

Abstract
The rising prevalence of chronic and end-stage kidney disease is accompanied by a concomitant rising risk of hyperkalemia in these patients. Sodium polystyrene sulfonate (Kayexalate, sanofi-aventis, Bridgemater, NJ) is a commonly used treatment of hyperkalemia. We present a case of Kayexalate-induced colonic necrosis as a reminder of this rare, but potentially avoidable, toxicity of a commonly used medication.
A 56-year-old woman with chronic kidney disease stage 3 due to diabetic glomerulopathy and focal segmental glomerulosclerosis presented to our emergency department after 1 day of epigastric pain associated with nausea, vomiting, and diarrhea. She denied melena but endorsed a single episode of bright red blood per rectum. On examination, her abdomen was nondistended with active bowel sounds, but there was tenderness in her epigastric and left upper quadrant. Her initial laboratory examinations detected a mild hyperkalemia (5.8 mmol/L). She was treated with sodium polystyrene sulfonate (Kayexalate, sanofi-aventis, Bridgemater, NJ), 15 g by oral route; morphine, 4 mg by intravenous (IV) route; and promethazine, 12.5 mg IV, before undergoing computed tomographic scan with oral and IV contrast that showed focal inflammation in the transverse colon (Fig. 1A). She was subsequently hospitalized.
Fig. 1.
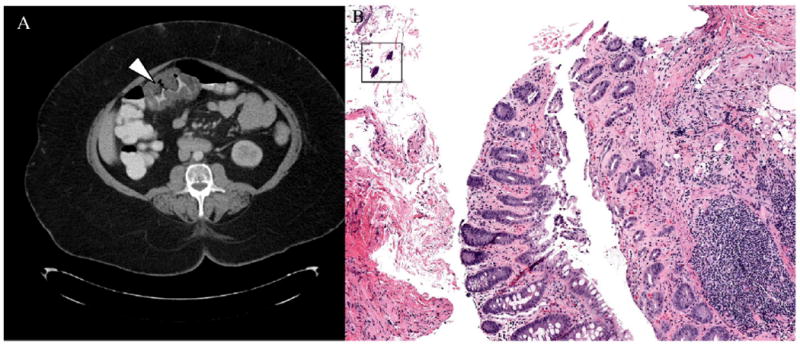
A, On computed tomographic scan of the abdomen, with IV and oral contrast, a focal region (arrowhead) of large bowel in the proximal transverse colon, near the hepatic flexure, demonstrates circumferential wall thickening and pericolonic stranding. This region of inflammation extends for approximately 7.5 cm. B, Fragments of colonic mucosa have miniaturized crypts (a few normal-sized crypts are present at the bottom center for comparison) with leakage of red blood cells and fibrin into the surrounding lamina propria. A box surrounds angulated, basophilic crystals, a typical appearance of Kayexalate in histologic sections, ×100.
After gastroenterology consult, she underwent endoscopy, which uncovered gastritis, and colonoscopy, during which a large, sessile mass in the midtransverse colon was subjected to biopsy. Microscopic examination of the specimen revealed crypt miniaturization with leakage of red blood cells and fibrin into the lamina propria associated with polygonal basophilic crystals (Fig. 1B), findings consistent with Kayexalate-induced colonic injury. She was started on a proton pump inhibitor, which relieved her epigastric discomfort; in outpatient follow-up 2 weeks later, she reported no abdominal pain, nausea, diarrhea, melena, or hematochezia.
Kayexalate, a cation exchange resin, has been used orally or as an enema in the management of hyperkalemia for more than 30 years. The sodium polystyrene sulfate is usually mixed with sorbitol, a cathartic, to avoid constipation and fecal impaction. Colonic necrosis is a rare complication of Kayexalate therapy first described in a 1987 series of 5 uremic patients [1]. Subsequent reports have focused on postsurgical patients, as decreased colonic motility due to postoperative ileus and/or opiate use may increase the duration of drug contact with the intestinal mucosa [2-5]. Cases have been diagnosed from hours to several days after drug administration and over a range of doses. Patients typically report abdominal pain, nausea, diarrhea, and/or hematochezia. Our patient had similar complaints, but these preceded her exposure to Kayexalate and were likely due to gastritis. She had no recent surgeries but, notably, was given IV morphine along with Kayexalate. Histologic evidence of angulated crystals of sodium polystyrene sulfate in areas of mucosal erosions, ulceration, or frank necrosis suggests the diagnosis, which can only be made by biopsy.
With the rising prevalence rates of chronic and end-stage kidney disease, clinicians can expect to see a concomitant increase in hyperkalemic events. Therefore, surveillance against even a rare side effect such as Kayexalate-induced colonic necrosis, which in one series occurred in 1.8% of patients (2/117) exposed to Kayexalate within 1 week of surgery [2], is crucial. Avoiding the use of this medication in the postoperative period and in patients with gastrointestinal motility disorders (either idiopathic or medication-induced) should decrease the risk for colonic necrosis. As hypertonic sorbitol may directly damage intestinal mucosa, Kayexalate preparations using another cathartic may be less toxic. Perhaps most importantly, this exchange resin should only be used in episodes of severe, potentially life-threatening hyperkalemia, as there are other available routes of lowering serum potassium (eg, diuretics, β-agonists, insulin) and mild elevations in serum potassium without electrocardiogram changes may not be clinically meaningful. In retrospect, our patient, who had never run potassium levels greater than 5.0 mmol/L, whose bicarbonate was low reflecting gastrointestinal losses from diarrhea, whose electrocardiogram was unremarkable, and whose potassium 7 hours after initial laboratories had come down to 4.7 mmol/L, did not need to receive Kayexalate therapy. Her mild hyperkalemia, which was not life-threatening, resolved due to IV fluids correcting a mild metabolic acidosis.
Contributor Information
Andrew S. Bomback, Email: abomback@unch.unc.edu, Division of Nephrology and Hypertension, Department of Medicine, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, University of North Carolina Kidney Center, Campus Box 7155, Chapel Hill, NC 27599-7155, USA.
John T. Woosley, Department of Pathology and Laboratory Medicine, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Abhijit V. Kshirsagar, Division of Nephrology and Hypertension, Department of Medicine, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
References
- 1.Lillemoe KD, Romolo JL, Hamilton SR, Pennington LR, Burdick JF, Williams GM. Intestinal necrosis due to sodium polystyrene (Kayexalate) in sorbitol enemas: clinical and experimental support for the hypothesis. Surgery. 1987;101(3):267–72. [PubMed] [Google Scholar]
- 2.Gerstman BB, Kirkman R, Platt R. Intestinal necrosis associated with postoperative orally administered sodium polystyrene sulfonate in sorbitol. Am J Kidney Dis. 1992;20(2):159–61. doi: 10.1016/s0272-6386(12)80544-0. [DOI] [PubMed] [Google Scholar]
- 3.Scott TR, Graham SM, Schweitzer EJ, Bartlett ST. Colonic necrosis following sodium polystyrene sulfonate (Kayexalate)-sorbitol enema in a renal transplant patient. Report of a case and review of the literature. Dis Colon Rectum. 1993;36(6):607–9. doi: 10.1007/BF02049870. [DOI] [PubMed] [Google Scholar]
- 4.Rashid A, Hamilton SR. Necrosis of the gastrointestinal tract in uremic patients as a result of sodium polystyrene sulfonate (Kayexalate) in sorbitol: an underrecognized condition. Am J Surg Pathol. 1997;21(1):60–9. doi: 10.1097/00000478-199701000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Rogers FB, Li SC. Acute colonic necrosis associated with sodium polystyrene sulfonate (Kayexalate) enemas in a critically ill patient: case report and review of the literature. J Trauma. 2001;51(2):395–7. doi: 10.1097/00005373-200108000-00031. [DOI] [PubMed] [Google Scholar]