

Abstract
Background
Although comprehensive burn care requires significant resources, patients may be treated at verified burn centers, non-verified burn centers, or other facilities due to a variety of factors. The purpose of this study was to evaluate the association between patient and injury characteristics and treatment location using a national database.
Study Design
We performed an analysis of all burn patients admitted to United States hospitals participating in the Healthcare Cost and Utilization Project over 2 years. Univariate and multivariate analyses were performed to identify patient and injury factors associated with the likelihood of treatment at designated burn care facilities. Definitve care facilities were categorized as American Burn Association verified centers, non-verified burn centers, or other facilities.
Results
Over the two years, 29,971 burn patients were treated in 1,376 hospitals located in 19 participating states. A total of 6,712 (22%) patients were treated at verified centers, with 26% and 52% treated at non-verified or other facilities, respectively. Patients treated at verified centers were younger than those at non-verified or other facilities (33.1 years vs. 33.7 years vs. 41.9 years, p<0.001) and had a higher rate of inhalation injury (3.4% vs. 3.2% vs. 2.2%, p<0.001). Independent factors associated with treatment at verified centers include burns to the head/neck (RR 2.4, CI 2.1-2.7), hand (RR 1.8, CI 1.6-1.9), electrical injury (RR 1.4, CI 1.4, CI 1.2-1.7), and fewer co-morbidities (RR 0.55, CI 0.5-0.6).
Conclusions
More than two-thirds of significantly burned patients are treated at non-verified burn centers in the U.S. Many patients meeting ABA criteria for transfer to a burn center are being treated at non-burn center facilities.
Introduction
Over the past 60 years of organized burn care in the United States, there have been great advances to improve the mortality and outcomes of those who survive injury. The evolution of organized burn care has included multi-disciplinary care of the burned patient and the development of specialized burn centers. Although comprehensive burn care requires significant resource allocation, patients may be treated in various hospital settings. Currently, there are 132 burn facilities listed in the American Burn Association (ABA) directory; only 56 of these are verified as burn centers by the American College of Surgeons/American Burn Association—the sole mechanism to receive verification.(1) In addition, burn patients may receive a portion or the entirety of their care at other facilities not designated as specialized burn care facilities.
A number of factors likely guide patient treatment location. The ABA has established burn center referral criteria to help guide decisions regarding triage and transfer based on patient age, injury mechanism and extent and other factors that may complicate burn wound management.(2) However, other factors may also influence treatment location such as geographic location of injury and, potentially, payer status. We have previously demonstrated that payer status significantly impacted burn patient treatment location in Washington State.(3) This relationship between payer status and treatment location has also been demonstrated in the general, non-burn trauma population.(4)
The purpose of this study was to evaluate the patient and injury characteristics that influence burn patient treatment location on a national level.
Methods
We performed an analysis of burn patients admitted to United States hospitals, utilizing the State Inpatient Databases (SID) for 2001 and 2004. The SID are relational databases under the sponsorship of the Agency for Healthcare Research and Quality's Health Care Cost and Utilization Project. The SID includes hospital admissions for all-payers, with a core set of uniform data elements for cross state comparisons. Of the twenty-two participating states available, nineteen identified the treatment facility. Treatment facilities were categorized as ABA verified centers, non-verified burn centers (i.e. those centers self-listed in the ABA directory of burn facilities but not verified), or other facilities based on verification status at the time of patient admission. Regional comparisons were based on census categorization (Northeast, Southeast, Midwest, and West).
Patients were identified by using International Classification of Disease-9 codes for burn injury (ICD-9 codes 940-949). Patients with isolated inhalation injury were excluded. Data collected from 2001 and 2004 were aggregated to develop a single cohort of patients for analysis. We examined baseline patient characteristics (age and gender), injury characteristics (total burn surface area burn (TBSA), anatomic burn location, burn depth, and presence of inhalation injury) as well as the presence of a verified center in the State where treatment occurred. To examine the potential impact of co-morbid health states on treatment location, the presence of the following conditions (ICD-9) were evaluated: diabetes (250), cardiovascular disease (414), and pulmonary disease (460-519). Primary payer status was also examined. Finally, each of the major transfer criteria for treatment at a burn center was recorded for each patient (partial thickness burn >10% TBSA, face burns, hand burns, feet burns, genitalia burns, electrical burns, full thickness burns, chemical burns, inhalation injury, burns with co-morbid conditions, concomitant traumatic injury).(5)
Univariate and multivariate analyses were performed to identify patient and injury factors associated with the likelihood of treatment at designated burn care facilities. First, a univariate analysis was performed to identify significant factors associated with treatment location. A student's t-test was used for parametric data and the Mann-Whitney U test was used for non-parametric data. The Chi-square test of significance was used for univariate categorical data analysis. Next, we performed a multivariate logistic analysis to determine the patient and injury factor independently associated with treatment facility. Since HCUP is an administrative, not clinical, data set, ICD-9 codes for burn extent were not available for all patients. Because of the danger of biased estimates due to dropping cases with missing data, missing data was imputed using a system of multivariate imputation by chained equations.(6) Multiple imputation, and the MICE system in particular, has been shown to produce superior estimates to a complete-case analysis.(7) Variables that successfully predicted burn size in the non-missing data and variables that successfully predicted the likelihood of missingness were included in a multivariate model that over ten iterations refined the prediction of missing data. The process was duplicated ten times to produce ten multiply imputed datasets. The results of these datasets allowed us to model both the point estimates and the variance, or accuracy, of our imputed data.(8, 9) All analyses were performed using STATA version 10.0 (StataCorp, College Station, TX).
Results
Over the two-year period, 29,971 burn patients were discharged from 1,376 hospitals located in the 19 included states. There were 6,712 (22%) patients treated at verified centers, 7,697 (26%) and 15,576 (52%) treated at non-verified or other facilities, respectively. A higher proportion of males were treated at verified and non-verified centers compared to other facilities (72% vs. 68% vs. 59%, p<0.001) (Table 1). Patients treated at verified centers had a lower average age (33.1 ± 22.7 vs. 33.7 ± 23.7 vs. 41.9 ± 25.8, p<0.001). Verified and non-verified burn centers treated a higher proportion of young patients (<5 years of age), whereas non-burn hospitals treated a higher proportion of those ≥ 55 years of age (Table 1). When stratified by pediatric (< 18 years of age) or adult patient, a similar relationship existed (data not shown).
Table 1.
Patient and Injury Characteristics
| Variable | Hospital Type | p Value | ||
|---|---|---|---|---|
| Verified | Nonverified | Other | ||
| Total | 67,100 (22.3%) | 76,920 (25.7%) | 155,690 (52.0%) | |
| Age, y | ||||
| Mean ± SD | 33.1 ± 22.7 | 33.7 ± 23.7 | 41.9 ± 25.8 | <0.001 |
| 0-5 y | 17.1% | 18.8% | 13.6% | |
| 6-15 y | 7.7% | 7.4% | 5.8% | |
| 16-54 y | 57.6% | 54.5% | 47.8% | <0.001 |
| 55-75 y | 13.2% | 13.9% | 20.9% | |
| ≥75 y | 4.4% | 5.4% | 11.9% | |
| TBSA (full thickness) | ||||
| <10% | 63.1% | 64.8% | 65.1% | |
| 11-20% | 19.8% | 18.3% | 16.8% | <0.001 |
| 21-40% | 11.1% | 11.3% | 12.4% | |
| >41% | 6.0% | 5.6% | 5.7% | |
| Gender (% male) | 72% | 67% | 59% | <0.001 |
| Inhalation injury | 3.0% | 3.9% | 2.2% | <0.001 |
| Obesity | 0.7% | 0.9% | 2.7% | <0.001 |
Verified and non-verified centers treated more patients with inhalation injury compared to other hospitals (3.0% vs. 3.9% vs. 2.2%, p<0.001). This was also the case for head and neck burns (39.2% vs. 35.7% vs. 18.9%, p<0.001) and electrical injuries (3.7% vs. 2.3% vs. 1.8%, p<0.001). Among all hospital types, the mean burn size was <10% TBSA full thickness injury. Compared to other hospitals, verified burn centers were slightly more likely to treat those with >40% TBSA (RR 1.09, 95% CI 1.05-1.14).
However, regardless of total burn size, almost half of all patients were treated at non-burn hospitals (Figure 1). Although 90% of patients in the HCUP sample lived in a state that had a verified burn center, treatment location varied by geographic region (Table 2). Patients in states with a verified burn center were less likely to be treated at non-verified burn centers (RR 0.52, 95% CI 0.51-0.54). A higher proportion of those who lived in Western states were treated in verified burn centers.
Figure 1.
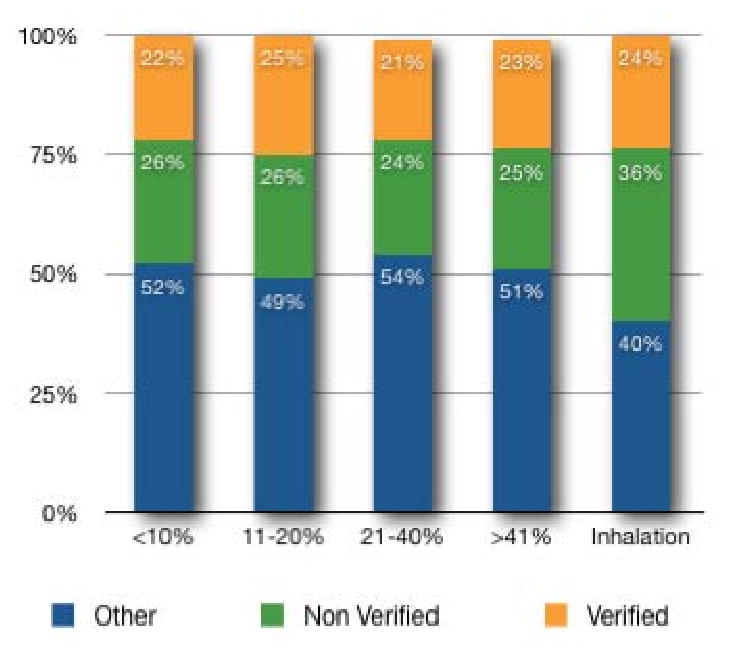
Type of treating facility by the proportion of total burn surface area burned.
Table 2.
Regional Variability
| Hospital type | ||||
|---|---|---|---|---|
| Variable | Verified, % | Nonverified, % | Other, % | p Value |
| Northeast | 16 | 30 | 54 | |
| Southeast | 18 | 30 | 52 | <0.001 |
| Midwest | 19 | 28 | 53 | |
| West | 44 | 9 | 47 | |
We examined the extent to which treatment location reflects ABA guidelines for referral to a burn center. Figure 2 demonstrates that for many of the referral criteria, the majority of patients are treated at non-burn facilities. While verified centers were more likely to care for patients with head and neck burns (RR 2.76, 95% CI 2.71-2.82), hand burns (RR 2.15, 95% CI 2.11-2.19), electrical injuries (RR 2.05, 95% CI 1.94-2.17) and patients with inhalation injuries (RR 1.40, 95% CI 1.32-1.48), the majority of patients (67%) with comorbidities were treated at other facilities.
Figure 2.

Type of treating facility for patients meeting ABA burn center transfer criteria.
The payer status of patients admitted to each facility type is shown in Figure 3. A higher proportion of Medicare patients (70%) were treated at non-burn hospitals. Non-verified hospitals treated a slightly higher proportion of those with Medicaid; commercial insurance was similar across all hospitals. Verified and non-verified hospitals treated a higher proportion of patients with workers compensation.
Figure 3.
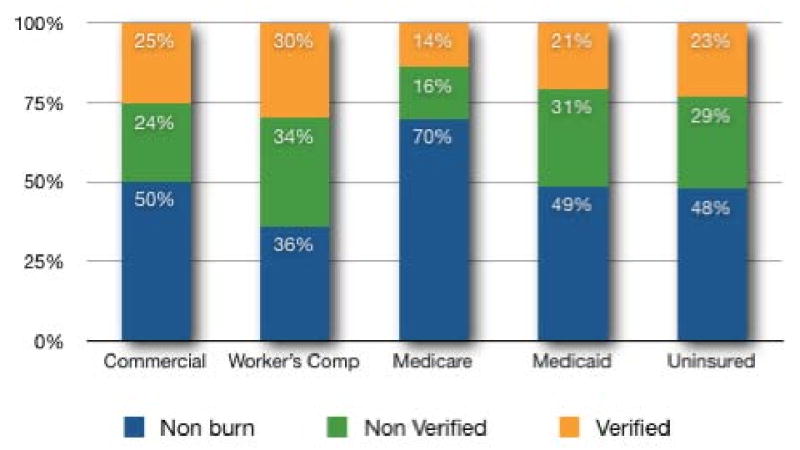
Type of treating facility by patient's payer status.
On multivariate analysis, independent characteristics associated with treatment at verified centers include burns to the head and neck (RR 2.40, 95% CI 2.13-2.71) and hand (RR 1.77, 95% CI 1.64-1.90) (table 3). Those with >40% burns and evidence of an inhalation injury were 3.29 fold more likely to be treated at a burn center compared to other facilities (aRR 3.29, 95% CI 1.32-8.18). Elderly patients were half as likely to be treated at a verified burn center (aRR 0.45, 95% CI 0.63-0.72) as were patients with co-morbidities (aRR 0.55, 95% CI 0.50-0.60). Those with hand burns (aRR 1.8, 95% CI 1.64-1.90), head and neck burns (aRR 2.40, 95%CI 2.13-2.71), and electrical injuries (aRR 1.41, 95% CI 1.16-1.70) were more likely to be treated at a verified burn center.
Table 3.
Predictors of Treatment at Verified and Nonverified Burn Hospitals Compared to Other Hospitals (Comparison Group)
| Hospital type | ||||||
|---|---|---|---|---|---|---|
| Verified | Nonverified | |||||
| aRR | 95% CI | p Value | aRR | 95% CI | p Value | |
| Age, y | ||||||
| 0-5 | Ref | Ref | -- | Ref | Ref | -- |
| 6-15 | 1.04 | (0.90, 1.19) | 0.60 | 0.91 | (0.80, 1.04) | 0.17 |
| 16-54 | 0.92 | (0.81, 1.04) | 0.18 | 0.82 | (0.73, 0.92) | 0.001 |
| 55-75 | 0.66 | (0.57, 0.77) | <0.001 | 0.63 | (0.55, 0.72) | <0.001 |
| ≥75 | 0.44 | (0.36, 0.53) | <0.001 | 0.46 | (0.39, 0.54) | <0.001 |
| Gender (female) | 0.67 | (0.63, 0.73) | <0.001 | 0.78 | (0.73, 0.82) | <0.001 |
| TBSA, %* | ||||||
| 0-10 | Ref | -- | -- | Ref | -- | -- |
| 11-20 | 1.09 | (0.48, 2.45) | 0.80 | 0.99 | (0.49, 2.00) | 0.98 |
| 21-40 | 0.89 | (0.23, 2.79) | 0.81 | 0.88 | (0.31, 2.43) | 0.77 |
| >40 | 0.91 | (0.32, 3.70) | 0.86 | 0.97 | (0.33, 3.17) | 0.95 |
| TBSA, %† | ||||||
| 0-10% | Ref | -- | -- | Ref | -- | -- |
| 11-20% | 0.63 | (0.14, 2.79) | 0.11 | 1.04 | (0.28, 3.78) | 0.86 |
| 21-40% | 1.58 | (0.26, 9.55) | 0.09 | 1.75 | (0.36, 8.49) | 0.02 |
| >40% | 3.18 | (0.42, 23.7) | 0.01 | 2.17 | (0.32, 14.6) | 0.06 |
| Inhalation | 0.96 | (0.78, 1.28) | 0.76 | 1.25 | (0.95, 1.64) | 0.11 |
| Electrical injury | 1.41 | (1.16, 1.70) | <0.001 | 0.91 | (0.74, 1.13) | 0.41 |
| Burn location | ||||||
| Hand | 1.77 | (1.64, 1.90) | <0.001 | 1.59 | (1.47, 1.71) | <0.001 |
| Head/neck | 2.40 | (2.13, 2.71) | <0.001 | 2.11 | (1.90, 2.34) | <0.001 |
| ≥ 1 comorbidity | 0.55 | (0.50, 0.60) | <0.001 | 0.56 | (0.22, 0.61) | <0.001 |
Without an inhalation injury.
With inhalation injury.
Finally, we explored the relationship between payer status and treatment location (Table 4). On multivariate analysis, verified centers were less likely to treat Medicaid (0.77, 95% CI 0.69-0.85) or Medicare (0.58, 95% CI 0.50-0.67) burn patients, but more likely to care for patients with worker's compensation claims or government insurance (1.72, 95% CI 1.52-1.95).
Table 4.
Effect of Payer Status on Treatment Location*
| Hospital type | ||||||
|---|---|---|---|---|---|---|
| Verified | Nonverified | |||||
| aRR | 95% CI | p Value | aRR | 95% CI | p Value | |
| Medicaid | 0.77 | (0.69, 0.85) | <0.001 | 1.20 | (1.09, 1.31) | <0.001 |
| Medicare | 0.58 | (0.50, 0.67) | <0.001 | 0.63 | (0.54, 0.72) | <0.001 |
| Uninsured | 0.97 | (0.85, 1.11) | 0.69 | 1.11 | (0.98, 1.26) | 0.09 |
| Workers comp/govt | 1.72 | (1.52, 1.95) | <0.001 | 2.02 | (1.79, 2.27) | <0.001 |
Reference: Commercial.
Adjusted for age, burn size, inhalation injury.
Discussion
The data generated by the Healthcare Cost and Utilization Project provide a unique opportunity to examine the delivery of burn care on a national level. In this study, we found that almost half of all burned patients were treated at facilities that are not only non-verified burn centers but are not even self-designated burn care facilities. It appears that burn extent and location remain primary determinants of burn treatment location.
Overall, age was an important determinant of treatment location with younger patients being more likely to be treated at verified and non-verified burn hospitals, especially those younger than 5 years of age. At the other extreme, older adults were more likely to be treated at non-burn facilities. This finding is consistent with the trauma literature, where MacKenzie demonstrated that those treated in non-trauma centers tended to be older and female, with multiple co-morbidities (unadjusted data).(10) Although more likely to be treated at non-burn hospitals, the median burn size for elderly patients was smaller than those presenting at verified and non-verified burn facilities. Further, verified burn centers treated twice as many elderly patients with burns >40% TBSA than those at non-burn hospitals.
One speculative reason for non-burn center treatment of the elderly may be the desire to remain closer to home rather than travelling sometimes hundreds of miles to a burn center. A less intuitive reason may be the greater number of comorbidities in this population. In general, patients with fewer comorbid conditions were less likely to be treated at a verified or non-verified burn hospital. Data from the national burn repository suggest that mortality dramatically increases in the older population, two-fold among 65-74 year olds and five-fold in those older than 75.(11) In addition, there may be social pressures why elderly patients are not transported to burn centers. If a patient had been treated for decades by a family physician familiar with their medical history, there may be a reluctance to transfer the patient to a verified or non-verified burn hospital. With less experience managing large burn injury, there may also be a tendency to accept clinical nihilism. That is, the assumption that an injury or burn in the elderly patient will result in a poor outcome and that the initiation of aggressive burn care may still ultimately lead to a poor outcome. Such attitudes toward early prognosis after severe injury have been well documented in the neurosurgical literature.(12, 13) The potential danger in such a nihilistic approach is that it will certainly lead to a self-fulfilling outcome. Treatment location and outcomes in this segment of society will become increasingly prominent with our aging population.
We examined the extent to which treatment at a burn center was consistent with the triage and referral guidelines established by the ABA. Patients with evidence of inhalation injury and burns to the head and neck were more likely to be treated at verified or non-verified burn centers. Further, patients who sustained electrical injury were more likely to be treated at a verified center. These findings are consistent with previous studies examining factors associated with burn center treatment.(2, 3, 14) Interestingly, patients with >40% TBSA burns were treated at non-burn hospitals—this was particularly true for patients with multiple co-morbidities. With an inter-disciplinary focus as a component of burn center designation, it would be expected that medically complex burn patients should be treated at such centers. In fact, several studies have demonstrated that patients who receive optimal burn care at verified centers may have a better functional outcome after discharge.(5, 15) This may provide an opportunity for the burn community to educate and reinforce transfer criteria to non-burn hospitals, as well as for CMS to consider whether payment for treatment of large burns outside of burns centers is appropriate.
Neither inhalation injury nor %TBSA was an independent predictor of treatment at a verified burn center. However, when inhalation injury was present, %TBSA was highly predictive of treatment at both non-verified and verified burn centers. This may be due to the high correlation between burn severity and the likelihood of having an inhalation injury. However, this effect modification may represent an unmeasured relationship between burn severity and treatment location.
Regional variability of burn care was heterogeneous with the exception of Western states. Although 90% of the population studied lived in a state with a verified burn center, fewer than half were treated at one. Although many patients were treated in non-burn hospitals, states with verified burn centers were less likely to treat burned patients at non-burn hospitals or non-verified burn centers.
Payer status varied by hospital type, with a significantly lower proportion of Medicare patients treated at verified burn centers. This is correlated with older, co-morbid patients treated at non-burn hospitals. As previously stated, it is difficult to determine whether payer status, age, co-morbidity, or a combination of these was the major factor that determined burn treatment location. Half of all patients with commercial insurance were treated in a non-burn hospital, with an equal distribution between non-verified and verified burn centers. Patients with worker's compensation were almost twice as likely to be treated at a verified burn hospital, where non-verified centers were slightly more likely to treat those with Medicaid. Payer status appeared to be an independent predictor of treatment location, even after accounting for age, burn size, and the presence of an inhalation injury. This finding differs from the trauma literature where uninsured patients were twice as likely to be treated at a trauma center.(4) Burn hospitals were more likely to treat those with commercial or workers compensation insurance.
There are several limitations to this study. First, the Healthcare Cost and Utilization Project is not designed specifically to collect detailed information on burn patients. As an administrative database, it is likely that estimation of burn size may be misclassified as either over- or underestimated. Collis et. al. described significant underestimation of burns larger than 20% TBSA and overestimation of smaller burns.(16) More commonly, there is overestimation in burn size, especially among non-specialists who may assess few burned patients per year. We have demonstrated that referring physicians can incorrectly estimate burn size up to 3-fold greater than true burn size.(14) Such misclassification of burn size, especially among non-burn hospitals, may have overestimated the severely burned population. Further, the outcome measures captured in a database not designed for that purpose are crude and may not reflect a useful measure of quality among facility types. For these reasons, we did not address outcome measures in this study.
Quality control in analyses of large datasets is an important consideration. The HCUP-SID used in our study generates its data from UB-92 billing forms. Although purely administrative in nature, it remains one of the most comprehensive datasets because it represents over 90% of all U.S. hospitals. HCUP quality control is the internal responsibility of each participating hospital. Although burn-specific databases such as the National Burn Repository exist, it is only comprised of patients admitted to participating burn centers. As we have demonstrated, this represents a fraction of all U.S. burn patients. Both the HCUP and NBR are patient de-identified, therefore a direct comparison of data quality would not be possible. Furthermore, burn center verification status cannot be ascertained in the NBR.
In the current economic climate, private and government agencies are becoming more interested in defining therapies, systems, and proven guidelines that improve patient outcome. The trauma verification process has been shown to improve patient mortality, length of stay, and overall care of the severely injured patient.(17, 18) Such convincing data is less prevalent in the burn literature. Palmieri et. al. attempted to examine outcomes between burn centers that were verified and non-verified in California.(19) They found that verified centers had longer lengths of stay without a mortality difference. Our study is one of the first to not only examine the characteristics of treatment location among burn hospitals, but compares multiple states. Future exploration of national treatment and outcome measures among burn and non-burn centers, similar to those performed for trauma care, should be encouraged.
In conclusion, more than three-quarters of significantly burned patients are treated at non-verified burn centers in the United States. Factors associated with treatment at verified centers include younger age, fewer comorbidities, burns to the hand, head and neck, and electrical injury. Currently, given that the only mechanism for assuring quality of burn care is through the ACS/ABA verification process, further studies are needed to determine the extent to which treatment quality is influenced by treatment location.
Acknowledgments
Supported by the National Center for Research Resources #1KL2RR025015-01, Harborview Injury Prevention and Research Center (HIPRC) R49/CE000197 from the Centers for Disease Control, and by the David and Nancy Auth-Washington Research Foundation Endowment.
Footnotes
Disclosure Information: Nothing to disclose.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
David Zonies, University of Washington Burn Center, Harborview Medical Center, Seattle, WA.
Christopher Mack, Harborview Injury Prevention and Research Center, Seattle, WA.
Bradley Kramer, University of Washington Burn Center, Harborview Medical Center, Seattle, WA.
Frederick Rivara, Harborview Injury Prevention and Research Center, Seattle, WA.
Matthew Klein, University of Washington Burn Center, Harborview Medical Center, Seattle, WA.
References
- 1.Association AB. Burn Center Verification. [1 March 2008];2008 2008. Available at: http://www.ameriburn.org/verification_verifiedcenters.php.
- 2.Association AB. Burn Center Referal Criteria. [15 December 2008];2008 2008. Available at: www.ameriburn.org.
- 3.Klein MB, Mack CD, Kramer CB, et al. Influence of injury characteristics and payer status on burn treatment location in Washington state. J Burn Care Res. 2008;29:435–440. doi: 10.1097/BCR.0b013e3181710846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nathens AB, Maier RV, Copass MK, et al. Payer status: the unspoken triage criterion. J Trauma. 2001;50:776–783. doi: 10.1097/00005373-200105000-00002. [DOI] [PubMed] [Google Scholar]
- 5.American College of Surgeons. Committee on T Resources for optimal care of the injured patient 2006. Chicago, IL.: American College of Surgeons; 2006. [Google Scholar]
- 6.van Buuren S, Boshuizen HC, Knook DL. Multiple imputation of missing blood pressure covariates in survival analysis. Stat Med. 1999;18:681–694. doi: 10.1002/(sici)1097-0258(19990330)18:6<681::aid-sim71>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 7.Ambler G, Omar RZ, Royston P. A comparison of imputation techniques for handling missing predictor values in a risk model with a binary outcome. Stat Methods Med Res. 2007;16:277–298. doi: 10.1177/0962280206074466. [DOI] [PubMed] [Google Scholar]
- 8.Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159:702–706. doi: 10.1093/aje/kwh090. [DOI] [PubMed] [Google Scholar]
- 9.Raghunathan TE. What do we do with missing data? Some options for analysis of incomplete data. Annu Rev Public Health. 2004;25:99–117. doi: 10.1146/annurev.publhealth.25.102802.124410. [DOI] [PubMed] [Google Scholar]
- 10.MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354:366–378. doi: 10.1056/NEJMsa052049. [DOI] [PubMed] [Google Scholar]
- 11.Pham TN, Kramer CB, Wang J, et al. Epidemiology and outcomes of older adults with burn injury: an analysis of the National Burn Repository. J Burn Care Res. 2009;30:30–36. doi: 10.1097/BCR.0b013e3181921efc. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ausman JI. Therapeutic nihilism and the elderly. Surg Neurol. 2008;69:546–547. doi: 10.1016/j.surneu.2008.02.019. [DOI] [PubMed] [Google Scholar]
- 13.Hemphill JC, 3rd, White DB. Clinical nihilism in neuroemergencies. Emerg Med Clin North Am. 2009;27:27–37. vii–viii. doi: 10.1016/j.emc.2008.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Klein MB, Nathens AB, Emerson D, et al. An analysis of the long-distance transport of burn patients to a regional burn center. J Burn Care Res. 2007;28:49–55. doi: 10.1097/BCR.0B013E31802C894B. [DOI] [PubMed] [Google Scholar]
- 15.Brigham PA, Dimick AR. The evolution of burn care facilities in the United States. J Burn Care Res. 2008;29:248–256. doi: 10.1097/BCR.0b013e31815f366c. [DOI] [PubMed] [Google Scholar]
- 16.Collis N, Smith G, Fenton OM. Accuracy of burn size estimation and subsequent fluid resuscitation prior to arrival at the Yorkshire Regional Burns Unit. A three year retrospective study Burns. 1999;25:345–351. doi: 10.1016/s0305-4179(99)00007-8. [DOI] [PubMed] [Google Scholar]
- 17.Ehrlich PF, Rockwell S, Kincaid S, et al. American College of Surgeons, Committee on Trauma Verification Review: does it really make a difference? J Trauma. 2002;53:811–816. doi: 10.1097/00005373-200211000-00001. [DOI] [PubMed] [Google Scholar]
- 18.MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354:366–378. doi: 10.1056/NEJMsa052049. [DOI] [PubMed] [Google Scholar]
- 19.Palmieri TL, London JA, O'Mara MS, et al. Analysis of admissions and outcomes in verified and nonverified burn centers. J Burn Care Res. 2008;29:208–212. doi: 10.1097/BCR.0b013e31815f31b4. [DOI] [PubMed] [Google Scholar]