

Abstract
Synopsis
OCD is a common debilitating condition affecting individuals from childhood through adult life. There is good evidence of genetic contribution to its etiology, but environmental risk factors also are likely to be involved. The condition probably has a complex pattern of inheritance. Molecular studies have identified several potentially relevant genes, but much additional research is needed to establish definitive causes of the condition.
Keywords: Obsessive-compulsive disorder, Genetics, Psychiatry
Obsessive-compulsive disorder (OCD) is a psychiatric condition first described 100 years ago[1]. The pathognomic features of the disorder are persistent, intrusive, senseless thoughts and impulses (obsessions) and repetitive, intentional behaviors (compulsions). Patients with the disorder recognize that their thoughts and behaviors are excessive and unreasonable, and they struggle to resist them. The lifetime prevalence of OCD is estimated to be 1–3%, based on population-based surveys conducted in many communities nationally and internationally[2;3]. Although the disorder affects individuals of all ages, the period of greatest risk is from childhood to early adulthood[4;5]. Patients experience a chronic or episodic course with exacerbations that can substantially impair social, occupational, and academic functioning; according to the World Health Organization, OCD is among the ten most disabling medical conditions worldwide[6]. Moreover, the burden placed on, and stresses experienced by, family members are considerable[7]. Medications and behavioral therapy can partially control symptoms, but the course is chronic or relapsing in most cases, and cure is rare.
There is compelling evidence for a biological basis of OCD. First, obsessions and compulsions are common in several medical conditions, including Huntington’s chorea, encephalitis lethargica (von Economo’s encephalitis), Parkinson’s disease, Tourette disorder, schizophrenia, Sydenham’s chorea, certain epilepsies, and insults to specific brain regions due to trauma, ischemia, and tumors [8]. Second, serotonin reuptake inhibitors (clomipramine) and selective serotonin reuptake inhibitors (e.g., fluoxetine, fluvoxamine, and sertraline) have demonstrated efficacy in controlling obsessions and compulsions.[9;10]. Third, functional imaging studies have revealed increased metabolic activity in specific brain regions of patients with OCD, at rest and when challenged with stimuli that provoke obsessions and compulsions[11].
Evidence implicating cortico-striatal-thalamic-cortico (CSTC) pathways in the manifestation of the disorder is accumulating[12;13], and the neurocircuitry models of OCD are the most developed of any neuropsychiatric disorder. There has been a considerable body of neuroimaging[14], and to a lesser extent, cognitive neuroscience research in this area[15]. Although a primary pathological process underlying core OCD symptoms has not yet been definitively identified, functional imaging studies have established that metabolism or perfusion in CSTC circuits is affected. Further, MRI and MR spectroscopy studies in OCD also suggest striatal pathology. Influential theories suggest that these patterns of activity arise from failed striato-thalamic inhibition[13]. Therefore, genes affecting development, connectivity, and neurotransmission and signal transduction in CSTC circuits are natural foci of interest.
Neuropharmacological hypotheses of OCD pathophysiology have been greatly influenced by strong evidence that serotonergic systems modulate OCD symptomatology. Interestingly, both the serotonin transporter and the serotonin receptor subtypes implicated in OCD are at their highest levels in the brain in the ventral striatum[16] where they could influence the functioning of the CSTC circuits. In theory, other neurotransmitter systems within CSTC circuits, individually or via their interactions, may play a role in susceptibility, course, or response to OCD treatment. For example, dopaminergic mechanisms have been implicated by controlled studies demonstrating that neuroleptics are beneficial when added to ongoing SRI treatment[17;18]. Other CSTC neurotransmitter systems that are candidates for involvement in OCD on the basis of their anatomical localization or functional roles in CSTC circuits include glutamate, GABA, Substance P, cholinergic, and endogenous opioid systems[13;19;20].
The discovery of the genetic etiology of obsessive-compulsive disorder (OCD) is our best hope at present of unraveling the pathophysiology of this condition. There is compelling evidence that the disorder has a genetic basis. In contrast, other than the reported relationship of streptococcal infection in a subset of OCD[21] cases, there are no current environmental hypotheses with strong empirical support. The discovery of genes is crucial for elucidation of pathogenic mechanisms and for developing rational treatments.
Genetic Epidemiology
Since the early years of the twentieth century, clinicians have suspected that heredity plays an important role in the development of OCD. One of the first reports in the English literature was based on fifty cases of ‘obsessional neurosis’ treated at the Maudsley Hospital in London. 37% of parents and 21% of siblings of cases were diagnosed with this disorder[22]. The findings from the Hopkins OCD family study are remarkably similar[23]. There have been over 15 family studies of OCD, and most support the familial transmission of OCD [24-32]. Black et al.,[33] found that the age-corrected morbid risk of “broadly defined OCD” (i.e., OCD plus sub-syndromal obsessive-compulsive symptoms) was substantially greater in the parents of OCD probands as compared to those of controls (16% vs 3%). Pauls et al[34]. found that the morbid risk of OCD was significantly greater in first-degree relatives of OCD subjects as compared to relatives of psychiatrically normal controls (10% vs 1.9%); they found similar results for the morbid risks of OCD plus subthreshold OCD (18% vs 4%). The Hopkins OCD family study [23] found that the prevalence of OCD in the first-degree relatives of case probands was 11.7%, compared to 2.7% in the relatives of controls; also the prevalence of OCD in the siblings of early onset probands was 17.9% (λsib =7.8) within the range of other psychiatric disorders, such as bipolar disorder and panic disorder.
Family studies report prevalence rates of 7% to 15% in first-degree relatives of child and adolescent probands with OCD [28;29;31;35]., These findings are consistent with reports of an increased familial loading in probands with early age at onset. Pauls et al [34] reported a significantly higher morbid risk of OCD in the relatives of probands with an onset age less than 19 years. In the Hopkins OCD Family Study, there were no secondary cases of OCD in the families of probands with an age at onset greater than 17 years: the prevalence of OCD in all relatives of probands with an onset before eighteen was 13.8%, compared to 0% in probands with older age at onset (p=0.006). Hanna et al [36] reported a risk ratio (λsib=8.7) in a family study of early onset OCD probands, similar to our finding (λsib =7.8) in that subgroup. Finally, results from a recent study of families ascertained through children and adolescents with OCD, are consistent with these findings; the estimated odd ratios for OCD in first degree relatives was 32.5 (95% CI, 4.5–230.8)[37]. Early age at onset differentiates a strongly inherited subtype in other conditions[35;38] and has been fruitfully employed in the sub-classification of disorders such as schizophrenia,[39] breast cancer,[40;41] and Alzheimer’s disease[42].
Since Lewis’ first report in 1936 [22], there have been several reports of monozygotic twins concordant for obsessive-compulsive symptoms[43-46]. One series reported a concordance of 80% in monozygotic (MZ) twin pairs, as compared to 50% in dizygotic (DZ) pairs[47]. Carey and Gottesman[48] reported concordance rates in MZ and DZ twin pairs of 87% and 47%, respectively, giving a heritability estimate of 80%. Overall, in the twin studies published to date, 54 of 80 MZ twin pairs (68%) were reported as concordant, as compared to 9 of 29 DZ twin pairs (31%). In larger studies, in which diagnoses were questionnaire-derived, moderate heritabilities were found[49-51]. There have been no adoption studies in OCD.
Published segregation analyses of OCD implicate a gene of major effect in the etiology of OCD. Nicolini et al.[52] concluded that their family data are most consistent with a highly penetrant dominant major gene. In a more recent study, based on a much larger sample, the data best fit a dominant model of transmission[53]. Alsobrook et al.[54] reported statistical evidence for transmission consistent with genetic models; no specific model fit the data better than any other. However, when they analyzed a subset of 52 families in which at least two individuals were affected with OCD, they found that models of no inheritance, polygenic inheritance and single locus inheritance could all be statistically rejected and that the most parsimonious explanation for the inheritance patterns in these families was a mixed model of inheritance. Segregation analyses of the Hopkins OCD Family Study data strongly rejected sporadic and environmental models whereas Mendelian dominant and codominant models could not be rejected[55].
Candidate Gene Studies
Candidate genes for association studies have been selected based on knowledge of the pathophysiology and pharmacology of the condition. The serotonergic system has been a primary focus. The 5-HTTLPR serotonin transporter[56-62], 5HT1-D beta serotonin receptor gene [63;64], 5HT2A serotonin receptor; [65-67], and the serotonin 5HT2C receptor [68] have all been investigated with several positive studies; Murphy et al., [69] have recently shown, in two independent families, that a novel, uncommon gain-of-function missense variant in the serotonin transporter coding region (SLC6A4-Ile425Val) was associated with OCD plus comorbid disorders (anorexia nervosa, Asperger’s syndrome/autism). This finding is intriguing since the probands and their siblings who had the coding region variant and the more highly transcribed allele of the serotonin transporter promoter polymorphism had OCD of unusual severity and treatment resistance, suggesting a possible ‘double-hit’ effect of two variants that increase transporter function[69]. This finding has been supported in two more recent studies of OCD families [70;71]. However, this particular variant may play a role in only a small number of affected families. Also, Goldman and colleagues [72]. have observed the overtransmission of the L(a) allele to individuals with OCD. However, these findings have not been consistently replicated, and recent family-based and case-control association studies have not found associations with serotonin transporter, trypophan hydroxylase, or serotonin 1B, 2A, or 1D-beta receptor polymorphisms [63;66;73].
An association between OCD and a repeat in the dopamine receptor type 4 (DRD4) gene has been found by some[74;75], while others have reported suggestive evidence (not quite statistically significant). Associations have not been found between OCD and the dopamine D2 receptor[61;76;77], except in individuals with OCD and tics[78]. Associations were not found for the DRD3 dopamine receptor[76;77], or the dopamine transporter[61;63].
Karayiorgou et al.[79] reported that OCD is associated with a low-activity allele of an enzyme involved in the degradation of dopamine, catechol-O-methyltransferase (COMT), particularly in male probands. Niehaus et al.[80] found that the heterozygous genotype was more frequent in OCD patients, but these results have not been confirmed. [81-83]. In contrast to Karyiorgou et al., Alsobrook et al. found an association between COMT and OCD in females but not males[84]. Similarly, OCD was found to be associated with monoamine oxidase A (MAO-A) in male subjects in one study[85] but female subjects in another[58]. Recently, there have been reported associations between OCD and the BDNF locus[86], glutamate (NMDA) subunit receptor gene[87], GABA type B receptor 1 (GABBR1) gene has been observed to be overtransmitted at the A-7265G polymorphism[88], OLIG2 [89] and myelin oligodendrocyte glycoprotein (MOG) gene [69;90].
In summary, the limited state of knowledge about pathophysiological pathways and networks of interacting genes in OCD, and conflicting results from association studies, makes it premature to restrict our focus to associations of OCD with specific candidate genes.
A productive research approach has been to identify and study animal models relevant to OCD. Welch et al [91] showed that mice with a genetic deletion of Sapap3 (a postsynaptic scaffolding protein at excitatory synapses) exhibited compulsive grooming behavior leading to facial hair loss and skin lesions. These behaviors were alleviated by a selective serotonin reuptake inhibitor. Electrophysiological, structural and biochemical studies of Sapap3-mutant mice revealed defects in cortico-striatal synapses. Sequencing exons and exon/intron junctions of the SAPAP3 gene in 165 OCD and trichotillomania (TTM) samples revealed six nonsynonymous changes [92]. Furthermore, Bienvenu et al.[93] showed evidence for association for a SNP in the Sapap3 gene in a sample of ‘grooming disordered’ patients with OCD.
Linkage Studies
There have been only three genome-wide linkage studies of OCD. In 56 relatives in seven families ascertained through pediatric probands, Hanna et al [36] found suggestive linkage to a region near the telomere of chromosome 9 (9p24;LOD 1.97). The JHU group replicated this finding in fifty families, finding linkage peaks within 0.5 cM (<350 kb) of the original 9p24 linkage signal[94]. Subsequently, five independent groups have replicated evidence for association within SLC1A1, a glutamatergic transporter gene in that region [95-99]. In a sequencing experiment of this gene, Wang et al, 2009 identified one nonsynonymous coding SNP in a single family (c.490A>G, T164A) [100].
The largest linkage scan for OCD was conducted by the OCD Collaborative Genetics Study (OCGS; including Johns Hopkins, UCLA, Columbia, Brown, and Harvard Universities, and NIMH) group. Genotyping for the OCGS was performed at the Center for Inherited Disease Research (CIDR) using 386 microsatellite markers spaced at an average of 9 cM across the genome. For the whole genome scan, 1,008 subjects in 219 families were genotyped. The analysis was conducted using a non-parametric linkage (NPL) method [101] implemented in the analysis program Merlin. Both Kong and Cox LODall and Kong and Cox LODpairs statistics were computed, and empirical p-values for all “significant signals” were computed with Merlin using 10,000 replicates. The genome-scan results for multiple point analysis are presented in the figure below. The locations of the chromosomal regions are shown on the X-axis, and the statistical significance of the linkage signals (in units of -log of the p-values) are shown on the Y-axis.
The multipoint non-parametric analyses showed suggestive linkage regions on chromosomes 1 (p-value = 0.003) and 3 (p-value =0.0002). The highest Kong and Cox LOD score of 2.67 (asymptotic p-value of 0.0002) was obtained at marker D3S2398). We also computed an empirical p-value for a marker situated at this location using the same allele frequencies and 10,000 replicates. The chance of observing a Kong and Cox LOD score of 2.67 was 4 in 10,000, making it unlikely that this is a chance finding.
More recently, Hanna et al. [103] conducted a genome-wide linkage scan in 121 individuals from 26 families ascertained through probands with early-onset OCD. They found suggestive evidence for linkage on chromosome 10p15. They also found association with three SNPs in a gene in this linkage region, ADAR3.
Employing OCD Subtypes
The limited success identifying genetic determinants for OCD may be related to the etiological heterogeneity of OCD. Multiple approaches have been proposed to delineate more etiologically homogeneous groups within the broader definition of the disorder. Below we address some of the possible subtypes that may usefully be employed to identify genetic etiologies.
Age at onset (AAO) has proven useful in the clinical categorization of patients with respect to their genetic risk. Results from the Hopkins OCD Family Study and the Childhood OCD Family Study suggest an inverse relationship between age of onset of OCD in probands, and the risk of OCD in relatives. This is consistent with findings from other family studies[34;36]. We found a significant inverse relationship between the proband’s AAO and the prevalence of OCD in their first-degree relatives (odds per year = 0.92 (0.85–0.99), p=0.02). Interestingly, this relationship was found for relatives of female, but not male, probands.
In addition to the increased familial risk, early-onset OCD has been distinguished from later-onset OCD, based on the nature of the OCD symptoms [104], patterns of comorbidity [105;106], course and treatment response[107],and regional cerebral blood flow in frontal-subcortical circuits.[108] Unfortunately, no twin study has compared age-at-onset concordance patterns. To date, there is no clinical or other type of variable with stronger support in OCD.
Family studies found that AAO of OCD before18 years indicates a substantially more familial subgroup[23;33;34]. Using familiality as the outcome measure, the Hopkins group found evidence that an AAO earlier than 18 years was more useful than the standard phenotype[23;33;34]. In the linkage study described above, age of onset was used as a covariate in covariate-based linkage analysis. The LOD score was 2.94 at D1S1679 (empirical P-value = 0.001). After stratifying the sample by age at onset it was determined that it was younger age at onset that increased the linkage estimate[109].
Given our previous work of differential penetrance by gender (segregation analysis), we stratified the sample based on proband gender (78 male proband families; 141 female proband families), with a subsequent substantial increase in the linkage signal at 11p15[110]. After genotyping additional microsatellite markers, at approximately a 1–2cM density, from 2.8cM to 15cM, the stratified analyses showed a LOD= 5.66 (p<0.00001) in the male group. This first stage fine-mapping reduced the 1-LOD support interval from 25.9Mb to 4Mb. This region contains plausible candidate genes, such as Dopamine D4 receptor (DRD4), Tyrosine Hydroxylase (TH), Neuronal Nicotinic, Alpha Polypeptide 10 (CHRNA10), and the Cholecystokinin B Receptor (CCKBR), amongst others.
In addition to age at onset and gender, several clinical features potentially may be useful for categorizing OCD into homogeneous phenotypes for etiologic investigation. Clinical characteristics that may distinguish a familial subtype of OCD include: tic disorders [34;111;112], affective and anxiety disorders[33;113;114], obsessive-compulsive personality disorder[115], and specific obsessive-compulsive symptom classes[116-119].
In a large sample of multiply-affected families, we identified three OCD classes: OCD ‘Simplex’, Comorbid OCD ‘tic-related’, and comorbid OCD “affective-related.” These classes suggest that the co-occurrence of other psychiatric disorders (e.g. tics, anxiety, and affective disorders) with OCD may be indicative of different phenotypic subgroups [131]. It is possible that one or more of the above OCD subtypes represents a more homogenous genetic group yielding greater ability to detect genetic variation relevant to the disorder. The tic-related group points to the widely investigated relationship between Tourette Disease (TS) and OCD. There is compelling evidence that OCD is a familially related phenotype in families with TS [132]. However, it has not been established whether those individuals with OCD in TS families share, or do not share, a genetic etiology with other cases of OCD.
Several groups have reported that OCD subjects with hoarding behaviors are clinically distinct from other individuals with OCD[120-123]. The Hopkins OCD Family Study also found that relatives of hoarding OCD probands had a higher prevalence of hoarding behaviors[124].
In addition to subtyping by individual clinical features, it may be fruitful to subtype based on symptom clusters. Consistent with several prior studies[125], our research group found four or five OCD symptom dimensions using different statistical approaches on data collected with the Y-BOCS symptom checklist. In 221 OCD-affected individuals examined during the JHU OCD Family Study, Cullen et al[126], using dichotomous factor analysis of 16 YBOCS symptom categories, found four symptom factors: aggressive/sexual/ religious obsessions; contamination/cleaning; symmetry/order and hoarding. These dimensions were differentially associated with onset of symptoms, treatment responsiveness, and comorbid diagnoses, as well as magnitude of sib-sib correlation[126]. Similar dimensions were evident using principal components factor analysis of YBOCS symptom checklist categories in 418 OCD-affected individuals (251 affected sibling pairs) ascertained during the OCD Collaborative Genetics Study. These factors had significant sib-sib correlations, with the hoarding dimension being the most familial[127]. More recently, using exploratory dichotomous factor analysis on individual YBOCS symptom checklist items in 485 adults ascertained in the OCGS, we found similar dimensions (as well as a taboo factor) and strong sib-sib correlations, especially for the hoarding factor[128]. This structure has been replicated in children and adolescents[129].
It has been reported that OCD subjects with hoarding behaviors were clinically different from other OCD subjects, and that hoarding was more frequent in their first-degree relatives[124]. When families were stratified based on the presence of two or more relatives with compulsive hoarding (74 hoarding families; 145 non-hoarding families), we found suggestive linkage for the stratum with hoarding (LOD= 2.99; p= 0.0001).[130]. The 1-LOD support region at 14q31-32 is 10.9Mb. This region contains the positional candidate genes Potassium Channel, Voltage-Gated, Subfamily H, Member 5 (KCNH5), Potassium Channel, Subfamily K, Member 10 (KCNK10), Estrogen Receptor 2 (ESR2), Neurexin 3 (NRXN3), and others. These analyses were repeated using OCD hoarding as the phenotypic outcome (i.e., ONLY subjects with OCD hoarding, regardless of the presence of any other OCD symptoms were the affected phenotype). This reduced the number of informative families to an N =60 but still there was a signal (LOD =1.6; p =0.003), albeit the peak was marginally proximal to the one using the stratified sample. The linkage signal on the X chromosome, when stratified for compulsive hoarding, was strengthened considerably (LOD=2.81, p=0.0002) suggesting that these two chromosomal regions are likely to harbour susceptibility genes for compulsive hoarding.
Intermediate Phenotypes
Another phenotypic approach to OCD genetics is through the use of intermediate phenotypes. Recently, measures of specific cognitive domains have been found to be associated with OCD; moreover, several studies have shown the familial nature of the measures in OCD such that unaffected relatives of probands with OCD also have abnormalities on these measures [133-135]. Cognitive measures investigated in OCD have attempted to address both the clinical characteristics of the phenomena (obsessions & compulsions) and the brain regions implicated in OCD. This is illustrated by the executive task ‘set shifting,’ which is intended to measure the apparent inability of the OCD patient to stop repetitive behaviors.Tests of this process (e.g. the Wisconsin Card Sort (WCS) have been found to be impaired in OCD patients and their unaffected first-degree relatives [136]. Other tasks involve impaired decision making, also considered a hallmark of OCD. The Iowa Gambling Task aims to simulate real-life decision-making and is known to be sensitive to frontal lobe dysfunction. OCD patients are impaired in completing this task, however there are some negative findings [137-139]. Response inhibition deficits have been reported in OCD patients when performing the Stop Signal Reaction Time (SSRT), which measures the time taken to internally suppress pre-potent motor responses [140]. Unaffected first-degree relatives of OCD patients are also impaired on this task compared with unrelated healthy controls, suggesting that response inhibition may be an endophenotype for OCD. Menzies et al [135] showed that two anatomical brain systems; a parieto-cingulo-striatal system (increased grey matter), and a predominantly fronto-temporal system including OFC and inferior frontal gyri (decreased grey matter), were associated with impairment on the SSRT, in both OCD patients and their unaffected first-degree relatives, compared with healthy controls. Recently, Chamberlain et al (2008) [134] found that a reversal learning paradigm, the facilitation of behavioral flexibility after negative feedback, distinguished both OCD patients and their unaffected relatives from controls and was associated with abnormally reduced activation of several cortical regions, including the lateral orbitofrontal cortex, suggesting another potential OCD endophenotype.
It seems plausible that, like other neuropsychiatric conditions, OCD is an etiologically heterogeneous condition, and that in addition to genetic causes (involving one or more major genes and several genes of smaller effect), there are environmental causes (e.g., trauma and infection), and gene-by-environmental interaction that are all involved in the emergence of the disorder.
Future Directions
With advances in analytic and molecular genetic technology today, investigators are faced with several options to identify the genetic causes of diseases. The field has been enormously successful identifying genes responsible for Mendelian disorders; however, complex genetic conditions have been less tractable to study. Linkage studies remain the design of choice for rare, highly penetrant conditions with genes of major effect. For disorders accounted for by genes of modest effect, linkage studies have been less rewarding. In fact, the sample size required for detecting genes of small effect by linkage is prohibitively large. In contrast, association studies are promising for detecting genetic variants of modest effect[120]. Genome-wide association studies are now feasible and, as Carlson et al[141] state, “the technical, informatic, and statistical foundations have been laid for whole genome analyses.” Indeed, there are several recent examples of the success of the genome-wide association approach. For example, although Hirschsprung Disease is a well-studied condition with eight identified mutations, a genome-wide association study identified a chromosomal region not previously known to be related to the disorder, and epistasis between two known genes was detected and confirmed in an animal model[142]. More recently, investigators compared 96 cases with age-related macular degeneration (AMD) to 50 control subjects at 116,204 SNPs [143] and found a highly significant association with the CFH gene, which was located within a region of previously reported linkage to AMD. Two WGAs for OCD are in progress, and we are hopeful that findings from these studies will inform our understanding of the etiology of OCD.
There are limitations to the association approach. A negative linkage-disequilibrium result in a particular genomic region does not exclude a significant gene effect in that region. It may be that the SNPs used through the region are too widely spaced to detect the extent of LD in the region. Thus, in a genome-wide random SNP approach, even at high density, disease-causing genes might be missed[144]. Moreover, while LD is useful in identifying common variants affecting disease susceptibility, if there are many rare susceptibility variants at a disease locus, LD is unlikely to be useful to identify the locus [145].
In summary, OCD is a complex genetic disorder with unknown genetic and environmental bases; There are likely common genetic influences of modest effect (possibly in addition to other less common genetic factors); and many of these genetic determinants have probably not been detected using traditional linkage methodologies. Moreover, the biological basis of OCD is largely unknown, preventing a more focused genetic search in particular metabolic pathways. We recognize the merits of gene-based association studies, [146] but this is premature in OCD. There are biological hypotheses regarding the pathophysiology of OCD, and a few studies have found associations with candidate genes; however, these studies have had limited power, results have not been replicated, and the available evidence does not support a sustainable biological hypothesis. We are awaiting the results of GWA studies using dense genome-wide SNP panels to identify SNPs and ultimately genes associated with OCD in biologically plausible pathways. The optimal approach in determining genetic variants relevant to OCD will require a variety of strategies, some of which are in progress and others of which have yet to be applied to this condition. These strategies will involve improved understanding of the phenotype from both clinical and cognitive perspectives, approaching investigations from an epigenetic perspective, searching for copy number variations in the genome, and employing deep genetic sequencing techniques.
The identification of genetic and environmental causes of OCD should ultimately be of substantial benefit to those that suffer from this debilitating condition. The expectation is that rational treatments will become available and preventive measures will be possible.
Figure 1.
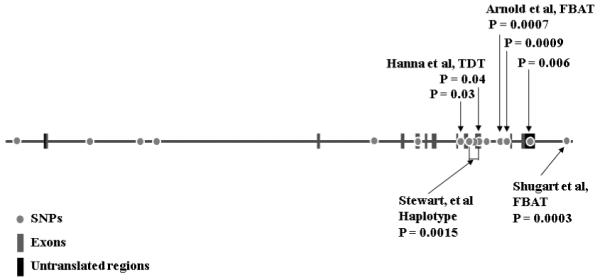
Results of association studies of SLC1A1 in OCD.
Figure 2.

Linkage results from the OCGS.
Acknowledgements
Supported by National Institutes of Health grants R01-MH-50214 R01-MH-071507, and NCRR/OPD-GERCRR00052.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Interest: None
Bibliography and References Cited
- 1.Janet P. Les Obsessions et al Psychasthenie. Bailliere; Paris: 1903. [Google Scholar]
- 2.Karno M, Golding JM. Obsessive compulsive disorder. In: Robins LN, Regier DA, editors. Psychiatric Disorders in America. Free Press; New York: 1991. pp. 204–219. [Google Scholar]
- 3.Weissman MM, Bland RC, Canino GJ, et al. The Cross National Collaborative Group The cross national epidemiology of obsessive compulsive disorder. J.Clin.Psychiatry. 1994;55(Suppl):5–10. [PubMed] [Google Scholar]
- 4.Nestadt G, Samuels JF, Romanoski AJ, et al. Obsessions and compulsions in the community. Acta Psychiatr.Scand. 1994;89:219–224. doi: 10.1111/j.1600-0447.1994.tb01504.x. [DOI] [PubMed] [Google Scholar]
- 5.Nestadt G, Bienvenu OJ, Cai G, et al. Incidence of obsessive-compulsive disorder in adults. J.Nerv.Ment.Dis. 1998;186:401–406. doi: 10.1097/00005053-199807000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Murray CL, Lopez AD. The Global Burden of Disease. Harvard University Press; Cambridge: 1996. [Google Scholar]
- 7.Steketee G. Disability and family burden in obsessive-compulsive disorder. Can.J.Psychiatry. 1997;42:919–928. doi: 10.1177/070674379704200902. [DOI] [PubMed] [Google Scholar]
- 8.Stein DJ. Advances in the neurobiology of obsessive-compulsive disorder. Implications for conceptualizing putative obsessive-compulsive and spectrum disorders. Psychiatr.Clin.North Am. 2000;23:545–562. doi: 10.1016/s0193-953x(05)70180-5. [DOI] [PubMed] [Google Scholar]
- 9.Clomipramine Collaborative Study Group. The Clomipramine Collaborative Study Group Clomipramine in the treatment of patients with obsessive-compulsive disorder. Arch.Gen.Psychiatry. 1991;48:730–738. doi: 10.1001/archpsyc.1991.01810320054008. [DOI] [PubMed] [Google Scholar]
- 10.Goodman WK, Price LH, Rasmussen SA, et al. Efficacy of fluvoxamine in obsessive-compulsive disorder. A double-blind comparison with placebo. Arch.Gen.Psychiatry. 1989;46:36–44. doi: 10.1001/archpsyc.1989.01810010038006. [DOI] [PubMed] [Google Scholar]
- 11.Hoehn-Saric RGB. Psychobiology of obsessive-compulsive disorder: anatomical and physiological considerations. International Review of Psychiatry. 1997;9:15–29. [Google Scholar]
- 12.Rauch SL, Savage CR, Alpert NM, et al. Probing striatal function in obsessive-compulsive disorder: a PET study of implicit sequence learning. J.Neuropsychiatry Clin.Neurosci. 1997;9:568–573. doi: 10.1176/jnp.9.4.568. [DOI] [PubMed] [Google Scholar]
- 13.Saxena S, Rauch SL. Functional neuroimaging and the neuroanatomy of obsessive-compulsive disorder. Psychiatr.Clin.North Am. 2000;23:563–586. doi: 10.1016/s0193-953x(05)70181-7. [DOI] [PubMed] [Google Scholar]
- 14.Saxena S, Brody AL, Schwartz JM, et al. Neuroimaging and frontal-subcortical circuitry in obsessive-compulsive disorder. Br.J.Psychiatry Suppl. 1998:26–37. [PubMed] [Google Scholar]
- 15.Rauch SL. Neuroimaging and neurocircuitry models pertaining to the neurosurgical treatment of psychiatric disorders. Neurosurg.Clin.N.Am. 2003;14:213–viii. doi: 10.1016/s1042-3680(02)00114-6. [DOI] [PubMed] [Google Scholar]
- 16.Hoyer D, Pazos A, Probst A, et al. Serotonin receptors in the human brain. I. Characterization and autoradiographic localization of 5-HT1A recognition sites. Apparent absence of 5-HT1B recognition sites. Brain Res. 1986;376:85–96. doi: 10.1016/0006-8993(86)90902-9. [DOI] [PubMed] [Google Scholar]
- 17.McDougle CJ, Goodman WK, Leckman JF, et al. Haloperidol addition in fluvoxamine-refractory obsessive-compulsive disorder. A double-blind, placebo-controlled study in patients with and without tics. Arch.Gen.Psychiatry. 1994;51:302–308. doi: 10.1001/archpsyc.1994.03950040046006. [DOI] [PubMed] [Google Scholar]
- 18.McDougle CJ, Epperson CN, Pelton GH, et al. A double-blind, placebo-controlled study of risperidone addition in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2000;57:794–801. doi: 10.1001/archpsyc.57.8.794. [DOI] [PubMed] [Google Scholar]
- 19.Carlsson ML. On the role of cortical glutamate in obsessive-compulsive disorder and attention-deficit hyperactivity disorder, two phenomenologically antithetical conditions. Acta Psychiatr.Scand. 2000;102:401–413. doi: 10.1034/j.1600-0447.2000.102006401.x. [DOI] [PubMed] [Google Scholar]
- 20.Haber SN, McFarland NR. The concept of the ventral striatum in nonhuman primates. Ann.N.Y.Acad.Sci. 1999;877:33–48. doi: 10.1111/j.1749-6632.1999.tb09259.x. [DOI] [PubMed] [Google Scholar]
- 21.Leonard HL, Swedo SE. Paediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) Int.J.Neuropsychopharmacol. 2001;4:191–198. doi: 10.1017/S1461145701002371. [DOI] [PubMed] [Google Scholar]
- 22.Lewis A. Problems of obsessional illness. Proc Roy Soc Med. 1936;29:325–336. doi: 10.1177/003591573602900418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nestadt G, Samuels J, Riddle M, et al. A family study of obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2000;57:358–363. doi: 10.1001/archpsyc.57.4.358. [DOI] [PubMed] [Google Scholar]
- 24.Bellodi L, Sciuto G, Diaferia G, et al. Psychiatric disorders in the families of patients with obsessive-compulsive disorder. Psychiatry Res. 1992;42:111–120. doi: 10.1016/0165-1781(92)90075-e. [DOI] [PubMed] [Google Scholar]
- 25.Brown FW. Heredity in the psychoneuroses. Proceedings of the Royal Society of Medicine. 1942;35:785–790. doi: 10.1177/003591574203501215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hoover CF, Insel TR. Families of origin in obsessive-compulsive disorder. J.Nerv.Ment.Dis. 1984;172:207–215. doi: 10.1097/00005053-198404000-00004. [DOI] [PubMed] [Google Scholar]
- 27.Insel TR, Hoover C, Murphy DL. Parents of patients with obsessive-compulsive disorder. Psychol.Med. 1983;13:807–811. doi: 10.1017/s0033291700051515. [DOI] [PubMed] [Google Scholar]
- 28.Lenane MC, Swedo SE, Leonard H, et al. Psychiatric disorders in first degree relatives of children and adolescents with obsessive compulsive disorder. J.Am.Acad.Child Adolesc.Psychiatry. 1990;29:407–412. doi: 10.1097/00004583-199005000-00012. [DOI] [PubMed] [Google Scholar]
- 29.Leonard HL, Lenane MC, Swedo SE, et al. Tics and Tourette’s disorder: a 2- to 7-year follow-up of 54 obsessive-compulsive children. Am.J.Psychiatry. 1992;149:1244–1251. doi: 10.1176/ajp.149.9.1244. [DOI] [PubMed] [Google Scholar]
- 30.Rasmussen SA, Tsuang MT. Clinical characteristics and family history in DSM-III obsessive-compulsive disorder. Am.J.Psychiatry. 1986;143:317–322. doi: 10.1176/ajp.143.3.317. [DOI] [PubMed] [Google Scholar]
- 31.Riddle MA, Scahill L, King R, et al. Obsessive compulsive disorder in children and adolescents: phenomenology and family history. J.Am.Acad.Child Adolesc.Psychiatry. 1990;29:766–772. doi: 10.1097/00004583-199009000-00015. [DOI] [PubMed] [Google Scholar]
- 32.Rosenberg CM. Familial aspects of obsessional neurosis. Br.J.Psychiatry. 1967;113:405–413. doi: 10.1192/bjp.113.497.405. [DOI] [PubMed] [Google Scholar]
- 33.Black DW, Noyes R, Jr., Goldstein RB, et al. A family study of obsessive-compulsive disorder. Arch.Gen.Psychiatry. 1992;49:362–368. doi: 10.1001/archpsyc.1992.01820050026004. [DOI] [PubMed] [Google Scholar]
- 34.Pauls DL, Alsobrook JP, Goodman W, et al. A family study of obsessive-compulsive disorder. Am.J.Psychiatry. 1995;152:76–84. doi: 10.1176/ajp.152.1.76. [DOI] [PubMed] [Google Scholar]
- 35.Swedo SE, Rapoport JL, Leonard H, et al. Obsessive-compulsive disorder in children and adolescents. Clinical phenomenology of 70 consecutive cases. Arch.Gen.Psychiatry. 1989;46:335–341. doi: 10.1001/archpsyc.1989.01810040041007. [DOI] [PubMed] [Google Scholar]
- 36.Hanna G. Abstract. Biological Psychiatry Conference; May 2000 2004. [Google Scholar]
- 37.do Rosario-Campos MC, Leckman JF, Curi M, et al. A family study of early-onset obsessive-compulsive disorder. Am.J.Med.Genet.B Neuropsychiatr.Genet. 2005 doi: 10.1002/ajmg.b.30149. [DOI] [PubMed] [Google Scholar]
- 38.Childs B, Scriver CR. Age at onset and causes of disease. Perspect.Biol.Med. 1986;29:437–460. doi: 10.1353/pbm.1986.0056. [DOI] [PubMed] [Google Scholar]
- 39.Pulver AE, Liang KY. Estimating effects of proband characteristics on familial risk: II. The association between age at onset and familial risk in the Maryland schizophrenia sample. Genet.Epidemiol. 1991;8:339–350. doi: 10.1002/gepi.1370080506. [DOI] [PubMed] [Google Scholar]
- 40.Claus EB. Monographs of the National Cancer Institute. 1994. Genetic epidemiology of breast cancer in younger women; pp. 49–53. [PubMed] [Google Scholar]
- 41.Hall JM, Lee MK, Newman B, et al. Linkage of early-onset familial breast cancer to chromosome 17q21. Science. 1990;250:1684–1689. doi: 10.1126/science.2270482. [DOI] [PubMed] [Google Scholar]
- 42.Roses AD. Alzheimer diseases: a model of gene mutations and susceptibility polymorphisms for complex psychiatric diseases. Am.J.Med.Genet. 1998;81:49–57. doi: 10.1002/(sici)1096-8628(19980207)81:1<49::aid-ajmg10>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 43.Cryan EM, Butcher GJ, Webb MG. Obsessive-compulsive disorder and paraphilia in a monozygotic twin pair. Br.J.Psychiatry. 1992;161:694–698. doi: 10.1192/bjp.161.5.694. [DOI] [PubMed] [Google Scholar]
- 44.Marks IM, Crowe M, Drewe E, et al. Obsessive compulsive neurosis in identical twins. Br.J.Psychiatry. 1969;115:991–998. doi: 10.1192/bjp.115.526.991. [DOI] [PubMed] [Google Scholar]
- 45.McGuffin P, Mawson D. Obsessive-compulsive neurosis: two identical twin pairs. Br.J.Psychiatry. 1980;137:285–287. doi: 10.1192/bjp.137.3.285. [DOI] [PubMed] [Google Scholar]
- 46.Woodruff R, Pitts FM. Monozygotic twins with obsessional illness. Am J Psych. 1964;120:1075–1080. doi: 10.1176/ajp.120.11.1075. [DOI] [PubMed] [Google Scholar]
- 47.Inyoue E. Similar and dissimilar manifestations of obsessive-compulsive neurosis in monozygotic twins. Am J Psych. 1965;121:1171–1175. doi: 10.1176/ajp.121.12.1171. [DOI] [PubMed] [Google Scholar]
- 48.Carey G, Gottesman II. Twin and family studies of anxiety, phobic, and obsessive disordersAnxiety: New research and changing concepts. In: Klein DF, Rabkin JG, editors. Anxiety: New research and changing concepts. Raven Press; New York: 1981. pp. 117–136. [Google Scholar]
- 49.Jonnal AH, Gardner CO, Prescott CA, et al. Obsessive and compulsive symptoms in a general population sample of female twins. Am.J.Med.Genet. 2000;96:791–796. doi: 10.1002/1096-8628(20001204)96:6<791::aid-ajmg19>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 50.Bolton D, Rijsdijk F, O’Connor TG, et al. Obsessive-compulsive disorder, tics and anxiety in 6-year-old twins. Psychol.Med. 2007;37:39–48. doi: 10.1017/S0033291706008816. [DOI] [PubMed] [Google Scholar]
- 51.Hudziak JJ, Van Beijsterveldt CE, Althoff RR, et al. Genetic and environmental contributions to the Child Behavior Checklist Obsessive-Compulsive Scale: a cross-cultural twin study. Arch Gen Psychiatry. 2004 Jun;61(6):608–616. doi: 10.1001/archpsyc.61.6.608. 608.-16. 61. 2004. [DOI] [PubMed] [Google Scholar]
- 52.Nicolini H, Hanna G, Baxter L, et al. Segregation analysis of obsessive compulsive and associated disorders: preliminary results. Ursus Medicus. 1991;1:25–28. [Google Scholar]
- 53.Cavallini MC, Pasquale L, Bellodi L, et al. Complex segregation analysis for obsessive compulsive disorder and related disorders. Am J Med Genet. 1999;88:38–43. doi: 10.1002/(sici)1096-8628(19990205)88:1<38::aid-ajmg7>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 54.Alsobrook JP, II, Leckman JF, Goodman WK, et al. Segregation analysis of obsessive-compulsive disorder using symptom-based factor scores. Am.J.Med.Genet. 1999;88:669–675. doi: 10.1002/(sici)1096-8628(19991215)88:6<669::aid-ajmg17>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- 55.Nestadt G, Lan T, Samuels J, et al. Complex segregation analysis provides compelling evidence for a major gene underlying obsessive-compulsive disorder and for heterogeneity by sex. Am.J.Hum.Genet. 2000;67:1611–1616. doi: 10.1086/316898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Bengel D, Greenberg BD, Cora-Locatelli G, et al. Association of the serotonin transporter promoter regulatory region polymorphism and obsessive-compulsive disorder. Mol.Psychiatry. 1999;4:463–466. doi: 10.1038/sj.mp.4000550. [DOI] [PubMed] [Google Scholar]
- 57.Billett EA, Richter MA, King N, et al. Obsessive compulsive disorder, response to serotonin reuptake inhibitors and the serotonin transporter gene. Mol.Psychiatry. 1997;2:403–406. doi: 10.1038/sj.mp.4000257. [DOI] [PubMed] [Google Scholar]
- 58.Camarena B, Rinetti G, Cruz C, et al. Additional evidence that genetic variation of MAO-A gene supports a gender subtype in obsessive-compulsive disorder. Am.J.Med.Genet. 2001;105:279–282. doi: 10.1002/ajmg.1323. [DOI] [PubMed] [Google Scholar]
- 59.Camarena B, Rinetti G, Cruz C, et al. Association study of the serotonin transporter gene polymorphism in obsessive-compulsive disorder. Int.J.Neuropsychopharmacol. 2001;4:269–272. doi: 10.1017/S1461145701002516. [DOI] [PubMed] [Google Scholar]
- 60.Di Bella D, Erzegovesi S, Cavallini MC, et al. Obsessive-Compulsive Disorder, 5-HTTLPR polymorphism and treatment response. Pharmacogenomics.J. 2002;2:176–181. doi: 10.1038/sj.tpj.6500090. [DOI] [PubMed] [Google Scholar]
- 61.Frisch A, Michaelovsky E, Rockah R, et al. Association between obsessive-compulsive disorder and polymorphisms of genes encoding components of the serotonergic and dopaminergic pathways. Eur.Neuropsychopharmacol. 2000;10:205–209. doi: 10.1016/s0924-977x(00)00071-7. [DOI] [PubMed] [Google Scholar]
- 62.McDougle CJ, Epperson CN, Price LH, et al. Evidence for linkage disequilibrium between serotonin transporter protein gene (SLC6A4) and obsessive compulsive disorder. Mol.Psychiatry. 1998;3:270–273. doi: 10.1038/sj.mp.4000391. [DOI] [PubMed] [Google Scholar]
- 63.Hemmings SM, Kinnear CJ, Niehaus DJ, et al. Investigating the role of dopaminergic and serotonergic candidate genes in obsessive-compulsive disorder. Eur.Neuropsychopharmacol. 2003;13:93–98. doi: 10.1016/s0924-977x(02)00129-3. [DOI] [PubMed] [Google Scholar]
- 64.Mundo E, Richter MA, Zai G, et al. 5HT1Dbeta Receptor gene implicated in the pathogenesis of Obsessive-Compulsive Disorder: further evidence from a family-based association study. Mol.Psychiatry. 2002;7:805–809. doi: 10.1038/sj.mp.4001059. [DOI] [PubMed] [Google Scholar]
- 65.Enoch MA, Greenberg BD, Murphy DL, et al. Sexually dimorphic relationship of a 5-HT2A promoter polymorphism with obsessive-compulsive disorder. Biol.Psychiatry. 2001;49:385–388. doi: 10.1016/s0006-3223(00)01040-4. [DOI] [PubMed] [Google Scholar]
- 66.Walitza S, Wewetzer C, Warnke A, et al. 5-HT2A promoter polymorphism - 1438G/A in children and adolescents with obsessive-compulsive disorders. Mol.Psychiatry. 2002;7:1054–1057. doi: 10.1038/sj.mp.4001105. [DOI] [PubMed] [Google Scholar]
- 67.Meira-Lima I, Shavitt RG, Miguita K, et al. Association analysis of the catechol-o-methyltransferase (COMT), serotonin transporter (5-HTT) and serotonin 2A receptor (5HT2A) gene polymorphisms with obsessive-compulsive disorder. Genes Brain Behav. 2004;3:75–79. doi: 10.1046/j.1601-1848.2003.0042.x. [DOI] [PubMed] [Google Scholar]
- 68.Cavallini MC, Di Bella D, Pasquale L, et al. 5HT2C CYS23/SER23 polymorphism is not associated with obsessive-compulsive disorder. Psychiatry Res. 1998;77:97–104. doi: 10.1016/s0165-1781(97)00151-0. [DOI] [PubMed] [Google Scholar]
- 69.Ozaki N, Goldman D, Kaye WH, et al. Serotonin transporter missense mutation associated with a complex neuropsychiatric phenotype. Mol.Psychiatry. 2003;8:933–936. doi: 10.1038/sj.mp.4001365. [DOI] [PubMed] [Google Scholar]
- 70.Delorme R, Betancur C, Wagner M, et al. Support for the association between the rare functional variant I425V of the serotonin transporter gene and susceptibility to obsessive compulsive disorder. Mol.Psychiatry. 2005;10:1059–1061. doi: 10.1038/sj.mp.4001728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Wendland JR, DeGuzman TB, Rudnick G, et al. SERT Ileu425Val and Other Uncommon SERT Variants in Asperger Syndrome, Autism and Obsessive-Compulsive Disorder. Psychiatric Genetics. 2007 doi: 10.1097/YPG.0b013e3282f08a06. In press. [DOI] [PubMed] [Google Scholar]
- 72.Hu XZ, Lipsky RH, Zhu G, et al. Serotonin transporter promoter gain-of-function genotypes are linked to obsessive-compulsive disorder. Am J Hum Genet. 2006;78:815–826. doi: 10.1086/503850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Chabane N, Millet B, Delorme R, et al. Lack of evidence for association between serotonin transporter gene (5-HTTLPR) and obsessive-compulsive disorder by case control and family association study in humans. Neurosci.Lett. 2004;363:154–156. doi: 10.1016/j.neulet.2004.03.065. [DOI] [PubMed] [Google Scholar]
- 74.Cruz C, Camarena B, King N, et al. Increased prevalence of the seven-repeat variant of the dopamine D4 receptor gene in patients with obsessive-compulsive disorder with tics. Neurosci.Lett. 1997;231:1–4. doi: 10.1016/s0304-3940(97)00523-5. [DOI] [PubMed] [Google Scholar]
- 75.Millet B, Chabane N, Delorme R, et al. Association between the dopamine receptor D4 (DRD4) gene and obsessive-compulsive disorder. Am.J.Med.Genet. 2003;116B:55–59. doi: 10.1002/ajmg.b.10034. [DOI] [PubMed] [Google Scholar]
- 76.Billett EA, Richter MA, Sam F, et al. Investigation of dopamine system genes in obsessive-compulsive disorder. Psychiatr.Genet. 1998;8:163–169. doi: 10.1097/00041444-199800830-00005. [DOI] [PubMed] [Google Scholar]
- 77.Catalano M, Sciuto G, Di Bella D, et al. Lack of association between obsessive-compulsive disorder and the dopamine D3 receptor gene: some preliminary considerations. Am.J.Med.Genet. 1994;54:253–255. doi: 10.1002/ajmg.1320540312. [DOI] [PubMed] [Google Scholar]
- 78.Nicolini H, Cruz C, Camarena B, et al. DRD2, DRD3 and 5HT2A receptor genes polymorphisms in obsessive-compulsive disorder. Mol.Psychiatry. 1996;1:461–465. [PubMed] [Google Scholar]
- 79.Karayiorgou M, Altemus M, Galke BL, et al. Genotype determining low catechol-O-methyltransferase activity as a risk factor for obsessive-compulsive disorder. Proc.Natl.Acad.Sci.U.S.A. 1997;94:4572–4575. doi: 10.1073/pnas.94.9.4572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Niehaus DJ, Kinnear CJ, Corfield VA, et al. Association between a catechol-o-methyltransferase polymorphism and obsessive-compulsive disorder in the Afrikaner population. J.Affect.Disord. 2001;65:61–65. doi: 10.1016/s0165-0327(00)00246-9. [DOI] [PubMed] [Google Scholar]
- 81.Schindler KM, Richter MA, Kennedy JL, et al. Association between homozygosity at the COMT gene locus and obsessive compulsive disorder. Am.J.Med.Genet. 2000;96:721–724. doi: 10.1002/1096-8628(20001204)96:6<721::aid-ajmg4>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 82.Azzam A, Mathews CA. Meta-analysis of the association between the catecholamine-O-methyl-transferase gene and obsessive-compulsive disorder. Am J Med Genet. 2003;123B:64–69. doi: 10.1002/ajmg.b.20013. [DOI] [PubMed] [Google Scholar]
- 83.Erdal ME, Tot S, Yazici K, et al. Lack of association of catechol-O-methyltransferase gene polymorphism in obsessive-compulsive disorder. Depress.Anxiety. 2003;18:41–45. doi: 10.1002/da.10114. [DOI] [PubMed] [Google Scholar]
- 84.Alsobrook JP, Zohar AH, Leboyer M, et al. Association between the COMT locus and obsessive-compulsive disorder in females but not males. Am.J.Med.Genet. 2002;114:116–120. doi: 10.1002/ajmg.10040. [DOI] [PubMed] [Google Scholar]
- 85.Karayiorgou M, Sobin C, Blundell ML, et al. Family-based association studies support a sexually dimorphic effect of COMT and MAOA on genetic susceptibility to obsessive-compulsive disorder. Biol.Psychiatry. 1999;45:1178–1189. doi: 10.1016/s0006-3223(98)00319-9. [DOI] [PubMed] [Google Scholar]
- 86.Hall D, Dhilla A, Charalambous A, et al. Sequence variants of the brain-derived neurotrophic factor (BDNF) gene are strongly associated with obsessive-compulsive disorder. Am.J.Hum.Genet. 2003;73:370–376. doi: 10.1086/377003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Arnold PD, Rosenberg DR, Mundo E, et al. Association of a glutamate (NMDA) subunit receptor gene (GRIN2B) with obsessive-compulsive disorder: a preliminary study. Psychopharmacology (Berl) 2004;174:530–538. doi: 10.1007/s00213-004-1847-1. [DOI] [PubMed] [Google Scholar]
- 88.Zai G, Arnold P, Burroughs E, et al. Evidence for the gamma-amino-butyric acid type B receptor 1 (GABBR1) gene as a susceptibility factor in obsessive-compulsive disorder. Am J Med Genet B Neuropsychiatr.Genet. 2005 Apr 5;134B(1):25–29. doi: 10.1002/ajmg.b.30152. 25.-9. 134B. 2005. [DOI] [PubMed] [Google Scholar]
- 89.Stewart SE, Platko J, Fagerness J, et al. A genetic family-based association study of OLIG2 in obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2007;64:209–214. doi: 10.1001/archpsyc.64.2.209. [DOI] [PubMed] [Google Scholar]
- 90.Zai G, Bezchlibnyk YB, Richter MA, et al. Myelin oligodendrocyte glycoprotein (MOG) gene is associated with obsessive-compulsive disorder. Am J Med Genet. 2004;129B:64–68. doi: 10.1002/ajmg.b.30077. [DOI] [PubMed] [Google Scholar]
- 91.Welch JM, Lu J, Rodriguiz RM, et al. Cortico-striatal synaptic defects and OCD-like behaviours in Sapap3-mutant mice. Nature. 2007;448:894–900. doi: 10.1038/nature06104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Zuchner S, Wendland JR, Ashley-Koch AE, et al. Multiple rare SAPAP3 missense variants in trichotillomania and OCD. Mol.Psychiatry. 2009;14:6–9. doi: 10.1038/mp.2008.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Bienvenu OJ, Wang Y, Shugart YY, et al. Sapap3 and pathological grooming in humans: Results from the OCD collaborative genetics study. Am J Med Genet B Neuropsychiatr.Genet. 2009 Jul 5;150B(5):710–720. doi: 10.1002/ajmg.b.30897. 710.-20. 150B. 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Willour VL, Yao SY, Samuels J, et al. Replication study supports evidence for linkage to 9p24 in obsessive-compulsive disorder. Am.J.Hum.Genet. 2004;75:508–513. doi: 10.1086/423899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Arnold PD, Sicard T, Burroughs E, et al. Glutamate transporter gene SLC1A1 associated with obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2006;63:769–776. doi: 10.1001/archpsyc.63.7.769. [DOI] [PubMed] [Google Scholar]
- 96.Dickel DE, Veenstra-VanderWeele J, Cox NJ, et al. Association testing of the positional and functional candidate gene SLC1A1/EAAC1 in early-onset obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2006;63:778–785. doi: 10.1001/archpsyc.63.7.778. [DOI] [PubMed] [Google Scholar]
- 97.Shugart Y, Wang Y, Samuels J, et al. A family-based association study of the glutamate transporter gene SLC1A1 obsessive-compulsive disorder in 378 families. Am J Med Genet B Neuropsychiatr.Genet. 2008 doi: 10.1002/ajmg.b.30914. in press. [DOI] [PubMed] [Google Scholar]
- 98.Stewart SE, Fagerness JA, Platko J, et al. Association of the SLC1A1 glutamate transporter gene and obsessive-compulsive disorder. Am J Med Genet B Neuropsychiatr.Genet. 2007;144:1027–1033. doi: 10.1002/ajmg.b.30533. [DOI] [PubMed] [Google Scholar]
- 99.Wendland JR, Moya PR, Timpano KR, et al. A haplotype containing quantitative trait loci for SLC1A1 gene expression and its association with obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2009;66:408–416. doi: 10.1001/archgenpsychiatry.2009.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Wang Y, Adamczyk A, Shugart Y, et al. A Screen of SLC1A1 for OCD-Related Alleles. Am J Med Genet. 2009 doi: 10.1002/ajmg.b.31001. in press. [DOI] [PubMed] [Google Scholar]
- 101.Kong A, Cox NJ. Allele-sharing models: LOD scores and accurate linkage tests. Am.J.Hum.Genet. 1997;61:1179–1188. doi: 10.1086/301592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Abecasis GR, Cherny SS, Cookson WO, et al. Merlin--rapid analysis of dense genetic maps using sparse gene flow trees. Nat.Genet. 2002;30:97–101. doi: 10.1038/ng786. [DOI] [PubMed] [Google Scholar]
- 103.Hanna GL, Veenstra-VanderWeele J, Cox NJ, et al. Evidence for a Susceptibility Locus on Chromosome 10p15 in Early-Onset Obsessive-Compulsive Disorder. Biol.Psychiatry. 2007;62:856–62. doi: 10.1016/j.biopsych.2007.01.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Geller D, Biederman J, Jones J, et al. Is juvenile obsessive-compulsive disorder a developmental subtype of the disorder? A review of the pediatric literature. J.Am.Acad.Child Adolesc.Psychiatry. 1998;37:420–427. doi: 10.1097/00004583-199804000-00020. [DOI] [PubMed] [Google Scholar]
- 105.March JS, Leonard HL. Obsessive-compulsive disorder in children and adolescents: a review of the past 10 years. J.Am.Acad.Child Adolesc.Psychiatry. 1996;35:1265–1273. doi: 10.1097/00004583-199610000-00012. [DOI] [PubMed] [Google Scholar]
- 106.Rosario-Campos MC, Leckman JF, Mercadante MT, et al. Adults with early-onset obsessive-compulsive disorder. Am.J.Psychiatry. 2001;158:1899–1903. doi: 10.1176/appi.ajp.158.11.1899. [DOI] [PubMed] [Google Scholar]
- 107.Skoog G, Skoog I. A 40-year follow-up of patients with obsessive-compulsive disorder. Arch.Gen.Psychiatry. 1999;56:121–127. doi: 10.1001/archpsyc.56.2.121. see commetns. [DOI] [PubMed] [Google Scholar]
- 108.Busatto GF, Buchpiguel CA, Zamignani DR, et al. Regional cerebral blood flow abnormalities in early-onset obsessive-compulsive disorder: an exploratory SPECT study. J.Am.Acad.Child Adolesc.Psychiatry. 2001;40:347–354. doi: 10.1097/00004583-200103000-00015. [DOI] [PubMed] [Google Scholar]
- 109.Shugart YY, Samuels J, Willour VL, et al. Genomewide linkage scan for obsessive-compulsive disorder: evidence for susceptibility loci on chromosomes 3q, 7p, 1q, 15q, and 6q. Mol.Psychiatry. 2006;11:763–770. doi: 10.1038/sj.mp.4001847. [DOI] [PubMed] [Google Scholar]
- 110.Wang Y, Samuels JF, Chang YC, et al. Gender differences in genetic linkage and association on 11p15 in obsessive-compulsive disorder families. Am J Med Genet B Neuropsychiatr.Genet. 2009 Jan 5;150B(1):33–40. doi: 10.1002/ajmg.b.30760. 150B:33-40, 2009. [DOI] [PubMed] [Google Scholar]
- 111.Grados MA, Riddle MA, Samuels JF, et al. The familial phenotype of obsessive-compulsive disorder in relation to tic disorders: the Hopkins OCD family study. Biol.Psychiatry. 2001 Oct 15;50(8):559–565. doi: 10.1016/s0006-3223(01)01074-5. 559.-65. 50. 2001. [DOI] [PubMed] [Google Scholar]
- 112.Pauls DL, Leckman JF. The inheritance of Gilles de la Tourette’s syndrome and associated behaviors. Evidence for autosomal dominant transmission. N.Engl.J Med. 1986;315:993–997. doi: 10.1056/NEJM198610163151604. [DOI] [PubMed] [Google Scholar]
- 113.Nestadt G, Samuels J, Riddle MA, et al. The relationship between obsessive-compulsive disorder and anxiety and affective disorders: results from the Johns Hopkins OCD Family Study. Psychol.Med. 2001 Apr;31(3):481–487. doi: 10.1017/s0033291701003579. 481.-7. 31. 2001. [DOI] [PubMed] [Google Scholar]
- 114.Nestadt G, Addington A, Samuels J, et al. The identification of OCD-related subgroups based on comorbidity. Biol.Psychiatry. 2003;53:914–920. doi: 10.1016/s0006-3223(02)01677-3. [DOI] [PubMed] [Google Scholar]
- 115.Samuels J, Nestadt G, Bienvenu OJ, et al. Personality disorders and normal personality dimensions in obsessive-compulsive disorder. Br.J.Psychiatry. 2000 Nov;177:457–462. doi: 10.1192/bjp.177.5.457. 457.-62. 177. 2000. [DOI] [PubMed] [Google Scholar]
- 116.Baer L. Factor analysis of symptom subtypes of obsessive compulsive disorder and their relation to personality and tic disorders. J Clin.Psychiatry. 1994;55(Suppl):18–23. [PubMed] [Google Scholar]
- 117.Leckman JF, Grice DE, Boardman J, et al. Symptoms of obsessive-compulsive disorder. Am J Psychiatry. 1997;154:911–917. doi: 10.1176/ajp.154.7.911. [DOI] [PubMed] [Google Scholar]
- 118.Mataix-Cols D, Rauch SL, Manzo PA, et al. Use of factor-analyzed symptom dimensions to predict outcome with serotonin reuptake inhibitors and placebo in the treatment of obsessive-compulsive disorder. Am J Psychiatry. 1999;156:1409–1416. doi: 10.1176/ajp.156.9.1409. [DOI] [PubMed] [Google Scholar]
- 119.Rasmussen SA, Eisen JL. The epidemiology and clinical features of obsessive compulsive disorder. Psychiatr.Clin.North Am. 1992;15:743–758. [PubMed] [Google Scholar]
- 120.Frost RO, Steketee G, Williams LF, et al. Mood, personality disorder symptoms and disability in obsessive compulsive hoarders: a comparison with clinical and nonclinical controls. Behav.Res.Ther. 2000;38:1071–1081. doi: 10.1016/s0005-7967(99)00137-0. [DOI] [PubMed] [Google Scholar]
- 121.Winsberg ME, Cassic KS, Koran LM. Hoarding in obsessive-compulsive disorder: a report of 20 cases. J.Clin.Psychiatry. 1999;60:591–597. doi: 10.4088/jcp.v60n0905. [DOI] [PubMed] [Google Scholar]
- 122.Saxena S, Brody AL, Maidment KM, et al. Cerebral glucose metabolism in obsessive-compulsive hoarding. Am.J.Psychiatry. 2004;161:1038–1048. doi: 10.1176/appi.ajp.161.6.1038. [DOI] [PubMed] [Google Scholar]
- 123.Mataix-Cols D, Wooderson S, Lawrence N, et al. Distinct neural correlates of washing, checking, and hoarding symptom dimensions in obsessive-compulsive disorder. Arch.Gen.Psychiatry. 2004;61:564–576. doi: 10.1001/archpsyc.61.6.564. [DOI] [PubMed] [Google Scholar]
- 124.Samuels J, Bienvenu OJ, III, Riddle MA, et al. Hoarding in obsessive compulsive disorder: results from a case-control study. Behav.Res.Ther. 2002;40:517–528. doi: 10.1016/s0005-7967(01)00026-2. [DOI] [PubMed] [Google Scholar]
- 125.Mataix-Cols D, Rosario-Campos MC, Leckman JF. A multidimensional model of obsessive-compulsive disorder. Am.J.Psychiatry. 2005;162:228–238. doi: 10.1176/appi.ajp.162.2.228. [DOI] [PubMed] [Google Scholar]
- 126.Cullen B, Brown CH, Riddle MA, et al. Factor analysis of the Yale-Brown Obsessive Compulsive Scale in a family study of obsessive-compulsive disorder. Depress.Anxiety. 2007;24:130–138. doi: 10.1002/da.20204. [DOI] [PubMed] [Google Scholar]
- 127.Hasler G, Pinto A, Greenberg BD, et al. Familiality of Factor Analysis-Derived YBOCS Dimensions in OCD-Affected Sibling Pairs from the OCD Collaborative Genetics Study. Biol.Psychiatry. 2007;61:617–625. doi: 10.1016/j.biopsych.2006.05.040. [DOI] [PubMed] [Google Scholar]
- 128.Pinto A, Greenberg B, Grados M, et al. OCD Collaborative Genetics Study: Furthter development of YBOCS dimensions in the OCD Collaborative Genetics Study: symptoms vs. catergories. Psychiatry Research. 2008;160:83–93. doi: 10.1016/j.psychres.2007.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Stewart SE, Rosario MC, Brown TA, et al. Principal components analysis of obsessive-compulsive disorder symptoms in children and adolescents. Biol.Psychiatry. 2007;61:285–291. doi: 10.1016/j.biopsych.2006.08.040. [DOI] [PubMed] [Google Scholar]
- 130.Samuels J, Shugart Y, Grados M, et al. Significant linkage to compulsive hoarding on chromosome 14 in families with obsessive-compulsive disorder: Results from the OCD Collaborative Genetics Study. American Journal of Psychiatry. 2007;164:493–499. doi: 10.1176/ajp.2007.164.3.493. [DOI] [PubMed] [Google Scholar]
- 131.Nestadt G, Di CZ, Riddle MA, et al. Obsessive-compulsive disorder: subclassification based on co-morbidity. Psychol.Med. 2008:1–11. doi: 10.1017/S0033291708004753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Pauls DL, Towbin KE, Leckman JF, et al. Gilles de la Tourette’s syndrome and obsessive-compulsive disorder. Evidence supporting a genetic relationship. Arch.Gen.Psychiatry. 1986;43:1180–1182. doi: 10.1001/archpsyc.1986.01800120066013. [DOI] [PubMed] [Google Scholar]
- 133.Tolin DF, Kiehl KA, Worhunsky P, et al. An exploratory study of the neural mechanisms of decision making in compulsive hoarding. Psychol.Med. 2009;39:325–336. doi: 10.1017/S0033291708003371. [DOI] [PubMed] [Google Scholar]
- 134.Chamberlain SR, Menzies L, Hampshire A, et al. Orbitofrontal dysfunction in patients with obsessive-compulsive disorder and their unaffected relatives. Science. 2008;321:421–422. doi: 10.1126/science.1154433. [DOI] [PubMed] [Google Scholar]
- 135.Menzies L, Achard S, Chamberlain SR, et al. Neurocognitive endophenotypes of obsessive-compulsive disorder. Brain. 2007;130:3223–3236. doi: 10.1093/brain/awm205. [DOI] [PubMed] [Google Scholar]
- 136.Chamberlain SR, Fineberg NA, Menzies LA, et al. Impaired cognitive flexibility and motor inhibition in unaffected first-degree relatives of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164:335–338. doi: 10.1176/appi.ajp.164.2.335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Bechara A, Damasio AR, Damasio H, et al. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50:7–15. doi: 10.1016/0010-0277(94)90018-3. [DOI] [PubMed] [Google Scholar]
- 138.Cavedini P, Riboldi G, D’Annucci A, et al. Decision-making heterogeneity in obsessive-compulsive disorder: ventromedial prefrontal cortex function predicts different treatment outcomes. Neuropsychologia. 2002;40:205–211. doi: 10.1016/s0028-3932(01)00077-x. [DOI] [PubMed] [Google Scholar]
- 139.Nielen MM, Veltman DJ, de Jong R, et al. Decision making performance in obsessive compulsive disorder. J Affect.Disord. 2002;69:257–260. doi: 10.1016/s0165-0327(00)00381-5. [DOI] [PubMed] [Google Scholar]
- 140.Chamberlain SR, Fineberg NA, Blackwell AD, et al. Motor inhibition and cognitive flexibility in obsessive-compulsive disorder and trichotillomania. Am J Psychiatry. 2006;163:1282–1284. doi: 10.1176/ajp.2006.163.7.1282. [DOI] [PubMed] [Google Scholar]
- 141.Carlson CS, Eberle MA, Kruglyak L, et al. Mapping complex disease loci in whole-genome association studies. Nature. 2004;429:446–452. doi: 10.1038/nature02623. [DOI] [PubMed] [Google Scholar]
- 142.Carrasquillo MM, McCallion AS, Puffenberger EG, et al. Genome-wide association study and mouse model identify interaction between RET and EDNRB pathways in Hirschsprung disease. Nat.Genet. 2002;32:237–244. doi: 10.1038/ng998. [DOI] [PubMed] [Google Scholar]
- 143.Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymorphism in age-related macular degeneration. Science. 2005;308:385–389. doi: 10.1126/science.1109557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Botstein D, Risch N. Discovering genotypes underlying human phenotypes: past successes for mendelian disease, future approaches for complex disease. Nat.Genet. 2003;33(Suppl):228–237. doi: 10.1038/ng1090. [DOI] [PubMed] [Google Scholar]
- 145.Ohashi J, Tokunaga K. The expected power of genome-wide linkage disequilibrium testing using single nucleotide polymorphism markers for detecting a low-frequency disease variant. Ann.Hum.Genet. 2002;66:297–306. doi: 10.1017/S0003480002001197. [DOI] [PubMed] [Google Scholar]
- 146.Neale BM, Sham PC. The future of association studies: gene-based analysis and replication. Am J Hum Genet. 2004;75:353–362. doi: 10.1086/423901. [DOI] [PMC free article] [PubMed] [Google Scholar]