

Abstract
Background
Immediate defibrillation is the traditional approach to resuscitation of cardiac arrest due to ventricular fibrillation or tachycardia (VF/VT). Delaying defibrillation to provide chest compressions may improve survival. We examined the effect of the duration of Emergency Medical Services (EMS) cardiopulmonary resuscitation (CPR) prior to first defibrillation on survival in patients with out-of-hospital VF/VT.
Materials and Methods
From a prospective multi-center observational registry of EMS-treated out-of-hospital cardiac arrest, we identified 1,638 EMS-treated cardiac arrests with first recorded rhythm VF/VT or “shockable” and complete data for analysis. Survival to hospital discharge was determined as a function of EMS CPR duration prior to first shock.
Results
Compared to the reference group of first EMS CPR duration ≤ 45 seconds, the odds of survival was greater among patients who received between 46 seconds to 195 seconds of EMS CPR before first shock (46 to 75 seconds odds ratio [OR] 1.15, 95% confidence interval [CI] 0.71-1.87; 76 to 105 seconds, OR 1.37, 95% CI 0.80-2.35; 106 to 135 seconds, OR 1.53, 95% CI 0.96-2.45; 136 to 165 seconds, OR 1.24, 95% CI 0.71-2.15; 166 to 195 seconds, OR 1.47, 95% CI 0.85-2.52). The benefit of EMS CPR before defibrillation was reduced when the duration of CPR exceeded 195 seconds (196 to 225 seconds, OR 0.95, 95% CI 0.47-1.81; 226 to 255 seconds, OR 0.91, 95% CI 0.46-1.79; 256 to 285 seconds, OR 0.46, 95% CI 0.17-1.29; 286 to 315 seconds, OR 1.29, 95% CI 0.59-2.85). An optimal EMS CPR duration was not identified and no duration achieved statistical significance.
Conclusion
In this observational analysis of VF/VT arrest, between 46 and 195 seconds of EMS CPR prior to defibrillation was weakly associated with improved survival compared to ≤ 45 seconds. Randomized trials are needed to confirm the optimal duration of EMS CPR prior to defibrillation and to assess the impact of first CPR duration on all initial rhythms.
Keywords: Cardiopulmonary resuscitation, heart arrest, defibrillation, registries, survival
Introduction
Treatment of out-of-hospital cardiac arrest (OHCA) due to ventricular tachycardia or ventricular fibrillation (VF/VT) has traditionally included defibrillation at the earliest opportunity.1-3 Use of automatic external defibrillators by first-responders has reduced the time to defibrillation, but the anticipated improvement in survival has not been observed.4-6 Delaying defibrillation to provide a period of cardiopulmonary resuscitation (CPR) may improve survival compared to immediate defibrillation by limiting end-organ ischemia, metabolically preparing the heart for defibrillation, and reducing reperfusion injury.7-10 Previous studies have provided conflicting results concerning the potential benefit of EMS CPR before defibrillation for OHCA.5, 11-13 Within Resuscitation Outcomes Consortium (ROC) Epistry – Cardiac Arrest, we evaluated the effect of the duration of EMS CPR prior to the first defibrillation on survival in patients with out-of-hospital VF/VT.
Methods
Design and Setting
The ROC Epistry – Cardiac Arrest is a prospective multicenter observational registry of OHCA in EMS agencies and receiving institutions in eight U.S. sites and three Canadian sites participating in the ROC clinical research network. Details of the ROC Epistry – Cardiac Arrest data management and quality assurance mechanisms have been described previously.14, 15
Patient Population
The study cohort was drawn from all OHCA cases occurring within the catchment area of a participating EMS agency from December 1, 2005 to May 31, 2007. Included were non-traumatic cardiac arrests occurring outside the hospital that were evaluated by EMS and received lay or EMS external defibrillation or chest compressions from EMS personnel. Included cases had a first recorded rhythm of VF or VT by manual defibrillator or “shockable” if initially treated with an automated external defibrillator. We excluded patients with missing data on EMS CPR duration prior to defibrillation, on survival to hospital discharge, or in covariates that were included in the adjusted analysis. We excluded OHCA witnessed by EMS personnel. We also excluded patients with a first EMS CPR duration of > 315 seconds before the first shock as these likely represented unexpected resuscitation circumstances that could not be adequately accounted for in the analysis. Two ROC sites that self-reported incomplete case capture (San Diego, CA and Dallas, TX) were excluded from all analyses.
Exposure and Outcome Variables
First EMS CPR duration was calculated from the time chest compressions were initiated by EMS to time of first defibrillation. CPR times were determined from EMS responder documentation. When available, synchronized defibrillator time stamps were used to identify the time of first shock. The primary outcome variable was survival to hospital discharge. Patients transferred to a non-acute care facility or non-acute ward were considered discharged. Patients transferred to another acute care facility were considered to be still hospitalized.
Statistical analysis
Baseline patient characteristics and EMS-response variables are reported with descriptive summary statistics. Multiple logistic regression evaluated survival to hospital discharge as a function of first EMS CPR duration in our main-effects model. The duration of first EMS CPR was grouped into centered on 30 second intervals from the initiation of EMS CPR and modeled as indicator variables. This allowed for non-linear associations between EMS CPR duration and survival to be represented by the model. In centering duration of EMS CPR, we chose to collapse the interval from 0 to 15 seconds with the interval from 16 to 45 seconds because of expected imprecision in EMS CPR duration and to allow adequate sample size in the referent group. All subsequent intervals were 30 seconds in length. All variables included for adjustment in our models were determined a priori. The adjusted model included covariates for age as a continuous variable, sex, public location, bystander witnessed, bystander CPR, time from call receipt to first EMS unit arrival dichotomized as arrival before or after 5-minutes, and study site. A random effects model with adjustment for covariates as above was undertaken to account for clustering of data within ROC sites and estimate the association of first EMS CPR duration and survival at an average site. In addition to our main-effects model, we performed post-hoc analyses stratified on bystander witnessed status, time to first EMS unit < 5 minutes, and receipt of bystander CPR to explore differences in the effect of EMS CPR prior to defibrillation related to duration of cardiac arrest or bystander CPR.
Analyses were conducted with S-PLUS, version 6.2 (Insightful Corporation, Seattle, WA), STATA, version 8.0 (StataCorp, College Station, TX), and R version 2.1.1 (R Foundation for Statistical Computing, Vienna, Austria). All hypotheses were evaluated at a two-sided significance level of 0.05, with calculation of 95% confidence intervals.
Results
There were 13,601 cases of EMS-treated non-traumatic OHCA during the study period. An initial rhythm of VF/VT/shockable was reported in 3,292 (24%). Of patients with VF/VT/shockable, we excluded 1,304 (40%) with missing duration of EMS CPR or vital status at discharge, 26 (0.7%) with missing covariates for adjustment in the regression model, 143 (4%) EMS witnessed arrests, and 184 (6%) with a first EMS CPR duration of > 315 seconds (Figure 1). This resulted in 1,638 cases of OHCA with an initial rhythm of VF/VT/shockable and complete data available for analysis.
Figure 1. Study Cohort.

The baseline patient and EMS-response characteristics are shown in Table 1. Within the VF/VT initial rhythm analysis cohort, the mean age was 63.9±15.4 years, 356 (22%) were women, 1133 (69%) were bystander witnessed, and 807 (49%) received bystander CPR. The median time from call to first EMS unit arrival was 5:28 (IQR 4:10-6:47) within the analysis cohort of VF/VT initial rhythm. Of the 10 ROC sites contributing cases to the analysis cohort, 95% of the cases were contributed from 7 ROC sites (range 0.37% to 27.48%).
Table 1. Baseline Patient and EMS-Response Characteristics.
| EMS-Treated Cardiac Arrest n=13,601 |
VF/VT* Initial Rhythm n=3,292 |
VF/VT* Analysis Set n=1,638 |
|
|---|---|---|---|
| Age, Mean (SD) | 64.4 (19.6) | 64 (15.7) | 63.9 (15.4) |
| (min-max) | (0-106) | (0-101) | (0.1-100) |
| Female, No. (%) | 4891 (36) | 770 (23) | 356 (22) |
| Location of arrest, No. (%) | |||
| Home/non-public | 9911 (73) | 2119 (64) | 1049 (64) |
| Public | 2199 (16) | 986 (30) | 506 (31) |
| Health care setting | 1475 (11) | 183 (6) | 83 (5) |
| Bystander witnessed, No. (%) | 5335 (39) | 2002 (61) | 1133 (69) |
| Bystander CPR performed, No. (%) | 4545 (33) | 1376 (42) | 807 (49) |
| Time from call to first EMS unit arrival, min Median (IQR) | 5:20 (4:00-7:00) | 5:10 (4:00-6:45) | 5:28 (4:10-6:47) |
The baseline patient and EMS-response characteristics by duration of first EMS CPR interval are shown in Table 2. Overall, there was little variation in the mean age or the proportion that were women, bystander witnessed, or received bystander CPR over time intervals of EMS CPR. The time from call to first EMS unit arrival was longer among patients with a longer duration of first EMS CPR interval (p = 0.01).
Table 2. Baseline Patient Demographics and EMS-Response Characteristics by Duration of EMS CPR Prior to First Defibrillation.
| Initial CPR Duration (seconds) | ≤ 45 n=210 |
46-75 n=277 |
76-105 n=158 |
106-135 n=308 |
136-165 n=203 |
166-195 n=173 |
196-225 n=93 |
226-255 n=105 |
256-285 n=51 |
286-315 n=60 |
p-value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, Mean (SD) | 64.2 (14.7) | 63.2 (15.2) | 64.2 (16.0) | 64.4 (15.6) | 61.8 (14.5) | 65.5 (14.7) | 63.3 (16.4) | 66.1 (16.9) | 61.4 (16.6) | 64.9 (19.0) | 0.34 |
| Female, No. (%) | 56 (27) | 55 (20) | 23 (15) | 62 (20) | 55 (27) | 37 (21) | 21 (23) | 20 (19) | 9 (18) | 17 (28) | 0.07 |
| Location of arrest, No. (%) | |||||||||||
| Home/non-public | 141 (67) | 174 (63) | 91 (58) | 210 (68) | 124 (61) | 105 (61) | 66 (71) | 66 (63) | 30 (59) | 41 (68) | |
| Public | 55 (26) | 90 (32) | 59 (37) | 87 (28) | 68 (33) | 58 (34) | 24 (26) | 35 (33) | 14 (27) | 16 (27) | 0.59 |
| Health care setting | 14 (7) | 13 (5) | 8 (5) | 11 (4) | 11 (5) | 10 (6) | 3 (3) | 4 (4) | 7 (14) | 2 (3) | |
| Bystander witnessed, No. (%) | 142 (68) | 198 (71) | 110 (70) | 217 (70) | 139 (68) | 121 (70) | 61 (66) | 72 (69) | 32 (63) | 41(68) | 0.98 |
| Bystander CPR performed, No. (%) | 106 (50) | 152 (55) | 72 (46) | 137 (44) | 107 (53) | 87 (50) | 47 (51) | 50 (48) | 24 (47) | 24 (40) | 0.37 |
| Time from call to first EMS unit arrival, min Median (IQR) | 5:10 (4:00-7:00) | 5:00 (3:52-6:47) | 5:14 (4:17-6:45) | 5:11 (4:00-6:38) | 5:09 (4:00-6.44) | 5:13 (4:15-6:34) | 5:56 (5:08-7:34) | 5:16 (4:22-6:38) | 5:45 (4:34-6:27) | 5:35 (4:43-7:14) | 0.01 |
The survival of out-of-hospital VF/VT by duration of EMS CPR prior to first defibrillation is shown in Table 3. After adjustment by multiple logistic regression, the odds of survival to discharge were greater among patients who received between 46 seconds and 195 seconds of EMS CPR before defibrillation compared to the reference group of ≤ 45 seconds. Specifically, the odds of survival were nearly 25% greater among patients who received 46 to 75 seconds of EMS CPR (OR 1.15, 95% confidence interval [CI] 0.71-1.87, p = 0.530) and more than 25% greater among patients receiving 76 to 105 seconds (OR 1.37, 95% CI 0.80-2.35, p = 0.239), 106 to 135 seconds (OR 1.53, 95% CI 0.96-2.45, p = 0.068), 136 to 165 seconds (OR 1.24, 95% CI 0.71-2.15, p = 0.421) or 166 to 195 seconds (OR 1.47, 95% CI 0.85-2.52, p = 0.169) of EMS CPR before first shock. The regression analysis suggested a decreasing survival among patients receiving > 195 seconds of EMS CPR prior to first shock compared to the reference group of ≤ 45 seconds of EMS CPR. The random-effects regression model demonstrated the same results. No time interval of EMS CPR reached statistical significance compared to the reference group. In exploratory analyses with first EMS CPR duration collapsed into intervals ≤ 45 seconds, 46-195 seconds, and > 195 seconds, survival was similar to that observed in regressions with first EMS CPR modeled more continuously. These results were further explored using an unadjusted restricted cubic spline analysis (Figure 2).16 This analysis was found to be statistically significant (p=0.02) and mirrored the trends observed in the main effect and random-effects models.
Table 3. Survival of Out-of-Hospital VF/VT by Duration of EMS CPR Prior to First Defibrillation.
| Initial CPR Duration (seconds) | ≤ 45 | 46-75 | 76-105 | 106-135 | 136-165 | 166-195 | 196-225 | 226-255 | 256-285 | 286-315 |
|---|---|---|---|---|---|---|---|---|---|---|
| Treated, n | 210 | 277 | 158 | 308 | 203 | 173 | 93 | 105 | 51 | 60 |
| Survived to Discharge, % | 17.6 | 23.1 | 24.7 | 23.1 | 26.6 | 21.4 | 15.1 | 15.2 | 9.8 | 18.3 |
| Adjusted OR of Survival in Logistic Regression Model* (95% CI) | Reference | 1.15 (0.71, 1.87) | 1.37 (0.80, 2.35) | 1.53 (0.96, 2.45) | 1.24 (0.71, 2.15) | 1.47 (0.85, 2.52) | 0.95 (0.47, 1.81) | 0.91 (0.46, 1.79) | 0.46 (0.17, 1.29) | 1.29 (0.59, 2.85) |
| Adjusted OR of Survival in Random-Effects Model* (95% CI) | Reference | 1.19 (0.73, 1.92) | 1.43 (0.81, 2.47) | 1.54 (0.97, 2.49) | 1.34 (0.77, 2.33) | 1.47 (0.85, 2.52) | 0.98 (0.48, 2.02) | 0.93 (0.46, 1.83) | 0.47 (0.17, 1.35) | 1.30 (0.59, 2.90) |
Adjusted for age, sex, public location, witnessed arrest, bystander CPR, time to first EMS unit, and study site.
Figure 2. Restricted Smoothed Splines Curve by Duration of EMS CPR Prior to First Defibrillation.
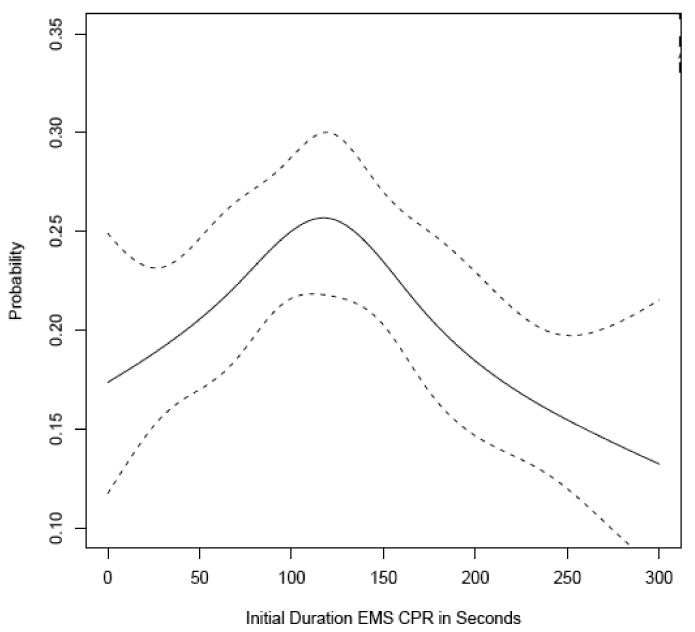
Best fit curve of probability of survival against initial duration of EMS CPR as modeled by smoothed splines with five knots auto-selected at restricted quintiles of CPR duration.
Our regression analyses were designed to account for site effects that contribute to differences in survival. In sensitivity analysis, we excluded sites with known CPR duration protocols to further ensure the influence of site did not account for our results. Exclusion of these sites did not change the results of our analysis.
The results of analyses stratified on the EMS-response time, bystander witnessed status, and receipt of bystander CPR are shown in Table 4. The evidence of increased survival with between 46 and 195 seconds of EMS CPR compared to the reference group of ≤ 45 seconds was most pronounced in patients with time to first EMS unit arrival > 5 minutes or witnessed OHCA. Among patients with time to first EMS unit > 5 minutes, between 46 and 195 seconds of EMS CPR was associated with > 40% increased odds of survival compared to the reference group for most EMS CPR time intervals in that range. In episodes of bystander witnessed OHCA, there was a >50% increased odds of survival among patients receiving between 46 and 195 seconds of EMS CPR compared to the reference group for most of EMS CPR time intervals in that range. Comparatively, in patients with time to first EMS unit ≤ 5 minutes, there was little evidence for increased survival with 46 to 195 seconds of EMS CPR. Among non-witnessed OHCA, there was no evidence of survival benefit with more than 45 seconds of EMS CPR. Survival after stratification on receipt of bystander CPR was very similar to the main-effects model. Regardless of whether CPR was performed prior to EMS arrival, between 46 and 195 seconds of EMS CPR was associated with a greater than 20% increased odds of survival compared to the reference group for most of the EMS CPR time intervals in that range.
Table 4. Survival of Out-of-Hospital VF/VT by Duration of EMS CPR Prior to First Defibrillation versus Key Patient and EMS-Response Characteristics.
| Initial CPR Duration (seconds) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient and EMS Characteristics | ≤ 45 | 46-75 | 76-105 | 106-135 | 136-165 | 166-195 | 196-225 | 226-255 | 256-285 | 286-315 | |
| Time to EMS ≤ 5 minutes | Treated, n | 99 | 140 | 73 | 143 | 94 | 75 | 22 | 47 | 17 | 19 |
| Survived to Discharge, % | 21.2 | 30.0 | 31.5 | 24.5 | 31.9 | 24.0 | 18.2 | 14.9 | 17.6 | 22.2 | |
| Adjusted OR of Survival* (95% CI) | Reference | 1.17 (0.60, 2.20) | 1.27 (0.60, 2.30) | 1.11 (0.59, 2.15) | 1.17 (0.53, 2.70) | 1.14 (0.54, 2.45) | 0.74 (0.21, 2.55) | 0.64 (0.24, 1.70) | 0.75 (0.19, 3.10) | 0.84 (0.23, 3.15) | |
| Time to EMS > 5 minutes | Treated, n | 111 | 137 | 85 | 165 | 109 | 98 | 71 | 58 | 34 | 41 |
| Survived to Discharge, % | 14.4 | 16.1 | 18.8 | 21.8 | 22.0 | 19.4 | 14.1 | 15.5 | 5.9 | 17.1 | |
| Adjusted OR of Survival* (95% CI) | Reference | 1.11 (0.53, 2.33) | 1.61 (0.69, 3.50) | 2.24 (1.10, 4.49) | 1.39 (0.60, 3.00) | 1.83 (0.83, 3.99) | 0.98 (0.38, 2.49) | 1.24 (0.48, 3.16) | 0.30 (0.06, 1.44) | 1.80 (0.60, 5.10) | |
| Bystander Witnessed Arrest | Treated, n | 142 | 198 | 110 | 217 | 139 | 121 | 61 | 72 | 32 | 41 |
| Survived to Discharge, % | 19.7 | 28.8 | 30.9 | 27.2 | 34.5 | 24.0 | 16.4 | 19.4 | 9.4 | 19.5 | |
| Adjusted OR of Survival* (95% CI) | Reference | 1.43 (0.83, 2.47) | 1.68 (0.94, 3.10) | 1.69 (0.97, 2.90) | 1.74 (0.93, 3.26) | 1.51 (0.80, 2.82) | 0.93 (0.40, 2.16) | 1.10 (0.51, 2.35) | 0.37 (0.10, 1.36) | 1.37 (0.54, 3.49) | |
| Unwitnessed Arrest | Treated, n | 68 | 79 | 48 | 91 | 64 | 52 | 32 | 33 | 19 | 19 |
| Survived to Discharge, % | 13.2 | 8.9 | 10.4 | 13.2 | 9.4 | 15.4 | 12.5 | 6.1 | 10.5 | 16.7 | |
| Adjusted OR of Survival* (95% CI) | Reference | 0.45 (0.15, 1.33) | 0.56 (0.17, 1.96) | 1.18 (0.43, 3.21) | 0.28 (0.07, 1.08) | 1.08 (0.35, 3.25) | 0.70 (0.18, 2.69) | 0.40 (0.08, 2.08) | 0.70 (0.13, 3.78) | 1.03 (0.21, 4.79) | |
| Bystander CPR | Treated, n | 106 | 152 | 72 | 137 | 107 | 87 | 47 | 50 | 24 | 24 |
| Survived to Discharge, % | 19.8 | 28.9 | 33.3 | 27.7 | 22.4 | 25.3 | 21.3 | 18.0 | 16.7 | 16.7 | |
| Adjusted OR of Survival* (95% CI) | Reference | 1.30 (0.69, 2.46) | 1.51 (0.72, 3.17) | 1.69 (0.88, 3.26) | 0.71 (0.32, 1.56) | 1.46 (0.70, 3.07) | 1.07 (0.43, 2.66) | 0.92 (0.36, 2.37) | 0.88 (0.25, 3.13) | 1.35 (0.40, 4.60) | |
| No CPR Prior to EMS Arrival | Treated, n | 104 | 125 | 86 | 171 | 96 | 86 | 46 | 55 | 27 | 36 |
| Survived to Discharge, % | 15.4 | 16.0 | 17.4 | 19.3 | 31.3 | 17.4 | 8.7 | 12.7 | 3.7 | 20.0 | |
| Adjusted OR of Survival* (95% CI) | Reference | 1.00 (0.46, 2.14) | 1.22 (0.53, 2.80) | 1.32 (0.65, 2.65) | 2.16 (0.96, 4.84) | 1.53 (0.67, 3.48) | 0.72 (0.22, 2.39) | 0.90 (0.33, 2.50) | 0.18 (0.02, 1.50) | 1.50 (0.50, 4.38) | |
Adjusted for age, sex, public location, witnessed arrest, bystander CPR, time to first EMS unit, and study site.
Discussion
Within this prospective multi-center observational cohort of VF/VT out-of-hospital cardiac arrest, between 46 and 195 seconds of EMS CPR before defibrillation was weakly associated with improved survival compared to ≤ 45 seconds of EMS CPR. The association between increased survival and 46 to 195 seconds of EMS CPR was more pronounced among patients with a longer time to first EMS unit arrival and witnessed OHCA. Among patients with unwitnessed OHCA or a short time to EMS unit arrival, there was no clear evidence of survival benefit with more than 45 seconds of first EMS CPR, but a consistent trend toward decreasing survival with more than 195 seconds of EMS CPR. Receipt of bystander CPR did not affect the association between first EMS CPR duration and survival seen in the main-effects model.
The potential benefit of CPR before defibrillation was first suggested from animal models.17-20 In the study by Yakaitis et al. the benefit of CPR before defibrillation was only observed when VF duration exceeded 5 minutes. In human studies, the duration of cardiac arrest has been approximated by the time to first EMS unit arrival. In the study by Cobb, EMS CPR prior to defibrillation improved survival when compared to historical controls, particularly among patients with time to first EMS greater than 4 minutes.5 Within the randomized trial of Wik, delaying defibrillation to provide EMS CPR resulted in greater survival when time to first EMS unit was more than 5 minutes.11 In our cohort, the time to first EMS unit was greater than 5 minutes for 55% of individuals. The results of our main-effects model thus reflect a weighted average of the effect of EMS CPR prior to defibrillation among patients with both short and long times to EMS arrival. When stratified on time to first EMS unit arrival, a more pronounced survival benefit was associated with 46 to 195 seconds of EMS CPR prior to defibrillation when time to EMS unit arrival was greater than 5 minutes. These results are consistent with the findings of Cobb and Wik.
Unwitnessed cardiac arrests would presumably have a longer arrest duration given the delay in recognition of the event. Surprisingly, in our analyses stratified on bystander witnessed status, EMS CPR prior to defibrillation was not associated with a survival benefit among unwitnessed arrests. Given the delay in recognition of OHCA in unwitnessed arrest, it is possible that a greater proportion of these patients entered the metabolic phase of the three phase model of cardiac arrest.21 As opposed to the circulatory phase of cardiac arrest where EMS CPR may mechanically prime the heart and condition the body for reperfusion, EMS CPR prior to defibrillation may provide no benefit or even accelerate the injury cascade of reperfusion among patients who have entered the metabolic phase. Recent work demonstrated remarkable survival with controlled reperfusion in a pig model of 15 minutes of ventricular fibrillation. This benefit was negated by the provision of CPR immediately prior to the initiation of reperfusion (Allen BS, unpublished data, presented at AHA Resuscitation Science Symposium, November 8, 2008). This may also explain the negative findings of Jacobs et al. and Baker et al. in their randomized trials of EMS CPR prior to defibrillation.12, 13 In these studies, the proportion of witnessed arrests was smaller than in the study by Wik and the mean time to first EMS unit was longer than that reported in the study by Cobb. As a result, a greater proportion of patients in the negative studies may have entered the metabolic phase of cardiac arrest compared to the positive studies. Further study of the interactions between arrest duration, CPR, and reperfusion are necessary to identify the most appropriate initial therapy for out-of-hospital cardiac arrest.
Survival of OHCA is strongly influenced by bystander provision of CPR prior to EMS arrival,22-24 however the time to initiation and quality of bystander CPR varies greatly and is independently associated with survival.25, 26 As a result, a homogenous effect of bystander CPR on the association between first EMS CPR duration and survival is unlikely. This may explain the lack of influence of bystander CPR on the duration of EMS CPR associated with improved survival in our analysis. It remains plausible that high quality bystander CPR initiated immediately after arrest may reduce or eliminate the period of CPR provided by EMS necessary to improve the effect of defibrillation. Ongoing work to define the optimum timing of defibrillation according to characteristics of the VF waveform may be helpful in determining the effect of the combination of bystander and professional CPR and determine the best timing of defibrillation.27
Previous studies have evaluated 90 seconds or 180 seconds of EMS CPR prior to defibrillation.5, 11-13 The size of our cohort allowed for evaluation of a continuum of EMS CPR duration. Aside from suggesting between 46 and 195 seconds of EMS CPR prior to defibrillation is associated with improved survival, we did not observe an optimal duration within this range. In post-hoc secondary analyses with EMS CPR time intervals collapsed to create larger comparator groups and identify time intervals associated with greatest survival benefit, similar qualitative results for the effect of EMS CPR time on survival were observed (details available from authors). This agrees with results from a recent swine model of VF, where no difference in survival was noted when animals received 90, 180, or 300 seconds of CPR prior to defibrillation.28
Our findings are also consistent with the observations from studies of resuscitation with minimally interrupted chest compressions by EMS responders, also known as cardiocerebral resuscitation. In these studies, OHCA survival improved after EMS protocols were changed to incorporate 200 chest compressions at a rate of 100 compressions per minute before defibrillation, single shock defibrillation followed immediately by chest compressions, elimination of post-shock rhythm and pulse checks, and delaying intubation to emphasize chest compressions.29-32 Although the improvements in survival in these studies cannot be attributed to any single component of the resuscitation protocol change, the duration of EMS CPR associated with greatest survival in our analysis is similar to the duration of chest compressions provided in these studies.
Our study has several strengths. In addition to the overall size of our cohort, our study incorporated data from multiple sites and EMS agencies evaluating OHCA. Additionally, the study was conducted during a period in which high-quality CPR was emphasized by resuscitation guidelines and by agreement within the ROC agencies to promote quality CPR as a pre-requisite to cardiac arrest clinical trials.33 Finally, we designed our analysis to account for site effects because of the known variation in survival between participating ROC sites.15 The observed associations persisted even after exclusion of sites with known protocols for initial EMS CPR duration.
This study has several limitations. In this observational cohort, duration of CPR was determined by the EMS provider. We cannot exclude the possibility of unmeasured variables that guided EMS in the choice of CPR interval prior to defibrillation. Second, resuscitation process such as minimizing interruptions in chest compressions, avoidance of excessive ventilation, and prognostic factors such as gasping are increasingly understood to influence survival.33-36 Although we were unable to account for these factors in our analysis, we do not suspect they were differentially associated with initial duration of EMS CPR. This is further suggested by our sensitivity analysis in which exclusion of sites with established EMS CPR protocols did not influence our results. Third, our study is complicated by the challenge of obtaining accurate times for therapies provided during OHCA. The similar effect size observed over a range of EMS CPR durations suggests misclassification of EMS CPR duration should not dramatically impact our findings. Fourth, we were unable to account for the effect of post-resuscitation care on outcomes after out-of-hospital cardiac arrest due to lack of patient specific data about in-hospital processes of care. Fifth, our study is also limited by the exclusion of 40% of patients with initial rhythm of VF/VT due to missing EMS CPR duration or vital status at discharge. As a result, the analysis cohort may differ from the entire population of patients with VF/VT. Finally, our findings are limited to patients with VF/VT as the initial rhythm in out-of-hospital cardiac arrest. Ultimately, randomized controlled trials are necessary and currently underway to determine the impact of EMS CPR prior to defibrillation in all initial rhythms.37
Conclusion
In this observational study of OHCA due to VF/VT, delaying defibrillation to provide up to 195 seconds of EMS CPR was weakly associated with improved survival of VF/VT arrest. The strength of this association was more robust among patients with time to first EMS unit arrival of > 5 minutes. Randomized trials are needed to evaluate this association and to assess the impact of EMS CPR before defibrillation in rhythms other than VF/VT.
Acknowledgments
Sources of Funding
The ROC is supported by a series of cooperative agreements to 10 regional clinical centers and one Data Coordinating Center (5U01 HL077863, HL077881, HL077871 HL077872, HL077866, HL077908, HL077867, HL077885, HL077887, HL077873, HL077865) from the National Heart, Lung and Blood Institute in partnership with the National Institute of Neurological Disorders and Stroke, U.S. Army Medical Research & Material Command, The Canadian Institutes of Health Research (CIHR) - Institute of Circulatory and Respiratory Health, Defence Research and Development Canada, the American Heart Association and the Heart and Stroke Foundation of Canada.
Footnotes
Disclosures
Tom Aufderheide reported that he is a member of the American Heart Association BLS Subcommittee; has received research grants from the National Institutes of Health (NIH); and has served as a consultant for Take Heart America, JoLife, and Medtronic. Graham Nichol reported that he is a member of the American Heart Association ACLS Subcommittee and the Medic One Foundation Board of Directors; has received research grants from the NIH; has received equipment donations to support overseas medical missions from the Asmund S. Laerdal Foundation for Acute Medicine, Laerdal Inc., and Medtronic Physio-Control Inc.; has received travel expenses payments from INNERcool Inc. and Radiant Inc., and has served as a consultant to Northfield Laboratories Inc. and Paracor Medical Inc. No other disclosures were reported.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Weaver WD, Hill D, Fahrenbruch CE, Copass MK, Martin JS, Cobb LA, Hallstrom AP. Use of the automatic external defibrillator in the management of out-of-hospital cardiac arrest. N Engl J Med. 1988;319:661–666. doi: 10.1056/NEJM198809153191101. [DOI] [PubMed] [Google Scholar]
- 2.Weaver WD, Cobb LA, Hallstrom AP, Fahrenbruch C, Copass MK, Ray R. Factors influencing survival after out-of-hospital cardiac arrest. J Am Coll Cardiol. 1986;7:752–757. doi: 10.1016/s0735-1097(86)80332-1. [DOI] [PubMed] [Google Scholar]
- 3.White RD, Hankins DG, Bugliosi TF. Seven years' experience with early defibrillation by police and paramedics in an emergency medical services system. Resuscitation. 1998;39:145–151. doi: 10.1016/s0300-9572(98)00135-x. [DOI] [PubMed] [Google Scholar]
- 4.Kellermann AL, Hackman BB, Somes G, Kreth TK, Nail L, Dobyns P. Impact of first-responder defibrillation in an urban emergency medical services system. JAMA. 1993;270:1708–1713. doi: 10.1001/jama.270.14.1708. [DOI] [PubMed] [Google Scholar]
- 5.Cobb LA, Fahrenbruch CE, Walsh TR, Copass MK, Olsufka M, Breskin M, Hallstrom AP. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out-of-hospital ventricular fibrillation. JAMA. 1999;281:1182–1188. doi: 10.1001/jama.281.13.1182. [DOI] [PubMed] [Google Scholar]
- 6.van Alem AP, Vrenken RH, de Vos R, Tijssen JG, Koster RW. Use of automated external defibrillator by first responders in out of hospital cardiac arrest: prospective controlled trial. BMJ. 2003;327:1312. doi: 10.1136/bmj.327.7427.1312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chandra NC. Mechanisms of blood flow during CPR. Ann Emerg Med. 1993;22:281–288. [PubMed] [Google Scholar]
- 8.Steen S, Liao Q, Pierre L, Paskevicius A, Sjoberg T. The critical importance of minimal delay between chest compressions and subsequent defibrillation: a haemodynamic explanation. Resuscitation. 2003;58:249–258. doi: 10.1016/s0300-9572(03)00265-x. [DOI] [PubMed] [Google Scholar]
- 9.Rea TD, Cook AJ, Hallstrom A. CPR during ischemia and reperfusion: a model for survival benefits. Resuscitation. 2008;77:6–9. doi: 10.1016/j.resuscitation.2007.10.010. [DOI] [PubMed] [Google Scholar]
- 10.Chamberlain D, Frenneaux M, Fletcher D. The primacy of basics in advanced life support. Curr Opin Crit Care. 2009;15:198–202. doi: 10.1097/MCC.0b013e3283293138. [DOI] [PubMed] [Google Scholar]
- 11.Wik L, Hansen TB, Fylling F, Steen T, Vaagenes P, Auestad BH, Steen PA. Delaying defibrillation to give basic cardiopulmonary resuscitation to patients with out-of-hospital ventricular fibrillation: a randomized trial. JAMA. 2003;289:1389–1395. doi: 10.1001/jama.289.11.1389. [DOI] [PubMed] [Google Scholar]
- 12.Jacobs IG, Finn JC, Oxer HF, Jelinek GA. CPR before defibrillation in out-of-hospital cardiac arrest: a randomized trial. Emerg Med Australas. 2005;17:39–45. doi: 10.1111/j.1742-6723.2005.00694.x. [DOI] [PubMed] [Google Scholar]
- 13.Baker PW, Conway J, Cotton C, Ashby DT, Smyth J, Woodman RJ, Grantham H, Clinical Investigators Defibrillation or cardiopulmonary resuscitation first for patients with out-of-hospital cardiac arrests found by paramedics to be in ventricular fibrillation? A randomised control trial. Resuscitation. 2008;79:424–431. doi: 10.1016/j.resuscitation.2008.07.017. [DOI] [PubMed] [Google Scholar]
- 14.Morrison LJ, Nichol G, Rea TD, Christenson J, Callaway CW, Stephens S, Pirrallo RG, Atkins DL, Davis DP, Idris AH, Newgard C, ROC Investigators Rationale, development and implementation of the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest. Resuscitation. 2008;78:161–169. doi: 10.1016/j.resuscitation.2008.02.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nichol G, Thomas E, Callaway CW, Hedges J, Powell JL, Aufderheide TP, Rea T, Lowe R, Brown T, Dreyer J, Davis D, Idris A, Stiell I, Resuscitation Outcomes Consortium Investigators Regional variation in out-of-hospital cardiac arrest incidence and outcome. JAMA. 2008;300:1423–1431. doi: 10.1001/jama.300.12.1423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Harrell FE, Jr, et al. Hmisc: Harrell Miscellaneous. [2/1, 2009]; Available at: http://biostat.mc.vanderbilt.edu/s/Hmisc.
- 17.Yakaitis RW, Ewy GA, Otto CW, Taren DL, Moon TE. Influence of time and therapy on ventricular defibrillation in dogs. Crit Care Med. 1980;8:157–163. doi: 10.1097/00003246-198003000-00014. [DOI] [PubMed] [Google Scholar]
- 18.Niemann JT, Cairns CB, Sharma J, Lewis RJ. Treatment of prolonged ventricular fibrillation. Immediate countershock versus high-dose epinephrine and CPR preceding countershock. Circulation. 1992;85:281–287. doi: 10.1161/01.cir.85.1.281. [DOI] [PubMed] [Google Scholar]
- 19.Menegazzi JJ, Davis EA, Yealy DM, Molner RL, Nicklas KA, Hosack GM, Honingford EA, Klain MM. An experimental algorithm versus standard advanced cardiac life support in a swine model of out-of-hospital cardiac arrest. Ann Emerg Med. 1993;22:235–239. doi: 10.1016/s0196-0644(05)80211-2. [DOI] [PubMed] [Google Scholar]
- 20.Berg RA, Hilwig RW, Ewy GA, Kern KB. Precountershock cardiopulmonary resuscitation improves initial response to defibrillation from prolonged ventricular fibrillation: a randomized, controlled swine study. Crit Care Med. 2004;32:1352–1357. doi: 10.1097/01.ccm.0000127780.01362.e5. [DOI] [PubMed] [Google Scholar]
- 21.Weisfeldt ML, Becker LB. Resuscitation after cardiac arrest: a 3-phase time-sensitive model. JAMA. 2002;288:3035–3038. doi: 10.1001/jama.288.23.3035. [DOI] [PubMed] [Google Scholar]
- 22.Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M, Ontario Prehospital Advanced Life Support Study Group Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656. doi: 10.1056/NEJMoa040325. [DOI] [PubMed] [Google Scholar]
- 23.Swor RA, Boji B, Cynar M, Sadler E, Basse E, Dalbec DL, Grubb W, Jacobson R, Jackson RE, Maher A. Bystander vs EMS first-responder CPR: initial rhythm and outcome in witnessed nonmonitored out-of-hospital cardiac arrest. Acad Emerg Med. 1995;2:494–498. doi: 10.1111/j.1553-2712.1995.tb03246.x. [DOI] [PubMed] [Google Scholar]
- 24.Van Hoeyweghen RJ, Bossaert LL, Mullie A, Calle P, Martens P, Buylaert WA, Delooz H. Quality and efficiency of bystander CPR. Belgian Cerebral Resuscitation Study Group. Resuscitation. 1993;26:47–52. doi: 10.1016/0300-9572(93)90162-j. [DOI] [PubMed] [Google Scholar]
- 25.Cummins RO, Ornato JP, Thies WH, Pepe PE. Improving survival from sudden cardiac arrest: the “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation. 1991;83:1832–1847. doi: 10.1161/01.cir.83.5.1832. [DOI] [PubMed] [Google Scholar]
- 26.Gallagher EJ, Lombardi G, Gennis P. Effectiveness of bystander cardiopulmonary resuscitation and survival following out-of-hospital cardiac arrest. JAMA. 1995;274:1922–1925. [PubMed] [Google Scholar]
- 27.Sherman LD, Rea TD, Waters JD, Menegazzi JJ, Callaway CW. Logarithm of the absolute correlations of the ECG waveform estimates duration of ventricular fibrillation and predicts successful defibrillation. Resuscitation. 2008;78:346–354. doi: 10.1016/j.resuscitation.2008.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rittenberger JC, Suffoletto B, Salcido D, Logue E, Menegazzi JJ. Increasing CPR duration prior to first defibrillation does not improve return of spontaneous circulation or survival in a swine model of prolonged ventricular fibrillation. Resuscitation. 2008;79:155–160. doi: 10.1016/j.resuscitation.2008.04.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kellum MJ, Kennedy KW, Ewy GA. Cardiocerebral resuscitation improves survival of patients with out-of-hospital cardiac arrest. Am J Med. 2006;119:335–340. doi: 10.1016/j.amjmed.2005.11.014. [DOI] [PubMed] [Google Scholar]
- 30.Kellum MJ, Kennedy KW, Barney R, Keilhauer FA, Bellino M, Zuercher M, Ewy GA. Cardiocerebral resuscitation improves neurologically intact survival of patients with out-of-hospital cardiac arrest. Ann Emerg Med. 2008;52:244–252. doi: 10.1016/j.annemergmed.2008.02.006. [DOI] [PubMed] [Google Scholar]
- 31.Garza AG, Gratton MC, Salomone JA, Lindholm D, McElroy J, Archer R. Improved patient survival using a modified resuscitation protocol for out-of-hospital cardiac arrest. Circulation. 2009;119:2597–2605. doi: 10.1161/CIRCULATIONAHA.108.815621. [DOI] [PubMed] [Google Scholar]
- 32.Bobrow BJ, Clark LL, Ewy GA, Chikani V, Sanders AB, Berg RA, Richman PB, Kern KB. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA. 2008;299:1158–1165. doi: 10.1001/jama.299.10.1158. [DOI] [PubMed] [Google Scholar]
- 33.ECC Committee, Subcommittees and Task Forces of the American Heart Association. Circulation. Vol. 112. 2005. 2005. American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care; pp. IV1–203. [DOI] [PubMed] [Google Scholar]
- 34.Rea TD, Helbock M, Perry S, Garcia M, Cloyd D, Becker L, Eisenberg M. Increasing use of cardiopulmonary resuscitation during out-of-hospital ventricular fibrillation arrest: survival implications of guideline changes. Circulation. 2006;114:2760–2765. doi: 10.1161/CIRCULATIONAHA.106.654715. [DOI] [PubMed] [Google Scholar]
- 35.Aufderheide TP, Sigurdsson G, Pirrallo RG, Yannopoulos D, McKnite S, von Briesen C, Sparks CW, Conrad CJ, Provo TA, Lurie KG. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation. 2004;109:1960–1965. doi: 10.1161/01.CIR.0000126594.79136.61. [DOI] [PubMed] [Google Scholar]
- 36.Bobrow BJ, Zuercher M, Ewy GA, Clark L, Chikani V, Donahue D, Sanders AB, Hilwig RW, Berg RA, Kern KB. Gasping during cardiac arrest in humans is frequent and associated with improved survival. Circulation. 2008;118:2550–2554. doi: 10.1161/CIRCULATIONAHA.108.799940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stiell IG, Callaway C, Davis D, Terndrup T, Powell J, Cook A, Kudenchuk PJ, Daya M, Kerber R, Idris A, Morrison LJ, Aufderheide T, ROC Investigators Resuscitation Outcomes Consortium (ROC) PRIMED cardiac arrest trial methods part 2: rationale and methodology for “Analyze Later vs. Analyze Early” protocol. Resuscitation. 2008;78:186–195. doi: 10.1016/j.resuscitation.2008.01.027. [DOI] [PMC free article] [PubMed] [Google Scholar]