

Abstract
Using a cross-lagged panel design, we investigated the impact of positive family processes on change in autism symptoms and behaviors. A sample of 149 co-residing mothers and their adolescent or adult child with autism was drawn from a large, longitudinal study. Maternal warmth and praise were measured using coded speech samples in which mothers talked about their son or daughter. A high level of relationship quality was associated with subsequent reductions in internalizing and externalizing problems as well as reductions in impairments in social reciprocity and repetitive behaviors. Maternal warmth and praise were also related to symptom abatement in the repetitive behaviors domain.
Autism spectrum disorders are lifelong disabilities that present multiple challenges for families. The behavior problems and autism symptoms of children with autism spectrum disorder have repeatedly been documented as a significant source of stress for parents (Hastings & Brown, 2002; Hastings, Kovshoff et al., 2005; Herring et al., 2006; Lecavalier, Leone, & Wiltz, 2006; Lounds, Seltzer, Greenberg, & Shattuck, 2007). Despite evidence that the behaviors and symptoms of autism spectrum disorder profoundly impact families, few researchers have examined reciprocally the role that the family environment may have on the course of symptoms and maladaptive behaviors over time. Specifically, questions remain regarding how positive aspects of the family environment, particularly affective expression and relationship quality, may be related to the developmental course of autism spectrum disorder.
In the general child development literature, maternal warmth and the quality of the parent– child relationship have long been shown to be predictive of child adaptation and behavioral functioning (Borkowski, Ramey, & Bristol-Powers, 2002). Similarly, parent–child relationship quality is an important factor for adjustment during adolescence and young adulthood among families with typically developing children (Overbeek, Stattin, Vermulst, Ha, & Engels, 2007). Less is known, however, about the association between family processes and developmental outcomes for adolescents and adults with autism. In the past, the prevailing belief was that mothers of children with autism were cold and rejecting, and they were labeled by professionals as “refrigerator mothers,” perhaps explaining why few researchers have examined the role of positive family processes, such as relationship quality and warmth (for an exception, see Orsmond, Seltzer, Green-berg, & Krauss, 2006) on the development of children with autism. In this study we investigated the bidirectional interplay between positive family processes and behavior problems and autism symptoms in families of adolescents and adults with autism spectrum disorder.
In populations at-risk for behavior problems, family processes, including positive maternal affective expression, have been consistently hypothesized as potential mechanisms in behavioral development. For instance, in a study of low birth weight babies, maternal warmth moderated the effect of birth weight on behavior problems, with higher warmth associated with fewer problems when risk was high (Tully, Arseneault, Caspi, Moffitt, & Morgan, 2004). Main effects of the family environment on behavioral outcomes have likewise been demonstrated. Work with monozygotic twins has shown less negativity and more warmth from mothers to predict fewer antisocial behavior problems in high-risk children, demonstrating how environmental effects can be causal factors in the development of behavior problems (Caspi et al., 2004). Similarly, negative and positive emotional expressions have been associated with externalizing behaviors and social competence, respectively (Eisenberg et al., 2001). Collectively, these studies elucidate how environmental factors, specifically positive maternal affect, can influence the course of behavioral development among individuals with biological risks for behavior problems.
Positive family processes may also be influential in promoting mental health and reducing symptomatology during adulthood. For instance, connections between positive family environments and more optimal outcomes have been demonstrated in studies of individuals with schizophrenia and their families. In a study of ethnicity and schizophrenia, warmer family environments post-hospitalization were associated with a lower risk of relapse for Mexican American individuals with schizophrenia (Lopez et al., 2004). Relatedly, mothers' expressions of warmth and praise toward their son or daughter with schizophrenia, in addition to the quality of the parent– child relationship, have been linked with greater life satisfaction among adults with schizophrenia (Greenberg, Knudsen, & Aschbrenner, 2006). Given the similarities associated with some aspects of parenting an individual with schizophrenia and an individual with autism (Greenberg, Seltzer, Krauss, Chou, & Hong, 2004; Seltzer, Abbeduto, Krauss, Greenberg, & Swe, 2004), these findings suggest that positive aspects of the family environment might also serve a protective function for autism symptomatology during adolescence and adulthood.
Although associations between family-level factors and children's developmental trajectories have been widely examined in studies of typically developing children (Borkowski et al., 2002), less attention has been given to understanding family processes within families of individuals with an autism spectrum disorder. This lack of research on the role of the family environment in the developmental course of autism spectrum disorder presumably stems from the prevailing consensus that autism is a complex genetic disorder and clearly not caused by poor parenting, as earlier theorists had incorrectly postulated (Folstein & Rosen-Sheidley, 2001). However, even given the strong role of genetics in the etiology of autism, there is evidence that the phenotypic expression of the disorder is still influenced by the family environment (Greenberg, Seltzer, Hong, & Orsmond, 2006). As such, positive family processes may operate as potential mechanisms in the development of autism symptoms and maladaptive behaviors.
Recently, attention has been given to one unique family environmental factor, expressed emotion, as a potential explanatory variable among families of children with disabilities. Expressed emotion is defined by high levels of criticism and/or emotional overinvolvement from one family member directed toward another family member with a disability or illness. Family expressed emotion has long been related to relapse among adults with schizophrenia (Sutcliff & Hooley, 1998) and has been examined more recently in families of children with intellectual disabilities (Beck, Daley, Hastings, & Stevenson, 2004; Hastings, Daley, Burns, & Beck, 2006) as well as autism spectrum disorder (Greenberg, Seltzer et al., 2006). High levels of criticism, in particular, have been associated with elevated levels of maladaptive behaviors in individuals with disabilities (Hastings, Daley et al., 2006). However, only examining the negative aspects of the family affective climate may be limiting for understanding the full range of family processes that influence development. Negative and positive well-being, for instance, are not necessarily on the same continuum of mental functioning (Ryff et al., 2006). There remains a need to examine the positive aspects of emotional expression and other family processes among families with children with autism spectrum disorder.
Although researchers have begun to examine the impact of the family environment on the development of individuals with autism, gaps still remain in understanding the specific processes by which families adapt and change over time, especially later in the life course (Seltzer, Krauss, Orsmond, & Vestal, 2001). Maternal warmth, praise, and the quality of the relationship between mother and son or daughter might be potential mechanisms that impact the developmental course of autism. As such, in the current study our aim was to extend the work of Greenberg, Seltzer et al. (2006), in which they examined negative components of expressed emotion (criticism and emotional overinvolvement) among families of adolescents and adults with autism. In the present study we examined linkages between the positive aspects of the family environment and subsequent child behavior and symptomatology in the same sample. Specifically, the influences of maternal warmth, praise, and relationship quality on change in children's autism symptoms and behaviors problems were investigated using a cross-lagged panel design. This longitudinal design allowed for an examination of the direction of effects between family process variables and behavior problems and symptoms in adolescents and adults with autism spectrum disorder.
We had three primary research questions: (a) What is the stability of warmth, praise, and relationship quality over an 18-month period among mothers of adolescents and adults with an autism spectrum disorder? (b) Are levels of maternal warmth, praise, and relationship quality predictive of later behavior problems and autism symptoms? (c) Are severity of behavior problems and autism symptoms predictive of later maternal warmth, praise, and relationship quality?
In examining these questions, we used a cross-lagged panel design, which allowed us to test the stability of effects over time as well as the lagged effects across domains. We also included control variables of important child characteristics. Because mother–child interactions across the life-span often vary depending on the gender of the child (Rossi & Rossi, 1990), we controlled for child's gender in the bidirectional models of positive family processes and behavior problems and autism symptoms. Additionally, we controlled for a comorbid diagnosis of mental retardation because of the strong association between mental retardation and behavior problems and autism symptoms (Shattuck et al., 2007).
Based on previous research, we hypothesized that high levels of maternal warmth, praise, and relationship quality would be associated with lower levels of behavior problems (internalizing, externalizing, and asocial), even after controlling for prior levels of behavior problems, child gender, and mental retardation status. Similarly, we hypothesized that these positive family factors (warmth, praise, and relationship quality) would be related to decreases in core autism symptoms (impairments in communication, impairments in social reciprocity, and repetitive behaviors and restricted interests) over an 18-month period. Reciprocally, we also expected that high levels of behavior problems and autism symptoms would be related to lower levels of maternal warmth, praise, and relationship quality.
Method
Participants
Participants were drawn from an ongoing longitudinal study of 406 families of adolescents and adults with an autism spectrum disorder. Families in Wisconsin (n = 202) and Massachusetts (n = 204) were recruited via agencies, schools, diagnostic clinics, and media announcements. Identical recruitment procedures were used in both states, with information packets being distributed to families inviting them to participate in the research. We utilized data from the second and third waves of the study (Time 2, conducted in 2000–2001, and Time 3, in 2002–2003). Time 2 was the first point in the present research when the Five Minute Speech Sample, which is used to derive measures of maternal warmth and praise (as well as measures of criticism and over involvement), was administered.
Families met three initial inclusion criteria: (a) the family had a son or daughter 10 years of age or older; (b) the child had received a diagnosis on the autism spectrum from a medical, psychological, or educational professional, as reported by parents; and (c) administration of the Autism Diagnostic Interview-Revised (Lord, Rutter, & Le Couture, 1994; Rutter, Le Couture, & Lord, 2003) confirmed the parental report of an autism spectrum disorder. Of the 406 individuals in the sample, 384 (94.6%) met all criteria for autistic disorder on the Autism Diagnostic Interview-Revised (qualitative impairments in communication and language; qualitative impairments in reciprocal social interaction; repetitive, restrictive, and stereotyped behaviors; and onset of symptoms prior to 36 months). The remaining 22 individuals (5.4% of the sample) demonstrated a pattern of impairments on the Autism Diagnostic Interview-Revised consistent with their diagnosis of Asperger's disorder or pervasive developmental disorder-not otherwise specified and, thus, were also included in the sample.
The present analysis consisted of 149 mothers who lived continuously with their son or daughter during the period between the second and third waves of the study. Co-residence was used as an inclusion criterion in order to be consistent with studies of family environments in the general population (Borkowski et al., 2002). In addition, families were excluded from the present analysis if the mother had died, declined participation, or could not be located at Time 2 or Time 3 (n = 96); cases for which the child's father was the primary respondent (n = 10); cases for which there were missing data on the measures of interest at Time 2 or Time 3 (n = 48); and when the child was not living with the mother at Time 2 and/or Time 3 (n = 103).
The mothers included in the subsample used for the present study ranged in age from 34.0 to 80.8 years at Time 2 (M = 49.3 SD = 8.8). Most mothers were married (81.6%) and nearly all had completed high school (98.0%). Approximately 22% of mothers did not have schooling beyond high school, 44% had some college or BA degree, and 33% had some graduate education or graduate degree. Over two thirds of mothers were employed either part- or full-time (70.1%). The median annual household income was $50,000–$59,000 in 2000–2001. The majority of participants were White, with 7.4% persons of color.
The adolescents and adults with autism spectrum disorder in the subsample used for the present study ranged in age from 11.3 to 48.9 years at Time 2 (M = 19.9, SD = 7.84). Consistent with the higher prevalence of autism among males compared with females (American Psychiatric Association, 2000), the majority of the sample was male (75.5%). Fifty-seven percent of the sample had a comorbid diagnosis of mental retardation.
Procedure and Measures
At both Times 2 and 3, mothers completed self-administered questionnaires and participated in a 2- to 3-hr in-home interview. Data collection for Time 2 and Time 3 occurred approximately 18 months apart.
Praise about the child
The Five Minute Speech Sample was used to code praise based on the coding manual developed by Magaña et al. (1986). For the measure, mothers were asked to speak about their child with autism spectrum disorder for 5 min uninterrupted. The speech sample was tape-recorded, transcribed, and coded for various components of expressed emotion, including criticism, overinvolvement, positive remarks, and warmth. In a previous paper, we reported our findings about criticism and emotional overinvolvement (Greenberg, Seltzer et al., 2006). In this present paper, we focused on maternal praise (as indicated by the number of positive remarks) and maternal warmth. Although positive remarks have been conceptualized as one indicator of overinvolvement, some researchers have argued that for families of children with chronic illnesses or disabilities, it likely reflects positivity and is conceptually distinct from other indicators of overinvolvement, such as excessive self-sacrificing behavior and overprotectiveness that have a more negative valence (Wamboldt, O'Connor, Wamboldt, Gavin, & Klinnert, 2000). This may be particularly the case because positive remarks may be viewed as efforts of the parent to praise the child's positive behaviors and to enhance the child's self-esteem. Therefore, in this analysis, we conceptualized the number of positive remarks as a distinct dimension of the family environment reflecting maternal praise and one that represents a prosocial family behavior.
As part of the protocol for coding the Five Minute Speech Sample, raters record the number of times a mother praises her son or daughter. Because few mothers made more than five positive remarks, scores of five or greater were recoded to five. The ratings of the Five Minute Speech Sample were performed by a coder with 20 years experience in coding all aspects of expressed emotion. An independent second rater also coded 15 tapes with a correlation coefficient of .83 in their coding of the number of positive remarks. The following transcript, which represents a composite case, provides an example of a mother high on our measure of praise (i.e., made a high number of positive remarks about the child during the Five Minute Speech Sample).
George has a fantastic sense of humor, and is caring and affectionate. We are really proud of George and the progress he has made. He is very courageous. He has faced a lot of horrendous treatment in school and from certain people, and he continues to have a wonderful outlook on life and be very positive.
Warmth
Ratings of warmth were also coded from the Five Minute Speech Sample. Because this measure typically is not used to generate individual ratings of warmth, we used the guidelines from the Camberwell Family Interview (Vaughn & Leff, 1976). Warmth ratings were based on (a) tone of voice; (b) spontaneity of expression of sympathy, concern, and empathy; and (b) expression of interest in the child with autism. Level of warmth was rated on a 5-point scale from 0 (no warmth) to 4 (high warmth). Warmth ratings were coded by the same rater who coded praise. A second rater independently coded 15 taped speech samples. The two raters had an interrater reliability of .79 for ratings of warmth. The following transcript represents a composite case of how a mother classified as high in warmth speaks about her child.
Carrie's taking Spanish this year. At first she was quite concerned and kept saying this is just too much to remember. And I just kept encouraging her. And I enjoy Spanish, so I enjoyed helping her. I always feel that she does the best she can and tries to pull her weight around the house. Last fall, to our surprise, she wanted to join the tennis group with me and my husband, and she did very well. Of course, she was the lowest ranked on the team but she still had fun, which I think was great. It wasn't about winning, but about being able to play. It's always so interesting to see her perspective on things. She looks at things just the way they are.
It is important to note that the ratings of warmth and praise taken from the Five Minute Speech Sample are measures of maternal verbal behavior about the child and are not observed measures of behavior directed at the child. Past research, however, has shown that this measure is a strong predictor of child outcomes (Butzlaff & Hooley, 1998; Greenberg, Seltzer et al., 2006). Additionally, researchers have found a significant relationship between observed family behavior and expressed emotion ratings (Hahlweg et al., 1989; McCarty, Lau, Valeri, & Weisz, 2004; Woo, Goldstein, & Nuechterlein, 2004).
Mother–child relationship quality
Mother–child relationship quality was assessed using the Positive Affect Index (Bengtson & Schrader, 1982). Five self-report items that reflected the mother's feelings toward her son or daughter (e.g. “How much affection do you have toward your son/daughter?”) were used from this scale. Items rated understanding, trust, fairness, respect, and affection in the relationship on a 6-point scale (1 = not at all, 2 = not much, 3 = some, 4 = pretty much, 5 = very much, 6 = extremely). Previous researchers have established the construct and discriminant validity of the Positive Affect Index (Bengtson & Allen, 1993; Bengtson & Schrader, 1982; Greenberg, Seltzer, Krauss, Chou, & Hong, 2004). This index has been found to be a reliable measure of maternal positive affect toward adolescent and adult children with autism (Orsmond et al., 2006).
Autism symptoms
Autism symptoms were measured using the Autism Diagnostic Interview-Revised–ADI-R (Lord, Rutter, & Le Couteur, 1994; Rutter et al., 2003). The ADI-R is a standardized, structured interview with items based on the criteria for an autism diagnosis in the Diagnostic and Statistical Manual of Mental Disorder-fourth edition, text revision–DSM-IV-TR (American Psychiatric Association, 2000). Only items required for the diagnostic algorithm of the ADI-R were administered (C. Lord, personal communication, February 1999). Each item was coded with a score of 0, indicating no abnormality present; 1, possible abnormality; 2, definite abnormality; or 3, extreme abnormality with respect to behavior. Based on the suggestions of Lord et al. (1994), we recoded scores of 3 to be scores of 2. The lifetime ratings for the algorithm items were used to confirm a diagnosis of autism spectrum disorder, whereas the current ratings of behavior derived from algorithm items were used in the present analyses.
The ADI-R provides items that assess the three core symptoms used in the diagnosis of autism: impairments in communication, impairments in reciprocal social interaction, and repetitive behaviors and interests. The Communication domain of the ADI-R consists of 11 items reflecting impairments in communication. Only 4 of these items, however, are administered to both verbal and nonverbal individuals: pointing to express interest, gestures, nodding, and head-shaking. Scores for these 4 items were summed to calculate an overall score for current level of impairments in nonverbal communication. Impairments in the Reciprocal Social Interaction domain were measured by summing ratings of 14 items: direct gaze, social smiling, range of facial expression, interest in people, response to others' approaches, friendships, directing attention, offering to share, sharing enjoyment with others, use of other's body, offering comfort, quality of social overtures, inappropriate facial expressions, and appropriateness of social response. The Repetitive Behaviors and Restricted Interest domain assesses 7 symptoms of autism: circumscribed interests, unusual preoccupations, compulsion/rituals, hand and finger mannerisms, other complex mannerisms/body movements, repetitive use of objects/interest in parts, and unusual sensory interest. Ratings of these items were summed to calculate a total Repetitive Behaviors and Restricted Interests score. An 8th item, verbal rituals, was not used for this analysis because it is not administered to nonverbal individuals.
Prior to administering the ADI-R, each interviewer participated in an approved ADI-R training program. All interviews were taperecorded. Agreement among all interviewers and two PhD clinical psychologists experienced in the diagnosis of autism and the use of the ADI-R averaged 88%. Previous work has documented the test–retest reliability, diagnostic and convergent validity, and specificity and sensitivity of the ADI-R (Hill et al., 2001; Lord et al., 1997).
Behavior problems
The Problem Behavior subscale of the Scales of Independent Behavior-Revised–SIB-R (Bruininks, Woodcock, Weatherman, & Hill, 1996) was used to measure behavior problems. This subscale assesses eight behavior problems: hurtful to self, unusual or repetitive, withdrawn or inattentive, socially offensive, uncooperative, hurtful to others, destructive to property, and disruptive. For each behavior, mothers were asked to indicate whether their child had manifested the behavior in the last 6 months and, if so, to rate the frequency (1, less than once a month, to 5, one or more times an hour) and severity of each behavior (1, not serious, to 5, extremely serious). Using standardized algorithms (Bruininks et al., 1996), we translated frequency and severity scores into three subscale scores: Internalized Maladaptive Behavior (hurtful to self, unusual or repetitive habits, and withdrawn or inattentive behavior), Asocial Maladaptive Behavior (socially offensive and uncooperative behavior), and Externalized Maladaptive Behavior (hurtful to others, destructive to property, and disruptive behavior). The reliability and validity of the SIB-R has been previously demonstrated (Bruininks et al., 1996). Higher scores on the SIB-R reflect more severe behavior problems.
Mental retardation
Mental retardation status was determined using a variety of sources of information. Under the supervision of a PhD clinical psychologist, trained interviewers assessed IQ with the Wide Range Intelligence Test (Glutting, Adams, & Sheslow, 2000) and adaptive behavior, with the Vineland Screener (Sparrow, Carter, & Cicchetti, 1993). Individuals with standard scores of 70 or below on both measures were classified as having mental retardation, consistent with diagnostic guidelines (Luckasson et al., 2002). Those with scores above 75 on either measure were classified as not having mental retardation. For those sample members with scores between 71 and 75 on one or both measures, or for whom either of the measures was missing, we reviewed available records (standardized assessments; parent report of prior diagnoses, intellectual functioning, and adaptive behavior; and clinical and school records) and combined these records with a clinical consensus procedure to determine mental retardation status. Agreement among three independent raters (all psychologists, 1 master's level, and 2 PhDs) was reached on 77.8% of cases following the initial review. The remaining cases were discussed until 100% consensus was reached. Of the 149 participants in the present sample, 87 (58.4%) were classified as having mental retardation and 62 participants (41.6%) were classified as not having mental retardation.
Results
High Levels of Warmth and Praise
The means and SDs for the positive family process variables of maternal warmth, praise, and relationship quality are presented in Table 1 for both Time 2 and Time 3. It is important to note that many mothers demonstrated high levels of praise toward their son or daughter with autism spectrum disorder. For instance, at both time points almost 40% of mothers made three or more praise statements about their son or daughter during the Five Minute Speech Sample. In addition, the average number of praise statements in the current sample at Time 2 (M = 2.1, SD = 1.8) and Time 3 (M = 2.0, SD = 1.8) were higher than the number of praise statements found by Greenberg, Knudsen, and colleagues (2006; M = 1.6, SD = 1.6) among families of individuals with schizophrenia.
Table 1.
Means and SDs of Study Variables by Time
| Time/Variable | Mean | SD |
|---|---|---|
| Time 2 | ||
| Praise | 2.14 | 1.75 |
| Warmth | 3.13 | 1.06 |
| Relationship quality | 23.67 | 3.44 |
| SIB-Ra | ||
| Externalizing | 104.98 | 9.79 |
| Internalizing | 113.37 | 9.55 |
| Asocial | 110.50 | 11.39 |
| ADI-Rb | ||
| Repetitive Behaviors | 4.66 | 2.09 |
| Social Reciprocity | 14.79 | 6.12 |
| Communication | 4.69 | 2.59 |
| Time 3 | ||
| Praise | 1.95 | 1.79 |
| Warmth | 3.32 | 1.05 |
| Relationship quality | 23.59 | 3.46 |
| SIB-R | ||
| Externalizing | 106.09 | 11.41 |
| Internalizing | 113.20 | 10.11 |
| Asocial | 111.11 | 12.16 |
| ADI-R | ||
| Repetitive Behaviors | 4.62 | 2.30 |
| Social Reciprocity | 14.01 | 6.03 |
| Communication | 4.56 | 2.54 |
| Gender | .77 | .43 |
| Mental retardation status | .58 | .50 |
Scales of Independent Behavior-Revised.
Autism Diagnostic Interview-Revised.
Similarly, 37% and 46% of mothers at Time 2 and Time 3, respectively, were rated as moderately high or high on warmth. The average warmth ratings at both Time 2 (M = 3.1, SD = 1.1) and Time 3 (M = 3.3, SD = 1.1) were similar to the warmth ratings (M = 3.1, SD = 1.1) reported by Greenberg, Knudsen et al. (2006) and slightly higher than warmth ratings (M = 2.8, SD = 1.4) reported by Lopez et al. (2004) and King and Dixon in 1999 (M = 2.9, SD = 1.0). The three dimensions of warmth, praise, and relationship quality were moderately intercorrelated, r = .22 to .49, suggesting that these are related, but not redundant indicators of the family environment.
Bidirectional Effects
We employed a cross-lagged panel analysis to examine the bidirectional effects of positive family processes (maternal warmth, praise, and quality of the mother–child relationship) and children's behavior problems and autism symptoms. Cross-lagged models are frequently utilized in family research to consider bidirectional effects of family characteristics and children's behavior (Delsing, Oud, & Bruyn, 2005), including studies of families with children who have developmental disabilities (Greenberg, Seltzer et al., 2006; Orsmond, Seltzer, Krauss, & Hong, 2003). We used LISREL 8.54 to test 6 two-wave, cross-lagged models. The cross-lagged design allows for tests of both stability effects and cross-lagged effects. For each variable, the Time 3 value (e.g., autism symptoms) was predicted by the Time 2 value (e.g., autism symptoms) as well as the cross-lagged variable (e.g., praise). In each model, children's gender and mental retardation status were included as control variables. All variables measured at the same time point were allowed to correlate, resulting in a fully saturated model. A conceptual model is presented in Figure 1. The Pearson product-moment correlations among all study variables at Time 2 and Time 3 are shown in Table 2.
Figure 1.
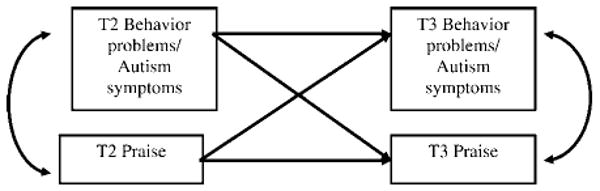
Conceptual model of relationship between praise and behavior problems and symptoms of autism.
Table 2.
Pearson Correlations Among Study Variables by Time
| Time/Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time 2 | ||||||||||||||||||||
| 1. Praise | 1 | |||||||||||||||||||
| 2. Warmth | .46 | 1 | ||||||||||||||||||
| 3. RQa | .22 | .34 | 1 | |||||||||||||||||
| 4. SIB-Rb Externalizing | −.19 | −.20 | −.34 | 1 | ||||||||||||||||
| 5. SIB-R Internalizing | −.09 | .10 | −.33 | .46 | 1 | |||||||||||||||
| 6. SIB-R Asocial | −.10 | .18 | −.30 | .62 | .55 | 1 | ||||||||||||||
| 7. ADI-Rc Repetitive Behaviors | −.12 | −.20 | −.13 | .32 | .37 | .29 | 1 | |||||||||||||
| 8. AID-R Social Reciprocity | −.25 | −.18 | −.18 | .19 | .39 | .18 | .28 | 1 | ||||||||||||
| 9. ADI-R Communication | −.29 | −.18 | −.11 | .00 | .14 | .03 | .03 | .59 | 1 | |||||||||||
| Time 3 | ||||||||||||||||||||
| 10. Praise | −.12 | .37 | .27 | −.19 | −.16 | −.07 | −.10 | −.30 | −.24 | 1 | ||||||||||
| 11. Warmth | .35 | .70 | .36 | −.23 | −.08 | −.14 | −.15 | −.17 | −.18 | .49 | 1 | |||||||||
| 12. RQ | .11 | .27 | .77 | −.34 | −.24 | −.26 | −.13 | −.08 | −.04 | .26 | .35 | 1 | ||||||||
| 13. SIB-R Externalizing | −.11 | −.16 | −.40 | .76 | .47 | .58 | .27 | .24 | .06 | −.27 | −.34 | −.44 | 1 | |||||||
| 14. SIB-R Internalizing | −.13 | −.13 | −.39 | .41 | .64 | .37 | .27 | .39 | .08 | −.24 | −.16 | −.38 | .57 | 1 | ||||||
| 15. SIB-R Asocial | −.16 | −.11 | −.31 | .54 | .37 | .63 | .14 | .13 | .04 | −.16 | −.19 | −.27 | .67 | .50 | 1 | |||||
| 16. ADI-R Repetitive Behaviors | −.27 | −.25 | −.26 | .31 | .44 | .38 | .59 | .33 | .08 | −.22 | −.18 | −.17 | .34 | .43 | .33 | 1 | ||||
| 17. AID-R Social Reciprocity | −.23 | −.15 | −.23 | .20 | .33 | .15 | .27 | .87 | .54 | −.31 | −.20 | −.16 | .29 | .38 | .19 | .29 | 1 | |||
| 18. ADI-R Communication | −.19 | −.18 | −.06 | .02 | .07 | .04 | .07 | .57 | .83 | −.17 | −.10 | −.02 | .05 | .07 | −.01 | .10 | .51 | 1 | ||
| 19. Gender | .01 | .07 | .12 | .03 | .01 | −.03 | .06 | .02 | .03 | .04 | .06 | .08 | −.02 | −.02 | .04 | .04 | .09 | .08 | 1 | |
| 20. MR status | −.16 | .06 | −.10 | .10 | .13 | .08 | .13 | .37 | .30 | −.26 | −.09 | −.02 | .19 | .17 | .22 | .22 | .40 | .21 | −.02 | 1 |
Relationship quality.
Scales of Independent Behavior-Revised.
Autism Diagnostic Interview-Revised.
Behavior problems
The three models in Table 3 show the bidirectional effects of positive family processes (praise, warmth, and relationship quality) and behavior problems of the son or daughter with autism as measured using the SIB-R. The coefficients for praise are provided in Model 1, followed by the coefficients for warmth and relationship quality in Models 2 and 3, respectively.
Table 3.
Unstandardized Path Coefficients for Two-Wave Cross-Lagged Models for Subscales of the Scales of Independents Behavior-Revised (SIB-R)
| Behavior | |||
|---|---|---|---|
| Model | Externalizing | Internalizing | Asocial |
| Model 1: Praise | |||
| Stability effects | |||
| T2 Praise to T3 Praise | .26 (.08)*** | .28 (.08)*** | .28 (.08)*** |
| T2 SIB-R to T3 SIB-R | .88 (.06)*** | .66 (.07)*** | .65 (.07)*** |
| Cross-lagged effects | |||
| T2 Praise to T3 SIB-R | .36 (.36) | −.36 (.37) | −.53 (.44) |
| T2 SIB-R to T3 Praise | −.02 (.01) | −.02 (.02) | .00 (.01) |
| Control variables | |||
| Gender of child to T3 SIB-R | −.94 (1.44) | −.43 (1.50) | 1.65 (1.79) |
| Gender of child to T3 Praise | .14 (.32) | .13 (.32) | .13 (.33) |
| MRa to T3 SIB-R | 2.76 (1.26)* | 1.71 (1.32) | 3.93 (1.56)* |
| MR to T3 Praise | −.73 (.28)* | −.71 (.28)* | −.76 (.28)* |
| Model 2: Warmth | |||
| Stability effects | |||
| T2 Warmth to T3 Warmth | .69 (.06)*** | .70 (.06)*** | .70 (.06)*** |
| T2 SIB-R to T3 SIB-R | .86 (.06)*** | .66 (.07)*** | .66 (.07)*** |
| Cross-lagged effects | |||
| T2 Warmth to T3 SIB-R | −.20 (.59) | −.72 (.61) | −.21 (.74) |
| T2 SIB-R to T3 Warmth | −.01 (.01) | .00 (.01) | .00 (.01) |
| Control variables | |||
| Gender of child to T3 SIB-R | −.88 (1.45) | −.31 (1.50) | 1.68 (1.80) |
| Gender of child to T3 Warmth | .04 (.14) | .03 (.15) | .03 (.15) |
| MR to T3 SIB-R | 2.62 (1.25)* | 2.0 (1.30) | 4.25 (1.56)** |
| MR to T3 Warmth | −.26 (.12)* | −.28 (.13)* | −.28 (.13)* |
| Model 3: Relationship Quality (RQ) | |||
| Stability effects | |||
| T2 RQ to T3 RQ | .75 (.06)*** | .78 (.06)*** | .77 (.06)*** |
| T2 SIB-R to T3 SIB-R | .81 (.07)*** | .60 (.07)*** | .62 (.07)*** |
| Cross-lagged effects | |||
| T2 RQ to T3 SIB-R | −.52 (.19)** | −.56 (.19)** | −.45 (.23)† |
| T2 SIB-R to T3 RQ | −.03 (.02)† | .00 (.02) | −.01 (.02) |
| Control variables | |||
| Gender of child to T3 SIB-R | −.38 (1.42) | .11 (1.48) | 2.05 (1.79) |
| Gender of child to T3 RQ | −.05 (.44) | −.11 (.44) | −.10 (.44) |
| MR to T3 SIB-R | 2.35 (1.22)† | 1.68 (1.27) | 3.98 (1.54)* |
| MR to T3 RQ | .49 (.37) | .44 (.38) | .46 (.38) |
Note. Unstandardized coefficients with standard errors presented in parentheses. T2 = Time 2, T3 = Time 3.
Mental retardation.
p < .10.
p <.05.
p <.01.
p < .001.
In Model 1, all three of the SIB-R subscales demonstrated significant stability effects from Time 2 to Time 3. In the analysis of praise, the stability coefficients for externalizing, internalizing, and asocial behavior were .88, .66, and .65, respectively. In the analysis of warmth and relationship quality, the stability coefficients for the SIB-R subscales were similarly significant, ranging from .60 to .86 with ps less than .001.
Each of the indicators of positive family processes also displayed significant stability from Time 2 to Time 3. The stability coefficients for praise ranged from .25 to .28 in all models. The stability coefficients for warmth and relationship quality were considerably higher, ranging from .69 to .70 for warmth and from .75 to .79 for relationship quality.
Next, we examined the cross-lagged effects of positive family processes and the three SIB-R subscales. Counter to our hypothesis, as shown in Models 1 and 2 described in Table 3, there were no significant cross-lagged effects for praise or warmth and the SIB-R measures of behavior problems. However, consistent with our hypothesis, there were significant cross-lagged effects between relationship quality and the SIB-R subscales.
As shown in Model 3 in Table 3, a high level of relationship quality at Time 2 was associated with significantly fewer externalizing problems at Time 3, B = −.52, SE = .19, and reciprocally, a high level of externalizing problems at Time 2 showed a trend toward decreases in relationship quality at Time 3, B = −.03, SE = .02, thus demonstrating a bidirectional relationship between relationship quality and externalizing behaviors. A high level of relationship quality at Time 2 was also associated with a decrease in internalizing behaviors, B = −.56, SE = .19, and there was a trend toward decreased asocial problems at Time 3, B = −.45, SE = .23. Neither internalizing problems at Time 2 nor asocial problems at Time 2 had a reciprocal effect on relationship quality at Time 3.
Autism symptoms
The three models presented in Table 4 show the bidirectional effects of positive family processes (praise, warmth, and relationship quality) and children's autism symptoms. As with children's behavior problems, autism symptoms were highly stable from Time 2 to Time 3. Stability coefficients ranged from .59 to .83, with ps < .001.
Table 4.
Unstandardized Path Coefficients for Two-Wave Cross-Lagged Models for Autism Diagnostic Inventory-Revised (ADI-R) Measures of Symptoms
| Model | Repetitive behaviors and restricted interests | Impairments in reciprocal social interactions | Impairments in nonverbal communication |
|---|---|---|---|
| Model 1: Praise | |||
| Stability effects | |||
| T2 Praise to T3 Praise | .28 (.08)*** | .25 (.08)*** | .26 (.08)*** |
| T2 ADI-R to T3 ADI-R | .61 (.07)*** | .82 (.04)*** | .83 (.05)*** |
| Cross-lagged effects | |||
| T2 Praise to T3 ADI-R | −.24 (.09)** | −.04 (.14) | .07 (.07) |
| T2 ADI-R to T3 Praise | −.04 (.07) | −.06 (.02)* | −.08 (.06) |
| Control variables | |||
| Gender of child to T3 ADI-R | .05 (.35) | 1.05 (.57) | .31 (.28) |
| Gender of child to T3 Praise | .14 (.33) | .15 (.32) | .15 (.32) |
| MRa to T3 ADI-R | .57 (.31)† | 1.15 (.52)* | −.21 (.25) |
| MR to T3 Praise | −.74 (.29)* | −.53 (.30) | −.66 (.29)* |
| Model 2: Warmth | |||
| Stability effects | |||
| T2 Warmth to T3 Warmth | .70 (.06)*** | .70 (.06)*** | .70 (.06)*** |
| T2 ADI-R to T3 ADI-R | .59 (.07)*** | .82 (.04)*** | .81 (.05)*** |
| Cross-lagged effects | |||
| T2 Warmth to T3 ADI-R | −.33 (.14)* | −.04 (.23) | −.06 (.12) |
| T2 ADI-R to T3 Warmth | .00 (.03) | .00 (.01) | −.01 (.03) |
| Control variables | |||
| Gender of child to T3 ADI-R | .11 (.35) | 1.06 (.57) | .32 (.28) |
| Gender of child to T3 Warmth | .03 (.15) | .03 (.15) | .03 (.15) |
| MR to T3 ADI-R | .75 (.31)* | 1.17 (.53)* | −.22 (.25) |
| MR to T3 Warmth | −.28 (.13)* | −.28 (.14)* | −.27 (.13)* |
| Model 3: Relationship Quality (RQ) | |||
| Stability effects | |||
| T2 RQ to T3 RQ | .78 (.06)*** | .79 (.06)*** | .78 (.06)*** |
| T2 ADI-R to T3 ADI-R | .60 (.07)*** | .81 (.04)*** | .82 (.05)*** |
| Cross-lagged effects | |||
| T2 RQ to T3 ADI-R | −.12 (.04)** | −.15 (.07)* | .02 (.04) |
| T2 ADI-R to T3 RQ | −.06 (.09) | .03 (.03) | .05 (.08) |
| Control variables | |||
| Gender of child to T3 ADI-R | .16 (.35) | 1.2 (.56)* | .29 (.28) |
| Gender of child to T3 RQ | −.08 (.44) | −.12 (.44) | −.12 (.44) |
| MR to T3 ADI-R | .62 (.31)* | 1.12 (.51)* | −.22 (.25) |
| MR to T3 RQ | .47 (.38) | .33 (.40) | .37 (.39) |
Note. T2 = Time 2, T3 = Time 3.
Mental retardation.
p < .10.
p <.05.
p <.01.
p < .001.
Next, we examined the cross-lagged effects for autism symptoms and positive family processes. As presented in Model 1 of Table 4, there were significant cross-lagged effects between praise and the ADI-R subscales. As predicted, a high level of praise at Time 2 was associated with decreases in repetitive behaviors at Time 3, B = −.24, SE = .09. However, repetitive behaviors at Time 2 did not have a significant effect on praise at Time 3. In contrast, a high level of impairments in social reciprocity at Time 2 was related to a low level of praise at Time 3, B = −.06, SE = .02, but the reciprocal effect between praise at Time 2 and social reciprocity impairments at Time 3 was not evident. There were no significant cross-lagged effects in either direction for praise and impairments in nonverbal communication.
Model 2 (Table 4) presents the coefficients for maternal warmth and the ADI-R subscales. Similar to the cross-lagged effects reported above, a high level of warmth at Time 2 was associated with decreases in repetitive behaviors at Time 3, B = −.33, SE = .14. However, repetitive behaviors at Time 2 were not related to warmth at Time 3. There were no significant cross-lagged effects in either direction between warmth and impairments in social reciprocity or communication.
As seen in Model 3 in Table 4, there were significant cross-lagged effects between relationship quality and autism symptoms. As predicted, a high level of relationship quality at Time 2 was associated with decreases in both repetitive behaviors, B = −.12, SE = .04, and social reciprocity impairments, B = −.15, SE = .07, Time 3. These autism symptoms at Time 2, however, were not related to the quality of the relationship at Time 3. There were no significant associations between relationship quality and impairments in communication.
Control variables
In each of the aforementioned models, the relationships between the control variables (gender and mental retardation status) and behavior problems and autism symptoms were examined. As anticipated, mental retardation status was associated with more externalizing and asocial behaviors as well as more severe repetitive behaviors and more severe impairments in reciprocal social interactions. Consistent with other studies indicating poorer social functioning among girls (Carter et al., 2007), females had more severe social reciprocity impairments.
The associations between the control variables and the measures of prosocial family processes were also included in each of the models. Mothers of a son or daughter with mental retardation had lower levels of warmth and praise than did mothers of children without mental retardation. Indicators of prosocial family processes did not differ by gender of the child.
Finally, as part of a post-hoc examination of the data, we adapted our original analytic framework to examine the potential moderating effects of age of child and mental retardation status on the aforementioned models. We additionally evaluated models in which family environmental factors (warmth, praise, and relationship status at Time 2) interacted with autism symptoms and behavior problems at Time 2 to predict autism symptoms and behavior problems at Time 3. Of these numerous models involving interactions, very few interaction terms were significant (3 out of 36), indicating that our original main effects model was more appropriate for understanding these relationships. Results of these post-hoc models are available from the first author.
Discussion
In the present study we highlighted how positive aspects of the family environment are linked with autism symptoms and problem behaviors within families of adolescents and adults with autism spectrum disorder. Specifically, the findings demonstrated that maternal warmth, praise, and relationship quality were related to subsequent reductions in behavior problems and abatement of autism symptoms. Previous work in this area has revealed relationships between negative emotional expression in families of children with disabilities and autism-related symptomatology and problem behaviors. For instance, our recent work has shown that high levels of maternal expressed emotion are associated with increases in maladaptive behaviors and symptoms for adolescent and adult children with autism (Greenberg, Seltzer et al., 2006). Similarly, in a sample of children with intellectual disabilities, high maternal criticism, but not emotional overinvolvement, was related to children's externalizing problems (Hastings, Daley et al., 2006). The emphasis on positive familial interaction in the present study represents a shift away from deficit-based conceptualizations of developmental disabilities to a more comprehensive view of family factors as mechanisms of positive change for individuals with autism.
We hypothesized that maternal warmth, praise, and relationship quality would be important predictors of declining problem behaviors over time. Consistent with our hypothesis, positive relationship quality between mothers and their sons or daughters with autism spectrum disorder was associated with decreases in internalizing and externalizing behaviors and a trend toward fewer asocial behavior problems in the adolescents and adults in our sample. Also consistent with our hypotheses, relationship quality, warmth, and praise were stable over an 18-month period; the stability coefficients for warmth and relationship quality were particularly high. These results echo previous findings that expressed emotion remains moderately stable over time (Greenberg, Seltzer et al., 2006), perhaps indicating that emotional expressiveness is an enduring quality of families. It is also particularly interesting to note that although family members of individuals with autism are at a higher biological risk for affective problems (Micali, Chakrabarti, & Fombonne, 2004; Piven & Palmer, 1999), most mothers in the current study displayed positive emotional expression in reference to their child.
Positive aspects of the family environment were also associated with abatement of autism symptoms over an 18-month period. Specifically, high levels of maternal warmth, praise, and relationship quality were related to subsequent reductions in repetitive behaviors. A high level of relationship quality between mother and child was likewise predictive of improvements in impairments in social reciprocity. These findings are analogous to studies of children's behavior problems and symptomatology in other populations. In studies of children without developmental disabilities, high maternal warmth has been associated with better behavioral outcomes in children (Caspi et al., 2004; Eisenberg et al., 2001; Tully et al., 2004). Warmth from family members has also been related to better life satisfaction (Greenberg, Knudsen et al., 2006) for individuals with schizophrenia. Furthermore, interventions that have demonstrated improvements in family affective climate (e.g., decreased criticism, increased praise) have resulted in better behavioral outcomes for children and adolescents (Webster-Stratton, Reid, & Hammond, 2004). The results of the current study emphasize the important role of positive parent–child interactions in reducing symptoms and behavior problems in adolescents and adults with autism.
Cross-sectional as well as longitudinal studies have demonstrated that improvements in autism symptoms are often evident as children grow into adulthood (Seltzer, Shattuck, Abbeduto, & Greenberg, 2004), particularly in the domain of repetitive behaviors and restricted interests (Shattuck et al., 2007). Several factors, including medications, intervention, and other treatments, may be associated with this abatement of symptoms. The present study showed that aspects of the family environment (maternal warmth, praise, and relationship quality) are related to improvements in repetitive behaviors. These results highlight how a positive family climate may be an additional mechanism for change in repetitive behaviors over time. As such, interventions aiming to increase warmth and praise among families of individuals with autism spectrum disorder may in turn result in significant improvements in autism symptoms.
The present study also revealed that parent– child interactions in families of individuals with autism are not exclusively unidirectional. Although the direction of effects for most findings in the present study was from mother to child, there was some evidence of children's symptoms influencing mothers. Specifically, children's impairments in social reciprocity were associated with lower levels of maternal praise 18 months later. These results are consistent with the cross-sectional findings of Orsmond et al. (2006), who demonstrated that child characteristics, specifically, less severe maladaptive behaviors, better health, and less severe social impairments, predicted higher levels of relationship quality. Thus, parental behavior does not occur in a vacuum. Instead, there is some evidence for bidirectional processes among adolescents and adults with autism spectrum disorder and their families.
It is also interesting that although mothers' perceptions of relationship quality were associated with both children's behavior problems and autism symptoms, maternal warmth and praise were only predictive of autism symptoms, specifically repetitive behaviors. Although this apparent differential prediction may be related to the specific methods by which the factors were measured, it may also be that repetitive behaviors are more influenced by these positive aspects of the family environment than general maladaptive behaviors or other autism symptoms. A mother's expressed warmth and praise, for instance, may create an environment associated with less stress and aggravation for the child, which in turn may lead to a reduction in repetitive behaviors. It may be that these environmental factors have more salience for repetitive behaviors than for communication or social abilities. In contrast, relationship quality may be a better measure of the family processes that impact a wide range of symptoms and behaviors. Future researchers should further investigate how specific aspects of the parent–child relationship may act as mechanisms of change for both autism symptoms and behavior problems.
The present study was not without limitations. First, we only examined the parent–child relationship with two measurement points over an 18-month window of time. Because patterns of interactions develop over the course of the lifespan (Aquilino, 1997; Belsky, Jaffee, Caspi, Moffitt, & Silva, 2003), deeper insights into the processes by which parents and children influence each other could be gained by extending the measurement window and/or by using different measurement intervals. Second, mothers reported on their son or daughter's behaviors as well as the quality of the parent–child relationship, resulting in shared method variance between these two measures. However, the measures of warmth and praise were independently rated. Third, the measures of warmth and praise were based on mother's verbal behavior about the child, not direct observation of behavior toward the child. However, the predictive utility of these ratings from the Five Minute Speech Sample highlights the value of using short speech samples as an alternative to intensive observations. Fourth, the sample was predominately White and from Wisconsin and Massachusetts, limiting the generalizability of the findings. Finally, in the current study we did not address the positive characteristics of the son or daughter with autism spectrum disorder, but instead only examined behavior problems and autism symptoms. Future work should incorporate measures of positive characteristics, such as individual strengths and well-being into investigations of family processes and development in families of children with autism spectrum disorder (Dykens, 2006).
In conclusion, results of the present study highlight the positive ways in which mothers influence their child's development within the adolescent and adult period. When taken in conjunction with our previous findings that criticism and overinvolvement are low in this sample of mothers (Greenberg, Seltzer et al., 2006), the current findings stand in sharp contrast to the unmerited, negative characterizations of mothers of autism in the past. Most mothers in this sample were agents of positive change in their child's lives. Furthermore, in the present study we used a sample of adolescents and adults with autism spectrum disorder and their mothers in contrast with most researchers investigating autism and the family system, who have focused on the early part of the lifespan (Seltzer et al., 2001). In the present study we demonstrated that the family environment is an important contributor to children's developmental and behavioral functioning during adolescence and adulthood. Given the reduction in problems and symptoms associated with positive family environments in the present study, future multicomponent interventions should better tailor services to meet family needs by increasing warmth and praise among family members in addition to addressing problems related to symptoms and behaviors.
Acknowledgments
Support for the preparation of this paper was provided by grants from the National Institute on Aging (R01 AG08768), National Institute of Mental Health (R01 MH55928), National Institute of Child Health and Human Development (P30 HD03352, T32 HD07489), and National Institute on Disability and Rehabilitation Research (H133B031134) through the Rehabilitation Research and Training Center on Aging and Developmental Disabilities at the University of Illinois at Chicago.
Footnotes
Editor-in-charge: Frank Floyd and Leonard Abbeduto
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th. Washington, DC: Author; 2000. text rev. [Google Scholar]
- Aquilino WS. From adolescent to young adult: A prospective study of parent-child relations during the transition to adulthood. Journal of Marriage and the Family. 1997;59:670–686. [Google Scholar]
- Beck A, Daley D, Hastings RP, Stevenson J. Mothers' expressed emotion towards children with and without intellectual disabilities. Journal of Intellectual Disability Research. 2004;48:628–638. doi: 10.1111/j.1365-2788.2003.00564.x. [DOI] [PubMed] [Google Scholar]
- Belsky J, Jaffee SR, Caspi A, Moffitt T, Silva PA. Intergenerational relationships in young adulthood and their life course, mental health, and personality correlates. Journal of Family Psychology. 2003;17:460–471. doi: 10.1037/0893-3200.17.4.460. [DOI] [PubMed] [Google Scholar]
- Bengtson VL, Allen KR. The life course perspective applied to families over time. In: Boss P, Doherty W, LaRossa R, Schumm W, Steinmetz S, editors. Sourcebook of family theories and methods: A contextual approach. New York: Plenum Press; 1993. pp. 469–498. [Google Scholar]
- Bengtson VL, Schrader SS. Parent-child relationship. In: Mangon DJ, Peterson WA, editors. Research instruments in social gerontology. Vol. 2. Minneapolis: University of Minnesota Press; 1982. pp. 115–185. [Google Scholar]
- Borkowski JG, Ramey SL, Bristol-Power M, editors. Parenting and the child's world: Influences on academic, intellectual, and social-emotional development. Mahwah, NJ: Erlbaum; 2002. [Google Scholar]
- Bruininks RH, Woodcock RW, Weatherman RF, Hill BK. Scales of Independent Behavior-Revised. Itasca, IL: Riverside; 1996. [Google Scholar]
- Butzlaff RL, Hooley JM. Expressed emotion and psychiatric relapse: A meta-analysis. Archives of General Psychiatry. 1998;55:547–552. doi: 10.1001/archpsyc.55.6.547. [DOI] [PubMed] [Google Scholar]
- Carter AC, Black DO, Tewani S, Connolly CE, Kadlec MB, Tager-Flusberg H. Sex differences in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2007;37:86–97. doi: 10.1007/s10803-006-0331-7. [DOI] [PubMed] [Google Scholar]
- Caspi A, Moffitt TE, Morgan J, Rutter M, Taylor A, Arseneault L, Tully L, Jacobs C, Kim-Cohen J, Polo-Tomas M. Maternal expressed emotion predicts children's antisocial behavior problems: Using monozygotic-twin differences to identify environmental effects on behavior development. Developmental Psychology. 2004;40:149–161. doi: 10.1037/0012-1649.40.2.149. [DOI] [PubMed] [Google Scholar]
- Delsing MJMH, Oud JHL, De Bruyn EEJ. Assessment of bidirectional influences between family relationships and adolescent problem behavior: Discrete vs. continuous time analysis. European Journal of Psychological Assessment. 2005;21:226–231. [Google Scholar]
- Dykens EM. Toward a positive psychology of mental retardation. American Journal of Orthopsychiatry. 2006;76:185–193. doi: 10.1037/0002-9432.76.2.185. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Gershoff ET, Fabes RA, Shepard SA, Cumberland AJ, Losoya SH, Guthrie IK, Murphy BC. Mothers' emotional expressivity and children's behavior problems and social competence: Mediation through children's regulation. Developmental Psychology. 2001;37:475–490. doi: 10.1037//0012-1649.37.4.475. [DOI] [PubMed] [Google Scholar]
- Folstein SE, Rosen-Sheidley B. Genetics of autism: Complex aetiology for a heterogeneous disorder. Nature Reviews Genetics. 2001;2:943–955. doi: 10.1038/35103559. [DOI] [PubMed] [Google Scholar]
- Glutting J, Adams W, Sheslow D. Wide Range Intelligence Test. Wilmington, DE: Wide Range; 2000. [Google Scholar]
- Greenberg JS, Knudsen KJ, Aschbrenner KA. Prosocial family processes and the quality of life of persons with schizophrenia. Psychiatric Services. 2006;57:1771–1777. doi: 10.1176/appi.ps.57.12.1771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenberg JS, Seltzer MM, Hong J, Orsmond GI. Bidirectional effects of expressed emotion and behavior problems and symptoms in adolescents and adults with autism. American Journal on Mental Retardation. 2006;111:229–249. doi: 10.1352/0895-8017(2006)111[229:BEOEEA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Greenberg JS, Seltzer MM, Krauss MW, Chou RJ, Hong J. The effect of quality of the relationship between mothers and adult children with disabilities: The mediating role of optimism. American Journal of Orthopsychiatry. 2004;74:14–25. doi: 10.1037/0002-9432.74.1.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hahlweg K, Goldstein MJ, Nuechterlein KH, Magaña AB, Mintz J, Doane JA, Miklowitz DG, Snyder KS. Expressed emotion and patient-relative interaction in families of recent onset schizophrenics. Journal of Consulting and Clinical Psychology. 1989;57:11–18. doi: 10.1037//0022-006x.57.1.11. [DOI] [PubMed] [Google Scholar]
- Hastings RP, Brown T. Behavior problems of children with autism, parental self-efficacy, and mental health. American Journal on Mental Retardation. 2002;107:222–232. doi: 10.1352/0895-8017(2002)107<0222:BPOCWA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Hastings RP, Daley D, Burns C, Beck A. Maternal distress and expressed emotion: Cross-sectional and longitudinal relationships with behavior problems of children with intellectual disabilities. American Journal on Mental Retardation. 2006;111:48–61. doi: 10.1352/0895-8017(2006)111[48:MDAEEC]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Hastings RP, Kovshoff H, Ward NJ, degli Espinosa F, Brown T, Remington B. Systems analysis of stress and positive perceptions in mothers and fathers of preschool children with autism. Journal of Autism and Developmental Disorders. 2005;35:635–644. doi: 10.1007/s10803-005-0007-8. [DOI] [PubMed] [Google Scholar]
- Herring S, Gray K, Taffe J, Tonge B, Sweeney D, Einfeld S. Behavioral and emotional problems in toddlers with pervasive developmental disorders and developmental delay: Associations with parental mental health and family functioning. Journal of Intellectual Disability Review. 2006;50:874–883. doi: 10.1111/j.1365-2788.2006.00904.x. [DOI] [PubMed] [Google Scholar]
- Hill A, Boelte S, Petrova G, Beltcheva D, Tacheva S, Poustka F. Stability and interpersonal agreement of the interview-based diagnosis of autism. Psychopathology. 2001;34:187–191. doi: 10.1159/000049305. [DOI] [PubMed] [Google Scholar]
- King S, Dixon MJ. Expressed emotion and relapse in young schizophrenia outpatients. Schizophrenia Bulletin. 1999;25:377–386. doi: 10.1093/oxfordjournals.schbul.a033385. [DOI] [PubMed] [Google Scholar]
- Lecavalier L, Leone S, Wiltz J. The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research. 2006;50:172–183. doi: 10.1111/j.1365-2788.2005.00732.x. [DOI] [PubMed] [Google Scholar]
- Lopez SR, Hipke KN, Polo AJ, Jenkins JH, Karno M, Vaughn C, Snyder KS. Ethnicity, expressed emotion, attributions, and course of schizophrenia: Family warmth matters. Journal of Abnormal Psychology. 2004;113:428–439. doi: 10.1037/0021-843X.113.3.428. [DOI] [PubMed] [Google Scholar]
- Lord C, Pickles A, McLennan J, Rutter M, Bregman J, Folstein S, Fombonne E, Leboyer M, Minshew N. Diagnosing autism: Analyses of data from the Autistic Diagnostic Interview. Journal of Autism and Developmental Disorders. 1997;27:501–517. doi: 10.1023/a:1025873925661. [DOI] [PubMed] [Google Scholar]
- Lord C, Rutter M, Le Couteur A. Autism Diagnostic Interview–Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders. 1994;24:659–685. doi: 10.1007/BF02172145. [DOI] [PubMed] [Google Scholar]
- Lounds JJ, Seltzer MM, Greenberg JS, Shattuck P. Transition and change in adolescents and young adults with autism: Longitudinal effects on maternal well-being. American Journal on Mental Retardation. 2007;112:401–417. doi: 10.1352/0895-8017(2007)112[401:TACIAA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Luckasson R, Borthwick-Duffy S, Buntinx WHE, Coulter DL, Craig EM, Reeve A, Schalock RL, Snell ME, Spitalnik DM, Spreat S, Tassé MJ. Mental retardation: Definition, classification, and systems of supports. 10th. Washington, DC: American Association on Mental Retardation; 2002. [Google Scholar]
- Magaña AB, Goldstein MJ, Karno M, Miklowitz DJ, Jenkins J, Falloon IRH. A brief method for assessing expressed emotion in relatives of psychiatric patients. Psychiatry Research. 1986;17:203–212. doi: 10.1016/0165-1781(86)90049-1. [DOI] [PubMed] [Google Scholar]
- McCarty CA, Lau AS, Valeri SM, Weisz JR. Parent-child interactions in relation to critical and emotionally over-involved expressed emotion (EE): Is EE a proxy for behavior? Journal of Abnormal Child Psychology. 2004;32:83–93. doi: 10.1023/b:jacp.0000007582.61879.6f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Micali N, Chakrabarti S, Fombonne E. The broad autism phenotype: Findings from an epidemiological survey. Autism. 2004;8:21–37. doi: 10.1177/1362361304040636. [DOI] [PubMed] [Google Scholar]
- Orsmond GI, Seltzer MM, Greenberg JS, Krauss MW. Mother–child relationship quality among adolescents and adults with autism. American Journal on Mental Retardation. 2006;111:121–137. doi: 10.1352/0895-8017(2006)111[121:MRQAAA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Orsmond GI, Seltzer MM, Krauss MW, Hong J. Behavior problems in adults with mental retardation and maternal well-being: Examination of the direction of effects. American Journal on Mental Retardation. 2003;108:257–271. doi: 10.1352/0895-8017(2003)108<257:BPIAWM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Overbeek G, Stattin H, Vermulst A, Ha T, Engels RCME. Parent-child relationships, partner relationships, and emotional adjustment: A birth-to-maturity prospective study. Developmental Psychology. 2007;43:429–437. doi: 10.1037/0012-1649.43.2.429. [DOI] [PubMed] [Google Scholar]
- Piven J, Palmer P. Psychiatric disorders and the broad autism phenotype: Evidence from a family study of multiple incidence autism families. American Journal of Psychiatry. 1999;156:557–563. doi: 10.1176/ajp.156.4.557. [DOI] [PubMed] [Google Scholar]
- Rossi AS, Rossi PH. Of human bonding: Parent-child relations across the life course. Hawthorne, NY: Aldine de Gruyter; 1990. [Google Scholar]
- Rutter M, Le Couteur A, Lord C. ADI-R Autism Diagnostic Interview-Revised WPS Edition. Los Angeles: Western Psychological Services; 2003. [Google Scholar]
- Ryff CD, Love GD, Urry HL, Muller D, Rosenkranz MA, Friedman EM, Davidson RJ, Singer B. Psychological well-being and ill-being: Do they have distinct or mirrored biological correlates? Psychotherapy and Psychosomatics. 2006;75:85–95. doi: 10.1159/000090892. [DOI] [PubMed] [Google Scholar]
- Seltzer MM, Abbeduto L, Krauss MW, Greenberg J, Swe A. Comparison groups in autism family research: Down syndrome, fragile X syndrome, and schizophrenia. Journal of Autism and Developmental Disorders. 2004;34:41–48. doi: 10.1023/b:jadd.0000018073.92982.64. [DOI] [PubMed] [Google Scholar]
- Seltzer MM, Krauss MW, Orsmond GI, Vestal C. Families of adolescents and adults with autism: Uncharted territory. International Review of Research in Mental Retardation. 2001;23:267–294. [Google Scholar]
- Seltzer MM, Krauss MW, Shattuck PT, Orsmond G, Swe A, Lord C. The symptoms of autism spectrum disorders in adolescence and adulthood. Journal of Autism and Developmental Disorders. 2003;33:565–581. doi: 10.1023/b:jadd.0000005995.02453.0b. [DOI] [PubMed] [Google Scholar]
- Seltzer MM, Shattuck P, Abbeduto L, Greenberg JS. Trajectory of development in adolescents and adults with autism. Mental Retardation and Developmental Disabilities Research Reviews. 2004;10:234–247. doi: 10.1002/mrdd.20038. [DOI] [PubMed] [Google Scholar]
- Shattuck PT, Seltzer MM, Greenberg JS, Orsmond GI, Bolt D, Kring S, Lounds J, Lord C. Change in autism symptoms and maladaptive behaviors in adolescents and adults with an autism spectrum disorder. Journal of Autism and Developmental Disorders. 2007;13:129–135. doi: 10.1007/s10803-006-0307-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sparrow SS, Carter AS, Cicchetti DV. Vineland Screener: Overview, reliability, validity, administration, and scoring. New Haven, CT: Yale University Child Study Center; 1993. [Google Scholar]
- Tully LA, Arseneault L, Caspi A, Moffitt TE, Morgan J. Does maternal warmth moderate the effects of birth weight on twins' attention deficit/hyperactivity disorder (ADHD) symptoms and low IQ? Journal of Consulting and Clinical Psychology. 2004;72:218–226. doi: 10.1037/0022-006X.72.2.218. [DOI] [PubMed] [Google Scholar]
- Vaughn CE, Leff JP. The measurement of expressed emotion in the families of psychiatric patients. British Journal of Social and Clinical Psychology. 1976;15:157–165. doi: 10.1111/j.2044-8260.1976.tb00021.x. [DOI] [PubMed] [Google Scholar]
- Wamboldt FS, O'Connor SL, Wamboldt MZ, Gavin LA, Klinnert MD. The Five Minute Speech Sample in children with asthma: Deconstructing the construct of expressed emotion. Journal of Child Psychology and Psychiatry. 2000;41:887–898. [PubMed] [Google Scholar]
- Webster-Stratton C, Reid J, Hammond M. Treating children with early-onset conduct problems: Intervention outcomes for parent, child, and teacher training. Journal of Clinical Child and Adolescent Psychiatry. 2004;33:105–124. doi: 10.1207/S15374424JCCP3301_11. [DOI] [PubMed] [Google Scholar]
- Woo SM, Goldstein MJ, Nuechterlein KH. Relatives' affective style and the expression of subclinical psychopathology in patients with schizophrenia. Family Process. 2004;43:233–247. doi: 10.1111/j.1545-5300.2004.04302008.x. [DOI] [PubMed] [Google Scholar]