

Abstract
The current study tested the assumption that bilinguals with dementia regress to using primarily the dominant language. Spanish-English bilinguals with probable Alzheimer's disease (AD; n=29), and matched bilingual controls (n=42) named Boston Naming Test pictures in their dominant and nondominant languages. Surprisingly, differences between patients and controls were larger using dominant-language than nondominant-language naming scores, and bilinguals with AD were either more likely than controls (in English-dominant bilinguals), or equally likely (in Spanish-dominant bilinguals), to name some pictures in the nondominant language that they could not produce in their dominant language. These findings suggest that dominant language testing may provide the best assessment of language deficits in bilingual AD, and argue against the common notion that the nondominant language is particularly susceptible to dementia. The greater vulnerability of the dominant language may reflect the increased probability of AD affecting richer semantic representations associated with dominant compared to nondominant language names.
The ability to proficiently use more than one language – or bilingualism – has been in the spotlight of attention recently among psychologists attempting to understand the relationship between language and cognition. Interest in the topic has also extended itself beyond the academic literature into the popular press because of reports that bilingualism improves some aspects of executive functioning (e.g., Bialystok, Craik, & Luk, 2008; Costa, Hernández, & Sebastián-Gallés, 2008; Prior & MacWhinney, in press), and that bilingualism or multilingualism may protect against age- and dementia-related decline in cognitive functioning (e.g., Bialystok, Craik, Klein, & Viswanathan, 2004; Bialystok, Craik, & Freedman, 2007; Chertkow, Whitehead, Phillips, Wolfson, Atherton, & Bergman, in press; Kavé, Eyal, Shorek, & Cohen-Mansfield, 2008). Despite this considerable interest in bilingualism, only a very small number of studies have addressed more basic questions concerning the joint consequences of bilingualism and dementia for language processing. Information on this topic has been described as “extremely scarce” by experts in the field (Ardila, 2007, pp. 151), even though aging bilinguals at risk for developing Alzheimer's disease (AD) are rapidly increasing in numbers.
A recent report from the Alzheimer's Association (2004) warns that dementia is a
“…looming unrecognized public health crisis in Hispanic/Latino communities in the United States. During the first half of the 21st century, the number of Hispanic elders suffering from Alzheimer's and related dementias could increase more than six-fold, from fewer than 200,000 today to as many as 1.3 million by 2050.”
The report further outlines that these projections may underestimate the problem because they assume the same prevalence of dementia in Hispanics as in the general population when in fact there is evidence that Hispanics are at greater risk for developing the disease compared to other ethnic and racial groups (Tang et al., 1998; 2001; Fitten, 2001). Because many Hispanics speak both English and Spanish, these statistics indicate a great need for research into the combined effects of bilingualism and Alzheimer's disease on cognitive test performance. Information about the presentation and progression of impairments in bilingual AD is needed to correctly diagnose, and to effectively treat and manage, AD in bilinguals. This simultaneously presents neuropsychologists with challenges and an opportunity to investigate how the cognitive system maintains two languages when faced with dementia. In the current study we take a step towards addressing this important problem while also taking the opportunity to consider the possible theoretical implications of this work for understanding the nature of cognitive impairments in AD and the cognitive mechanisms underlying bilingualism.
Information about the assessment of language impairments in bilinguals comes mostly from the study of children. A useful approach for testing vocabulary knowledge in bilingual children is to allow them to use names in either language (Umbel, Pearson, Fernández, & Oller, 1992; sometimes called “conceptual scoring,” Bedore, Peña, García, & Cortez, 2005; or “composite scoring,” Kohnert, Hernandez, & Bates, 1998). Bilingual children obtain higher vocabulary scores when given the option of using either language because they encounter certain things mostly in the context of one language and other things mostly in the context of the other language (e.g., they might know frying pan only in the home-spoken language where most cooking takes place, but ruler only in the school-spoken language where most measuring takes place; Grosjean, 2008). Thus, allowing children to use names in either-language provides a more accurate estimation of their semantic knowledge (Pearson, Fernández, & Oller, 1993). Interestingly, adult bilinguals (who presumably have fully developed systems of semantic knowledge) exhibit a similar pattern of results on picture naming tests. That is, young adult bilinguals (Kohnert, et al., 1998; Gollan & Silverberg, 2001) and aging bilinguals (Gollan, Fennema-Notestine, Montoya, & Jernigan, 2007), can name a greater number of pictures when credited for pictures named in the nondominant language but not in the dominant language. The persistence of an either-language benefit in bilingual adults suggests that in addition to providing a more accurate representation of conceptual familiarity, the either-language option provides bilingual speakers with a way around some of the challenges associated with being bilingual (i.e., needing to learn, remember, and retrieve roughly twice as many names as monolinguals). Even after having had a long life-time in which to learn two names for each concept (one in each language; Gollan, Montoya, Cera, & Sandoval, 2008), elderly bilinguals still may not use words in each language frequently enough to have translation equivalents readily accessible for most concepts.
Some open questions with respect to bilingual AD are: (a) which scoring method will reveal the greatest difference between patients and controls (either-language, dominant-language, nondominant language, or both languages), (b) will bilinguals with AD also benefit from the either-language scoring method (i.e., will they name more pictures with the alternative scoring method), and (c) will the same pattern of results be obtained for different types of bilinguals. Studies investigating the neural correlates of bilingual language processing reveal that proficient and relatively balanced bilinguals activate the same brain regions when using each of their languages, and that this seems to be true for both early and late bilinguals (i.e., bilinguals who acquired their two languages relatively early and those who acquired their second language later in life) so long as they are proficient in both languages (e.g., for a review see Abutalebi & Green, 2007). In contrast, bilinguals with more limited second language proficiency reveal differences in the brain regions activated in each language, most frequently with the nondominant language revealing greater degrees of activation, or activation of regions not used in processing the dominant language (e.g., Abutalebi et al., 2008; Chee et al., 2001; De Bleser et al., 2003 Hernandez, 2009; for reviews see Abutalebi & Green, 2007; Perani & Abutalebi, 2005). Both imaging (see review by Abutalebi, Cappa, & Perani, 2005) and behavioral studies (e.g., Gollan et al., 2008; Kohnert et al., 1998) seem to suggest that the degree of proficiency in the two languages matters relatively more than age-of-acquisition of the two languages. Thus, we focus largely on the contrast between the dominant and nondominant languages. However, where possibly relevant we also consider the implications of differences between early and late bilinguals.
A common assumption about aging bilinguals, and particularly concerning dementia in bilingualism, is that there is regression to the language that is both first-learned and dominant (Ardila & Ramos, 2008), that there is reduced control over language choice and switching (De Santi, Obler, Sabo-Abramson, & Goldberger, 1989; Hernandez & Kohnert, 1999; Hyltenstam & Stroud, 1994), and reduced ability to maintain fluency in two languages (Hyltenstam & Obler, 1989; Obler, Albert, & Lozowick, 1986; for a different view see Gollan et al., 2008). These views are supported by caregiver reports of increasing preference for the first-learned and dominant language, and increased unintended intrusions of this language into the second-learned and non-dominant language with dementia progression (Mendez, Perryman, Pontón, & Cummings, 1999). Because retrieval of words in a less dominant language is more difficult and less automatic than retrieval in the dominant language, these ideas are also consistent with the notion that AD leads to deficits in effortful retrieval (Balota, Watson, Duchek, & Ferraro, 1999; McGlinchey-Berroth & Milberg, 1993; Ober, Shenaut, & Reed, 1995; Nebes, Martin, & Horn, 1984).
The either-language benefit only occurs to the extent that bilinguals can name some pictures in their nondominant language that they cannot name in their usually more dominant language. Thus, if bilinguals with AD have reduced ability to produce a nondominant language, they may also be less likely to benefit from the either-language scoring method. Furthermore, direct comparisons of naming ability in the two languages should reveal greater sensitivity to dementia for nondominant language than dominant language naming scores. Consistent with these notions, a study of English-Afrikaans bilinguals who were instructed that they could use either language during a verbal fluency task found that bilinguals with AD did not switch-languages at all, whereas matched elderly controls chose to switch languages during the fluency trial (De Picciotto & Friedland, 2001; but note that use of either-language does not increase fluency scores; see also Gollan, Montoya, & Werner, 2002).
An alternative possibility is that the dominant language would reveal larger differences between patients and controls than the nondominant language. It may seem counterintuitive to predict that a relatively easier task (retrieval in a dominant language) would produce a greater difference between bilinguals with and without AD than a more difficult task (retrieval in a nondominant language). However, such a pattern of results might be expected if lexical representations in the dominant language are more richly connected to conceptual representations than the nondominant language. If AD primarily reduces the integrity of semantic representations (Butters, Granholm, Salmon, Grant, & Wolfe, 1987; Cherktow & Bub, 1990), then the existence of richer connections from concepts to words in the dominant language may also make it more likely that one (or more) of these connections will be disrupted by brain damage, and therefore the dominant language would be more sensitive to AD related changes than the nondominant language. The notion of more elaborate connections between concepts and the dominant language is supported by studies which demonstrated greater activation of semantic representations with increasing degrees of language proficiency (e.g., Talamas, Kroll, & Dufour, 1999; for review see Kroll & Tokowicz, 2005). It also makes sense to assume that the dominant language which has been used relatively more often will be associated with a greater diversity of contexts (Adelman, Brown, & Quesada, 2006), and with a larger number of automatic associations than the nondominant language (for similar ideas see Finkbeiner, Forster, Nicol, & Nakamura, 2004; Wang & Forster, in press). On this view, dominant language words are easier to produce in part because meaning representations provide a greater number of connections to dominant language word forms than to nondominant language word forms. Interestingly, if dominant-language names are more sensitive to decline associated with AD, then the either-language benefit would be expected to increase in bilinguals with AD. That is, bilinguals with AD should be more likely to benefit from the either-language scoring alternative than healthy controls.
A recent study of timed picture naming comparing young and older bilinguals produced some results that seem in line with this prediction. In this study bilinguals were instructed to name pictures using “whatever language comes to mind” thereby inviting voluntary language switching (Gollan & Ferreira, 2009). Previous studies of cued language switches revealed significant age-related decline in language switching ability (i.e., larger language switching costs in older relative to young bilinguals; Hernandez & Kohnert, 1999). In contrast, when switching voluntarily older bilinguals exhibited a pattern of language switch costs that greatly resembled that seen in younger bilinguals (voluntary switching also allowed unbalanced young bilinguals to function more like balanced young bilinguals). Moreover, older bilinguals chose to switch languages voluntarily as often as younger bilinguals, implying no age-related decline in planning and producing voluntary language switches. These observations suggest that the either-language option may obscure some of the consequences of age-related decline in language control. An analogous situation may occur in the comparison of aging bilinguals with and without AD if the either-language scoring method produces relatively smaller difference between patients and controls thereby obscuring differences between them when compared with dominant-language only naming scores.
Predictions can be further refined to consider different types of bilinguals. The either-language scoring benefit may be modulated by language dominance. In children, Spanish-dominant bilinguals tended to benefit relatively more from the option to use either-language than English-dominant bilinguals (e.g., Bedore et al., 2005). In aging bilinguals it has not yet been established whether older bilinguals who prefer to be tested in English will exhibit an either-language scoring benefit on the Boston Naming Test (BNT; in Gollan et al., 2007 most of the balanced bilinguals were Spanish-dominant and unbalanced bilinguals benefited less from the either-language scoring). Cognitively intact Spanish-dominant bilinguals in the USA may be more likely to benefit from the either-language scoring method because their immersion in English leads them to know some words in English that they do not know in Spanish (see discussion in Acevedo & Loewenstein, 2007; Bialystok & Craik, 2007; Gollan & Fennema-Notestine, 2007). Conversely, with the onset of AD Spanish-dominant bilinguals may be less likely to benefit from recent exposures to the nondominant language in the immersion context because of their episodic memory impairments, and this would lead to a reduced either-language scoring benefit relative to matched controls. Thus, in the current study we divided participants by language preference, and consider the implications of any differences in results obtained by language group.
Summarizing the questions of interest, we asked which language would reveal greater differences between patients and controls. Based on the notion that AD introduces retrieval deficits, and the fact that retrieval is more effortful in a nondominant language, it would be predicted that the nondominant language should produce the greatest difference between patients and controls, and that bilinguals with AD should be less likely to benefit from the either-language scoring option. Further refining this prediction, different types of bilinguals might exhibit a different pattern of relative language impairments in AD. For example, if the nondominant language seems to be more affected by AD than the dominant language, but only in bilinguals who acquired their non-dominant language relatively late in life, this would support the proposal that late-learned languages are represented more episodically (Jiang & Forster, 2001; Paradis, 1994; Ullman, 2001; 2004) and therefore are also more sensitive to the cognitive impairments associated with AD (which has profound effects on episodic memory).
In contrast, based on the hypothesis that semantic representations are more richly connected with words in the dominant language, the dominant language should produce the greatest difference between patients and controls, and bilinguals with AD might show an increased benefit from the either-language scoring procedure. Finally, we anticipated possible differences between early bilinguals immersed in their dominant language versus late bilinguals immersed in their nondominant language. A similar pattern of results across these different bilingual types would be consistent with suggestions that language-dominance is the critical factor for determining how AD affects the maintenance of bilingualism.
Methods
Participants
Seventy-one bilinguals (29 with probable AD, and 42 cognitively healthy) were recruited for participation from the University of California, San Diego (UCSD) Alzheimer's Disease Research Center (ADRC). Participants were diagnosed as either cognitively intact or as having probable AD by two senior staff neurologists using criteria developed by the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer's Disease and Related Disorders Association (ADRDA; McKhann, et al., 1984) based on medical, neurological, and neuropsychological evaluations and a number of laboratory tests. Language dominance was determined by asking participants about their language history; participants who felt they would obtain higher neuropsychological test scores if tested primarily in English were classified as English-dominant and participants who preferred to be tested in Spanish were classified as Spanish-dominant. There were sixteen (9 female) English-dominant bilinguals with a diagnosis of probable AD, and twenty-two cognitively healthy matched controls (14 females). There were thirteen (9 females) Spanish-dominant bilinguals with a diagnosis of probable AD, and twenty (13 females) cognitively healthy matched controls.
Tables 1 and 2 provide participant characteristics and language history questionnaire responses for English-dominant and Spanish-dominant bilinguals respectively. The right side of each table displays t-tests for differences between bilinguals with AD and matched controls for each characteristic reported. Although on average the English-dominant bilinguals with AD were in a less advanced stage of disease than the Spanish-dominant bilinguals with AD, in both language-dominance groups, the majority of bilinguals with AD were in a mild stage (with MMSE scores between 19-25; 38% of English-dominant bilinguals with AD, and 54% of Spanish-dominant bilinguals with AD), or a moderate stage of progression at the time of testing (with MMSE scores between 12-18; 25% of English-dominant bilinguals with AD, and 38% of Spanish-dominant bilinguals with AD). Only one participant in each dominance group was in a severe stage of dementia (with MMSE scores of 7 and 8). The English-dominant group also included five participants who were in a very-mild stage of disease (with MMSE scores between 26-29).
Table 1. Characteristics of participants who prefer to be tested in English.
| Bilinguals with Alzheimer's Disease | Bilingual Controls | |||||||
|---|---|---|---|---|---|---|---|---|
| na | M | SD | na | M | SD | t | p | |
| Age | 16 | 74.8 | 9.5 | 22 | 74.4 | 9.8 | < 1 | 0.90 |
| Education | 16 | 14.4 | 3.0 | 22 | 13.6 | 2.7 | < 1 | 0.43 |
| DRSb | 16 | 109.7 | 16.9 | 22 | 136.3 | 5.2 | 7.00 | < .01 |
| MMSEc | 16 | 21.6 | 6.4 | 22 | 29.7 | 0.6 | 5.90 | < .01 |
| Age of Regular English Use | 15 | 3.6 | 7.5 | 22 | 3.7 | 3.8 | < 1 | 0.96 |
| Percent Daily English use | 16 | 90.3 | 13.4 | 22 | 84.5 | 20.8 | < 1 | 0.34 |
| English Speakingd | 16 | 6.6 | 0.6 | 22 | 6.7 | 0.6 | < 1 | 0.59 |
| English Readingd | 16 | 6.7 | 0.7 | 22 | 6.6 | 0.7 | < 1 | 0.93 |
| English Writingd | 16 | 6.5 | 1.1 | 22 | 6.5 | 1.0 | < 1 | 0.93 |
| English Comprehensiond | 16 | 6.7 | 0.8 | 22 | 6.8 | 0.5 | < 1 | 0.60 |
| Spanish Speakingd | 16 | 5.0 | 1.6 | 22 | 4.7 | 1.5 | < 1 | 0.56 |
| Spanish Readingd | 16 | 4.4 | 2.3 | 22 | 4.2 | 1.8 | < 1 | 0.83 |
| Spanish Writingd | 16 | 4.1 | 2.3 | 22 | 3.9 | 1.9 | < 1 | 0.71 |
| Spanish Comprehensiond | 16 | 5.5 | 1.5 | 22 | 5.3 | 1.5 | < 1 | 0.71 |
The number varies from characteristic to characteristic because of missing data.
The Dementia Rating Scale (DRS; Mattis, 1988)
The Mini Mental State Examination (MMSE; Folstein, Folstein & McHugh, 1975)
Proficiency level based on self-ratings using a scale of 1-7 with 1 being “little to no knowledge” and 7 being “like a native speaker.”
Table 2. Characteristics of participants who prefer to be tested in Spanish.
| Bilinguals with Alzheimer's Disease | Bilingual Controls | |||||||
|---|---|---|---|---|---|---|---|---|
| na | M | SD | na | M | SD | t | p | |
| Age | 13 | 76.7 | 6.5 | 20 | 74.4 | 5.0 | 1.14 | 0.26 |
| Education | 13 | 7.5 | 5.1 | 20 | 9.5 | 3.4 | 1.35 | 0.19 |
| DRSb | 13 | 100.9 | 18.2 | 20 | 134.9 | 5.3 | 7.88 | < .01 |
| MMSEc | 13 | 18.2 | 4.2 | 20 | 29.8 | 0.6 | 12.25 | < .01 |
| Age of Regular English Use | 10 | 33.1 | 13.9 | 20 | 31.0 | 18.8 | < 1 | 0.75 |
| Percent Daily English use | 11 | 16.4 | 30.8 | 20 | 13.6 | 17.9 | < 1 | 0.76 |
| English Speakingd | 9 | 3.1 | 2.1 | 19 | 3.9 | 1.6 | 1.12 | 0.28 |
| English Readingd | 9 | 3.2 | 2.2 | 19 | 4.3 | 1.8 | 1.33 | 0.19 |
| English Writingd | 9 | 2.8 | 2.3 | 19 | 3.5 | 1.9 | < 1 | 0.38 |
| English Comprehensiond | 9 | 3.6 | 2.5 | 19 | 4.4 | 1.6 | 1.08 | 0.29 |
| Spanish Speakingd | 11 | 6.4 | 0.8 | 20 | 6.7 | 0.6 | 1.35 | 0.19 |
| Spanish Readingd | 11 | 5.2 | 1.9 | 20 | 6.7 | 0.5 | 3.35 | < .01 |
| Spanish Writingd | 11 | 5.6 | 1.9 | 20 | 6.6 | 0.7 | 2.15 | 0.04 |
| Spanish Comprehensiond | 11 | 6.4 | 0.9 | 20 | 6.8 | 0.4 | 1.83 | 0.08 |
The number varies from characteristic to characteristic because of missing data.
The Dementia Rating Scale (DRS; Mattis, 1988)
The Mini Mental State Examination (MMSE; Folstein, Folstein & McHugh, 1975)
Proficiency level based on self-ratings using a scale of 1-7 with 1 being “little to no knowledge” and 7 being “like a native speaker.”
Within each language-dominance group participants were matched for age and years of education anchored by degree level completed (e.g., 12 years for high school, 16 for a BA, 18 for Master's degree, etc). All participants in the current study reported learning Spanish at home as the native language. Within each language-dominance group participants did not differ significantly in self-reported age of acquisition of English (defined as the age at which regular use of English began), current daily use of English, or in self-rated ability to speak English and Spanish (for further details about the aging bilingual population at the ADRC see Gollan, et al., 2007; 2008; Gollan & Ferreira, 2009). English-dominant bilinguals with and without AD were well matched on all participant characteristics (most ts < 1; see Table 1). Among Spanish-dominant bilinguals, those with AD reported slightly but not significantly lower years of education, though their self-reported ability to read and write in Spanish was significantly lower than matched controls (see Table 2) possibly reflecting disease related decline and/or differences in quality of education (not detected by the years-of-education measure). We consider these subtle but possibly important differences in our discussion of the results below. The study procedures conformed to Federal guidelines for the protection of human subjects and were approved by the UCSD Institutional Review Board. Informed consent was obtained from cognitively intact controls and from patients and caregivers (usually the next of kin) prior to neuropsychological testing and after the procedures of the study had been fully explained.
Materials
Participants named pictures from the Boston Naming Test (Kaplan et al., 1983). Approximately half (32) of the participants named all 60 pictures (13 controls and 4 patients from the English-dominant group; 14 controls and 1 patient from the Spanish-dominant group), and the other participants (35) named just the odd numbered items (9 controls and 12 AD from the English-dominant group; 5 controls and 9 AD from the Spanish-dominant group). A small number of Spanish-dominant participants (1 control and 3 AD) named 30 items from the Uniform Data Set (UDS) version of the BNT designed for use with Spanish speakers (Weintraub et al., 2009; Acevedo et al., 2009).
Procedure
Participants were tested either in their homes or at the ADRC by a proficient Spanish-English bilingual psychometrist who instructed them to name pictures in their dominant language. Subsequently, participants were tested with the same pictures again, but this time attempting to name them in their less-dominant language. The psychometrist recorded naming accuracy during testing. Naming trials were administered according to the standardized BNT instructions except that participants were asked to name all items (i.e., testing began at item #1 not in the middle of the test), and testing was not discontinued after 8 failed naming trials. For those tested on the 30 items versions, testing also began at item #1 but was discontinued after 6 failed naming trials.
Results
For each bilingual we calculated the proportion of pictures named correctly in four different ways: 1) dominant-language correct, 2) nondominant language correct, 3) either-language correct (pictures named correctly in at least one of the two languages), and 4) both languages correct (pictures named correctly in both languages). For several reasons we report the results separately by language dominance groups. First, the BNT was designed for English and is not designed for use with Spanish speakers. The use of a discontinuation rule (sometimes employed here; see above) is not appropriate in such cases given that the ordering of item-difficulty does not always match between languages (e.g., Kohnert et al, 1998). Additionally, the English-dominant bilinguals were immersed in their dominant language whereas the Spanish-dominant bilinguals were immersed in their nondominant language. Ideally, early and late bilinguals should be matched for language dominance (either both should be English-dominant or both should be Spanish-dominant); however, it is rare (if not impossible) to find bilinguals in the USA who learn English at an early age and also remain Spanish-dominant. For these reasons (and others) we separated our analyses by dominance groups and interpret any comparisons between them with caution.
English-dominant bilinguals
To determine which language exhibits a greater difference between patients and controls we compared dominant and nondominant naming scores in a 2 × 2 ANOVA with diagnosis (probable AD vs. control) as a between subjects variable and scoring method (dominant versus nondominant) as a repeated measures variable. Figure 1 shows the results for English-dominant bilinguals. English-dominant bilinguals named more pictures in their dominant than in their nondominant language, (a main effect of language dominance), F(1,36) = 116.45, MSE = .017, ηp2 = .76, p < .01, and English-dominant bilinguals with AD named fewer pictures than controls, (a main effect of diagnosis), F(1,36) = 9.52, MSE = .043, ηp2 = .21, p < .01. Of great interest, the difference between bilinguals with AD and controls was considerably and significantly larger for dominant than for nondominant language naming scores (a significant interaction between language of testing and diagnosis), F(1,36) = 6.29, MSE = .017, ηp2 = .15, p = .02. More specifically, English-dominant bilinguals with AD named approximately 24% fewer pictures than controls in the dominant language, but only about 7% fewer pictures than controls in the nondominant language.
Figure 1.

Mean proportion of Boston Naming Test pictures named correctly in each of the four scoring methods in English-dominant bilinguals with Alzheimer's disease and healthy controls. Error bars show standard errors.
To determine whether English-dominant bilinguals benefit from the either-language scoring method, and if this benefit is modulated by AD, we submitted the either-language and dominant-language naming scores to a 2 × 2 ANOVA with diagnosis (probable AD versus control) as a between subjects variable and scoring method (either versus dominant) as a repeated measures variable. English-dominant bilinguals named a significantly higher proportion of pictures with the either-language scoring method than with the dominant-language only method (a main effect of scoring method), F(1,36) = 21.34, MSE = .001, ηp2 = .37, p < .01. In addition, bilinguals with AD had lower naming scores than controls (a main effect of diagnosis), F(1,36) = 13.47, MSE = .059, ηp2 = .27, p < .01. Of great interest, bilinguals with AD benefited significantly more than controls from the either-language scoring alternative (a significant interaction between diagnosis and scoring method), F(1,36) = 7.19, MSE = .001, ηp2 = .17, p = .01. Additional comparisons revealed that both English-dominant bilinguals with AD (p < .01) and their matched controls (p = .01) benefited significantly from the either-language scoring procedure. However, in controls this benefit was rather small (naming scores increased by 1.3%), relative to that seen in bilinguals with AD (who named 4.8% more pictures when using the either-language scoring method than with the dominant-language only method).
The either-language scoring results provide additional evidence of dominant language decline, and are surprising from the common assumption that AD should impair the ability to access names in a nondominant language much more than names in the dominant language. Instead English-dominant bilinguals with AD were relatively more likely than their controls to access a name in their nondominant language that they could not access in the dominant language.
These results suggest that although production of a nondominant language is more difficult than production of a dominant language (for bilinguals with and without AD), the effect of dementia on lexical accessibility is greater in the dominant than the nondominant language. It should be noted, however, that the English-dominant bilinguals in the current study acquired both languages at a relatively early age. It is possible that bilinguals lose the ability to produce a nondominant language with the progression of dementia only when they learned a second language later in life. On this view, regression to a single language in bilinguals with AD would be analogous to age-of-acquisition effects seen in monolinguals with AD (e.g., Forbes-McKay, Ellis, Shanks, & Venneri, 2005). To address this possibility we next consider the results for the Spanish-dominant bilinguals who acquired English at a later age (on average; see Table 2).
Spanish-dominant bilinguals
Figure 2 shows the results for Spanish-dominant bilinguals. As above, we first considered which language exhibits a greater difference between patients and controls. Spanish-dominant bilinguals named more pictures in their dominant than their nondominant language, (a main effect of language dominance), F(1,31) = 56.91, MSE = .016, ηp2 = .65, p < .01, and bilinguals with AD named fewer pictures than controls, (a main effect of diagnosis), F(1,31) = 21.21, MSE = .051, ηp2 = .41, p < .01. As for English-dominant bilinguals, the difference between AD and controls was greater with dominant than with nondominant language naming scores. However, in this case the difference (i.e., the interaction between language of testing and diagnosis) was not significant, F(1,31) = 1.28, MSE = .016, ηp2 = .04, p = .27. Spanish-dominant bilinguals with AD named approximately 30% fewer pictures than controls in the dominant language, and about 25% fewer pictures in the nondominant language. Thus, both English-dominant and Spanish-dominant bilinguals, exhibited greater disease-related decline in the dominant language than in the nondominant language (but significantly so only for English-dominant bilinguals).
Figure 2.
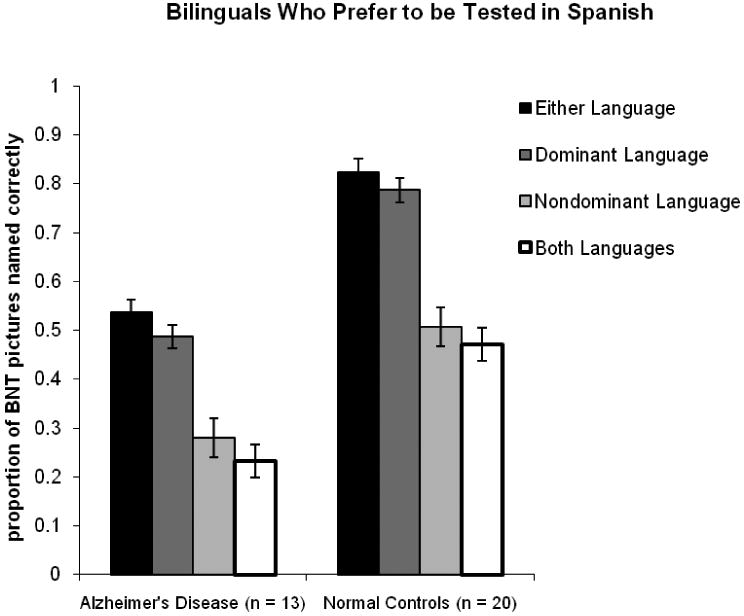
Mean proportion of Boston Naming Test pictures named correctly in each of the four scoring methods in Spanish-dominant bilinguals with Alzheimer's disease and healthy controls. Error bars show standard errors.
Considering the benefit of the either-language scoring method in Spanish-dominant bilinguals, naming scores were significantly higher with the either-language than with the dominant-language scoring method (a main effect of scoring method), F(1,31) = 27.62, MSE = .001, ηp2 = .47, p < .01, and Spanish-dominant bilinguals with AD had lower naming scores than their controls (a main effect of diagnosis), F(1,31) = 34.22, MSE = .040, ηp2 = .53, p < .01. In this case however, there was no significant interaction (F < 1) although the numbers trended in the same direction as reported above with a greater either-language scoring benefit for Spanish-dominant bilinguals with AD (4.8% increase) than for controls (3.6% increase). Additional comparisons revealed that both Spanish-dominant bilinguals with AD (p = .01) and controls (p < .01) benefited significantly from the either-language scoring procedure. Although these results present a slightly different pattern from that seen with English-dominant bilinguals, in both cases bilinguals with AD benefited from the either-language scoring method (either significantly more than controls, or to the same extent as controls). Thus, it can be concluded that AD did not decrease the chances of having access to some nondominant language names that are inaccessible in the dominant language (and in English-dominant bilinguals AD may even have increased this chance).
Additional Statistical Analyses
For ease of interpretation, we reported means and analyses of raw proportion correct data. Because of the restricted range in possible means using percent correct data (which can vary only between zero and 1) there is a potential for scaling artifact and distortion of effects particularly if some conditions approach floor or ceiling values (Winer, 1971). In our data set all the group means are far from ceiling and floor (see Figures 1 and 2). However, some individual participants' means were outside the range considered ideal for avoiding scaling artifacts with accuracy data (floor/ceiling effects are less likely in data sets with values that range between 25-75% correct; Dixon, 2008). Specifically, ceiling effects might be a concern given that some of the participants' dominant-language naming scores were above 75% correct (particularly in more educated English-dominant participants of which 4/22 scored at 95% correct or better). Similarly, floor effects might be a concern given that a number of individual participants' nondominant language naming scores were below 25% (4/16 or 25% of cases in English-dominant participants with AD, and even more 7/13 or 54% of cases in Spanish-dominant participants with AD). However, despite potential for ceiling level in dominant language naming scores in our higher education-level English-dominant participants, we observed greater differences between patients and controls in the dominant than in the nondominant language. Similarly, although Spanish-dominant bilinguals with AD exhibited the strongest potential for floor effects, the Spanish dominant participants in fact exhibited greater difference between patients and controls in nondominant language naming scores (in all naming scores) than did English-dominant bilinguals (see Figure 3). Thus, if ceiling and floor effects were influencing interpretation then the interactions we reported should be even stronger without the restriction in measurement range.
Figure 3.
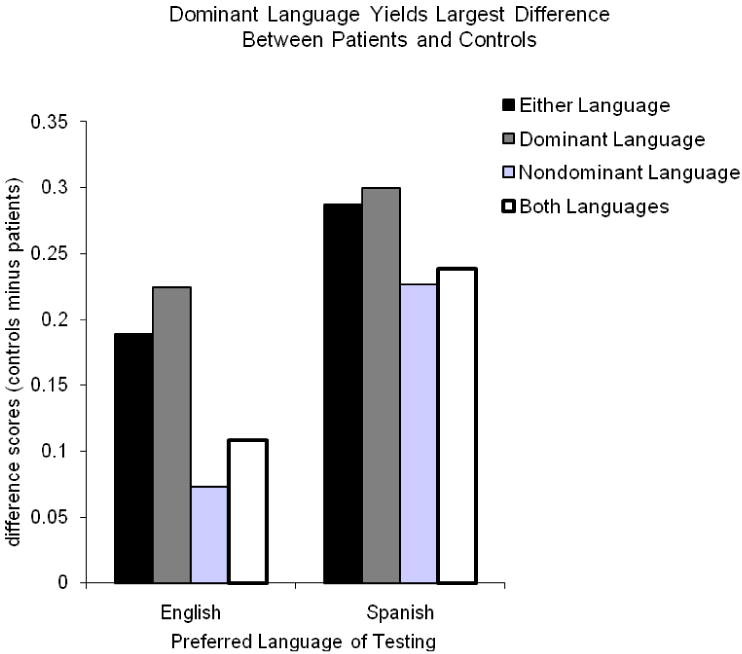
Degree of difference in the proportion of pictures named correctly between bilinguals with Alzheimer's disease and healthy controls in each of the four scoring methods.
To consider these possibilities we carried out an additional analysis to compare patients' and controls' dominant and nondominant language naming scores in each group of bilinguals. As recently recommended by Dixon (2008) for modeling accuracy in repeated-measures designs we modeled the log odds (logit) of proportion correct as a linear function of diagnosis (AD, control) and language dominance (dominant, nondominant), with the interaction between these included as a predictor. For these logistic regressions we used the lme4 package (Bates, 2007) in the statistical software R (version 2.5.0; R Development Core Team, 2007). In addition, we specified both subjects and items simultaneously as random effects in our models (below we note one instance in which the inclusion of items as a random factor led to one small change in results). This statistical technique addresses a number of shortcomings with traditional ANOVA analyses in repeated measures designs (Baayen, 2004, in press; Baayen, Davidson, & Bates, 2008; Pinheiro & Bates, 2000; Richter, 2006).
The shift from traditional ANOVA to this approach provided us with increased confidence in our conclusion that the two groups of bilinguals exhibit the same pattern of results. Because we were mainly interested in the interaction effect between diagnosis and language-dominance we focus our discussion on these but note that the main effects of diagnosis and language dominance were highly robust in all of our analyses (all ps < .001). In the English-dominant participants we observed a significant interaction between language-dominance and diagnosis that was highly robust (coefficient = -1.43, SE = 0.21, Wald Z = -6.90, p < .001). Thus, for English-dominant participants the change to logistic regression with both subjects and items as random effects does not change the pattern of results relative to that above using traditional ANOVA and raw percent correct as the dependent variable. The change in approach led to a difference in results with the Spanish-dominant participants who did not exhibit a significant interaction in the above-reported ANOVAs, but exhibited a significant interaction in the same direction as the English-dominant participants with this new approach to data analysis [coefficient = -0.54, SE = 0.23, Wald Z = -2.38, p = .02; note that this interaction was just marginally significant (p = .08) when we excluded items as a random factor in the analysis]. Moreover, the inclusion of the interaction term improved the model fit (log-likelihood) from 2651.2 for the reduced model to 2653.7 for the full model, a statistically significant difference (Χ2(1) = 5.47, p = 0.02), which meant the interaction could not be excluded without a significant loss of fit.
Thus, these analyses provide statistical support for our conclusion that both groups of bilinguals exhibit the same pattern of effects of AD on ability to access names. In both cases the dominant language exhibits the largest difference between patients and controls, a result that is in the opposite direction as that predicted by the retrieval deficit model, and that is consistent with the semantic deficit model of AD, and with the notion of richer semantic representations in the dominant than the nondominant language.
Discussion
The current study was designed to consider how Alzheimer's disease affects bilinguals' ability to access picture names in their dominant and nondominant languages. In both English-dominant (early) bilinguals, and Spanish-dominant (late) bilinguals, the naming score that consistently yielded the largest difference between bilinguals with and without AD was the dominant-language naming score. In addition, we replicated and extended to Alzheimer's disease previous reports of an either-language benefit. That is, bilinguals obtain higher naming scores when credited for pictures named in a nondominant language that they could not produce in their dominant language. In our study, this benefit was significant in both English-dominant and Spanish-dominant cognitively healthy bilinguals. In bilinguals with Alzheimer's disease, English-dominant patients exhibited a significantly greater benefit from the either-language scoring method than controls, and Spanish-dominant patients exhibited equal benefit from the either-language scoring method as controls.
Figure 3 shows the extent to which the four scoring methods revealed differences between patients and controls. The dominant-language shows the largest difference scores regardless of language dominance. In English-dominant bilinguals the dominant-language score produced a significantly larger difference between patients and controls than the either-language score. In Spanish-dominant bilinguals the two scores produced about equally large differences between patients and controls but trended in the same direction as that seen with English-dominant bilinguals. Most importantly, it was never the case that the nondominant language exhibited a greater difference between patients and controls than the dominant language. Although the pattern of results was slightly different across language-dominance groups, overall the data are similar in the two language-dominance groups (the bars showing the four scoring methods exhibit the same pattern of relative heights in both the right and left sides of both Figure 1 and Figure 2). These findings have implications for neuropsychological assessment of bilingual speakers, provide clues as to the origin of the either-language scoring benefit in bilingual speakers, and also provide information about the nature of bilingual lexical retrieval and how it is affected by AD.
As discussed above, the greater sensitivity of dominant language naming to the effects of AD is consistent with proposals of stronger connections from conceptual representations to the dominant than the nondominant language, the notion that the dominant language has richer semantic representations, and that AD primarily affects the integrity of semantic representations. More specifically, a greater number of associations may connect concepts with dominant language names, and a relatively smaller number may connect concepts with nondominant language names. Assuming equal probability of any particular connection being damaged by AD, the greater number of connections makes the dominant language more sensitive to impairment. Though it is counterintuitive to find that richer representations are more vulnerable to change associated with disease it makes sense from the perspective that AD will damage representations without consideration of language membership, and with the above-reviewed literature suggesting that the two languages of bilingual speakers are served by largely shared brain regions.
The finding of an increased or intact either-language scoring benefit in bilinguals with AD (increased for English-dominant bilinguals and intact for Spanish-dominant bilinguals) is also consistent with these claims. As AD impairs bilinguals' ability to access dominant language names, there may even be a greater probability that they will be able to produce some names in their nondominant language that they cannot access in their dominant language. By implication the either-language scoring alternative allows bilinguals with AD to compensate for some of their disease related decline in the ability to access picture names. This resembles the effects of the either-language option for obscuring aging-related (and low-proficiency-related) inefficiencies in language switching (Gollan & Ferreira, 2009), and suggests that use of either-language might benefit communication in bilinguals with AD, but will be counterproductive in attempts to distinguish patients from controls.
It could be argued that our procedure of always testing in the dominant language first spuriously enhanced the difference in sensitivity of the dominant versus nondominant languages to disease related decline. That is, in our study the dominant language might have exhibited greater sensitivity to AD because the nondominant language was negatively affected by prior retrieval of names in the dominant language. For a number of reasons we consider this to be an unlikely explanation. First, if prior naming served to increase interference between languages during attempted retrieval of nondominant language names, then it could easily be argued that bilinguals with AD should be less able to manage such increased competition, and therefore this manipulation should have served only to decrease the ability of bilinguals with AD to benefit from the either-language scoring method. However, we observed precisely the opposite outcome. Second, studies of bilingual language switching reveal that activating a nondominant language (by requiring bilinguals to name pictures in it) can have dramatic effects on the ability to rapidly retrieve dominant language names, however, there is often little or no effect of language mixing on the ability to rapidly retrieve nondominant language names (e.g., Costa & Santesteban, 2004; Christoffels et al., 2007; Meuter & Allport, 1999).
Alternatively, it might be argued that Spanish-dominant bilinguals in fact did exhibit greater decline in the nondominant than the dominant language if the baseline level of performance is considered. As Figure 2 shows, there is similarly sized decline in naming scores (comparing bilinguals with and without AD) for the two languages even though naming scores were much lower in English than in Spanish. This possible difference between early (English-dominant) and late (Spanish-dominant) bilinguals is consistent with above reviewed proposals that late-learned second languages are represented more episodically, which in turn leaves them more vulnerable to impairments in episodic memory resulting from damage to the medial temporal lobe structures in AD (especially the hippocampus; Braak & Braak, 1991). If so Spanish-dominant bilinguals' greater decline in ability to access the dominant-language names would be partially offset by AD-related difficulties in retrieving later-learned nondominant language names (here we assume that AD could cause both dominant language decline and difficulty retrieving later-learned episodically represented words). If so, English-dominant bilinguals in the current study might exhibit a different pattern of results because they learned both languages at a relatively early age.
Any discussion along these lines must be considered with caution because our study was not designed to directly compare English-dominant and Spanish-dominant participants and several possibly relevant differences between them compromise the possibility of attributing differences to age of acquisition of the two languages. First, although we matched patients and controls within language-dominance groups we did not match English-dominant and Spanish-dominant bilinguals for age, years of education, degree of cognitive impairment, or age-of-acquisition of English (see Tables 1-2). Also, as noted above early and late bilinguals differed in which language is dominant, and difference in appropriateness of the BNT for testing in each language could have powerful effects on the results. Even if it is conceded that Spanish-dominant bilinguals may exhibit greater proportional decline in the nondominant language, this would not necessarily support the retrieval deficit account of AD (both in raw difference scores and in proportional decline). This is because it would still be the case that only some types of bilinguals exhibit deficits in effortful retrieval. For bilinguals who acquired both languages around the same (early) age, the dominant language was clearly more sensitive to AD. The retrieval deficit model was developed as a model of monolingual lexical retrieval in AD, and certainly therefore should not apply exclusively to bilinguals who (at least partially) represent their nondominant language episodically (quite the opposite given that monolinguals do not represent their lexicon in episodic memory).
Also potentially relevant for considering baseline differences between dominant and nondominant naming scores is that higher naming scores do not always reveal larger differences between patients and controls2. For example, studies of lexical retrieval in monolinguals with AD revealed greater differences between patients and controls in naming pictures with low-frequency than high-frequency names even though high-frequency names yield significantly higher naming scores (Hodges, Salmon, & Butters, 1992; Kirshner, Webb, & Kelly, 1984; Ober & Shenaut, 1988; Thompson-Schill et al., 1999). There may be important differences between low-frequency of occurrence within a single language, and low frequency of occurrence resulting from relatively reduced use of an entire language (see also Gollan et al., 2008). Normal controls exhibited extremely low error rates for naming even the lowest frequency words in previous studies (only about 7% errors in the lowest frequency band of Figure 1 in Hodges et al., 1992). In contrast healthy controls in the current study could not name 15-21% of BNT pictures in the dominant language, and 49-56% of pictures in the nondominant language (see Figures 1-2). Such direct comparisons are to be interpreted with caution because it is impossible to match frequency of use between languages in bilinguals who vary in terms of how frequently they use the nondominant language. Furthermore, in monolinguals low word frequency tends to coincide with low conceptual frequency, whereas in bilinguals low word frequency can co-occur with high concept frequency (e.g., even highly common objects have necessarily lower frequency of use in a nondominant language). Nevertheless, these considerations suggest that differences between patients and controls in both monolinguals and bilinguals may be maximized in a medium difficulty range (not too difficult, and not too easy). This might be an important consideration in future studies designed to consider the effects of AD on language processing.
Another result that is consistent with our interpretation that the nondominant language is not particularly vulnerable to AD is that Spanish-dominant bilinguals with AD and controls benefitted equally from the either-language scoring alternative. If ability to access the nondominant language declines with AD relatively more than the dominant language declines, then the Spanish-dominant bilinguals with AD should have benefitted relatively less from this scoring alternative. A question that arises under this interpretation, however, is why didn't Spanish-dominant bilinguals with AD exhibit an enhanced either-language scoring benefit relative to matched controls? It seems possible that multiple factors contribute to the either-language benefit, and these may vary in terms of how they are affected by AD and by the language of testing. The BNT was designed for use with English speakers – and this may have increased the chances that some pictures would be more easily named in English than in Spanish. Such an effect should not vary with AD but could increase the either-language scoring benefit to its maximum in Spanish-dominant bilinguals with and without AD. Note that this same consideration could increase sensitivity for detecting nondominant language decline in Spanish-dominant speakers.
Some aspects of the data seem to support the idea that different factors allow English-dominant versus Spanish-dominant bilinguals to benefit from the either-language scoring alternative. Table 3 shows the correlations between a number of predictor variables and the degree to which naming scores improved using the either-language versus dominant-language scoring methods. For bilinguals who prefer to be tested in English, a greater either-language scoring benefit is seen in those with high education levels, and those who are more cognitively impaired (low DRS scores are associated with a larger benefit). In contrast, for bilinguals who prefer to be tested in Spanish, greater either-language scoring benefits are found in those who report using English more often, who acquired English at a relatively younger age, and in those who rate their ability to speak both languages as similarly strong. Finally, a relatively large number of items contributed to the either-language benefit in both bilingual types (30 items for English-dominant participants, and 34 for Spanish-dominant bilinguals). Thus, it was not the case that a few items spuriously introduced the greater either-language benefit in English-dominant bilinguals with AD.
Table 3. Correlations between degree of either-language scoring benefit (either-language minus dominant-language score) and language-proficiency and use ratings, education, and level of cognitive impairment.
|
English-dominant (n = 38) |
Spanish-dominant (n = 28) |
|
|---|---|---|
| Self-Rating Dominant minus Nondominanta | -0.259 | -0.561** |
| p-value | 0.117 | 0.002 |
| Years of Education | 0.362* | 0.234 |
| p-value | 0.026 | 0.190 |
| Age of Regular use of English | 0.180 | -0.524** |
| p-value | 0.286 | 0.003 |
| Percent Daily Use of English | 0.169 | 0.630** |
| p-value | 0.310 | 0.000 |
| Dementia Rating Scale score | -0.333* | 0.141 |
| p-value | 0.041 | 0.433 |
| MMSE | -0.184 | -0.025 |
| p-value | 0.269 | 0.892 |
It might be asked why patients with Alzheimer's disease continue to show better naming scores in the dominant than in the nondominant language if the disease affects dominant language retrieval more than nondominant language retrieval. That is, why do language dominance effects persist despite the presence of AD? However, language dominance effects primarily reflect language learning history and patterns of language use. Only an extreme (and in our opinion obviously incorrect) claim - that AD affects only the dominant language (and not the nondominant language) - would predict that language dominance effects should disappear entirely. Such a claim would also predict that eventually the nondominant language should become dominant (dominance reversal). Instead, our claim is that AD affects representations in both languages but the nature of language representation leaves the dominant language more sensitive to changes. Similarly with respect to the either-language scoring benefit, AD increases the probability of naming a picture in the nondominant language that cannot be named in the dominant language. However, there remain more cases in which the reverse is true (pictures named in the dominant but not in the non-dominant language). Nevertheless, what is of interest in both cases is the size of the difference between patients and controls (not language dominance itself).
The current findings have implications for the assessment of naming skills in bilinguals. The use of either-language seems to increase communication ability in bilinguals with AD but may obscure the effects of cognitive decline (at least in English-dominant early bilinguals). In addition, it was previously suggested that relatively balanced bilinguals are more likely to benefit from the either-language scoring alternative (Gollan et al., 2007; Kohnert et al., 1998), however, our data show that not all balanced bilinguals will exhibit this benefit, and conversely some relatively unbalanced bilinguals do exhibit improved naming scores with the either-language scoring alternative. Table 4 shows the range, M and SD of either-language benefit in cognitively healthy English- and Spanish-dominant bilinguals who rated their ability to speak the two languages as relatively similar or dissimilar (for this purpose we chose an arbitrary cutoff for balanced versus unbalanced bilinguals; but see Gollan et al., 2007 for continuous analyses along these lines). Although balanced bilinguals tended to benefit more on average than unbalanced bilinguals from the either-language scoring alternative (see also Kohnert et al., 1998) some balanced bilinguals in both the English-dominant and Spanish-dominant groups exhibited no improvement in naming scores when using the either-language scoring alternative (the minimum value is zero in both cases), and some relatively unbalanced bilinguals exhibited the alternative scoring benefit (1% for English-dominant, and 3% for Spanish-dominant unbalanced bilinguals).
Table 4. Proportion of either-language benefit in cognitively healthy bilinguals who rated themselves as balanceda or unbalancedb bilinguals by preferred language of testing.
| Self-Rated Balanced Bilinguals | |||||
|---|---|---|---|---|---|
| n | min | max | mean | SD | |
| English-dominant | 7 | 0.00 | 0.08 | 0.03 | 0.03 |
| Spanish-dominant | 5 | 0.00 | 0.10 | 0.07 | 0.04 |
| Self-Rated Unbalanced Bilinguals | |||||
| n | min | max | mean | SD | |
| English-dominant | 15 | 0.00 | 0.03 | 0.01 | 0.01 |
| Spanish-dominant | 14 | 0.00 | 0.10 | 0.03 | 0.03 |
Balanced Bilinguals = Rated ability to speak Spanish and English as the same or up to a difference of 1 between languages on 1-7 scale
Unbalanced = Rated ability to speak Spanish and English as at least 2 or up to difference of 6 on a 1-7 scale
It may seem inconsistent to claim that the either-language scoring method provides a more accurate assessment of semantic knowledge in children but simultaneously provides a weaker assessment of semantic impairment in bilinguals with AD. A key difference here may be the goals of the assessment. Bilingual children (especially very young children) have experienced their two languages – and the world of concepts – in a much more limited set of contexts than bilingual adults (especially older bilinguals). In assessing semantic knowledge in children it may be more accurate to count objects that are sufficiently familiar to be named in at least one language. In trying to distinguish bilinguals with AD from healthy controls it may be less useful to include objects that bilingual adults continue to be able to name only in their relatively less used language even in older age. Such objects may have relatively impoverished semantic representations relative to objects that occur in a wider range of contexts. In addition, bilingual children may well exhibit an either-language scoring benefit for many items that they will ultimately retrieve very easily in both languages as their range of experiences in the two languages broadens. Thus, the either-language scoring benefit may provide a more accurate assessment of which objects are familiar to at least some degree, but not for detecting subtle changes in semantic representation with disease onset and progression.
Although we suggested that richer semantic representations allow dominant language naming scores to be more sensitive to the effects of AD than any other scoring method, alternative explanations are possible. First, the BNT was not designed to assess naming in a nondominant language, and may lack sensitivity for detecting change in the ability to access a nondominant language because it does not contain a sufficiently large number of pictures with names that cognitively intact speakers could access relatively easily even in a nondominant language. A second possibility is that decline in the ability to access the nondominant language (and previous observations of this effect in natural settings; Mendez et al., 1999) primarily reflects difficulty with maintaining fluent bilingualism at a level of grammatical encoding (in putting together multi-word utterances, or sentences). Such effects would be observed in natural settings, but would not be detected in a test of single picture naming. These possibilities (or a combination of them) cannot be ruled out without further investigation.
A more general prediction that follows from our interpretation of the results is that rich semantic representations, or words with many associations to conceptual representations, may be more sensitive to cognitive change associated with AD even in monolinguals. To identify factors that produce rich versus less rich semantic representations in monolinguals a number of possible avenues might be pursued. For example, despite monolingual language use some objects may occur in a greater diversity of contexts than others (Adelman et al., 2006). Names that are associated with multiple contexts should be easier to retrieve, but should nevertheless exhibit a greater difference between monolinguals with and without AD than names that occur in a more narrow range of contexts. For retrieval of abstract words the same prediction might apply when comparing words with many versus few senses (Rodd, Gaskell, & Marslen-Wilson, 2002), or words with strong versus no strong associates (see Gollan, Salmon, & Paxton, 2006). Other means for defining richness of semantic representation could also be considered (Griffiths, Steyvers, & Tenenbaum, 2007; Hare, Jones, Thomson, Kelly, & McRae, 2009). In addition, retrieval deficits associated with AD may be more readily observed when the degree of semantic richness is controlled (perhaps in studies that manipulate frequency but control other variables; e.g., Thompson-Schill et al., 1999). In this respect, our observation that the dominant language is more sensitive than the nondominant language to the cognitive decline associated with AD constitutes powerful evidence against the hypothesis that AD primarily entails a deficit in effortful retrieval, and provides a demonstration of how studies of bilingualism can reveal aspects of the cognitive system that may otherwise be more difficult to observe.
Acknowledgments
This research was supported by an R01 from NICHD (HD050287) and by a Career Development Award from NIDCD (DC00191) both awarded to Tamar H. Gollan, and by a P50 (AG05131) from NIH/NIA to the University of California. Correspondence concerning this article should be addressed to Tamar H. Gollan, 9500 Gilman Drive, La Jolla, CA 92093-0949 (e-mail: tgollan@ucsd.edu).
Footnotes
Figure 3 also appears to show that the degree of AD-related decline in naming scores was not driven exclusively by task difficulty. Both English-dominant and Spanish-dominant bilinguals obtain the lowest naming scores with the both-languages scoring method but the both-languages score did not yield the smallest difference between patients and controls. Note, however, that this is because the contrast between the both-languages and nondominant scores is simply the mirror image of the contrast between the either-language and dominant-language scores. Whereas the either-language benefit reflects pictures that can be named in the nondominant but not the dominant language, the both-languages score reflects the subset of pictures that can be named in the nondominant and the dominant languages.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Abutalebi J, Annoni JM, Zimine I, Pegna AJ, Seghier ML, Lee-Jahnke H, Lazeyras F, Cappa SF, Khateb A. Language control and lexical competition in bilinguals: An event-related fMRI study. Cerebral Cortex. 2008;18:1496–1505. doi: 10.1093/cercor/bhm182. [DOI] [PubMed] [Google Scholar]
- Abutalebi J, Cappa SF, Perani D. Functional neuroimaging of the bilingual brain. In: Kroll JFK, De Groot A, editors. Handbook of bilingualism: Psycholinguistic approaches. Oxford: Oxford University Press; 2005. pp. 497–515. [Google Scholar]
- Acevedo A, Krueger KR, Navarro E, Ortiz F, Manly JJ, Padilla-Velez MM, Weintraub S, Lopez OL, Mungas D. The Spanish translation and adaptation of the Uniform Data Set of the National Institute on Aging Alzheimer's Disease Centers. Alzheimer Disease and Associated Disorders. 2009;23:102–109. doi: 10.1097/WAD.0b013e318193e376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Acevedo A, Loewenstein DA. Performance on the Boston Naming Test in English-Spanish bilingual older adults: Some considerations. The Journal of the International Neuropsychological Society. 2007;13:212–214. doi: 10.1017/S1355617707070415. [DOI] [PubMed] [Google Scholar]
- Adelman JS, Brown GDA, Quesada JF. Contextual diversity, not word frequency, determines word-naming and lexical decision times. Psychological Science. 2006;17:814–823. doi: 10.1111/j.1467-9280.2006.01787.x. [DOI] [PubMed] [Google Scholar]
- Allegri RF, Mangone CA, Fernandez Villavicencio A, Rymberg S, Taragano FE, Baumann D. Spanish Boston Naming Test norms. The Clinical Neuropsychologist. 1997;11:416–420. [Google Scholar]
- Ardila A. Bilingualism across the life-span under normal and abnormal conditions. In: Ardila A, Ramos E, editors. Speech and Language Disorders in Bilinguals. Nova Science Publishers; 2007. pp. 151–160. [Google Scholar]
- Ardila A, Ramos E. Normal and abnormal aging in bilinguals. Dementia and Neuropsychologia. 2008;2:242–247. doi: 10.1590/S1980-57642009DN20400002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alzheimer's Association. Hispanics/Latinos and Alzheimer's disease. 2004 http://www.alz.org/national/documents/report_hispanic.pdf.
- Baayen RH. Statistics in psycholinguistics: A critique of some current gold standards. Mental Lexicon Working Papers. 2004;1:1–45. [Google Scholar]
- Baayen RH. languageR: Data sets and functions with “Analyzing Linguistic Data: A practical introduction to statistics.”. R package version 2.9.2. 2007 Retrieved October 2009, from http://cran.r-project.org/web/packages/languageR/index.html.
- Baayen RH. Analyzing linguistic data: A practical introduction to statistics. Cambridge, England: Cambridge University Press; 2008. [Google Scholar]
- Baayen RH, Davidson DJ, Bates DM, editors. Journal of Memory and Language. Vol. 59. 2008. Mixed effects modeling with crossed random effects for participants and items; pp. 390–412. [Google Scholar]
- Balota DA, Watson JM, Duchek JM, Ferraro FR. Cross-modal semantic and homograph priming in healthy young, healthy old, and in Alzheimer's disease individuals. Journal of the International Neuropsychological Society. 1999;5:626–640. doi: 10.1017/s1355617799577060. [DOI] [PubMed] [Google Scholar]
- Bedore LM, Peña ED, García M, Cortez C. Conceptual Versus Monolingual Scoring: When Does It Make a Difference? Language, Speech, and Hearing Services in Schools. 2005;36:188–200. [PubMed] [Google Scholar]
- Bialystok E, Craik FIM. Bilingualism and naming: Implications for cognitive assessment. The Journal of the International Neuropsychological Society. 2007;13:209–211. doi: 10.1017/S1355617707070403. [DOI] [PubMed] [Google Scholar]
- Bialystok E, Craik FIM, Freedman M. Bilingualism as a protection against the onset of symptoms of dementia. Neuropsychologia. 2007;45:459–464. doi: 10.1016/j.neuropsychologia.2006.10.009. [DOI] [PubMed] [Google Scholar]
- Bialystok E, Craik FIM, Klein R, Viswanathan M. Bilingualism, aging, and cognitive control: Evidence from the Simon Task. Psychology and Aging. 2004;19:290–303. doi: 10.1037/0882-7974.19.2.290. [DOI] [PubMed] [Google Scholar]
- Bialystok E, Craik FIM, Luk G. Cognitive control and lexical access in younger and older bilinguals. Journal of Experimental Psychology: Learning, Memory and Cognition. 2008;34:859–873. doi: 10.1037/0278-7393.34.4.859. [DOI] [PubMed] [Google Scholar]
- Braak H, Braak E. Neuropathological staging of Alzheimer-related changes. Acta Neuropathologica. 1991;82:239–259. doi: 10.1007/BF00308809. [DOI] [PubMed] [Google Scholar]
- Butters N, Granholm E, Salmon DP, Grant I, Wolfe J. Episodic and semantic memory: A comparison of amnesic and demented patients. Journal of Clinical and Experimental Neuropsychology. 1987;9:479–497. doi: 10.1080/01688638708410764. [DOI] [PubMed] [Google Scholar]
- Chee MWL, Hon N, Ling Lee H, Soon CS. Relative language proficiency modulates BOLD signal change when bilinguals perform semantic judgments. Neuroimage. 2001;13:1155–1163. doi: 10.1006/nimg.2001.0781. [DOI] [PubMed] [Google Scholar]
- Chertkow H, Bub D. Semantic memory loss in dementia of Alzheimer's type. Brain. 1990;113:397–417. doi: 10.1093/brain/113.2.397. [DOI] [PubMed] [Google Scholar]
- Chertkow H, Whitehead V, Phillips N, Wolfson C, Atherton J, Bergman H. Multilingualism (but not always bilingualism) delays the onset of Alzheimer's disease: Evidence from a bilingual community. Alzheimer's Disease and Associated Disorders. doi: 10.1097/WAD.0b013e3181ca1221. in press. [DOI] [PubMed] [Google Scholar]
- Christoffels IK, Firk C, Schiller NO. Bilingual language control: An event-related brain potential study. Brain Research. 2007;1147:192–208. doi: 10.1016/j.brainres.2007.01.137. [DOI] [PubMed] [Google Scholar]
- Costa A, Hernandez M, Sebastián-Gallés N. Bilingualism aids conflict resolution: Evidence from ANT task. Cognition. 2008;106:59–86. doi: 10.1016/j.cognition.2006.12.013. [DOI] [PubMed] [Google Scholar]
- Costa A, Santesteban M. Lexical access in bilingual speech production: Evidence from language switching in highly proficient bilinguals and L2 learners. Journal of Memory and Language. 2004;50:491–511. [Google Scholar]
- De Bleser R, Dupont P, Postler J, Bormans G, Speelman D, Mortelmans L, et al. The organization of the bilingual lexicon: A PET study. Journal of Neurolinguistics. 2003;16:439–456. [Google Scholar]
- De Santi S, Obler LK, Sabo-Abramson H, Goldberger J. Discourse Abilities and Deficits in Multilingual Dementia. In: Joanette Y, Brownell H, editors. Discourse Abilities in Brain Damage: Theoretical and Empirical Perspectives. NY: Springer-Verlag; 1989. [Google Scholar]
- De Picciotto J, Friedland D. Verbal fluency in elderly bilingual speakers: Normative data and preliminary application to Alzheimer's disease. Folia Phoniatrica et Logopaedica. 2001;53:145–152. doi: 10.1159/000052669. [DOI] [PubMed] [Google Scholar]
- Dixon P. Models of accuracy in repeated-measures designs. Journal of Memory and Language. 2008;59:447–456. [Google Scholar]
- Finkbeiner M. Doctoral dissertation, University of Arizona, 2002. 12. Vol. 63. 2002. Bilingual lexical memory: Towards a psycholinguistic model of adult L2 lexical acquisition, representation, and processing; p. 6114B. Dissertation Abstracts International. UMI No. AAT 3073282. [Google Scholar]
- Finkbeiner M, Forster KI, Nicol J, Nakamura K. The role of polysemy in masked semantic and translation priming. Journal of Memory and Language. 2004;51:1–22. [Google Scholar]
- Fitten LJ, et al. Frequency of Alzheimer's Disease and Other Dementias in a Community Outreach Sample of Hispanics. JAGS. 2001;49:1301–1308. doi: 10.1046/j.1532-5415.2001.49257.x. [DOI] [PubMed] [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975;12:189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Forbes-McKay KE, Ellis AW, Shanks MF, Venneri A. The age of acquisition of words in a semantic fluency task can reliably differentiate normal from pathological age related cognitive decline. Neuropsychologia. 2005;43:1625–1632. doi: 10.1016/j.neuropsychologia.2005.01.008. [DOI] [PubMed] [Google Scholar]
- Gollan TH, Fennema-Notestine C. What is it about bilingualism that affects BNT performance? A reply to commentaries. The Journal of the International Neuropsychological Society. 2007;13:215–218. [Google Scholar]
- Gollan TH, Fennema-Notestine C, Montoya RI, Jernigan TL. The Bilingual Effect on Boston Naming Test performance. The Journal of the International Neuropsychological Society. 2007;13:197–208. doi: 10.1017/S1355617707070038. [DOI] [PubMed] [Google Scholar]
- Gollan TH, Ferreira VS. Should I stay or should I switch? A cost-benefit analysis of voluntary language switching in young and aging bilinguals. Journal of Expermental Psychology: Learning, Memory, & Cognition. 2009;35:640–665. doi: 10.1037/a0014981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gollan TH, Montoya R, Cera C, Sandoval T. More use almost always means a smaller frequency effect: Aging, bilingualism, and the weaker links hypothesis. Journal of Memory and Language. 2008;58:787–814. doi: 10.1016/j.jml.2007.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gollan TH, Montoya RI, Werner G. Semantic and letter fluency in Spanish-English bilinguals. Neuropsychology. 2002;16:562–576. [PubMed] [Google Scholar]
- Gollan TH, Salmon DP, Paxton JL. Word association in early Alzheimer's disease. Brain and Language. 2006;99:289–303. doi: 10.1016/j.bandl.2005.07.001. [DOI] [PubMed] [Google Scholar]
- Gollan TH, Silverberg NB. Tip-of-the-tongue states in Hebrew–English bilinguals. Bilingualism: Language and Cognition. 2001;4:63–83. [Google Scholar]
- Griffiths TL, Steyvers M, Tenenbaum JB. Topics in semantic representation. Psychological Review. 2007;114:211–244. doi: 10.1037/0033-295X.114.2.211. [DOI] [PubMed] [Google Scholar]
- Grosjean F. Studying Bilinguals. Oxford: Oxford University Press; 2008. The complementarity principle and language; pp. 22–34. [Google Scholar]
- Hare M, Jones M, Thomson C, Kelly S, McRae K. Activating event knowledge. Cognition. 2009:151–167. doi: 10.1016/j.cognition.2009.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hernandez AE. Language switching in the bilingual brain: What's next? Brain & Langauge. 2009;109:133–140. doi: 10.1016/j.bandl.2008.12.005. [DOI] [PubMed] [Google Scholar]
- Hernandez AE, Kohnert KJ. Aging and language switching in bilinguals. Aging, Neuropsychology, and Cognition. 1999;6:69–83. [Google Scholar]
- Hyltenstam K, Stroud C. Second language regression in Alzheimer's Dementia. In: Hyltenstam K, Viberg A, editors. Progression and Regression in Language: Sociocultural, Neuropsychological, and Linguistic Perspectives. Cambridge University Press; 1994. pp. 222–293. [Google Scholar]
- Hodges JR, Salmon DP, Butters N. Semantic memory impairment in Alzheimer's disease: Failure of access or degraded knowledge? Neuropsychologia. 1992;30:301–314. doi: 10.1016/0028-3932(92)90104-t. [DOI] [PubMed] [Google Scholar]
- Jiang N, Forster KI. Cross-language priming asymmetries in lexical decision and episodic recognition. Journal of Memory and Language. 2001;44:32–51. [Google Scholar]
- Kaplan E, Goodglass H, Weintraub S. The Boston Naming Test. Philadelphia: Lea & Febiger; 1983. [Google Scholar]
- Kavé G, Eyal N, Shorek A, Cohen-Mansfield J. Multilingualism and cognitive state in the oldest old. Psychology and Aging. 2008;23:70–78. doi: 10.1037/0882-7974.23.1.70. [DOI] [PubMed] [Google Scholar]
- Kirshner HS, Webb WG, Kelly MP. The naming disorder of dementia. Neuropsychologia. 1984;22:23–30. doi: 10.1016/0028-3932(84)90004-6. [DOI] [PubMed] [Google Scholar]
- Kohnert KJ, Hernandez AE, Bates E. Bilingual performance on the Boston Naming Test: Preliminary norms in Spanish and English. Brain and Language. 1998;65:422–440. doi: 10.1006/brln.1998.2001. [DOI] [PubMed] [Google Scholar]
- Kroll JF, Tokowicz N. Models of bilingual representation and processing: Looking back and to the future. In: Kroll JFK, De Groot A, editors. Handbook of bilingualism: Psycholinguistic approaches. Oxford: Oxford University Press; 2005. pp. 531–553. [Google Scholar]
- Mattis S. Dementia Rating Scale: Professional Manual. Odessa, Florida: Psychological Assessment Resources; 1988. [Google Scholar]
- McGlinchey-Berroth R, Milberg WP. Preserved semantic memory structure in Alzheimer's disease. In: Cerella J, Rybash J, Hoyer W, Commons ML, editors. Adult Information Processing: Limits On Loss. New York: Academic Press; 1993. pp. 407–422. [Google Scholar]
- Meuter RF, Allport A. Bilingual language switching in naming: Asymmetrical costs of language selection. Journal of Memory & Language. 1999;40:25–40. [Google Scholar]
- Nebes R, Martin D, Horn L. Sparing of semantic memory in Alzheimer's disease. Journal of Abnormal Psychology. 1984;93:321–330. doi: 10.1037//0021-843x.93.3.321. [DOI] [PubMed] [Google Scholar]
- Ober BA, Shenaut GK. Lexical decision and priming in Alzheimer's disease. Neuropsychologia. 1988;26:273–286. doi: 10.1016/0028-3932(88)90080-2. [DOI] [PubMed] [Google Scholar]
- Ober BA, Shenaut GK, Reed BR. Assessment of associative relations in Alzheimer's disease: Evidence for preservation of semantic memory. Aging and Cognition. 1995;2:254–267. [Google Scholar]
- Obler LK, Albert M, Lozowick S. The Aging Bilingual. In: Vaid J, editor. Language Processing in Bilinguals: Psycholinguistic and Neuropsychological Perspectives. Hillsdale, NJ: Erlbaum; 1986. pp. 221–231. [Google Scholar]
- Oller DK, Pearson BZ. Assessing the effects of bilingualism: A background. In: Oller DK, Eilers RE, editors. Language and literacy in bilingual children. Clevedon: Multilingual Matters; 2002. pp. 3–21. [Google Scholar]
- Paradis M. Neurolingustic aspects of implicit and explict memory: Implications for bilingualism. In: Ellis N, editor. Implicit and explicit learning of second languages. London: Academic Press; 1994. pp. 393–419. [Google Scholar]
- Pinheiro JC, Bates DM. Mixed-effects models in S and S-PLUS. New York: Springer-Verlag; 2000. [Google Scholar]
- Pearson BZ, Fernández S, Oiler DK. Lexical development in bilingual infants and toddlers: Comparison to monolingual norms. Language and Learning. 1993;43:93–120. [Google Scholar]
- Prior A, MacWhinney B. A bilingual advantage in task switching. Bilingualism: Language and Cognition. doi: 10.1017/S1366728909990526. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perani D, Abutalebi J. Neural basis of first and second language processing. Current Opinion of Neurobiology. 2005;15:202–206. doi: 10.1016/j.conb.2005.03.007. [DOI] [PubMed] [Google Scholar]
- R Development Core Team. The R project for statistical computing. 2007 Retrieved October, 2009, from http://www.R-project.org.
- Richter T. What is wrong with ANOVA and multiple regression? Analyzing sentence reading times with hierarchical linear models. Discourse Processes. 2006;41:221–250. [Google Scholar]
- Rodd J, Gaskell G, Marslen-Wilson W. Making sense of semantic ambiguity: Semantic competition in lexical access. Journal of Memory and Langauge. 2002;46:245–266. [Google Scholar]
- Talamas A, Kroll JF, Dufour R. Form related errors in second language learning: A preliminary stage in the acquisition of L2 vocabulary. Bilingualism: Language and Cognition. 1999;2:45–58. [Google Scholar]
- Tang MX, et al. Incidence of AD in African-Americans, Caribbean Hispanics and Caucasians in Northern Manhattan. Neurology. 2001;56:49–56. doi: 10.1212/wnl.56.1.49. [DOI] [PubMed] [Google Scholar]
- Tang MX, et al. The APOE-e4 Allele and the Risk of AD among African Americans, Whites and Hispanics. JAMA. 1998;279:751–755. doi: 10.1001/jama.279.10.751. [DOI] [PubMed] [Google Scholar]
- Thompson-Schill SL, Gabrieli JDE, Fleischman DA. Effects of structural similarity and name frequency on picture naming in Alzheimer's disease. The Journal of the International Neuropsychological Society. 1999;5:659–667. doi: 10.1017/s1355617799577084. [DOI] [PubMed] [Google Scholar]
- Ullman MT. The neural basis of lexicon and grammar in first and second language: The declarative/procedural model. Bilingualism: Language and Cognition. 2001;4:105–122. [Google Scholar]
- Ullman MT. Contributions of memory circuits to language: The declarative/procedural model. Cognition. 2004;92:231–270. doi: 10.1016/j.cognition.2003.10.008. [DOI] [PubMed] [Google Scholar]
- Umbel VM, Pearson BZ, Fernández MC, Oller DK. Measuring bilingual children's receptive vocabularies. Child Development. 1992;63:1012–1020. [PubMed] [Google Scholar]
- Wang X, Forster KI. Masked translation priming with semantic categorization: Testing the Sense Model. Bilingualism: Language and Cognition in press. [Google Scholar]
- Weintraub S, Salmon D, Mercaldo N, Ferris S, Graff-Radford NR, Chui H, Cummings J, DeCarli C, Foster NL, Galasko D, Peskind E, Dietrich W, Beekly DL, Kukull WA, Morris JC. The Alzheimer's Disease Centers' Uniform Data Set (UDS): the neuropsychologic test battery. Alzheimer Disease and Associated Disorders. 2009;23:91–101. doi: 10.1097/WAD.0b013e318191c7dd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winer BJ. Statistical principles in experimental design. 2nd. New York: McGraw-Hill; 1971. [Google Scholar]