

Abstract
We conducted a cross-sectional survey of MSM using a time-location-sampling design in San Francisco during 2007–2008. The investigation focused on the selection of sexual partners, partner preferences, perceptions of HIV risk, and social mixing with respect to race/ethnicity. The sample of 1,142 MSM was 56% White, 22% Latino, 14% Asian, and 9% Black and reported on 3,532 sexual partnerships. Black MSM had a significant, threefold higher level of same race sexual partnering than would be expected by chance alone (i.e., in the absence of selective forces with respect to race among partners). Black MSM were reported as the least preferred as sexual partners, believed at higher risk for HIV, counted less often among friends, were considered hardest to meet, and perceived as less welcome at the common venues that cater to gay men in San Francisco by other MSM. Our findings support the hypothesis that the sexual networks of Black MSM, constrained by the preferences and attitudes of non-Blacks and the social environment, are pushed to be more highly interconnected than other groups with the potential consequence of more rapid spread of HIV and a higher sustained prevalence of infection. The racial disparity in HIV observed for more than a decade will not disappear until the challenges posed by a legacy of racism towards Blacks in the US are addressed.
Keywords: Race/ethnicity, HIV, MSM, Disparities, Sexual mixing, Sexual networks, Social networks, Social epidemiology
Introduction
An unfortunate characteristic of the current HIV epidemic in the United States is the disproportionate burden of infection borne by Black Americans (CDC 2006). Blacks accounted for nearly half of all HIV/AIDS cases diagnosed in 2006, producing a per capita rate four times the national average. Among MSM, numerous studies from multiple American cities consistently find Black MSM with significantly higher incidence and prevalence of HIV (Harawa et al. 2004; Millett et al. 2007; Valleroy et al. 2000). In San Francisco, the estimated prevalence of HIV among Black MSM is 32% compared to an overall figure of 24% (San Francsico Department of Public Health [SFDPH] 2004).
In an apparent paradox, most studies find that Black MSM do not engage in high-risk sexual behavior at greater rates than other race/ethnic groups of MSM (Millett et al. 2007; Harawa et al. 2004; Meyers et al. 2003). In fact, Black MSM tend to report lower levels of unprotected anal intercourse, fewer sexual partners, fewer HIV-positive sex partners, lower use of substances related to high risk sex (including methamphetamine and injection drugs), and engaging in less commercial sex work than MSM of other race/ethnicities. A recent review of the qualitative scientific literature generated several other hypotheses that may explain the higher rates of HIV among Black MSM (Millett et al. 2006). One hypothesis focused on the sexual networks of Black MSM; namely, that there might be less choice in sexual partners for Black MSM subsequently creating more closely-knit sexual networks than other groups. Tightly interconnected sexual networks can create conditions for rapid spread of HIV even if the numbers of partners and episodes of unprotected sex reported by individuals within the network were no higher than in other groups. That is, if HIV infection enters one part of the network, it can quickly reach a large portion of the population connected through the network. The high viral load during acute infection can further amplify HIV transmission when the sexual networks overlap in time. This situation appears to have been the case among young Black MSM in one study of acute HIV infection in North Carolina (CDC 2004). Other research finds that assortative mixing (i.e., sexual partnering that tends towards homogeneously intra-racial) can increase sexually transmitted disease burden within ethnic groups where disease prevalence is already elevated (Aral 2000). Thus, a sexual network structure may cause a rapid spread of HIV and maintain a high level of HIV infection over time even if other factors are constant. In a subsequent review of the quantitative data on the subject, the authors concluded that the sexual network hypothesis remained viable in light of the evidence for and against other possibilities, but there were insufficient specific data on the topic (Millett et al. 2007).
A previously reported survey of MSM conducted in San Francisco in 2004 that found Black MSM significantly more likely to partner with other Black MSM, in contrast to MSM of other race/ethnicities (Berry et al. 2007). These findings corroborated previous research from Los Angeles (Bingham et al. 2003). While the study recorded the race/ethnicities of respondents and their sexual partners; the data, however, did not explore any of the possible reasons for the higher level of same race partnering among Black MSM. We report here on the findings of a larger survey of MSM, conducted 4 years later in San Francisco that included a series of questions related to social and sexual mixing between different race/ethnicities. The aims of the present study are to assess the current levels of sexual mixing between the racial and ethnic groups of MSM in San Francisco and to identify potential reasons that underlie the patterns of sexual mixing.
Methods
Study Subjects, Recruitment and Sampling Design
We conducted a cross-sectional survey of MSM attending public venues in San Francisco from December 2007 through October 2008 using time-location sampling (TLS). The TLS methodology is used to approximate a probability sample in hidden or hard-to-reach populations through creation of a sampling frame that comprises the universe of venues, days, and time periods where and when the population can be found to congregate. From the roster of all possible venue-day-time (VDT) periods, a random sample of VDT is drawn. At the randomly selected VDT, the attendance of all potentially eligible subjects is recorded and individuals entering or exiting the venue or crossing a predetermined line are intercepted, assessed for eligibility, and invited to participate. Intercepts and interviews are done consecutively without choice on the part of field staff until all staff are occupied. Once a staff is available, intercepts and interviews resume. In the analysis, data are weighted according to the sample fraction obtained at the VDT and adjustments are made to standard errors to account for clustering. TLS is the sampling methodology selected for the US National HIV Behavioral Surveillance (NHBS) system for MSM coordinated by the Centers for Disease Control and Prevention (CDC) in several cities throughout the US and is used for biological and behavioral surveillance in diverse “most-at-risk populations” throughout the world (Valleroy et al. 2000; CDC 2005; Magnani et al. 2005; MacKellar et al. 1996; MacKellar et al. 2007). The methods have been applied to several previous surveys of MSM in San Francisco and have been described in detail previously (CDC 2005; MacKellar et al. 1996, 2007).
The present study recruited a sample of MSM separately from the NHBS but using the same TLS methods. The formative research phase constructed an up-to-date universe or sampling frame of gay-identified recruitment venues, which included bars, dance clubs, cruising areas, bookstores, gyms, social organizations, churches, street locations, and other venue types and the days and time periods of attendance. Venues included in the sampling frame were any venues known to be frequented by MSM and did not only focus on venues that were perceived to be more openly gay identified. Persons eligible for the study were male gender, age 18 years and older, being a resident of any of ten Bay Area counties, and had to be consecutively approached by the staff at the randomly selected VDT (i.e., they could not approach staff on their own or at a later time). Of note, identifying as MSM at the time of screening was not an eligibility criterion, thus allowing non-gay identified MSM to participate and reducing the risk that persons who did not wish to initially acknowledge male–male sexual behavior would not be excluded. For analysis, we included any participant reporting a male partner in the past year or who identified as gay or bisexual. After determining eligibility, staff obtained written informed consent.
Measures
The measures on race/ethnicity and sexual mixing presented in this current report were collected as part of a larger survey on sexual risk, drug use, and other health related behaviors. After informed consent, staff oriented participants to a handheld computer-assisted interview completed in a private area near the venue. Once participants were familiar with the operation of the handheld computer, they completed a self-administered questionnaire approximately 30 min in length. Participants self-identified their own race/ethnicity using the following questions: “Are you Latino/Hispanic?” (yes/no) and then “Which of the following racial group or groups do you consider yourself to be? (Check all that apply) Asian, African American/Black, American Indian/Alaska Native, Native Hawaiian/Pacific Islander, Caucasian, Other (specify)”. All participants responding yes to Latino/Hispanic were classified as Latino/Hispanic and nothing else. Those respondents reporting just one of the groups (but not Latino/Hispanic) were classified as the self-reported race. Those participants who respond to more than one of the racial groups (but not Latino/Hispanic) were classified as multi-racial and are not included in the analysis of mixing. Observations with an “other” response written in were examined and re-coded if appropriate (e.g., “Irish” would be re-coded to “Caucasian”). In the present report, we use the words “Asian”, “Black”, “White”, and “Latino” for simplicity. A similar procedure was used to classify the race/ethnicity of sexual partners by the respondent. Respondents were asked the race/ethnicity of each sexual partner, consecutively backwards starting with the most recent, for up to 5 partners in the last 6 months.
At the end of the survey, a series of questions were included that pertained to race/ethnicity and social and sexual mixing. Race/ethnicity preference in sexual partners was measured using a four-point Likert-like scale (from “strongly disagree” to “strongly agree”) in response to four separate questions phrased as “I prefer to have sexual partners who are—(Asian, Black, White, Latino)”. The same scale as was used for perceived ease of meeting sexual partners of different race/ethnicities (“It seems easier for me to meet sexual partners who are—[Asian, Black, White, Latino]” and for describing the environments of places to meet sex partners (“Bars and dance clubs catering to gay men in San Francisco are less welcoming to—[Asians, Blacks, Whites, Latinos]”. Perception of risk for HIV infection was measured using four questions with a three point scale to the question “Having sex with a—(Asian, Black, White, Latino) partner has (more risk, no difference in risk, or less risk) for HIV infection.” A measure of friendship networks was constructed using four questions with a five-point scale in response to this statement “(None, a few, some, most, all) of my friends are (Asian, Black, White, Latino)”.
Statistical Methods
Observations were included in this study's race/ethnicity analyses if respondents reported their race as Asian, Black, White, or Latino. Other racial groups (e.g., Native Americans, Native Alaskans, Native Hawaiians, and those reporting being “Other” or “Mixed”) were not included in these analyses due to small cell sizes. To assess a statistical tendency towards partnering with the same versus other race/ethnic groups we compared the expected number of race–race partnerships based on the race/ethnicity distribution of the sample and number of partnerships reported by respondents' race/ethnicity to the observed number of same-race and different-race partnerships using the chi-square test. Differences in preferences, perceptions, and numbers of friends by race/ethnicities were assessed using paired T-tests. All statistical comparisons are within respondents' race/ethnicity groups.
We also preliminarily explored correlates of interracial mixing among MSM overall to better understand this phenomenon. We explored differences in interracial mixing by classifying MSM as having sexual partners of all the same race as their own (“assortative”) or having at least one partner of a different race/ethnicity (“disassortative”) and using the chi-square test or Fisher's exact test to identify factors associated with these distinctions. Due to multiple, exploratory comparisons, we used p < 0.01 as the cut off for significance. Due to small sample sizes of each individual group we collapsed our sample into White versus Men of color. All statistical analyses were conducted using SAS version 9.13.
Results
Data were collected between December 2007 and October 2008. Study staff enumerated 24,333 men at 153 randomly selected venue-day-time periods and consecutively approached 2,558 men as interviewers were available. Of the 2,558 men approached, 2,186 (85%) agreed to eligibility screening; 1,769 (81%) were eligible; 1,321 (75%) agreed to participate in the survey; and 1,305 (99%) men completed the interview. During the interview, 92 men identified as heterosexual and did not report any male partners in the past 12 months or were duplicate enrollments, leaving 1,213 unique MSM. Of these, analyses were conducted on those self-identifying as Asian, Black, White, and Latino (N = 1,142).
A majority of MSM reported being White (56%), with the next largest group Latino (22%), followed by Asian (14%), and Black (9%). Table 1 shows demographic characteristics by race/ethnicity. Overall, subjects ranged in age from 18 to 77 years old (median 35, interquartile range 27–45). A large majority of participants identified as gay (89%) or bisexual (9%) with the remaining men identifying as heterosexual or some other orientation (2%) while also reporting male sexual partners in the last 12 months. In terms of educational attainment, 13% reported a high school or less level of education, 33% had attended some college, and 53% had a college degree.
Table 1.
(a) Participant demographic characteristics by race/ethnicity, men who have sex with men, San Francisco, 2008 (N = 1,142); (b) Race/ethnicity of reported sexual partnerships among men who have sex with men past 6 months, San Francisco, 2008 (N = 3,532)
| Asian n (%) | Black n (%) | White n (%) | Latino n (%) | |
|---|---|---|---|---|
| (a) Characteristic | ||||
| Total men | 160 | 98 | 641 | 243 |
| Age group (years) | ||||
| 18–25 | 36 (23) | 26 (27) | 85 (13) | 68 (28) |
| 26–35 | 83 (52) | 30 (31) | 164 (26) | 91 (38) |
| 36–45 | 30 (19) | 22 (22) | 183 (29) | 56 (23) |
| 46+ | 11 (7) | 20 (20) | 209 (33) | 27 (11) |
| Sexual identity | ||||
| Gay | 148 (93) | 74 (76) | 589 (92) | 207 (85) |
| Bisexual | 10 (6) | 19 (19) | 44 (7) | 29 (12) |
| Straight (and had male partners) | 0 | 2 (2) | 6 (1) | 5 (2) |
| Other (and had male partners) | 2 (1) | 3 (3) | 2 (<1) | 2 (1) |
| Highest education level achieved | ||||
| High school or less | 6 (4) | 18 (18) | 72 (11) | 51 (21) |
| Some college | 43 (27) | 43 (44) | 200 (31) | 96 (40) |
| College degree | 111 (69) | 36 (37) | 361 (56) | 95 (39) |
| Other | 0 | 1 (1) | 8 (1) | 1 (<1) |
| Residence | ||||
| San Francisco county | 112 (70) | 69 (70) | 548 (85) | 195 (80) |
| Other San Francisco Bay Area county | 48 (30) | 29 (30) | 93 (15) | 48 (20) |
| (b) Respondent race/ethnicity | ||||
| Total men | 160 | 98 | 641 | 243 |
| Total partnerships | 457 | 288 | 2,021 | 766 |
| Partner race/ethnicity (n, %) | ||||
| Asian | 79 (17) | 28 (10) | 303 (15) | 103 (13) |
| Black | 10 (46) | 76 (26) | 115 (6) | 57 (7) |
| White | 333 (76) | 151 (52) | 1,332 (66) | 472 (62) |
| Latino | 35 (8) | 33 (11) | 271 (13) | 134 (17) |
The 1,142 men in our analysis reported on 3,532 sexual partnerships (inlcuding 59 non-male partners) with other men during the past 6 months. Overall, 17, 9, 14 and 13% of partnerships of Asian, Black, White and Latino respondents were with partners of the same race/ethnicity, respectively (Table 1). Among partnerships for all men in our analyses, we compared the observed number of same race/ethnicity partnerships to the expected number that would occur under a null hypothesis of no racial/ethnic tendency in partnering. Black men were 3 times more likely to have partners that were also Black compared to what would be expected by chance; that is, for all partnerships, 2.1% were observed to be Black–Black partnerships compared to 0.7% expected by chance, χ2 78.5, p < 0.001. Put another way, within the partnerships of Black MSM, 8.5% would be expected to be with other Black MSM, yet 29% were observed to be. In addition, White MSM were about one and a third times more likely to partner with another White MSM than would be expected by chance (37% observed vs. 32% expected, χ2 45.4, p < 0.001). This finding is significant but most likely due to the greater numbers of White MSM in the sample. We detected no significant race/ethnicity tendencies in partners of Asian and Latino men; that is, the number of partnerships of same race/ethnicity neither exceeded nor fell short of what would be expected by chance.
After reporting the race/ethnicities of their sexual partners in the preceding 6 months, men were subsequently asked about their general preferences when choosing sexual partners (Fig. 1). With the exception of Blacks themselves, all other racial/ethnic groups scored Blacks lowest in terms of their preference for sexual partners (all p-values < 0.01 when comparing Black preference scores to scores for all other race/ethnicities). Black MSM significantly preferred Latinos over other Black MSM (p < 0.01), while their preferences for men from other racial/ethnic groups did not differ significantly. No other racial preferences scores were significantly different; that is, the only evidence of racial/ethnic preferences in sex partners was against Black MSM by all other groups and towards Latinos by Black MSM.
Fig. 1.
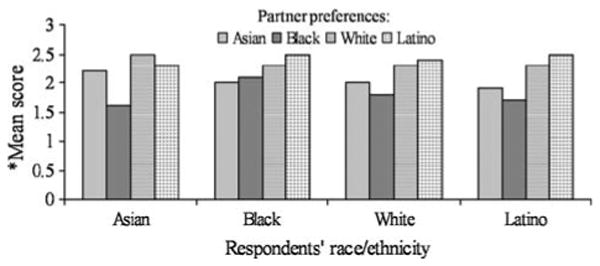
Agreement with a series of questions posed as: “I prefer to have sexual partners who are—(Asian, Black, White, Latino)” by respondents' race/ethnicity, men who have sex with men, San Francisco, 2008
When asked to report whether having sex with men of specific race/ethnicities presented more or less risk for HIV infection, all race/ethnicity groups, including Blacks themselves, perceived Black men to be riskier (Fig. 2). The pattern of perceiving Latinos as second most risky, followed by Whites, and Asians as least risky was consistent for all groups although not all comparisons achieved statistical significance. Of note, these perceptions approximate the relative prevalence of HIV for these groups in the US and San Francisco.
Fig. 2.
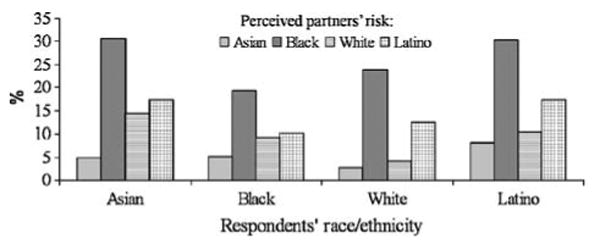
Percent agreeing with statement: “Having sex with a(n)— (Asian, Black, White, Latino) partner has more risk of HIV infection” by respondents' race/ethnicity, men who have sex with men, San Francisco, 2008
With the exception of Black MSM themselves, all other groups reported fewer Blacks in the make up of their friendships (Fig. 3, p < 0.001 for all differences between having Black friends versus all other race/ethnicity friends). Also with the exception of Black MSM, all other groups counted their own race/ethnicity most common among their friendships, but only for Whites was this significantly so (p < 0.001). Black MSM reported having Black, White, and Latino friends in similar numbers; however, they had fewer Asian friends compared to each of the other groups (all p-values < 0.001). Latino MSM reported higher but equal numbers of Latino and White friends but significantly lower numbers of Black and Asian friends groups (p-values < 0.001).
Fig. 3.
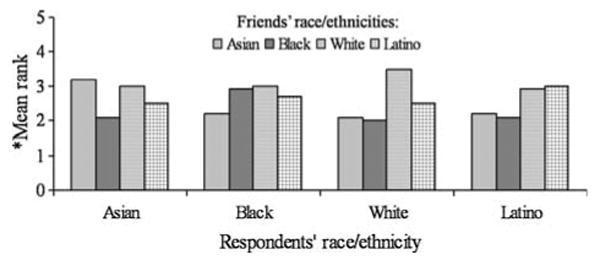
Responses to a series of questions posed as:”How many of your friends are—(Asian, Black, White, Latino)” by respondents' race/ethnicity, men who have sex with men, San Francisco, 2008
All racial/ethnic groups of MSM found Blacks less easy to meet compared to Whites (Fig. 4, all p-values < 0.001), including Black MSM themselves. Asian, White, and Latino MSM also ranked Whites easiest to meet, followed by Latino, then Asian least easy, although not all differences were significant. Moreover, there was equal agreement among all racial/ethnic groups that Whites felt more welcome than others at gay bars and dance clubs. For example, 90% of White MSM and 81% of Asian, Black, and Latino men agreed with the statement “It is easy for White men to feel welcome in most bars and dance clubs that cater to gay men in San Francisco”. Conversely, only 50% of White and 52% of Asian, Black, and Latino men agreed with “It is easy for men of color to feel welcome in most bars and dance clubs that cater to gay men in San Francisco”.
Fig. 4.
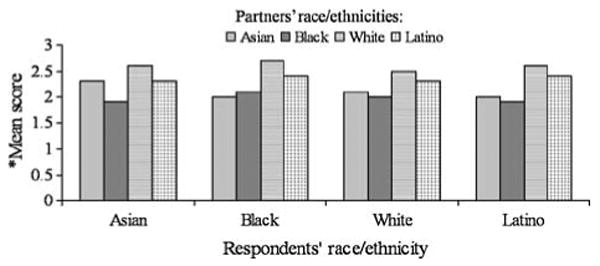
Agreement with a series of questions posed as: “It seems easier for me to meet sexual partners who are—(Asian, Black, White, Latino) by respondents' race/ethnicity, men who have sex with men, San Francisco, 2008
In order to identify correlates of inter-racial partnering, we classified MSM as “assortative” (i.e., where all their sex partners are of the same race/ethnicity) and “disassortive” (i.e., where at least one of their partners was of a different race/ethnicity). Men must have reported having more than one partner to be included in this analysis. Table 2 compares assortative and disassortative MSM separately for MSM of color (n = 343) and White MSM (n = 462). Among MSM of color, 7% were assortative while 93% were disassortative. White MSM were evenly split between assortative and disassortative. For White MSM being 26–45 years old (χ2 10.26, p < 0.01), having all/most friends of the same race (χ2 21.78, p < 0.01), preferring partners of the same race (χ2 29.28, p < 0.01), and perceiving it easier to meet men of the same race (χ2 23.14, p < 0.01) were associated with assortative partnering. Only having all/most friends of the same race (χ2 13.83, p < 0.01) and preferring the same race (χ2 8.05, p < 0.01) were associated with assortative partnering among MSM of color.
Table 2.
Characteristics of persons with more than one partner whose sex partners are all of the same race/ethnicity as the respondent (“assortative”) versus not all of the same race/ethnicity (“disassortative”), men who have sex with men, San Francisco, 2008 (N = 805)
| Variable | Men of color (N = 343) | White (N = 462) | ||||
|---|---|---|---|---|---|---|
| Assortative n (%) |
Disassortative n (%) |
χ2 | Assortative n (%) |
Disassortative n (%) |
χ2 | |
| Total | 25 | 318 | – | 231 | 231 | – |
| Age group (years) | ||||||
| 18–25 | 3 (12) | 72 (23) | 3.57 | 36 (16) | 5 (11) | 10.26* |
| 26–35 | 10 (40) | 142 (45) | 71 (31) | 59 (26) | ||
| 36–45 | 7 (23) | 71 (22) | 73 (32) | 66 (29) | ||
| 46+ | 5 (20) | 33 (10) | 51 (22) | 81 (35) | ||
| Sexual identity | ||||||
| Gay | 22 (88) | 277 (87) | 0.689 | 218 (94) | 210 (91) | 3.34 |
| Bisexual | 3 (12) | 33 (10) | 12 (5) | 18 (8) | ||
| Straight (and had male partners) | 0 | 4 (1) | 1 (<1) | 1 (<1) | ||
| Other (and had male partners) | 0 | 4 (1) | 0 | 2 (1) | ||
| Somewhat agree/strongly agree with: “I only feel comfortable going to gay bars and dance clubs in San Francisco that cater to people of the same race as I am” | 8 (32) | 68 (21) | 1.5 | 68 (29) | 41 (18) | 8.75* |
| All/Most friends are the same race/ethnicity as the respondent | 16 (64) | 90 (28) | 13.83* | 173 (75) | 125 (54) | 21.78* |
| Somewhat agree/strongly agree with: “I prefer to have sexual partner who are of the same race/ethnicity as I am” | 19 (76) | 148 (47) | 8.05* | 136 (59) | 78 (34) | 29.28* |
| Somewhat agree/strongly agree with: “It seems easier for me to meet sexual partners who are of the same race/ethnicity as I am” | 17 (68) | 141 (44) | 5.22 | 160 (69) | 109 (47) | 23.14* |
p < 0.01
Discussion
Our data describe a pattern of factors in San Francisco that potentially reflect in the relative sexual segregation of Black MSM from other groups of MSM. As in our previous survey conducted in 2004 (Berry et al. 2007), we found that Black MSM partner with other Black MSM at rates several-fold higher than would be expected by chance alone. Unlike our previous survey, we document potential reasons why this is occurring. First, Black MSM are the least preferred as sexual partners by other MSM. Second, Black MSM are perceived to be higher risk for HIV compared to other partners which may lead to men of other races avoid Black MSM as sexual partners. Third, Black MSM are counted less frequently among the friendships of other MSM. Fourth, Black MSM are ranked as the least easy to meet by other MSM. Fifth, Black MSM are perceived to be less welcome in the common venues for socializing among MSM in San Francisco. New to this study was the finding that White MSM were significantly less likely to have sexual partners of non-White race/ethnicities. We conclude that the combination of attitudes on the part of non-Black MSM, friendship and social networks that are less likely to include Black MSM, and the environments found in gay venues serve to separate Black MSM from other groups. While the numbers of intra-racial partnerships of Black MSM appears modestly raised from 8.5% expected to 29% observed, this three-fold effect may serve to intensify the interconnections within this minority population relative to other MSM populations enough to accelerate the spread of HIV to the appreciable degree witnessed.
While this pattern may tempt one to conclude that racism towards Black MSM is prevalent among MSM in our city, we call for extreme caution before using this label. Inherent to a definition of overt racism are beliefs that qualities are particular to certain races and that these qualities make one race superior or inferior to another. We purposely did not include questions on these aspects of racism in an effort to avoid the social desirability response bias that this line of questioning is likely to engender. Our first goal was to confirm the level of same race partnering among Black MSM seen 4 years earlier. Second, if still apparent, to explore whether the phenomenon was associated with the stated preferences of Black or non-Black MSM, perceptions on the epidemiology of HIV, prevailing social networks, the environment of the venues where MSM meet sexual partners, or combinations of these factors. We also wish to point to the quite high level of interracial partnering in our sample. Overall, 46% of partnerships described were interracial. Moreover, the interpretation of racism would be unfair without comparable data from other populations. While population-based data on the race/ethnicity of sexual partners are rare, the US Census estimated around 2% of marriages were interracial from 1970 through 1992 (US Census Bureau 1998). More recent estimates raise this to only 7% (Cary 2007). While same sex marriage is currently illegal in California, therefore precluding truly comparable figures for MSM, these estimates are many-fold lower than the interracial partnering we observed in our study. We do not believe our data should be bluntly interpreted as evidence of racism among MSM. Rather, we do interpret that our data capture less overt, more subtle factors stemming from the history and legacy of racism towards Blacks and segregation of Blacks in the US. Moreover, we acknowledge that our analyses only address racism towards Black MSM and does not address racism towards other racial groups.
We also interpret serious consequences of this legacy on the HIV epidemic through their effects on the sexual networks of Black MSM. Previous research highlighting the paradox of higher HIV prevalence among Black MSM despite lower levels of individual risk behavior suggest that the sexual networks of Black MSM create the circumstances for high incidence and prevalence of HIV. Our data are consistent with this hypothesis in that the sexual networks of Black MSM are constrained to smaller numbers and are therefore potentially more highly interconnected than other groups. Once HIV enters one part of such tightly connected network, it is likely to spread rapidly throughout. This rapid spread could also easily be greater if reports of sexual risk are lower than what is actually occurring and if the rates of partner change are greater. If the networks persist over time or across age groups, then the high prevalence of HIV could be sustained for a long time.
A major limitation to our study is that we do not characterize the complete sexual networks and their interconnections, rather our conclusions are inferred from individuals' responses about their partnerships. We also note potential limitations in the representativeness of the sample. There is no true Census of MSM populations in the US and therefore no gold standard to which to compare the make up of our sample. Nonetheless, the sampling method employed in our study is identical to our previous survey and to that used by the CDC for National HIV Behavioral Surveillance among MSM (MacKellar et al. 2007). Our data may therefore be reasonably consistent over time and could be compared to other cities included in the national system. Another limitation on interpretation is that some findings will be influenced by the relative numbers of MSM of different race/ethnicities. For example, the relative numbers of friends of different race/ethnicities and the ease in meeting such friends can be expected to be influenced by the relative numbers in each group. However, the analysis of partnerships corrects for these relative proportions, and this bias should not be the case for preferences, welcoming of venues, or perception of risk (the latter actually appears to mirrored the relative prevalence of HIV). Moreover, despite being the most predominant in numbers, Whites were not in fact counted most frequently among the friendships of Asian and Latino MSM. An additional limitation is our lack of measures that probed mediators and moderators of partner selection (e.g. fear of rejection, stigma, availability of partners of different races) thus we are limited to the current analyses. Future research on the topic of partner selection will need to include these types of measures. Finally, we also note the limitations in self-reported data. In American culture, questions on race are very sensitive and answers may be biased against responses that might be construed as “racist”. Such a bias may have resulted in diminishing or under-estimating many of the effects described here.
Such limitations and potential biases should not thwart the investigation of the factors that have created the unacceptable disparity in HIV incidence and prevalence by race/ethnicity in the US today. Given their potential relevance to HIV transmission, epidemiological surveys need to track questions on race/ethnicity that are, strangely, considered too sensitive or intrusive in such surveys. Further investigations will need to draw upon social-behavioral theories that will help frame and explain complex patterns of sexual mixing. For example, researchers might use social cognitive theory as a framework to better understand the interactions between individuals and those around them and those interactions' effect on sexual mixing (Bandura 2004). Social capital concepts may also be a useful framework to quantify the resources of individuals and their social networks and to explore how those resources influence sexual partnering (Bourdieu 1986). More difficult than describing such factors will be the means to intervene upon them. One finding, that social spaces are not welcoming to MSM of color raises the possibility of structural interventions to address the disparities in HIV infection. Group level interventions to reduce negative attitudes based on race might be implemented but these interventions to change preferences and attitudes will not be easy. Progress in interracial relationships in the US has been painstakingly slow, even since the decades following civil rights legislation. A starting point is to raise awareness among MSM that social barriers are having serious effects on the health and well-being on different parts the community. We believe that such a dialog needs to be infused with rigorous data rather than stereotypes and misperceptions.
Acknowledgments
We wish to thank John Newsome for his thoughtful feedback to earlier versions of this manuscript.
References
- Aral SO. Patterns of sexual mixing: Mechanisms for or limits to the spread of STIs. Sexually Transmitted Infections. 2000;76:415–416. doi: 10.1136/sti.76.6.415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandura A. Health promotion by social cognitive means. Health Education & Behavior. 2004;31(2):143–164. doi: 10.1177/1090198104263660. [DOI] [PubMed] [Google Scholar]
- Berry M, Raymond HF, McFarland W. Same race and older partner selection may explain higher HIV prevalence among black men who have sex with men. AIDS (London, England) 2007;21:2349–2350. doi: 10.1097/QAD.0b013e3282f12f41. [DOI] [PubMed] [Google Scholar]
- Bingham TA, Harawa NT, Johnson DF, Secura GM, MacKellar D, Valleroy LA. The effect of partner characteristics on HIV infection among African American men who have sex with men in the Young Men's Survey, Los Angeles 1999–2000. AIDS Education and Prevention. 2003;15(Suppl A):39–52. doi: 10.1521/aeap.15.1.5.39.23613. [DOI] [PubMed] [Google Scholar]
- Bourdieu P. The forms of capital. In: Richardson J, editor. Handbook of theory and research for the sociology of education. New York: Macmillan; 1986. [Google Scholar]
- Cary D. [2 Jan 2009];Interracial marriages surge across US. 2007 http://www.usatoday.com/news/health/2007-04-12-interracial-marriage_n.html.
- CDC. [6 Jan 2009];HIV/AIDS Surveillance Report. 2006 13(1) http://www.cdc.gov/hiv/topics/surveillance/resources/reports/2008supp_vol13no1/default.htm.
- CDC. HIV transmission among black college student and non-student men who have sex with men—North Carolina, 2003. Morbidity Mortality Weekly Report. 2004;53(32):731–734. [PubMed] [Google Scholar]
- CDC. HIV prevalence, unrecognized infection and HIV testing among men who have sex with men—five U.S. cities. June 2004–April 2005. Morbidity Mortality Weekly Report. 2005;54(24):597–601. [PubMed] [Google Scholar]
- Harawa NT, Greenland S, Bingham TA, Johnson DF, Cochran SD, Cunningham WE, et al. Associations of race/ethnicity with HIV prevalence and HIV-related behaviors among young men who have sex with men in 7 urban centers in the United States. Journal of Acquired Immune Deficiency Syndromes. 2004;35(5):526–536. doi: 10.1097/00126334-200404150-00011. [DOI] [PubMed] [Google Scholar]
- MacKellar DA, Valleroy L, Karon J, Lemp G, Janssen R. The Young Men's Survey: Methods for estimating HIV seroprevalence and risk factors among young men who have sex with men. Public Health Reports. 1996;111:138–144. [PMC free article] [PubMed] [Google Scholar]
- MacKellar D, Gallagher KM, Finlayson T, Sanchez T, Lansky A, Sullivan PS. Surveillance of HIV risk and prevention behaviors of men who have sex with men—a national application of venue based, time-space sampling. Public Health Reports. 2007;122(Suppl 1):39–47. doi: 10.1177/00333549071220S107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magnani R, Sabin K, Saidel T, Heckathorn D. Review of sampling hard-to-reach and hidden populations for HIV surveillance. AIDS. 2005;19:S67–S72. doi: 10.1097/01.aids.0000172879.20628.e1. [DOI] [PubMed] [Google Scholar]
- Meyers HF, Javanbakht M, Martinez M, Obedia S. Psychosocial predictors of risky sexual behaviors in African American men: Implications for prevention. AIDS Education and Prevention. 2003;15(Suppl A):66–79. doi: 10.1521/aeap.15.1.5.66.23615. [DOI] [PubMed] [Google Scholar]
- Millett GA, Peterson JL, Wolitski RJ, Stall R. Greater risk for HIV infection of black men who have sex with men: A critical literature review. American Journal of Public Health. 2006;96(6):1007–1019. doi: 10.2105/AJPH.2005.066720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Millett GA, Flores SA, Peterson JL, Bakeman R. Explaining disparities in HIV infection among black and white men who have sex with men: A meta-analysis of HIV risk behaviors. AIDS. 2007;21:2083–2091. doi: 10.1097/QAD.0b013e3282e9a64b. [DOI] [PubMed] [Google Scholar]
- San Francisco Department of Public Health. San Francisco HIV prevention plan. [6 Jan 2009];2004 http://www.sfhiv.org/files/plan_2004/2004_plan_ch_2.pdf.
- US Census Bureau. Race of wife by race of husband: 1960, 1970, 1980, 1991, and 1992. [2 Jan 2009];1998 http://www.2010census.biz/population/socdemo/race/interractab1.txt.
- Valleroy LA, MacKellar DA, Karon JM, Rosen DH, McFarland W, Shehan DA, et al. HIV prevalence and associated risks in young men who have sex with men. JAMA. 2000;284(2):198–204. doi: 10.1001/jama.284.2.198. [DOI] [PubMed] [Google Scholar]