

Abstract
This Classic article is a reprint of the original work by Royal Whitman, A Study of the Weak Foot, with Reference to its Causes, its Diagnosis, and its Cure; with an Analysis of a Thousand Cases of So-Called Flat-Foot. An accompanying biographical sketch on Royal Whitman, MD, is available at DOI 10.1007/s11999-009-1129-7. The Classic Article is © 1896 by the Journal of Bone and Joint Surgery, Inc. and is reprinted with permission from Whitman R. A study of the weak foot, with reference to its causes, its diagnosis, and its cure; with an analysis of a thousand cases of so-called flat-foot. J Bone Joint Surg Am. 1896;s-1-8:42–77.
The function of the foot is to bear the weight of the body and to serve as a lever for its work. Normally, this weight and strain fall through the centre of the foot and are balanced there by muscular activity. If for any cause this normal relation is disturbed, the foot is thereby placed at a mechanical disadvantage in the performance of its functions, for in spite of the accommodative power of nature to disease and deformity, its mechanisms are subject to the same laws that govern other machines, a fact that must be appreciated if weakness is to be recognized and deformity overcome. If the foot, for example, is to perform its functions, its component parts must be in normal condition and held in proper relation to one another, the muscular power must be sufficient, and the strain and weight must not be too great for the strength of the mechanism. If any one of these conditions is lacking, the foot becomes unbalanced and ineffective as a lever; in other words, it loses its spring and elasticity, the ability to raise and propel the body.
When the foot ceases to act or to be used as a lever it loses the support and control of the muscles which have balanced the weight in its proper relation to it, and the attitude of passive support must be assumed, in which the burden falls on the inner side and the strain upon the ligaments. Whether this attitude is voluntarily assumed or whether it is forced upon the foot, the disuse of function and the mechanical disadvantages to which the foot is subjected predispose to weakness and deformity.
The type and exemplification of the weak foot is the so-called flat-foot, which not only has lost its ability as a lever, but is a source of discomfort and pain when used at all.
Flat foot, when fully developed, is practically a dislocation in which the astragalus has slipped downward and inward from the remainder of the foot to which the muscles are attached : this causes the bulging on the inner side, the most noticeable and characteristic sign of the affection. When such a foot is in use it is apparent that the deformity is made up of three elements:
The weight of the body falls upon its inner side; the foot is in a position of valgus.
The leg resting on the displaced astragalus turns in; the foot turns out, so that the line of strain through which the power is transmitted to the fulcrum no longer falls through the centre of the foot, but to its inner side; the foot is abducted or everted in its relation to the leg.
There are broadening and flattening of the arched portion of the foot; the foot is flat (Fig. 1).
Fig. 1.

Typical flat-foot of moderate degree, illustrating the component elements of valgus, abduction, and depression of the arch.
As a consequence of the displacements, the foot, considered as a machine, is twisted and out of gear, for the relation of the joint surfaces is so changed that motion is restricted and normal muscular action impossible. The foot is weak and vulnerable, constantly exposed to overstrain and injury; thus the deformity is usually progressive and is accompanied by spasm, secondary contraction, and atrophy of muscles, and by similar nutritive and accommodative changes in the bones and ligaments.
The compound deformity of flat-foot may be regarded simply as the development of the weak foot. Weak foot may be found in every grade, from the foot intrinsically strong, which is doing its work at a disadvantage because of improper attitudes unwittingly assumed, to the foot intrinsically weak or overburdened, and therefore obliged to assume the improper attitude.
As flat-foot is the further development of the weak foot, so the weak foot is often in its appearance and function the exaggeration or improper use of a normal attitude. To illustrate this fact, let one evert the foot and bear the entire weight of the body upon it, the leg being inclined somewhat forward to bring the weight over the head of the astragalus, and an approximation to the appearance of flat-foot may be produced; the inner border of the foot becomes slightly convex, the arch is lowered, and the line of strain is displaced to the inner side (Fig. 2). Yet this and a much greater burden may be borne without a semblance of deformity if the weight is thrown to the outer side of the foot and this great toe pressed firmly against the floor (Fig. 3).
Fig. 2.
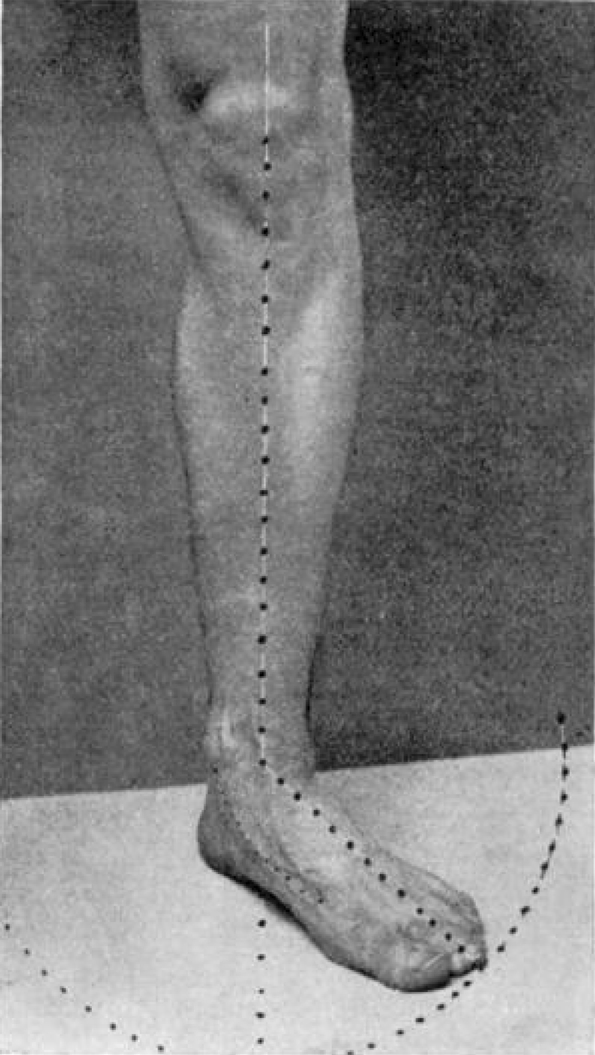
An attitude that simulates flat-foot.
Fig. 3.
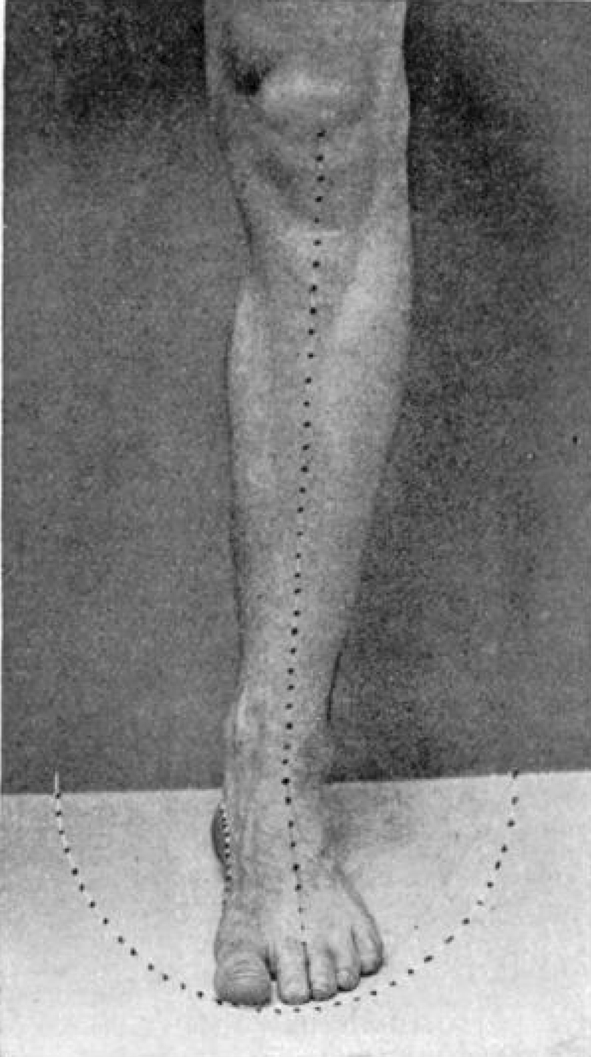
Compared with Fig. 2, illustrates the voluntary protection of the foot from overstrain.
This attitude illustrates the voluntary protection in which the weight is balanced by muscular activity. In the first illustration the strain falls on the inner, elastic, and mechanically weaker side, for the os calcis, hollowed out on its inner side for the passage of vessels and tendons, occupies a position of unstable equilibrium (Fig. 4); so that the weight of the body tends to tip it over into the flat-foot position of valgus (Fig. 5). Under the same influence the astragalus rotates downward and inward, still further increasing the instability of the os calcis. In this position the foot receives but little aid from the muscles, so that exaggeration to deformity is only prevented by the ligaments and by the shape of the articular surfaces; thus weakness may be induced by the excessive use of a normal attitude, and not only by that, as in long standing, but also by its improper use in work that demands active motion, and in which this active motion and alternation of postures, and thus relief from constant strain, are essential to its integrity. For, although the work performed in walking is greater than that required for standing, yet long standing is the more fatiguing. The fatigue of long standing is relieved by walking, but if the passive attitude of standing, or an approximation to it, is still used in walking, the foot is subjected to constant and unrelieved strain.
Fig. 4.

The relation of the astragalus to the os calcis.
Fig. 5.

The relation of the astragalus to the os calcis in flat-foot.
As an illustration of the protection afforded by muscular activity, the gait of one who walks properly should be noticed. The foot is advanced almost in the line of the walk, with but slight eversion, so that the weight, falling momentarily on the heel, follows the outer or strong side of the foot around to the great toe. As the leg is extended the body is raised on the foot, and as its outer border, from the heel to the head of the fifth metatarsal bone, is shorter than the corresponding inner border, the forefoot is mechanically or involuntarily turned in or adducted, so that the weight is thrown off to the outer side at the moment of greatest strain. At the same time the muscles passing behind the inner malleolus, working to advantage, give the final push or spring to the step. The gait is elastic and graceful. There is the proper alternation of attitudes, for at every step the foot assumes the posture most opposed to passive weight-bearing and flat-foot, and at every step there is active exercise of the muscles that protect the foot (Fig. 6).
Fig. 6.

Illustrating the involuntary adduction of the right forefoot in the proper attitude.
Let this be contrasted with the slouchy, cloddy, ungraceful, jarring walk of the weak-footed or flat-footed person, in which the everted foot is lifted and set down as a lifeless mass, its normal motion replaced by exaggerated flexion of the knee, the leg never completely extended, the weight borne on the heel, the strain falling on the weakest part of the foot, and the loss of the function of leverage and the use of passive attitudes in work that demands muscular activity will have been sufficiently illustrated.
In the developed deformity, normal use of the foot is, of course, impossible, and inherent weakness of structure or other cause may make the improper attitude necessary, but just as the deformity or the weakness induces the gait and attitude, so the assumption of the improper attitude, whether by inclination or force of circumstances, may lead to and aggravate weakness and deformity (Fig. 7). The facts that such attitudes are unnecessarily assumed through ignorance or want of training, and that the weak foot may be protected in its weakness by the voluntary avoidance of postures that place it at a disadvantage, are of the greatest importance in treatment.
Fig. 7.

The improper attitude of eversion of the feet.
The safeguards of the foot are muscular activity, perfect freedom of painless motion, and normal alternations of attitude. On looking at the foot as a familiar machine, some of the common causes of limitation of its activity, its leverage, and balance will be very evident. The custom of cramping the toes in tight shoes and perching the foot on an insecure heel is certainly not conducive to the well-being of the machine.
Both the great and little toes are provided with special muscles to aid in balancing the weight, and the great toe is also a powerful brace to the arch and an aid in the work of leverage. Yet the muscles are often atrophied by disuse and the toes are distorted by compression, while the incidental corns and bunions make active motion of the foot painful, and it is avoided by assuming the passive attitude of eversion or by disuse of the active lift of the calf-muscles.
The joints of the foot may be weakened by the local effects of gout or rheumatism, or sprains or similar diseases or injuries, and the improper use of the foot necessary during the stage of actual disease or weakness may persist, either as a habit or because of more or less disturbance of structure, after the cure or subsidence of the original cause.
Distortions of the leg or fractures about the ankle may displace the weight of the body to the disadvantage of the foot, or the arch may be directly broken down, as in falls.
The foot may be overworked, as in occupations that require long standing, like those of bakers, barbers, grocers, and the like, or overweighted by the burdens put upon it.
As the foot is the mechanism subjected to the greatest strain, it is usually the first to show the effect of weakness on the resumption of work after acute or chronic disease or during childbearing.
Predisposing causes are often apparent in childhood, in general weakness and relaxation of tissues, in the inherited vulnerability and predisposition to postural deformities with which flat-foot may be associated. Weakness due to rhachitis or other forms of defective assimilation may prevent the proper use of the foot, or the weakness or deformity may be congenital. At a later period improper attitudes are common, and may even be the result of instruction, such as that of turning out the feet, a posture that interferes with effective leverage and induces an awkward, jarring walk.
The foot may be unbalanced by paralysis of certain muscles, and flat-foot may be one of the resulting deformities; but, as in such cases the cause is obvious and the prognosis and treatment are quite different, the subject does not properly come within the scope of this paper. In certain exceptional instances, however, the foot may be weakened by muscular inequalities whose cause is more obscure; but, as a rule, such cases yield very readily to proper treatment.
In estimating the relative ability of a foot from the mechanical standpoint, it will be evident that valgus must be a source of weakness, because the weight of the body is improperly distributed on the foot; that abduction is a source of weakness, because the strain of the calf muscles tends to bend the foot laterally; and that a low arch may be a source of weakness, because the lax ligaments do not hold the joints properly. These three elements combined in varying degree make up the typical flat-foot deformity, but they are by no means always combined. Valgus may accompany an exaggerated arch, and valgus with abduction is the condition often found in the so-called chronic sprain of the ankle.
Restriction of motion and improper attitudes, whether voluntary, the result of habit, or involuntary, because of pain or weakness or permanent change in any of the structures that make up the foot, are sources of weakness, because they prevent the proper alternation of attitudes. All the elements of weakness may be found in developed flat-foot, and they must be overcome before it can be cured. Any of the elements of weakness may cause symptoms of disability, and ultimately lead to deformity.
It must be very evident that the foot may be abused and deformed, and yet be able to perform its work; the predisposing causes of weakness are present, yet because little is required of the mechanism it is still efficient. It needs, however, but temporary weakness or slight injury or overwork to give the impulse, and the foot breaks down. Thus symptoms of the weak or flat-foot may develop at any age, in the robust as well as in the anaemic individual, and it is thus explained why the very evident weak and flat-foot of childhood often causes no symptoms until the period of rapid growth and increased weight of adolescence, or later, when the life-occupation is begun.
The term “flat-foot,” as it is generally understood, is inadequate and misleading, in that it directs attention to a minor element of weakness and a secondary element of the deformity; for the symptoms of flat-foot do not result because the foot is flat, but because it is becoming flat; they are the symptoms of the strain upon the weak foot and of the injuries and changes accompanying a progressive dislocation. The mere depth of the arch, which varies in different races and individuals, is of small importance. An unarched foot is not graceful in outline, and it is not usually powerful as a lever, but if it is an inherited peculiarity, or if the arch has never developed, or if the acquired deformity even is no longer progressive, the individual does not, as a rule, suffer discomfort; while the normal foot, beginning to give way in abduction and valgus, may cause disabling pain before the imprint of the sole shows the slightest flattening of the arch.
The term “weak-foot” has been adopted because it implies loss of function rather than deformity, for, although the so-called flat-foot is always a weak foot, yet a weak foot is by no means necessarily a flat-foot. The term is here used in its broader sense, to include not only the deformed foot, but the various elements of weakness and deformity which may cause symptoms similar to, and ultimately lead to, flat-foot, of which the symptoms and the deformity may be regarded as the result of a disproportion between the work to be performed and the ability of the supporting structures.
This theory of disproportionate work, which includes such a variety of predisposing and exciting causes that may weaken the mechanism on the one side or overburden it on the other, has been explained at length because of the conflicting and confusing hypotheses to be found in text-books and elsewhere, in which the effects of deformity have been mistaken for the causes, or in which a contributing or exciting factor in a special class of cases has been alleged as the primary and important element of all cases; and because the treatment to be described is conducted on the principle that the foot is a human machine that may be protected in the exercise of its functions by a knowledge of its mechanism.
If it is weak or disabled, the cause of the weakness, whether it lies primarily in the muscles or in the other component parts, may be made clear by comparing the disabled member with the normal standard. Once the cause is discovered and the obstructions to normal use are removed, the weak foot may be protected in its weakness and become a strong foot, although the conditions still exist under which it originally broke down.
The symptoms of the weak foot, though similar in type, vary in severity according to the local condition and disturbance of function, the work to be performed, and the susceptibility of the patient.
The earliest symptom is usually a sensation of weakness; the patient begins to recognize as familiar a feeling of discomfort, of tire and strain about the inner side of the foot and ankle; sometimes, after long standing, a dull ache in the calf of the leg, or after overexertion a momentary sharp pain radiating from the point of weakness; thus the patient often dates the history of his trouble from a long walk. After a time the patient may become aware that he is accommodating his habits to his feet; he rides when he once walked, he sits when he once stood, he no longer runs up or down stairs or jumps off the street car. His feet have lost their spring, as he expresses it, which means that the foot is no longer supported and controlled by muscular activity, and is no longer used as a lever. Not infrequently, early symptoms are pain and tenderness at the centre of the heel, explained in part by the jarring heel-walk which is always assumed when the foot is weak, and in part by the strain upon the attachments of the deep plantar ligaments. The patient may complain that he cannot buy comfortable shoes; the reason is, that the weak foot under use is changed in shape, so that the shoe which was comfortable in the morning compresses the foot painfully at night, thus increasing discomfort from corns, bunions, painful great-toe joints, and deformities of the toes, is experienced. Coldness and numbness and increased perspiration, caused by the impaired circulation and weakness, are common symptoms in this class of cases.
Actual pain is, as a rule, felt only when the foot is in use; it ceases under temporary rest or relief from disproportionate work, and it is this remittence of symptoms, together with the fact that the discomfort is often more marked in damp weather, that leads to the mistaken diagnosis of rheumatism. The foot remains, however, weak and vulnerable; the patient recognizes the fact that he has what he speaks of as a weak ankle, or sprain, or gout, or rheumatism, but, as he has accommodated himself to the weakness, little discomfort is experienced.
In many instances such relief or accommodation is impossible, and it is therefore among the working class that one oftener sees the frank and rapid development of the disability and deformity. The range of motion becomes more and more restricted; the habitual attitude, at first exaggerated to deformity only under the influence of the weight of the body, remains as a permanent displacement of the bones. The weak and dislocated foot is subjected to constant injury, to what may be likened to a succession of slight sprains, so that local congestion and tenderness appear, and consequent muscular spasm and rigidity.
Because of this rigidity of the foot, which has lost the power to accommodate itself to inequalities of the surface, the patient dreads to cross a rough pavement, for every misstep is a source of pain. Another symptom which is usually present in slight degree at every stage now becomes more prominent, the discomfort felt in changing from a position of rest to activity. The patient, after sitting or on rising in the morning, is unable to walk, but staggers and limps for several minutes, a symptom explained by the fact that when the foot is at rest there is a partial reposition of the displaced bones, which must again be forced into the deformed posture that has become habitual.
The local tenderness and muscular spasm are increased by use, so that the patient may have difficulty in removing the shoes at night, and the symptoms relieved by the rest of Sunday become progressively worse during the week; the pain and discomfort are more general in character, and are often referred to the dorsum of the foot, representing muscular rigidity and tension, and to the outer side of the ankle, where the external malleolus is grinding out a facet in the projecting os calcis. The patient may now complain of discomfort in the feet and cramps in the legs, even when in bed, and the appearance of weakness, awkwardness, and depression of spirits may be so noticeable that the case is sometimes mistaken for one of incurable nervous disease.
One can hardly exaggerate the pitiable condition to which the sufferer from painful flat-foot may be reduced. There is something peculiarly exasperating and depressing in an affection which prevents a person otherwise in perfect health from earning his living; and the duration of the symptoms, the mistakes in diagnosis, the ineffectiveness of treatment and the apparent hopelessness of relief, combined, have a very evident effect upon the mental and moral, as well as the physical condition of the patient. It is in this class that a definite promise of relief and probability of cure in a definite time is the best and most necessary of tonics.
If these facts are taken into consideration, that the inherited flat-foot, or that acquired in early life, or the complete flat-foot of long duration, or the weak foot to which the individual has accommodated himself, may cause no actual discomfort or pain—in other words, that there is no definite relation between the degree of deformity and the severity of the symptoms—one of the most important stumbling-blocks in the way of a proper apprehension of the true nature of the disability and its effective treatment will have been removed.
One must also rid one’s mind of the notion that the weak and flat-foot is a necessary sign of degeneration, to be found only among the weak-fibred and ill-nourished. The predisposition to deformity and the weak foot in its slighter grades are perhaps as common in the well-born and well-fed as among the traditional “mill girls.” The development of the deformity, the exchange of discomfort for disability, the inherited or acquired predisposition existing, will naturally be more frequent, more rapid, and more marked among those who are obliged to use the feet constantly than among those who are not.
In all cases of weakness of the foot, a thorough and orderly examination should be made of its functional ability and use, not only for the purpose of diagnosis, but in order that the amount and character of the temporary or permanent changes in structure may be estimated. One begins the examination by noting the manner of standing and walking. The heel-walk, the exaggerated eversion of the feet, the slouchy gait, in which the leg is never completely extended, in which the power of the calf muscles is not applied, and in which the essential postures of the foot are disused, are all elements of weakness, and should be corrected whether they cause symptoms or not. The distribution of the weight of the body and the habitual use of the foot are often made evident by examining the worn shoe. If it is bulged inward at the arch or worn away on the inner side of the sole it shows weakness.
Fig. 8.
Voluntary dorsal flexion.
The same observations are then made on the bare feet, particular attention being paid to the line of strain or leverage : thus, a line drawn down the crest of the tibia from the centre of the patella, continued over the foot, should meet the interval between the second and third toes; if it falls over or inside the great toe, it shows that the foot is working at a disadvantage. The contour of the foot should then be examined; its internal border should curve slightly outward, so that if the feet are placed side by side, with the toes and heels in apposition, a slight interval remains between them; if this slight concavity is replaced by a noticeable convexity when weight is borne, the foot is weak. This change in contour is often the earliest and sometimes the only evidence of deformity. The arch of the foot, properly protected by the muscles and by a proper attitude, sinks but slightly under weight; there is a slight elasticity only, and if the depression is marked it shows laxity of ligaments and weakness. The exact amount of bearing surface may be demonstrated by an imprint of the sole in a manner to be presently described.
Fig. 9.
Voluntary plantar flexion.
The balance of the foot as shown by the range of motion is next to be tested, for its limitation is one of the earliest signs of improper attitudes and weakness. This range of motion varies somewhat within normal limits; it is usually greater in childhood than in adult life, greater in the slender than in the massive foot, and greater in the foot used properly than in the foot that is not. The first test is applied to simple dorsal and plantar flexion; the leg must be fully extended at the knee; the line of strain must be in its normal relation, so that the foot may be neither adducted nor abducted, and the observation must be made on its outer border. In this position, the patient should be able to flex the foot well beyond a right angle, from ten to twenty degrees. Voluntary extension can be made to about one hundred and thirty or one hundred and forty degrees, the range of motion being from fifty to seventy degrees.
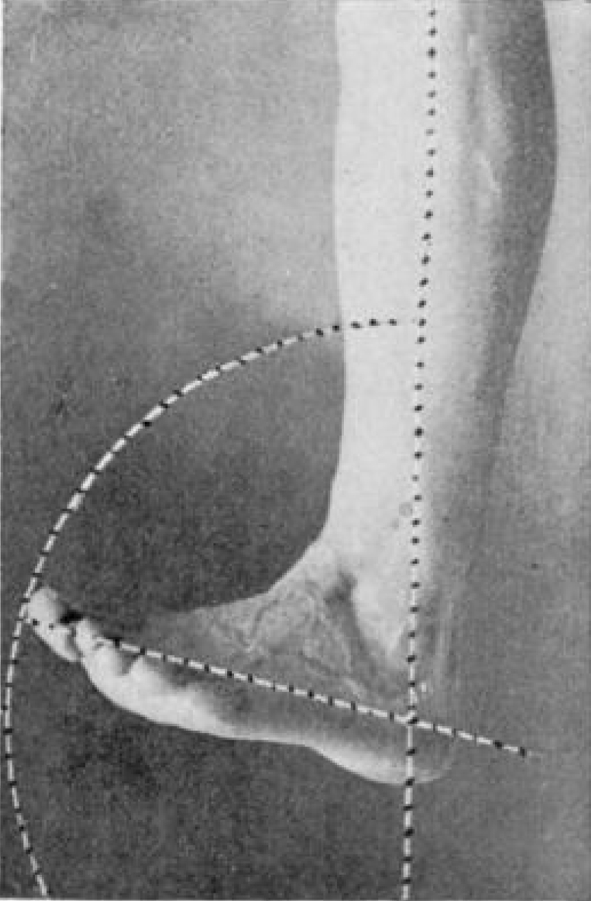
By far the most important test is that of the power of adduction or inversion of the foot, the test of the medio-tarsal and sub-astragaloid joints, because in this motion the os calcis is drawn forward and inward under the astragalus, while the forefoot is flexed about its head. With the leg extended and the patella pointing forward, the foot is turned in as far as possible; the elevation of its inner border, or supination, and the turning in of the heel are well illustrated in the photograph (Fig. 10); the actual adduction is some-what difficult to measure, but it is about thirty degrees. Even the mild and early cases of weak-foot usually show some limitation of this most important motion, and in many instances it is completely lost, the patient turning the entire leg in the effort to adduct the foot. The less important motion of abduction is also shown (Fig. 11). Its range is somewhat less than that of adduction.1 The range of passive motion is then tested by pushing the foot in all directions. The range of dorsal flexion is from five to ten degrees beyond that of voluntary motion, while passive extension, so far as it applies to the ankle-joint, is about the same as the voluntary, although the forefoot may still be further bent downward at the medio-tarsal joint. The limit of passive adduction is considerably beyond that of voluntary inversion.
Fig. 10.
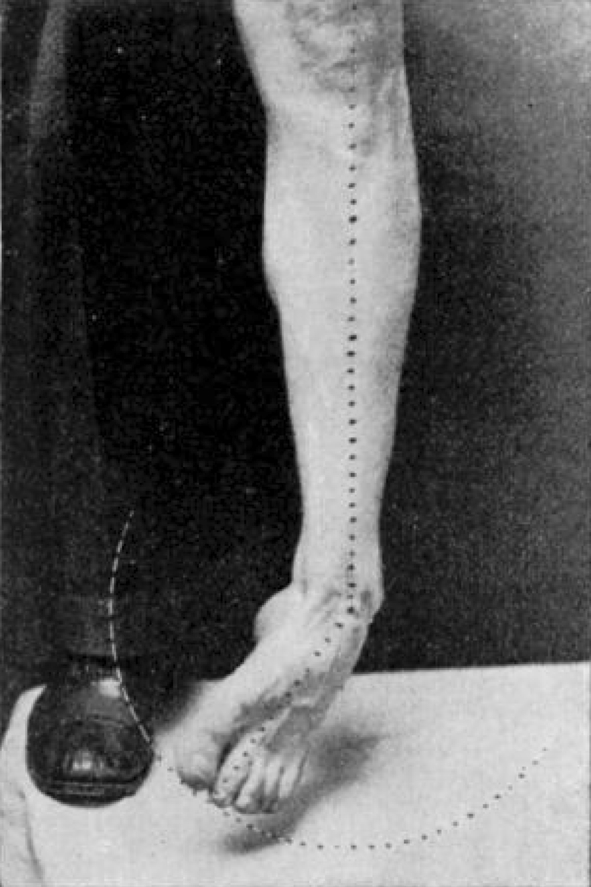
Voluntary adduction.
Fig. 11.
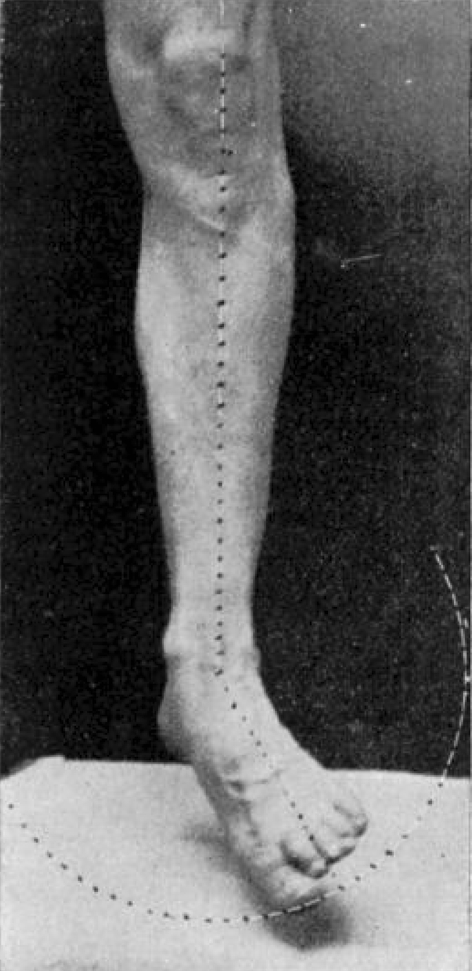
Voluntary abduction.
Passive motion serves several purposes; contrasted with the range of voluntary motion, it shows the habitual use of the foot, since the motion least used is most limited; it brings out the slight restrictions of motion and the presence of local tenderness, which, even in early cases, are usually present. Thus, if pressure is made just in front of and below the internal malleolus at the astragalo-scaphoid junction, and at the same time the foot is quickly inverted, the patient will notice the painful pressure-point and a feeling of constriction and tension about the dorsum of the foot before the normal limit of motion is reached. As the foot is dorsally flexed the plantar fascia is put upon the stretch, and its condition may be noted, for a contracted and sensitive plantar fascia may cause symptoms of disability that induce or are combined with abduction and valgus.
In other words, this mode of examination makes evident the amount of disability and permanent change in the machine which must be overcome before a cure can be accomplished. By it one will recognize several grades of weak-foot:
The normal foot improperly used, as shown by the method of standing and walking.
The foot in which the range of voluntary motion is restricted, showing disuse of function, and in which the elements of deformity are apparent when weight is borne.
That in which the passive range of motion is restricted, or in which there are evident weakness and deformity. This limitation of motion depends, as a rule, on the accommodative changes in structure to the habitual postures or to the deformity. These changes are first evident in the muscles and ligaments and finally in the articular surfaces of the bones. Added to this underlying limitation of motion there is always a varying degree of muscular spasm, dependent upon the local irritation and injury.
There can be no doubt that the origin of the weak foot may in many instances be traced to early childhood. Certainly deformities and improper attitudes are very common at this period, and it is much more likely that they are ingrown than outgrown. Actual pain from the weak foot is rare at this age. The child may complain of fatigue and may be weak and awkward, but it is usually because of the very evident deformity rather than because of symptoms that advice is asked. In these cases, as in every case, the habitual attitudes and use of the feet are of the first importance.
One of the most frequent of the improper postures is that of exaggerated eversion of the feet, which is not only an ungraceful attitude, but a direct cause of weakness. The opposite attitude of inversion of the feet, the so-called “pigeon-toed” walk, is most offensive to relatives and friends, and it is for the correction of the attitude that the child may be brought for treatment. This attitude is in many instances a sign of the weak foot, for, on examination, the bulging on the inner side, the inversion of the leg in its relation to the foot, and the flattened arch, show very plainly that it is the foot and not the attitude that requires treatment, and that the attitude is in this class of cases really a safeguard against increasing deformity, which will correct itself when its cause is removed. Particular emphasis is laid upon this point, which is very generally overlooked, because the routine treatment of the pigeon-toes in these cases might be the cause of direct harm.
“Weak ankle” is a term popularly applied to the weak foot of childhood, in which the shoe is worn away on its inner side. In these cases the foot is in a position of valgus when in use. Weak ankles are common in very young children, and are often caused by defective assimilation. At this age the foot is, in addition, usually flat; but in the valgus or weak ankle of later years the arch is often normal in outline.
Prominent or “outgrown joints” often attract the mother’s attention; the internal malleoli appear prominent because of the position of the valgus, or because of the eversion of the feet the malleoli may strike against one another, “interfere,” and thus there may be an actual hypertrophy from local irritation.
Another type is the long, slender foot of adolescence, in which the scaphoid may be hypertrophied because of the strain and pressure put upon it by the improper attitudes; its position is often shown by the point of wear in the leather of the shoe. In the weak foot of childhood, although marked restriction of voluntary and passive motion may be present, there are, as a rule, but little local tenderness and muscular spasm, and, as has been said, but little actual pain, thus differing greatly from the adult type.
The principles of the treatment which leads to the permanent cure of the weak foot and flat-foot are very simple, but their application varies somewhat according to the grade and duration of the deformity. The object of treatment is to change the weak foot, not only in contour, but in habitual attitudes and in power of voluntary motion to those of the normal foot, because a cure is impossible until function is regained. The first step must therefore be to make passive motion free and painless to the normal limit, for the obstructions to the motion of the machine must be removed before the power can be properly applied. The increase of muscular strength and ability on which ultimate cure depends is not possible while motion is restrained by deformity or pain or by adhesions or contractions.
The weak foot, because of inefficient ligaments and muscles, unable to hold itself in proper position, must in many instances be supported until regenerative changes have taken place in its structure. Such support is necessary to retain the joints in proper position, otherwise normal motion is impossible, and to hold the weight in its proper relation to the heel and the strain in its normal relation to the foot.
When these essentials are provided the patient may cure himself by the proper functional use of the foot and by an avoidance of attitudes that place it at a disadvantage.
It may be well to describe, first, the treatment that must be applied to all classes of weak foot in which a cure is to be attempted, and which by itself is sufficient in the milder types, before calling attention to the modifications that may be necessary in special cases.
In practically all cases it will be necessary to provide the patient with a proper shoe, for the shoe is usually directly the cause of the minor deformities, and indirectly, in many instances, of more serious disability.
The proper shoe should contain sufficient space for the independent movements of the toes. This motion is illustrated in the walk of the barefoot child. As the weight falls on the foot the toes expand, and as the body is raised on the foot they contract. The important leverage action of the great toe and the support afforded the arch of the foot by it have already been mentioned.
The ordinary shoe often cramps the toes into a distorted mass, so that independent motion is quite impossible. The sole of the shoe should be a protection and a support to the foot; the sole of the ordinary shoe is neither, and is of such shape that distortion of the toes is inevitable. A very good demonstration of a proper sole may be made as follows : The bottom of a normal foot is smeared with vaseline, and an imprint made on a sheet of white paper. As the weight is borne, the outline of the foot is traced with a pencil; the imprint will show the weight-bearing portion of the foot, the outline its actual size. The sole of the shoe should at least be wide enough to support the entire imprint, and ought to be sufficiently wide to include the entire outline of the foot. The ludicrous disproportion between the size, width, and shape of the ordinary woman’s shoe and the imprint and tracing of the foot is often a very convincing argument in favor of a change.
If the imprint of a normal foot is made, the tracing of its outline will correspond to a slightly exaggerated waukenphast last, practically straight on the inner side, so that slight lateral motion of the great toe is allowed. There can be but one proper shape for the shoe—that which corresponds to the outline of the undistorted foot. It is not, therefore, a question of square or pointed toes, or so-called common-sense shoes, but the simple relation of the sole to the shape of the foot (Fig. 12). The wider the sole and the heel, the greater will be the stability and security afforded the weak foot as contrasted with the narrow sole and high heel.
Fig. 12.

The proper relation of the sole to the shape of the foot. A, outline of sole; B, outline of foot; C, imprint of foot.
The prevention of distorted toes and the discomfort of the abused foot is a matter of great importance in childhood. It should be insisted that the sole of the shoe be of such shape and width as to allow of independent movement of the toes. Unfortunately, little children are often seen wearing shoes of the shape usually assumed at years of discretion. In this regard girls suffer more than boys, as women do more than men. The girl who may have worn comparatively harmless shoes until the age of ten years or thereabouts changes suddenly to the high heel and narrow sole, and the process of distortion begins, the amount of distortion and the degree of discomfort depending on the amount of work required of the foot. Wide soles and no heels should be worn as long as possible by children because of the greater security and because the high heel limits the necessity for, and therefore the use of, the entire range of motion of the foot and ankle.
A simple expedient in the treatment of the weak foot, and an aid in balancing it properly, is to raise the sole and heel of the shoe slightly on the inner side to simulate the wearing away on the outer side, as in the use of the normal foot. This aids in overcoming the valgus, and is of special importance in the treatment of the weak foot of childhood.
When the patient stands properly balanced in the proper shoe his attention is called to the three elements of weakness. He is instructed to guard against valgus by throwing the weight on the outer side of the heel; to guard against abduction by keeping the toes almost straight in front of the body; the significance of the bulging on the inner side of the foot is pointed out to him; that he must prevent this by aiding the arch by the power of the great toe, as already illustrated. The importance of leverage is shown him, that he must try to feel the sole of the shoe with his toes, and the active lift of the calf muscles by fully extending the leg and raising the body on the foot from time to time; that he must avoid long continuance in one position, especially the passive posture, which simulates the attitude and deformity of flat-foot. In short, he is instructed in the mechanics of the foot and its voluntary protection.
Although the proper walk is the best of exercises, it is important to show the patient the normal range of motion in all directions and let him endeavor to reach it by voluntary exercises. Raising the body on the toes, first on both feet, finally on one foot, for from twenty to a hundred times, is a very good exercise for the foot and for the calf. In many instances this very simple treatment is all that is necessary, and the symptoms of strain and tire completely disappear, but in cases of more severity the patient is not able to prevent deformity voluntarily, consequently a support is necessary to hold the foot in proper position and to relieve discomfort. It is usually necessary in the weak and flat-foot of childhood, because one cannot command the aid of the patient.
In applying a support to the weak foot the nature of the deformity that is to be prevented must be borne in mind : that the flat-foot, for example, is not a direct breaking down of the arch, as is usually taught, but a lateral deviation and sinking—a compound deformity, as has been already described—so that a brace, to be efficient, must hold the foot laterally as well as support the arch. At the same time it should not prevent the normal motions of the foot, and thus interfere with the increase of muscular strength and ability, on which ultimate cure depends. The supports that have been ordinarily used for flat-foot do not fulfil the conditions; the pads and springs placed beneath the arch are intended to support it by direct pressure, without regard to the valgus or the abduction; they are usually ill-fitting and often of such length and shape as to splint the foot and thus prevent its motion. Leg-braces which control the valgus do not often accurately hold the foot, and their weight and unsightliness are fatal objections to their use in the early cases, in which prevention of subsequent deformity is of such importance. No brace should be applied to a deformed and rigid foot, because it is unable to shape itself to the support; the spasm and rigidity must first be relieved by preliminary treatment, as will presently be described.
The brace that has been used by me for nearly ten years was designed to meet the conditions which have been mentioned, and, notwithstanding the time and care necessary for its application, it has come into very general use here and elsewhere. On the theory that a perfect fit is essential in a brace, it has always been insisted that a plaster cast of the corrected foot should be taken in every case. Casts may be easily and quickly made in the following manner : Seat the patient in a chair; in front of him place another chair of equal height; on it lay a thick pad of cotton batting and cover it with a square of cotton cloth. Put about a quart of cold water into a basin and sprinkle plaster-of-Paris on the surface until it does not readily sink to the bottom; then stir. When the mixture is of the consistence of very thick cream pour it upon the cloth. The patient’s knee is then flexed, and the outer side of the foot, previously smeared lightly with vaseline, is allowed to sink into the plaster, and, the borders of the cloth being raised, the plaster is pressed against the foot until rather more than half is covered. The foot should be at a right angle with the leg and in its normal relation to it, the sole being absolutely level with the leg, at a right angle to the floor. As soon as the plaster is hard its upper surface is coated with vaseline and the remainder of the foot covered with plaster; the two halves are then removed, smeared lightly with vaseline, and bandaged together. The interior is dampened with soapsuds and is then filled with the plaster cream. In a few moments the plaster shell may be removed, and one has a reproduction of the foot, which, when properly made, should stand upright, without inclination to one side or the other. In many instances it will be of advantage to deepen the inner and outer arches of the cast, in order that the arch may be slightly exaggerated, especially at the heel, so that the depression and inversion of the anterior extremity of the os calcis may be prevented. This model should be reproduced in iron for an anvil, upon which the brace, cut of the best sheet steel, 18 to 20 gauge, as illustrated in the diagrams, is moulded and tempered, so that as it is applied for the purpose of preventing deformity it may be practically unyielding to the weight of the body.
It will be noticed that the brace clasps the weak part of the foot and holds it together; the broad internal upright portion covers and protects the astragalo-scaphoid junction (Fig. 13), rising well above the scaphoid; the external arm covers the calcaneocuboid junction (Fig. 14) and the outer aspect of the foot to a height sufficient to hold the foot securely; the lower portion provides a firm, comfortable support for the sole, yet, reaching only from the centre of the heel to the head of the metatarsal bone of the great toe, it does not restrain the normal motions of the foot (Fig. 15).
Fig. 13.

A, the astragalo-scaphoid joint.
Fig. 14.

B, the calcaneocuboid junction.
Fig. 15.

C, the great-toe joint; D, the centre of the heel.
This brace may be nickel-plated and japanned, which makes the smoother finish, or tin-plated, or galvanized, or covered with hard rubber, which is much more durable, as rusting is prevented. It may be covered with leather, or an inner sole may be placed on its upper surface; but this is not usually necessary. As it is fitted to the foot, it finds and holds its own place in the shoe so that no attachment is necessary; it may be changed from one shoe to another, and its presence in the shoe is not evident.
Not only does it hold the foot laterally and from beneath, but there is an element of suggestiveness in the slight leverage action which is very important. The patient, instructed to throw his weight upon the outer side of the foot, presses down the external arm, and this tightens the internal flange against the inner side of the foot, so that he instinctively draws in the weak part of the foot away from the pressure or into the normal contour; he no longer everts the foot in walking, and he is not likely to assume the passive attitude, because of the suggestive lateral pressure of the support. The shape of the brace, in general like that of the diagram, is modified in certain cases; for instance, the entire internal aspect of the foot may be weak and must be covered by the internal flange. In very heavy subjects the sole portion must be made larger, or other slight modifications may be necessary. If any portion of the rim of the plate causes discomfort, the edge may be turned away slightly at the point of pressure by a wrench. After a few days the patient no longer notices the presence of the brace, and as it does not show, it may be worn indefinitely. It is usually necessary for from three months to a year or longer, according to the condition of the patient and the use to which his feet are put. The brace, properly made and adjusted under the proper conditions, causes no more pressure or discomfort than a well-made shoe, for its principle is quite different from that of the pads that are in common use, to which this objection has been made; the brace should afford support when necessary, and at all times suggest a proper attitude; it is, however, but one of the essential factors in a general scheme of treatment.
In the treatment of children the passive movements of the foot should be carried out to the full limit at morning and night, until the child has regained the ability to perform them voluntarily. Special gymnastics and massage are always of service, and may be necessary in certain cases. Bicycling may be cited as one of the best, and roller-skating as one of the worst, exercises for the weak foot. A year is about the time required for a cure of the weak foot in childhood, although attention to the shoes and the attitudes must be kept up indefinitely.
One may now contrast with the mild types of weakness that have been described, those cases of extreme deformity in which the symptoms are disabling and in which the foot is rigidly held in the deformed position by muscular spasm. Such cases, often considered hopeless as regards a cure or even relief, are in reality the most satisfactory, and in no other type of painful deformity can so much be accomplished by rational treatment as in this class.
The deformity must be considered as a dislocation, in which the astragalus has slipped downward and inward from off the os calcis, which in turn is tipped downward and inward and into a position of valgus.
The remainder of the foot is turned outward, so that the relation of the leg and the forefoot is entirely changed; in fact, the forefoot is almost entirely disused. With the deformity one finds, it may be local periostitis, new facets in the bones, active and passive congestion, and the like.
The amount of permanent change in the bones and in the sense of irremediable deformity has been greatly exaggerated by the few post-mortem examinations that have been recorded, for by far the greater number of patients are young adults in whom the extreme deformity is of comparatively short duration and in whom complete cure is possible.
The problem in treatment, therefore, is first to replace the dislocation and to remove all the obstructions to free, passive motion, to rest the injured and congested tissues, and to relieve the sufferer from the continuous and debilitating pain. The patient is etherized and, the muscular spasm being completely relaxed, one may estimate the amount of restriction of the range of motion. Of this, muscular spasm makes about half; the aim now is to remove this residual obstruction to motion in every direction, and finally to place the foot in the attitude most opposed to that which has been habitual. This is the object of forcible overcorrection as the first step in the systematic repair of the disabled mechanism; its principle must not be confounded with forcible correction carried out with the object of remoulding the arch of the foot, or in which the simple correction of the deformity is the object in view.
One first extends the foot forcibly, then flexes it to the normal limit, then abducts and adducts, the various motions being carried out over and over until the rigid foot has become perfectly flexible; it is often necessary to allow the patient’s leg to hang over the table, so that the foot may be taken between the knees, in order to supply the required force by the thigh muscles. These motions are accompanied by the audible breaking of adhesions and the complete disappearance of the deformity.
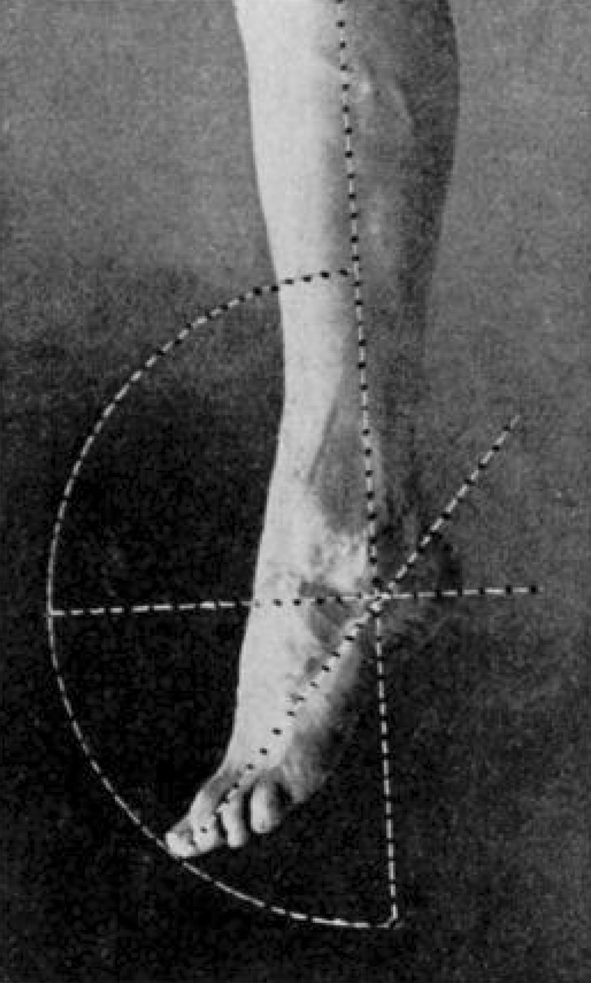
In a certain number of cases it will be necessary to divide the tendo-Achillis—when, for example, the range of dorsal flexion remains limited in spite of vigorous stretching, or when there has been very great pain and tenderness at the medio-tarsal joint, and it is desired to remove the strain of the calf muscle completely. Traumatic cases come especially under this head. This tenotomy has one great advantage, that it lengthens the course of treatment and gives the patient the benefit of a longer rest and opportunity for after-treatment. When the passive range of motion has been regained the foot is turned downward, then inward and upward into the position of extreme equino-varus, an exaggeration of the attitude of adduction, as shown in Fig. 10. By this manipulation the os calcis is drawn under the astragalus and thrown into an everted position, and the scaphoid is flexed about and under the head of the astragalus, which is then lifted to the limit of normal flexion (Figs. 15 and 16). The attempt is always made to bring the extreme outer border of the inverted foot up to a right angle with the leg, which is the limit of normal forced flexion in this attitude. The foot, thickly padded with absorbent cotton, is then fixed in this club-foot position by plaster-of-Paris bandages.
Fig. 17.

The overcorrected foot, with the reversal of the lines of displacement.
Fig. 16.

Flat-foot before operation. A, the projection of the displaced astragalus and scaphold; B, the inner malleolus; C, the medio-tarsal joint, showing the outward displacement before, the inward rotation behind, this point.
Surprisingly little discomfort, considering the force that it is sometimes necessary to apply, is experienced after the operation. The familiar and often intense pain from which the patient has suffered so long is entirely relieved by the correction of the deformity; there is often a sense of tension about the outer side of the ankle and dorsum of the foot; but this is not, as a rule, of long duration. As soon as possible, often on the following day, the patient is encouraged to stand and walk, bearing his weight on the foot. Walking serves two purposes—to still further overcorrect the deformity and to accustom the patient to a posture entirely different from that so long assumed.
Meanwhile the contracted tissues on the outer side become thoroughly overstretched, the weakened ligaments and muscles on the inner side are allowed to contract, and the local irritation rapidly subsides under the rest from the constant injury to which the foot has been subjected.
The patient is not confined to the bed or house; if both feet are in plaster bandages, crutches are of course necessary. The time that the feet should remain in the overcorrected position depends upon the duration of the deformity and the severity of symptoms; this is from one to six weeks, the usual time being about three weeks.
At the end of two weeks, or whenever the patient can support the weight on the plaster bandage without a sensation of discomfort, it is removed, the foot placed in the proper position, and a cast taken for the brace. Immediately after this is done, the foot is returned to the club-foot position and the plaster bandage reapplied. When the brace is ready, the plaster bandage is finally removed; the foot is now in good position, and in many instances the arch is exaggerated in depth.
For the first few days, prolonged soaking in hot water, with subsequent massage at intervals during the day, will be found useful in overcoming the swelling and local tenderness that may remain. It is always insisted that a new shoe of the waukenphast pattern shall be obtained, the sole and heel of which are raised a quarter of an inch on the inner side, to aid in the balancing of the weak foot; the brace is then applied, and the patient is never allowed to walk without its support. When the shoe is removed he is instructed to walk on the outer side of the foot or the toes until the foot again becomes strong; in other words, the deformity is never allowed to recur.
The systematic treatment is then begun by the surgeon and patient, the first essential being the attainment of free and painless passive motion in all directions. These motions, which have been so long restrained by deformity, cannot be regained without effort, and during this stage the treatment must be carried out by the surgeon himself; if he trusts to the patient or his friends, a cure is out of the question. At least once a day the full range of motion must be carried out to the normal limit.
Three motions—abduction, flexion, and extension—are usually free and painless; but the fourth, that of adduction, is almost invariably resisted by the same quality of muscular rigidity that was present before the operation. By far the most effective method of overcoming this resistance is conducted as follows: The patient is seated in a chair and the surgeon stands in front of him. Let us suppose that the left foot is to be adducted, or, as the patients express it, twisted. The surgeon places the foot between his knees; his left hand encircles the heel, the fingers grasping the projecting os calcis and tendo-Achillis; the ball of the palm lies against the medio-tarsal joint on the inner aspect of the foot; the right hand grasps the outer side of the forefoot and toes; then, by steady pressure of the thigh muscles, the forefoot is forced downward and inward over the fulcrum formed by the projecting palm which lies upon the left knee, the fingers holding the heel steadily in place. This inward twisting is at first resisted by a mixed voluntary and involuntary muscular spasm, which gradually gives way under steady pressure. When the limit of adduction has been reached the foot is firmly held until all pain has subsided, when the patient is instructed to make voluntary movements while the foot is in the corrected position, flexion and extension of the toes, and to contract the flexor muscles of the foot. Finally the patient attempts to adduct the foot, the surgeon supplying the power, which in all cases of this type has been completely lost.
This passive manipulation from time to time to the extreme limit of normal adduction is necessary until there is no longer any sensation of pain or tension, for as long as there is the slightest spasm or painful restriction so long is the voluntary motion limited, cure delayed, and relapse of deformity probable.
During active treatment the patient by the use of massage, active and passive motion, is constantly working to one end—namely, to regain the lost power of voluntary adduction.
The time necessary to rest the feet, to overcome the local inflammation and muscular spasm, and to regain, in part at least, the range of passive motion, to place the patient in the same position as regards a cure as that of the milder type of deformity, is from three to six weeks.
Usually the patients are told that a month will be necessary, and that at the end of that time they may return to work, free from pain and from the danger of relapse, and that the feet will constantly grow stronger under the work which was before too great for their strength. The time necessary to re-educate the adductor muscles in their proper function depends in great degree upon the intelligence and persistence of the patient. Although in after-treatment massage and special exercises are of benefit, the essentials are very simple; they are an effective brace, a proper shoe, and the passive manipulation which has been described until its object has been attained; the proper walk, the best and easiest of exercises; and, lastly, to force into the patient’s understanding the method of protecting the weak foot by the alternation of strain and by proper postures.
There are other cases in which the deformity of flat-foot is complicated by rheumatoid arthritis or chronic rheumatism, of which the evidence is seen in various joints, but in which the pain and discomfort seem concentrated in the feet, which are absolutely stiff and deformed. In such cases one can hardly expect a complete cure; but, although the function of leverage may not be regained, still one may hope, by overcoming the deformity, to hold the weight of the body over the foot, so that the pain of a progressive dislocation may not be added to the pain of disease.
I have in a number of instances performed forcible over-correction with the happiest results, the improvement in the general condition, consequently in the resistance to the disease after the relief of the local pain and discomfort, being very marked.
Another type of weak foot is the common variety known as chronic sprain of the ankle, to which I have called attention under the title persistent abduction,2 in which the foot is rigidly held in an abducted or pronated position. The local condition in these cases varies from simple limitation of motion and slight deformity to subluxation of the astragalus; it is simply a variety of the weak and disabled foot, and is to be treated in exactly the same manner as the rigid flat-foot and with the same success. In most instances the so-called chronic sprains will be found to yield very readily to treatment conducted on the principle of an impaired function to be regained.
Between the two classes of cases, the mild and the severe, one finds every grade of deformity. All cases in which there is marked muscular spasm, local tenderness, and swelling, require temporary rest—in many instances, simply rest of function, combined with massage; in others, rest in a plaster bandage in an inverted position. In the milder and ordinary class of cases, the use of a brace and shoe will alone relieve spasm and pain, and the range of motion can usually be regained by manipulation, passive motion, and the proper use of the foot. Occasionally, even in childhood, limitation of normal motion which is not due to pain may prevent the proper use of the foot, and, if it does not readly yield to manipulation or mechanical stretching, tenotomy should be performed and followed by prolonged overcorrection of the deformity. The origin of the muscular inequality may very probably be in some instances an unnoticed and rapidly cured anterior poliomyelitis, which is still sufficient in its effects to imbalance the foot, and in others it is the result of the long duration of the deformity, but, whatever may be the theory of its causation, it is again emphasized that obstruction to motion in every direction must be overcome before a complete cure is possible.
It must be apparent that in many instances the cure of the weak foot is out of the question, either because of the want of energy or opportunity on the part of the patient, or because of the local or general condition, types familiar in out-patient practice. In such cases, raising and strengthening the inner side of the shoe by the wedge-shape leather sole, as used by Thomas, splints the painful foot and aids in relieving the strain. If the symptoms are more acute, the adhesive-plaster strapping, as advocated by Cottrell and Gibney for the treatment of sprains, is often of service, although it is applied in a different manner and with a somewhat different object in view. One end of a strip of adhesive plaster, about fifteen inches long and three inches wide, is applied to the outer side of the ankle just below the external malleolus; the foot is then adducted and the band is drawn tightly beneath the sole and up the inner side of the arch and leg, and is stayed in this position by one or two plaster strips about the calf. Narrow plaster straps are then applied about the arch and ankle in a figure-of-eight manner, and a bandage is applied. The object of the dressing is to aid in holding the foot in the proper position by the support and suggestiveness of the plaster, and to provide the firm compression about the arch that is always agreeable to the sufferer from weak foot. This treatment, combined with the built-up shoe, is often very effective in overcoming the acute and disabling symptoms of the weak and injured foot.
The various cutting operations for the relief of flat-foot do not call for extended comment in a paper devoted to its prevention and cure. The typical operation aims at removal of deformity only; functional cure is made impossible by the destruction of the medio-tarsal joint. It hardly seems possible that adhesion between the astragalus and scaphoid bones can for any length of time withhold a recurrence of deformity of the nature and origin of flat-foot, and in all cases that I have examined in which this operation had been performed there was still local tenderness and muscular spasm, and even relapse of the deformity.
The operation of advancement of the extremity of the os calcis, as proposed by Gleich, in order that it may be placed in relation to the leg somewhat like that of a Pirogoff amputation, is not likely to be adopted, nor is the scoring of the sole of the foot with the hot iron likely to become popular, as advocated by Bond, for the purpose of obtaining scar contraction.
The most innocent and rational of the operations for flat-foot is the supra-malleolar osteotomy of Trendelenburg; it is, unfortunately, by no means always successful, and the necessarily pronounced artificial bowleg is likely to prevent its extended use in this country.
In all operations the element of rest necessary for weeks or months must be taken into consideration as explaining the immediate effect of whatever procedure is adopted. An investigation of final results will prove, I believe, as might be predicted from the nature of the deformity and the complex structure of the foot, that there is no short and easy method by which a cure may be attained.
A brief analysis of a thousand cases of so-called flat-foot may present certain points of interest. No cases of incidental or paralytic flat-foot are included in the statistics, which represent the new cases treated in the out-patient department of the Hospital for the Ruptured and Crippled during the past five years:
The age and sex of the patients
| Age | Males | Females | Total |
|---|---|---|---|
| Ten or less | 68 | 30 | 98 |
| Ten to fifteen | 112 | 87 | 199 |
| Fifteen to twenty | 144 | 83 | 227 |
| Twenty to twenty-five | 94 | 53 | 147 |
| Twenty-five to thirty | 68 | 41 | 109 |
| More than thirty | 132 | 88 | 220 |
| 618 | 382 | 1000 |
Foot affected: right, 133; left, 138; both, 729.
In fifty-eight cases the cause of the disability appeared to be injury, and in sixty-five instances it was apparently due to rheumatism or rheumatoid arthritis.
The symptoms usually appear first in one foot, and, as a rule, they are at all times more marked on one side. In five hundred and sixty-nine instances, the duration of symptoms was recorded, being six months or less in four hundred and nine.
The age of the patients is of interest as bearing on the question of prognosis. Four hundred and twenty-six were between ten and twenty years of age, and seven hundred and eighty were less than thirty.
Hospital statistics cannot adequately represent the subject of the weak foot, for, as a rule, it was because of disability and pain, not for the deformity or for the milder type of symptoms, that these patients applied for treatment. In the larger proportion muscular spasm and rigidity were present, and in two hundred and thirty-four cases to such a degree that forcible overcorrection was advised, an operation rarely necessary in private practice.
It is in childhood that the prevention of subsequent weakness and deformity is of the first importance, yet but ninety-eight children of ten years of age or less are recorded, and of these a large proportion were brought, not for weakness or deformity, but for treatment of the symptomatic in-toeing.
The philosophy of this theory of the cause and cure of the weak foot may be again briefly outlined:
The normal foot may be made to assume an attitude resembling that of the so-called flat-foot (Fig. 2).
The deformity of flat-foot is a permanent exaggeration of a normal attitude (Fig. 1); it follows, then, that the habitual assumption of the simulating posture predisposes to deformity.
This passive attitude that simulates deformity may be simply the result of habit; but, on the other hand, it must be assumed if the mechanism is weak or overburdened, or if leverage causes pain, or if normal motion is in any way restricted.
Weakness may be prevented by guarding the foot from injury and improper use. Deformity may be cured by the removal of obstructions to normal use, by protecting the foot during the period of weakness, and by restoring the normal balance between the work to be performed and the ability of the mechanism. In conclusion, the following points are again emphasized. Flat-foot, in its surgical sense, is a compound deformity, of which the elements of valgus and abduction, the improper distribution of the weight and strain, are of vastly greater importance than the depth of the arch.
The weak and flat foot can be cured, but only by the application of the simple principles that any mechanic would apply to a disabled machine whose structure and use were known to him; in other words, there can be no permanent cure of weakness and deformity unless normal function is regained, nor effective treatment unless it has this end in view.
The term weak-foot has at least this advantage, that it implies nothing that the student must unlearn, for, if functional weakness is recognized, its causes may be analyzed and appreciated; it is because of the misapplication and misapprehension of the term flat-foot, and because of the associations which have so long obscured the rational treatment of the deformity, that the term has been discarded from the title of this paper.
Previous articles on this subject by the writer may be found in the Boston Medical and Surgical Journal, June 14 and 21, 1888; vol. i. of the Transactionsofthe American Orthopedic Association for 1888; the New York Medical Journal, May 17, 1890, October 11, 1890, and February 27, 1892; and the Annals of Surgery, January, 1893.
Footnotes
The attitude of adduction is the strong attitude, because the weak part of the foot is protected by the muscles. The typical strong deformity is the club-foot, of which pain is not a symptom, and in which the weight of the body may be made use of to correct and prevent deformity. The attitude of abduction is the weak attitude of muscular relaxation, in which the weak part of the foot is subjected to overstrain. The typical weak deformity is the flat-foot, in which the strain and weight of use cause pain and increase the deformity.
New York Medical Journal, October 11, 1890.
Richard A. Brand MD (✉) Clinical Orthopaedics and Related Research, 1600 Spruce Street, Philadelphia, PA 19103, USA e-mail: dick.brand@clinorthop.org