

Abstract
Purpose
Talocalcaneal coalitions can be difficult to detect on plain radiographs, despite obvious clinical findings. The purpose of this study is two-fold: (1) to delineate the benefits of thin-cut computed tomography (CT) and 3D reconstructions and (2) to develop a classification scheme for talocalcaneal coalitions that will provide valuable information for surgical planning.
Methods
From 2005 to 2009, 54 feet (35 patients) with a talocalcaneal coalition were evaluated with thin-cut (1 mm) CT, using multi-planar 2D and 3D reconstructions. The talocalcaneal coalitions were classified into five types based on the cartilaginous or bony nature, location, and facet joint orientation.
Results
Bilateral coalitions were found in 22/35 patients. Types I and II were fibrocartilaginous coalitions, which was the most common type, comprising 40.7 and 16.7% of the coalitions, respectively. Of the patients, 14.8% had a shingled Type III coalition, while 11.1% of the feet examined had a complete bony coalition (Type IV). Small peripheral posterior bony coalitions (Type V), which are heretofore not described, were found in 16.7% of feet.
Conclusions
CT scans can provide valuable information regarding the bony or cartilaginous nature of coalitions, as well as the facet orientation, which is helpful in diagnosis and treatment. In this study, the 2D and 3D reconstructions revealed previously unreported peripheral posterior bony coalitions (Type V), as well as coalitions that are in the same plane as the standard CT cuts or Harris view radiographs (Type I). The CT scan also improved the crucial pre-operative planning of the resection in the more complex vertical and combined horizontal and vertical fibrocartilaginous coalitions (Type I and II). Additionally, the complete bony coalitions (Type IV) can be sized accurately, which is helpful in decision-making on the resectability of the coalition.
Keywords: Talocalcaneal coalition, 3D computed tomography
Introduction
The first anatomic description of talocalcaneal coalitions was by Zuckerkandl [1] in 1877. In 1921, Slomann [2] linked tarsal coalitions to flat feet, but it was Harris and Beath [3] who are credited with specifically identifying talocalcaneal coalitions as a significant cause of peroneal spastic flat foot. Radiographic signs were first reported by Conway and Cowell [4], who described three radiographic signs of talocalcaneal coalition and also designated tomography as critical for finding ‘hidden’ anterior coalitions. It was not until 1994 that Lateur et al. [5] described and named the well-known ‘C’ sign on a lateral X-ray, which can be indicative of a talocalcaneal coalition.
In the 1980s and 1990s, several authors reported on the use and importance of computed tomography (CT) for diagnosing and ruling out talocalcaneal coalitions, as well as mapping their size and location in relation to the subtalar joint facets [6–11]. More recently, three-dimensional (3D), multi-planar reformatted CT images have allowed for improved evaluation of the bony anatomy of the foot [12, 13]. To our knowledge, there have not been any studies reporting on the benefits of 3D CT scans to enhance the delineation of talocalcaneal coalitions and assist with surgical planning. Additionally, while the coalitions have been separated into different types (osseous, cartilaginous, fibrous), there has not, to date, been a classification scheme demonstrating the location, nature, and position of the coalition.
The purpose of this study is to identify the precise location and position of talocalcaneal coalitions and allow the identification of the easily missed posterior coalitions. We will develop a classification for these coalitions that includes the shape of the middle facet joint, as well as the location and nature of the coalition.
Materials and methods
After approval from the Institutional Review Board, a retrospective review was performed to identify all patients who had a suspected talocalcaneal coalition based on physical examination and radiographic findings, and confirmed by CT scan, between September 2005 and April 2009. A total of 35 patients (54 feet) were identified. 3D CT reconstructions were analyzed on all 54 feet. Conventional radiographic imaging was performed on all feet prior to proceeding with the CT scan.
A General Electric (GE) Lightspeed Volumetric CT scanner (General Electric, Milwaukee, WI, USA) was used to perform all examinations. As defined by the Tarsal Coalition Protocol at our institution, all patients were positioned supine on the examination table with both feet flat against a positioning box. The patients were scanned feet first, from the bottom of their feet proximally through their ankle joint. All examinations were performed without intravenous contrast. The raw axial 2D CT data was uploaded to a GE Advantage workstation and volume-rendering software was used to reconstruct the sagittal and coronal planes using a standard algorithm. 3D reconstructions were then generated after selecting the appropriate density threshold for bone.
All of the CT scans were reviewed by the primary author. The classification determination was made first by using the coronal CT images and combining that information with the information obtained from the 3D reconstructions. Each foot was then placed into the 1–5 classification scheme (Fig. 1).
Fig. 1.
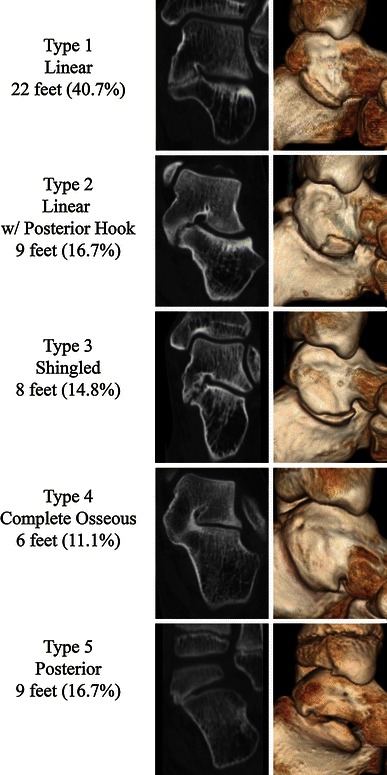
Talocalcaneal coalition classification scheme
Results
A total of 54 feet in 35 patients were included in this study (Fig. 2). There were 14 males and 21 females. The average age of the patients was 13.5 ± 2.9 years (range 8.5–18.6). Twenty-two patients (63%) were noted to have bilateral talocalcaneal coalitions. Of those, 13 had the same type on both feet, seven had different types, and two are unknown, as one foot had already had a prior resection upon presentation to our institution. Thirteen patients (37%) had unilateral involvement, seven involving the left foot and six involving the right foot. Interestingly, however, two of those patients were noted to have other fibrous coalitions in the opposite foot (one navicular-medial cuneiform, one third metatarsal-lateral cuneiform). Additionally, three feet with talocalcaneal coalitions were noted to also have a navicular-medial cuneiform coalition in the same foot. No other coalitions were identified in any of the feet studied.
Fig. 2.
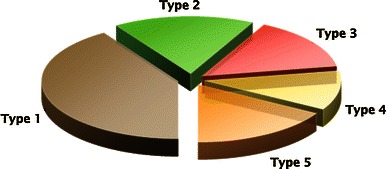
Distribution by type of coalition
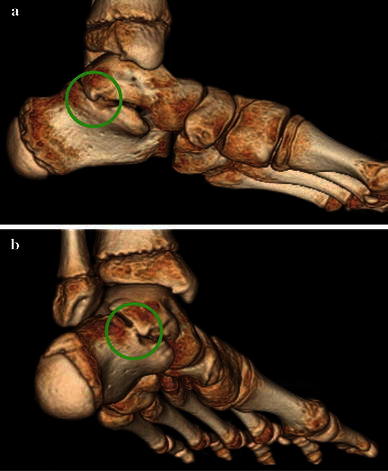
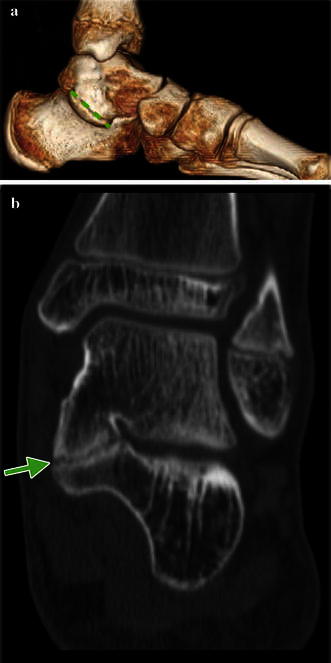
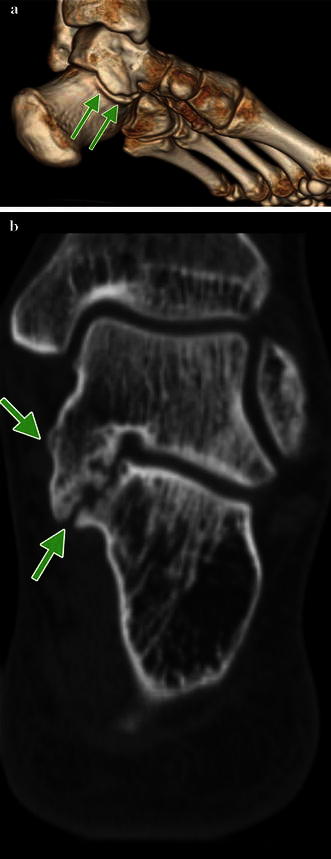
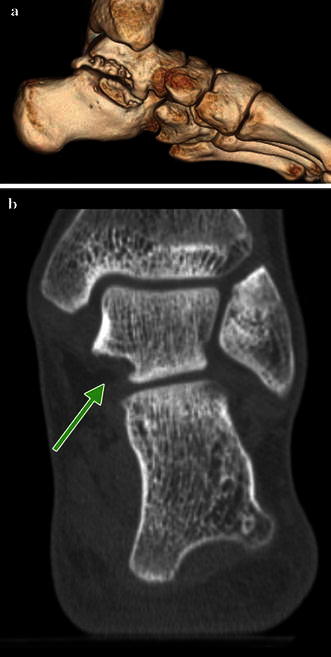
There were 22 feet (40.7%) that were classified as having a Type I talocalcaneal coalition. The average age for this group was 13.4 ± 2.9 years (range 9–18.6). Type I is a fibrocartilaginous linear coalition that runs parallel to the direction of the subtalar joint (Fig. 3). Nine feet (16.7%) with an average age of 14.8 ± 3.4 years (range 9.8–18.6) were classified as a Type II coalition, which is a fibrocartilaginous coalition that is linear anteriorly, but then curves into a posterior hook that overhangs medially, over and behind the sustentaculum tali (Fig. 4). There were eight feet (14.8%) classified as Type III, or shingled. The average age for this group was 13.9 ± 1.4 years (range 12.1–15.5). These coalitions had an orientation that sloped down in an overlapping fashion, with the talar portion shingled over the top of the calcaneal portion (Fig. 5). Six feet (11.1%) with an average age of 15.79 ± 2.2 years (range 12.4–18) were complete osseous coalitions of the middle facet, Type IV (Fig. 6). Nine feet (16.7%) were small, peripheral posterior coalitions, Type V (Fig. 7). The average age for this group was 10.77 ± 1.9 years (range 8.5–14). These were the most difficult to identify, and had even been missed previously on CT scans performed at external institutions.
Fig. 3.
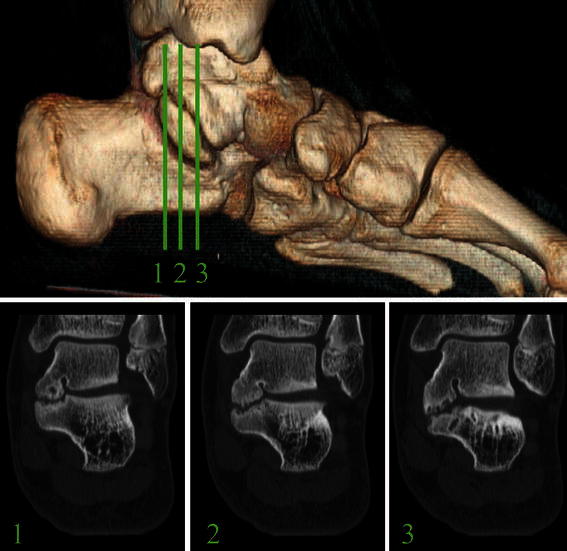
Type I linear coalition, 2D and 3D computed tomography (CT) scans
Fig. 4.

Type II linear coalition with posterior hook
Fig. 5.
a Type III shingled coalition, medial view. b Type III shingled coalition, posterior view
Fig. 6.

a Type IV complete osseous coalition, 3D CT. b Type IV complete osseous coalition, 2D CT
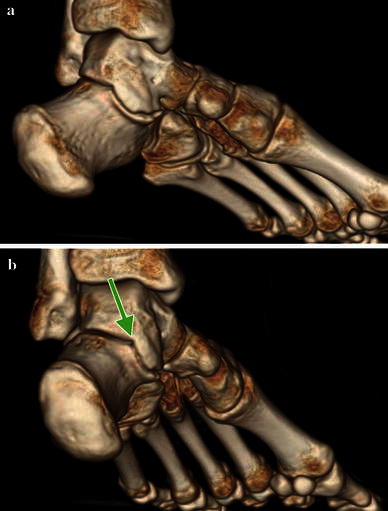
Fig. 7.
a Type V posterior coalition, medial view. b Type V posterior coalition, posteromedial view
Discussion
Three specific radiographic signs of talocalcaneal coalitions have been identified; talar beaking indicating decreased subtalar motion, broadening of the lateral process of the talus, and narrowing of the posterior talocalcaneal facet [4]. Additionally, Lateur et al. [5] described the ‘C’ sign on a lateral radiograph of the ankle. The C-shape, which is formed by the medial outline of the talar dome and the posteroinferior outline of the sustentaculum tali, is indicative of a talocalcaneal coalition. While these signs can often be seen on the plain radiographs, they do not necessarily confirm the coalition, nor do they give precise information regarding the location and orientation of the coalition. Herzenberg et al. [8] and Pineda et al. [9] clearly illustrated the benefits of CT scans to identify and rule out coalitions, determining CT scan to be the method of choice for diagnosis. These were 2D CT scans, however, and the details of the coalition were not as completely defined as can be done with a 3D CT scan. Wilde et al. [11] described the technique of mapping the size of a talocalcaneal coalition, but, again, the details of the orientation and precise location of the coalition were not clear.
This study demonstrates the extensive benefits of 3D CT scans to define the size, location, and orientation of talocalcaneal coalitions. By classifying talocalcaneal coalitions into five types, they can be more accurately described and, thus, be more accurately and easily resected. A CT classification scheme was proposed by Kumar et al. [14]; however, this scheme merely broke the coalitions down into osseous, cartilaginous, and fibrous, and did not provide significant clinical benefits for the excision of the coalition. Our classification system, by providing details that will assist in the surgical excision, can be clinically applied and utilized.
Type I: linear coalitions
Type I linear coalitions are the easiest to resect. The plane of coalition can be most easily identified (Fig. 8); however, 3D CT provides additional details regarding the plane of resection that cannot be visualized with 2D CT.
Fig. 8.
a Plane of resection for Type I coalition, 3D CT. b Plane of resection for Type I coalition, 2D CT
Type II: linear coalitions with posterior hook
With the Type II coalitions, the posterior hook can be easily missed on a standard 2D CT scan, potentially resulting in the wrong plane of cleavage (Fig. 9). If the plane of cleavage is started posteriorly at the overlapping hook and continued along this plane anteriorly, too much of the sustentaculum could be resected, resulting in destabilization of the flexor halluces longus tendon. Additionally, without the details of a 3D CT scan, the posterior hook could be missed altogether.
Fig. 9.

a Plane of resection for Type II coalition, 3D CT. b Plane of resection for Type II coalition, 2D CT
Type III: shingled coalitions
The shingled Type III coalitions may be related to a hypoplastic sustentaculum. The cleavage plane (Fig. 10), which may be quite inferior due to the overhanging talar portion, can be carefully identified on the 3D CT and aid in resection. Caution to identify this plane of cleavage is crucial, as starting too high may result in the resection wandering too far into the talus while searching for the subtalar joint (Fig. 11).
Fig. 10.
a Plane of resection for Type III coalition, 3D CT. b Plane of resection for Type III coalition, 2D CT
Fig. 11.
a Potential error of wandering into the talus when the wrong plane of resection is followed, 3D CT. b Potential error of wandering into the talus when the wrong plane of resection is followed, 2D CT
Type IV: complete osseous coalitions
The complete osseous coalitions, Type IV, are certainly the most difficult to resect, and debate still exists as to whether these should be resected at all. Scranton [15] arbitrarily determined that a coalition size of >50% of the width of the subtalar joint should not be resected, and others have indicated that a poor outcome is associated with the resection of talocalcaneal coalitions that were >50% of the size of the posterior facet. The size of the complete osseous coalitions is often quite large and, thus, a careful decision must be made as to whether or not to resect it [11, 16]. If a resection is to be undertaken, the 3D CT scan can provide additional help in determining the correct level of resection and illustrates improved bony landmarks.
Type V: posterior coalitions
The posterior coalitions that we define as Type V are previously unreported small coalitions that often lie directly under the posterior tibial artery and/or nerve (Fig. 12). These are easily missed on plain radiographs and even on standard 2D CT scans. 3D CT, however, beautifully illustrates these and certainly allows for a much easier surgical procedure. While these coalitions were typically small, they caused a similar limitation of subtalar motion and pain that accompanies the larger talocalcaneal coalitions. The resection, however, can be greatly simplified when the small area of bridging can be identified on 3D CT.
Fig. 12.

3D CT of Type V coalition, indicating the proximity of the posterior tibial artery/nerve
This study was limited by its retrospective nature. Additionally, a greater number of patients would strengthen the results. A clinical study, relating the surgical outcomes to this classification scheme, would also provide further insight and valuable information to validate this study. In conclusion, 3D CT scans illustrate the details of talocalcaneal coalitions, including the precise location, shape, and nature of the coalition, and provide significant information that is helpful for the resection of these coalitions.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
References
- 1.Zuckerkandl E. Ueber einen Fall von Synostose Zwischen talus und calcaneus. Allg Wein Med Zeitung. 1877;22:293–294. [Google Scholar]
- 2.Slomann HC. On coalition calcaneonavicularis. J Orthop Surg. 1921;3:586–588. [Google Scholar]
- 3.Harris RI, Beath T. Etiology of peroneal spastic flat foot. J Bone Joint Surg Br. 1948;30(4):624–634. [PubMed] [Google Scholar]
- 4.Conway JJ, Cowell HR. Tarsal coalition: clinical significance and roentgenographic demonstration. Radiology. 1969;92(4):799–809. doi: 10.1148/92.4.799. [DOI] [PubMed] [Google Scholar]
- 5.Lateur LM, Van Hoe LR, Van Ghillewe KV, Gryspeerdt SS, Baert AL, Dereymaeker GE. Subtalar coalition: diagnosis with the C sign on lateral radiographs of the ankle. Radiology. 1994;193(3):847–851. doi: 10.1148/radiology.193.3.7972836. [DOI] [PubMed] [Google Scholar]
- 6.Comfort TK, Johnson LO. Resection for symptomatic talocalcaneal coalition. J Pediatr Orthop. 1998;18(3):283–288. [PubMed] [Google Scholar]
- 7.Danielsson LG. Talo-calcaneal coalition treated with resection. J Pediatr Orthop. 1987;7(5):513–517. doi: 10.1097/01241398-198709000-00002. [DOI] [PubMed] [Google Scholar]
- 8.Herzenberg JE, Goldner JL, Martinez S, Silverman PM. Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study. Foot Ankle. 1986;6(6):273–288. doi: 10.1177/107110078600600601. [DOI] [PubMed] [Google Scholar]
- 9.Pineda C, Resnick D, Greenway G. Diagnosis of tarsal coalition with computed tomography. Clin Orthop Relat Res. 1986;208:282–288. [PubMed] [Google Scholar]
- 10.Stoskopf CA, Hernandez RJ, Kelikian A, Tachdjian MO, Dias LS. Evaluation of tarsal coalition by computed tomography. J Pediatr Orthop. 1984;4(3):365–369. doi: 10.1097/01241398-198405000-00016. [DOI] [PubMed] [Google Scholar]
- 11.Wilde PH, Torode IP, Dickens DR, Cole WG. Resection for symptomatic talocalcaneal coalition. J Bone Joint Surg Br. 1994;76(5):797–801. [PubMed] [Google Scholar]
- 12.Adler SJ, Vannier MW, Gilula LA, Knapp RH. Three-dimensional computed tomography of the foot: optimizing the image. Comput Med Imaging Graph. 1988;12(1):59–66. doi: 10.1016/0895-6111(88)90053-5. [DOI] [PubMed] [Google Scholar]
- 13.Charles YP, Louahem D, Diméglio A. Cavovarus foot deformity with multiple tarsal coalitions: functional and three-dimensional preoperative assessment. J Foot Ankle Surg. 2006;45:118–126. doi: 10.1053/j.jfas.2005.12.006. [DOI] [PubMed] [Google Scholar]
- 14.Kumar SJ, Guille JT, Lee MS, Couto JC. Osseous and non-osseous coalition of the middle facet of the talocalcaneal joint. J Bone Joint Surg Am. 1992;74(4):529–535. [PubMed] [Google Scholar]
- 15.Scranton PE., Jr Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am. 1987;69(4):533–539. [PubMed] [Google Scholar]
- 16.Luhmann SJ, Schoenecker PL. Symptomatic talocalcaneal coalition resection: indications and results. J Pediatr Orthop. 1998;18(6):748–754. [PubMed] [Google Scholar]