

Abstract
As India will ranks first in diabetes now and will continue to do so in 2025, we must prevent the disease by various measures. Before setting the programmes, we should have ample data on the population's knowledge, attitude and practice (KAP) of diabetes. There are some epidemiological studies from southern India, Mumbai and north India, but there is no KAP study from Gujarat. The study was conducted between the period of June 2007 to November 2007 at three centers of Saurashtra region. Out of 300 patients who were given questionnaire, 238 patients were included for the analysis, rest were excluded due to various reasons. 52% were male. Mean age of patients was 55.82±10.2 years (95% CI 54.5-57.1) with mean weight of 64.52±10.96 Kg (95% CI 62.8-66.2). Mean duration of diabetes was 8.2±6.8 years (95% CI 7.2-9.1). 46% of patients knew the pathophysiology of diabetes. Nearly 50% knew the complications of diabetes. Dietary modifications were relied more than exercises among the interviewed subjects. Most of the lacunae in knowledge prevailed in drug therapy of diabetes. Insulin was not favored by most of patients. An encouraging finding in our study was that most believed in self-care and ready to change. Consultation time given by their treating doctors was less than 5 minutes in nearly 50%. Foot care and education to prevent complications were least suggested by doctors.
Keywords: Knowledge, attitude and practice study, type 2 diabetes
Introduction
Prevalence of type 2 diabetes is increasing globally,[1] more so in developing countries like India due to rapid urbanization.[2,4] It is estimated that prevalence of diabetes will rise to 5.5% in 2025 as compared to 4% in year 1995.[3] The total direct cost for diabetes management has doubled from 1998 to 2005.[5] Therefore, prevention is important both on monetary and human matters. There is an increasing amount of evidence that the patient education is the most effective way to lessen the complications of diabetes and its management.[6] Education is likely to be effective if we know the characteristic of the patients in terms of knowledge, their attitude and practices about diabetes. There are numerous studies with special emphasis on epidemiology mainly from South India, Delhi and Mumbai.[7,8] However, despite our extensive literature search we could not find any KAP study of diabetes mellitus especially from the Saurashtra region.
Aims
The aim of the study was to assess the knowledge, attitude and practice of patients with type 2 DM in Saurashtra region.
Materials and Methods
The study was conducted between the period of June 2007 to November 2007 at three centers 1) G.G.Hospital, Jamnagar 2) Sir Takhatsinhji Hospital, Bhavnagar 3) S. J. Eye Hospital, Gondal, Rajkot. All these places belong to Saurashtra region, Gujarat. First two are tertiary care hospitals with teaching facilities and third is private sector in rural area run by a Non Government Organization (NGO). The patients attending out-door facility of these hospitals were included in the study and given predesigned proforma to fill the questionnaire. To avoid bias, the patients who were not being treated by authors at the time of this study were only included. The questionnaire did not contain any questions which can reveal the identity of patients or their treating doctors. Out of 300 patients who were given questionnaire, only 238 patients were included for the final analysis. Rest were excluded due to incomplete or irrelevant information and poor handwriting. Data were analyzed using Microsoft Excel 2006.
Results
Patients characteristic and demographic profile
A total of 238 (79.33%) patients out of 300 were included for final analysis. Out of these 238, 120 (50.42%) were males. 178 (74.78%) were Hindu by religion, 53 (22.26%) were Muslim. 192 (80.27%) cases were from urban area while 46 (19.32%) were from rural area. Age wise distributions of all patients were shown in Table 1. Mean age of patients was 55.82±10.2 years (95% CI 54.5-57.1) with mean weight of 64.52±10.96 Kg (95% CI 62.8-66.2). Mean duration of diabetes was 8.2±6.8 years (95% CI 7.2-9.1). Detail characteristics like occupation, family income and education, and their treating doctor are shown in Table 2.
Table 1.
Age wise distribution of patients (n=238)
| Age (years) | No of patients (%) |
|---|---|
| 30-39 | 9 (3.78) |
| 40-49 | 50 (21.08) |
| 50-59 | 96 (40.33) |
| 60-69 | 59 (24.78) |
| 70-79 | 20 (8.40) |
| > 80 | 4 (1.68) |
Table 2.
Characteristics of patients with type 2 diabetes (n=238)
| Patients characteristics | Percentage |
|---|---|
| Occupation | |
| Students | 3.8 |
| Housewife | 43.90 |
| Service | 17.46 |
| Laborer | 35.77 |
| Annual income | |
| < 20,000 | 39.47 |
| Up to 50,000 | 27.19 |
| >50,000 | 33.33 |
| Treating doctor | |
| General practitioner | 17.69 |
| Physicians | 79.20 |
| Endocrinologist | 3.07 |
| Source of information | |
| Doctor | 76.44 |
| Media | 4.44 |
| Another persons | 19.11 |
| Internet | |
| Educations | |
| Illiterate | 36.64 |
| Up to school | 52.35 |
| Graduation | 10.99 |
Knowledge regarding diabetes
Despite 8 years of average duration of diabetes, about 46% of patients knew the pathophysiology of diabetes. Fewer (38.23%) still believed that diabetes can be cured. Many other aspects are covered in Table 3. Among the knowledge of complications of diabetes, renal complication was least known to patients. Most were afraid of heart related complications. Details of knowledge of complications depicted in Figure 1. Table 4 shows the responder knowledge regarding diet and exercises. Dietary modifications were relied more than exercises among the evaluated patients. Most of the lacunae in knowledge prevailed in drug therapy of diabetes. Insulin was disfavored by most of patients. Details of knowledge of drug therapy in diabetes are shown in Table 5.
Table 3.
Frequency distribution of respondent's knowledge regarding etiology and features diabetes
| Questions to assess knowledge | Correct answers (%) |
|---|---|
| What is diabetes? | 46.63 |
| What causes diabetes? | 17.64 |
| Can diabetes be cured? | 38.23 |
| How can diabetes be detected? | 82.77 |
| Features of diabetes: | |
| Polyuria | 58.82 |
| Can be Asymptomatic | 5.42 |
| Weight loss | 2.52 |
| Increase hunger | 5.88 |
| Recurrent infection | 43.28 |
| Is diabetes hereditary? | 57.98 |
| Is diabetes infectious? | 5.042 |
Figure 1.
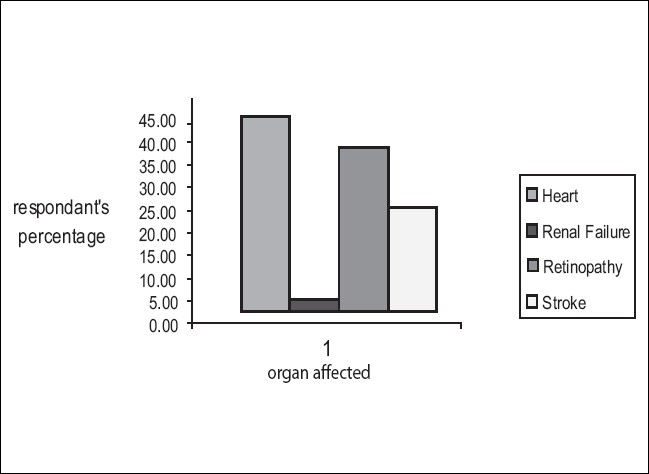
Frequency distribution of knowledge regarding complications of diabetes
Table 4.
Percentage of respondent's knowledge regarding exercise and diet in diabetes
| Knowledge of exercises and diet in diabetes | Percentage |
|---|---|
| What should be done to control DM? | |
| Exercises | 51.23 |
| Dietary modifications | 74.78 |
| Stop smoking/alcohol | 7.14 |
| Is exercise beneficial? | 83.16 |
| Exercises should be done by only obese person? | 84.05 |
| Bitter substances can cure DM | 53.37 |
Table 5.
Frequency distribution of respondent's knowledge of drug therapy in diabetes
| Once DM is controlled drugs should be stopped | 22.26% |
| Drug is more important than diet control | 51.26% |
| Insulin is to be avoided as far as possible | 48.31% |
| Herbal drugs are better | 39.49% |
| Insulin is habit forming | 51.68% |
Attitude and practices in diabetes
An encouraging part in our study was that most believed in self care in diabetes. Majority of the patients could not afford a blood glucose meter and hence, could not check their blood glucose level regularly. Practice of taking herbal drugs prevailed in approximately 40% of patients. Table 6 details the attitude and practices in our patients.
Table 6.
Frequency distribution of respondent's attitude and practice toward diabetes
| Respondent's attitude and practice | Percentage |
|---|---|
| Who is responsible for DM care? | |
| Your self | 65.12 |
| Doctor | 39.07 |
| Family | 34.03 |
| Do you include fruits in your diet regularly? | 54.21 |
| Do you take green leafy vegetables in diet? | 31.93 |
| Do you have glucometer? | 10.08 |
| Do you check your sugar regularly? | 70.16 (monthly) |
| Do you check your foot regularly? | 56 |
| Do you take herbal drugs? | 38.65 |
Appraisal of doctor by patients
Most patients were dissatisfied with the consultation time given by their treating doctors. The time given was less than 5 mins in nearly 50%. Foot care and watch for complications were least suggested by doctors [Table 7].
Table 7.
Frequency distribution of respondent's appraisal of their treating doctors
| How much time your doctor devotes to you? | |
| Five minutes | 43.27 |
| Ten minutes | 26.89 |
| More than 10 minutes. | 10.8 |
| Your doctor explains you diabetes thoroughly? | 85.29 |
| Does you doctor explain diet? | 85.29 |
| Does your doctor explain exercises? | 64.28 |
| Does your doctor check feet regularly? | 34.43 |
| Does your doctor motivate you for self care in diabetes? | 33.61 |
Discussion
Most studies regarding epidemiology and prevalence of diabetes were conducted from south India[9–12] and very few studies from north India.[13] There is no study regarding KAP is available for Saurastra region and hence, this study is in attempt to gather the data regarding the same.
Since the study conducted among patients with type 2, average age was between 50-59 years (40.33%) and average duration of diabetes among patients was 8.2years. nearly 60% of patients were from low socio-economical status and 36% were illiterate. Since the majority of patients were recruited from government-run hospitals, there may be bias regarding these two factors. Both affordability and literacy may be the problem in diabetes education and management. Education of vulnerable communities can become a cost-effective public health strategy. It has been shown that self-care among individuals with type 2 diabetes improved glycemic control[14] and reduced complications.[15]
American Diabetic Association has defined self management education as the process of providing the person with diabetes the knowledge and skill that is needed to perform self care, manage crises and make life style changes. National standard for self care management in diabetes has been set by Mensing[16]et al. To achieve such stanted self care patients and doctor should work together. There is emphasis on teaching pathophysiology and its relation with treatment, nutritional aspects, medications, complications, goal setting and psychosocial adjustments. Considering these standards, we formulated our questionnaire.
During evaluation of knowledge part, we found that most patients didn't know what diabetes is (63%) and what the consequences of diabetes are in the long run (nearly 60%). Our respondents only few knew that a common complications was heart attack. Another crucial finding of our study was limited knowledge of complications and importance of life style modification.
Three main findings of our study which may be responsible for low diabetes education among the patients were: 1) Nearly 40% of patients were below poverty line and hence could not afford even minimum standard care and therapy. 2) Only 3% of patients were treated by endocrinologists. This is because very few endocrinologists are available in Gujarat. None of them are available in government run hospital and, patients can not afford the private care. No single institute in Gujarat had superspeciality course on diabetology or endocrinology. There are a number of studies which showed that treatment by a diabetes specialist improves treatment outcomes compared to treatment by a generalist.[17–22] 3) Most important factor is low level of education, only 10% were graduate and nearly 37% were completely illiterate. Therefore, illiteracy may be the most important obstacle in diabetes management of such patients. It is rightly said that education of vulnerable communities can become a cost-effective public health strategy.[23]
Our study showed that people in Saurashtra region wrongly believe that diabetes can be cured with bitter substances and allopathic drugs are harmful to the body. They also have many misconceptions about insulin.
An encouraging part of the study is that although there was, quite low diabetes self education among patients, most of patients believed that they are responsible for their care and this implies that they were ready to change if motivated or educated properly.
Though it was not the aim of study, we studied the appraisal of doctors by their patients. The shocking fact was physicians could spare very limtied time for their patients and a search for complications was ignored by most. Foot care checking and self care motivation, the two main aspects of diabetes care were ignored by most of the treating practitioners. Though there are few studies regarding the cost analysis of diabetes in India, it is a proven fact that ignoring such vital aspects may increase cost steeply.[24] There are Indian standards set by Agrawal[25] and others on how to set up a diabetes clinic. There should be emphasized to strengthen the diabetic care.
Recommendations
Emphasis on improving the literacy rate of the population.
To increase the availability of endocrinologists.
Diabetes education must be imparted by every clinician as per standard norms.
Generalist or primary care physician should be enriched with more knowledge by CME and other programmes.
Media and Non Government Organisation should be involved in the daunting task of removing misbelieves, ignorance and instituting diabetes preventive measures in the community.
Acknowledgments
The help rendered by undergraduate students (Deval, Jilan and Parth) for entering data in to Microsoft excel is acknowledged.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Kuller LH. Dietary fat and chronic diseases epidemiologyc overview. J Am Diet Assoc. 1997;97:9–15. doi: 10.1016/s0002-8223(97)00724-4. [DOI] [PubMed] [Google Scholar]
- 2.Grol ME, HLLbi VT, Gersternbluth JF. Lifestyle in Curacao. Smoking, alcohol consumption, eating habits and exercise. West Indian Med J. 1997;46:8–14. [PubMed] [Google Scholar]
- 3.King H, Aubert RE, Herman W. Global burden of diabetes, 1995-2025. Diabetes Care. 1998;21:1414–31. doi: 10.2337/diacare.21.9.1414. [DOI] [PubMed] [Google Scholar]
- 4.Ramachandran A, Snehalatha C, Baskar AD, Mary S, Kumar CK, Selvam S, et al. Temporal Changes in Prevalence of Diabetes and Impaired Glucose Tolerance Associated With Life Style Transition Occurring in Rural Population in India. Diabetologia. 2004;47:860–5. doi: 10.1007/s00125-004-1387-6. [DOI] [PubMed] [Google Scholar]
- 5.Ramachandran A, Ramchandran S, Snehalatha C, Augustine C, Murugesan N, Viswanathan V, et al. Increasing Expenditure on Health Care Incurred by Diabetic Subjects in a Developing Country. Diabetes Care. 2007;30:252–6. doi: 10.2337/dc06-0144. [DOI] [PubMed] [Google Scholar]
- 6.Mazzuca SA, Moorman NH, Wheeler ML. The diabetes education study: a controlled trial of the effects of diabetes education. Diabetes care. 1986;9:1–10. doi: 10.2337/diacare.9.1.1. [DOI] [PubMed] [Google Scholar]
- 7.Madhu SV, Rao PV. Epidemiology of Diabetes mellitus in India. In: Tripathi BB, Chandalia HB, editors. RSSDI Textbook of Diabetes mellitus. 2nd ed. Hyderabad: RSSDI; 2008. pp. 209–26. [Google Scholar]
- 8.Ahuja MMS. Epidemiological studies in Diabetes mellitus in India. In: Ahuja MMS, editor. Epidemiology of diabetes mellitus in developing countries. New Delhi: Interprint; 1979. pp. 29–38. [Google Scholar]
- 9.Ramachandran A, Snehalatha C, Kapur A, et al. Diabetes Epidemiology Study Group in India (DESI): High prevalence of diabetes and impaired glucose tolerance in India: National Urban Diabetes Survey. Diabetologia. 2001;44:1094–101. doi: 10.1007/s001250100627. [DOI] [PubMed] [Google Scholar]
- 10.Kutty R, Soman CR, Joseph A, pisharody R, Vijaykumar K. Typer 2 Dibetes in sourthern kerala: Variation in prevalence in prevalavce among geographic devision within a reagion. Nat Med J India. 2000;13:287–92. [PubMed] [Google Scholar]
- 11.Ramachandran A, Jali MV, Mohan V, Snehlata C, Vishwanathan M. High prevelance of diabetes in an urban population of southern india. BMJ. 1988;297:587–90. doi: 10.1136/bmj.297.6648.587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ramachandran A, Snehalata C, Latha E, Vijav V, Vishwanathan M. Rising prevelance of NIDDM in urban population in India. Diabetologia. 1997;40:232–7. doi: 10.1007/s001250050668. [DOI] [PubMed] [Google Scholar]
- 13.Mishra A, Pandey RM, Ramadevi J. High prevelance of diabetes, obesity and dyslipidemia in urban slum population in northern India. Inter J Obesity. 2001;25:1–8. doi: 10.1038/sj.ijo.0801748. [DOI] [PubMed] [Google Scholar]
- 14.Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V. Indian Diabetes Prevention Programme (IDPP): The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1) Diabetologia. 2006;49:289–97. doi: 10.1007/s00125-005-0097-z. [DOI] [PubMed] [Google Scholar]
- 15.Heisler M, Pietee JD, Spencer M, Kieffer E, Vijan S. The relationship between knowledge of recent HbA1c values and diabetes care understanding and self-management. Diabetes Care. 2005;28:816–22. doi: 10.2337/diacare.28.4.816. [DOI] [PubMed] [Google Scholar]
- 16.Mencing C, Boucher J, Cypress M. National Standards for Diabetes self-Management Education. Diabetes care. 2006;29:S78–85. [PubMed] [Google Scholar]
- 17.Zgibor JC, Songer TJ, Kelsey SF, Weissfeld J, Drash AL, Becker D, et al. The association of diabetes specialist care with health care practices and glycemic control in patients with type 1 diabetes: a cross-sectional analysis from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetes Care. 2000;23:472–6. doi: 10.2337/diacare.23.4.472. [DOI] [PubMed] [Google Scholar]
- 18.Levetan CS, Passaro MD, Jablonski KA, Ratner RE. Effect of physician specialty on outcomes in diabetic ketoacidosis. Diabetes Care. 1999;22:1790–5. doi: 10.2337/diacare.22.11.1790. [DOI] [PubMed] [Google Scholar]
- 19.Ho M, Marger M, Beart J, Yip I, Shekele P. Is the quality of diabetes care better in a diabetes clinic or in a general medicine clinic? Diabetes Care. 1997;20:472–5. doi: 10.2337/diacare.20.4.472. [DOI] [PubMed] [Google Scholar]
- 20.Bloomfield S, Farquhar JW. Is a specialist paediatric diabetic clinic better? Arch Dis Child. 1990;65:139–40. doi: 10.1136/adc.65.1.139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Verlato G, Muggeo M, Bonora E, Corbellini M, Bressan F, de Marco R. Attending the diabetes center is associated with increased 5-year survival probability of diabetic patients: The Verona Diabetes Study. Diabetes Care. 1996;19:211–3. doi: 10.2337/diacare.19.3.211. [DOI] [PubMed] [Google Scholar]
- 22.Greenfield S, Rogers W, Mangotich M, Carney MF, Talov AR. Outcomes of patients with hypertension and non-insulin-dependent diabetes mellitus treated by different systems and specialties. JAMA. 1995;274:1436–44. [PubMed] [Google Scholar]
- 23.Balagopal P, Kamalamma N, Patel TG, Misra R. A Community-Based Diabetes Prevention and Management Education Program in a Rural Village in India Diabetes Care. 2008;31:1097–104. doi: 10.2337/dc07-1680. [DOI] [PubMed] [Google Scholar]
- 24.Shobhana R, Rama PR, Lavanya A, Vijay V. Ramachandran A: Cost burden to diabetic patients with foot complications: a study from southern India. J Assoc Physicians India. 2000;48:1147–50. [PubMed] [Google Scholar]
- 25.Agrawal Sk, Ganguli A, Kubaa S. The organization of diabetic clinics and research centers and the existing specialty diabetic clinics/centers and diabetes hospitals in India. In: Das S, Moses A, editors. Moses Manual on Diabetes Mellitus. New Delhi: IJCP group of publications; 2007. pp. 384–91. [Google Scholar]