

Abstract
Boiling is the most common means of treating water in the home and the benchmark against which alternative point-of-use water treatment options must be compared. In a 5-week study in rural Guatemala among 45 households who claimed they always or almost always boiled their drinking water, boiling was associated with a 86.2% reduction in geometric mean thermotolerant coliforms (TTC) (N = 206, P < 0.0001). Despite consistent levels of fecal contamination in source water, 71.2% of stored water samples from self-reported boilers met the World Health Organization guidelines for safe drinking water (0 TTC/100 mL), and 10.7% fell within the commonly accepted low-risk category of (1–10 TTC/100 mL). As actually practiced in the study community, boiling significantly improved the microbiological quality of drinking water, though boiled and stored drinking water is not always free of fecal contaminations.
Introduction
An estimated 1.1 billion people, or 21.6% of the population of 67 middle- and low-income countries report that they usually boil their water at home before drinking it, more than four times as many as report chlorinating or filtering their drinking water.1 No alternative method of household water treatment (HWT) is more accessible to most populations, and none is more effective under the variety of water conditions (turbidity, temperature, chlorine demand, etc.) that impact the performance of alternative HWT options.2,3 However, in the absence of safe storage, water that is boiled is immediately vulnerable to recontamination, especially in hygiene-challenged environments.4
Previous field studies in Vietnam5 and India6 showed boiling to be effective in improving microbiological water quality. In a previous study in Peru, however, water that was reportedly boiled at home before consumption was of no better quality than untreated stored water.7 Other studies of routine water treatment practices have shown mixed results about the microbiological effectiveness of boiling and chlorination.8,9
We undertook this study to assess the microbiological effectiveness of boiling unsafe water and to characterize certain practices associated with boiling in a remote village in northern Guatemala, a country where 43% of the population reported the boiling of their drinking water.1
Materials and Methods
Study setting.
The study was conducted over a period of 5 weeks (June 2008 to July 2008), coinciding with the wet season, in the town of San Mateo Ixtatán, Municipality of San Mateo Ixtatán, Huehuetenango Department. The town, with a population of about 10,000 people, is located in the northern highlands of Guatemala (elevation 2,540 m) and its main subsistence is agriculture (80%) with a minority relying in industry and commercial activities (20%). An estimated 91% of the population in the municipality is classified as poor and 41% as extreme poor. Literacy is just 30% and 90% of the population belongs to the Mayan ethnicity, Chuj.10
In this community, water from the surrounding highlands is provided to yard or indoor taps through a gravity-fed distribution system. Nine groundwater collection tanks are situated at varying distances from the town and supply water by polyvinylchloride (PVC) or metal pipes to closer distribution tanks, which then feed directly into household tap connections. There is no centralized water treatment. The municipal sewage system includes pipes that in some cases run parallel and proximate to the water distribution system, and leaks from this or privately owned latrines are assumed by water authorities to be common.
Sample size calculation and enrollment of participating households.
Following a pre-investigation assessment of the differences in bacterial loads of samples from source- and stored-water in adjacent communities, we estimated a sample size (with 80% power and 0.05 alpha) of 45 households, which we adjusted to 49 to account for loss to follow-up. A rough map of the study community was sketched with the help of the local translator and the community was divided into quadrants of roughly equal size. Approximately the same number of households in each of these quadrants was selected for the eligibility survey. Selection was based on accessibility and was not random. Households were eligible for enrollment in the study if, in response to this initial eligibility survey, the female head of the household reported that in their household they either “always” or “almost always” boiled their water before drinking it. After receiving full details of the study, all 49 households approached during the eligibility survey were eligible and consented to participate in the study.
Household surveys.
During the initial eligibility visit, the female head of the participating household provided information to a field investigator who completed a pre-piloted structured survey. The questionnaire was administered in Spanish if the participant was Spanish-speaking or verbally translated to the local language, Chuj, by a local, female translator, if this was the main language spoken. Information included household demographics, water collection, treatment and storage practices, hygiene practices, and sanitation facilities. Once during the study period, each participating household provided information in response to a second survey, focusing on the manner in which boiling was practiced in the home (definition of boiling, frequency, type of fuel used, amount of water boiled daily, time, method of procuring the fuel, etc.).
Boiling descriptions.
A convenience sample representing 20% of the participating households was randomly selected to describe how they normally treat their water. Step-by-step descriptions were provided by the person who reportedly conducted the boiling. This approach was adopted in lieu of direct observation or boiling demonstration because in most cases the water was on the fire for most of the day. Data on the amount of water boiled per batch, fuel and stove used, duration of boiling and the use of a lid, and the activities of the performer during boiling were to be recorded, as well as the use of the stove prior and post boiling.
Water sampling and analysis.
Commencing at the eligibility visit to each participating household and continuing once each week for the ensuing 4 weeks, two 125 mL water samples (one from the raw source water that the householder collected for use in the home and one from the water that the householder identified as stored, boiled drinking water) were collected and assayed for thermotolerant coliforms (TTC), a World Health Organization (WHO)-prescribed indicator of fecal contamination.3 All visits to participating households were unannounced. The water samples were preserved on ice and analyzed within 4 hours using the membrane filtration method in accordance with Standard Methods for the Examination of Water and Wastewater.11 Sample water was passed through a 0.45-µm membrane filter (Millipore, Bedford, MA) and incubated on membrane lauryl sulphate media (Oxoid Limited, Basingstoke, Hampshire, UK) at 44 ± 0.5°C for 18 hours in an Oxfam Delagua portable incubator (Robens Institute, University of Surrey, Gilford, Surrey, UK). The number of yellow colonies were counted and recorded as individual TTCs and reported as the number of colony forming units (CFUs) per 100 mL of analyzed sample water. Plates that yielded CFUs that were too numerous to count (TNTC) were reported as 300 TTC/100 mL for purposes of our analysis.
Data analysis.
Because bacterial counts tend to follow a skewed distribution, statistical analyses were performed after TTC counts were transformed to their log 10 values to satisfy the assumption of normality. For this purpose only, TTC count values of 0 were assigned a value of 1 so as not to lose the data in the log transformation. A paired t test was used to analyze TTC counts of paired (source and drinking) water samples. A linear regression model adjusting for repeated samples within the same household was used to explore the possible associations between bacterial counts in boiled water samples and household characteristics.
Ethics and consent.
The study was reviewed and approved by the Ethics Committee of the London School of Hygiene and Tropical Medicine. Before the commencement of the study, potential participants received complete details regarding the risks, expectations, and obligations of householders participating in the study, and had an opportunity to ask and receive answers to any questions. Informed, written consent was obtained from the household head (usually, the senior male) at the beginning of the study.
Results
Demographic and household characteristics.
After losing four households to follow-up (one because of refusing to continue with no material compensation, two because they had switched to using a filter provided by another study, and another because of non-presence at the time of the visits), data was collected from 45 households with 289 persons (mean of 6.4 occupants per household). Data from household surveys are summarized in Table 1. Most households (91%) were made of cement and disposed on average of a total of 4.2 rooms (2.2 bedrooms). All households had sanitation facilities, mostly connected toilets (80%) or pit latrines (20%). All but one household had access to the community water system (44.4% had access to an indoor tap and 53.3% to an outdoor tap). Drinking water was mainly stored in an aluminum pot (77.8%) and a lid was used in most cases to cover the container (97.8%). Just over two-thirds of the population drew drinking water from its container by dipping a cup or glass, while the remaining third poured water to a drinking container. Most households reported hand washing after defecation (95.6%) and before food preparation (100%). However, hand washing after child stool disposal was less common (8.9%). A great majority of households reported using soap for hand washing (91.1%) and in most of these households (97.6%) soap was available at the time of the visit.
Table 1.
Demographic characteristics
| N | % | |
|---|---|---|
| Number of households | 45 | |
| Total population | 289 | |
| Household size (mean, 95% CI*) | 6.4 (5.5–7.30) | |
| Total no. of rooms (mean, 95% CI) | 4.2 (3.5–4.9) | |
| Total no. of bedrooms (mean, 95% CI) | 2.2. (1.7–2.8) | |
| House construction | ||
| Mud | 1 | 2.2 |
| Cement | 41 | 91.1 |
| Wood | 3 | 6.7 |
| Sanitation | ||
| Pit latrine | 9 | 20.0 |
| Connected toilet | 36 | 80.0 |
| Water source | ||
| Indoor tap | 20 | 44.4 |
| Outdoor tap | 24 | 53.3 |
| River | 1 | 2.2 |
| Drinking water vessel | ||
| Bucket | 4 | 8.9 |
| Aluminium pot | 35 | 77.8 |
| Jerry can | 1 | 2.2 |
| Barrel | 1 | 2.2 |
| Other | 4 | 8.9 |
| Drinking water vessel covered | 44 | 97.8 |
| Mode of accessing drinking water | ||
| Pour from vessel into cup | 16 | 35.6 |
| Dip cup in vessel | 29 | 64.4 |
| Received hygiene promotion in last 6 months | 10 | 22.2 |
| Handwashing | ||
| After defecation | 43 | 95.6 |
| Before preparing food | 45 | 100 |
| After child stool disposal | 4 | 8.9 |
| Hand washing with soap | 41 | 91.1 |
CI = confidence interval.
Reported boiling practices.
The characteristics of boiling are presented in Table 2. All households reported boiling their drinking water, a condition for eligibility, and none reported practicing any other means of treating water, though two households switched to filtering during the third week of the study. From informal interviews with local health care workers and teachers, and during the administration of the questionnaire, it was observed that there was a general community consensus that it is not acceptable to drink untreated water directly from the tap and that it should be boiled before consumption. When asked who recommended or what factors guided the practice of boiling, 35.6% of household responded that their mother or a relative had influenced them, whereas 28.9% reported that the government or a radio advert had guided such behavior and 17.8% reported that a friend or neighbor had influenced them. It was noted that many participants recalled radio announcements encouraging the boiling of water to control cholera released during the late 1980s and early 1990s.
Table 2.
Boiling practice data
| N | % | |
|---|---|---|
| Recommendation/Motivation of boiling | ||
| Government/ad/radio | 13 | 28.9 |
| Mother/relative | 16 | 35.6 |
| Doctor/medical person | 4 | 8.9 |
| Friend/neighbor | 8 | 17.8 |
| Other | 4 | 8.9 |
| Definition of boiling | ||
| Until surface boil starts | 24 | 53.3 |
| Until bubbles from the base start to rise | 5 | 11.1 |
| Until vapors start rising on surface | 5 | 11.1 |
| Little warming | 11 | 24.4 |
| Fuel data | ||
| Fuel type | ||
| Firewood | 44 | 97.8 |
| Gas | 1 | 2.22 |
| Fuel source | ||
| Collect in forest | 13 | 28.9 |
| Purchase in store | 6 | 13.3 |
| Delivered at home | 25 | 55.6 |
| Other | 1 | 2.2 |
| Person collecting fuel | ||
| Female head of household | 1 | 5.3 |
| My spouse/ father/father-in-law | 9 | 47.4 |
| Spouse and son | 1 | 5.3 |
| Female head and other | 3 | 15.8 |
| Most/all family | 5 | 26.3 |
| Other purposes of the fuel used for boiling | ||
| Cooking and heating | 45 | 100 |
| Boiling practice | ||
| Person in charge of boiling | ||
| Female head of household | 32 | 71.1 |
| Female head or other | 6 | 4.4 |
| My mother/sister | 5 | 11.1 |
| My spouse | 2 | 4.4 |
| Boiling episodes per day | ||
| One | 15 | 33.3 |
| Two | 19 | 42.2 |
| Three to five | 11 | 24.4 |
| Vessel filling | ||
| Half full | 1 | 2.2 |
| Completely full | 44 | 97.8 |
| Use a lid while boiling | 42 | 93.3 |
| Mean daily water boiled/day (95% CI)* | 14.9 | (12.0 L–17.7l) |
| Boiling time | ||
| Pot left all day on stove | 23 | 52.3 |
| Pot left for extended period of time on stove (up to 8 hrs) | 13 | 29.5 |
| Taken off after boiling is reached | 8 | 18.2 |
| Post-boiling | ||
| Transfer water once boiled | 14 | 31.1 |
| Mode of transfer | ||
| Dip a vessel/ladle | 2 | 14.3 |
| Dip drinking vessel | 4 | 28.6 |
| Tilt the container | 8 | 57.1 |
| Mix boiled water with non-boiled | 15 | 33.3 |
CI = confidence interval.
Forty-four of the 45 households (98%) reported wood as their primary source of fuel for boiling water; the remaining household reported using gas. Excluding the gas user, 30% collected the wood from the forest, 11.4% purchased it in a store, and 57% had it delivered at home. Non-delivered wood was normally collected by a male family member. All households reported using the same fuel source for cooking and space heating.
Boiling was normally undertaken by the female head of the household (66.7%) or her mother (6.7%) or sister (4.4%). The mean number of times water was boiled daily was 2.0 (range 1–5) and the mean vessel size was 7.8 L (range 2–12 L), representing a mean of 14.9 L per day (range 3.75–50 L). Just over half of the households defined boiling as a surface boil, whereas 22.2% defined it as either bubbles from the base of the pot or when vapor starts rising. The remaining 24.4% defined boiling as a “little warming.” However, when asked about the time the water was left on the heat source, over 50% of the households reported that the pot would be left all day on the commonly used stove, the plancha. Twenty-four percent of households would leave it for an extended period over the heat source (mean 3.6 hrs, range 0.1–8 hrs), whereas only 17.8% reported removing the water after the boiling point had been reached. For this later group, the mean total boiling time was 21.6 min (range 5–60 min). All households reported performing some other activity while boiling, 95.6% reported housework, whereas the remaining 4.4% reported combining housework with an economic activity inside the home. It was common to observe that when participants were asked “how long does the water take to reach the boil?” and “how long do you heat the water after the boiling is reach?” they seemed confused and did not know how to answer these questions, suggesting that participants do not actively monitor the boiling of water.
Only one-third of households reported transferring the water to a different container once the water was boiled. In over half of the cases the water was transferred by tilting the container, whereas in 28.6% of households the storage vessel was dipped in the boiling pot or a small vessel/ladle was used to transfer the boiled water (14.3%). One-third of households reported mixing boiled water with non-boiled water, a potential source of contamination after treatment.
Detailed boiling descriptions.
Detailed descriptions of boiling practices were obtained from 10 (22%) of the participating households. Each boiled their water indoors over a plancha, a woodstove with a metal plate with three or six circular plates that can be removed to allow the pot to be in direct contact with the heat source. Householders reported that they would not actively ensure that the water had reached a boil, but instead reported that the pot would be placed over the wood stove and left over the heat for most of the day, occasionally being moved around the woodstove, and thus being subjected to different intensities of heat. In all cases, water for boiling was collected directly from the tap, although one household reported that from time to time a bucket with stored water would be used. Participants reported carrying out other tasks during the boiling process. This either involved preparing coffee or food, cleaning or doing laundry, or selling items in the household. In all cases the same fuel source was used for cooking or heating more water, either extra drinking water or water for cooking or bathing.
Water quality.
Water was sampled from five of the nine collection tanks, and one distribution tank, for which access was granted. Three of these tanks tested negative for TTC, whereas the remaining three had 3, 204, and 364 TTC/100 mL, respectively (overall geometric mean 7.8 TTC/100 mL), suggesting some source contamination. Table 3 shows the TTC count of samples from source and treated water by visit. Source water was consistently contaminated, but at a low to moderate level with an overall geometric mean of 15.8 TTC/100 mL (95% CI: 11.88–21.04). Stored boiled water showed considerable improvement in microbiological quality, with a geometric mean of 2.1 TTC/100 m (95% CI: 1.73–2.65). Analysis of paired water samples for each household showed a 0.88 Log10 reduction (95% CI: 0.74–1.02) in TTC after treatment; this is equivalent to an 86.2% reduction in TTC.
Table 3.
Geometric mean TTC counts in samples of source and boiled drinking water taken at the study households at each of five visits and overall (TTC/100 mL)*
| Source water | Drinking water | Log reduction of TTC | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean | 95% CI | N | Mean | 95% CI | N pairs | Mean difference | 95% CI | P value | |
| Round 1 | 48 | 17.1 | 9.23–31.74 | 44 | 1.8 | 1.17–2.67 | 44 | 1.02 | 0.74–1.31 | < 0.001 |
| Round 2 | 48 | 13.6 | 7.04–26.24 | 45 | 2 | 1.21–3.22 | 45 | 0.81 | 0.51–1.12 | < 0.001 |
| Round 3 | 44 | 12.2 | 6.40–23.21 | 41 | 2.1 | 1.32–3.34 | 41 | 0.71 | 0.38–1.04 | < 0.001 |
| Round 4 | 44 | 22.8 | 11.89–43. 77 | 41 | 2.3 | 1.40–3.92 | 41 | 1.01 | 0.66–1.36 | < 0.001 |
| Round 5 | 40 | 15.3 | 7.53–31.14 | 35 | 2.8 | 1.56–5.03 | 35 | 0.84 | 0.49–1.18 | < 0.001 |
| All | 224 | 15.8 | 11.88–21.04 | 206 | 2.1 | 1.73–2.65 | 206 | 0.88 | 0.74–1.02 | < 0.001 |
TTC = thermotolerant coliforms; CI = confidence interval.
Figure 1 presents the percentage of water samples by commonly used level of risk category for fecal contamination: 0 TTC/100 mL (in compliance with WHO guidelines), 1–10 TTC/100 mL (low risk), 11–100 TTC/100 mL (medium risk), 101–1,000 TTC/100 mL (high risk), and > 1,001 (very high risk).12 Overall, 71.4% of boiled water samples were free of TTC and 10.7% fell within the low-risk category of 1 to 10 TTC/100 mL. Only a small proportion (4.9%) was classified as high risk and none had contamination levels above 1,000 TTC/100 mL. By contrast, only 23.7% of source water was free of TTC and 21.4% classified as high risk, four times that of boiled water. Only a small proportion (2.7%) was classified as very high risk. Contamination levels of paired water samples were positively correlated (r = 0.206, P = 0.003). After adjusting for repeated measures over time, boiled water samples that were transferred to another container were associated with small, but significantly lower levels of contamination (geometric mean 1.4 versus 2.7, P value < 0.05). Mixing of boiled water with non-boiled water or duration over the heat source was not significantly associated with fecal contamination.
Figure 1.
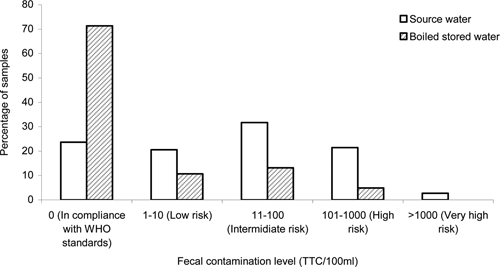
Percentage of water samples by risk category (N source = 224, N boiled = 206).
Discussion
Our results show that the practice of boiling in the study community significantly improves the microbiological quality of water, but does not fully remove the potential risk of waterborne pathogens. Although the 86.2% reduction observed here is lower than the 99% and 97% reductions reported in similar studies in India and Vietnam,6,13 this was largely a function of a lower level of contamination in the source water; the mean level of contamination in stored water that was reportedly boiled was similar in Guatemala (2.2 TTC/100 mL) to that in India (4.2) and Vietnam (5.8). As in the previous studies, we also observed a substantial shift in the risk profile of treated versus stored water. Over 70% of boiled water samples were free of TTC, only 4.9% of samples contained high (101–1,000) levels and none contained very high (> 1,000) levels.
It is important to note that these results reflect the effectiveness of the water treatment method as actually practiced by a remote, vulnerable community. This is in contrast to most recent studies in which short-term, research-driven interventions, which are usually accompanied by campaigns to instruct and encourage households to use the method being promoted. In Guatemala, as in Vietnam and India, boiling is not only effective but is widely and consistently practiced without any apparent need for recent interventions. This suggests that long-term use of HWT methods can provide drinking water of improved quality, though perhaps not in accordance to most strict guidelines.
While the results presented here are in accordance to our previous studies, other similar studies focused outside intervention and promotional efforts have reported little or no effect on the microbiological effect of routine HWT methods,7–9,14 suggesting that the effectiveness of these practices as actually performed at home may vary considerably.
Because the boiling practices reported by study participants suggested that they were heating water to levels sufficient to kill TTC, it seems likely that the observed levels of contamination in stored water were caused by recontamination of boiled water. Recontamination is a common problem where, as here, the treatment process does not leave a residual disinfectant (as chlorination would) and suitable vessels for safe storage are not always available.15 Participants reported both mixing boiled water with non-boiled water and dipping a cup into the container to draw water, practices that are highly likely to lead to recontamination.16 Although no statistical association between these practices and microbiological water quality were observed here, this study was not powered to identify statistically significant associations with such potential covariates. The transfer of boiled water to a second container, however, did show a small but significant decrease in contamination levels.
The manner in which the water is boiled in this rural Guatemalan community differed from those described in India and Vietnam. Although water was only boiled in those settings for short periods, and usually removed from the fire (or the fire extinguished) shortly after a rolling boil, in Guatemala boiling usually continued indefinitely. This could perhaps be solely driven by the difference between the plancha stove in Guatemala and the single-pot fires or stoves reportedly used in India and Vietnam. This difference in practices may make it difficult to estimate the cost of boiling and the potential savings on fuel and improvement in indoor air quality that could be obtained in Guatemala by shifting boilers to alternatives such as filtration, solar disinfection, or chlorination.
It was observed that overall, 8% of the households did not have boiled water at the time of the visit. This suggests that households may fail to treat their water at all times and perhaps supplement their water intake with untreated water. However, these values are lower than observed elsewhere.17,18 Furthermore, some people were occasionally observed to drink water from the tap, such as when washing their faces and it was also suspected that children sometimes drink from the tap. The inconsistency of HWT use has been observed by other researchers18–20 but unfortunately we did not formally collect any data on this aspect of boiling. A recent work has highlighted the risk of returning for short periods of time to untreated drinking water, the impact that this may have in this community is not clear.21
This study has important limitations that affect the generalizability of the results. First, the study community was not randomly selected and may not be representative of the country as a whole, much less other countries and settings. Second, the study was conducted over a relatively small period of time during the wet season; the microbial load in source waters typically increases in rainy seasons, which may not only affect source water quality but household water treatment practices. Third, boiling and post-boiling storage and use of water are culturally distinctive and can be expected to vary considerably between countries and ethnic groups. Fourth, the study population in this case was not affected by a disaster, displacement, or other emergency; field testing of reportedly boiled water in an emergency response has shown higher levels of contamination.22 Finally, while efforts were made to confirm survey results with direct observation, the effect of the research on study participants reported and observed behavior cannot be assessed.
Notwithstanding these limitations, our results are generally consistent with previous research on the microbiological effectiveness of boiling and the consistency of the practice among a population of self-reported boilers. In this respect, it provides additional guidance on how boiling—the most common household water treatment practice—is actually conducted. It also suggests the potential opportunities for optimizing the practice and further characterizes this benchmark of household water treatment.
Footnotes
Authors' addresses: Ghislaine Rosa, Laura Miller, and Thomas Clasen, Department of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, WC1E 7HT, United Kingdom, E-mails: ghislaine.rose@lshtm.ac.uk, l_miller@uwalumni.com, and thomas.clasen@lshtm.ac.uk.
References
- 1.Rosa G, Clasen T. Estimating the scope of household water treatment in low- and middle-income countries. Am J Trop Med Hyg. 2010;82:289–300. doi: 10.4269/ajtmh.2010.09-0382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sobsey MD. Managing Water in the Home: Accelerated Health Gains from Improved Water Supply. Geneva: The World Health Organization (WHO/SDE/WSH/02.07); 2002. [Google Scholar]
- 3.WHO . Guidelines for Drinking Water Quality. Third edition. Geneva: World Health Organization; 2008. [Google Scholar]
- 4.Wright J, Gundry S, Conroy R. Household drinking water in developing countries: a systematic review of microbiological contamination between source and point-of-use. Trop Med Int Health. 2004;9:106–117. doi: 10.1046/j.1365-3156.2003.01160.x. [DOI] [PubMed] [Google Scholar]
- 5.Clasen TF, Thao do H, Boisson S, Shipin O. Microbiological effectiveness and cost of boiling to disinfect drinking water in rural Vietnam. Environ Sci Technol. 2008;42:4255–4260. doi: 10.1021/es7024802. [DOI] [PubMed] [Google Scholar]
- 6.Clasen T, McLaughlin C, Nayaar N, Boisson S, Gupta R, Desai D, Shah N. Microbiological effectiveness and cost of disinfecting water by boiling in semi-urban India. Am J Trop Med Hyg. 2008;79:407–413. [PubMed] [Google Scholar]
- 7.Oswald WE, Lescano AG, Bern C, Calderon MM, Cabrera L, Gilman RH. Fecal contamination of drinking water within peri-urban households, Lima, Peru. Am J Trop Med Hyg. 2007;77:699–704. [PubMed] [Google Scholar]
- 8.Levy K, Hubbard AE, Nelson KL, Eisenberg JN. Drivers of water quality variability in northen coastal Ecuador. Environ Sci Technol. 2009;15:1788–1797. doi: 10.1021/es8022545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Luby SP, Syed AH, Atiullah N, Faizan MK, Fisher-Hoch S. Limited effectiveness of home drinking water purification efforts in Karachi, Pakistan. Int J Infect Dis. 1999;4:3–7. doi: 10.1016/s1201-9712(00)90058-4. [DOI] [PubMed] [Google Scholar]
- 10.PRESANCA . Fortalecimiento Municipal en Seguridad Alimentaria y Nutricional y Desarrollo Local 2006–2009. Resumen de Logros y Avances. Municipio de san Mateo Ixtatán: Departamento de Huehuetenango, Guatemala; 2009. [Google Scholar]
- 11.APHA . Standard Methods for the Examination of Water and Wastewater. 21st edition. Washington, DC: American Public Health Association/American Water Works Association/Water Environment Federation, Washington, DC; 2001. [Google Scholar]
- 12.Lloyd B, Helmer R. Surveillance of Drinking Water Quality in Rural Areas. Essex, England: Longman Scientific and Technical; 1991. [Google Scholar]
- 13.Clasen TF, Thao do H, Boisson S, Shipin O. Microbiological effectiveness and cost of boiling to disinfect drinking water in rural Vietnam. Environ Sci Technol. 2008;42:4255–4260. doi: 10.1021/es7024802. [DOI] [PubMed] [Google Scholar]
- 14.McLaughlin LA, Levy K, Beck NK, Shin GA, Meschke JS, Eisenberg JN. An observational study on the effectiveness of point-of-use chlorination. J Environ Health. 2009;71:48–53. [PMC free article] [PubMed] [Google Scholar]
- 15.Wright J, Gundry S, Conroy R. Household drinking water in developing countries: a systematic review of microbiological contamination between source and point-of-use. Trop Med Int Health. 2003;9:106–117. doi: 10.1046/j.1365-3156.2003.01160.x. [DOI] [PubMed] [Google Scholar]
- 16.Wright J, Gundry S, Conroy J. Household drinking water in developing countries: a systematic review of microbiological contamination between source and point-of-use. Trop Med Int Health. 2004;9:106. doi: 10.1046/j.1365-3156.2003.01160.x. [DOI] [PubMed] [Google Scholar]
- 17.Arnold B., Mäusezahl D, Hubbard A, Colford JM., Jr Evaluation of a pre-existing, 3-year household water treatment and handwashing intervention in rural Guatemala. Int J Epidemiol. 2009;38:1651–1661. doi: 10.1093/ije/dyp241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Moser S, Heri S, Mosler HJ. Determinants of the Diffusion of SODIS. A Qualitative Field Study in Bolivia: Summary Report. 2005.
- 19.Boisson S, Schmidt WP, Berhanu T, Gerrage K, Gairaj V. Randomized controlled trial in rural Ethiopia to assess a portable water treatment device. Environ Sci Technol. 2009;43:407–413. doi: 10.1021/es9000664. [DOI] [PubMed] [Google Scholar]
- 20.Rose A, Roy S, Abraham V, Holmgren G, George K, Bairaj V, Abrahams S, Muliyil J, Joseph A, Kang G. Solar disinfection of water for diarrhoeal prevention in southern India. Arch Dis Child. 2006;91:139–141. doi: 10.1136/adc.2005.077867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hunter PR, Zmirou-Navier D, Hartemann P. Estimating the impact on health of poor reliability of drinking water interventions in developing countries. Sci Total Environ. 2009;407:2621–2624. doi: 10.1016/j.scitotenv.2009.01.018. [DOI] [PubMed] [Google Scholar]
- 22.Gupta SK, Suanatio O, Gray A, Widyastuti E, Jain N, Rolos R, Hoekstra RM, Quick R. Factors associated with E. coli contamination of household drinking water among tsunami and earthquake survivors, Indonesia. Am J Trop Med Hyg. 2007;76:1158–1162. [PubMed] [Google Scholar]