

Abstract
Diabetic neuropathy presents a major public health problem. It is defined by the symptoms and signs of peripheral nerve dysfunction in diabetic patients, in whom other causes of neuropathy have been excluded. Pathogenetic mechanisms that have been implicated in diabetic neuropathy are: a) increased flux through the polyol pathway, leading to accumulation of sorbitol, a reduction in myo-inositol, and an associated reduced Na+-K+-ATPase activity, and b) endoneurial microvascular damage and hypoxia due to nitric oxide inactivation by increased oxygen free radical activity. Alpha-lipoic acid seems to delay or reverse peripheral diabetic neuropathy through its multiple antioxidant properties. Treatment with alpha-lipoic acid increases reduced glutathione, an important endogenous antioxidant. In clinical trials, 600 mg alpha-lipoic acid has been shown to improve neuropathic deficits. This review focuses on the relationship of alpha-lipoic acid and auto-oxidative glycosylation. It discusses the impact of alpha-lipoic acid on hyperglycemia-induced oxidative stress, and examines the role of alpha-lipoic acid in preventing glycation process and nerve hypoxia.
Keywords: diabetes, alpha-lipoic acid, reactive oxygen species, advanced glycation end products, nuclear factor-kappaB, protein kinase C
Introduction
Diabetic neuropathy is defined by the signs and symptoms of peripheral nerve dysfunction in diabetic patients, in whom other causes of neuropathy have been excluded [1]. Diabetic neuropathy includes a number of different syndromes, depending on the classes of nerve fibers involved [2]. According to the San Antonio Convention, the major groups of neurologic disorders in patients with diabetes mellitus are: 1. subclinical neuropathy defined by abnormalities in electrodiagnostic and quantitative sensory testing, 2. diffuse clinical neuropathy with distal sensorimotor and autonomic syndromes, and 3. focal syndromes [3].
At least 25% of diabetic patients are affected by distal symmetric polyneuropathy, which is a major public health problem, as it is responsible for considerable morbidity and mortality [4-7]. Distal symmetric polyneuropathy is a major contributing factor for diabetic foot ulcer, osteoarthopathy, osteomyelitis, and lower limb amputation. The latter is fifteen times higher in diabetic patients than in the general population [5, 8]. Neuropathic pain affects approximately 16% of diabetic patients [9]. This subjective symptom impairs quality of life and sleeping as it usually gets worse at night [1, 8]. It is often the major complaint that motivates patients to seek health care [10]. However, treatment of painful diabetic symmetric polyneuropathy is still a challenge for the physician [11].
Treatment of diabetic neuropathy is based on: 1. aiming at near-normoglycemia, 2. pathogenetically oriented therapy, 3. symptomatic therapy, and 4. avoidance of risk factors [8]. Near-normoglycemia is generally accepted as the first approach towards preventing diabetic neuropathy [12, 13]. As normoglycemia is difficult to achieve, additional treatment of painful symptoms is frequently required [14]. Pathogenetically oriented therapy may delay, stop, or reverse the progression of neuropathy and may alleviate pain. Whilst symptomatic therapy does not influence the course leading to neuropathy, it may alleviate painful symptoms [15].
Antidepressants (SSRIs and tricyclic), opioids (e.g. controlled-release oxycodone), and older anticonvulsants (e.g. carbamazepine) all seem to alleviate pain, but have several adverse side effects [16]. Newer anticonvulsants such as gabapentin and pregabalin have a high affinity binding to α2-δ subunit of voltage-activated calcium channels. They combat painful diabetic neuropathy, partly via calcium channel modulation in the pathogenesis of diabetic neuropathy [16, 17].
Pathogenesis of diabetic neuropathy
The pathogenesis of diabetic neuropathy is complicated. The following mechanisms seem to be involved: 1. increased flux through the polyol pathway, mediated by aldose reductase and sorbitol dehydrogenase, leading to accumulation of sorbitol and depletion of myo-inositol. The latter reduction is associated with reduced Na+-K+-ATPase activity [8]. 2. Endoneurial microvascular damage and hypoxia due to nitric oxide inactivation [18]. 3. Accumulation of advanced glycation end products (AGEs) that exert their damaging effects by binding to specific receptors on the surface of neurons. Binding of AGEs to their receptors causes oxidative stress and activates nuclear factor-κB (NF-κB). There is increasing evidence that the diverse agents able to activate NF-κB elevate levels of reactive oxygen species (ROS). Also, chemically distinct antioxidants and overexpression of antioxidant enzymes can inhibit NF-κB activation [8, 18-20]. 4. Increased nerve lipid peroxidation in vivo. The most reliable index of increased oxidative stress is reduction in GSH [18]. 5. Activation of protein kinase C (PKC) by increased release of intracellular diacylglycerol (DAG) due to glycolysis. Hyperglycemia activates PKC, especially its βII isoform through increased de novo synthesis of DAG. The increased activity of PKCβ may impair endoneurial blood flow. Recently, hyperglycemia has been associated with activation of PKC and increase in Nav1.7 tetrodotoxin-sensitive voltage-gated sodium channel isoform; both of which play a critical role in the perception of pain [21-24]. 6. Alterations in mitogen-activated protein kinases (MAPKs) result in a signaling cascade involved in the pathogenesis of peripheral diabetic neuropathy [25]. 7. Abnormal Ca2+ homeostasis and signaling [26].
As mentioned above, hyperglycemia-induced ischemic and auto-oxidative lipid peroxidation is suggested to cause diabetic neuropathy (Figure 1). Streptozotocin-induced experimental diabetic neuropathy in rats is associated with a nerve blood flow deficit of 50% [18]. Endoneurial hypoxia is secondary to a reduction in nerve blood flow and increased endoneurial vascular resistance. Hyperglycemia acts via a reduction in nitric oxide resulting in impaired microvascular tone, reduced nerve blood flow, and endoneurial hypoxia [27, 28]. Hypoxic nerve can continue to function on glucose alone under anoxic circumstances via anaerobic glycolysis. A detrimental effect is hyperactivity of the polyol pathway resulting in an increase in sorbitol and a reduction in myo-inositol [27-30]. Nevertheless, sorbitol per se is non-toxic and it seems likely that mechanisms other than nerve sorbitol accumulation cause neuropathy. The reduction in myo-inositol has been linked to neuropathy via reduction in Na+-K+-ATPase activity [31-37]. The mechanism of myo-inositol reduction by hyperactivity of the polyol pathway is not completely known, but hyperglycemia could reduce nerve myo-inositol by competitive inhibition of peripheral nerve myo-inositol uptake. Osmolyte and non-osmolyte mechanisms could be involved [38, 39].
Figure 1.
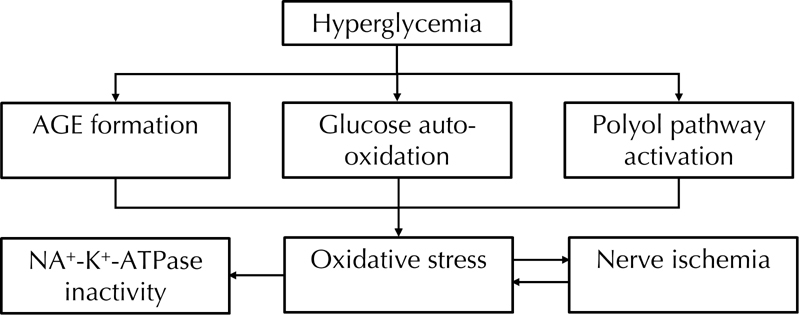
Increased oxidative stress in diabetes appears to be mainly due to hyperglycemia, which leads to AGE formation and polyol pathway activation, resulting in subsequent formation of reactive oxygen species. AGE: advanced glycation end product.
The effectiveness and tolerability of aldose reductase inhibitors and protein kinase C inhibitors are currently being investigated [40]. Besides, acetyl-L-carnitine is deficient in diabetes. Substitution with acetyl-L-carnitine corrects perturbations of neural Na+-K+-ATPase, myo-inositol, and nitric oxide. It also improves nerve fiber regeneration and alleviates symptoms, particularly pain in patients with established diabetic neuropathy [41-43]. Alpha-lipoic acid seems to normalize endoneurial Na+-K+-ATPase activity in experimental diabetic nerves [44]. As observed in retinal cells, the improved Na+-K+-ATPase activity could improve myo-inositol uptake by the Na+-myo-inositol co-transporter [34-37]. Alpha-lipoic acid has an effect on glucose uptake, thereby increasing polyol pathway activity [44]. It is known to increase Krebs cycle activity, too [45]. The effects of alpha-lipoic acid on glucose uptake and polyol metabolites, as well as the ability of alpha-lipoic acid to increase pyruvate dehydrogenase and α-ketoglutarate activity in a number of non-neural tissues, suggest that the effects of alpha-lipoic acid on the polyol pathway and the Krebs cycle are worth further exploration [44, 45].
Oxidative stress and alpha-lipoic acid
Hyperglycemia-induced oxidative stress induces programmed cell death of nerves, which contributes to the pathology of diabetic neuropathy [46, 47]. A study found reduced frequency of apoptosis in diabetic animals that were treated with the antioxidant taurine [48]. Another study reported increased frequency of programmed cell death in cultured dorsal root ganglia when glucose was added [49]. The role of oxidative stress in nerve damage has been extensively studied in experimental diabetes and in diabetic subjects [50-55]. Motor nerve and sensory nerve conduction velocities are the principal endpoints in studying the therapeutic effectiveness of alpha-lipoic acid on nerve function. Alpha-lipoic acid has been shown to improve motor nerve conduction velocity in experimental diabetic neuropathy and protect peripheral nerves from ischemia in rats [54, 55].
Treatment with alpha-lipoic acid increases reduced glutathione (GSH) in vivo and in vitro [56-59]. GSH is an important endogenous antioxidant. Together with lipoic acid it seem to play a major role in redox-dependent mechanisms of various cellular targets [18, 59-61]. Alpha-lipoic acid is a powerful lipophilic free radical scavenger of peripheral nerve both in vitro and in vivo [62, 63]. As diabetes has been associated with increased production and/or decreased clearance of ROS, oxidative stress has been suggested to contribute to defective nerve blood supply and endoneurial oxidative damage [64, 65]. The increased availability of glucose in diabetes induces enhanced production of AGEs. This process is defined as auto-oxidative glycosylation and is considered the major cause of increased ROS production among diabetic subjects [66]. The increased availability of glucose leads to glycation of antioxidant enzymes [67-70]. Therefore, the process of glucose auto-oxidation might be responsible for enhanced ROS production and for decreased availability or activity of antioxidant enzymes [71, 72]. Furthermore, fructose, which is increased due to the activation of the polyol pathway, leads to the formation of AGE precursors [73] (Figure 2). Alpha-lipoic acid has additional actions such as stimulating nerve growth factor and promoting fiber regeneration [74, 75].
Figure 2. The polyol pathway.
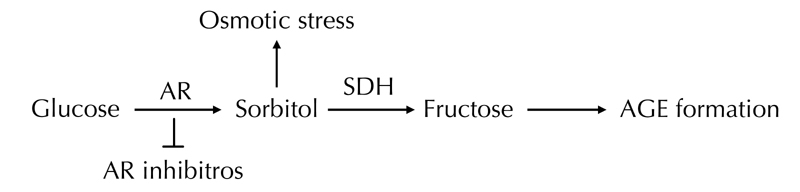
The polyol pathway converts glucose to fructose via production of sorbitol. AR: aldose reductase. SDH: sorbitol dehydrogenase. AR inhibitors: aldose reductase inhibitors. SDH: sorbitol dehydrogenase.
History of alpha-lipoic acid
R-alpha-lipoic acid (1, 2-dithiolane-3-pentanoic acid) was discovered in 1937 by Snell et al., who found that certain bacteria needed a compound from potato extract for growth [76]. In 1951, the so-called potato-growth factor was isolated by Reed and colleagues, and lipoic acid was discovered as a molecule that assists in acyl-group transfer and as a co-enzyme in the Krebs cycle [77, 78]. In the 1980s, alpha-lipoic acid was recognized as a powerful antioxidant. It is the only fat- and water-soluble antioxidant. It is produced by animals and humans [79], and can be found in liver, skeletal muscle, potatoes, and broccoli [80, 81]. Nutritional supplements of alpha-lipoic acid are typically comprised either of R-alpha-lipoic acid alone or a racemic mixture of R-alpha-lipoic acid and S-alpha-lipoic acid [79].
Alpha-lipoic acid in clinical practice
Diabetic patients with neuropathy treated with alpha-lipoic acid 600 mg i.v. daily for three weeks, have reduced pain, paresthesias, and numbness [14, 80, 81]. According to a recent meta-analysis comprising 1,258 patients, the same treatment ameliorated neuropathic symptoms and deficits after three weeks [81]. Acute infusion of alpha-lipoic acid improved nitric oxide-mediated endothelium-dependent vasodilation in diabetic patients, and improved microcirculation in patients with diabetic polyneuropathy [60-65, 81-89].
Oral treatment with alpha-lipoic acid for five weeks improved neuropathic symptoms and deficits in 187 patients with diabetic symmetrical polyneuropathy. This is an encouraging finding as deficits are major risk factors in the development of neuropathic foot ulcer [10, 90-92]. An oral dose of 600 mg once daily seems to provide the optimum risk-to-benefit ratio in the SYDNEY 2 trial [10]. The adverse effects (mainly nausea) with the 1,200 mg dose daily occurred in 21% of patients, somewhat higher than that observed in the ALADIN I (15%) and ALADIN II study (7%), with the same dose of alpha-lipoic acid [10, 93, 94]. In the seven-month ALADIN III trial, 509 subjects received either 600 mg of alpha-lipoic acid or placebo. While no significant difference was noted in subjective symptom evaluation among the groups, treatment with alpha-lipoic acid was associated with improved nerve function [95].
In the ISLAND Study, 300 mg of alpha-lipoic acid was applied as monotherapy and in combination with 150 mg imbesartan daily. There was a significant increase in endothelium-dependent flow-mediated vasodilation of the brachial artery, by 44% and 75% respectively, compared with placebo treatment after four weeks. This effect was accompanied by reductions in plasma levels of interleukin-6 and plasminogen activator-1, suggesting that alpha-lipoic acid may improve endothelial dysfunction via anti-inflammatory and antithrombotic mechanisms [96]. These anti-inflammatory and antithrombotic properties have previously been observed in streptozotocin-diabetic rats by significant decreases in fibrinogen factor VII and von Willebrand factor (vWF) after treatment with alpha-lipoic acid [97].
Alpha-lipoic acid has been shown to downregulate the expression of cell-adhesion molecules ICAM-1 and VCAM-1 in a dose-dependent manner [98]. These observations might be of preventive and/or therapeutic benefit in arteriosclerosis and other inflammatory disorders [18]. Clinical and postmarketing surveillance studies have revealed a highly favorable safety profile of the drug [99]. Nevertheless, further studies are necessary to assess the neurophysiological and clinical properties of alpha-lipoic acid.
Conclusions
Distal symmetric polyneuropathy is a major public health problem causing substantial morbidity and mortality among diabetic patients. Its pathogenesis remains complicated. Increased flux through the polyol pathway, which leads to accumulation of sorbitol, depletion of myo-inositol, endoneurial microvascular damage, and hypoxia seem to be the underlying pathogenetic mechanisms. The latter is due to nitric oxide inactivation and accumulation of AGEs that exert their damaging effects by binding to specific receptors on the surface of neurons, leading to activation of NF-κB.
The role of oxidative stress in nerve damage has been extensively studied in experimental and clinical diabetes. Alpha-lipoic acid has been shown to improve motor-nerve conduction velocity in experimental diabetic neuropathy, and to protect peripheral nerves from ischemia in rats.
Treatment with alpha-lipoic acid increases GSH in vivo and in vitro. GSH is an important endogenous antioxidant, and together with lipoic acid, it seems to play a predominant role in the redox-dependent mechanisms of various cellular targets. As diabetes has been associated with increased production and/or decreased clearance of ROS, oxidative stress has been suggested to contribute to defective nerve blood supply and endoneurial oxidative damage.
Recently, trials have been conducted with neuropathic diabetes patients who received 600 mg alpha-lipoic acid. The treatment reduced pain, paresthesias, and numbness. Further studies are needed to determine the effectiveness of alpha-lipoic acid in reducing pain and/or preventing the progression of diabetic neuropathy.
Disclosures: The authors report no conflict of interests.
References
- 1.Bansal V, Kalita J, Misra UK. Diabetic neuropathy. Postgrad Med J. 2006;82:95–100. doi: 10.1136/pgmj.2005.036137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vinik IA, Park TS, Stansberry KB, Pittenger GL. Diabetic neuropathies. Diabetologia. 2000;43:957–973. doi: 10.1007/s001250051477. [DOI] [PubMed] [Google Scholar]
- 3.Consensus Statement. Report and recommendations of the San Antonio conference on diabetic neuropathy. American Diabetes Association. American Academy of Neurology. Diabetes Care. 1988;11:592–597. doi: 10.2337/diacare.11.7.592. [DOI] [PubMed] [Google Scholar]
- 4.Shaw JE, Zimmet PZ, Gries FA, Ziegler D. Epidemiology of diabetic neuropathy. In: Gries FA, Cameron NE, Low PA, Ziegler D, editors. Textbook of Diabetic Neuropathy. Thieme; New York: 2003. pp. 64–82. [Google Scholar]
- 5.Boulton AJ, Malik RA, Arezzo JC, Sosenko JM. Diabetic somatic neuropathies. Diabetes Care. 2004;27:1458–1486. doi: 10.2337/diacare.27.6.1458. [DOI] [PubMed] [Google Scholar]
- 6.Boulton AJ, Vinik AL, Arezzo JC, Bril V, Feldman EL, Freeman R, Malik RA, Maser RE, Sosenko JM, Ziegler D. Diabetic neuropathies: a statement by the American Diabetes Association. Diabetes Care. 2005;28:956–962. doi: 10.2337/diacare.28.4.956. [DOI] [PubMed] [Google Scholar]
- 7.Coppini DV, Bowtell PA, Weng C, Young PJ, Sonksen PH. Showing neuropathy is related to increased mortality in diabetic patients: a survival analysis using an accelerated failure time model. J Clin Epidemiol. 2000;53:519–523. doi: 10.1016/s0895-4356(99)00170-5. [DOI] [PubMed] [Google Scholar]
- 8.Ziegler D. Treatment of Diabetic Polyneuropathy. Update 2006. Ann N Y Acad Sci. 2006;1084:250–266. doi: 10.1196/annals.1372.008. [DOI] [PubMed] [Google Scholar]
- 9.Dausi C, MacFarlane IA, Woodward A, Nurmikko TJ, Bundred PE, Benbow SJ. Chronic painful diabetic neuropathy in an urban community: a controlled comparison of people with and without diabetes. Diabetes Care. 2004;21:976–982. doi: 10.1111/j.1464-5491.2004.01271.x. [DOI] [PubMed] [Google Scholar]
- 10.Ziegler D, Ametov A, Barinov A, Dyck PJ, Gurieva I, Low PA, Munzel U, Yakhno N, Raz I, Novosadova M. et al. Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy. The SYDNEY 2 trial. Diabetes Care. 2006;29:2365–2370. doi: 10.2337/dc06-1216. [DOI] [PubMed] [Google Scholar]
- 11.Finnerup NB, Otto M, McQuay HJ, Jensen TS, Sindrup SH. Algorithm for neuropathic pain treatment: an evidence based proposal. Pain. 2005;118:289–305. doi: 10.1016/j.pain.2005.08.013. [DOI] [PubMed] [Google Scholar]
- 12.The Diabetes Control and Complications Trial Research Group. The effect of intensive diabetes therapy on the development and progression of neuropathy. Ann Intern Med. 1995;122:561–568. doi: 10.7326/0003-4819-122-8-199504150-00001. [DOI] [PubMed] [Google Scholar]
- 13.Diabetes Control and Complications Trial (DCCT) Research Group. Effect of intensive diabetes treatment on nerve conduction in the Diabetes Control and Complications Trial. Ann Neurol. 1995;38:869–880. doi: 10.1002/ana.410380607. [DOI] [PubMed] [Google Scholar]
- 14.Ziegler D, Gries FA. Alpha-lipoic acid in the treatment of diabetic peripheral and cardiac autonomic neuropathy. Diabetes. 1997;46(Suppl 2):S62–S66. doi: 10.2337/diab.46.2.s62. [DOI] [PubMed] [Google Scholar]
- 15.Varkonyi T, Kempler P. Diabetic neuropathy: new strategies for treatment. Diabetes Obes Metab. 2008;10:99–108. doi: 10.1111/j.1463-1326.2007.00741.x. [DOI] [PubMed] [Google Scholar]
- 16.Rutkove SB. A 52-year-old woman with disabling peripheral neuropathy: review of diabetic polyneuropathy. JAMA. 2009;302(13):1451–1458. doi: 10.1001/jama.2009.1377. [DOI] [PubMed] [Google Scholar]
- 17.Obrosova IG. Diabetes and the peripheral nerve. Biochim Biophys Acta. 2009;1792:931–940. doi: 10.1016/j.bbadis.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 18.Low PA, Nickander KK, Tritschler HJ. The roles of oxidative stress and antioxidant treatment in experimental diabetic neuropathy. Diabetes. 1997;46:S38–S42. doi: 10.2337/diab.46.2.s38. [DOI] [PubMed] [Google Scholar]
- 19.Packer L, Kraemer K, Rimbach G. Molecular aspects of lipoic acid in the prevention of diabetes complications. Nutrition. 2001;17:888–895. doi: 10.1016/s0899-9007(01)00658-x. [DOI] [PubMed] [Google Scholar]
- 20.Li N, Karin M. Is NF-kappaB the sensor of oxidative stress? FASEB J. 1999;13:1137. [PubMed] [Google Scholar]
- 21.Shiba T, Inoguchi T, Sportsman JR, Health W, Bursell S, King GL. Correlation of diacylglycerol and protein kinase C activity in rat retinal to retinal circulation. Am J Physiol. 1993;265:E783–E793. doi: 10.1152/ajpendo.1993.265.5.E783. [DOI] [PubMed] [Google Scholar]
- 22.Idris I, Donnelly R. Protein kinase Cbeta inhibition: a novel therapeutic strategy for diabetic microangiopathy. Diabetes Vasc Dis. 2006;3:172–178. doi: 10.3132/dvdr.2006.026. [DOI] [PubMed] [Google Scholar]
- 23.Nakamura J, Kato K, Hamada Y, Nakayama M, Chaya S, Nakashima E, Naruse K, Kasuya Y, Mizubayashi R, Miwa K, Yasuda Y. et al. A protein kinase C-beta selective inhibitor ameliorates neural dysfunction in streptozocin-induced diabetic rats. Diabetes. 1999;48:2090–2095. doi: 10.2337/diabetes.48.10.2090. [DOI] [PubMed] [Google Scholar]
- 24.Chattopadhyay M, Mata M, Fink D. Continuous delta-opioid receptor activation reduces neuronal voltage-gated sodium channel (Nav1.7) levels through activation of protein kinase C in painful diabetic neuropathy. J Neurosci. 2008;28:6652–6658. doi: 10.1523/JNEUROSCI.5530-07.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cavaletti G, Miloso M, Nicolini G, Scuteri A, Tredici G. Emerging role of mitogen-activated protein kinases in peripheral neuropathies. J Periph Nerv Syst. 2007;12:175–194. doi: 10.1111/j.1529-8027.2007.00138.x. [DOI] [PubMed] [Google Scholar]
- 26.Hall K, Liu KJ, Sima AA, Wiley JW. Impaired inhibitory G-protein function contributes to increased calcium currents in rats with diabetic neuropathy. J Neurophysiol. 2001;86:760–770. doi: 10.1152/jn.2001.86.2.760. [DOI] [PubMed] [Google Scholar]
- 27.Cameron NE, Cotter MA, Low PA. Nerve blood flow in early experimental diabetes in rats: relation to conduction deficits. Am J Physiol. 1991;261:E1–E8. doi: 10.1152/ajpendo.1991.261.1.E1. [DOI] [PubMed] [Google Scholar]
- 28.Cameron NE, Cotter MA, Archibald V, Dines KC, Maxfield EK. Antiooxidant and pro-oxidant effects on nerve conduction velocity, endoneurial blood flow and oxygen tension in non-diabetic and streptozotocin-diabetic rats. Diabetologia. 1994;37:449–459. doi: 10.1007/s001250050131. [DOI] [PubMed] [Google Scholar]
- 29.Stevens EJ, Carrington AL, Tomlinson DR. Nerve ischemia in diabetic rats: time-course of development, effect of insulin treatment plus comparison of streptozotocin and BB models. Diabetologia. 1994;37:43–48. doi: 10.1007/BF00428776. [DOI] [PubMed] [Google Scholar]
- 30.Fink BR, Cairns AM. Differential tolerance of mammalian myelinated and unmyelinated nerve fibers to oxygen lack. Re Anaesth. 1982;7:2–6. [Google Scholar]
- 31.Greene DA, Lattimer-Greene S, Sima AA. Pathogenesis of diabetic neuropathy: role of altered phosphoinositide metabolism. Crit Rev Neurobiol. 1989;5(2):143–219. [PubMed] [Google Scholar]
- 32.Greene DA, Lattimer SA. Sodium- and energy-dependent uptake of myo-inositol by rabbit peripheral nerve: competitive inhibition by glucose and lack of an insulin effect. J Clin Invest. 1982;70:1009–1018. doi: 10.1172/JCI110688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Greene DA, Chakrabarti S, Lattimer SA, Sima AA. Role of sorbitol accumulation and myo-inositol depletion in paranodal swelling of large myelinated nerve fibers in the insulin-deficient spontaneously diabetic bio-breeding rat: reversal by insulin replacement, an aldose reductase inhibitor and myo-inositol. J Clin Invest. 1987;79:1479–1485. doi: 10.1172/JCI112977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Thomas TP, Porcellati F, Kato K, Stevens MJ, Sherman WR, Greene DA. Effects of glucose on sorbitol pathway activation, cellular redox, and metabolism of myo-inositol, phosphoinositide, and diacylglycerol in cultured human retinal pigment epithelial cells. J Clin Invest. 1994;93:2718–2724. doi: 10.1172/JCI117286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Greene DA, Lattimer SA, Sima AA. Are disturbances of sorbitol, phosphoinositide and Na+-K+-ATPase regulation involved in pathogenesis of diabetic neuropathy? Diabetes. 1988;37:688–693. doi: 10.2337/diab.37.6.688. [DOI] [PubMed] [Google Scholar]
- 36.Kunisaki M, Bursell SE, Clermont AC, Ishii H, Ballas LM, Jirousek MR, Umeda F, Nawata H, King GL. Vitamin E prevents diabetes-induced abnormal retinal blood flow via the diacylglycerol-protein kinase C pathway. Am J Physiol. 1995;273:C671–C678. doi: 10.1152/ajpendo.1995.269.2.E239. [DOI] [PubMed] [Google Scholar]
- 37.Karihaloo A, Kato K, Greene DA, Thomas TP. Protein kinase and Ca2+ modulation of myo-inositol transport in cultured retinal pigment epithelial cells. Am J Physiol. 1997;273:C671–C678. doi: 10.1152/ajpcell.1997.273.2.C671. [DOI] [PubMed] [Google Scholar]
- 38.Fry MJ. Structure, regulation and function of phosphoinositide 3-kinases. Biochim Biophys Acta. 1994;1226(3):237–268. doi: 10.1016/0925-4439(94)90036-1. [DOI] [PubMed] [Google Scholar]
- 39.Volinia S, Dhand R, Vanhaesebroeckk B, MacDougall LK, Stein R, Zvelebil MJ, Domin J, Panaretou C, Waterfield MD. A human phosphatidylinositol 3-kinase complex related to the yeast Vp34p-Vp15p protein sorting system. EMBO. 1995;14:3339–3348. doi: 10.1002/j.1460-2075.1995.tb07340.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ziegler D. Painful diabetic neuropathy: treatment and future aspects. Diabetes Metab Res Rev. 2008;24(Suppl 1):S52–S57,. doi: 10.1002/dmrr.817. [DOI] [PubMed] [Google Scholar]
- 41.Scarpini E, Doneda P, Pizzul S, Chiodi P, Ramacci MT, Baron P, Conti G, Sacilotto G, Arduini A, Scarlato G. L-carnitine and acetyl-L-carnitine in human nerves from normal and diabetic subjects. J Peripher Nerv Syst. 1996;1:157–163. [PubMed] [Google Scholar]
- 42.Stevens MJ, Lattimer SA, Feldman EL, Helton E, Millington DS, Sima AA, Greene DA. Acetyl-L-carnitine deficiency as a cause of altered nerve myo-inositol content, Na+K+-ATPase activity and motor conduction velocity in the streptozocin diabetic rat. Metabolism. 1996;45:865–872. doi: 10.1016/s0026-0495(96)90161-4. [DOI] [PubMed] [Google Scholar]
- 43.Sima AA, Calvani M, Mehra M, Amato A. Acetyl-L-carnitine improves pain, nerve regeneration and vibratory perception in patients with chronic diabetic neuropathy. Diabetes Care. 2005;28:89–94. doi: 10.2337/diacare.28.1.89. [DOI] [PubMed] [Google Scholar]
- 44.Kishi Y, Schmelzer JD, Yao JK, Zollman PJ, Nickander KK, Tritschler HJ, Low PA. Alpha-lipoic acid: effect on glucose uptake, sorbitol pathway, and energy metabolism in experimental diabetic neuropathy. Diabetes. 1999;48:2045–2051. doi: 10.2337/diabetes.48.10.2045. [DOI] [PubMed] [Google Scholar]
- 45.Loffelhardt S, Bonaventura C, Locher M, Borbe HO, Bisswanger H. Interaction of alpha-lipoic acid enantiomers and homologues with the enzyme components of the mammalian pyruvate dehydrogenase complex. Biochem Pharmacol. 1995;50:637–646. doi: 10.1016/0006-2952(95)00175-y. [DOI] [PubMed] [Google Scholar]
- 46.Zimmer G. Overview of the role of lipoate in the enzyme complexes of energy metabolism and reducing equivalents. In: Fuchs J, Packer L, Zimmer G, editors. Lipoic acid in health and disease. Marcel Dekker; New York: 1997. pp. 67–86. [Google Scholar]
- 47.Packer L, Witt EH, Tritschler AG. Alpha-lipoic acid as a biological antioxidant. Free Radic Biol Med. 1995;19:227–250. doi: 10.1016/0891-5849(95)00017-r. [DOI] [PubMed] [Google Scholar]
- 48.Pop-Busui R, Sullivan K, Russel J. Taurine replacement prevents apoptosis in experimental diabetic neuropathy. Fifth Diabetic Neuropathy Satellite Symposium; 2000. 44. [Google Scholar]
- 49.Miinea C, Eichberg J. Antioxidant protection mechanisms and arachidonic acid synthesis are altered in Schwann cells grown in elevated glucose. Fifth Diabetic Neuropathy Satellite Symposium; 2000. 32. [Google Scholar]
- 50.Nickander KK, Schmelzer JD, Rohwer DA, Low PA. Effect of a-tocopherol deficiency on indices of oxidative stress in normal and peripheral diabetic nerve. J Neurol Sci. 1994;126:5–14. doi: 10.1016/0022-510x(94)90088-4. [DOI] [PubMed] [Google Scholar]
- 51.Garrett NE, Malcangio M, Dewhurst M, Tomlinson DR. Alpha-lipoic acid corrects neuropeptide deficits in diabetic rats via induction of trophic support. Neurosci Lett. 1997;222:191–194. doi: 10.1016/s0304-3940(97)13383-3. [DOI] [PubMed] [Google Scholar]
- 52.Nickander KK, McPhee BR, Low PA, Tritschler HJ. Alpha-lipoic acid: antioxidant potency against lipid peroxidation of neural tissues in vitro and implications for diabetic neuropathy. Free Radic Biol Med. 1996;21:631–639. doi: 10.1016/0891-5849(96)00172-4. [DOI] [PubMed] [Google Scholar]
- 53.Low PA, Yao JK, Kishi T, Tritschler HJ, Schmelzer JD, Zollman PJ, Nickander KK. Peripheral nerve energy metabolism in experimental diabetic neuropathy. Neurosci Res Comm. 1997;21:49–56. [Google Scholar]
- 54.Karasu C, Dewhurst M, Stevens EJ, Tomlinson DR. Effects of anti-oxidant treatment on sciatic nerve dysfunction in streptozocin-diabetic rats: comparison with essential fatty acids. Diabetologia. 1995;38:129–134. doi: 10.1007/BF00400086. [DOI] [PubMed] [Google Scholar]
- 55.Busse E, Zimmer G, Schopohl B, Kornhuber B. Influence of alpha-lipoic acid on intracellular glutathione in vitro and in vivo. Arzneimittelforschung. 1992;42:829–831. [PubMed] [Google Scholar]
- 56.Brownlee M, Cerami A, Vlassara H. Advanced glycosylation end products in tissue and the biochemical basis of diabetic complications. N Engl J Med. 1998;318:1315–1321. doi: 10.1056/NEJM198805193182007. [DOI] [PubMed] [Google Scholar]
- 57.Greene DA, Stevens MJ, Obrosova I, Feldman EL. Glucose-induced oxidative stress and programmed cell death in diabetic neuropathy. Eur J Pharmacol. 1999;375:217–223. doi: 10.1016/s0014-2999(99)00356-8. [DOI] [PubMed] [Google Scholar]
- 58.Vincent AM, McLean LL, Backus C, Feldman EL. Short-term hyperglycemia produces oxidative damage and apoptosis in neurons. FASEB J. 2005;19:638–640. doi: 10.1096/fj.04-2513fje. [DOI] [PubMed] [Google Scholar]
- 59.Nagamatsu M, Nicklander KK, Schmelzer JB, Raya A, Wittrock DA, Trischler HJ, Low PA. Lipoic acid improves nerve blood flow, reduces oxidative stress and improves distal nerve conduction in experimental diabetic neuropathy. Diabetes Care. 1995;18:1160–1167. doi: 10.2337/diacare.18.8.1160. [DOI] [PubMed] [Google Scholar]
- 60.Cameron NE, Cotter MA, Horrobin DH, Trischler HJ. Effects of alpha-lipoic acid on neurovascular function in diabetic rats: interaction with essential fatty acids. Diabetologia. 1998;41:390–399. doi: 10.1007/s001250050921. [DOI] [PubMed] [Google Scholar]
- 61.Mitsui Y, Schmelzer JD, Zollman P, Mitsui M, Kihara M, Low PA. Alpha-lipoic acid improves neuroprotection from ischemia-reperfusion injury on peripheral nerve. J Neurol Sci. 1999;163(1):11–16. doi: 10.1016/s0022-510x(99)00017-9. [DOI] [PubMed] [Google Scholar]
- 62.Podda M, Tritschler HJ, Ulrich H, Packer L. Alpha-lipoic acid supplementation prevents symptoms of vitamin E deficiency. Biochem Biophys Res Commun. 1994;204(1):98–104. doi: 10.1006/bbrc.1994.2431. [DOI] [PubMed] [Google Scholar]
- 63.Kozlov AV, Gille L, Staniek K, Nohl H. Dihydrolipoic acid maintains ubiquinone in the antioxidant active form by two-electron reduction of ubiquinone and one electron reduction of ubisemiquinone. Arch Biochem Biophys. 1999;363(1):148–154. doi: 10.1006/abbi.1998.1064. [DOI] [PubMed] [Google Scholar]
- 64.Han D, Handelman G, Marcocci L, Sen CK, Roy S, Kobuchi H, Tritschler HJ, Flohe L, Packer L. Lipoic acid increases de novo synthesis of cellular glutathione by improving cystine utilization. Biofactors. 1997;6(3):321–338. doi: 10.1002/biof.5520060303. [DOI] [PubMed] [Google Scholar]
- 65.Sen CK, Roy S, Han D, Packer L. Regulation of cellular thiols in human lymphocytes by alpha-lipoic acid: a flow cytometric analysis. Free Radic Biol Med. 1997;22:1241–1257. doi: 10.1016/s0891-5849(96)00552-7. [DOI] [PubMed] [Google Scholar]
- 66.Sen CK. Redox signaling and the emerging therapeutic potential of thiol antioxidants. Biochem Pharmacol. 1998;55(11):1747–1758. doi: 10.1016/s0006-2952(97)00672-2. [DOI] [PubMed] [Google Scholar]
- 67.Van Dam PS, Van Asbeck BS, Erkelens DW, Marx JJ, Gispen WH, Bravenboer B. The role of oxidative stress in neuropathy and other diabetic complications. Diabetes Metab Rev. 1995;11:181–192. doi: 10.1002/dmr.5610110303. [DOI] [PubMed] [Google Scholar]
- 68.Van Dam PS, Bravenboer B. Oxidative stress and antioxidant treatment in diabetic neuropathy. Neurosci Res Commun. 1997;21:41–48. [Google Scholar]
- 69.Wolff SP. Diabetes mellitus and free radicals. Free radicals, transition metals and oxidative stress in the aetiology of diabetes mellitus and complications. Br Med Bull. 1993;49:642–652. doi: 10.1093/oxfordjournals.bmb.a072637. [DOI] [PubMed] [Google Scholar]
- 70.Van Dam PS. Oxidative stress and diabetic neuropathy: pathophysiological mechanisms and treatment perspectives. Diabetes Metab Res Rev. 2002;18:176–184. doi: 10.1002/dmrr.287. [DOI] [PubMed] [Google Scholar]
- 71.Blakytny R, Harding JJ. Glycation (non enzymic glycosylation) inactivates glutathione reductase. Biochem J. 1992;288:303–307. doi: 10.1042/bj2880303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Kawamura N, Ookawara T, Suzuki K, Konishi K, Mino M, Taniguchi N. Increased glycated Cu, Zn-superoxide dismutase levels in erythrocytes of patients with insulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1992;74:1352–1354. doi: 10.1210/jcem.74.6.1592880. [DOI] [PubMed] [Google Scholar]
- 73.Takagi Y, Kashiwagi A, Tanaka Y, Asahina T, Kikkawa R, Shigeta Y. Significance of fructose-induced protein oxidation and formation of advanced glycation end product. J Diabet Complications. 1995;9:87–91. doi: 10.1016/1056-8727(94)00022-g. [DOI] [PubMed] [Google Scholar]
- 74.Murase K, Hattori A, Kohno M, Hayashi K. Stimulation of nerve growth factor synthesis/secretion in mouse astroglial cells by coenzymes. Biochem Mol Biol Int. 1993;30:615–621. [PubMed] [Google Scholar]
- 75.Dimpfel W, Spuler M, Pierau FK, Ulrich H. Thioctic acid induces dose-dependent sprouting of neurites in cultured rat neuroblastoma cells. Dev Pharmacol Ther. 1990;14:193–199. [PubMed] [Google Scholar]
- 76.Snell EE, Strong FM, Peterson WH. Growth factors for bacteria. VI: Fractionation and properties of an accessory factor for lactic acid bacteria. Biochem J. 1937;31(10):1789–1799. doi: 10.1042/bj0311789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Reed LJ, DeBusk BG, Gunsalus IC, Hornberger CS Jr. Cristalline alpha-lipoic acid: a catalytic agent associated with pyruvate dehydrogenase. Science. 1951;114(2952):93–94. doi: 10.1126/science.114.2952.93. [DOI] [PubMed] [Google Scholar]
- 78.Reed LJ. The chemistry and function of lipoic acid. Adv Enzymol. 1957;18:319–347. doi: 10.1002/9780470122631.ch8. [DOI] [PubMed] [Google Scholar]
- 79.Carreau JP. Biosynthesis of lipoic acid via unsaturated fatty acids. Methods Enzymol. 1979;62:152–158. doi: 10.1016/0076-6879(79)62212-7. [DOI] [PubMed] [Google Scholar]
- 80.Morelli V, Zoorob RJ. Alternative therapies: Part I. Depression, Diabetes, Obesity. Am Fam Physician. 2000;62:1051–1060. [PubMed] [Google Scholar]
- 81.Ziegler D, Nowak H, Kempler P, Vargha P, Low PA. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a meta-analysis. Diabet Med. 2004;21:114–121. doi: 10.1111/j.1464-5491.2004.01109.x. [DOI] [PubMed] [Google Scholar]
- 82.Coppey LJ, Gellett JS, Davidson EP, Dunlap JA, Lund DD, Yorek MA. Effect of antioxidant treatment of streptozocin-induced diabetic rats on endoneurial blood flow, motor nerve conduction velocity, and vascular reactivity of epineurial arterioles of the sciatic nerve. Diabetes. 2001;50:1927–1937. doi: 10.2337/diabetes.50.8.1927. [DOI] [PubMed] [Google Scholar]
- 83.Yorek MA, Coppey LJ, Gellett JS, Davidson EP, Lund DD. Effect of fidarestat and alpha-lipoic acid on diabetes-induced epineurial arteriole vascular dysfunction. Exp Diabesity Res. 2004;5:123–135. doi: 10.1080/15438600490277824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Kunt T, Forst T, Wilhelm A, Tritschler H, Pfuetzner A, Harzer O, Engelbach M. , Zscaebitz A, Stofft E, Beyer J. Alpha-lipoic acid reduces expression of vascular cell adhesion molecule-1 and endothelial adhesion of human monocytes after stimulation with advanced glycation end products. Clin Sci (Lond) 1999;96:75–82. [PubMed] [Google Scholar]
- 85.Bierhaus A, Chevion S, Chevion M, Hofmann M, Quehenberger B, Illmer T, Luther T, Berentshtein E, Tritschler H, Müller M, Wahl P, Ziegler R, Nawroth PP. Advanced glycation end product-induced activation of NF-kappaB is suppressed by alpha-lipoic acid in cultured endothelial cells. Diabetes. 1997;46(9):1481–1490. doi: 10.2337/diab.46.9.1481. [DOI] [PubMed] [Google Scholar]
- 86.Androne L, Gavan NA, Veresiu IA, Orasan R. In vivo effect of lipoic acid on lipid peroxidation in patients with diabetic neuropathy. In Vivo. 2000;14:327–330. [PubMed] [Google Scholar]
- 87.Haak E, Usadel KH, Kusterer K, Amini P, Frommeyer R, Tritschler HJ, Haak T. Effects of alpha-lipoic acid on microcirculation in patients with peripheral diabetic neuropathy. Exp Clin Endocrinol Diabetes. 2000;108:168–174. doi: 10.1055/s-2000-7739. [DOI] [PubMed] [Google Scholar]
- 88.Haak ES, Usadel KH, Kohleisen M, Yilmaz A, Kusturer K, Haak T. The effect of alpha-lipoic acid on the neurovascular reflex arc in patients with diabetic neuropathy assessed by capillary microscopy. Microvasc Res. 1999;58:28–34. doi: 10.1006/mvre.1999.2151. [DOI] [PubMed] [Google Scholar]
- 89.Heitzer T, Finckh B, Albers S, Krohn K, Koglschutter A, Meinertz T. Benefficial effects of alpha-lipoic acid and ascorbic acid on endothelium-dependent, nitric oxide-mediated vasodilation in diabetic patients: relation to parameters of oxidative stress. Free Radic Biol Med. 2001;31:53–61. doi: 10.1016/s0891-5849(01)00551-2. [DOI] [PubMed] [Google Scholar]
- 90.Head KA. Peripheral neuropathy: pathogenic mechanisms and alternative therapies. Altern Med Rev. 2006;11(4):294–329. [PubMed] [Google Scholar]
- 91.Gries FA. Alternative therapeutic principles in the prevention of microvascular and neuropathic complications. Diabetes Res Clin Pract. 1995;28:S201–S207. doi: 10.1016/0168-8227(95)01071-k. [DOI] [PubMed] [Google Scholar]
- 92.Abbott CA, Vileikyte L, Williamson S, Carrington AL, Boulton AJ. Multicenter study of the incidence of and predictive risk factors for diabetic neuropathic foot ulceration. Diabetes Care. 1998;21:1071–1075. doi: 10.2337/diacare.21.7.1071. [DOI] [PubMed] [Google Scholar]
- 93.Reljanovic M, Reichel G, Rett K, Lobisch M, Schuette K, Moller W, Tritschler HJ, Mehnert H. The ALADIN II Study Group: Treatment of diabetic polyneuropathy with the antioxidant thioctic acid (alpha-lipoic acid): a two-year mylticenter randomized double blind placebo contorolled trial (ALADIN II) Free Radic Res. 1999;31:171–179. doi: 10.1080/10715769900300721. [DOI] [PubMed] [Google Scholar]
- 94.Ziegler D, Hanefeld M, Ruhnau KJ, Meibner HP, Lobisch M, Shutte K, Gries FA. ALADIN I Study Group. Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic acid: a 3-week multicenter randomized controlled trial (ALADIN Study) Diabetologia. 1995;38:1425–1433. doi: 10.1007/BF00400603. [DOI] [PubMed] [Google Scholar]
- 95.Ziegler D, Hanefeld M, Ruhnau KJ, Hasche H, Lobisch M, Schutte K, Kerum G, Malessa R. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a 7-month multicenter randomized controlled trial (ALADIN III Study). ALADIN III Study Group. Alpha-lipoic acid in diabetic neuropathy. Diabetes Care. 1999;22:1296–1301. doi: 10.2337/diacare.22.8.1296. [DOI] [PubMed] [Google Scholar]
- 96.Sola M, Mir MQ, Cheema FA, Khan-Merchant N, Menon RG, Parthasarathy S, Khan BV. Imbesartan and lipoic acid improve endothelial function and reduce markers of inflammation in the metabolic syndrome: results of the Imbesartan and Lipoic acid in endothelial dysfunction (ISLAND) STUDY. Circulation. 2005;111:343–348. doi: 10.1161/01.CIR.0000153272.48711.B9. [DOI] [PubMed] [Google Scholar]
- 97.Ford I, Cotter MA, Cameron NE, Greaves M. The effects of treatment with alpha-lipoic acid or evening primrose oil on vascular hemostatic and lipid risk factors, blood flow, and peripheral nerve conduction in streptozocin-diabetic rat. Metabolism. 2001;50(8):868–875. doi: 10.1053/meta.2001.24914. [DOI] [PubMed] [Google Scholar]
- 98.Roy S, Sen CK, Kobuchi H, Packer L. Antioxidant regulation of phorbol ester-induced adhesion of human Jurkat T-cells to endothelial cells. Free Radic Biol Med. 1998;25(2):229–241. doi: 10.1016/s0891-5849(98)00062-8. [DOI] [PubMed] [Google Scholar]
- 99.Ziegler D. Thioctic acid for patients with symptomatic diabetic neuropathy: a critical review. Treat Endocrinol. 2004;3(3):173–189. doi: 10.2165/00024677-200403030-00005. [DOI] [PubMed] [Google Scholar]