

Abstract
Each day in India, an estimated 5,500 youth initiate tobacco use, contributing to predictions that by 2020, tobacco will account for 13% of all deaths in India. Project MYTRI (Mobilizing Youth for Tobacco-Related Initiatives in India) is a multi-component school-based intervention designed to prevent and reduce tobacco use among adolescents in Delhi and Chennai, India. The intervention was implemented over the 2004-2006 school years and involved 6th and 8th grade students in 32 classrooms. Students participated in peer-led classroom activities involving games, competitions, and other activities intended to target a number of psychosocial risk factors believed to prevent tobacco use among urban Indian youth. To more fully understand how Project MYTRI influenced students' intentions to smoke or chew tobacco, the current study used mediation analysis to investigate whether Project MYTRI altered the psychosocial risk factors as intended, and whether the changes in psychosocial risk factors were, in turn, responsible for altering students' tobacco-use intentions. Multi-level mediation models were estimated using student data from baseline and one-year follow-up surveys. Results indicated that the psychosocial risk factors Knowledge of Health Effects, Normative Beliefs, Reasons to Use Tobacco, and Perceived Prevalence were significant mediators between the intervention activities and students' tobacco use intentions. Evidence of inconsistent mediation was observed for the Perceived Prevalence factor. These findings, combined with those from qualitative research and the second-year student data, will help to illuminate the impact of Project MYTRI on participating youth.
Keywords: mediation analysis, tobacco prevention, adolescents, India, psychosocial risk factors
Introduction
Based on current trends, the World Health Organization predicts that by the year 2020, tobacco use will cause more than 10 million deaths per year (Warren et al. 2008). The majority of tobacco-related deaths are expected to occur in developing countries, where tobacco use is on the rise; in less developed countries, deaths due to tobacco are projected to increase from approximately 1 million in 1990 to 7 million in 2020 (The World Bank 1999; Warren et al. 2008). The climb in tobacco use is particularly evident in India, where tobacco is expected to account for 13.3% of all deaths by 2020 (Stigler et al. 2006). Of particular concern is the increasing number of India's youth who use tobacco. Each day in India, an estimated 5,500 youth start using tobacco either in smoked or smokeless form, and some of these adolescents initiate use as early as age 10 (Mishra et al. 2005; Reddy and Gupta 2004; Reddy et al. 2006; Stigler et al. 2006).
Project MYTRI (Mobilizing Youth for Tobacco-Related Initiatives in India) is a research study that directed the development, implementation, and evaluation of a multi-component school-based intervention designed to prevent and reduce tobacco use by 20% to 30% among adolescents in Delhi and Chennai, India (Perry et al. 2006). Project MYTRI is a collaborative effort between researchers and practitioners in the U.S. and India, and is funded by the Fogarty International Center 2002-2007 as part of a larger initiative to build capacity for conducting tobacco control research worldwide (Reddy et al. 2006).
A translational research process directed the design of the intervention. The intervention model was based on relevant theory (i.e. Social cognitive theory, Social influences model (Bandura 2001; Baranowski et al. 1996; US Department of Health and Human Services 1994), the researchers' prior experience with school-based prevention programs and efficacy trials in the U.S. and India, and tobacco prevention models in the West (Mishra et al. 2005; Perry et al. 2003; Perry et al. 2002, 2006; Reddy et al. 2002; Reddy and Gupta 2004). In addition, findings from audience research with Indian youth helped to identify important cultural and contextual factors relevant to the program design and implementation (Perry et al. 2006). The resultant behavioral model, shown in Figure 1, specified program components, defined the desired outcomes of the intervention, and identified a number of psychosocial risk factors believed to predict tobacco use among urban youth in India (Stigler et al. 2007). As illustrated by the model, a causal relationship was assumed among the intervention components, psychosocial risk factors, and outcomes; the four intervention components were intended to alter the psychosocial risk factors in order to prevent or reduce tobacco use among youth in Delhi and Chennai. Thus, the intrapersonal, social-contextual, and environmental psychosocial risk factors were the “targets” to be altered by the intervention.
Figure 1.

Behavioral intervention model for Project MYTRI
Evaluation of Project MYTRI began in 2004. Thirty-two schools were randomized to receive the intervention (n=16 schools) or serve as a delayed program control (n=16 schools). Students in these schools were surveyed before and immediately after the first year of the program implementation. Initial evaluative findings indicated that, after year one, students in the program had fewer intentions to smoke or chew tobacco in the future than students in the control condition (Stigler et al. 2007). The purpose of this paper is to offer insight into how Project MYTRI achieved these results by identifying which of the psychosocial risk factors were significant links—or mediators—between the program and outcomes. A variable may be considered a mediator if it accounts for the relationship between a treatment and outcome (Judd and Kenny 1981).
Statistical mediation analysis can be used to test the causal relationships among variables by testing the action and conceptual theories (Judd and Kenny 1981; MacKinnon 2008; MacKinnon and Dwyer 1993; MacKinnon and Lockwood 2003; MacKinnon, Lockwood et al. 2002; MacKinnon, Taborga et al. 2002). Action theory involves the process by which a treatment modifies selected mediating variables. The test of the action theory indicates whether an independent variable influenced a mediator variable as theory suggested it would (Chen 1990). Conceptual theory refers to the process that relates theoretical mediators to the outcome variable and is based on information from developmental theories as well as previously observed relations between intervening and outcome variables (MacKinnon, Taborga et al. 2002). The test of the conceptual theory investigates whether a mediator variable influenced a specified dependent variable according to theory (Chen 1990). In this study, mediation analysis was used to examine whether and to what extent the psychosocial risk factors mediated the relationship between intervention components and participants' tobacco-use intentions. In other words, statistical mediation analysis was performed to investigate (a) whether Project MYTRI altered the psychosocial risk factors as intended (action theory), and (b) whether the changes in psychosocial risk factors were, in turn, responsible for altering students' tobacco-use intentions (conceptual theory).
To our knowledge, no mediation analysis of a tobacco-use prevention program in India has previously been published. Findings presented here are valuable for improving and tailoring Project MYTRI and similar programs to enable the interventions to effectively reduce tobacco use among Indian youth. Understanding how the intervention elicited some, yet not all, effects is crucial to the progress of the intervention. Once both strengths and weaknesses are identified, program improvements can be made by bolstering important elements and altering or eliminating ineffectual elements.
Methods
Study Design
Project MYTRI was a two-year group-randomized trial involving students in 32 schools in Delhi and Chennai, India. The intervention was implemented over the 2004-2005 and 2005-2006 school years. This mediation analysis focuses on the first year of the two-year program. In the first year, 125 classrooms participated; 65 were 6th grade classrooms, and 60 were 8th grade classrooms. Participating schools were selected based on their representativeness of the range of schools in Delhi and Chennai in terms of socioeconomic level, school type (Private versus Government), and gender (co-ed, boys only, and girls only) (Mishra et al. 2005; Perry et al. 2006; Reddy et al. 2006). Schools were stratified by city, matched by school type and gender, and randomly assigned to intervention groups (n=16 schools) and delayed-intervention control groups (n=16 schools). Evaluation activities included student surveys, observations, training ratings, tracking documents, and others (Perry et al. 2006). The current study used only the student survey data. Ethical clearances for the trial were obtained from the Independent Ethics Committee in Mumbai, India and the Institutional Review Board in Minneapolis at the University of Minnesota. Informed passive parental consent obtained via a letter and response card was required for student participation.
Student Participants
Two surveys were considered in this mediation analysis: (1) a baseline survey in 2004 prior to program implementation when students were in 6th and 8th grades and (2) a one-year follow-up in 2005 when the original students were in 7th and 9th grade. The sample size of students who completed both the baseline and one-year follow-up surveys was N=8,369. This represented a 31.5% attrition rate for students in the control condition and a 24% attrition rate for students in the intervention group. Of the sample, 4,360 students were in the control condition and 4,009 were in the delayed-intervention condition. Just over half (56.4%) of the students attended Government schools. Students from Government schools were generally from low-to-middle SES backgrounds, while Private school students generally came from middle-to-high SES backgrounds. In the survey sample, 43.5% lived in Delhi (in northern India), and 56.5% lived in Chennai (in southern India). The average age of students in 2004 was 11.0 years for 6th graders and 12.8 years for 8th graders. Gender was evenly represented (51.6% male).
Program Implementation
Implementation of Project MYTRI involved four components, namely classroom sessions, school posters, parent postcards, and peer-led health activism. The first-year curriculum included seven, 70-minute classroom sessions. The curricula were adapted from activities implemented in previous social influence programs, such as the Minnesota Smoking Prevention Program (Perry et al. 1992) and HRIDAY-CATCH (Perry et al. 2006; Reddy et al. 2002). Students in 13 of the 16 intervention schools completed all seven classroom activities; students in 1 school completed four sessions, and students in 2 schools completed two sessions (Stigler et al. 2007). The classroom curricula involved games, competitions, and other activities that were designed to be fun and interactive. Activities were conducted in small groups of 10 to 15 students and were led by student-elected peer leaders who received training prior to classroom sessions. Similar to other social influences-based programs, peer leaders played a key role in the classroom curricula accordant with the belief that peers can effectively transfer knowledge, skills, and strategies to student observers, thus increasing the likelihood of program success (Tobler 1986). Teachers also received prior training and participated in implementing activities. Teachers and peer leaders were provided with instruction manuals and students worked from handbooks. Materials were provided in English, Hindi, or Tamil, depending on the primary language at each school.
The curriculum included knowledge components, skills building, and normative education, and focused on altering the psychosocial risk factors (Perry et al 2006; Stigler et al 2007). The program content addressed numerous forms of tobacco use, including cigarettes, chewing tobacco, and bidis. To complement classroom activities and reinforce student learning, themed posters that corresponded to session topics were hung inside classrooms and elsewhere on school grounds. Postcards with curriculum-related messages were hand delivered by students to parents. In addition, intra- and inter-school activities and competitions were held. In year one, the intervention spanned four months and involved 15 hours of activity (Stigler et al. 2007). More detailed information on the intervention can be found elsewhere (Perry et al. 2006; Stigler et al. 2007).
Measures
The student survey was adapted from the Global Youth Tobacco Survey (GYTS) developed by the WHO (World Health Organization) and the CDC (Centers for Disease Control and Prevention), as well as prior instruments used by the study investigators (Global Youth Tobacco Survey Collaborating Group 2002; Reddy et al. 2006; Warren et al. 2008). The survey was tailored for use by students involved with Project MYTRI based on findings from focus group discussions with 435 students in 6th and 8th grades in six schools in Delhi, India (Mishra et al. 2005). The survey was piloted in Delhi in several Private and Government schools prior to administration. A two-person team conducted the survey, which was self-administered in pencil-and-paper format in English in Private schools, Hindi in Delhi Government schools, and Tamil in Chennai Government schools. To track students over time, a unique ID was assigned to each respondent. The survey consisted of 84 items, 80 of which pertained to tobacco use, intentions to use tobacco, and psychosocial risk factors. The remaining four questions concerned student demographics (e.g., age, gender, grade level) and language characteristics.
Tobacco Use Outcomes
Variables representing current tobacco use and intentions to use tobacco in the future were considered as potential outcome variables. After one year of intervention, significant differences between the study conditions were observed for students' intentions to use tobacco in the future, but not for students' current tobacco use (Stigler et al. 2007). Therefore, “Intentions to chew tobacco” and “Intentions to smoke tobacco” were selected as the two outcome variables for use in the present mediation analyses. Each outcome was measured by a composite of a set of four questions. The four items included (1) Do you think you will try chewing/smoking tobacco in the next month, (2) … in the next year, (3) … when you enter college, and (4) … when you are an adult? The response scale was 1=surely yes, 2=maybe yes, 3=maybe no, and 4=surely no. Two raw scale scores (one for intentions to chew and one for intentions to smoke) were created by adding scores across the four items and subtracting 4 (# of items) so that the possible range of scores was 0 to 12, with a higher score indicating less risk (fewer intentions). Scale scores for the intentions outcome variables, as well as for the psychosocial risk variables, were created in this manner because each of the scales were composed of a different number of items and raw item scores differed in the direction of risk (i.e. for some items, a greater score meant greater risk). By reverse coding particular individual items and subtracting the number of items in a scale from the total scale score, all scales scores had a zero base point and a higher score meant less risk. For a student to receive an “intentions” scale score, he or she had to answer all four items in the scale; otherwise, the student had a missing “intentions” scale score. Separate scale scores were computed for the baseline and one-year follow up for both intentions to chew and smoke, yielding four intentions scale scores in total. Excluded cases due to missing data were less than 2% for each of the scales.
Psychosocial Risk Factors
Composite scale scores were created to represent each of the 14 psychosocial risk variables that corresponded to those specified by the behavioral model as the targeted mediators of the intervention. Each composite variable consisted of three to eight questions. Composite variables were formed in a manner similar to the intentions scale scores. Separate scores were computed on the 14 psychosocial risk factors for the baseline and one-year follow up, making 28 risk factor scale scores in total. Characteristics of the risk factor scale scores are given in Table 1. For scales composed of four or fewer items, students had to answer all questions in order for a composite score to be computed. For scales composed of five or more items, composites were computed for students missing no more than one response. In other words, if a student had missing responses to less than 20% of the items pertaining to a scale, an adjusted scale score was assigned; if a student was missing responses to greater than 20% of the items of a scale, a missing value was assigned. Treating scale scores with five or more questions in this manner helped to retain students in the study with minimal bias in results. Excluded cases due to missing data ranged from .3% to 5.7% for mediator scales at baseline, and from .2% to 3.7% for mediator scales at one-year follow-up. Cases with four or more inconsistent responses were excluded from the dataset; less than 1% of the data were excluded for this reason.
Table 1.
Psychosocial Risk Mediator Variables and Outcome Variables used in Mediation Analyses
| Composite Variable | Items | Scale range | Sample Questionsd |
|---|---|---|---|
| Knowledge of Health Effects | 5 | 0 – 10a | Are all kinds of tobacco use dangerous? Does using tobacco as a young person harm your health immediately? Is it safe to smoke or chew tobacco for only one or two years? |
| Knowledge of Tobacco Control Policy | 3 | 0 - 6a | Does your state have a law which stops people… from smoking in public places? …from selling tobacco products to minors under age 18? …from selling gutkha? |
| Beliefs about Social Consequences | 5 | 0 – 15b | If you used tobacco, do you think… your parents would get angry? …your friends would break off their friendship with you? …people would form a bad impression of you? |
| Normative Beliefs | 6 | 0 – 18b | Is it okay… for people of your age to try tobacco out of curiosity? …for adults to send children to buy tobacco for them? …for adults to smoke or chew tobacco in the presence of children? |
| Normative Expectations | 6 | 0 – 18b | If you were to use tobacco, do you think…your close friends would like it? …your parents would like it? …boys/girls in your school/neighborhood would like it? |
| Reasons to Use Tobacco | 6 | 0 – 18b | Are boys/girls who chew or smoke tobacco more attractive and have more friends? Does using tobacco make a person appear to be more brave and grown up? Does using tobacco reduce boredom (getting bored)? |
| Reasons Not to Use | 5 | 0 – 15b | I would not want to use tobacco because… I would be breaking my parents' rules….My friends don't use tobacco…People might form a bad impression of me. |
| Self-Efficacy in Refusal Skills | 5 | 0 – 15b | Do you think you could say “no” if…a family member gave you tobacco? …a close friend gave you tobacco? …another adult gave you tobacco? |
| Self-Efficacy in Advocacy | 8 | 0 – 21b | Do you think you could… help a friend stay away from trying tobacco? …help an adult stop using tobacco? …ask an adult to stop smoking around you? |
| Social Susceptibility to Smoking | 4 | 0 – 12b | If a group of friends gave you a cigarette or a bidi, would you smoke it? If a family member (like an uncle) gave you a cigarette or a bidi, would you smoke it? |
| Social Susceptibility to Chewing | 4 | 0 - 12b | If one of your close friends gave you chewing tobacco, would you chew it? If someone at a party (like a wedding) gave you chewing tobacco, would you chew it? |
| Perceived Prevalence of Smoking | 4 | 0 - 12c | How many adult males in India do you think smoke tobacco regularly? How many girls of your age in India do you think smoke tobacco regularly? |
| Perceived Prevalence of Chewing | 4 | 0 - 12c | How many adult females in India do you think chew tobacco regularly? How many boys of your age in India do you think chew tobacco regularly? |
| Support for Tobacco Control Policy | 5 | 0 - 15b | Should smoking be permitted in public places? Should adults be allowed to use tobacco in schools? Should any form of tobacco advertising be allowed? |
| Intentions to Chew | 4 | 0 - 12b | Do you think that you will try chewing tobacco… in the next month? …in the next year?…when you enter college? …when you are an adult? |
| Intentions to Smoke | 4 | 0 - 12b | Do you think that you will try smoking tobacco… in the next month? …in the next year?…when you enter college? …when you are an adult? |
Note: For all mediator and outcome composite variables, a higher scale score indicated less risk.
Rated on knowledge scale: Yes, No, Don't know
Rated on agreement scale: Surely yes, maybe yes, maybe no, surely no
Rated on frequency scale: None, Some, A few, Most
Sample questions were taken directly from the student survey
Analysis
Mediation analyses were conducted using the rationale and statistical procedures outlined by MacKinnon and colleagues (MacKinnon 2008; MacKinnon and Dwyer 1993; MacKinnon, Lockwood et al. 2002). A mediation model is a path model that specifies a hypothesized causal chain between independent (X), dependent (Y), and mediating (M) variables. Using a series of regression equations, statistical mediation analysis tests the X→M→Y relation, designating the independent variable as affecting a mediating variable which in turn affects the dependent variable (MacKinnon, Lockwood et al. 2002). Briefly, an effect was said to be mediated if (i) the program had a statistically significant effect on the hypothesized mediator, (ii) the hypothesized mediator was associated with the desired outcome after controlling for the intervention effect, and (iii) the mediated effect was statistically significant (MacKinnon 2008). Generally, a significant program effect (X→Y) is also considered a requirement for mediation to occur (Baron and Kenny 1986; Judd and Kenny 1981). However, opposite signs of the coefficients representing the effects of X→M and M→Y could result in a nonsignificant program effect due to canceling yet still produce a significant mediated effect (MacKinnon et al. 2000). Thus, a significant program effect is not always a necessary condition for mediation, and was not a requirement in the current analyses.
Single Mediation Models
Fourteen single mediator models were estimated for each outcome—Intentions to Chew and Intentions to Smoke. Mixed-effects regression models were used in order to account for multilevel data, since students were nested within schools and intraclass correlation coefficients indicated clustering among students. A lack of independence among students violates the assumption of independent observations and can affect the significance test of the indirect effect (MacKinnon 2008). To handle the repeated measures design involving measures at both baseline and 1-year follow up, an ANCOVA method was used, in which the baseline mediator and outcome measures were included in the model as covariates in predicting the 1-year follow up scores on these measures (MacKinnon 2008). In addition, each model was adjusted for gender, grade, school type, and region.
Figure 2 depicts a single multi-level mediation model using the psychosocial mediator “Knowledge of Health Effects” as an example. The independent variable (X) was Project MYTRI status (0=Control group, 1=Intervention group), and the dependent variable was the Intentions to Chew scale score. The α1 coefficient codes the relationship between X and the Knowledge of Health Effects mediator at Year 1 (M2), holding constant the baseline mediator (M1). The α path is associated with a test of the action theory (Chen 1990). The β1 coefficient codes the relationship between the Year 1 mediator variable (M2) and the Year 1 Intentions to Chew outcome variable (Y2), controlling for the baseline Intentions to Chew outcome variable (Y1) and M1. The β path is associated with a test of the conceptual theory (Chen 1990). The τ coefficient denotes the program effect between X and Y2, controlling for Y1, and the τ′ coefficient codes the relationship between X and Y2, holding constant Y1, M1, and M2. The coefficients labeled s1 and s2 represent stability estimates between the baseline and Year 1 measures, partialling out the other variables. The β2 coefficient codes the relationship between Y1 and M2, and β3 denotes the relationship between M1 and Y2, controlling for the other measures. The dotted lines in the figure are used to distinguish between paths that were used to calculate the total, mediated, and direct effects (solid lines) and those that were not (dotted lines).
Figure 2.
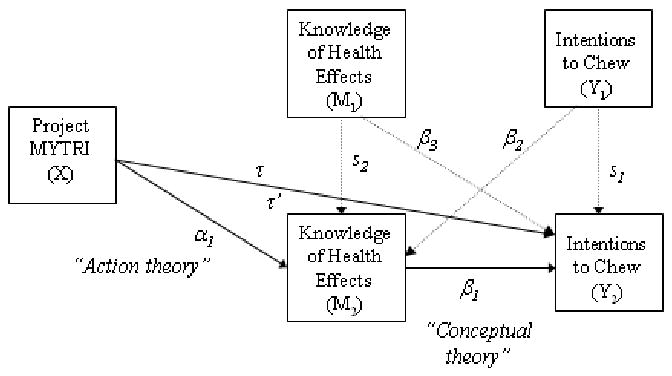
Single mediator model
The mediated effect was calculated using α1*β1, according to the product of coefficients method. Aroian's test was used to test the significance of the mediated effect. The formula was used to calculate the standard error of the mediated effect and a Z statistic was computed using the equation (MacKinnon, Lockwood et al. 2002). The standard error was also used to construct confidence intervals of the mediated effect (MacKinnon 2008). The direct effect was equivalent to τ′ and the total effect was equal to α1*β1 + τ′. The proportion mediated was calculated using the formula [α1β1/((α1β1) + τ′)]*100, and represented the percent of the overall effect of Project MYTRI on Intentions to Chew (or Intentions to Smoke) that was mediated by the focal psychosocial risk variable.
Multiple Mediator Models
Multi-level multiple mediator models were also estimated separately for the Intentions to Chew and Intentions to Smoke outcome variables. The models included only the psychosocial mediator variables that were identified as statistically significant in the single mediator models. Perceived Prevalence of Smoking was excluded from the Intentions to Chew multiple mediator model due to the high correlation between Perceived Prevalence of Chewing and Perceived Prevalence of Smoking (r=.68); the multicollinearity resulting from the inclusion of both prevalence predictors impeded interpretation of program effects. Similar to the single mediator models, the ANCOVA method was used to handle repeated measures, and the model adjusted for gender, grade, school type, and region. The multiple mediator model and equations were structured as advised in MacKinnon (2008). Nine single mediators were identified and their mediated effects in the multiple mediation model were calculated using αM*βM for each of the nine mediators. The total mediated effect was equal to the sum of the nine individual mediated effects, . Tests of the significance of the individual mediated effects were conducted in the same manner as those for the single mediator models. To test the significance of the total mediated effect, the standard error was first calculated according to the following formula:
where b1b2 is the covariance between the β estimates for two mediators, and the segment is repeated for all pairs of coefficients associated with pairs of mediator variables. A value for Z was calculated by dividing the total mediated effect by the standard error of the total mediated effect. To calculate the proportion mediated by an individual mediator within the model, the equation was used. The formula provided the total proportion mediated.
All models were estimated using PROC MIXED in SAS 9.1 (Littell et al. 1996). Since the mediation results were calculated using a series of equations, only cases with data for all variables within the series of equations were included in the sample. The restricted maximum likelihood method (REML default method in PROC MIXED) was used to estimate item parameters. The Satterthwaite method was used to compute the denominator degrees of freedom for the tests of the fixed effects. An unstructured covariance matrix was specified for defining random effects. The Akaike Information Criteria (AIC) and the chi-square statistic were used to evaluate the overall fit of the model.
Results
Single Mediator Models
Descriptive statistics, including estimates of the changes in the outcome and psychosocial risk factors variables between the study conditions over time, are presented in Stigler et al. (2007). Table 2 presents the single mediation model results for each psychosocial risk factor predicting Intentions to Chew and Intentions to Smoke. Significant program effects (τ) were observed for Intentions to Chew (t=-2.16, p=.04) but not for Intentions to Smoke (t = -1.85, p =.07). Although a significant program effect is generally considered a requirement to demonstrate mediation, analyses were not discontinued once nonsignificant program effects for Intentions to Smoke were observed because estimates of the effects associated with the X → M (α) and M → Y (β) paths were still of interest in order to describe the impact of Project MYTRI in terms of the action and conceptual theories (Chen 1990). In addition, as stated previously, a significant mediated effect could still be achieved despite a nonsignificant program effect if opposite signs of the α and β coefficients cancel each other out (MacKinnon 2008).
Table 2.
Parameter Estimates for the Single Mediator Models for the Intentions to Chew and Intentions to Smoke Outcome Variables
| N | τ (SE) | τ′(SE) | α (SE) | β (SE) | α*β (SE) | LCL, UCL | Z′ | % Med | |
|---|---|---|---|---|---|---|---|---|---|
| Knowledge of Health Effects | |||||||||
| Outcome: Chew | 7996 | -.11* (.05) | -.05 (.05) | -.42* (.06) | .16* (.01) | -.07* (.01) | -.09, -.05 | -6.26* | 57% |
| Outcome: Smoke | 7984 | -.13 (.07) | -.08 (.07) | -.43* (.07) | .11* (.01) | -.05* (.08) | -.06, -.03 | -5.62* | 36% |
| Knowledge of Tobacco Control Policy | |||||||||
| Outcome: Chew | 7895 | -.11* (.06) | -.10 (.05) | -.30* (.09) | .06* (.01) | -.02* (.01) | -.03, -.01 | -2.98* | 15% |
| Outcome: Smoke | 7879 | -.13 (.07) | -.12 (.07) | -.31* (.09) | .03* (.01) | -.01* (.00) | -.02, -.00 | -2.46* | 8% |
| Beliefs about Social Consequences | |||||||||
| Outcome: Chew | 8004 | -.12* (.05) | -.07 (.05) | -.57 (.29) | .07* (.00) | -.04* (.02) | -.08, .00 | -1.97* | 36% |
| Outcome: Smoke | 7990 | -.13 (.07) | -.11 (.07) | -.59 (.30) | .05* (.00) | -.03* (.02) | -.06, .00 | -1.97* | 21% |
| Normative Beliefs | |||||||||
| Outcome: Chew | 8057 | -.12* (.05) | -.01 (.04) | -.35* (.12) | .32* (.01) | -.11* (.04) | -.19, -.04 | -2.86* | 95% |
| Outcome: Smoke | 8043 | -.14 (.07) | -.02 (.04) | -.34* (.13) | .35* (.01) | -.12* (.04) | -.21, -.03 | -2.75* | 86% |
| Normative Expectations | |||||||||
| Outcome: Chew | 7948 | -.11* (.05) | -.08* (.04) | -.22 (.15) | .13* (.01) | -.03 (.02) | -.07, .01 | -1.45 | |
| Outcome: Smoke | 7927 | -.13 (.07) | -.11 (.06) | -.24 (.15) | .11* (.01) | -.03 (.02) | -.06, .01 | -1.61 | |
| Reasons to Use | |||||||||
| Outcome: Chew | 8036 | -.12* (.05) | -.05 (.05) | -.37* (.15) | .19* (.01) | -.07* (.02) | -.13, -.01 | -2.44* | 57% |
| Outcome: Smoke | 8021 | -.13 (.07) | -.06 (.06) | -.35* (.15) | .22* (.01) | -.08* (.03) | -.14, -.01 | -2.39* | 56% |
| Reasons Not to Use | |||||||||
| Outcome: Chew | 7680 | -.13* (.06) | -.11* (.05) | -.57* (.26) | .02* (.00) | -.01* (.01) | -.03, .00 | -2.00* | 11% |
| Outcome: Smoke | 7658 | -.14 (.07) | -.13 (.07) | -.59* (.27) | .02* (.00) | -.01* (.01) | -.02, .00 | -2.04* | 8% |
| Self-Efficacy in Refusal Skills | |||||||||
| Outcome: Chew | 7927 | -.12* (.05) | -.12* (.05) | .03 (.38) | .01* (.00) | .00 (.00) | -.01, .01 | .07 | |
| Outcome: Smoke | 7908 | -.14 (.07) | -.14 (.07) | -.01 (.38) | .01* (.00) | .00 (.00) | -.01, .01 | -.03 | |
| Self-Efficacy in Advocacy | |||||||||
| Outcome: Chew | 7945 | -.11* (.06) | -.08 (.06) | -.97* (.43) | .04* (.00) | -.03* (.02) | -.06, -.00 | -2.22* | 30% |
| Outcome: Smoke | 7927 | -.13 (.07) | -.11 (.07) | -1.04* (.43) | .02* (.00) | -.03* (.01) | -.05, -.00 | -2.36* | 19% |
| Susceptibility to Chewing | |||||||||
| Outcome: Chew | 7682 | -.11* (.05) | -.03 (.03) | -.11 (.05) | .79* (.01) | -.09* (.04) | -.17, -.00 | -1.98* | 73% |
| Outcome: Smoke | 7665 | -.12 (.07) | -.07 (.05) | -.11 (.06) | .52* (.01) | -.06* (.03) | -.11, -.00 | -2.00* | 45% |
| Susceptibility to Smoking | |||||||||
| Outcome: Chew | 7829 | -.12* (.06) | -.06 (.04) | -.08 (.06) | .60* (.01) | -.05 (.04) | -.13, .02 | -1.35 | |
| Outcome: Smoke | 7852 | -.13 (.07) | -.06 (.03) | -.08 (.06) | .83* (.01) | -.07 (.05) | -.17, .04 | -1.27 | |
| Prevalence of Chewing | |||||||||
| Outcome: Chew | 7615 | -.12* (.06) | -.16* (.06) | .62* (.11) | .06* (.01) | .04* (.01) | .02, .06 | 4.27* | 20% |
| Outcome: Smoke | 7581 | -.14 (.07) | -.16 (.07) | .59* (.11) | .03* (.01) | .02* (.01) | .00, .03 | 2.52* | 9% |
| Prevalence of Smoking | |||||||||
| Outcome: Chew | 7587 | -.11 (.06) | -.12* (.06) | .38* (.11) | .06* (.01) | .02* (.01) | .01, .04 | 2.90* | 15% |
| Outcome: Smoke | 7570 | -.13 (.07) | -.15 (.07) | .36* (.11) | .07* (.01) | .02* (.01) | .01, .04 | 3.03* | 14% |
| Support for Tobacco Control Policy | |||||||||
| Outcome: Chew | 7985 | -.11* (.06) | -.05 (.04) | -.20 (.11) | .26* (.01) | -.05 (.03) | -.11, .01 | -1.80 | |
| Outcome: Smoke | 7969 | -.13 (.07) | -.07 (.05) | -.21 (.12) | .26* (.01) | -.06 (.03) | -.11, .00 | -1.83 |
p<.05
Note: LCL=Lower Confidence Limit; UCL=Upper Confidence Limit. Specifies the upper and lower range likely to include the mediated effect. % Med. = Proportion Mediated.
The β path estimates associated with the conceptual theory indicated all of the psychosocial mediators were significantly related to both intentions outcome variables in a positive direction; that is, holding constant all other factors, an increase in the value of the mediator was associated with a decrease in intentions to smoke or chew. However, the α coefficients associated with the action theory showed that Project MYTRI altered only certain psychosocial mediators. The estimates indicated that Knowledge of Health Effects, Knowledge of Tobacco Control Policy, Normative Beliefs, Reasons to Use, Reasons Not to Use, and Self-Efficacy in Advocacy were significantly altered by Project MYTRI; holding constant all factors but treatment group, mediator scale scores for these psychosocial risk factors were higher (meaning less risk) for students in the intervention group compared to those in the control condition. Risk factors that were not significantly altered by Project MYTRI (i.e. non-significant α path) included Beliefs about Social Consequences, Normative Expectations, Self-Efficacy in Refusal Skills, Support for Tobacco Control Policy, and both social susceptibility variables.
Based on the α*β estimates (see Table 2), significant single mediators included Knowledge of Health Effects, Knowledge of Tobacco Control Policy, Beliefs about Social Consequences, Normative Beliefs, Reasons to Use Tobacco, Reasons Not to Use Tobacco, Self-efficacy in Advocacy Skills, Social Susceptibility to Chewing, and Perceived Prevalence of Chewing and Smoking. Beliefs about Social Consequences and Susceptibility to Chewing were significant mediators despite nonsignificant X → M (α) paths. Normative beliefs, Susceptibility to Chewing, Knowledge of Health Effects, and Reasons to Use tobacco contributed the most to the overall effect of Project MYTRI on the Intentions to Chew and Intentions to Smoke outcome variables as measured by the proportion mediated.
For the Perceived Prevalence factors, there was evidence of inconsistent mediation, which occurs when the direct effect and mediated effect have opposite signs (MacKinnon et al. 2000). The mediated effects (α*β) were positive for the Perceived Prevalence variables, while the direct effects were negative. As indicated by the α paths, the Perceived Prevalence variables were significantly altered by the intervention, but not in the intended direction; contrary to program intent, Project MYTRI increased rather than decreased students' perceptions of how common it was for people to use tobacco. The β paths for the Perceived Prevalence variables were also positive and consistent with the curriculum design (i.e. lower perceived prevalence of tobacco use helped to decrease students' intentions to use tobacco in the future). Thus, a positive mediated effect indicated Project MYTRI inadvertently increased students' perceived prevalence beliefs about tobacco use, thus increasing students' risk of having intentions to use tobacco in the future.
Multiple Mediator Models
Results for the multiple mediator models are presented in Table 3. In the multiple mediator model scenarios, Project MYTRI had a significant program effect on Intentions to Chew, but not on Intentions to Smoke. Similar to the single mediator models, multiple mediation analysis for Intentions to Smoke was still performed in order to gain insight into the action and conceptual theories. The estimate of the total mediated effect for Intentions to Chew was -.13 (seα*β=.02) and was significant (Z′= 10.35). Significant mediating psychosocial risk factors for Intentions to Chew included Knowledge of Health Effects, Normative Beliefs, Reasons to Use Tobacco, and Perceived Prevalence of Chewing. The proportion mediated was highest for Normative Beliefs (18% of the total mediated effect), followed by Knowledge of Health Effects (10%), Perceived Prevalence of Chewing (7%), and Reasons to Use Tobacco (6%).
Table 3.
Parameter Estimates for the Multiple Mediator Models for Intentions to Chew and Intentions to Smoke Outcome Variables
| Mediator | τ (SE) | τ′ (SE) | α (SE) | β (SE) | αM*βM (SE) | LCL, UCL | Z′ | % Med.a |
|---|---|---|---|---|---|---|---|---|
| Mediators Combined | ||||||||
| Outcome: Chew (N=6628) | -.13* (.06) | .00 (.04) | -.13* (.02) | -.16, -.10 | 10.35* | 99% | ||
| Outcome: Smoke (N=6271) | -.13 (.08) | .00 (.04) | -.14* (.04) | -.21, -.07 | -3.98* | 93% | ||
| Knowledge of Health Effects | ||||||||
| Outcome: Chew | -.40* (.06) | .04* (.01) | -.02* (.00) | -.02, -.01 | -4.04* | 10% | ||
| Outcome: Smoke | -.41* (.07) | .02* (.01) | -.01* (.00) | -.01, -.00 | -2.27* | 4% | ||
| Knowledge of Tobacco Control Policy | ||||||||
| Outcome: Chew | -.29* (.09) | -.00 (.01) | .00 (.00) | -.00, .01 | .12 | .2% | ||
| Outcome: Smoke | -.30* (.09) | -.02* (.01) | .01 (.00) | .00, .01 | 1.91 | 3% | ||
| Beliefs about Social Consequences | ||||||||
| Outcome: Chew | -.54 (.29) | .02* (.00) | -.01 (.01) | -.02, .00 | -1.64 | 6% | ||
| Outcome: Smoke | -.56 (.28) | .02* (.00) | -.01 (.01) | -.02, .00 | -1.72 | 4% | ||
| Normative Beliefs | ||||||||
| Outcome: Chew | -.36* (.13) | .08* (.01) | -.03* (.01) | -.05, -.01 | -2.60* | 18% | ||
| Outcome: Smoke | -.34* (.14) | .17* (.01) | -.06* (.02) | -.11, -.01 | -2.46* | 29% | ||
| Reasons to Use Tobacco | ||||||||
| Outcome: Chew | -.38* (.16) | .03* (.01) | -.01* (.01) | -.02, .00 | -2.04* | 6% | ||
| Outcome: Smoke | -.34* (.15) | .07* (.01) | -.03* (.01) | -.05, -.00 | -2.15* | 12% | ||
| Reasons Not To Use | ||||||||
| Outcome: Chew | -.49 (.27) | -.00 (.00) | .00 (.00) | -.00, .01 | .98 | 1% | ||
| Outcome: Smoke | -.49 (.28) | .00 (.00) | .00 (.00) | -.00, .01 | .89 | 1% | ||
| Self-Efficacy in Advocacy Skills | ||||||||
| Outcome: Chew | -.80 (.41) | .01* (.00) | -.01 (.01) | -.02, .00 | -1.78 | 5% | ||
| Outcome: Smoke | -.87* (.43) | .01* (.00) | -.01 (.00) | -.01. .00 | -1.48 | 2% | ||
| Susceptibility to Chewing | ||||||||
| Outcome: Chew | -.11 (.06) | .70* (.01) | -.07 (.00) | -.15, .01 | -1.81 | 47% | ||
| Outcome: Smoke | -.10 (.06) | .34* (.01) | -.04 (.02) | -.08, .01 | -1.69 | 17% | ||
| Perceived Prevalence of Chewing | ||||||||
| Outcome: Chew | .60* (.11) | .02* (.01) | .01* (.01) | .00, .02 | 2.04* | 7% | ||
| Outcome: Smoke | .55* (.11) | -.05* (.01) | -.03* (.01) | -.04, -.01 | -3.46* | 13% | ||
| Perceived Prevalence of Smoking | ||||||||
| Outcome: Chew | -- | -- | -- | -- | -- | -- | ||
| Outcome: Smoke | .34* (.11) | .05* (.01) | .02* (.01) | .01, .03 | 2.71* | 9% |
p<.05
Calculation based on dividing the sum of the absolute values of all α*β by the absolute value total effect (of significant mediators)
Note: LCL=Lower Confidence Limit; UCL=Upper Confidence Limit. Specifies the upper and lower range likely to include the mediated effect. % Med. = Proportion Mediated.
The estimate of the total mediated effect for Intentions to Smoke was -.14 (seα*β=.04) and was also significant (Z′= -3.98). The same four risk factors that were significant mediators for Intentions to Chew were significant for Intentions to Smoke with the addition of Perceived Prevalence of Smoking. Normative Beliefs again had the highest proportion mediated (29% of the total mediated effect), followed by Perceived Prevalence of Chewing (13%), Reasons to Use Tobacco (12%), Perceived Prevalence of Smoking (9%), and Knowledge of Health Effects (4%). The finding that fewer psychosocial variables were significant mediators in the multiple mediator models suggests variance overlap among the mediators (i.e., the mediators were significantly correlated with each other). Similar to the single mediator models, evidence of inconsistent mediation was also observed in the multiple mediator models. Specifically, Perceived Prevalence of Chewing was an inconsistent mediator for Intentions to Chew and Perceived Prevalence of Smoking was an inconsistent mediator for Intentions to Smoke. This indicated Project MYTRI unintentionally increased students' perceptions of the prevalence of chewing and smoking tobacco use, which subsequently increased students' intentions to (respectively) chew and smoke tobacco in the future. Perceived Prevalence of Chewing was a significant mediator for Intentions to Smoke, but not an inconsistent mediator; the positive α and negative β paths meant that Project MYTRI increased students' perceptions of how common it was for people to chew tobacco, but these increases in students' prevalence beliefs about chewing tobacco use actually decreased students risk of using smoking tobacco in the future.
Separate multiple mediator models by grade level showed fewer significant mediators for 8th graders than 6th graders. For 6th graders, significant mediators for Intentions to Chew were Susceptibility of Chewing (p=.05), Normative Beliefs (p=.01), and Knowledge of Health Effects (p=.01). The proportions mediated for those variables were 57%, 13%, and 11%, respectively. For the 8th Grade Intentions to Chew model, only Normative Beliefs (p=.01) and Knowledge of Health Effects (p<.01) were significant mediators. The proportions mediated were 22% and 8%, respectively. However, the total mediated effect was significant for the 6th Grade model (-.17, se=.05, Z′=-3.41) but not for the 8th Grade model (-.10, se=.06, Z′=-1.65). Statistics for total proportion mediated indicated the mediated effects for the 6th Grade sample accounted for a greater portion (100%) of the program effect between Project MYTRI and Intentions to Chew than for the 8th Grade sample (84%).
For Intentions to Smoke, a significant total mediated effect was observed for both the 6th and 8th Grade models (p=.04 and p=.05, respectively). For the 6th Grade sample, Susceptibility of Chewing (p=.02), Normative Beliefs (p=.02), Perceived Prevalence of Chewing (p=.01), Perceived Prevalence of Smoking (p=.01), and Knowledge of Health Effects (p=.01) were significant mediators. The proportions mediated for those variables were 20%, 16%, 14%, 8%, and 6%, respectively. For the 8th Grade Intentions to Smoke model, significant mediators included Normative Beliefs (p=.04), Beliefs about Social Consequences (p=.01), and Perceived Prevalence of Chewing (p=.01). The proportions mediated for those variables were 44%, 12%, and 11%, respectively. The total proportion mediated for the 8th grade model was higher (81%) compared to the 6th Grade model (72%).
Discussion
The intent of Project MYTRI was to impact students' tobacco-use practices and intentions over the two-year course of the intervention by influencing targeted mediating psychosocial factors. By using mediation analysis to assess the hypothesized causal chain between variables, the results presented here highlight several areas where Project MYTRI was successful in meeting its first-year program goals. Results likewise revealed areas in which modifications to the curriculum, implementation, or measurements might be necessary in order to meet intervention objectives.
During year one, Project MYTRI successfully altered the psychosocial risk factors Knowledge of Health Effects, Reasons to Use Tobacco, and Normative Beliefs—the observed increase in the estimates for these risk factors (meaning less risk) was associated with a decrease in students' intentions to use smoking or chewing tobacco in the future. This was consistent with the broad goal of the first-year curriculum—to fortify students' knowledge and beliefs about tobacco use. These three psychosocial factors have been shown to mediate the relationship between treatment and outcome effects of other school-based interventions aimed at reducing cigarette, alcohol, and/or other drug use among adolescents. Knowledge was a significant mediator associated with the Life Skills Training program, which was designed to equip students with skills to resist social influences to smoke. The program was administered to 7th grade urban minority students (N=3,153) in 47 New York City schools (Botvin et al. 1992). Mediation analysis of pre- and post-test data found that knowledge of the immediate consequences of smoking was one of five significant mediators between the program and the treatment effect on cigarette use (i.e. smoking prevalence and onset) (Botvin et al. 1992). However, some other mediational studies of school-based prevention programs in the West have not consistently shown knowledge to be an important mediator (Cuijpers 2002; MacKinnon et al. 1991; Orlando et al. 2005). Nonetheless, for Project MYTRI, increasing knowledge does appear to be a prerequisite for intervention success. According to social cognitive theorists, knowledge may be regarded as a “precondition for change,” an impetus to alter health behaviors (Bandura 2004).
Studies of school-based prevention programs in the West have also returned inconsistent results for reasons to use tobacco as a mediator (Cuijpers 2002). Programs such as Project Alert and Project Northland found variables similar to Reasons to Use Tobacco as significant mediators (Komro et al. 2001; Orlando et al. 2005). Project Alert was implemented with 4,227 middle school students in South Dakota. Positive beliefs about the consequences of smoking and drinking was a significant mediator between Project Alert and students' intentions to smoke in the next six months, as well as between the intervention and students' past month tobacco use (Orlando et al. 2005). Project Northland was administered to 1,901 students in 6th through 8th grade in 24 school districts in Michigan, and involved multiple strategies, including school curricula, peer leadership activities, parental education, and community wide activities. Functional meanings of alcohol use was a significant mediator between the intervention and alcohol use as measured on the Tendency to Use Alcohol Scale. While some other prevention programs did not show reasons to use tobacco as a significant mediator, it was nonetheless important for Project MYTRI participants (Hansen and McNeal 1997; MacKinnon et al. 1991). Generally, perceptions about reasons to use tobacco are important since adolescents who view tobacco as providing a positive function, such as to win friends, appear “cool” or mature, or help to cope with stress, are at a higher risk of tobacco use than adolescents who do not share those beliefs (US Department of Health and Human Services 1994).
The most common finding across mediation studies of school-based drug prevention programs is the importance of peer influence. For instance, friends' reactions to drug use was a key mediator for the Midwestern Prevention program, a multi-component community-based prevention program that targeted tobacco, alcohol, and other drug use (MacKinnon et al. 1991). Numerous other studies revealed similar findings for peer influence-related mediators (Botvin et al. 1992, 1999; Donaldson et al. 1994; Komro et al. 2001; Orlando et al. 2005; Wynn et al. 2000). Findings for Project MYTRI are accordant; peer influence represented by the Normative Beliefs mediator appears critical in this context. Changing normative beliefs can have a substantial impact on adolescents' tobacco use since perceptions about the approval (or disapproval) of others towards a specific behavior and the social pressure derived from motivation to comply with other's expectations can determine whether adolescents form attitudes that steer them away from tobacco use or persuade them into experimentation (Bandura 1998). A study by Hahn et al. (1990) found that over half of all adolescents who had tried a cigarette did so on the prompting of a close friend or peer.
For Project MYTRI, the risk factors Knowledge of Tobacco Control Policy, Self-Efficacy in Advocacy and Refusal Skills, and Social Susceptibility, were not emphasized until year two of the program implementation, so these factors were not expected to be strong mediators in the present analyses. However, the first-year curriculum did focus on Beliefs in Social Consequences, Normative Expectations, and Reasons Not to Use Tobacco. These factors were expected to emerge as significant mediators, but were not significant in this analysis. The observation of inconsistent mediation for the perceived prevalence variables (which represented an increase in students' perceived prevalence beliefs and consequently an increase in students' intentions to use tobacco in the future) was also unexpected, though not completely rare; a counterproductive effect on adolescents' prevalence estimates has been previously observed in substance abuse resistance-skills training programs in the U.S. (Donaldson et al. 1995; Hansen and Graham 1991). Because Project MYTRI's program effect was weakened by inflated perceived prevalence beliefs, correcting students' perceptions about the prevalence of tobacco use is one way to improve the intervention. Further scrutiny into Project MYTRI's curriculum is needed to discover the reasons for higher prevalence estimates of tobacco use among the intervention students after the first-year implementation and to identify appropriate modifications to the program.
Lack of significant effects can be due to curriculum design, implementation of the curriculum, and/or the efficacy and quality of research instruments and administration (MacKinnon 2008). For example, a nonsignificant effect could be due to how well associated classroom activities were implemented (e.g. whether the activities were completed, whether peer leaders and teachers properly performed their roles, etc). The curriculum could also contribute to a nonsignificant effect; the content or activity design could fail to address the topic effectively or fail to properly engage students' attention and participation. A nonsignificant effect could also be due to the way that questions were asked on the student questionnaire. Competing contextual influences, such as students' home environment or the amount of peer influence they face, could also undermine the messages communicated by Project MYTRI and result in nonsignificant effects. In addition, student factors, such as academic pressures or other personal matters, could influence the power of the intervention. Explanations may involve numerous, concurring factors. Qualitative research can be particularly useful in providing rich descriptions of the how the program was implemented and in characterizing contextual factors that could moderate the impacts of Project MYTRI. Future reports from our team will present qualitative research findings, including results from qualitative mediation analyses, which focus specifically on processes related to the psychosocial risk factors.
A recent systematic review and meta-analysis of three decades of research found strong evidence of the short-term effectiveness of school-based tobacco-use prevention interventions to reduce smoking initiation and decrease the prevalence of tobacco use among youth; long-term effects were rarely shown due to a lack of extended evaluation time-periods (Dobbins et al. 2008). Findings of the meta-analysis indicated that the most effective programs were those that focused on “social norms, influences, and reinforcements,” included a cognitive behavior or life skills component, and involved a strong role played by peers and teachers. Project MYTRI includes all three of these aspects, and thus has the potential to successfully impact participating youth. These findings, combined with those from the qualitative research and the second-year student data, will help to illuminate the impact of Project MYTRI on participating Indian youth.
References
- Bandura A. Health promotion from the perspective of social cognitive theory. Psychology and Health. 1998;13:623–649. [Google Scholar]
- Bandura A. Social cognitive theory: An agentic perspective. Annual Review of Psychology. 2001;52:1–26. doi: 10.1146/annurev.psych.52.1.1. [DOI] [PubMed] [Google Scholar]
- Bandura A. Health promotion by social cognitive means. Health Education & Behavior. 2004;31:143–164. doi: 10.1177/1090198104263660. [DOI] [PubMed] [Google Scholar]
- Baranowski T, Perry CL, Parcel GS. How individuals, environments and health behavior interact: Social cognitive theory. In: Glanz K, Lewis FM, Rimer B, editors. Health behavior and health education: Theory, research & practice. 2nd. San Francisco, CA: Jossey-Bass; 1996. pp. 246–279. [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Botvin GJ, Dusenbury L, Baker E, James-Ortiz S, Botvin EM, Kerner J. Smoking prevention among urban minority youth: assessing effects on outcome and mediating variables. Health Psychology. 1992;11:290–299. doi: 10.1037//0278-6133.11.5.290. [DOI] [PubMed] [Google Scholar]
- Botvin GJ, Griffin KW, Diaz T, Miller N, Ifill-Williams M. Smoking initiation and escalation in early adolescent girls: one-year follow-up of a school-based prevention intervention for minority youth. Journal of the American Medical Women's Association. 1999;54:139–143. 152. [PubMed] [Google Scholar]
- Chen H. Theory-driven evaluations. London: Sage Publications; 1990. [Google Scholar]
- Cuijpers P. Effective ingredients of school-based drug prevention programs. A systematic review. Addictive Behaviors. 2002;27:1009–1023. doi: 10.1016/s0306-4603(02)00295-2. [DOI] [PubMed] [Google Scholar]
- Dobbins M, Decorby K, Manske S, Goldblatt E. Effective practices for school-based tobacco use prevention. Preventive Medicine. 2008;46:289–297. doi: 10.1016/j.ypmed.2007.10.003. [DOI] [PubMed] [Google Scholar]
- Donaldson SI, Graham JW, Hansen WB. Testing the generalizability of intervening mechanism theories: understanding the effects of adolescent drug use prevention interventions. Journal of Behavioral Medicine. 1994;17:195–216. doi: 10.1007/BF01858105. [DOI] [PubMed] [Google Scholar]
- Donaldson SI, Graham JW, Piccinin AM, Hansen WB. Resistance-skills training and onset of alcohol use: evidence for beneficial and potentially harmful effects in public schools and in private Catholic schools. Health Psychology. 1995;14:291–300. doi: 10.1037//0278-6133.14.4.291. [DOI] [PubMed] [Google Scholar]
- Global Youth Tobacco Survey Collaborating Group. Tobacco use among youth: a cross country comparison. Tobacco Control. 2002;11:252–270. doi: 10.1136/tc.11.3.252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hahn G, Charlin VL, Sussman S, Dent CW, Manzi J, Stacy AW, et al. Adolescents' first and most recent use situations of smokeless tobacco and cigarettes: similarities and differences. Addictive Behaviors. 1990;15:439–448. doi: 10.1016/0306-4603(90)90030-2. [DOI] [PubMed] [Google Scholar]
- Hansen WB, Graham JW. Preventing alcohol, marijuana, and cigarette use among adolescents: peer pressure resistance training versus establishing conservative norms. Preventive Medicine. 1991;20:414–430. doi: 10.1016/0091-7435(91)90039-7. [DOI] [PubMed] [Google Scholar]
- Hansen WB, McNeal RB., Jr How D.A.R.E. works: an examination of program effects on mediating variables. Health Education & Behavior. 1997;24:165–176. doi: 10.1177/109019819702400205. [DOI] [PubMed] [Google Scholar]
- Judd CM, Kenny DA. Process analysis: Estimating mediation in treatment evaluations. Evaluation Review. 1981;5:602–619. [Google Scholar]
- Komro KA, Perry CL, Williams CL, Stigler MH, Farbakhsh K, Veblen-Mortenson S. How did Project Northland reduce alcohol use among young adolescents? Analysis of mediating variables. Health Education Research. 2001;16:59–70. doi: 10.1093/her/16.1.59. [DOI] [PubMed] [Google Scholar]
- Littell RC, Milliken GA, Stroup WW, Wolfinger RD. SAS system for mixed models. Cary, NC: SAS Institute; 1996. [Google Scholar]
- MacKinnon DP. Introduction to statistical mediation analysis. Mahway, NJ: 2008. [Google Scholar]
- MacKinnon DP, Dwyer JH. Estimating mediated effects in prevention studies. Evaluation Review. 1993;17:144–158. [Google Scholar]
- MacKinnon DP, Johnson CA, Pentz MA, Dwyer JH, Hansen WB, Flay BR, et al. Mediating mechanisms in a school-based drug prevention program: first-year effects of the Midwestern Prevention Project. Health Psychology. 1991;10:164–172. doi: 10.1037//0278-6133.10.3.164. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Krull JL, Lockwood CM. Equivalence of the mediation, confounding and suppression effect. Prevention Science. 2000;1:173–181. doi: 10.1023/a:1026595011371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM. Advances in statistical methods for substance abuse prevention research. Prevention Science. 2003;4:155–171. doi: 10.1023/a:1024649822872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Taborga MP, Morgan-Lopez AA. Mediation designs for tobacco prevention research. Drug and Alcohol Dependence. 2002;68:S69–S83. doi: 10.1016/s0376-8716(02)00216-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mishra A, Arora M, Stigler MH, Komro KA, Lytle LA, Reddy KS, et al. Indian youth speak about tobacco: results of focus group discussions with school students. Health Education & Behavior. 2005;32:363–379. doi: 10.1177/1090198104272332. [DOI] [PubMed] [Google Scholar]
- Orlando M, Ellickson PL, McCaffrey DF, Longshore DL. Mediation analysis of a school-based drug prevention program: effects of Project ALERT. Prevention Science. 2005;6:35–46. doi: 10.1007/s11121-005-1251-z. [DOI] [PubMed] [Google Scholar]
- Pentz MA. Effective prevention programs for tobacco use. Nicotine & Tobacco Research. 1999;1 2:S99–107. doi: 10.1080/14622299050011891. [DOI] [PubMed] [Google Scholar]
- Pentz MA, Jasuja GK, Rohrbach LA, Sussman S, Bardo MT. Translation in tobacco and drug abuse prevention research. Evaluation & the Health Professions. 2006;29:246–271. doi: 10.1177/0163278706287347. [DOI] [PubMed] [Google Scholar]
- Perry CL, Kelder SH, Murray DM, Klepp KI. Communitywide smoking prevention: Long-term outcomes of the Minnesota Heart Health Program and the Class of 1989 Study. American Journal of Public Health. 1992;82:1210–1216. doi: 10.2105/ajph.82.9.1210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry CL, Komro KA, Veblen-Mortenson S, Bosma LM, Farbakhsh K, Munson KA, et al. A randomized controlled trial of the middle and junior high school D.A.R.E. and D.A.R.E. Plus programs. Archives of Pediatric & Adolescent Medicine. 2003;157:178–184. doi: 10.1001/archpedi.157.2.178. [DOI] [PubMed] [Google Scholar]
- Perry CL, Stigler MH, Arora M, Reddy KS. Prevention in Translation: Tobacco Use Prevention in India. Health Promotion Practice. 2006 doi: 10.1177/1524839906289222. [DOI] [PubMed] [Google Scholar]
- Perry CL, Williams CL, Komro KA, Veblen-Mortenson S, Stigler MH, Munson KA, et al. Project Northland: long-term outcomes of community action to reduce adolescent alcohol use. Health Education Research. 2002;17:117–132. doi: 10.1093/her/17.1.117. [DOI] [PubMed] [Google Scholar]
- Reddy KS, Arora M, Perry CL, Nair B, Kohli A, Lytle LA, et al. Tobacco and alcohol use outcomes of a school-based intervention in New Delhi. American Journal of Health Behavior. 2002;26:173–181. doi: 10.5993/ajhb.26.3.2. [DOI] [PubMed] [Google Scholar]
- Reddy KS, Gupta PC. Report on Tobacco Control in India. New Delhi: Ministry of Health and Family Welfare, Government of India; 2004. [Google Scholar]
- Reddy KS, Perry CL, Stigler MH, Arora M. Differences in tobacco use among young people in urban India by sex, socioeconomic status, age, and school grade: assessment of baseline survey data. Lancet. 2006;367:589–594. doi: 10.1016/S0140-6736(06)68225-1. [DOI] [PubMed] [Google Scholar]
- Stigler MH, Perry CL, Arora M, Reddy KS. Why are urban Indian 6th graders using more tobacco than 8th graders? Findings from Project MYTRI. Tobacco Control. 2006;15:i54–i60. doi: 10.1136/tc.2005.014480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stigler MH, Perry CL, Arora M, Shrivastav R, Mathur C, Reddy KS. Intermediate outcomes from Project MYTRI: mobilizing youth for tobacco-related initiatives in India. Cancer Epidemiology Biomarkers & Prevention. 2007;16:1050–1056. doi: 10.1158/1055-9965.EPI-06-0929. [DOI] [PubMed] [Google Scholar]
- The World Bank. Curbing the Epidemic: Governments and the economics of tobacco control. Washington, D. C.: 1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tobler NS. Meta-analysis of 143 adolescent drug prevention programs: quantitative outcome results of program participants compared to a control or comparison group. Journal of Drug Issues. 1986;16:537–567. [Google Scholar]
- US Department of Health and Human Services. Preventing tobacco use among young people: A report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 1994. [Google Scholar]
- Warren CW, Jones NR, Peruga A, Chauvin J, Baptiste J, Costa de Silva V, et al. Global Youth Tobacco Surveillance, 2000-2007. MMWR Surveillance Summaries: Morbidity and mortality weekly report. 2008;57:1–28. [PubMed] [Google Scholar]
- Wynn SR, Schulenberg J, Maggs JL, Zucker RA. Preventing alcohol misuse: The impact of refusal skills and norms. Psychology of Addictive Behaviors. 2000;14:36–47. doi: 10.1037//0893-164x.14.1.36. [DOI] [PubMed] [Google Scholar]