

Abstract
During the 2008 Olympic and Paralympic Games, we conducted surveillance of illnesses among travelers at six Beijing clinics. Surveys asked about demographic, pre-travel, and vaccination information, and physician-provided diagnoses. Of 807 respondents, 38% and 57% were classified as foreign visitors (FV) and expatriates, respectively. Less than one-half of FV sought pre-travel advice; sources included health-care providers and friends/family. FV vaccination rate was also low; however, most vaccines given were recommended by the Centers for Disease Control and Prevention. The most common FV diagnoses were respiratory, injury/musculoskeletal, and gastrointestinal illnesses; for expatriates, injury/musculoskeletal, respiratory, and dermatologic were the most common illnesses. Respiratory illnesses in expatriates were significantly less in 2008 than during 2004–2007 (χ2 = 10.2; P = 0.0014), suggesting that control programs may have reduced pollutants/respiratory irritants during the 2008 Games. We found no previous studies of health outcomes among expatriates living in cities with mass travel events. These findings highlight the need to continuously disseminate information to health-care providers advising travelers.
Introduction
The 2008 Summer Olympic and Paralympic Games (2008 Beijing Games) were held in Beijing and other cities in China during August 8–24, 2008, and September 6–17, 2008, respectively. Approximately 500,000 foreign visitors and athletes and up to 3 million domestic visitors and volunteers attended or participated in the events.1 Mass travel events such as these present situations in which travelers can be exposed to a variety of health risks, including large crowds, new and different foods, unusual vector-borne and zoonotic pathogens, unfamiliar road traffic and public transportation, challenging security situations, and unfamiliar social customs. As a result, unexpected illnesses and injuries may occur.2,3
Surveillance for such illness and injury has alerted the travel health community to the need for special precautions before and during mass travel events, such as protection against Neisseria meningitidis for those who attend the Hajj pilgrimage.4 Surveillance during the 1996 Summer Olympic Games in Atlanta found that the most common reasons for medical encounters were injuries (28%) and heat-related complaints (8%).5 During the 1984 Summer Olympic Games in Los Angeles, musculoskeletal and dermatologic injuries (25%), heat-related problems (12%), and minor gastrointestinal (8%) illnesses were the most common diagnoses.6,7 Headaches, foot blisters, and cuts and falls were frequently reported at the 1982 World's Fair in Knoxville, Tennessee.8,9
Although temporary surveillance systems set up specifically for mass events are now common practice, systems already in place can be enhanced during such events to detect illness and injury related to travel. One such system is GeoSentinel (GeoS), a network of 48 travel/tropical medicine clinics worldwide that collects anonymous patient information, including diagnoses, among travelers crossing international borders.10 For the 2008 Beijing Games, the Centers for Disease Control and Prevention (CDC) undertook enhanced surveillance, enlisting clinics associated with GeoS as well as two additional clinics in Beijing. Our objective was to assess illnesses and injuries among travelers and expatriates as well as the association between pre-travel (PT) preparation and health outcomes in travelers.
We focused on the foreign visitors (FV) and expatriates, because (1) FV were more likely to represent travelers whose main purpose of travel was to attend the Games, and (2) expatriates in general may experience enhanced psychological stress11,12 and thus, may have an exacerbation of underlying health problems during such mass travel events at duty locations. To our knowledge, no previous studies of health outcomes have been conducted among expatriates living in cities where mass travel events are taking place. Our findings could provide insights that improve the health of both travelers and expatriates during such events.
Materials and Methods
Surveillance design and location.
Of nine clinics approached to collaborate in the study, six agreed to participate: four associated with the United Family Hospital, including the Beijing GeoS site, an International SOS clinic, and a clinic established in the Holland Heineken House (HHH) specifically to accommodate 2008 Beijing Games-related patients. The three other clinics that declined participation in the study were temporary clinics set up for the 2008 Beijing Games that cited not wanting to inconvenience patients visiting their clinics. The four United Family Hospital clinics and the SOS clinic were permanently operating facilities that had prepared for an increased volume of visits from both established and 2008 Beijing Games-related patients. The HHH clinic was a temporary clinic where medical care was provided by a Dutch volunteer organization for the duration of the Games.
The four United Family Hospital clinics were the community clinic (CC) located in a residential area near the airport, the downtown clinic (DC) located in a hotel near the city center near several foreign embassies, the emergency room (ER) located outside the downtown area but at a hospital close to the main 2008 Beijing Games site, and the family medicine clinic (FM) housed in the same hospital complex as the ER but for nonemergency care (Figure 1). The FM clinic is the primary GeoS site for Beijing. The SOS clinic was located near both the main 2008 Beijing Games site and many embassies. Finally, the HHH was located close to the downtown area and was primarily a venue for Dutch tourists attending or working at the 2008 Beijing Games, although it also welcomed other nationalities.
Figure 1.
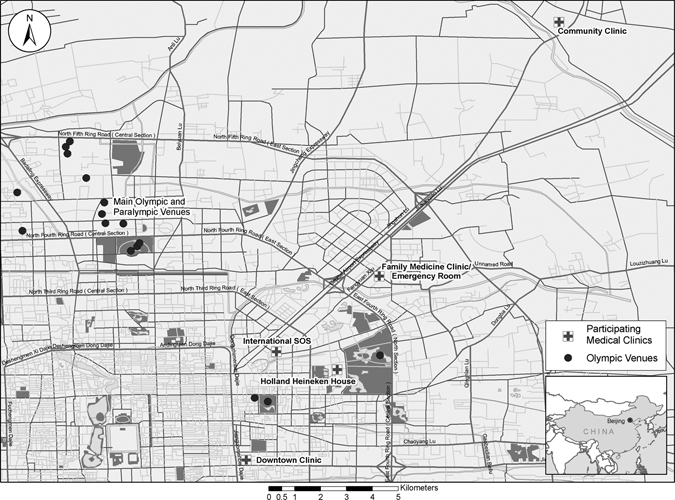
Locations of participating clinics conducting surveillance for the 2008 Summer Olympic and Paralympic Games in Beijing, China.
Time frame.
The Beijing Olympic and Paralympic Games were held during August 8–24, 2008, and September 6–17, 2008, respectively. To fully capture travelers visiting these events, our enhanced surveillance was conducted from August 4 to September 19 at the five permanent clinics. The temporary HHH clinic was open from August 8 through August 24.
Patient consent and enrollment.
All patients visiting the six clinics for treatment were eligible to participate. Although the protocol and surveillance form received a non-research determination by the CDC and was classified as public health surveillance, patients were provided at intake with a surveillance form and consent statement requesting their participation in a survey, in addition to the treatment-information forms. No personal identifying information was included on the intake form, and if the patient was under 18, a parent or guardian completed the patient section form for the patient.
The patients provided the information in the first section of the form, which included demographics, PT health preparation, and history of recent travel. Demographic information included sex, age, country of birth, country of current residence, and country of primary residence before the age of 10. Questions regarding PT health preparation included whether the patient had sought PT health advice before traveling to China, the source of the PT advice (if any), the vaccinations received, and the vaccinations received in the past. Patients were asked their arrival date in China, duration of stay, and history of recent travel in the past month to other countries. After the patient was seen, the clinician completed the second part of the form, entering the symptoms, the diagnosis, and if the illness was related to travel. Diagnoses were coded from a GeoS list of 507 diagnoses representing 24 syndrome groups.13 Vaccines defined as travel-related were hepatitis A, hepatitis B, typhoid, rabies, Japanese encephalitis, yellow fever (YF), and influenza. With the exception of YF, these vaccines are listed on the CDC website as vaccines recommended before travel to China.
Data analysis.
Completed forms were stored at a central location in Beijing until the end of the surveillance period, after which they were sent to CDC and entered into a Microsoft Access database. Data were analyzed by using Microsoft Excel and SAS software, version 9 (SAS Institute, Cary, NC). Descriptive statistics and χ2 tests were used in the analysis. A two-sided significance level of P < 0.05 was chosen.
Patient respondents were classified into one of four groups: (1) FV visiting Beijing for the 2008 Beijing Games, (2) expatriates living in Beijing, (3) Chinese nationals living outside China but visiting friends and/or family in China [also called travelers visiting friends and relatives (VFRs)], and (4) Chinese nationals living in China during the surveillance period. These classifications were made by using the respondent's country of birth and country of current residence. For example, if the respondent listed the United States as the country of current residence and Germany as the country of birth, the patient was classified as an FV. However, a respondent who listed China as the country of current residence and Uruguay as the country of birth would be classified as an expatriate.
Information from the expanded surveillance was compared with data from the Beijing GeoS site from 2004 to 2007 by applying the same aforementioned patient-classification scheme.
Results
Demographics.
During the 54-day study period, 807 surveys were completed from the six sites (Table 1). The number of patients who were offered participation in the surveillance but subsequently refused was not noted. Clinic staff at CC, DC, ER, and FM helped patients translate the clinical and consent forms if they did not read or write in English. However, at the SOS clinic, observers noted that many of the patients did not enter the study because of language barriers.
Table 1.
Patients visiting health clinics in Beijing during the 2008 Summer Olympic and Paralympic Games: demographic information [N (% of column)]
| CC* | DC* | ER | FM | HHH | SOS | Total | P value | |
|---|---|---|---|---|---|---|---|---|
| Sex (8 missing) | ||||||||
| Females | 37 (63) | 7 (29) | 20 (42) | 71 (44) | 20 (40) | 213 (47) | 368 (46) | 0.05 |
| Males | 22 (37) | 17 (71) | 28 (58) | 91 (56) | 30 (60) | 243 (53) | 431 (54) | 0.05 |
| Total | 59 | 24 | 48 | 162 | 50 | 456 | 799 | |
| Age group (38 missing) | ||||||||
| ≤ 15 years | 30 (51) | 2 (8) | 7 (15) | 15 (9) | 1 (2) | 60 (14) | 115 (15) | < 0.0001 |
| 16–54 years | 26 (44) | 20 (83) | 38 (79) | 133 (84) | 41 (85) | 326 (76) | 584 (76) | < 0.0001 |
| ≥ 55 years | 3 (5) | 2 (8) | 3 (6) | 11 (7) | 6 (13) | 45 (10) | 70 (9) | < 0.0001 |
| Total | 59 | 24 | 48 | 159 | 48 | 431 | 769 | |
| Classification (62 missing)† | ||||||||
| National | 5 (8) | 0 (0) | 2 (4) | 4 (3) | 0 (0) | 16 (4) | 27 (4) | < 0.0001 |
| Expatriate | 46 (78) | 14 (58) | 25 (52) | 125 (78) | 4 (8) | 212 (53) | 426 (57) | < 0.0001 |
| Foreign visitors | 8 (14) | 10 (42) | 20 (42) | 29 (18) | 47 (92) | 167 (42) | 281 (38) | < 0.0001 |
| Travelers visiting friends/relatives | 0 (0) | 0 (0) | 1 (2) | 2 (1) | 0 (0) | 6 (1) | 9 (1) | < 0.0001 |
| Total | 59 (7.9) | 24 (3.2) | 48 (6.5) | 160 (21.8) | 51 (6.9) | 401 (54.0) | 743 |
CC = community clinic, United Family Hospital; DC = downtown clinic, United Family Hospital; ER = emergency room, United Family Hospital; FM = family medicine clinic, United Family Hospital; HHH = Holland Heineken House; SOS = International SOS, Beijing, China.
Patients were classified as nationals if their countries of birth and current residence were both China. Patients were classified as expatriates if their country of birth was not China but their current residence was China. Patients were classified as foreign visitors if their country of birth and current residence were both not China. Patients were classified as travelers visiting friends and relatives if their country of birth was China, but current residence was not China. Sixty-two patients were not classifiable, because their country of birth and/or their country of current residence were missing.
Approximately half (54%) of patient respondents were male, and the percentage of males among respondents at the six clinics ranged from 37% to 71%. The distribution of males and females among the clinics was marginally significant (P = 0.05). Most (76%) patient respondents overall were between the ages of 16 and 54 years. HHH and SOS had a larger percentage of patients who were ≥ 55 years of age, 13% (N = 6) and 10% (N = 45), respectively. CC had the largest percentage of patients < 15 years of age (47%). The differences in age groups across clinics were statistically significant (P < 0.001).
Over half of the respondents were expatriates (57%) followed by FV (38%). There were very few Chinese nationals (4%) and VFRs (1%). SOS saw the largest percentage of FV (60%) followed by HHH (17%). This was expected, because both SOS and HHH catered specifically to FV, and HHH was a temporary clinic open only during the 2008 Beijing Games. The types of travelers differed significantly between clinics (P < 0.0001). Sixty-four patients were unclassifiable, because either their country of birth and/or country of current residence were missing; they were, therefore, excluded from analyses dependent on classifications.
Despite clinic variation on the sex, age, and type of travelers, the analysis focused on the attributes of FV and expatriates. The analyses regarding these attributes (e.g., PT preparation and patient diagnoses) were assumed to be independent of the clinic where the patient was seen.
Demographics of FVs and expatriates.
FV came from 46 countries; however, most came from the United States (24%), the Netherlands (19%), Australia (9%), the United Kingdom (9%), and Germany (6%) (Table 2). Table 2 is not associated with Germany only. Countries with fewer than 10 FV were grouped together as Other (33%). In total, there were more male FV (59%) than female FV; this finding was especially true for FV from the United States (61% male) and Germany (65% male). Children ≤ 15 years of age (11%) and older FV (≥ 55 years of age; 23%) were predominantly from the United States. Most expatriates were aged 16–54 (76%), and approximately half were male (51%).
Table 2.
Foreign visitors and expatriates visiting health clinics in Beijing during the 2008 Summer Olympic and Paralympic Games: demographic information of FV and expatriates [N (% of column in each section)]
| All FV | Foreign visitors (FV) | Expatriates | ||||||
|---|---|---|---|---|---|---|---|---|
| Country of current residence* | ||||||||
| U.S. | Netherlands | Australia | U.K. | Germany | Other | Total | ||
| Total respondents | 281 | 67 | 54 | 26 | 24 | 17 | 93 | 426 |
| Sex† | ||||||||
| Female | 116 (41) | 26 (39) | 22 (41) | 13 (50) | 11 (46) | 6 (35) | 38 (41) | 209 (49) |
| Male | 164 (59) | 41 (61) | 31 (57) | 13 (50) | 13 (54) | 11 (65) | 55 (59) | 217 (51) |
| Total | 280 | 67 | 53 | 26 | 24 | 17 | 93 | 426 |
| Age group† | ||||||||
| ≤ 15 years | 18 (7) | 7 (11) | 1 (2) | 1 (4) | 1 (4) | 1 (6) | 7 (8) | 69 (16) |
| 16–54 years | 224 (81) | 44 (67) | 45 (87) | 22 (85) | 21 (88) | 16 (94) | 76 (83) | 320 (76) |
| ≥ 55 years | 34 (12) | 15 (23) | 6 (12) | 3 (12) | 1 (4) | 0 (0) | 9 (10) | 30 (7) |
| Total | 276 | 66 | 52 | 26 | 24 | 17 | 92 | 419 |
| Pre-travel advice | ||||||||
| Respondents seeking ≥ 1 source | 128 (46) | 36 (52) | 28 (52) | 18 (69) | 14 (58) | 4 (24) | 28 (30) | 219 (51) |
| Sources of pre-travel advice‡ | ||||||||
| Health-care provider | 99/128 = 77% | 32/36 = 89% | 18/28 = 64% | 13/18 = 72% | 10/14 = 71% | 2/4 = 50% | 24/28 = 86% | 206/219 = 94% |
| Internet | 15 (12) | 3 (8) | 6 (21) | 0 (0) | 1 (7) | 1 (25) | 4 (14) | 13 (6) |
| Friends/family | 15 (12) | 5 (14) | 6 (21) | 0 (0) | 1 (7) | 0 (0) | 3 (11) | 13 (6) |
| Travel agent | 8 (6) | 1 (3) | 3 (11) | 1 (6) | 1 (7) | 0 (0) | 2 (7) | 1 (0) |
| Company advice | 7 (5) | 0 (0) | 1 (4) | 2 (11) | 2 (14) | 1 (25) | 1 (4) | 12 (5) |
| Respondents receiving travel-related vaccines | ||||||||
| No. of FV with vaccines for trip to China | 83 | 20 | 39 | 10 | 6 | 8 | NA | NA |
| No. of FV with vaccines in the past | 76 | 25 | 20 | 14 | 13 | 4 | NA | NA |
Countries listed individually had 10 or more travelers, whereas if a country had fewer than 10 travelers, it was included in the other category. Listed in decreasing order for numbers of individuals, other countries included France, Canada, Japan, New Zealand, Spain, Switzerland, Italy, Malaysia, Poland, Brazil, Hong Kong, India, Ireland, Republic of Korea, Russian Federation, Taiwan (Province of China), Thailand, Belgium, Chile, Indonesia, Israel, Mexico, Singapore, Angola, Argentina, Colombia, Cuba, Finland, Guyana, Hungary, Iran, Lebanon, Luxembourg, Malta, Nigeria, Norway, Romania, Sweden, Turkey, Uzbekistan, and Venezuela.
Missing data for FV included missing responses for gender (N = 1) and age (N = 5). Missing data for expatriates included missing responses for age (N = 7).
More than one selection could have been chosen, so percentages may be more than 100%.
PT advice-seeking behavior.
Fewer than half (46%) of all FV sought PT advice, although 19 FV reported seeking ≥ 1 source of advice. Sources of PT advice reported by FV included health-care providers (77%), friends and family (12%), the internet (12%), travel agents (6%), and employers (5%). The United States had the largest proportion of FV seeking PT advice from health-care providers (89%); however, this was marginally significant compared with all other countries' proportion of FV seeking PT advice (χ2 = 3.81; P = 0.05).
Approximately half (51%) of expatriates reported having sought PT advice before being placed overseas. Almost all the expatriates who sought advice did so from health-care providers (94%). Statistical comparisons between PT advice-seeking behaviors of FV and expatriates were not made, because the purpose, duration, and general conditions of travel between these two populations were different. Further, the vaccines received by expatriates for their travel to China were, for the most part, not associated with the 2008 Beijing Games; therefore, they were not analyzed here.
PT vaccinations for FV.
FV patients were asked about their PT preparations, including travel-related vaccines that they had received in the past as well as vaccinations for their trip to the 2008 Beijing Games (Table 3). For travel-related vaccines received in the past, Germany had the greatest number of reported vaccines per FV (3.3) followed by the United Kingdom (3.0), the United States (2.3), the Netherlands (2.4), and Australia (1.9). Australia had the highest number of travel-related vaccines per traveler (3.0) administered for the 2008 Beijing Games. Overall, the vaccines most frequently given to FV for their trips to China were hepatitis A (36%), hepatitis B (29%), and typhoid (20%). YF vaccine was administered to 4% (N = 10) of FV. Four FV who reported receiving the YF vaccines seemed to meet the criteria for YF vaccination; three were FV from YF-endemic areas (Brazil and Colombia) and therefore, were required by China to have YF before entry to China. One FV from the United States reported having visited a YF-endemic area (Brazil) immediately before or after the trip to China. Six FV seem to have received YF vaccination without meeting criteria for receiving the vaccine; five FV from the Netherlands and one FV from Australia reported receiving the vaccine but did not report a trip to a YF-endemic country before or after visiting China.
Table 3.
Foreign visitors visiting health clinics in Beijing during the 2008 Beijing Games: travel-related vaccination information [n (% of column total)]
| Country of Current Residence* | |||||||
|---|---|---|---|---|---|---|---|
| All FV | U.S. | Netherlands | Australia | U.K. | Germany | Other | |
| Past trips | |||||||
| Hepatitis A | 76 (31) | 18 (28) | 17 (35) | 7 (23) | 9 (23) | 4 (40) | 21 (40) |
| Hepatitis B | 66 (27) | 21 (32) | 13 (27) | 9 (29) | 6 (15) | 4 (40) | 13 (25) |
| Typhoid | 37 (15) | 8 (12) | 6 (13) | 6 (19) | 10 (26) | 1 (10) | 6 (12) |
| Rabies | 11 (4) | 2 (3) | 2 (4) | 2 (6) | 3 (8) | 0 (0) | 2 (4) |
| Japanese encephalitis | 6 (2) | 3 (5) | 1 (2) | 1 (3) | 0 (0) | 0 (0) | 1 (2) |
| Yellow fever | 27 (11) | 5 (8) | 6 (13) | 2 (6) | 8 (21) | 0 (0) | 6 (12) |
| Influenza | 22 (9) | 8 (12) | 3 (6) | 4 (13) | 3 (8) | 1 (10) | 3 (6) |
| Total | 245 | 65 | 48 | 31 | 39 | 10 | 52 |
| Travel-related vaccine per traveler† | NA | 65/25 = 2.6 | 48/20 = 2.4 | 31/14 = 2.2 | 39/13 = 3.0 | 13/4 = 3.3 | NA |
| 2008 trip to China | |||||||
| Hepatitis A | 80 (36) | 15 (34) | 33 (37) | 9 (30) | 5 (36) | 7 (39) | 11 (39) |
| Hepatitis B | 64 (29) | 12 (27) | 28 (31) | 7 (23) | 3 (21) | 7 (39) | 7 (25) |
| Typhoid | 45 (20) | 7 (16) | 19 (21) | 7 (23) | 5 (36) | 2 (11) | 5 (18) |
| Rabies | 10 (4) | 3 (7) | 4 (4) | 1 (3) | 1 (7) | 1 (6) | 0 (0) |
| Japanese encephalitis | 5 (2) | 3 (7) | 0 (0) | 0 (0) | 0 (0) | 1 (6) | 1 (4) |
| Yellow fever | 10 (4) | 1 (2) | 5 (6) | 1 (3) | 0 (0) | 0 (0) | 3 (11) |
| Influenza | 10 (4) | 3 (7) | 1 (1) | 5 (17) | 0 (0) | 0 (0) | 1 (4) |
| Total | 224 | 44 | 90 | 30 | 14 | 18 | 28 |
| Travel-related vaccine per traveler‡ | NA | 44/20 = 2.2 | 90/39 = 2.3 | 30/10 = 3.0 | 14/6 = 2.3 | 18/8 = 2.3 | NA |
Countries listed individually had 10 or more travelers, whereas if a country had fewer than 10 travelers, it was included in the other category.
Travel-related vaccines are based on CDC recommendations for vaccinations for some or most travelers to China: hepatitis A, hepatitis B, typhoid, rabies, and Japanese encephalitis. Travel-related vaccine per traveler is the number of travel-related vaccines administered in preparation for trip to China divided by the number of travelers receiving ≥ 1 travel-related vaccine in preparation for trip to China.
Travel-related vaccine per traveler is the number of travel-related vaccines administered in the past divided by the number of travelers receiving ≥ 1 travel-related vaccine in the past.
Health outcomes.
Table 4 lists the most common diagnoses according to syndrome groups for FV and expatriates during the 2008 Beijing Games. The most common diagnoses among FV visiting the 2008 Beijing Games were illnesses in the respiratory (23%) and injury and musculoskeletal (14%) groups. The most common diagnoses among expatriates were illnesses in the injuries and musculoskeletal group (18%) followed by illnesses in the respiratory group (17%). Other gastrointestinal illnesses represented 13% and 3% in FV and expatriates, respectively. Interestingly, psychological diagnoses at the 2008 Beijing Games constituted 9% of diagnoses among expatriates but only 3% among FV.
Table 4.
Most frequent diagnoses* according to syndrome group and time of travel to China [2008 Beijing Games or Beijing in August and/or September 2004–2007 at the Beijing GeoS clinic; n (% of column total)]
| Syndrome group | Foreign visitors | Expatriates | ||
|---|---|---|---|---|
| 2008 Beijing Games (N = 322) | 2004–2007 Beijing GeoS clinic (N = 33) | 2008 Beijing Games (N = 496) | 2004–2007 Beijing GeoS clinic (N = 329) | |
| Respiratory† | 73 (23) | 7 (21) | 84 (17) | 86 (26) |
| Injury and musculoskeletal | 46 (14) | 6 (18) | 88 (18) | 48 (15) |
| Other gastrointestinal | 42 (13) | 4 (12) | 16 (3) | 18 (5) |
| Dermatologic | 34 (11) | 0 (0) | 58 (12) | 46 (14) |
| Acute diarrhea | 21 (7) | 3 (9) | 30 (6) | 19 (6) |
| Febrile/systemic illness | 19 (6) | 1 (3) | 31 (6) | 24 (7) |
| Oral and dental | 18 (6) | 1 (3) | 23 (5) | 11 (3) |
| Psychologic | 11 (3) | 4 (12) | 44 (9) | 33 (10) |
| Cardiovascular | 7 (2) | 1 (3) | 20 (4) | 5 (2) |
| Other syndromes‡ | 51 (16) | 6 (18) | 102 (21) | 39 (12) |
| Total diagnoses | 322 | 33 | 496 | 329 |
Patients may have received one or more diagnoses; therefore, the number of diagnoses may exceed the number of total patients.
The number of respiratory illnesses between expatriates who were seen during the 2008 Beijing Games compared with patients seen between 2004–2008 at the Beijing GeoS site was statistically significant (χ2 = 10.2; P < 0.01).
Other syndromes/types of visits included genitourinary and STDs, neurologic, healthy visits, adverse events to medication or vaccine, chronic disease, OB/GYN, miscellaneous tissue parasites, ophthalmologic, and screening diagnoses.
The 2008 Beijing Games data were compared with data collected from FV to China during the same period (months of August and September) from 2004 to 2007 by the Beijing GeoS clinic (Table 4). The most common diagnoses among both FV to the 2008 Beijing Games and to China during 2004–2007 were respiratory syndromes (2008 Beijing Games FV = 23%; China 2004–2007 FV = 21%), injury and musculoskeletal syndromes (14% and 18%, respectively), and other gastrointestinal syndromes (13% and 12%, respectively; Table 4). Psychological syndromes were more common among FV to China during 2004–2007 (12%) than among FV to the 2008 Beijing Games (3%).
For expatriates, respiratory syndromes, injury and musculoskeletal syndromes, and dermatologic syndromes were most common in both periods examined. However, injury and musculoskeletal syndromes ranked higher in the 2008 Beijing Games expatriates than respiratory illnesses (Table 4). In fact, the number of respiratory illnesses diagnosed in expatriates during the 2008 Beijing Games was significantly less than the number of respiratory illnesses diagnosed in expatriates during 2004–2007 (χ2 = 10.2; P = 0.0014). Psychological syndromes were the fourth most common syndromes in both 2008 and 2004–2007. When specific diagnoses in the psychological syndromes group were evaluated for expatriates, anxiety reactions, stress, and depression were the most common in both time periods.
To further evaluate the specific diagnoses among FV and expatriates during the 2008 Beijing Games, we analyzed the top three ranked specific diagnoses in five syndrome groups: respiratory, injury and musculoskeletal, other gastrointestinal, dermatologic, and acute diarrhea (Table 5). In both groups, upper respiratory tract infections were most common in the respiratory syndrome group, sprains/strains in the injury and musculoskeletal, and gastroenteritis in the other gastrointestinal group.
Table 5.
Top three ranked diagnoses in each syndrome group for foreign visitors and expatriates seen during the 2008 Beijing Games
| FV seen during 2008 Olympics (N = 281 patients) | Expatriates (N = 426) | |
|---|---|---|
| Respiratory (no. of diagnoses) | ||
| 1 | upper respiratory tract infection (28) | upper respiratory tract infection (29) |
| 2 | acute bronchitis (12) | acute bronchitis (12) |
| 3 | acute sinusitis (5); asthma (5); otitis externa (5); acute otitis media (5) | allergic rhinitis (9) |
| Injury and musculoskeletal (no. of diagnoses) | ||
| 1 | sprain/strain (18) | sprain/strain (33) |
| 2 | abrasion (6); laceration (6) | back pain (9) |
| 3 | fracture (2); contusion (2); nonseptic arthritis (2); sciatica (2); miscellaneous trauma or injury (2) | abrasion (7) |
| Other gastrointestinal (no. of diagnoses) | ||
| 1 | gastroenteritis (22); | gastroenteritis (10) |
| 2 | abdominal pain (3); constipation (3); vomiting/nausea (3) | hemorrhoids (3) |
| 3 | appendicitis (2); hemorrhoids (2) | dyspepsia (2); unspecified gastritis (2); abdominal pain (2); unspecified other gastrointestinal (2) |
| Dermatological (no. of diagnoses) | ||
| 1 | superficial skin infection or infected wound (5) | eczema (6) |
| 2 | eczema (3); rash of unknown etiology (3); herpes zoster (3); allergic, nondrug-related rash (3) | cyst (5); insect bite/sting (5) |
| 3 | insect bite (2); erysipelas (2); lice (2); paronychia (2) | skin abscess (e.g., furuncle, carbuncle, folliculitis) (4); superficial skin infection or infected wound (4); nongenital warts (4) |
| Acute diarrhea (no. of diagnoses) | ||
| 1 | acute unspecified diarrhea (12); | acute bacterial diarrhea (10) |
| 2 | acute bacterial diarrhea (4) | acute unspecified diarrhea (4) |
| 3 | acute viral diarrhea (2); Giardia (2) | Giardia (3) |
Discussion
Consistent with previous studies regarding travel to China, our surveillance found that respiratory illnesses, specifically upper respiratory-tract infections and acute bronchitis, were the most common diagnoses in foreign travelers.12,14,15 This finding may be because of poor air quality associated with air pollution in Beijing, which was of concern in planning for the 2008 Beijing Games. Despite clean-air programs implemented to improve the levels of particulates in the air,16–18 respiratory illnesses in our study were the most common diagnoses in FV and the second most common in expatriates. However, the proportion of expatriates being diagnosed with respiratory illnesses during the 2008 Beijing Games was significantly less than expatriates in the same months during 2004–2007. One possible explanation for this decrease may be that the control programs were effective in reducing pollutants and respiratory irritants during the 2008 Beijing Games. Levels of pollution may have still been high enough to exacerbate conditions in naïve populations, such as FV, but may have alleviated some symptoms for long-term Beijing expatriate residents. Further studies into the specific control measures taken, the particulate reductions, the other environmental changes in Beijing during the 2008 Games, and their potential effects on health would be needed to confirm this hypothesis. In addition, expatriates with minor respiratory illnesses during the 2008 Beijing Games could have decided to avoid seeking health care at that time because of concerns that wait times might be long because of the influx of tourists.
The surveillance described here is unique, because it provides information on the expatriates living in Beijing during the 2008 Beijing Games. We believe this is the first Olympic or mass travel study to include expatriates in its surveillance system. In contrast with FV, the most common diagnoses for expatriates were sprains and strains, upper respiratory infections, and a number of dermatologic diagnoses. Because our surveillance system was limited in the type and depth of data collected, we could not discern if these injuries, respiratory infections, or dermatologic illnesses were related to the Olympic events. The expatriates may have spent more time outside as spectators of these events and therefore, may have been exposed to increased physical activity outdoors. Expatriates may also have retreated to locations outside the city of Beijing for part or all of the Olympic period and therefore, could have been exposed to different surroundings that may have increased the likelihood of injuries, insect bites, skin irritations, etc. However, many expatriate families would have been in Beijing by the end of August, because children were starting school.
Previous research has found that expatriates may have increased levels of stress, anxiety, and depression while living away from their home countries.11,12,19 However, in our study, the 2008 Olympics did not seem to have had an impact on psychological syndromes among expatriates. The rate of psychological syndromes did not differ significantly among expatriates during the 2008 Beijing Games (9%) and expatriates from 2004–2007 (10%). Future mass events would provide an opportunity to corroborate whether or not mass travel events, such as Olympic or Paralympic Games, affect the levels of stress, anxiety, and depression among expatriates.
Only half of all foreign visitors in our study sought PT health advice before their trip. Previous studies conducted among transit passengers in airports have found similar results.20–23 Although our study did not address why FV did not seek PT health advice, several possibilities may have influenced seeking this advice, including the duration of travel, travel confined to only cities, group travel, previous travel to China, or the FV's level of education or awareness of the importance of travel health.
The most common source of PT advice for FV from all countries was health-care providers. FV from the United States overwhelmingly consulted health-care providers; these findings highlight the importance of continued support and dissemination of information to U.S. health-care providers advising traveling patients. Our surveillance questions did not distinguish between health-care providers with travel-medicine training and those without, and therefore, educational messages should be targeted to all physicians and should focus on travel risks and health preparations necessary before international travel. The CDC's Yellow Book: Health Information for International Travel24 and the CDC Travelers' Health website (www.cdc.gov/travel) represent the two principal mechanisms by which the CDC disseminates its recommendations for U.S. travelers. Further research is necessary to determine the extent to which U.S. health-care providers consult these sources for travel health recommendations.
The vaccinations CDC recommends for most travelers to China include hepatitis A, hepatitis B, typhoid, and influenza, when available. For travelers with prolonged outdoor exposure or travel to rural areas in China, CDC recommends rabies and Japanese encephalitis vaccines. The vaccines reported by U.S. travelers for this trip to China corresponded with these recommendations. The largest number of vaccines reported was for prevention of hepatitis A and hepatitis B.
The YF vaccine is a live virus vaccine that has been associated with rare but potentially severe adverse complications. CDC does not recommend it for travelers to China, because China is not a YF-endemic area. Our study was unable to determine why six FV (one from Australia and five from the Netherlands) reported receiving YF vaccine. Recent adverse events caused by the YF vaccine underscore the importance of administering the vaccine only to travelers visiting areas at risk.
Our study had several limitations. First, the study sites were convenience samples consisting of health facilities that were willing to participate, a subset of all possible health facilities for travelers to seek care while in Beijing. The patients may not have been representative of all travelers to China during the 2008 Beijing Games. There may have been differences in the populations at the clinics in 2008 versus the populations in the GeoS clinics in 2004–2007. Second, within each site, there may have been reporting biases. For example, the SOS clinic observers noted that one-third of the eligible patients could not participate in the study, because they spoke only Japanese. Thus, language barriers may have limited the number of respondents in each site. In addition, biases may have resulted from variations between the six clinics in staff, patient populations, diagnoses, and inclusion of eligible patients. Third, five of our clinics were permanent clinics in Beijing; therefore, our sample was biased toward expatriates. Fourth, very few VFRs participated in our study, even though large number of VFRs could have attended the 2008 Beijing Games. In addition, the vaccination data consisted of self-reports whose accuracy cannot be independently confirmed. This issue requires further research, because some studies have suggested that as many as 25% of patients who report receiving immunizations may actually be unprotected.25
In summary, the 2008 Beijing Games presented a complex public-health environment for travelers, because it was a mass travel event in a developing country. Our findings highlight the need for continued support and dissemination of information to health-care providers advising traveling patients. Based on our study, PT preparations for international events in China should focus on prevention of respiratory illness, injuries, and gastrointestinal illnesses, including gastroenteritis. To our knowledge, there have been no known studies of health outcomes among expatriates living in cities where mass travel events are taking place. Our findings provide insights on preparing and improving the health of expatriate populations during such events. Future considerations for mass travel events should include potential needs of populations already living in the event's location, such as expatriates, who may have unique medical needs.
Acknowledgments
The authors thank the staff of Service Medical Foundation, Belgium, for their assistance with this surveillance. We also thank Katherine Johnson, Theresa Sommers, Amanda Cantor, Clive Brown, and Ava Navin for reviewing the manuscript. Finally, we thank Kevin Liske for creating the Beijing map.
Footnotes
Authors' addresses: Emily S. Jentes, Division of Global Migration and Quarantine, Centers for Disease Control and Prevention, Atlanta, GA, E-mail: ejentes@cdc.gov. Xiaohong M. Davis, Victor Balaban, Cinzia Marano, Katherine Mues, Phyllis Kozarsky, and Nina Marano, Division of Global Migration and Quarantine, Centers for Disease Control and Prevention, Atlanta, GA. Susan MacDonald, Department of Primary Care, Beijing United Family Hospital and Clinics, Beijing, China, E-mail: susanmacdonald@telus. P. Johann Snyman and Hugh Nelson, Beijing International SOS Clinic, Beijing, P.R. China. Doug Quarry and Irene Lai, International SOS, Sydney, New South Wales, Australia. Erik W. N. van Vliet, Heineken International, Amsterdam, The Netherlands.
References
- 1.Anonymous Visitors to Beijing. WHO Guide Shows How to Avoid Foodborne Illnesses: United Nations in China. 2008. http://www.un.org.cn/cms/p/news/27/721/content.html Available at. Accessed September 2, 2008.
- 2.Rashid H, Haworth E, Shafi S, Memish ZA, Booy R. Pandemic influenza: mass gatherings and mass infection. Lancet Infect Dis. 2008;8:526–527. doi: 10.1016/S1473-3099(08)70186-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Anonymous . Communicable Disease Alert and Response for Mass Gatherings. Geneva: World Health Organization; 2008. pp. 1–26. [Google Scholar]
- 4.Wilder-Smith A. Meningococcal disease in international travel: vaccine strategies. J Travel Med. 2005;12(Suppl 1):S22–S29. doi: 10.2310/7060.2005.12054. [DOI] [PubMed] [Google Scholar]
- 5.Barnett BJ, Harper L, Yang WM, Kozarsky PE. Experience of corporate medical assistance clinics during the Centennial Olympic Games, Atlanta, 1996. J Travel Med. 2000;7:25–26. doi: 10.2310/7060.2000.00006. [DOI] [PubMed] [Google Scholar]
- 6.Weiss BP, Mascola L, Fannin SL. Public health at the 1984 Summer Olympics: the Los Angeles County experience. Am J Public Health. 1988;78:686–688. doi: 10.2105/ajph.78.6.686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baker WM, Simone BM, Niemann JT, Daly A. Special event medical care: the 1984 Los Angeles Summer Olympics experience. Ann Emerg Med. 1986;15:185–190. doi: 10.1016/s0196-0644(86)80019-1. [DOI] [PubMed] [Google Scholar]
- 8.Booth A. Disease surveillance at the World's Fair in Knoxville, Tennessee. J Tenn Med Assoc. 1983;76:242–243. [PubMed] [Google Scholar]
- 9.Gustafson TL, Booth AL, Fricker RS, Cureton E, Fowinkle EW, Hutcheson RH, Jr, Schaffner W. Disease surveillance and emergency services at the 1982 World's Fair. Am J Public Health. 1987;77:861–863. doi: 10.2105/ajph.77.7.861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Freedman DO, Kozarsky PE, Weld LH, Cetron MS. GeoSentinel: the global emerging infections sentinel network of the International Society of Travel Medicine. J Travel Med. 1999;6:94–98. doi: 10.1111/j.1708-8305.1999.tb00839.x. [DOI] [PubMed] [Google Scholar]
- 11.Eytan A, Loutan L. Travel and psychiatric problems. Rev Med Suisse. 2006;2:1251–1255. [PubMed] [Google Scholar]
- 12.Davis XM, MacDonald S, Borwein S, Freedman DO, Kozarsky PE, von Sonnenburg F, Keystone JS, Lim PL, Marano N. Health risks in travelers to China: the GeoSentinel experience and implications for the 2008 Beijing Olympics. Am J Trop Med Hyg. 2008;79:4–8. [PubMed] [Google Scholar]
- 13.Freedman D, Weld L, Kozarsky P, Fisk T, Robins R, von Sonnenburg F, Keystone J, Pandey P, Cetron M. Spectrum of disease and relation to place of exposure among ill returned travelers. N Engl J Med. 2006;354:119–130. doi: 10.1056/NEJMoa051331. [DOI] [PubMed] [Google Scholar]
- 14.Leder K, Sundararajan V, Weld L, Pandey P, Brown G, Torresi J. Respiratory tract infections in travelers: a review of the GeoSentinel surveillance network. Clin Infect Dis. 2003;36:399–406. doi: 10.1086/346155. [DOI] [PubMed] [Google Scholar]
- 15.Wilson ME, Weld LH, Boggild A, Keystone JS, Kain KC, von Sonnenburg F, Schwartz E. Fever in returned travelers: results from the GeoSentinel Surveillance Network. Clin Infect Dis. 2007;44:1560–1568. doi: 10.1086/518173. [DOI] [PubMed] [Google Scholar]
- 16.Li J, Lu Y, Huang K, Wang C, Lu J, Zhang C, Zhong N. Chinese response to allergy and asthma in Olympic athletes. Allergy. 2008;63:962–968. doi: 10.1111/j.1398-9995.2008.01816.x. [DOI] [PubMed] [Google Scholar]
- 17.Streets DG, Fu JS, Jang CJ, Hao J, He K, Tang X, Zhang Y, Wang Z, Li Z, Zhang Q, Wang L, Wang B, Yu C. Air quality during the 2008 Beijing Olympic Games. Atmos Environ. 2007;41:480–492. [Google Scholar]
- 18.Wang L, Hao J, He K, Wang S, Li J, Zhang Q, Streets DG, Fu JS, Jang CJ, Takekawa H, Chatani S. A modeling study of coarse particulate matter pollution in Beijing: regional source contributions and control implications for the 2008 Summer Olympics. J Air Waste Manag Assoc. 2008;58:1057–1069. doi: 10.3155/1047-3289.58.8.1057. [DOI] [PubMed] [Google Scholar]
- 19.Balaban V. In: CDC Health Information for International Travel 2010. Brunette GW, editor. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service; 2009. pp. 239–241. (Mental health and travel). [Google Scholar]
- 20.Hamer DH, Connor BA. Travel health knowledge, attitudes and practices among United States travelers. J Travel Med. 2004;11:23–26. doi: 10.2310/7060.2004.13577. [DOI] [PubMed] [Google Scholar]
- 21.Toovey S, Jamieson A, Holloway M. Travelers' knowledge, attitudes and practices on the prevention of infectious diseases: results from a study at Johannesburg International Airport. J Travel Med. 2004;11:16–22. doi: 10.2310/7060.2004.13587. [DOI] [PubMed] [Google Scholar]
- 22.Van Herck K, Van Damme P, Castelli F, Zuckerman J, Nothdurft H, Dahlgren AL, Gisler S, Steffen R, Gargalianos P, Lopez-Velez R, Overbosch D, Caumes E, Walker E. Knowledge, attitudes and practices in travel-related infectious diseases: the European airport survey. J Travel Med. 2004;11:3–8. doi: 10.2310/7060.2004.13609. [DOI] [PubMed] [Google Scholar]
- 23.Wilder-Smith A, Khairullah NS, Song JH, Chen CY, Torresi J. Travel health knowledge, attitudes and practices among Australasian travelers. J Travel Med. 2004;11:9–15. doi: 10.2310/7060.2004.13600. [DOI] [PubMed] [Google Scholar]
- 24.CDC . CDC Health Information for International Travel 2010. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service; 2009. [Google Scholar]
- 25.Shenson D, Dimartino D, Bolen J, Campbell M, Lu PJ, Singleton JA. Validation of self-reported pneumococcal vaccination in behavioral risk factor surveillance surveys: experience from the sickness prevention achieved through regional collaboration (SPARC) program. Vaccine. 2005;23:1015–1020. doi: 10.1016/j.vaccine.2004.07.039. [DOI] [PubMed] [Google Scholar]