

Abstract
PURPOSE
To report the delayed development of idiopathic fullthickness macular hole in eyes with previously documented complete posterior vitreous detachment that were vitrectomized during surgery for rhegmatogenous retinal detachment.
METHODS
Two interventional case reports with serial color fundus photographs and optical coherence tomography scans.
RESULTS
Case 1
A 62yearold man underwent vitrectomy, cryoretinopexy, and intraocular gas tamponade for rhegmatogenous retinal detachment associated with a complete posterior vitreous detachment. Three years later, he developed a fullthickness macular hole in the same eye. Peeling of the inner limiting membrane and gas tamponade resulted in complete closure of the macular hole with improvement in visual acuity.
Case 2
A 70yearold man presented with a maculaoff inferior retinal detachment and counting fingers vision. Vitrectomy, cryoretinopexy to a single tear, and gas tamponade was successful and acuity improved to 6/9. He subsequently developed retinal redetachment associated with a new retinal tear and was treated by further vitrectomy and gas. He developed a fullthickness macular hole in the same eye 2 years later with acuity dropping to 1/60.
CONCLUSIONS
Macular hole formation may occur in the context of vitrectomized eyes. These observations support the hypothesis that anteroposterior vitreomacular traction, while traditionally implicated, is not always essential for the development of macular holes.
Keywords: Macular hole, Vitrectomy, Posterior vitreous detachment
INTRODUCTION
Macular hole formation is believed to be the result of anteroposterior vitreofoveal and tangential traction on the basis of Gass’ theories, histopathologic studies, and more recent optical coherence tomography (OCT) imaging series. Traction is thought to cause umbo dehiscence, and progressive enlargement of the hole is believed to ensue as a result of the inherent elasticity and tension of the inner retina (1, 2). However, development of macular holes in vitrectomized eyes is now being reported in the literature (3, 4). We describe two such cases and postulate etiologic mechanisms.
Case reports
Case 1
A 62yearold man presented in 2004 with rhegmatogenous retinal detachment of 1 week’s duration, involving the macula and associated with a complete posterior vitreous detachment and retinal utear. There was no history of ocular trauma and he underwent successful vitrectomy, cryoretinopexy, and sulphahexafluoride intraocular gas tamponade. He subsequently had uncomplicated phacoemulsification with lens implant in the same eye, resulting in a visual acuity of 6/9. He presented again in 2007 with recent onset blurred vision and acuity of 6/24 associated with a fullthickness macular hole (Fig. 1) also confirmed on OCT scan (Fig. 2A). During this further vitrectomy for the macular hole, intraoperative examination aided by trypan blue dye did not reveal residual vitreous cortex or epiretinal membrane and peeling of the inner limiting membrane and longacting intraocular gas tamponade with C3F8 resulted in complete closure of the macular hole with improvement in visual acuity to 6/9 (Fig. 2B).
Fig. 1.

Case 1 right eye (A) with stage IV macular hole and left eye (B) with healthy macula.
Fig. 2.
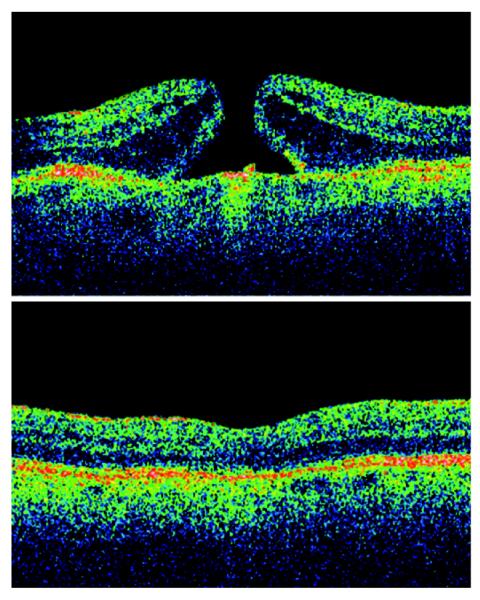
Case 1 preoperative optical coherence tomography (OCT) (A) and postoperative OCT (B) of right eye.
Case 2
A 70yearold man presented in 2005 with a 1month history of decreased vision. Visual acuity was counting fingers left and an inferior maculaoff retinal detachment with a single tear was diagnosed. He underwent prompt vitrectomy and cryotherapy with SF6 gas tamponade and at 6 weeks visual acuity was 6/9 and the retina was attached. He represented 2 weeks later with a recurrent inferior maculaon retinal detachment with a new tear and an acuity of 6/12. He underwent a second vitrectomy with cryoretinopexy, endolaser, and oil insertion. The retina remained attached under oil and acuity stable at 6/12. Removal of oil was undertaken at 2 years after the second vitrectomy, due to persistent ocular hypertension, but visual acuity gradually declined to 1/60 and clinical examination and OCT scan confirmed development of a new fullthickness macular hole with an associated epiretinal membrane (Fig. 3). Further surgery was declined by the patient.
Fig. 3.

Case 2 combined color photograph (A) and optical coherence tomography (OCT) (B) of left eye showing stage IV macular hole, despite two previous vitrectomies, and also an associated epiretinal membrane
DISCUSSION
To our knowledge, the development of macular hole following vitrectomy for retinal detachment has not previously been reported. The only published series (3) describes such a phenomenon in three patients who had undergone previous vitrectomy for macular pucker or vitreous hemorrhage related to a retinal break. The authors postulated that a degenerative process might occur in the inner retinal layers either in the form of atrophic attenuation of tissue or a coalescence of perifoveal cystic spaces. The other reported case (4) is of a pseudophakic eye which developed spontaneous formation, closure, and then recurrence of a macular hole over a 1year period following vitrectomy for vitreous hemorrhage secondary to a retinal macroaneurysm. Macular hole formation in vitrectomized eyes is thus rare. Following vitrectomy, the anteroposterior vitreofoveal traction implicated in macular hole development cannot be relevant. This would be particularly true in our second case, where any remaining vitreous was meticulously removed following redetachment. We can speculate that macular holes in vitrectomized eyes might result from tangentially acting subclinical tractional elements, such as residual cortical vitreous or epiretinal membrane formation as seen in case 2. Cystic degenerative changes may be involved and lowgrade inflammation might be associated with activation of retinal glial cells. In Case 1, development of asymptomatic subclinical cystoid macular edema following cataract surgery with later coalescence of such cystic spaces may potentially have been associated with hole development. Retinal glial tissue contraction could then cause gradual hole enlargement. In conclusion, our two cases show that macular hole formation may rarely occur in the context of a vitrectomized eye. We also illustrate that in such eyes, careful peeling of the internal limiting membrane and intraocular gas tamponade can result in hole closure and successful restoration of useful vision.
ACKNOWLEDGEMENTS
We are grateful to NIHR Biomedical Research Centre for Ophthalmology at Moorfields and University College London.
Footnotes
The authors have no proprietary interest in this work, received no funding, and have not submitted or presented it elsewhere.
REFERENCES
- 1.Smiddy WE, Flynn HW. Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol. 2004;137:52537. doi: 10.1016/j.ajo.2003.12.011. [DOI] [PubMed] [Google Scholar]
- 2.Altaweel M, Ip M. Macular hole: improved understanding of pathogenesis, staging and management based on optical coherence tomography. Semin Ophthalmol. 2003;18:5866. doi: 10.1076/soph.18.2.58.15858. [DOI] [PubMed] [Google Scholar]
- 3.Lipham WJ, Smiddy WE. Idiopathic macular hole following vitrectomy: implications for pathogenesis. Ophthalmic Surg Lasers. 1997;28:6339. [PubMed] [Google Scholar]
- 4.Lo WR, Hubbard G Baker. Macular hole formation, spontaneous closure and recurrence in a previously vitrectomised eye. Am J Ophthalmol. 2006;141:9624. doi: 10.1016/j.ajo.2005.12.012. [DOI] [PubMed] [Google Scholar]