

Abstract
This article reviews possible neural correlates of tinnitus, including an increase in rate, a decrease in rate, periodic activity, synchronous activity across neurons, and an edge between active and inactive neurons. We make some suggestions regarding how electrical current might alter these patterns of neural activity. For example, if tinnitus were represented with periodic neural activity, then electrical stimulation would need to disrupt this periodicity. Some cases of cochlear electrical stimulation are reviewed that show the tinnitus can be reduced or eliminated with cochlear electrical stimulation although it varies across individuals. Finally, after summarizing some key observations, we suggest some next steps to bring this into a clinical application.
Keywords: Tinnitus, cochlear implants, electrical stimulation
MECHANISMS OF TINNITUS AND OF INFLUENCING TINNITUS
“Sensorineural tinnitus probably has many different sources, and therefore finding any single treatment”1 is unlikely. The differences in perceptions and psychophysical behavior across subjects are large.2 Tinnitus can be perceived as a broadband noise (buzzing or humming), a tone (e.g., ringing), a frequency or amplitude modulated tone (crickets), or variations in between.3 Each of these percepts could be coded in neuron responses in a different manner.4
It seems reasonable that tinnitus must be coded (“perceived”) in the auditory temporal lobe, although it can have its source any place in the auditory system and may be altered by other systems as well.5-7 The importance of the central nervous system in tinnitus has been emphasized for decades. Evidence of central involvement include the following:8
When the 8th nerve ipsilateral to the tinnitus is cut, there is often no change in the perception of the tinnitus.
When an ipsilateral tinnitus is masked with noise in the same ear, patients sometimes remark that the tinnitus can appear in the other ear.
Ipsilateral tinnitus can be masked at comparable and at low levels in ipsilateral and contralateral ears.9
Tinnitus can be coded in the temporal lobe in the following manner:
Increased spontaneous activity10
Periodic spontaneous activity11
More neurons with similar best frequency following hearing loss14
To perceive tinnitus, certain kinds of analysis must be performed in the auditory temporal lobe, such as:
Determining that high levels of spontaneous activity are present among some neurons but not others.
Determining there are periodic time intervals between action potentials on individual neurons (equivalent to performing an interval histogram).
Detecting synchronous activity across neurons.
Wherever the coding of tinnitus takes place, it is likely it can be influenced by cochlea activity assuming the cochlea and auditory pathway are relatively intact. Although tinnitus activity is interpreted in the auditory cortex, in many cases it might originate in the cochlea from alterations of the spontaneous activity, including:
An increase in rate
A decrease in rate
Periodic activity
Synchronous activity across neurons
Edge between active and inactive neurons10
Changing this spontaneous activity is the likely mechanism by which electrical stimulation of the cochlea can affect tinnitus.
MECHANISMS OF INFLUENCING TINNITUS FROM THE COCHLEA
To change tinnitus, electrical activity in the cochlea must change the activity of auditory nerve fibers by a variety of mechanisms:
Decreasing activity
Increasing activity
Desynchronizing activity across nerve neurons
Interfering with periodic activity
Electrical stimulation with noise will not create uncorrelated activity across neurons because several nerves will fire synchronously to an electrical waveform.15 For example, when a periodic electrical pulse train is the stimulus, many auditory neurons will respond at the frequency of the stimulus. This is true at least at stimulus repetitions <∼3000 pulses per second (pps). Rubinstein et al16 proposed a high rate (>3000 pps) conditioner stimulus driving the nerve at rates beyond which it can follow the electrical waveform. At that point, activity across the neurons more closely follows a Poisson process.
If Tinnitus Results from a Decrease in Spontaneous Rate
If tinnitus resulted from a decrease in spontaneous rate, stimulating the auditory nerve directly with electrical current might increase the neural activity. If this created an ongoing activity that was more like the normal spontaneous rate that mirrors a Poisson process with a dead time, it could eliminate tinnitus. In addition to direct stimulation of the auditory nerve, electrical stimulation also might alter the resting state of remaining hair cells. If this resulted in an increase in neurotransmitter release, then the activity on the nerve might increase. Again, if the resultant ongoing activity was close to the normal spontaneous rate, it could eliminate tinnitus.
If Tinnitus Results from an Increase in Spontaneous Rate
If tinnitus resulted from an increase in spontaneous rate originating from a narrow region of the cochlea, then electrically stimulating a larger adjacent array of neurons might decrease the prominence of the tinnitus. Alternatively, continuous electrical stimulation of the hyperactive neurons might adapt the abnormal neurons so they could no longer transmit activity. This reduction in the prominence could eliminate the tinnitus. However, these neurons might no longer be available to code acoustic speech sounds (although they might be able to code speech with electrical stimulation).
If Tinnitus Results from a Periodic Activity in Spontaneous Rate
If tinnitus was coded on a small number of neurons that exhibit strong periodicity, electrical stimulation with noise could disrupt periodicity. The use of a conditioner stimulus16 might be able to accomplish this without audibility of the stimulation.
If Tinnitus Results from a Synchronous Activity in Spontaneous Rate across Neurons
Tinnitus might also result from synchronous activity across many nerve fibers. Electrical stimulation could disrupt this synchronous activity. The use of noise as a stimulus could disrupt or change the synchrony but might create its own (random) synchronous activity across neurons. Again, a conditioner stimulus might be able to do this without synchrony across neurons and without perception.
If Tinnitus Is the Edge between Active and Inactive Hair Cells
Another source of tinnitus might result from the difference in activity originating between the edge of normal (with normal spontaneous activity) and no spontaneous activity (e.g., a region with hair cell loss).10 This edge effect might result from a loss of inhibition from the inactive region. If the inactive region received electrical stimulation and activation of neural responses, the edge could be eliminated and the source of tinnitus might be removed.
REVIEW OF STUDIES USING ELECTRICITY TO REDUCE TINNITUS
Cochlear Implant Studies
Patients who have tinnitus and use cochlear implants to improve their speech perception often report a reduction in their tinnitus while they are using their speech processors. Several studies and reviews are available.17-31 These are some of the more noteworthy observations:
Some patients get tinnitus from receiving a cochlear implant.32
Some patients experience a total elimination of tinnitus after the cochlear implant surgery.22
Some patients report a reduction in their tinnitus only when the speech processor is turned on.19
Some patients report a reduction in their tinnitus after the speech processor is turned off.33
Some patients with bilateral tinnitus report a reduction of tinnitus on both sides after receiving a unilateral cochlear implant.34
Some patients report changes in the quality or pitch of their tinnitus.33
Extracochlear Stimulation
Kuk et al35 used a ball electrode at the eardrum in an attempt to reduce tinnitus. They used square, sine, and triangular waveforms at frequencies from 62 to 8000 Hz. In the screening phase, they first increased the level and noted changes in the patient’s tinnitus. Stimulation placebo trials were used initially but later abandoned because patients were aware if they were or were not being stimulated. Five of the 10 patients reported tinnitus reduction in the screening phase and were then tested in a second phase. Patients were required to judge loudness ratings and to mask their tinnitus acoustically in the nonstimulated ear before, during, and after the 10-minute electrical stimulation. Figure 1 shows data from five subjects for whom tinnitus could be reduced. This study is important because it used a psychoacoustical measurement that was the amount of masking required to mask the tinnitus to document the tinnitus reduction. Tinnitus reduction was accomplished without stimulus audibility in 60% of patients and the reduction was restricted to the stimulated ear in 75% of patients with bilateral tinnitus. Tinnitus was completely eliminated in three patients. The optimum stimuli varied among patients. The poststimulation reduction lasted from 40 seconds to 4 hours. Hazell et al36 and many others25 also reported being able to reduce tinnitus with a platinum ball electrode on the round window.
Figure 1.
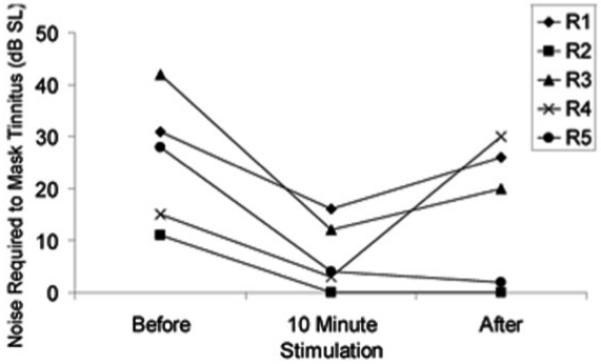
The amount of acoustic masking in the contralateral ear required to mask the tinnitus before, during, and after 10 minutes of electrical stimulation at the eardrum. Adapted from Kuk et al (1989). Individual results are shown for five subjects.
Intracochlear Stimulation
McKerrow et al37 used an inaudible 2- to 6-MHz carrier and a 30-minute broadband noise (stimulating the speech processor) at a comfortable level to stimulate six cochlear implant patients electrically. Five of six patients reported a rapid decrease to inaudible tinnitus. Figure 2 shows data from one patient implanted in the right ear. A 2- to 6-MHz inaudible electrical stimulation was presented to the right ear for ∼5 minutes. This reduced the tinnitus in both ears, but after ∼15 minutes the stimulation was no longer effective. A noise was then presented through the speech processor at a comfortable level, which also reduced the tinnitus in both ears. This remained effective for 20 minutes. When the electrical noise was turned off, the tinnitus returned gradually in the left ear but remained absent in the right ear for another 20 minutes. Similar findings were reported by Dauman et al38 and Dauman and Tyler.39
Figure 2.
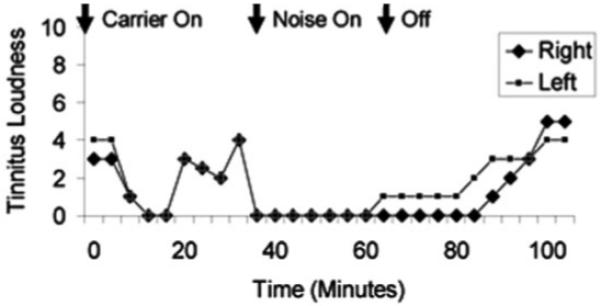
Intracochlear stimulation in a cochlear-implant patient. The loudness of the tinnitus is plotted for the right and left ear as a function of time during the trial. First a 2- to 6-MHz inaudible carrier is presented, followed by the application of a broadband noise stimulation to the speech processor (both presented unilaterally to the right ear). Tinnitus loudness was judged on a scale from 10, extremely loud, to 0, not heard. (Adapted from McKerrow et al, 1991.) SL, sensation level. R1 through R5, individual’s subject number.
Rubinstein et al16 and Rubinstein and Tyler25 used a high-frequency conditioner stimulus and were able to suppress tinnitus in subjects with cochlear implants and with round window electrodes. For some subjects it required several minutes of stimulation before the tinnitus was suppressed. Once tinnitus suppression was achieved, continuous stimulation with the conditioner stimulus sometimes became ineffective. Changes in the amplitude or repetition rate of the pulse train sometimes reinstated tinnitus suppression.
Figure 3 reports some previously unpublished results from one subject. Shown are both the loudness of the tinnitus and the loudness of the electrical pulse train stimulus. During ∼10 minutes of stimulation, the loudness of the tinnitus gradually decreased while the electrical stimulation was perceived at a soft loudness. When the stimulus was turned off, the tinnitus remained at a soft level for ∼5 minutes and then gradually returned to its initial level over the next 10 minutes. The electrical stimulation was turned on again, and once again the tinnitus reduced in loudness over ∼10 minutes; this time without any perception of the conditioner.
Figure 3.
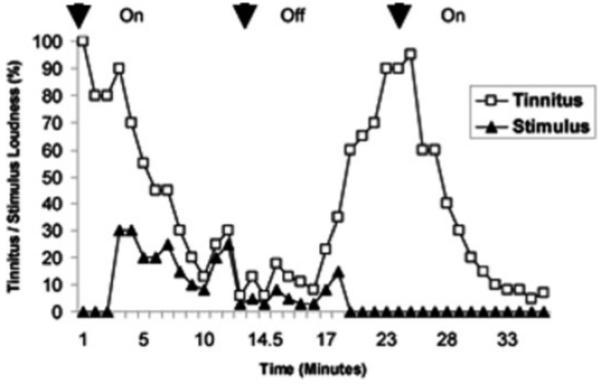
Tinnitus perception over time for one cochlear implant subject. The loudness of the tinnitus and of the high rate electrical pulse train is plotted as a function of time during the trial. The electrical stimulus was turned on, off, and then on again. Tinnitus loudness was judged on a scale from 100, the loudness of their normal tinnitus, to 0, not heard.
Summary of What Is Known
Although no large-scale studies have been reported to clarify the important parameters necessary to produce a clinical device to suppress tinnitus electrically, we have several leads:
Electrical stimulation of the cochlea can suppress tinnitus in some patients.
The optimal stimulus parameters are likely different for different subjects.
The optimum place in the cochlea for electrical stimulation of tinnitus is likely different for different subjects.
Unilateral stimulation of the cochlea usually produces a monaural tinnitus reduction, but some subjects report a binaural reduction of tinnitus.
It is possible to suppress tinnitus without perceiving the stimulation.
There is a possible advantage to a conditioning stimulus to suppress tinnitus without perceiving the electrical stimulus.
The effectiveness of electrical stimulation for tinnitus can decrease over time (over several minutes).
When the effectiveness of electrical stimulation decreases over time, the effectiveness can be recovered by changes to the stimulus parameters.
In some patients, tinnitus can be reduced for several minutes and even hours after the electrical stimulus is turned off.
Next Steps
Electrical stimulation of the cochlea can suppress tinnitus in some subjects. There appears to be great potential to develop a clinical device to treat tinnitus using this approach. The following are the next steps to accomplish this:
Studies are needed to determine what changes in the stimulus are needed to continuously suppress tinnitus during continuous stimulation.
Studies should include both placebo and replication trials to provide broader validity.
The long-term time course (hours) of tinnitus reduction during continuous stimulation needs to be better mapped out.
Studies with more subjects are needed to determine which patient characteristics identify subjects who will show significant tinnitus suppression from electrical stimulation of the cochlea.
Studies are needed to explore the effectiveness of short and long intracochlear electrodes as well as extracochlear stimulation.
ACKNOWLEDGMENTS
We wish to acknowledge grant support provided by the Tinnitus Research Consortium and the National Institutes of Health (NIH Grant 5R01DC005972-02). Richard Tyler is an Obermann Scholar at the Obermann Center for Advanced Studies at the University of Iowa.
Footnotes
Learning Outcomes: As a result of this activity, the participant will be able to (1) describe some of the possible mechanisms of the coding of tinnitus in the cochlea, and (2) describe how electrical suppression might alter tinnitus.
REFERENCES
- 1.Tyler RS, Babin RW. Tinnitus. In: Cummings CW, Fredrickson JM, Harker L, Krause CJ, Schuller DE, editors. Otolaryngology Head and Neck Surgery. CV Mosby; St. Louis, MO: 1986. pp. 3201–3217. [Google Scholar]
- 2.Tyler RS. The psychoacoustical measurement of tinnitus. In: Tyler RS, editor. Tinnitus Handbook. Singular; San Diego, CA: 2000. pp. 149–179. [Google Scholar]
- 3.Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord. 1990;55:439–453. doi: 10.1044/jshd.5503.439. [DOI] [PubMed] [Google Scholar]
- 4.Tyler RS. Neurophysiological Models, Psychological Models, and Treatments for Tinnitus. In: Tyler RS, editor. Tinnitus Treatment: Clinical Protocols. Thieme; New York, NY: 2006. pp. 1–22. [Google Scholar]
- 5.Cacace AT, Lovely TJ, Winter DF, Parnes SM, McFarland DJ. Auditory perceptual and visual-spatial characteristics of gaze-evoked tinnitus. Audiology. 1994;33:291–303. doi: 10.3109/00206099409071889. [DOI] [PubMed] [Google Scholar]
- 6.Kaltenbach JA. Neurophysiologic mechanisms of tinnitus. J Am Acad Audiol. 2000;11(3):125–137. [PubMed] [Google Scholar]
- 7.Shore SE. Sensory nuclei in tinnitus. In: Snow J, editor. Tinnitus: Theory and Management. BC Decker; Hamilton, Ontario, Canada: 2004. [Google Scholar]
- 8.Tyler RS. In: Evered D, Lawrenson G, editors. Invited discussant. Tinnitus; Tinnitus (Ciba Foundation Symposium 85); London, UK: Pitman. 1981.pp. 136–137. [Google Scholar]
- 9.Tyler RS, Conrad-Armes D. Masking of tinnitus compared to the masking of pure tones. J Speech Hear Res. 1984;27:106–111. doi: 10.1044/jshr.2701.106. [DOI] [PubMed] [Google Scholar]
- 10.Kiang NYS, Moxon EC, Levine RA. Auditory-nerve activity in cats with normal and abnormal cochleas. In: Wolstenholme GEW, Knight J, editors. Sensorineural Hearing Loss. Churchill Livingston; London, UK: 1970. pp. 241–268. [DOI] [PubMed] [Google Scholar]
- 11.Eggermont JJ. Tinnitus: some thought about its origin. J Laryngol Otol. 1984;(suppl 9):31. [Google Scholar]
- 12.Eggermont JJ. Psychological mechanisms and neural models. In: Tyler RS, editor. Tinnitus Handbook. Singular; San Diego, CA: 2000. pp. 85–122. [Google Scholar]
- 13.Moller AR. Pathophysiology of tinnitus. Ann Otol Rhinol Laryngol. 1984;93:39–44. [PubMed] [Google Scholar]
- 14.Salvi RJ, Wang J, Powers NJ. Plasticity and reorganization in the auditory brainstem: implications for tinnitus. In: Reich GE, Vernon JE, editors. Proceedings of the Fifth International Tinnitus Seminar. American Tinnitus Association; Portland, OR: 1996. pp. 457–466. [Google Scholar]
- 15.Abbas PJ. Electrophysiology. In: Tyler RS, editor. Cochlear Implants: Audiological Foundations. Singular; San Diego, CA: 1993. pp. 317–355. [Google Scholar]
- 16.Rubinstein JT, Tyler RS, Johnson A, Brown CJ. Electrical suppression of tinnitus with high-rate pulse trains. Otol Neurotol. 2003;24:478–485. doi: 10.1097/00129492-200305000-00021. [DOI] [PubMed] [Google Scholar]
- 17.Ito J, Sakakihara J. Suppression of tinnitus by cochlear implantation. Am J Otolaryngol. 1994;15:145–148. doi: 10.1016/0196-0709(94)90064-7. [DOI] [PubMed] [Google Scholar]
- 18.Demajumdar R, Stoddart R, Donaldson I, Proops DW. Tinnitus, cochlear implants and how they affect patients. J Laryngol Otol Suppl. 1999;24:24–26. [PubMed] [Google Scholar]
- 19.Tyler RS, Kelsay D. Advantages and disadvantages reported by some of the better cochlear-implant patients. Am J Otol. 1990;11:282–289. [PubMed] [Google Scholar]
- 20.Tyler RS. Tinnitus in the profoundly hearing-impaired and the effects of cochlear implants. Ann Otol Rhinol Laryngol Suppl. 1995;165:25–30. [PubMed] [Google Scholar]
- 21.Gibson WPR. In: Aran JM, Dauman R, editors. The effect of electrical stimulation and cochlear implantation on tinnitus; Proceedings of the Fourth International Tinnitus Seminar, Bordeaux, 1991; Amsterdam, The Netherlands/New York, NY: Kugler. 1992.pp. 403–408. [Google Scholar]
- 22.Kim HN, Shim YJ, Kim YM, Kim ES. In: Reich GE, Vernon J, editors. Effect of electrical stimulation on tinnitus in the profoundly deaf; Proceedings of the Fifth International Tinnitus Seminar; Portland, OR: American Tinnitus Association. 1995.pp. 508–517. [Google Scholar]
- 23.Dauman R. Electrical stimulation for tinnitus suppression. In: Tyler RS, editor. Tinnitus Handbook. Singular; San Diego, CA: 2000. pp. 377–398. [Google Scholar]
- 24.Quaranta N, Wagstaff S, Baguley DM. Tinnitus and cochlear implantation. Int J Audiol. 2004;43:245–251. doi: 10.1080/14992020400050033. [DOI] [PubMed] [Google Scholar]
- 25.Rubinstein JT, Tyler RS. Electrical suppression of tinnitus. In: Snow J, editor. Tinnitus: Theory and Management. BC Decker; Hamilton, Ontario, Canada: 2004. pp. 326–335. [Google Scholar]
- 26.Portmann D, Felix F, Negrevergne M, et al. Bilateral cochlear implantation in a patient with long-term deafness. Rev Laryngol Otol Rhinol (Bord) 2007;128(1-2):65–68. [PubMed] [Google Scholar]
- 27.Dobie RA, Hoberg KE, Rees T. Electrical tinnitus suppression: a double-blind crossover study. Otolaryngol Head Neck Surg. 1986;95:319–323. doi: 10.1177/01945998860953P110. [DOI] [PubMed] [Google Scholar]
- 28.Matsushima J, Sakai N, Takeichi N, et al. Implanted electrical tinnitus suppressor. In: Reich GE, Vernon JA, editors. Proceedings of the Fifth International Tinnitus Seminar. American Tinnitus Association; Portland, OR: 1996. pp. 329–334. [Google Scholar]
- 29.Okusa M, Shiraishi T, Kubo T, Matsunaga T. Tinnitus suppression by electrical promontory stimulation in sensorineural deaf patients. Acta Otolaryngol Suppl. 1993;501:54–58. doi: 10.3109/00016489309126215. [DOI] [PubMed] [Google Scholar]
- 30.Ruckenstein MJ, Hedgepeth C, Rafter KO, Montes ML, Bigelow DC. Tinnitus suppression in patients with cochlear implants. Otol Neurotol. 2001;22(2):200–204. doi: 10.1097/00129492-200103000-00014. [DOI] [PubMed] [Google Scholar]
- 31.Miyamoto RT, Bichey BG. Cochlear implantation for tinnitus suppression. Otolaryngol Clin North Am. 2003;36(2):345–352. doi: 10.1016/s0030-6665(02)00165-2. [DOI] [PubMed] [Google Scholar]
- 32.Kou BS, Ship DB, Nedzelski JM. Subjective benefits reported by adult Nucleus 22-channel cochlear implant users. J Otolaryngol. 1994;23(1):8–14. [PubMed] [Google Scholar]
- 33.Souliere CR, Jr, Kileny PR, Zwolan TA, Kemink JL. Tinnitus suppression following cochlear implantation. A multifactorial investigation. Arch Otolaryngol Head Neck Surg. 1992;118(12):1291–1297. doi: 10.1001/archotol.1992.01880120017004. [DOI] [PubMed] [Google Scholar]
- 34.Zwolan TA, Kileny PR, Souliere CR, Kemink JL. In: Aran J-M, Dauman R, editors. Tinnitus suppression following cochlear implantation; Tinnitus 91: Proceedings of the Fourth International Tinnitus Seminar; Amsterdam, The Netherlands: Kugler. 1992.pp. 423–426. [Google Scholar]
- 35.Kuk FK, Tyler RS, Rustad N, Harker LA, Tye-Murray N. Alternating current at the eardrum for tinnitus reduction. J Speech Hear Res. 1989;32:393–400. doi: 10.1044/jshr.3202.393. [DOI] [PubMed] [Google Scholar]
- 36.Hazell JWP, Meerton LJ, Conway MJ. Electrical tinnitus suppression (ETS) with a single channel cochlear implant. J Laryngol Otol Suppl. 1989;18:39–44. [PubMed] [Google Scholar]
- 37.McKerrow WS, Schreiner CE, Snyder RL, Merzenich MM, Toner JG. Tinnitus suppression by cochlear implants. Ann Otol Rhinol Laryngol. 1991;100:552–558. doi: 10.1177/000348949110000706. [DOI] [PubMed] [Google Scholar]
- 38.Dauman R, Tyler RS, Aran JM. Intracochlear electrical tinnitus reduction. Acta Otolaryngol. 1993;113:291–295. doi: 10.3109/00016489309135811. [DOI] [PubMed] [Google Scholar]
- 39.Dauman R, Tyler RS. Tinnitus suppression in cochlear implant users. Adv Otorhinolaryngol. 1993;48:168–173. doi: 10.1159/000422577. [DOI] [PubMed] [Google Scholar]