior and lateral radiographs were taken of the affected limb within 2 weeks, 1 month, 1.5 months till fracture healing, then within 6, 12, and 24 months. Scanometry of the lower ends was performed within 6, 12, 24 months, and at the last evaluation. The measures taken on the last radiographs were analyzed, and only those collected after 24 months were taken into consideration for this study. Measures were taken concerning angle deformities, discrepancies (in centimeters), excessive growth, and final shortening.
The period of traction and hospitalization was recorded, as well as the time until the patient was able to bear weight on the limb and return to his/her daily activities, the period of consolidation, the presence of complications, the number of subsequent hospitalizations, the complaints, and the follow-up time.
After the fracture healing and remodeling, 6–8 months later, the nails have to be removed surgically. The time taken for the removal was only several hours (the patient was admitted in the morning and dismissed by the afternoon). Children could walk freely after nail removal, since they had the fractures consolidated.
Data analysis
The data were analyzed as absolute and relatives frequencies [11] for quantitative measures, and are presented as means, frequencies (%), and standard deviations. Comparisons were made with the Fisher [12] and Mann–Whitney [13] tests.
Results
Surgery and early post-operative period
The majority of patients were submitted to skeletal traction (28, or 93.3%); only two patients received skin traction (6.7%) and only two patients (6.7%) had open fractures grade II of Gustillo and Anderson. The mean traction time before surgery was 5.3 days, with a minimum of 1 and a maximum of 14 days. All fractures were reduced by closed reduction. The mean period of hospitalization for TEN insertion was 9.4 days.
After surgery, the mean time for healing was 7.7 weeks. The average time for the patients to resume their daily activities was 3.7 weeks (ranging between 1 and 10 weeks). Partial weight bearing was allowed after 3.3 weeks on average (ranging from 1 to 8 weeks). The average time for total weight bearing allowance was 8.8 weeks (range 1 to 16 weeks). The minimum follow-up time was 24 months (35.4 months on average). All of the timings are described in Table 2.
Table 2.
Times for hospitalization, healing, activity, and follow-up among 30 children operated for femur fractures
| Variable | Average | SD | Minimum | Maximum |
|---|---|---|---|---|
| Hospitalization time (days) | 9.43 | 4.01 | 4 | 21 |
| Healing time (weeks) | 7.73 | 1.60 | 5 | 10 |
| Resumption of activities (weeks) | 3.70 | 2.23 | 1 | 10 |
| Total weight bearing (weeks) | 8.83 | 3.71 | 1 | 16 |
| Partial weight bearing (weeks) | 3.33 | 2.04 | 0 | 8 |
| Follow-up (months) | 35.40 | 11.17 | 24 | 68 |
Acute complications were seen in two patients (6.7%). One had a migration of a nail and the other had a soft tissue irritation. The first patient needed a second intervention in order to have the tip of the nail cut. One felt pain during the first week post-operatively and needed another surgery to correct the loss of reduction of the fracture. There were two ipsilateral tibial fractures; one was operated and fixed with intramedullary nails (TEN) and the other was treated with a short cast (under the knee) because it was a non-displaced distal tibia fracture.
Late follow-up results
The percentage of patients that were hospitalized to have the nails removed was 90% (27 patients): the other three patients (10%) did not have the nails removed and were lost to follow-up. Only one patient was hospitalized to have the nail shortened due to nail migration. None of the patients suffered a re-fracture.
The final shortening on the limb, after a follow-up period of at least 24 months, occurred in 6.7% of the cases (two patients), with 0.25 cm on average. There was overgrowth in 60% (18) of the patients and the overgrowth was 0.66 cm on average (range 0–1.50 cm). Each patient presented some type of deformity (Table 3), but the average of the deformities did not exceed 10°. Shortening and deformities are described in Table 4.
Table 3.
Types of deformities and complaints of 30 children operated for femur fractures
| Variable | Frequency (n = 30) | Percentage |
|---|---|---|
| Valgus | 12 | 40.0 |
| Varus | 3 | 10.0 |
| Anterior angulation | 23 | 76.7 |
| Posterior angulation | 5 | 16.7 |
| Others hospitalizations | 28 | 93.3 |
| Complaints | 3 | 10.0 |
Table 4.
Limb shortening or overgrowth and deformities after surgery for femur fracture among 30 children operated for femur fractures
| Variable | Average | SD | Minimum | Maximum |
|---|---|---|---|---|
| Shortening (cm) | 0.25 | 0.06 | 0.25 | 0.25 |
| Overgrowth (cm) | 0.66 | 0.43 | 0 | 1.5 |
| Valgus (°) | 6.80 | 4.10 | 0 | 18.0 |
| Varus (°) | 4.30 | 0.60 | 0 | 4.0 |
| Posterior angulation (°) | 2.30 | 1.30 | 0 | 3.0 |
| Anterior angulation (°) | 6.60 | 3.70 | 0 | 14.0 |
Complaints about the treatment were noted among three (10%) of the patients. One patient complained about pain in his knee. The second patient complained about knee pain and about deformity (18° of valgus) as well. A third patient complained about pain in his thigh.
When transverse and oblique fractures are taken into account, excluding the less frequent spiral and comminuted fractures, and comparing these results using Fisher and Mann–Whitney tests, the results, shown in Tables 5 and 6, indicate that neither the characteristics of the patients nor the results of the treatment vary with regard to the types of fracture, transverse or oblique (P > 0.05).
Table 5.
Characteristics of 26 children operated for femur fractures and type of fracture
| Variable | Type | Average | DP | Minimum | Maximum | n | P value |
|---|---|---|---|---|---|---|---|
| Age when fracture occurred (years) | Transverse | 9.68 | 1.92 | 5.4 | 12.7 | 18 | 0.429 |
| Oblique | 10.30 | 2.71 | 5.7 | 13.5 | 8 | ||
| Traction time (days) | Transverse | 5.56 | 2.99 | 1.0 | 14.0 | 18 | 0.978 |
| Oblique | 5.25 | 2.82 | 1.0 | 8.0 | 8 | ||
| Hospitalization time (days) | Transverse | 9.56 | 4.02 | 4.0 | 21.0 | 18 | 0.644 |
| Oblique | 9.13 | 3.98 | 5.0 | 18.0 | 8 | ||
| Healing time (weeks) | Transverse | 7.67 | 1.68 | 5.0 | 10.0 | 18 | 0.935 |
| Oblique | 7.75 | 1.58 | 6.0 | 10.0 | 8 | ||
| Shortening (cm) | Transverse | 0.03 | 0.08 | 0.0 | 0.3 | 18 | 0.683 |
| Oblique | 0.00 | 0.00 | 0.0 | 0.0 | 8 | ||
| Overgrowth (cm) | Transverse | 0.45 | 0.42 | 0.0 | 1.5 | 18 | 0.461 |
| Oblique | 0.34 | 0.50 | 0.0 | 1.2 | 8 | ||
| Resumption of activities | Transverse | 3.89 | 2.22 | 1.0 | 10.0 | 18 | 0.311 |
| Oblique | 2.88 | 1.89 | 1.0 | 6.0 | 8 | ||
| Total weight bearing (weeks) | Transverse | 9.56 | 3.35 | 4.0 | 16.0 | 18 | 0.080 |
| Oblique | 7.25 | 4.30 | 1.0 | 16.0 | 8 | ||
| Partial weight bearing (weeks) | Transverse | 3.33 | 1.81 | 0.0 | 6.0 | 18 | 0.531 |
| Oblique | 2.75 | 2.05 | 0.0 | 6.0 | 8 | ||
| Follow-up (months) | Transverse | 34.44 | 10.16 | 24.0 | 64.0 | 18 | 0.724 |
| Oblique | 36.38 | 15.18 | 25.0 | 68.0 | 8 |
Table 6.
Results for the treatment of femur fracture among 30 children according the type of fracture
| Variable | Category | Type | Total | P value | ||||
|---|---|---|---|---|---|---|---|---|
| Transverse | Oblique | |||||||
| n | % | n | % | n | % | |||
| Traction | Skin traction | 0 | 0.0 | 2 | 25.0 | 2 | 7.7 | 0.086 |
| Skeletal traction | 18 | 100.0 | 6 | 75.0 | 24 | 92.3 | ||
| Acute complications | Yes | 1 | 5.6 | 1 | 12.5 | 2 | 7.7 | 0.529 |
| No | 17 | 94.4 | 7 | 87.5 | 24 | 92.3 | ||
| Shortening | No | 16 | 88.9 | 8 | 100.0 | 24 | 92.3 | >0.999 |
| Yes | 2 | 11.1 | 0 | 0.0 | 2 | 7.7 | ||
| Overgrowth | No | 6 | 33.3 | 5 | 62.5 | 11 | 42.3 | 0.218 |
| Yes | 12 | 66.7 | 3 | 37.5 | 15 | 57.7 | ||
| Valgus | No | 11 | 61.1 | 3 | 37.5 | 14 | 53.8 | 0.401 |
| Yes | 7 | 38.9 | 5 | 62.5 | 12 | 46.2 | ||
| Varus | No | 17 | 94.4 | 7 | 87.5 | 24 | 92.3 | 0.529 |
| Yes | 1 | 5.6 | 1 | 12.5 | 2 | 7.7 | ||
| Anterior angulation | No | 7 | 38.9 | 0 | 0.0 | 7 | 26.9 | 0.062 |
| Yes | 11 | 61.1 | 8 | 100.0 | 19 | 73.1 | ||
| Posterior angulation | No | 14 | 77.8 | 8 | 100.0 | 22 | 84.6 | 0.277 |
| Yes | 4 | 22.2 | 0 | 0.0 | 4 | 15.4 | ||
| Others hospitalizations | No | 15 | 83.3 | 5 | 62.5 | 20 | 76.9 | 0.330 |
| Yes | 3 | 16.7 | 3 | 37.5 | 6 | 23.1 | ||
| Complaints | No | 18 | 100 | 5 | 62.5 | 23 | 88.5 | 0.232 |
| Yes | 0 | 0 | 3 | 37.5 | 3 | 11.5 | ||
| Total | 18 | 100 | 8 | 100 | 26 | 100 | ||
Discussion
There is controversy concerning the best method of treatment for femoral shaft fractures in children at different ages, especially for those between 6 and 10 years of age. All of them can be treated well with a cast, but surgical treatment has become attractive with regard to independence: surgically treated children, without casts, can go to school and do not need an adult to carry them.
The conservative treatment using an early spica cast is indicated for children under the age of 11 years by many authors [2, 3, 14–17]. Others advocate the conservative method, with a cast, only to children under 6 years of age [4, 18]. Due to the possibility of significant limb shortening and bad alignment in children over the age of 5 years, traction may be used before the spica cast application [19]. However, the conservative methods still bring complications even with the traction, such as limb discrepancy, angle deviation, longer hospitalization period, higher cost, compartment syndrome from skin traction, and possible psychological harm [5, 20, 21]. Yet, such treatments do not bring the inherent risks of surgery and they can be performed in every hospital.
The treatment using fixing rods, on the other hand, is more indicated to patients between the ages of 5 and 16 years, according to the literature [7, 8, 22, 23], although more recently, we found reports of the use of this method for preschool children [24]. The age group of 5 to 16 years comprises the phase in which these patients attend school, where independence is important during their treatment. Furthermore, there is the possibility of reducing the hospitalization period and the child can return to school earlier without the associated social isolation and need for an adult for caring, which makes the surgical method more appealing. One should also consider the difficulty in maintaining hygiene when treated with casts, its psychological implications, and prolonged hospitalization due to the traction period [7, 8, 22, 23].
The type of the fracture also influences the method of treatment. In children with long spiral or comminuted fractures, external fixation is usually chosen, as well as in open fractures, in multiple trauma, and head trauma [25–27]. In this study, children with unilateral single fractures of the femur were treated with TEN insertion. The use of a dynamic compression plate (DCP plate) is less often used in children due to the morbidity associated with the surgery, such as infection and overgrowth; yet, it is still indicated to multiple and skull trauma patients [9, 28]. Nowadays, however, the percutaneous technique (DCP plate) is being warranted, in particular for comminuted fractures of the femur (fractures with large comminution should not be treated with flexible nails) [1, 29].
For children between the age of 5 and 16 years, the use of TEN or semi-rigid Ender rods for transverse and short oblique fractures is cited in the literature as the treatment of choice. Using these methods, lesions to the growth cartilage are avoided. These nails allow the control of the length of the extremity, they are of easy application, and they also reduce the hospitalization period, with a faster recovery [7, 8, 10, 17, 22, 30]. The use of TEN has been accepted as a good choice, even for subtrochanteric femur fractures, with safeness [31]. Some authors reported problems to control alignment and limb discrepancies in patients older than 11 years and heavier than 50 kg, and they advise, in these cases, the consideration of other methods, such as locked nailing or plating [29, 32–34].
In our service, TEN is the choice treatment for transverse and short oblique shaft fractures and in patients over the age of 5 years. However, difficulties with the public financial support for nails acquisition limited the inclusion of patients in this study. Despite this, we treated two patients with comminuted and two with spiral fractures using flexible intramedullary nails. For the alignment control of one of the comminuted fractures, the application of three nails was needed. Excluding these four fractures, the comminuted and the spiral ones, we compared statistically the results of the two most common types of fracture of our patients, transverse and oblique, and we did not find any statistical differences between the results.
Newton and Mubarak [35] report a minimum hospitalization period for skin traction of 20.6 days prior to cast placement, for skeletal traction of 20.8 days, for intramedullary nails of 8.5 days, and for early cast placement of 2.5 days. On the other hand, Ligier et al. [7] and Heinrich et al. [10] analyzed fractures treated using flexible nails and found a hospitalization period ranging between 4.5 and 8 days. The patients in this study, treated surgically, presented an average hospitalization period of 9.4 days. This period may have been influenced, in our setting, by the waiting time needed for nails acquisition and by the low availability of operating rooms in a public trauma hospital situated in a central part of a large metropolis as São Paulo, to which a high number of traumatized patients are referred every day. In settings with operating rooms and nails readily available, probably, this period of hospitalization is lower.
According to Stans et al. [27], the use of flexible nails allows a faster healing period with fewer complications than with the external fixation. Ligier et al. [7] report that the elastic movement of the nail promotes faster and more abundant callus formation.
Some authors report earlier return to school of patients treated with TEN compared to other treatments, because the patient can walk with the aid of crutches (partial weight bearing). This time varies from 2 days up to 4 weeks, and for total weight bearing, from 3 to 4 weeks [7, 21, 22]. Other authors report an average of 10 to 11 weeks to begin partial weight bearing allowance [20, 21, 27]. In our group, the average time for fracture healing was 7.7 weeks. The resuming of daily activities begins when the patient is able to walk on his own, with crutches, which corresponds to partial weight bearing allowance. Partial and total weight bearing are allowed after 3.3 and 8.8 weeks, on average, respectively. Total weight bearing depends on consolidation.
The bone shortening incidence in this study was 6.7%, an average of 0.25 cm, which is clinically very well tolerated. Flynn et al. [23] reported 48 patients with 49 fractures, and the largest inequality in the lower-extremity length of their sample was 1 cm. They consider inequalities between 1 and 2 cm as satisfactory results. Based on our results, we believe that the intramedullary method of nail insertion, in most cases, acutely corrects the shortening of the limb. The recently suggested device using cups for distal ends of nails threaded into the bone that can prevent shortening and nail migration was not available in our setting and should be considered, especially in comminuted and long oblique fractures, and evaluated in future cases.
Overgrowth is associated with surgical treatment. Ligier et al. [7] report, in cases treated with ESIN, an average overgrowth of 1.2 mm, and a greater overgrowth in transverse fractures (average of 2.06 mm), with four cases of lengthening of more than 10 mm (11, 15, 17, and 23 mm). Spiral fractures present an average overgrowth of 0.7 mm. Heinrich et al. [10] report, in children treated with TEN between the ages of 6 and 9 years, that 22% have an average overgrowth of 11 mm, and in children over the age of 10 years, 14% of the children have an average overgrowth of 7 mm. Overgrowth was present in 60% of our patients, with an average of 0.66 cm. This result is comparable to those found in the literature [7, 8, 10, 19, 26, 28, 36].
Some angular deviation is accepted (because neither aesthetics nor function is altered) when considering the patient’s age. Cadman and Neer [36] accept angulation and rotation of 15° as a maximum. Heinrich et al. [10] and Buford et al. [37] accept, in children over the age of 6 years, varus and valgus deviation, and anterior and posterior angulation below 10°. Other authors, such as Buehler et al. [16], accept, for any limb treatment in children over the age of 6 years, greater values, with varus and valgus deviation less than or equal to 20° and anterior and posterior deviation less than or equal to 30°. All of the patients in the present study present some type of deviation. The average varus, valgus, and rotational deviations were always lower than 10° (anterior angulation of 6.6°, posterior angulation of 2.3°, varus of 4.3°, and valgus of 6.8°). Only one girl with ipsilateral humerus fracture and contralateral tibia fracture had 18° of valgus. These three fractures were operated and fixed by the intramedullary method. However, this patient did not follow the medical instructions and walked without crutches after 1 week. These angulations were perceived during the follow-up and this is the reason why the authors did not use a complementary cast. According to Flynn et al. [8], an angulation lower than 10° is considered to be satisfactory; thus, we can regard our results as being in accordance with the literature.
We should also take into consideration the fact that the cases treated surgically require further hospitalization for the removal of the nails. Our choice is to remove the nails after 6–8 months after their implantation, which is in accordance to other authors, such as Buford et al. [37] and Flynn et al. [8]. Around this time, the fracture presents a very solid union. Ligier et al. [7] recommend nail removal after 3 months of surgery. Despite this, we had some patients that had their nails removed later because of difficulty in returning to the hospital. We had also three patients lost to follow-up. In our group, in addition to hospitalization for nail removal, there was one case in which the patient needed yet another hospitalization, besides the time to remove the nails, in order to have the tip of one nail that migrated cut.
Some authors report a reduction in the associated psychological problems with the use of nails compared with traction plus cast placement, for they reduce the period of hospital stay, avoid prolonged traction, and allow the patient to return home earlier, with equivalent or lower costs [8, 10]. However, the use of TEN for this morbidity and population was never studied in a public hospital of a developing country. The experience shown in this study prompts the beginning of an economic investigation about the cost of hospitalization versus the conservative (spica cast) treatment.
The majority of the complications occur, according to Flynn et al. [8], in the proximal, distal, and comminuted fractures, with TEN being the ideal implant for transverse fractures of the medium third of the diaphysis. As we described previously, we had one patient that had a migration of one nail that probably occurred because the fragments had slid. Finally, one patient had the nails removed early, at 4 months, because of soft tissue irritation caused by the tip of the nails, which were too long. Flynn et al. [38], in 2002, reported that the most common problem they encountered was irritation at the nail insertion site with 18% of the cases.
Conclusion
Patients older than 5 years of age, with femoral shaft fracture, especially oblique and transverse fractures, are well treated with flexible intramedullary insertion, with good alignment, short period of traction and hospitalization, early return to daily activities and school, and few complications.
References
- 1.Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg. 2004;12(5):347–359. doi: 10.5435/00124635-200409000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Irani RN, Nicholson JT, Chung SM. Long-term results in the treatment of femoral-shaft fractures in young children by immediate spica immobilization. J Bone Joint Surg Am. 1976;58(7):945–951. [PubMed] [Google Scholar]
- 3.Sugi M, Cole WG. Early plaster treatment for fractures of the femoral shaft in childhood. J Bone Joint Surg Br. 1987;69(5):743–745. doi: 10.1302/0301-620X.69B5.2824519. [DOI] [PubMed] [Google Scholar]
- 4.Czertak DJ, Hennrikus WL. The treatment of pediatric femur fractures with early 90–90 spica casting. J Pediatr Orthop. 1999;19(2):229–232. doi: 10.1097/01241398-199903000-00018. [DOI] [PubMed] [Google Scholar]
- 5.Kirby RM, Winquist RA, Hansen ST., Jr Femoral shaft fractures in adolescents: a comparison between traction plus cast treatment and closed intramedullary nailing. J Pediatr Orthop. 1981;1(2):193–197. doi: 10.1097/01241398-198110000-00010. [DOI] [PubMed] [Google Scholar]
- 6.Mann DC, Weddington J, Davenport K. Closed Ender nailing of femoral shaft fractures in adolescents. J Pediatr Orthop. 1986;6(6):651–655. doi: 10.1097/01241398-198611000-00002. [DOI] [PubMed] [Google Scholar]
- 7.Ligier JN, Metaizeau JP, Prévot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988;70(1):74–77. doi: 10.1302/0301-620X.70B1.3339064. [DOI] [PubMed] [Google Scholar]
- 8.Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop. 2001;21(1):4–8. doi: 10.1097/01241398-200101000-00003. [DOI] [PubMed] [Google Scholar]
- 9.Reeves RB, Ballard RI, Hughes JL. Internal fixation versus traction and casting of adolescent femoral shaft fractures. J Pediatr Orthop. 1990;10(5):592–595. doi: 10.1097/01241398-199009000-00004. [DOI] [PubMed] [Google Scholar]
- 10.Heinrich SD, Drvaric DM, Darr K, MacEwen GD. The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: a prospective analysis. J Pediatr Orthop. 1994;14(4):501–507. doi: 10.1097/01241398-199407000-00016. [DOI] [PubMed] [Google Scholar]
- 11.Bussab WO, Morettin PA. Métodos quantitativos: estatística básica. 4. São Paulo: Atual; 1987. [Google Scholar]
- 12.Agresti A. Categorical data analysis. New York: Wiley; 1990. [Google Scholar]
- 13.Conover WJ. Practical nonparametric statistics. 2. New York: Wiley; 1980. [Google Scholar]
- 14.Staheli LT, Sheridan GW. Early spica cast management of femoral shaft fractures in young children. A technique utilizing bilateral fixed skin traction. Clin Orthop Relat Res. 1977;126:162–166. [PubMed] [Google Scholar]
- 15.Martinez AG, Carroll NC, Sarwark JF, Dias LS, Kelikian AS, Sisson GA., Jr Femoral shaft fractures in children treated with early spica cast. J Pediatr Orthop. 1991;11(6):712–716. doi: 10.1097/01241398-199111000-00002. [DOI] [PubMed] [Google Scholar]
- 16.Buehler KC, Thompson JD, Sponseller PD, Black BE, Buckley SL, Griffin PP. A prospective study of early spica casting outcomes in the treatment of femoral shaft fractures in children. J Pediatr Orthop. 1995;15(1):30–35. doi: 10.1097/01241398-199501000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Templeton PA, Wright JG. Femoral shaft fractures: North American and European perspectives. Curr Orthop. 1998;12(3):153–158. doi: 10.1016/S0268-0890(98)90019-6. [DOI] [Google Scholar]
- 18.Illgen R, II, Rodgers WB, Hresko MT, Waters PM, Zurakowski D, Kasser JR. Femur fractures in children: treatment with early sitting spica casting. J Pediatr Orthop. 1998;18(4):481–487. [PubMed] [Google Scholar]
- 19.Viljanto J, Linna MI, Kiviluoto H, Paananen M. Indications and results of operative treatment of femoral shaft fractures in children. Acta Chir Scand. 1975;141(5):366–369. [PubMed] [Google Scholar]
- 20.Kissel EU, Miller ME. Closed Ender nailing of femur fractures in older children. J Trauma. 1989;29(11):1585–1588. doi: 10.1097/00005373-198911000-00020. [DOI] [PubMed] [Google Scholar]
- 21.Timmerman LA, Rab GT. Intramedullary nailing of femoral shaft fractures in adolescents. J Orthop Trauma. 1993;7(4):331–337. doi: 10.1097/00005131-199308000-00008. [DOI] [PubMed] [Google Scholar]
- 22.Vrsansky P, Bourdelat D, Al Faour A. Flexible stable intramedullary pinning technique in the treatment of pediatric fractures. J Pediatr Orthop. 2000;20(1):23–27. [PubMed] [Google Scholar]
- 23.Flynn JM, Luedtke LM, Ganley TJ, Dawson J, Davidson RS, Dormans JP, et al. Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am. 2004;86-A(4):770–777. doi: 10.2106/00004623-200404000-00015. [DOI] [PubMed] [Google Scholar]
- 24.Bopst L, Reinberg O, Lutz N. Femur fracture in preschool children: experience with flexible intramedullary nailing in 72 children. J Pediatric Orthop. 2007;27(3):299–303. doi: 10.1097/BPO.0b013e3180326713. [DOI] [PubMed] [Google Scholar]
- 25.Alonso J, Geissler W, Hughes JL. External fixation of femoral fractures. Indications and limitations. Clin Orthop Relat Res. 1989;241:83–88. [PubMed] [Google Scholar]
- 26.Aronson J, Tursky EA. External fixation of femur fractures in children. J Pediatr Orthop. 1992;12(2):157–163. doi: 10.1097/01241398-199203000-00003. [DOI] [PubMed] [Google Scholar]
- 27.Stans AA, Morrissy RT, Renwick SE. Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop. 1999;19(2):222–228. doi: 10.1097/01241398-199903000-00017. [DOI] [PubMed] [Google Scholar]
- 28.Kregor PJ, Song KM, Routt ML, Jr, Sangeorzan BJ, Liddell RM, Hansen ST., Jr Plate fixation of femoral shaft fractures in multiply injured children. J Bone Joint Surg Am. 1993;75(12):1774–1780. doi: 10.2106/00004623-199312000-00006. [DOI] [PubMed] [Google Scholar]
- 29.Hunter JB. Femoral shaft fractures in children. Injury. 2005;36(Suppl 1):A86–A93. doi: 10.1016/j.injury.2004.12.018. [DOI] [PubMed] [Google Scholar]
- 30.Huber RI, Keller HW, Huber PM, Rehm KE. Flexible intramedullary nailing as fracture treatment in children. J Pediatr Orthop. 1996;16(5):602–605. doi: 10.1097/01241398-199609000-00011. [DOI] [PubMed] [Google Scholar]
- 31.Pombo MW, Shilt JS. The definition and treatment of pediatric subtrochanteric femur fractures with titanium elastic nails. J Pediatr Orthop. 2006;26(3):364–370. doi: 10.1097/01.bpo.0000203005.50906.41. [DOI] [PubMed] [Google Scholar]
- 32.Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE. Complications of titanium elastic nails for pediatric femoral shaft fractures. J Pediatr Orthop. 2003;23(4):443–447. [PubMed] [Google Scholar]
- 33.Moroz LA, Launay F, Kocher MS, Newton PO, Frick SL, Sponseller PD, et al. Titanium elastic nailing of fractures of the femur in children. Predictors of complications and poor outcome. J Bone Joint Surg Br. 2006;88(10):1361–1366. doi: 10.1302/0301-620X.88B10.17517. [DOI] [PubMed] [Google Scholar]
- 34.Kuremsky MA, Frick SL. Advances in the surgical management of pediatric femoral shaft fractures. Curr Opin Pediatr. 2007;19(1):51–57. doi: 10.1097/MOP.0b013e3280123142. [DOI] [PubMed] [Google Scholar]
- 35.Newton PO, Mubarak SJ. Financial aspects of femoral shaft fracture treatment in children and adolescents. J Pediatr Orthop. 1994;14(4):508–512. doi: 10.1097/01241398-199407000-00017. [DOI] [PubMed] [Google Scholar]
- 36.Cadman EF, Neer CS., 2nd Treatment of fractures of the femoral shaft in children. J Am Med Assoc. 1957;163(8):634–637. doi: 10.1001/jama.1957.02970430024008. [DOI] [PubMed] [Google Scholar]
- 37.Buford D, Jr, Christensen K, Weatherall P. Intramedullary nailing of femoral fractures in adolescents. Clin Orthop Relat Res. 1998;350:85–89. [PubMed] [Google Scholar]
- 38.Flynn JM, Luedtke L, Ganley TJ, Pill SG. Titanium elastic nails for pediatric femur fractures: lessons from the learning curve. Am J Orthop. 2002;31(2):71–74. [PubMed] [Google Scholar]