

Abstract
Aims
To evaluate multinational patterns of gender- and age-specific alcohol consumption.
Design and participants
Large general-population surveys of men’s and women’s drinking behavior (N’s > 900) in 35 countries in 1997–2007 used a standardized questionnaire (25 countries) or measures comparable to those in the standardized questionnaire.
Measurements
Data from men and women in three age groups (18–34, 35–49, 50–65) showed the prevalence of drinkers, former drinkers, and lifetime abstainers; and the prevalence of high-frequency, high-volume, and heavy episodic drinking among current drinkers. Analyses examined gender ratios for prevalence rates and the direction of changes in prevalence rates across age groups.
Findings
Drinking per se and high-volume drinking were consistently more prevalent among men than among women, but lifetime abstention from alcohol was consistently more prevalent among women. Among respondents who had ever been drinkers, women in all age groups were consistently more likely to have stopped drinking than men were. Among drinkers, the prevalence of high-frequency drinking was consistently greatest in the oldest age group, particularly among men. Unexpectedly, the prevalence of drinking per se did not decline consistently with increasing age, and declines in high-volume and heavy episodic drinking with increasing age were more typical in Europe and English-speaking countries.
Conclusions
As expected, men still exceed women in drinking and high-volume drinking, although gender ratios vary. Better explanations are needed for why more women than men quit drinking, and why aging does not consistently reduce drinking and heavy drinking outside Europe and English-speaking countries.
Keywords: alcohol, drinking patterns, gender differences, age differences, multinational
INTRODUCTION
Research attention to gender differences in alcohol consumption, and attention to the ways that such gender differences both cut across and are influenced by cultural differences, has greatly increased in recent decades (e.g., [1–3]), in part through the efforts of the International Research Group on Gender and Alcohol [4–6].
This research has generally focused on a few basic questions. The simplest question is whether there are consistent differences between how men and women drink. Wherever in the world research is carried out, the answers to this question are consistently that men are more likely to consume alcohol than women are (e.g., [6–8]); male drinkers consume larger quantities of alcohol than female drinkers do (e.g., [9–11]); and male drinkers experience more behavioral problems related to their drinking than female drinkers do (e.g., [12–14]).
A more complex question is, how do gender differences in alcohol consumption vary across different settings and drinking patterns? One approach to answering this question has sought to learn whether gender differences in drinking patterns are declining historically, because of increases in women’s drinking related to other changes in women’s roles, or because men may have reduced their drinking more than women have. There is evidence for such convergence in particular time periods, age groups, places, and/or drinking patterns [15–18], but there is no evidence that gender differences have been entirely erased anywhere in the world [5, 19–21].
A second answer to the question of how gender differences vary across settings has been the claim, supported by some evidence [6, 22, 23], that men and women differ most in the likelihood of engaging in extremely heavy drinking (predominantly male behavior) and differ least in the prevalence of drinking per se. A third and more challenging way to answer the question is to discover whether patterns of cultural differences may help to explain why gender differences in drinking patterns are larger in some places and smaller in others. The third approach is one of the major tasks undertaken by the GENACIS project (Gender, Alcohol and Culture: An International Study), which has now produced comparable general-population data on men’s and women’s drinking behavior in more than 40 countries [24–26].
In research on consistencies and variations of gender differences in drinking patterns, two important questions have not received adequate attention. The first and more obvious question is whether gender influences on drinking patterns differ consistently in different regions of the world (for example, between well-studied countries of Europe and North America and less-well-studied countries of Africa, Asia, and Latin America). A second neglected question is whether aging or stages of adult life affect drinking patterns similarly or differently for men and women [1]. Answers to this second question might also vary because of conditions in the larger social environment. Analyses of data from the GENACIS surveys presented here provide some partial answers to these two questions, indicating patterns in gender-specific drinking behavior that are in need of further cultural and theoretical analysis.
METHODS
Survey characteristics and methods
Data for this paper come from general population surveys in 35 countries: Argentina, Australia, Belize, Brazil, Canada, Costa Rica, Czech Republic, Denmark, Finland, France, Germany, Great Britain, Hungary, Iceland, India, Ireland, Isle of Man, Israel, Italy, Japan, Kazakhstan, Mexico, the Netherlands, New Zealand, Nicaragua, Nigeria, Norway, Peru, Spain, Sri Lanka, Sweden, Switzerland, Uganda, the United States, and Uruguay. In one country (Great Britain) portions of two surveys were used to allow more complete measurement of drinking variables.
Table 1 summarizes characteristics of the surveys analyzed here. The surveys differ somewhat in sampling frame (regional vs. national), sampling method (probability, replacement, or quota), age range of samples, and modes of administration. Because of variations in sampling methods and recording of nonrespondents, response rates were not available for all surveys; response rates of surveys with random probability sampling ranged from 38% to 96%, with a median of 68%. Despite these variations, the GENACIS surveys are more similar than data sets for many other multinational studies (see, e.g., [27, 28]. All surveys conducted after November 2001, when the GENACIS questionnaire was finalized (see below), were expected to meet certain minimum standards: (1) sample size of at least 1,000; (2) inclusion of both women and men; (3) multi-stage random sampling, with clusters (e.g., a village or a defined area within a town); (4) either a national sample or, in large countries such as India, sampling of an entire province or region that (a) included both urban and rural areas, (b) corresponded to a governmental unit for which there are aggregate statistics, and (c) included a large population of drinkers; (5) strenuous effort to attain a completion rate of 70% or higher; and (6) inclusion of all questions from the common GENACIS questionnaire, with a few (rare) exceptions of specific questions judged by the survey leader and staff to be culturally inappropriate for their country.
Table 1.
GENACIS Survey Characteristics
| Country | Survey Year | Age Range | Women n | Men n | Sampling Frame | Survey Mode |
|---|---|---|---|---|---|---|
| Argentina | 2003 | 18–65 | 598 | 402 | regional1 | face-to-face |
| Australia | 2007 | 18+ | 1284 | 1199 | regional2 | telephone |
| Belize | 2005 | 18+ | 2172 | 1990 | national | face-to-face |
| Brazil | 2002 | 17+ | 696 | 562 | regional3 | face-to-face |
| Canada | 2004 | 18–76 | 8054 | 6009 | national | telephone |
| Costa Rica | 2003 | 18+ | 857 | 416 | regional4 | face-to-face |
| Czech Republic | 2002 | 18–64 | 1282 | 1244 | national | face-to-face |
| Denmark | 2003 | 15–99 | 1133 | 897 | national | telephone |
| Finland | 2000 | 16–70 | 987 | 945 | national | face-to-face |
| Francea | 2000 | 18–64 | 525 | 475 | national | telephone |
| Germany | 2000 | 18–60 | 4459 | 3688 | national | postal |
| Great Britain | 2000 | 18+ | 1038 | 963 | national | face-to-face |
| Hungary | 2001 | 19–65 | 1198 | 1094 | national | face-to-face |
| Iceland | 2001 | 18–75 | 1271 | 1168 | national | postal/ telephone |
| India | 2003 | 16+ | 1347 | 1250 | regional5 | face-to-face |
| Ireland | 2002 | 18+ | 551 | 518 | national | face-to-face |
| Isle of Man | 2005 | 18+ | 547 | 453 | national | telephone/ face-to-face |
| Israel | 2001 | 18–40 | 3393 | 2611 | national | face-to-face |
| Italya | 2000 | 18–64 | 514 | 486 | national | telephone |
| Japan | 2001 | 20–70 | 1138 | 1116 | national | SAQb |
| Kazakhstan | 2002 | 18+ | 631 | 539 | regional | face-to-face |
| Mexico | 1998 | 18–65 | 3329 | 2382 | national | face-to-face |
| Netherlands | 1999 | 16–69 | 2214 | 2008 | regional6 | postal |
| New Zealand | 2007 | 18–70 | 1055 | 820 | national | postal |
| Nicaragua | 2005 | 18+ | 1416 | 614 | regional7 | face-to-face |
| Nigeria | 2003 | 18+ | 956 | 1114 | regional8 | face-to-face |
| Norway | 1999 | 15+ | 1136 | 1034 | national | face-to-face |
| Peru | 2005 | 18–65 | 1015 | 516 | regional9 | face-to-face |
| Spain | 2002 | 18+ | 956 | 894 | regional10 | face-to-face |
| Sri Lanka | 2002 | 18+ | 593 | 608 | regional11 | face-to-face |
| Sweden | 2002 | 17+ | 2816 | 2656 | national | telephone |
| Switzerland | 1997 | 15+ | 7239 | 5755 | national | telephone |
| Uganda | 2003 | 18+ | 758 | 721 | regional12 | face-to-face |
| UKa,c | 2000 | 18–64 | 581 | 403 | national | telephone |
| USA | 2000 | 18+ | 4142 | 3470 | national | telephone |
| Uruguay | 2004 | 18–65 | 624 | 376 | national | face-to-face |
European Comparative Alcohol Study (ECAS).
Self-administered questionnaire delivered by survey staff, returned by mail.
Used only for HED estimate.
Province of Buenos Aires and city of Buenos Aires.
State of Victoria.
Greater São Paulo (city of São Paulo plus 38 other municipalities).
Greater Metropolitan Area.
Five districts in the state of Karnataka: Bangalore (urban and rural districts), Dakshina Kannada, Davanagere, and Bidar.
Province of Limburg.
Five mid-sized cities: Bluefields, Estelí, Juigalpa, León, and Rivas.
Three states in the north: Benue, Nasarawa, and Plateu; two states in the south: Akwa Ibom, and Rivers.
Lima and Ayacucho regions.
Valencia region.
17 of 25 districts.
Four districts: Kabale, Wakiso, Tororo, and Lira.
Survey leaders in all countries had experience conducting survey research and drew on expertise in sampling and statistical methods from regional universities and government agencies. Interviewers were generally mental health professionals (e.g., psychologists, social workers), graduate and professional students, or other persons with university education. Additional information about sampling and data collection procedures in individual countries can be found in other GENACIS publications [24, 25, 29]. All relevant ethical guidelines for protection of human subjects were followed. Individual country surveys were reviewed according to procedures created to protect research participants in their countries. The overall GENACIS project was reviewed and approved by the Institutional Review Board of the University of North Dakota.
Survey questionnaire
Development and use of the GENACIS questionnaire
Project members collaborated over a two-year period to design the GENACIS questionnaire. In addition to demographic characteristics, drinking patterns, drinking contexts, and drinking-related problems, major questionnaire domains included social roles, intimacy and sexuality, violence and victimization, and health and lifestyle. Measures of alcohol use patterns are described in more detail below.
Surveys conducted after the standard GENACIS questionnaire was completed used that questionnaire. Of the 36 surveys providing data for the analyses here, 25 used some version of the GENACIS questionnaire. The remaining 11 surveys measured drinking variables in ways quite similar to the GENACIS questionnaire. Most of the surveys not using the GENACIS questionnaire were conducted before 2002 in European Union countries that made up an EU sub-study of the GENACIS project. Detailed descriptions of how comparable drinking variables were developed from these EU surveys can be found in reports from the EU sub-study [22–24].
Translating the questionnaire
Most questions and measures were taken from well-validated survey instruments, and wherever possible from instruments that had been used in several different countries. Most questions were written initially in English. Guidelines for question translation were adapted from procedures used by the World Health Organization [30] and other sources. (Translation guidelines can be found at the GENACIS website: http://www.med.und.nodak.edu/depts/irgga.) Prior to survey use, all questions were translated into the language of that survey and then back-translated to check for accuracy and cultural appropriateness of translation, with subsequent independent review of the translation [31]. Where surveys required the use of more than one language, the questionnaire was translated into the most commonly understood language, and then interviewers were selected and trained so that they could translate the questionnaire for other language groups.
Data centralization
The Swiss Institute for the Prevention of Alcohol and Drug Problems (SIPA) in Lausanne, Switzerland, provides centralized management of the GENACIS data base. After local cleaning and editing, de-identified survey data sets are transmitted to SIPA, where further standardized data editing is conducted and each data set is merged with the central GENACIS data base. Data are stored in a secure password-protected file with back-up files stored securely offsite.
Measures
Drinking patterns
Questions in the GENACIS questionnaire were designed to obtain information about drinking patterns as well as the total volume of alcohol consumed. Questions asked about the generic frequency of drinking (any type of alcoholic beverage) in the past 12 months, generic quantity (typical number of drinks, combining all types of alcoholic beverages, on a drinking day), and beverage-specific frequency and quantity (separate questions for wine, beer, and liquor). The questionnaire included provisions for asking about local or culturally unique alcoholic beverages, and it contained a reference chart for estimating average sizes of “drinks” of each type of alcoholic beverage in the survey country and for converting drinks of each beverage type into grams of ethanol.
Lifetime abstention, former drinking, and current drinking
Nearly all GENACIS surveys could identify respondents who had never consumed alcohol (lifetime abstainers), those who had consumed alcohol but not in the past 12 months (former drinkers), and those who had consumed alcoholic beverages during the past 12 months (current drinkers).
Drinking frequency
Surveys using the GENACIS questionnaire had nine categories of drinking frequency (generic, i.e., across all beverage types) in the past 12 months: never, once, twice, 3–6 times, 7–11 times, 1–3 times a month, once or twice a week, 3 or 4 times a week, every day or nearly every day. In other surveys, frequency data were recoded to be as comparable as possible to the GENACIS frequency categories (see [24], Chapter 1 and Appendix A1). The present analyses focused on the prevalence of high-frequency drinking (five or more days a week) among individuals who had consumed alcohol in the preceding 12 months.
Drinking volume
For most countries using the GENACIS questionnaire, volume was calculated by multiplying generic drinking frequency by generic quantity per drinking day (in drinks per day postcoded as grams of ethanol), to give the estimated grams of ethanol consumed in the past 12 months. Standardized guidelines for calculating 12-month volume from surveys asking only beverage-specific frequency and quantity questions are described in Bloomfield et al. [24]. The analyses here focus on high-volume drinking. The threshold for high-volume drinking was set at the equivalent of consuming >1 ounce of ethanol per day for the preceding year; this amount was converted into grams of ethanol, giving a threshold for high-volume drinking of >8468 grams of ethanol per year (on average, >23.2 g/day).
Heavy episodic drinking
To detect heavy episodic drinking (HED), surveys using the GENACIS questionnaire asked about consumption of five or more drinks in a single day. In most other surveys, questions about HED used a threshold of five or six drinks in a day [24, Appendix A1]. Because ethanol content varies by beverage and drink size, the threshold for HED was set at 60 grams of ethanol in a day, based on the ethanol content of an average drink in each country (with a few exceptions specified in Table 2). Ideally a measure of heavy episodic drinking would assess consumption of a large amount of alcohol in a relatively short period of time (e.g., 2–3 hours; see [32]). However, few GENACIS surveys asked about periods of time shorter than a day, over which drinking occurred, so this more precise measure of HED was not possible. Therefore the analyses here examined the prevalence among current drinkers of ever vs. never consuming at least 60 grams of ethanol in a day in the preceding 12 months.
Table 2.
Drinking Status and Drinking Patterns: Gender Ratios by Country and Age
| Total Sample | Ever Drinker | 12-Month Drinkers Only | |||||
|---|---|---|---|---|---|---|---|
| Country | Age Category | Lifetime Abstainer (M/F) | Current Drinkers (M/F) | Former Drinkers (M/F) | High Frequency (M/F) | High Volume (M/F) | Any HED (M/F) |
| Argentina | 18 – 34 | 1.06 | 1.14 | 0.17 | 25.80 | ∞ | 3.51 |
| 35 – 49 | 0.33 | 1.16 | 0.54 | 3.37 | 31.86 | 10.21 | |
| 50 – 65 | 0.00 | 1.33 | 0.27 | 1.96 | 4.10 | 3.94 | |
| Total | 0.37 | 1.20 | 0.30 | 3.04 | 14.64 | 4.83 | |
| Australia | 18 – 34 | 1.67 | 1.10 | 0.20 | 2.23 | 2.92 | 1.37 |
| 35 – 49 | 0.56 | 1.09 | 0.46 | 2.06 | 3.33 | 1.67 | |
| 50 – 65 | 0.61 | 1.11 | 0.54 | 1.37 | 4.42 | 4.15 | |
| Total | 1.05 | 1.10 | 0.40 | 1.68 | 3.43 | 1.73 | |
| Belizea | 18 – 34 | 0.43 | 2.34 | 0.57 | 1.00 | 4.74 | 1.62 |
| 35 – 49 | 0.29 | 2.57 | 0.66 | 8.57 | 4.08 | 1.44 | |
| 50 – 65 | 0.27 | 4.01 | 0.67 | ∞ | 5.50 | 1.78 | |
| Total | 0.35 | 2.57 | 0.64 | 3.08 | 4.55 | 1.56 | |
| Brazil | 18 – 34 | 0.47 | 1.62 | 0.58 | 0.97 | 1.23 | 1.32 |
| 35 – 49 | 0.57 | 1.87 | 0.53 | 5.71 | 2.95 | 1.24 | |
| 50 – 65 | 0.65 | 1.20 | 0.89 | 0.77 | 1.37 | 1.10 | |
| Total | 0.57 | 1.54 | 0.62 | 1.26 | 1.58 | 1.28 | |
| Canada | 18 – 34 | 0.65 | 1.11 | 0.55 | 3.30 | 3.24 | 1.37 |
| 35 – 49 | 0.57 | 1.06 | 0.87 | 1.73 | 3.19 | 1.65 | |
| 50 – 65 | 0.53 | 1.07 | 0.94 | 2.00 | 4.04 | 2.45 | |
| Total | 0.57 | 1.08 | 0.80 | 2.00 | 3.49 | 1.68 | |
| Costa Rica | 18 – 34 | 0.55 | 1.61 | 0.35 | ∞ | 4.75 | 1.64 |
| 35 – 49 | 0.51 | 1.46 | 0.65 | 1.36 | 6.27 | 1.95 | |
| 50 – 65 | 0.35 | 1.56 | 0.71 | ∞ | ∞ | 5.65 | |
| Total | 0.49 | 1.54 | 0.54 | 7.50 | 5.56 | 1.89 | |
| Czech Republica,b | 18 – 34 | 0.73 | 1.06 | 0.61 | 5.90 | 3.41 | 1.50 |
| 35 – 49 | 0.57 | 1.14 | 0.32 | 3.30 | 3.85 | 1.73 | |
| 50 – 65 | 0.13 | 1.23 | 0.47 | 4.85 | 5.11 | 2.09 | |
| Total | 0.49 | 1.13 | 0.47 | 4.44 | 3.90 | 1.67 | |
| Denmarka | 18 – 34 | 1.36 | 1.04 | 0.41 | 5.75 | 3.49 | 1.18 |
| 35 – 49 | 0.64 | 1.04 | 0.16 | 3.07 | 3.96 | 1.47 | |
| 50 – 65 | 0.27 | 1.02 | 0.73 | 2.21 | 3.86 | 1.70 | |
| Total | 0.75 | 1.03 | 0.42 | 2.57 | 3.65 | 1.40 | |
| Finland | 18 – 34 | 0.23 | 1.03 | 1.39 | ∞ | 7.52 | 1.24 |
| 35 – 49 | 1.43 | 0.97 | 1.59 | 5.71 | 5.82 | 1.72 | |
| 50 – 65 | 0.53 | 1.04 | 0.96 | 13.75 | 4.71 | 2.27 | |
| Total | 0.57 | 1.01 | 1.19 | 8.50 | 5.87 | 1.60 | |
| Francea,b,c | 18 – 34 | 1.26 | 4.79 | 5.51 | 1.48 | ||
| 35 – 49 | 1.15 | 2.33 | 3.16 | 1.64 | |||
| 50 – 65 | 1.18 | 1.77 | 7.02 | 2.00 | |||
| Total | 1.20 | 1.83 | 4.59 | 1.68 | |||
| Germanya,b | 18 – 34 | 0.85 | 1.01 | 0.89 | 4.22 | 3.18 | 2.42 |
| 35 – 49 | 0.36 | 1.01 | 1.24 | 2.47 | 2.89 | 3.19 | |
| 50 – 65 | 0.29 | 1.04 | 0.70 | 2.56 | 3.06 | 4.29 | |
| Total | 0.58 | 1.01 | 0.91 | 2.82 | 3.02 | 2.91 | |
| Great Britaina,d | 18 – 34 | 0.80 | 1.03 | 0.80 | 1.15 | 3.19 | 1.11 |
| 35 – 49 | 0.81 | 1.04 | 0.69 | 1.41 | 3.62 | 1.37 | |
| 50 – 65 | 0.35 | 1.22 | 0.84 | 1.56 | 3.95 | 1.68 | |
| Total | 0.57 | 1.09 | 0.77 | 1.39 | 3.53 | 1.31 | |
| Hungaryb | 18 – 34 | 0.30 | 1.13 | 0.46 | ∞ | 13.17 | 1.71 |
| 35 – 49 | 0.33 | 1.18 | 0.69 | 9.57 | 24.00 | 1.91 | |
| 50 – 65 | 0.20 | 1.36 | 0.62 | 4.75 | 31.50 | 2.50 | |
| Total | 0.27 | 1.21 | 0.61 | 8.14 | 20.17 | 1.92 | |
| Icelanda | 18 – 34 | 1.29 | 1.00 | 0.77 | 3.00 | 5.89 | 1.20 |
| 35 – 49 | 0.68 | 1.00 | 1.11 | 1.80 | 6.38 | 1.44 | |
| 50 – 65 | 0.46 | 1.06 | 0.99 | ∞ | 3.61 | 1.81 | |
| Total | 0.76 | 1.01 | 0.98 | 3.67 | 5.22 | 1.35 | |
| Indiaa | 18 – 34 | 0.63 | 18.78 | 0.29 | 3.10 | 2.14 | 2.74 |
| 35 – 49 | 0.48 | 7.67 | 0.31 | 2.04 | 1.91 | 2.07 | |
| 50 – 65 | 0.64 | 13.04 | 0.40 | 1.70 | 1.92 | 2.17 | |
| Total | 0.60 | 12.33 | 0.31 | 1.83 | 1.74 | 2.17 | |
| Ireland | 18 – 34 | 0.69 | 1.06 | 0.99 | ∞ | 2.23 | 1.25 |
| 35 – 49 | 0.56 | 1.10 | 1.33 | ∞ | 3.42 | 1.72 | |
| 50 – 65 | 0.90 | 1.05 | 0.94 | 2.08 | 5.57 | 1.70 | |
| Total | 0.73 | 1.07 | 1.06 | 7.00 | 2.90 | 1.47 | |
| Isle of Man | 18 – 34 | N/A | 1.05 | 0.44 | 1.91 | 2.48 | 1.46 |
| 35 – 49 | 0.00 | 1.02 | 0.78 | 1.69 | 2.71 | 1.92 | |
| 50 – 65 | 0.44 | 1.15 | 0.26 | 1.42 | 4.33 | 3.50 | |
| Total | 0.33 | 1.08 | 0.40 | 1.54 | 3.09 | 2.03 | |
| Israelb,c | 18 – 34 | 1.38 | 2.74 | 1.81 | |||
| 35 – 49 | 1.27 | 3.79 | 2.38 | ||||
| 50 – 65 | |||||||
| Total | 1.36 | 3.00 | 1.96 | ||||
| Italya,b,c | 18 – 34 | 1.17 | 1.55 | 2.99 | 1.55 | ||
| 35 – 49 | 1.15 | 1.77 | 2.31 | 1.30 | |||
| 50 – 65 | 1.09 | 1.26 | 3.64 | 1.54 | |||
| Total | 1.14 | 1.41 | 3.00 | 1.50 | |||
| Japana,b | 18 – 34 | 1.09 | 1.06 | 0.29 | 2.78 | 4.64 | 1.69 |
| 35 – 49 | 0.33 | 1.14 | 0.28 | 2.53 | 4.83 | 1.95 | |
| 50 – 65 | 0.27 | 1.26 | 0.56 | 2.93 | 6.77 | 2.04 | |
| Total | 0.35 | 1.16 | 0.39 | 2.75 | 5.54 | 1.89 | |
| Kazakhstan | 18 – 34 | 0.52 | 1.16 | 0.70 | ∞ | 9.05 | 1.24 |
| 35 – 49 | 0.27 | 1.06 | 1.02 | 7.50 | 13.29 | 1.39 | |
| 50 – 65 | 0.41 | 1.30 | 0.56 | 3.82 | 22.00 | 1.38 | |
| Total | 0.43 | 1.16 | 0.74 | 5.67 | 12.47 | 1.32 | |
| Mexicoa | 18 – 34 | 0.28 | 1.77 | 0.43 | 19.00 | 8.48 | 3.91 |
| 35 – 49 | 0.19 | 1.59 | 0.65 | 6.67 | 10.04 | 3.45 | |
| 50 – 65 | 0.13 | 1.88 | 0.70 | 11.00 | 9.64 | 3.07 | |
| Total | 0.23 | 1.72 | 0.56 | 8.86 | 9.24 | 3.64 | |
| The Netherlands | 18 – 34 | 0.62 | 1.18 | 0.53 | 3.80 | 5.58 | 1.71 |
| 35 – 49 | 0.28 | 1.19 | 0.49 | 1.64 | 3.02 | 1.78 | |
| 50 – 65 | 0.29 | 1.37 | 0.48 | 1.63 | 2.96 | 2.04 | |
| Total | 0.40 | 1.23 | 0.51 | 1.89 | 3.61 | 1.79 | |
| New Zealanda | 18 – 34 | 1.62 | 0.93 | 1.79 | 2.02 | 2.78 | 1.23 |
| 35 – 49 | 0.43 | 1.04 | 0.88 | 0.74 | 1.83 | 1.34 | |
| 50 – 65 | 0.39 | 1.05 | 0.98 | 1.10 | 2.25 | 2.60 | |
| Total | 0.75 | 1.00 | 1.23 | 1.08 | 2.30 | 1.39 | |
| Nicaragua | 18 – 34 | 0.22 | 4.01 | 0.56 | 0.60 | 2.39 | 1.42 |
| 35 – 49 | 0.29 | 4.22 | 0.67 | 0.56 | 3.18 | 1.69 | |
| 50 – 65 | 0.20 | 5.87 | 0.79 | ∞ | 2.00 | 1.47 | |
| Total | 0.24 | 4.12 | 0.63 | 0.68 | 2.51 | 1.48 | |
| Nigeria | 18 – 34 | 0.83 | 1.87 | 0.57 | 4.36 | 1.53 | 0.88 |
| 35 – 49 | 0.70 | 1.84 | 0.54 | 1.50 | 1.27 | 1.36 | |
| 50 – 65 | 0.95 | 1.54 | 0.59 | 1.59 | 1.14 | 1.27 | |
| Total | 0.75 | 1.87 | 0.56 | 2.09 | 1.34 | 1.21 | |
| Norwaya | 18 – 34 | 1.31 | 1.00 | 0.86 | 1.00 | 5.32 | 1.46 |
| 35 – 49 | 1.22 | 0.99 | 1.27 | 4.10 | 7.42 | 1.63 | |
| 50 – 65 | 0.30 | 1.04 | 1.02 | 4.00 | 14.00 | 2.33 | |
| Total | 0.67 | 1.00 | 1.04 | 3.88 | 6.38 | 1.58 | |
| Peru | 18 – 34 | 0.51 | 1.35 | 0.36 | N/A | 26.00 | 1.69 |
| 35 – 49 | 0.00 | 1.45 | 0.38 | ∞ | ∞ | 1.55 | |
| 50 – 65 | 0.30 | 1.24 | 0.74 | 1.75 | 1.69 | 1.24 | |
| Total | 0.38 | 1.36 | 0.46 | 2.50 | 10.40 | 1.57 | |
| Spaina | 18 – 34 | 0.63 | 1.26 | 0.58 | 3.68 | 2.74 | 1.51 |
| 35 – 49 | 0.44 | 1.43 | 0.55 | 1.99 | 4.40 | 1.51 | |
| 50 – 65 | 0.24 | 1.79 | 0.54 | 2.03 | 10.34 | 2.28 | |
| Total | 0.43 | 1.43 | 0.56 | 2.41 | 4.29 | 1.58 | |
| Sri Lanka | 18 – 34 | 0.31 | 7.46 | 0.59 | ∞ | 2.64 | ∞ |
| 35 – 49 | 0.17 | 8.55 | 0.50 | ∞ | ∞ | ∞ | |
| 50 – 65 | 0.18 | 10.61 | 0.61 | ∞ | ∞ | ∞ | |
| Total | 0.22 | 8.37 | 0.58 | ∞ | 10.23 | ∞ | |
| Swedena | 18 – 34 | 0.69 | 1.08 | 0.32 | 7.67 | 5.08 | 1.40 |
| 35 – 49 | 0.59 | 1.06 | 0.60 | 2.11 | 3.86 | 1.83 | |
| 50 – 65 | 0.47 | 1.08 | 0.66 | 2.71 | 6.00 | 2.51 | |
| Total | 0.57 | 1.08 | 0.54 | 2.88 | 4.95 | 1.72 | |
| Switzerlanda | 18 – 34 | 0.46 | 1.16 | 0.42 | 3.14 | 4.94 | 3.41 |
| 35 – 49 | 0.23 | 1.15 | 0.92 | 2.25 | 4.29 | 3.29 | |
| 50 – 65 | 0.29 | 1.17 | 0.65 | 2.05 | 4.50 | 5.70 | |
| Total | 0.34 | 1.16 | 0.65 | 2.22 | 4.47 | 3.60 | |
| Uganda | 18 – 34 | 0.88 | 1.18 | 0.84 | 3.28 | 2.82 | 1.95 |
| 35 – 49 | 0.67 | 1.47 | 0.52 | 3.54 | 3.28 | 1.67 | |
| 50 – 65 | 0.71 | 1.50 | 0.47 | 1.50 | 1.88 | 2.03 | |
| Total | 0.82 | 1.30 | 0.70 | 3.02 | 2.87 | 1.88 | |
| USAa | 18 – 34 | 0.72 | 1.13 | 0.72 | 3.23 | 3.75 | 1.71 |
| 35 – 49 | 0.63 | 1.14 | 0.79 | 2.80 | 2.87 | 2.06 | |
| 50 – 65 | 0.50 | 1.18 | 0.91 | 2.17 | 3.22 | 4.95 | |
| Total | 0.62e | 1.14e | 0.81e | 2.67 | 3.30 | 2.00 | |
| Uruguay | 18 – 34 | 0.24 | 1.21 | 0.49 | 2.06 | 4.71 | 2.59 |
| 35 – 49 | 0.31 | 1.38 | 0.57 | 1.27 | 7.61 | 8.31 | |
| 50 – 65 | 0.29 | 1.48 | 0.60 | 3.48 | 7.26 | 4.98 | |
| Total | 0.28 | 1.34 | 0.55 | 2.17 | 5.79 | 3.70 | |
Note. High frequency = 5+ days per week. High volume = 8468+ grams of pure ethanol in a year. HED = 60+ grams of pure ethanol in a day (exceptions noted below).
HED = 50+ grams (Belize, India, New Zealand, Spain); 65+ grams (Iceland, Mexico); 70+ grams (Germany, USA); 72+ grams (Japan, Sweden); 75+ grams (Denmark, France, Italy, UK); 80+ grams (Switzerland); 90+ grams (Czech Republic); 74–112 grams (average 87 grams, Norway).
Age ranges used in these analyses: 18–64 (Czech Republic, France, Italy, UK); 18–60 (Germany); 19–65 (Hungary); 18–40 (Israel); 20–65 (Japan). All other countries 18–65.
Survey did not differentiate lifetime abstainers from former drinkers.
HED estimate obtained from UK survey.
Mean of values from 1996 and 2005 U.S. national surveys because of difficulties in identifying former drinkers in the 2000 survey.
No female respondents.
Gender and age
To describe patterns in the prevalence of drinking behavior, we divided the survey samples by gender and age. To obtain comparable age groups in as many surveys as possible, with an adequate number of men and women in each age group for each survey, we divided the age ranges for each survey into three categories: ages 18–34, 35–49, and 50–65, excluding respondents under age 18 or over age 65.
Data Analysis
The purpose of this paper is to describe the consistency or variation of patterns in the prevalence of different forms of drinking behavior, in gender × age subgroups of survey samples in 35 countries. For each age group in each survey, gender ratios (male/female) were calculated for the prevalence rates of each form of drinking behavior evaluated (see [6]). For economy of space, the tables that follow present only (1) the gender ratios of prevalence rates, and (2) indicators of gender-specific age groups with the highest prevalence rates, and patterns of change across age groups. Tables of n’s and prevalence rates are available in Tables S1-S5 (see supporting information details at the end of this paper).
To evaluate the consistency of drinking patterns across surveys, we used the binomial theorem. Binomial distributions showed (1) the likelihood that gender ratios >1.0 (or <1.0) occurred as consistently as we observed (e.g., in N surveys), if gender ratios varied entirely by chance; and (2) the likelihood that prevalence rates increased (or decreased) monotonically across three age groups as consistently as we observed (e.g., in N surveys), if that monotonic sequence was one of six equally likely chance orderings of the three age groups.
RESULTS
Expected findings
Results from the analyses of abstention and current drinking show several familiar and expected patterns. Men were consistently more likely than women to be current drinkers. As shown in Table 2, gender ratios of male to female drinking prevalence rates were greater than 1.0 in 98 of 104 comparisons available for separate age groups in 35 surveys, and in all age groups in 31 of 35 surveys (p’s <.001, two-tailed, based on the binomial distribution). The exceptions were gender ratios of 1.00 or less among respondents in some age groups in Finland, Iceland, New Zealand, and Norway. However, male/female ratios for 12-month drinking versus abstention were generally small, with ratios greater than 1.5 in only nine countries (Belize, Brazil, Costa Rica, India, Mexico, Nicaragua, Nigeria, Sri Lanka, and Spain).
Lifetime abstention from alcohol, on the other hand, was consistently reported more often by women than by men. In age-specific data available in 32 surveys, male/female gender ratios were less than 1.0 in 86 of 95 comparisons and in the majority of age groups for 31 of the 32 surveys (p’s <.001). The exceptions were in some age groups in Argentina, Australia, Denmark, Finland, Iceland, Japan, New Zealand, and Norway. In these exceptions, male lifetime abstention exceeded female lifetime abstention by relatively small margins (all but two gender ratios less than 1.5); the exceptions occurred mainly in young adulthood (ages 18–34); and all the exceptions occurred in groups where the lifetime abstention rates for both men and women were quite low (less than 7%) (See Table S2).
At the other end of the drinking spectrum, among 12-month drinkers in all age groups, men were always more likely than women to be high-volume drinkers (consuming >8468 grams of ethanol per year) (104 out of 104 age-specific comparisons, and in all age groups in all 35 countries) (p’s <.001). Drinking men were also consistently more likely than drinking women to be high-frequency drinkers (5 or more days per week) (94 of 101 age-specific comparisons, and in the majority of age groups in 32 of 34 countries, p’s <.001). Exceptions were gender ratios of 1.00 among drinkers aged 18–34 in Belize and Norway; 0.97 and 0.77 among drinkers aged 18–34 and 50–65 in Brazil; 0.74 among drinkers aged 35–49 in New Zealand; and 0.60 and 0.56 among drinkers aged 18–34 and 35–49 in Nicaragua. And male drinkers were consistently more likely than female drinkers to engage in heavy episodic drinking (≥60 grams of ethanol in a drinking day) (103 of 104 age-specific comparisons, and the majority of age groups in all 35 countries, p’s <.001); the one exception was a gender ratio of 0.88 among drinkers aged 18–34 in Nigeria.
Unexpected findings
Former drinkers
The GENACIS data also revealed several unexpected patterns that have not received much attention in alcohol research. One such finding was a consistent gender difference in the likelihood that drinkers would eventually quit drinking. Among survey respondents who were not lifetime abstainers, data available from surveys in 32 countries showed that women were more likely than men to be former rather than current drinkers in 87 of 96 age-specific comparisons, and in the majority of age groups in 30 of the 32 countries (p’s <.001). The exceptions, where men were more likely to have quit drinking than women, were mainly among middle-aged respondents in Finland, Germany, Iceland, Ireland, Kazakhstan, and Norway (but among young drinkers in New Zealand). Thus the exceptions occurred mainly in northern Europe, in age groups where quitting drinking was relatively uncommon (less than 10% of those who had ever been drinkers).
High-frequency drinkers
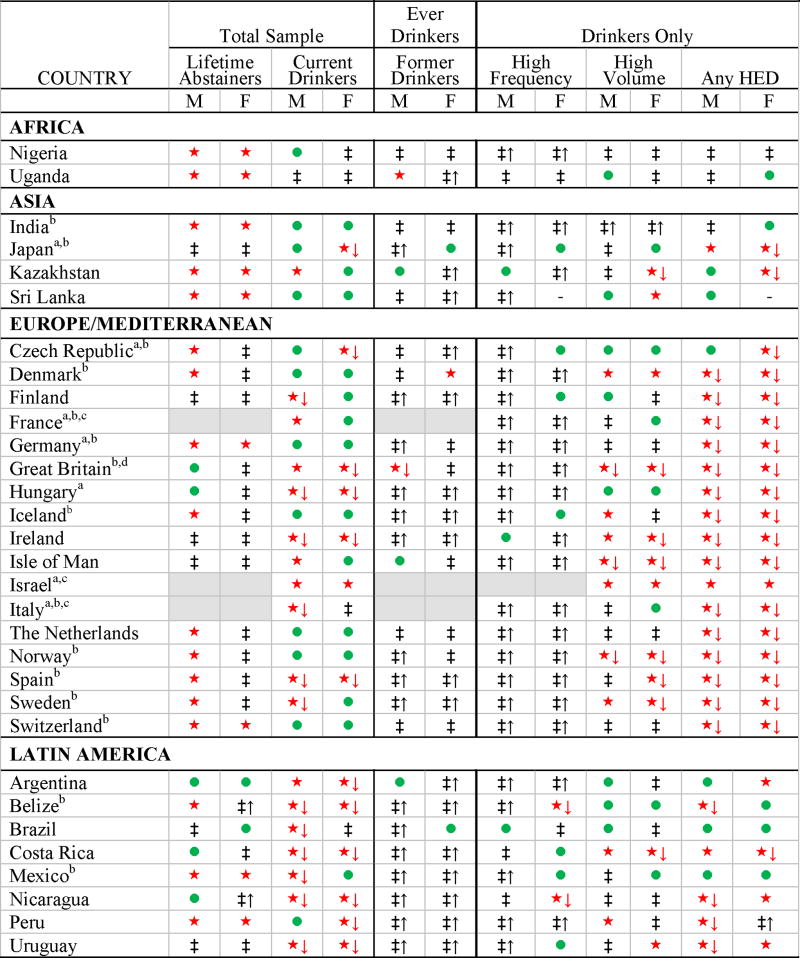
A second unexpected finding was that among drinkers, the prevalence of high-frequency drinking (five or more days a week) tended to increase with age. As shown by the symbols in Table 3, the percentage of male drinkers who reported high-frequency drinking increased monotonically from the youngest to the oldest age group in 28 of the 34 surveys providing such data. The six exceptions were that the prevalence of high-frequency drinking among drinking men was highest at ages 35–49 in Brazil, Ireland, and Kazakhstan, and was lowest at ages 35–49 in Costa Rica, Nicaragua, and Uganda. The pattern for women drinkers was not quite as consistent: the prevalence of high-frequency drinking increased monotonically across the three age groups in 22 of the 34 surveys. However, if the random likelihood that a series of prevalence rates would increase monotonically with age (A<B<C) was 1/6, the probability of this sequence occurring so often by chance was less than 0.001 for both men and women who drank. What the data do not tell us is the extent to which this apparent effect of aging may be a consequence of less frequent drinkers being more likely to quit drinking altogether at older ages. Table 3 shows that among individuals who had ever been drinkers, becoming a former drinker was monotonically more likely in older age groups, in 19 of 32 surveys for men, and in 19 of 32 surveys for women, patterns that were also unlikely to occur by chance (P’s <.001).
Table 3.
Drinking Status and Drinking Patterns: Age Comparisons by World Region, Country, and Gender
 |
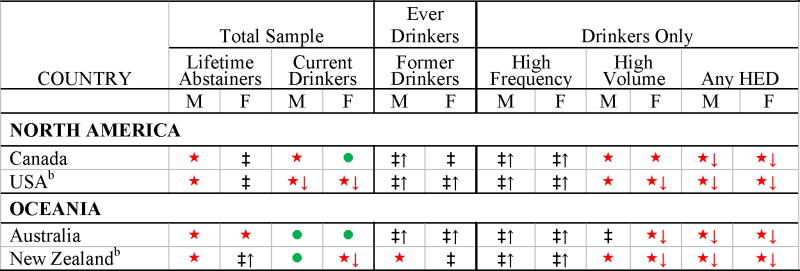 |
Note. High frequency = 5+ times a week. High volume = 8468+ grams of pure ethanol in a year. Heavy episodic drinking (HED) = 60+ grams of pure ethanol in a day (exceptions noted below).
Age group with highest prevalence:

18 – 34;

35 – 49;
50 – 65.

Monotonic increase with age.

Monotonic decrease with age.
Age ranges used in these analyses: 18–64 (Czech Republic, France, Italy, UK); 18–60 (Germany); 19–65 (Hungary); 18–40 (Israel); 20–65 (Japan). All other countries 18–65.
HED = 50+ grams (Belize, India, New Zealand, Spain); 65+ grams (Iceland, Mexico); 70+ grams (Germany, USA); 72+ grams (Japan, Sweden); 75+ grams (Denmark, France, Italy, UK); 80+ grams (Switzerland); 90+ grams (Czech Republic); 74–112 grams (mean=87 grams, Norway).
Survey did not differentiate lifetime abstainers from former drinkers.
HED estimate obtained from UK survey.
Age and drinking
The third surprise was the frequent absence of an expected pattern. Past research in Europe and North America had led us to expect that alcohol use in general, and heavy drinking in particular, would be a pattern of youth that would decline as individuals grew older and developed increased social responsibilities [20, 33–35]. We expected that increasing age would be monotonically associated with a lower prevalence of current drinking, and a lower prevalence among drinkers of high-volume drinking. These patterns did not occur as consistently as we expected. The prevalence of current drinking declined monotonically with advancing age in only a minority of the surveys with three age groups (13 out of 34 for men and 14 out of 34 for women), although this was more often than would have occurred by chance (P <.003). Among current drinkers, the prevalence of high-volume drinking declined monotonically with advancing age among men in only three of the 34 surveys (P >.94), and among women in only 11 of the 34 surveys (P<.008). Furthermore, most age-linked declines in high-volume drinking took place in Europe, the U.S., Australia, or New Zealand (all three surveys of men and 9 of the 11 surveys of women).
Age and heavy episodic drinking
Although high-frequency drinking became more prevalent with advancing age, particularly among men, heavy episodic drinking (HED) generally became less prevalent with advancing age, particularly among women. In 23 of 33 surveys in which women in all three age groups reported HED, the prevalence of HED among women drinkers declined monotonically as age increased (p <.001). The countries with this monotonic decline with increased age were predominantly in Europe plus Australia, New Zealand, Canada, and the U.S. (20 of the 23 surveys). In contrast, HED among women drinkers did not decline consistently with greater age among women drinkers in Argentina, Belize, Brazil, India, Mexico, Nicaragua, Nigeria, Peru, Uganda, and Uruguay. A monotonic decline in the prevalence of heavy episodic drinking with age also occurred commonly among men (23 of 34 surveys, p <.001). However, this consistency was also concentrated in Western Europe, Australia, New Zealand, Canada, and the U.S.; 10 of the 11 surveys that did not fit the pattern were in Africa, Asia, and Latin America (Argentina, Brazil, Costa Rica, India, Japan, Kazakhstan, Mexico, Nigeria, Sri Lanka, and Uganda).
DISCUSSION
What implications can we draw from these relatively simple analyses? First, gender differences in alcohol consumption remain universal, although the sizes of gender differences vary. More drinking and heavy drinking occur among men, more long-term abstention occurs among women, and no cultural differences or historical changes have entirely erased these differences. As there are relatively few universals in human social behavior, these findings suggest that biological differences play some role in how men and women drink. However, because the gender differences vary in magnitude across cultures and across different drinking patterns, it is also very likely that gender differences in drinking behavior are modified by cultural and not just biological factors [6]. For example, giving men but not women the license and tolerance to get drunk in public may be important to men in some cultural settings to symbolize men’s superiority to women in status and authority. Self-restraint of drinking by women in some cultural settings may demonstrate their roles as social guardians and restraining influences on male recklessness [5, 36].
Additional support for the importance of cultural influences on gender differences in drinking behavior is provided by the large between-country differences in patterns of alcohol consumption. As discussed below, some surveys in the GENACIS project were regional rather than national, and for this reason we have de-emphasized the absolute prevalence levels of drinking patterns in this paper. However, the prevalence rates in Tables S2 - S5 (see supporting information details at the end of the paper) reveal large differences across countries. For example, rates of current drinking ranged from 97% of men and 94% of women in Denmark to 37% of men and 3% of women in the Indian state of Karnataka (Table S2); rates of heavy episodic drinking among drinkers ranged from 91% and 62% of male and female drinkers respectively in Ireland to 22% and 11% of male and female drinkers in Israel (Table S5). In a number of countries women’s alcohol consumption (although lower than men’s in the same country) exceeded men’s alcohol consumption in other countries (which was greater than women’s in the same country). Substantial variation also occurred in same-age groups across countries. These large between-country differences suggest a strong influence of social and cultural factors, such as alcohol-related norms, values, and constraints, which may interact with biological gender to influence drinking patterns.
The finding that women are generally more likely than men to quit drinking is consistent with other data on former drinkers and on declines in current drinking over time, in Australia [37], China [38], Finland [39], Japan [40], and the U.S. (e.g., [41]). However, this gender difference is rarely discussed, and typically must be identified through secondary analysis of published data. Current attention to reasons why adolescents start drinking may have drawn attention away from reasons why adults (other than those who are alcohol dependent) stop drinking. It is possible that women find it easier than men to quit drinking because (1) women are generally lighter drinkers than men are; (2) drinking is not as important to women’s social roles as it is to men’s; and/or (3) women who cease drinking during pregnancy and early childrearing may then not resume drinking later on. These hypotheses could be evaluated to some extent with longitudinal data from adult general population samples, preferably allowing cross-cultural comparisons. Such analyses might examine how similar baseline drinking patterns affect men’s versus women’s probabilities of quitting drinking later on (Hypothesis 1); how baseline drinking with coworkers or as part of work roles differs by gender and influences how long into adult life men and women continue to drink (Hypothesis 2); and how initiating abstention from alcohol during pregnancy and early childrearing affects women’s probability of drinking later in life (Hypothesis 3).
Higher prevalence of high-frequency drinking in older age groups of drinkers is reported also in at least a few other surveys [35, 42, 43]. Such increases in the prevalence of high-frequency drinking with age are an important puzzle because of conflicting views in the research literature about daily drinking. Numerous studies have associated daily drinking either with health benefits of light-to-moderate drinking (e.g., [44, 45]) or with health hazards of heavy drinking (e.g., [46, 47]), but these studies often do not take into account the ages and genders of daily drinkers, or variations in the amounts of alcohol consumed daily (for exceptions, see [48, 49]). It is also unclear whether daily drinking and the amounts consumed vary independently, and whether daily light drinking is an unusual pattern that may not occur by itself without cultural reinforcement.
Finally, the evidence here clearly challenges generalizations in the literature that heavy drinking and heavy episodic drinking are habits of reckless youth, habits that decline as people mature and take on more responsibilities (or develop more health problems). The data here are not consistent with any universal decline of heavy drinking with increasing age, a hypothesis that has also been challenged by other studies in individual countries (e.g., [8, 50–52]).
Furthermore, the association of youth with heavy episodic drinking may be primarily an Anglo-European pattern. Other studies that report data about the age distribution of hazardous or heavy episodic drinking tend to confirm our findings: such drinking may be a youthful pattern in Europe and English-speaking countries [53–55], but it is as prevalent or more prevalent in middle or later adulthood in many other parts of the world (see, e.g., [8, 56, 57]). One reason why some people do not age out of heavy episodic drinking may be that in some cultural environments such drinking traditionally is a privilege or obligation associated with higher status or seniority [58, 59]. However, further research is needed to better understand the cultural circumstances in which heavy episodic drinking is not limited to the young.
The data reported here have at least three important limitations. First, the data are cross-sectional, and thus do not allow causal inferences; and possible cohort differences must be taken into consideration when interpreting age associations with drinking patterns. Second, some of the surveys were regional (rather than national) and/or used quota or replacement sampling; therefore, the data from these surveys may not be generalizable to the entire countries where those surveys occurred. Third, questions about drinking patterns were not exactly the same in all countries, particularly among countries (mainly in Europe) where data were collected before the standardized GENACIS questionnaire could be used. Because of these limitations, the data are less valuable for precise prevalence estimates, and most valuable for identifying consistencies and patterns of inconsistency across the diverse GENACIS countries. In that context, the GENACIS data show not only that some gender differences in drinking and in abstention from alcohol are consistent cross-culturally, but also that some often assumed effects of aging on drinking do not occur as consistently as was once thought. We hope that both the consistencies and the inconsistencies in these data will inspire future cross-cultural and longitudinal research.
Supplementary Material
Acknowledgments
Preparation of this paper was supported by Grant Number R01AA015775 from the National Institute on Alcohol Abuse and Alcoholism/National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Alcohol Abuse and Alcoholism or the National Institutes of Health.
The data used in this paper are from the project, Gender, Alcohol and Culture: An International Study (GENACIS). GENACIS is a collaborative international project affiliated with the Kettil Bruun Society for Social and Epidemiological Research on Alcohol and coordinated by GENACIS partners from the University of North Dakota, Aarhus University, the Charité University Medicine Berlin, the Pan American Health Organization, and the Swiss Institute for the Prevention of Alcohol and Drug Problems. Support for aspects of the project has come from the World Health Organization, the Quality of Life and Management of Living Resources Programme of the European Commission (Concerted Action QLG4-CT-2001-0196), the US National Institute on Alcohol Abuse and Alcoholism/National Institutes of Health (Grants R21 AA012941 and R01 AA015775), the German Federal Ministry of Health, the Pan American Health Organization, and Swiss national funds. Support for individual country surveys was provided by government agencies and other national sources. The study leaders and funding sources for data sets used in this paper are: Argentina: Myriam Munné, M.S., World Health Organization; Australia: Paul Dietz, Ph.D., National Health and Medical Research Council (Grant 398500); Belize: Claudina Cayetano, M.D., Pan American Health Organization; Brazil: Florence Kerr-Corréa, M.D., Ph.D., Foundation for the Support of Sao Paulo State Research (Fundação de Amparo a Pesquisa do Estado de São Paulo, FAPESP) (Grant 01/03150-6); Canada: Kathryn Graham, Ph.D., Canadian Institutes of Health Research (CIHR); Costa Rica: Julio Bejarano, M.Sc., World Health Organization; Czech Republic: Ladislav Csémy, Ph.D., Ministry of Health (Grant MZ 23752); Denmark: Kim Bloomfield, Dr.P.H., Sygekassernes Helsefond; Danish Medical Research Council; Finland: Pia Mäkelä, Ph.D., National Research and Development Centre for Welfare and Health (STAKES); Germany: Ludwig Kraus, Ph.D., German Federal Ministry of Health (BMGS) and in cooperation with the Institute for Therapy Research, Munich, Germany; Great Britain: Martin Plant, Ph.D., and Moira Plant, Ph.D., Alcohol Education and Research Council; European Forum for Responsible Drinking; University of the West of England, Bristol; Hungary: Zsuzsanna Elkes, Ph.D., Ministry of Youth and Sport; Iceland: Hildigunnur Ólafsdóttir, Ph.D., Alcohol and Drug Abuse Prevention Council, Public Health Institute of Iceland, Reykjavík, Iceland; India: Vivek Benegal, M.D., World Health Organization; Ireland: Ann Hope, Ph.D., Department of Health and Children (HPU); Isle of Man: Martin Plant, Ph.D., and Moira Plant, Ph.D., Isle of Man Medical Research; University of the West of England, Bristol; Israel: Giora Rahav, Ph.D., and Meir Teichman, Ph.D., Anti Drugs Authority of Israel; Japan: Shinji Shimizu, Ph.D., Japan Society for the Promotion of Science (Grant 13410072); Kazakhstan: Bedel Sarbayev, Ph.D., World Health Organization; Mexico: Maria-Elena Medina-Mora, Ph.D., Ministry of Health, Mexico, Office of Antinarcotics Issues; U. S. Embassy in Mexico; National Institute of Psychiatry; National Council Against Addictions; General Directorate of Epidemiology and Subsecretary of Prevention and Control of Diseases, Ministry of Health, Mexico; The Netherlands: Ronald Knibbe, Ph.D., Ministry of Health and Welfare of the Netherlands; New Zealand: Jennie Connor, Ph.D., Otago University Research Grant; Nicaragua: José Trinidad Caldera Aburto, M.D., Ph.D., Pan American Health Organization; Nigeria: Akanidomo Ibanga, M.Sc., World Health Organization; Norway: Sturla Nordlund, Ph.D., Norwegian Institute for Alcohol and Drug Research; Peru: Marina Piazza, MPH, Sc.D., Pan American Health Organization; Spain: Juan Carlos Valderrama, M.D., Dirección General de Atención a la Dependencia, Conselleria de Sanidad, Generalitat Valenciana; Comisionado do Plan de Galicia sobre Drogas, Conselleria de Sanidade, Xunta de Galicia; Dirección General de Drogodependencias y Servicios Sociales, Gobierno de Cantabria; Sri Lanka: Siri Hettige, Ph.D., World Health Organization; Sweden: Karin Helmersson Bergmark, Ph.D., Ministry for Social Affairs and Health, Sweden; Switzerland: Gerhard Gmel, Ph.D., Swiss Federal Office for Education and Science (Contract 01.0366); Swiss Federal Statistical Office; University of North Dakota (Subcontract No. 254, Amendment No.2, UND Fund 4153-0425); Uganda: M. Nazarius Tumwesigye, Ph.D., World Health Organization; USA: Thomas Greenfield, Ph.D., National Institute on Alcohol Abuse and Alcoholism/National Institutes of Health (Grant P50 AA05595); Uruguay: Raquel Magri, M.D., World Health Organization. European Comparative Alcohol Study (ECAS) surveys in France, Italy, Sweden and the UK, were supported by the European Commission (DG V); National Institute of Public Health (Sweden); Swedish Ministry of Health and Social Affairs; and National Research and Developmental Centre for Welfare and Health, STAKES (Finland).
Footnotes
Declarations of interest
None.
References
- 1.Fillmore KM, Hartka E, Johnstone BM, Leino EV, Motoyoshi M, Temple MT. A meta-analysis of life course variation in drinking. Br J Addict. 1991;8:1221–1268. doi: 10.1111/j.1360-0443.1991.tb01702.x. [DOI] [PubMed] [Google Scholar]
- 2.Popova S, Rehm J, Patra J, Zatonski W. Comparing alcohol consumption in central and eastern Europe to other European countries. Alcohol Alcohol. 2007;42:465–473. doi: 10.1093/alcalc/agl124. [DOI] [PubMed] [Google Scholar]
- 3.Van Gundy K, Schieman S, Kelley MS, Rebellon CJ. Gender role orientations and alcohol use among Moscow and Toronto adults. Soc Sci Med. 2005;61:2317–2330. doi: 10.1016/j.socscimed.2005.07.033. [DOI] [PubMed] [Google Scholar]
- 4.Allamani A, Voller F, Kubiçka L, Bloomfield K. Drinking cultures and the position of women in nine European countries. Subst Abuse. 2000;21:231–247. doi: 10.1080/08897070009511436. [DOI] [PubMed] [Google Scholar]
- 5.Holmila M, Raitasalo K. Gender differences in drinking: Why do they still exist? Addiction. 2005;100:1763–1769. doi: 10.1111/j.1360-0443.2005.01249.x. [DOI] [PubMed] [Google Scholar]
- 6.Wilsnack RW, Vogeltanz ND, Wilsnack SC, Harris TR, et al. Gender differences in alcohol consumption and adverse drinking consequences: Cross-cultural patterns. Addiction. 2000;95:251–265. doi: 10.1046/j.1360-0443.2000.95225112.x. [DOI] [PubMed] [Google Scholar]
- 7.Almeido-Filho N, Lessa I, Magalhaes L, Araujo MJ, Aquino EA, Kawachi I, James SA. Alcohol drinking patterns by gender, ethnicity, and social class in Bahia, Brazil. Revista de Saude Publica. 2004;38:45–54. doi: 10.1590/s0034-89102004000100007. [DOI] [PubMed] [Google Scholar]
- 8.Parry CDH, Plüddemann A, Steyn K, Bradshaw D, Norman R, Laubscher R. Alcohol use in South Africa: Findings from the first Demographic and Health Survey (1998) J Stud Alcohol. 2005;66:91–97. doi: 10.15288/jsa.2005.66.91. [DOI] [PubMed] [Google Scholar]
- 9.Balabanova D, McKee M. Patterns of alcohol consumption in Bulgaria. Alcohol Alcohol. 1999;34:622–628. doi: 10.1093/alcalc/34.4.622. [DOI] [PubMed] [Google Scholar]
- 10.Hao W, Su Z, Liu B, Zhang K, Yang H, Chen S, et al. Drinking and drinking patterns and health status in the general population of five areas of China. Alcohol Alcohol. 2004;39:43–52. doi: 10.1093/alcalc/agh018. [DOI] [PubMed] [Google Scholar]
- 11.Higuchi S, Parrish KM, Dufour MC, Towle LH, Harford TC. Relationship between age and drinking patterns and drinking problems among Japanese, Japanese-Americans, and Caucasians. Alcohol Clin Exp Res. 1994;18:305–310. doi: 10.1111/j.1530-0277.1994.tb00018.x. [DOI] [PubMed] [Google Scholar]
- 12.Bobak M, Room R, Pikhart H, Kubinova R, Malyutina S, Pajak A, Kurilovitch S, Topor R, Nikitin Y, Marmot M. Contribution of drinking patterns to differences in rates of alcohol related problems between three urban populations. J Epidemiol Community Health. 2004;58:238–242. doi: 10.1136/jech.2003.011825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nolen-Hoeksema S. Gender differences in risk factors and consequences for alcohol use and problems. Clin Psychol Rev. 2004;24:981–1010. doi: 10.1016/j.cpr.2004.08.003. [DOI] [PubMed] [Google Scholar]
- 14.Slone LB, Norris FH, Gutierrez Rodriguez F, Gutierrez Rodriguez José de Jesus, Murphy AM, Perilla JL. Alcohol use and misuse in urban Mexican men and women: An epidemiological perspective. Drug Alcohol Depend. 2006;85:163–170. doi: 10.1016/j.drugalcdep.2006.04.006. [DOI] [PubMed] [Google Scholar]
- 15.Keyes KM, Grant BF, Hasin DS. Evidence for a closing gender gap in alcohol use, abuse, and dependence in the United States population. Drug Alcohol Depend. 2008;93:21–29. doi: 10.1016/j.drugalcdep.2007.08.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lim WY, Fong CW, Chan JML, Heng D, Bhalla V, Chew SK. Trends in alcohol consumption in Singapore 1992–2004. Alcohol Alcohol. 2007;42:354–361. doi: 10.1093/alcalc/agm017. [DOI] [PubMed] [Google Scholar]
- 17.Mäkelä P, Bloomfield K, Gustafsson NK, Huhtanen P, Room R. Changes in volume of drinking after changes in alcohol taxes and travellers’ allowances: Results from a panel study. Addiction. 2008;102:181–191. doi: 10.1111/j.1360-0443.2007.02049.x. [DOI] [PubMed] [Google Scholar]
- 18.McPherson M, Casswell S, Pledger M. Gender convergence in alcohol consumption and related problems: Issues and outcomes from comparisons of New Zealand survey data. Addiction. 2004;99:738–748. doi: 10.1111/j.1360-0443.2004.00758.x. [DOI] [PubMed] [Google Scholar]
- 19.Bloomfield K, Gmel G, Neve R, Mustonen H. Investigating gender convergence in alcohol consumption in Finland, Germany, the Netherlands, and Switzerland: A repeated survey analysis. Subst Abuse. 2001;22:39–54. doi: 10.1080/08897070109511444. [DOI] [PubMed] [Google Scholar]
- 20.Grant BF, Dawson DA, Stinson FS, Chou SP, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991–1992 and 2001–2002. Drug Alcohol Depend. 2004;74:223–234. doi: 10.1016/j.drugalcdep.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 21.Hahm BJ, Cho MJ. Prevalence of alcohol use disorder in a South Korean community: Changes in the pattern of prevalence over the past 15 years. Soc Psychiatry Psychiatr Epidemiol. 2005;40:114–119. doi: 10.1007/s00127-005-0854-9. [DOI] [PubMed] [Google Scholar]
- 22.Knibbe R, Bloomfield K. Alcohol consumption estimates in surveys in Europe: Comparability and sensitivity for gender differences. Subst Abuse. 2001;22:23–38. doi: 10.1080/08897070109511443. [DOI] [PubMed] [Google Scholar]
- 23.Mäkelä P, Gmel G, Grittner U, Kuendig H, Kuntsche S, Bloomfield K, Room R. Drinking patterns and their gender differences in Europe. Alcohol Alcohol. 2006;41(Supplement 1):8–18. doi: 10.1093/alcalc/agl071. [DOI] [PubMed] [Google Scholar]
- 24.Bloomfield K, Allamani A, Beck F, Bergmark KH, Csemy L, Eisenbach-Stangl I, Elekes Z, Gmel G, Kerr-Corea F, Knibbe R, Mäkelä P, Monteiro M, Medina Mora ME, Nordlund S, Obot I, Plant M, Rahav G, Romero Mendoza M. Project Final Report. Berlin: Institute for Medical Informatics, Biometrics and Epidemiology, Charité Universtitätsmedizin; 2005. Gender, Culture, and Alcohol Problems: A Multi-National Study. http://www.genacis.org/history.php. [Google Scholar]
- 25.Obot IS, Room R, editors. Alcohol, Gender and Drinking Problems: Perspectives from Low and Middle Income Countries. Geneva: World Health Organization; 2005. [Google Scholar]
- 26.Wilsnack SC, Wilsnack RW. International gender and alcohol research: recent findings and future directions. Alcohol Res Health. 2002;26:245–250. [PMC free article] [PubMed] [Google Scholar]
- 27.Rehm J, Rehn N, Room R, Monteiro M, Gmel G, Jernigan D, Frick U. The global distribution of average volume of alcohol consumption and patterns of drinking. Eur Addict Res. 2003;9:147–156. doi: 10.1159/000072221. [DOI] [PubMed] [Google Scholar]
- 28.Smart RG, Ogburne A. Drinking and heavy drinking by students in 18 countries. Drug Alcohol Depend. 2000;60:315–318. doi: 10.1016/s0376-8716(00)00117-4. [DOI] [PubMed] [Google Scholar]
- 29.Graham K, Bernards S, Munné M, Wilsnack SC. Unhappy Hours: Alcohol and Partner Aggression in the Americas. Washington, DC: Pan American Health Organization; 2008. [Google Scholar]
- 30.Trotter R. Guide to Drug Abuse Epidemiolgy. Geneva: World Health Organization; 1997. Translation guidelines Model questionnaire on drug abuse epidemiology. WHO/PSA/91.14. [Google Scholar]
- 31.World Health Organization. WHO Multi-Country Study of Women’s Health and Domestic Violence: Core Protocol. Geneva: World Health Organization; 1999. WHO/EIP/GPE/99.3. [Google Scholar]
- 32.National Institute on Alcohol Abuse and Alcoholism. NIAAA Council approves definition of binge drinking. NIAAA Newsletter. 2004;3:3. http://pubs.niaaa.nih.gov/publications/Newsletter/winter2004/Newsletter_Number3.pdf.
- 33.Hajema KJ, Knibbe RA, Drop MJ. Changes in alcohol consumption in a general population in The Netherlands: A 9-year follow-up study. Addiction. 1997;92:49–60. [PubMed] [Google Scholar]
- 34.Kemm J. An analysis by birth cohort of alcohol consumption by adults in Great Britain, 1978–1998. Alcohol Alcohol. 2003;38:142–147. doi: 10.1093/alcalc/agg039. [DOI] [PubMed] [Google Scholar]
- 35.Ramstedt M, Hope A. The Irish drinking habits of 2002: Drinking and drinking related harm in a European comparative perspective. J Subst Use. 2005;10:273–283. [Google Scholar]
- 36.Wilsnack RW, Wilsnack SC, Obot IS. Why study gender, alcohol, and culture? In: Obot IS, Room R, editors. Alcohol, Gender and Drinking Problems: Perspectives from Low and Middle Income Countries. Geneva: World Health Organization; 2005. pp. 1–23. [Google Scholar]
- 37.Harriss LR, English DR, Hopper JL, Powles J, Simpson JA, O’Dea K, Giles GG, Tonkin AM. Alcohol consumption and cardiovascular mortality accounting for possible misclassification of intake: 11-year follow-up of the Melbourne Collaborative Cohort Study. Addiction. 2007;102:1574–1585. doi: 10.1111/j.1360-0443.2007.01947.x. [DOI] [PubMed] [Google Scholar]
- 38.Ji BT, Dai Q, Gao YT, Hsing AW, McLaughlin JK, Fraumeni JF, Chow WH. Cigarette and alcohol consumption and the risk of colorectal cancer in Shanghai, China. Eur J Cancer Prev. 2002;11:237–244. doi: 10.1097/00008469-200206000-00007. [DOI] [PubMed] [Google Scholar]
- 39.Vahtera J, Poikolainen K, Kivimaki M, Ala-Mursula L, Pentti J. Alcohol intake and sickness absence: A curvilinear relation. Am J Epidemol. 2002;156:969–976. doi: 10.1093/aje/kwf138. [DOI] [PubMed] [Google Scholar]
- 40.Kawado M, Suzuki S, Hashimoto S, Tokudome S, Yoshimura T, Tamakoshi A. Smoking and drinking habits five years after baseline in the JACC study. J Epidemol. 2005;15 (Supplement 1):S56–S66. doi: 10.2188/jea.15.S56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Fillmore KM, Kerr WC, Bostrom A. Changes in drinking status, serious illness and mortality. J Stud Alcohol. 2003;64:278–285. doi: 10.15288/jsa.2003.64.278. [DOI] [PubMed] [Google Scholar]
- 42.Bloomfield K. West German drinking patterns in 1984 and 1990. Eur Addict Res. 1998;4:163–171. doi: 10.1159/000018949. [DOI] [PubMed] [Google Scholar]
- 43.Gual A. Alcohol in Spain: Is it different? Addiction. 2006;101:1073–1077. doi: 10.1111/j.1360-0443.2006.01518.x. [DOI] [PubMed] [Google Scholar]
- 44.Luchsinger JA, Tang MX, Siddiqui M, Shea S, Mayeux R. Alcohol intake and risk of dementia. J Am Geriatr Soc. 2004;52:540–546. doi: 10.1111/j.1532-5415.2004.52159.x. [DOI] [PubMed] [Google Scholar]
- 45.Mukamal KJ, Conigrave KM, Mittleman MA, Camargo CAJ, Stampfer MJ, Willett WC, Rimm EB. Roles of drinking patterns and type of alcohol consumed in coronary heart disease in men. N Engl J Med. 2003;348:109–118. doi: 10.1056/NEJMoa022095. [DOI] [PubMed] [Google Scholar]
- 46.Sharpe CR, Siemiatycki J. Case-control study of alcohol consumption and prostate cancer in Montreal, Canada. Cancer Causes Control. 2001;12:589–598. doi: 10.1023/a:1011289108040. [DOI] [PubMed] [Google Scholar]
- 47.Swade TF, Emanuele NV. Alcohol and diabetes. Compr Ther. 1997;23:135–140. [PubMed] [Google Scholar]
- 48.Dorn JM, Hovey K, Muti P, Freudenheim JL, Russell M, Nochajski TH, Trevisan M. Alcohol drinking patterns differentially affect central adiposity as measured by abdominal height in women and men. J Nutr. 2003;133:2655–2662. doi: 10.1093/jn/133.8.2655. [DOI] [PubMed] [Google Scholar]
- 49.Stranges S, Wu TJ, Dorn JM, Freudenheim JL, Muti P, Farinaro E, Russell M, Nochajski TH, Trevisan M. Relationship of alcohol drinking pattern to risk of hypertension: A population-based study. Hypertension. 2004;44:813–819. doi: 10.1161/01.HYP.0000146537.03103.f2. [DOI] [PubMed] [Google Scholar]
- 50.Akvardar Y, Turkcan A, Yazman U, Aytaclar S, Ergor G, Cakmak D. Prevalence of alcohol use in Istanbul. Psychol Rep. 2003;93:1081–1088. doi: 10.2466/pr0.2003.92.3c.1081. [DOI] [PubMed] [Google Scholar]
- 51.Kerr-Corrêa F, Tucci AM, Hegedus AM, Trinca LA, de Oliveira JB, Floripes TMF, Kerr-Pontes LRS. Drinking patterns between men and women in two distinct Brazilian communities. Rev Bras Psiquiatr. 2008;30:235–242. doi: 10.1590/s1516-44462008000300010. [DOI] [PubMed] [Google Scholar]
- 52.Park JT, Kim BG, Jhun H-J. Alcohol consumption and the CAGE questionnaire in Korean adults: Reports from the Second Korea National Health and Nutrition Examination Survey. J Korean Med Sci. 2008;23:199–206. doi: 10.3346/jkms.2008.23.2.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kuntsche E, Rehm J, Gmel G. Characteristics of binge drinkers in Europe. Soc Sci Med. 2004;59:113–127. doi: 10.1016/j.socscimed.2003.10.009. [DOI] [PubMed] [Google Scholar]
- 54.Miller JW, Gfroerer JC, Brewer RD, Naimi TS, Mokdad A, Giles H. Prevalence of adult binge drinking: A comparison of two national surveys. Am J Prev Med. 2004;27:197–204. doi: 10.1016/j.amepre.2004.05.004. [DOI] [PubMed] [Google Scholar]
- 55.Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge drinking among U. S. adults. JAMA. 2003;289:70–75. doi: 10.1001/jama.289.1.70. [DOI] [PubMed] [Google Scholar]
- 56.Aekplakorna W, Hogan MC, Tiptaradol S, Wibulpolprasert S, Punyaratbanhu P, Lim SS. Tobacco and hazardous or harmful alcohol use in Thailand: Joint prevalence and associations with socioeconomic factors. Addict Behav. 2008;33:503–514. doi: 10.1016/j.addbeh.2007.10.010. [DOI] [PubMed] [Google Scholar]
- 57.Almeido-Filho N, Lessa I, Magalhaes L, Araujo MJ, Aquino EA, James SA, Kawachi I. Social inequality and alcohol consumption-abuse in Bahia, Brazil. Soc Psychiatry Psychiatr Epidemiol. 2005;40:214–222. doi: 10.1007/s00127-005-0883-4. [DOI] [PubMed] [Google Scholar]
- 58.Nghe LT, Mahalik JR, Lowe SM. Influences on Vietnamese men: Examining traditional gender roles, the refugee experience, acculturation, and racism in the United States. J Multicult Couns Devel. 2003;31:245–261. [Google Scholar]
- 59.Willis J. ‘Beer used to belong to older men’: Drinking and authority among the Nyakyusa of Tanzania. Africa. 2001;71:377–390. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.