

Abstract
Multiple theories suggest mechanisms by which the use of alcohol and drugs during adolescence could dampen growth in psychosocial maturity. However, scant empirical evidence exists to support this proposition. The current study tested whether alcohol and marijuana use predicted suppressed growth in psychosocial maturity among a sample of male serious juvenile offenders (n = 1,170) who were followed from ages 15 to 21. Alcohol and marijuana use prospectively predicted lower maturity six months later. Moreover, boys with the greatest increases in marijuana use showed the smallest increases in psychosocial maturity. Finally, heterogeneity in the form of age-related alcohol and marijuana trajectories was related to growth in maturity, such that only boys who decreased their alcohol and marijuana use significantly increased in psychosocial maturity. Taken together, these findings suggest that patterns of elevated alcohol and marijuana use in adolescence may suppress age-typical growth in psychosocial maturity from adolescence to young adulthood, but that effects are not necessarily permanent, because decreasing use is associated with increases in maturity.
Keywords: Adolescent Substance Use, Maturity Trajectories
Adolescent substance use is highly prevalent, particularly among males, with recent data reporting that over 35% of male high school seniors have used marijuana in the last year and over 30% have been drunk in the last month (Johnston, O’Malley, Bachman, & Schulenberg, 2008). At the same time, adolescence is a period of rapid developmental change, when biological, cognitive, and psychosocial capacities are altered in the transition to adulthood (Brown et al., 2008; Moss, 2008; Spear, 2000). Given this period of rapid change, concern has been raised that high levels of exposure to alcohol and drugs during adolescence may produce negative effects on adolescent neurobiological development and on the development of psychosocial maturity (Brown et al., 2008; Spear, 2000; Squeglia et al., 2009), as well as ripple effects on multiple life-course domains (Odgers et al., 2008).
According to Steinberg and Cauffman (1996) psychosocial maturity is a broad aggregate of multiple dispositions, which follow a developmental progression between adolescence and adulthood and likely affect adult outcomes. Over the course of adolescence, psychosocial maturity increases so that by adulthood, individuals are able to function independently, to interact appropriately with others, and to contribute to social cohesion (Greenberger & Sorensen, 1974). Psychosocially mature individuals take responsibility for their actions, autonomously rely on personal resources, and have a clear sense of identity. They exhibit temperance in curbing impulsive and aggressive behavior and are able to adopt multiple temporal and social perspectives (Steinberg & Cauffman, 1996).
Studies have demonstrated developmental changes in indicators of psychosocial maturity over the course of adolescence (e.g. Cauffman & Steinberg, 2000; Grisso et al, 2003; Modecki, 2008). Of most relevance for the current study, research suggests that developmental increases in indicators of psychosocial maturity continue to occur even in late adolescence and into early adulthood (Cauffman & Steinberg, 2000; Modecki, 2008; Steinberg & Cauffman; 1996; Steinberg, Cauffman, Woolard, Graham & Banich, in press). Thus, substance use that begins in adolescence has the potential to influence the future development of psychosocial maturity. Moreover, psychosocial maturity shows significant age-related increases, even within samples of male juvenile delinquents (Monahan, Steinberg, Cauffman, & Mulvey, in press), albeit their levels of maturity may be lower than their non-offending peers (Modecki, 2008).
Why would adolescent substance use hamper the development of psychosocial maturity? There are several possible mechanisms. For example, Baumrind and Moselle (1985) argued that growth in psychosocial maturity is promoted through adolescents’ engagement and coping with normative developmental challenges, including those encountered in school, family, and peer environments. They theorized that substance use might suppress growth in psychosocial maturity by short-circuiting these processes of engagement and coping. That is, rather than confronting challenges, adolescent substance use can promote avoidance of environmental demands. By directly influencing mood, drug and alcohol use enables adolescents to remain egocentrically focused and obviate the need for dealing with challenges. This short-circuiting of the need to cope suppresses the development of more mature coping strategies. In short, adolescent substance use may undermine the processes of engagement with typical developmental challenges, thereby suppressing the growth of psychosocial maturity (Brown et al., 2008).
A complementary perspective suggests that adolescent substance use may impair psychosocial maturity by affecting the development of brain structures that regulate behavioral, emotional, and cognitive processes (Clark, Thatcher, & Tapert, 2008; Moss, 2008). During adolescence, prefrontal and limbic areas, and their dopamine inputs are significantly altered (Sowell & Jernigan, 1998), and these areas are linked to decision-making and reward sensitivity (Spear, 2000). Consistent with these findings, recent studies document that, over the course of adolescence and early adulthood, both males and females show normative growth in planning (Albert et al., 2009), preference for delayed rather than immediate rewards (Steinberg et al., 2009), attentiveness to the salience of costs (as opposed to rewards; Cauffman et al., in press), resistance to peer influence (Steinberg & Monahan, 2007), and impulse control (Steinberg et al., 2008). However, many of the brain regions that undergo developmental change during adolescence are also affected by alcohol and drug use (Volkow & Li, 2005). For example, fMRI studies suggest that the prefrontal cortex and sub-cortical striatal areas are both actively engaged in decision-making and affected by addictive substances (Chambers, Taylor, & Potenza, 2003) and substance use may also affect brain circuits involved in the experience of reward and self-regulation (e.g. Brown & Tapert, 2004). A recent review suggests that adolescent substance use leads to poorer neurocognitive performance, poorer white matter quality, and changes in brain volume (Squeglia, Jacobus, & Tapert, 2009). Gender may moderate this relation, as evidence suggests that neurodevelopment among males may be less sensitive to the neurotoxic effects of alcohol use relative to females (Medina et al., 2008).
If adolescent substance use affects neurobiological substrates underlying processes of decision-making, reward sensitivity, and self-regulation, these brain changes would be predicted to slow the development of psychosocial maturity. This mechanism may be particularly relevant for serious juvenile offenders, who are at elevated risk for exposure to early environmental adversity (e.g., chronic stress, poverty, maltreatment, Loeber et al., 2009). Given the negative effects of such early adversity on later brain development (McEwen, 2008; Teicher et al., 2006), juvenile offenders may be particularly vulnerable to any further neurobiological insult such as the effects of alcohol and marijuana use.
Whatever the underlying mechanisms, previous studies of adolescent samples (usually including both males and females) have yielded considerable evidence that substance use is related to multiple dimensions of psychosocial maturity. Consistent cross-sectional evidence shows that substance use is associated with heightened impulsivity (Colder & Chassin, 1997), impaired affect regulation (Cooper, Agocha, & Sheldon, 2000), poor judgment (Giancola, Martin, & Tarter, 1996), and less successful decision-making (White, 1990). In addition, individuals with substance dependence tend to choose small immediate rewards over larger postponed incentives (Potenza, 2007), display a reduced sensitivity to natural reinforcers, and show decreased inhibitory control (Volkow, Fowler, & Wang, 2003). Finally, adolescent alcohol and marijuana users require increased effort during behavioral inhibition tasks (Tapert et al., 2007). However, these cross-sectional findings cannot determine whether these deficits in maturity are antecedents or consequences of adolescent substance use (Clark et al., 2008), and longitudinal studies have most often tested dimensions of psychosocial maturity as predictors rather than consequences of adolescent substance use. For example, low conventionality (Brook, Brook, Arencibia-Mireles, Richter, & Whiteman, 2001), sensation seeking (Horvath, Milich, Lynam, Leukefeld, & Clayton, 2004), impulsivity (Colder & Stice, 1998), disinhibition (Pedersen, 1991), and nonadaptive coping (Wills, Vaccaro, McNamara, & Hirky, 1996) prospectively predict adolescent substance use.
Even though there are few longitudinal studies to directly examine psychosocial maturity, some studies have connected adolescent substance use to maturity-related adult outcomes. For example, adolescent substance use has been associated with adult adjustment problems (Fergusson, Horwood, & Swain-Campbell, 2002), relationship problems (Newcomb & Bentler, 1988), decreased educational attainment (King, Meehan, Trim, & Chassin, 2006), increased internalizing symptoms (Trim, Meehan, King, & Chassin, 2007) and antisocial behavior (White, Bates, & Labouvie, 1998). In addition, Chassin, Pitts, and DeLucia (1999) found that adolescent drug use had a negative effect on later autonomy, and Goudriaan, Grekin and Sher (2007) found that heavy alcohol use in late adolescence was associated with poor behavioral decision-making performance two years later. Finally, Tapert et al. (2002) compared adolescents with and without alcohol or drug problems in their neuropsychological performance over 8 years and found that heavy drinking predicted a divergence from age-expected performance.
All told, then, there is both cross-sectional evidence and some prospective support for the effects of adolescent substance use on psychosocial maturity. Importantly, however, studies have not examined the relation between adolescent substance use and developmental changes in maturity during adolescence. Moreover, attempts to study the relation of adolescent substance use to psychosocial maturity also require attention to methodological issues, most notably to confounding variables. That is, adolescent substance use is associated with a broad array of risk factors that themselves may influence the development of psychosocial maturity (Brown et al., 2008), and research must consider these co-occurring risk factors in order to determine whether adolescent substance use is a true risk factor for suppressed growth in psychosocial maturity or merely a marker for co-occurring risk factors (King et al., 2006; Trim et al., 2007).
To address these questions, the current study tested the relation between adolescent alcohol and marijuana use and the development of psychosocial maturity in a sample of male serious offenders who were followed from age 15 to 21. As noted earlier, at these ages, the developmental expectation is to see growth in psychosocial maturity (Cauffman & Steinberg, 2000). The current study tested whether there was significant age-related growth in maturity overall in the sample, and whether growth in maturity was suppressed as a function of alcohol and marijuana use. Moreover, based on previous literature showing that there may be meaningful heterogeneity in the form of age-related trajectories of alcohol and marijuana use during adolescence and early adulthood (e.g., Ellickson et al., 2004; Li et al, 2001; Schulenberg et al., 1996, 2005; Windle & Weisner, 2004) our analyses considered both overall growth in substance use as well as heterogeneous patterns of growth. Adopting this two-pronged approach can reveal both relations between alcohol and marijuana use and psychosocial maturity that exist overall and also different relations for differing alcohol or marijuana trajectory patterns.
Our use of a serious juvenile offender sample has several advantages. First, these adolescents show higher levels of substance use than does the general adolescent population. If high levels of substance use are necessary to produce an impact on psychosocial maturity, then this impact should be easier to detect among a sample of heavier substance users than in the general adolescent population. Second, because participants were all serious juvenile offenders (i.e., adjudicated of a felony offense), there is likely to be more homogeneity in terms of “third variable” risk factors associated with substance use in this sample than in the general adolescent population. Nevertheless, given the potential importance of antisociality as a “third variable” in the relation between substance use and maturity trajectories (because of the strong correlation between antisociality and adolescent substance use, e.g., Wanner et al., 2009), we tested the relation of substance use to psychosocial maturity above and beyond boys’ initial levels of antisociality and their antisocial history. Moreover, the choice of an offender sample requires consideration of additional covariates. First, because substance use among juvenile offenders varies as a function of their placement in supervised correctional settings (Mauricio et al., 2009), we also considered the effects of supervised residential placements in our models. Second, because of the ethnic diversity of the sample, and because adolescent substance use varies with ethnicity (Barrera et al., 1999), we considered the effects of ethnicity both on substance use and on psychosocial maturity. 1 Finally, by including only male participants, we avoid the potentially confounding effects of gender on neurodevelopmental trajectories (Medina et al., 2008).
Method
Participants
The current sample consisted of 1,170 male adolescents enrolled in Pathways to Desistance, a prospective study of serious juvenile offenders2 (Mulvey et al., 2004). Participants were ages 14 – 17 at the time of the offense that brought them into the study (Mage = 16.55), and were African-American (42.1%), Latino (34.0%), non-Hispanic Caucasian (19.2%), and from other ethnic/racial backgrounds (4.6%).
Participants were recruited in Phoenix and Philadelphia after a review of court files indicated that they had been adjudicated of a serious offense (almost entirely felonies). Given that drug violations represent such a large proportion of the offenses committed by this age group, the proportion of males recruited with a drug offense was restricted to 15% so that the heterogeneity of the sample would not be compromised. The cap did not apply to those adolescents who were processed in the adult criminal system.
Participating juvenile courts provided names of eligible individuals and cases were assigned to interviewers who contacted juveniles and their families. Upon obtaining juvenile and parent/guardian informed consent, participants were interviewed on average, 36.9 days (standard deviation = 20.6) after their adjudication (for those in the juvenile system) or their decertification hearing in Philadelphia or an adult arraignment in Phoenix (if in the adult system), and then interviewed every six months for 3 years. All recruitment and assessment procedures were approved by the IRBs of the participating universities, and adolescents were paid between $50 and $150 over the interviews (when allowed by facility rules).
The participation rate (number of enrolled participants divided by the number invited to participate) was 67%. To assess participation bias, we compared enrolled and non-enrolled eligible participants. Enrolled participants were somewhat younger at adjudication (15.9 vs. 16.1 for non-participants) had more prior court petitions (2.1 vs. 1.5 for non-participants), were younger at first petition (13.9 years vs. 14.2 for non-participants) and were somewhat more likely to be non-Hispanic Caucasian (25% vs. 20% for non-participants). Although statistically significant, these differences are modest in magnitude. Throughout the course of the study, retention rates have been high; youth have completed 90–93% of expected interviews over the six follow-up periods, with 3% of participants having died. Details regarding recruitment and full sample characteristics are discussed in Schubert et al. (2004).
Procedures
Data were collected with computer-assisted interviews at the participants’ homes, in libraries or other public places, or in facilities. The interview measures and skip patterns were programmed onto a laptop computer. Trained interviewers read items aloud and, to maximize privacy, respondents could choose to enter their responses on a key pad. Honest reporting was encouraged, and confidentiality was reinforced by informing participants of the requirement for confidentiality placed upon us by the U.S. Department of Justice that prohibits our disclosure of any personally identifiable information to anyone outside the research staff, except in cases of suspected child abuse or imminent danger. Baseline interviews were administered over 2 days in two 2-hr sessions. Each follow-up interview took about 2 hours to complete.
Measures
Proportion of Supervised Time (PST)
Because placement in an institutional setting affects opportunities for substance use, we controlled for this factor in our analyses (see Piquero et al., 2001). At each wave, the proportion of time spent in a supervised setting (e.g., prison, detention, residential or secure treatment) was equal to the number of days spent in a supervised setting divided by total number of days from one interview to the next. For the current analyses, the days spent in a supervised environment was transformed into a proportion of the number of days elapsed from one interview to the next interview, resulting in proportion scores ranging from 0 to 1. For example, an adolescent who was in a secure placement at wave one for three months would receive a PST score of .50 at wave two (since assessments are conducted every six months). The average PST scores for each wave ranged from .31 to .50. Considered cumulatively, across 36 months of this study, the average time spent in a supervised setting was .39 (SD = .31), or 14.04 months, with 16.8% of adolescents never in a supervised setting. Because of the lack of PST scores at baseline (i.e., there was no PST information for the six months prior to the baseline interview), baseline observations were omitted from analyses.
Antisocial History
To control for antisociality, we used a composite factor score measure from prior research with this sample (Mulvey, Schubert, & Chung, 2007). The items (from the baseline assessment; factor loadings in parentheses) were: age at first arrest from court records (.26), number of prior court petitions in past year from court records (.33), self-reported aggressive offending (.29), and self-reported income-related offending (.34, both from the Self Report of Offending scale; Huizinga, Esbensen, & Weiher, 1991). The composite measure was derived from a confirmatory factor analysis (CFA) of the Pathways sample and results showed good model fit: chi-square, df=1, = 2.96; CFI=1.00; RMSEA=.04.
Psychosocial Maturity
Following Cauffman and Steinberg’s (2000) measurement of psychosocial maturity, we used a composite of items based on three factors, responsibility, temperance, and perspective-taking. Responsibility items were from the Psychosocial Maturity Inventory (Greenberger et al., 1974), and the Resistance to Peer Pressure Inventory (Steinberg & Monahan, 2007). Sample items include “I hate to admit it, but I give up on my work when things go wrong,” [reverse coded] and “In a group I prefer to let other people make the decisions” [reverse coded]. Temperance, or the ability to control one’s impulses, was assessed with items from the Weinberger Adjustment Inventory (WAI; Weinberger & Schwartz, 1990). Sample items include “I say the first thing that comes into my mind without thinking enough about it”, “People who get me angry better watch out” (reverse coded). Perspective taking was measured with items tapping both time perspective and social perspective taking. Items were taken from the Future Outlook Inventory (FOI; Cauffman & Woolard, 1999, e.g., “I think about how things might be in the future.”) and the Weinberger Adjustment Inventory (WAI, Weinberger & Schwartz, 1990, e.g. “I often go out of my way to do things for other people”).
Confirmatory factor analysis with baseline data evaluated the structure of the psychosocial maturity construct. We tested a model in which the three first-order factors (i.e., temperance, responsibility, and perspective-taking) were subsumed under a higher order global psychosocial maturity factor. This model provided an excellent fit to the data: χ2(5) = 13.49, p =.02; CFI = .991, RMSEA = .038. Based on this model, we standardized the component measures and combined them into a single score.
Substance Use
We focused on alcohol and marijuana use because these are the most prevalent forms of adolescent substance use (Chen & Kandel, 1995). At each wave, boys self-reported their frequency of alcohol and marijuana use over the past six months. Because of the non-normal distribution, responses were collapsed from eight categories into five: 0 (Not at all), 1 (1–5 times), 2 (1–3 times per month), 3 (1–3 times per week) and 4 (4 or more times per week). As expected with an offender sample, there was substantial substance use involvement. At baseline, 53% used alcohol; 56% used marijuana, and approximately one–third met DSM-IV diagnostic criteria for an alcohol or drug disorder using the CIDI (WHO, 1997). As noted earlier, we omitted baseline data because of the lack of a PST score and analyzed substance use data from wave 1 through wave 6.
Results
To begin, latent growth curve analysis was used to identify average developmental trajectories of psychosocial maturity, alcohol use, and marijuana use over age. In all analyses, observations were structured by the participant’s age (as opposed to assessment times, N=1,153 due to missing data). Quadratic growth models were tested, but dropped if the quadratic term was not significant and its removal did not produce a significant increase in chi-square. Models were specified such that time scores increased by 0.1 for each 6-month period; thus, the linear slope can be interpreted as the amount of change estimated over the age period. All substance use models controlled for the time-varying proportion of time spent in a supervised setting. Thus, growth curve parameters for the substance use models represent the estimated trajectories of substance use for adolescents when they were not under direct supervision.
In order to test ethnic differences in developmental trajectories, multiple group analyses were implemented. Models with and without equality constraints for the growth terms across ethnic groups were compared with chi-square difference tests. Whenever significant differences were found, follow-up analyses tested pair-wise differences among the ethnic groups and subsequent analyses for that outcome included ethnicity as a control variable.
For all models, fit was assessed with the CFI, TLI, and RMSEA fit indices, and these are reported in Table 1. As shown in Table 1, the models fit the data well for the average trajectories of psychosocial maturity, alcohol use, and marijuana use.
Table 1.
Fit Coefficients for the Key Models
| χ2 | d.f. | CFI | TLI | RMSEA | |
|---|---|---|---|---|---|
| Latent Growth Curve Models for average trajectories of: |
|||||
| Psychosocial Maturity (N=1,153) | 155.72*** | 58 | .977 | .980 | .038 |
| Alcohol Use (N=1,153) | 327.42*** | 182 | .955 | .947 | .026 |
| Marijuana Use (N=1,153) | 313.06*** | 180 | .951 | .942 | .026 |
| Autoregressive Latent Trajectories Models of Psychosocial Maturity and Substance Use | |||||
| Alcohol Use (N=1,170) | 731.97*** | 524 | .973 | .971 | .018 |
| Marijuana Use (N=1,170) | 753.74*** | 524 | .970 | .968 | .019 |
Average Trajectories of Psychosocial Maturity and Substance Use
Psychosocial maturity, on average, did not show significant growth (mean intercept = −.05 and mean slope = .05, n.s.). However, there was significant variation in both intercept and slope (SD intercept = .61 and SD slope = .68, both p’s < .001), indicating that youths started from different levels of maturity and also varied in their age-related changes in maturity. Adolescents with lower initial maturity showed greater increases in maturity with age (r = −.62, p < .001).
Controlling for time-varying proportion of supervised time, alcohol use followed a pattern of significant linear growth that decelerated over age (mean intercept = .75, mean linear slope = 1.08, p < .001, and mean quadratic term = −.47, p < .05). There was significant heterogeneity in developmental trajectories of alcohol use (SD intercept = .83, p < .001, and SD linear slope = 1.10, p < .001), but there was no significant variation in the SD for quadratic slope. Those who started with higher alcohol use tended to increase less with age (r = −.64, p < .001).
Controlling for time-varying proportion of supervised time, marijuana use also followed a trajectory of significant positive linear growth that decelerated over age (mean intercept = .81, mean linear slope = 1.39, p < .001, and mean quadratic term = −1.12, p < .001). Individual differences in trajectories of marijuana use were not significant (SD intercept = .44, n.s., SD linear slope = .26, n.s.), and SD quadratic term was not significant. Marijuana use intercept and slopes were not significantly correlated.
Ethnic Differences in Trajectories of Psychosocial Maturity and Substance Use
Trajectories of psychosocial maturity varied by ethnicity, but only for the initial level of psychosocial maturity (Δχ2 (2) = 56.94, p < .001) and not the rate of change: (Δχ2 (2) = 5.06, n.s.). African American participants had significantly higher intercepts (Δχ2 (1) = 54.79, < .001) than did non-Hispanic Caucasian and Hispanic American youths. There were no significant differences between the intercepts of non-Hispanic Caucasian and Hispanic American youths.
For alcohol use, there were significant ethnic differences in intercepts (Δχ2 (2) = 8.11, p < .05), but not the linear or quadratic growth terms. African American youths had a significantly lower intercept of alcohol use than did non-Hispanic Caucasian and Hispanic American youths: Δχ2 (1) = 7.96, p < .01. Intercepts of non-Hispanic Caucasian American and Hispanic American participants were not significantly different. Because of the ethnic differences in alcohol intercepts, subsequent models included the effect of ethnicity on alcohol use intercept.
Developmental trajectories of marijuana use for Hispanic American youths differed significantly from those for non-Hispanic Caucasian and African American adolescents (Δχ2 (3) = 34.86, p < .001), and there were ethnic differences in both slopes and intercepts. Hispanic American youths started at a significantly higher level of marijuana use than did non-Hispanic Caucasian American and African American youths (Δχ2 (1) = 6.68, p < .01) but they did not increase marijuana use over age; whereas non-Hispanic Caucasian and African American adolescents started at a lower level of marijuana use than did Hispanic American youths but exhibited a significant linear increase in marijuana use that decelerated over age. The linear and quadratic change coefficients for Hispanic American youths were significantly different from those for non-Hispanic Caucasian and African American adolescents (Δχ2 (1) = 11.69, p < .001 for the slope and Δχ2 (3) = 7.54, p < .01 for the quadratic term). Non-Hispanic Caucasian and African American youths did not differ in their developmental trajectories of marijuana use. Because of these ethnic differences, subsequent models controlled for ethnic differences in marijuana use intercept and slope.
Autoregressive Latent Transition (ALT) Analyses
The next series of models tested both how individual age-related trajectories of psychosocial maturity were associated with trajectories of substance use and whether short-term changes in one of these variables (i.e., psychosocial maturity or substance use) led to changes in the other six months later. To do this, we used Autoregressive Latent Transitions models (ALT; Bollen & Curran, 2004). Here, two types of associations are modeled: the association between the growth parameters of the latent growth curves (i.e., correlations between the intercepts and slopes of substance use and psychosocial maturity), and cross-lagged effects between substance use and psychosocial maturity at individual time points. An example of an ALT model for psychosocial maturity and alcohol use is presented in Figure 1. The paths from alcohol and marijuana use intercepts to maturity slope were not significant and were trimmed from the models. Again, the models controlled for the effects of ethnicity on the psychosocial maturity and substance use intercepts and on the slope of marijuana use, and the effects of antisocial risk on psychosocial maturity and substance use intercepts and slopes. The time-varying effects of proportion of supervised time on alcohol and marijuana use were also controlled.
Figure 1.

Example of an Autoregressive Latent Transition Model for Psychosocial Maturity and Alcohol Use
Note. PST = proportion of time in a supervised setting. For ease of presentation, some correlations were represented with a single squared line. These were correlations between: alcohol use at age 15 and alcohol use intercept, alcohol use slope, and maturity at age 15; alcohol use intercept and alcohol use slope; maturity at age 15, maturity intercept and maturity slope; maturity intercept and maturity slope; alcohol use intercept and maturity intercept, alcohol use slope and maturity slope, and the correlations between PST and alcohol use at age 15, alcohol use intercept, alcohol use slope, maturity at age 15, maturity intercept, and maturity slope.
Because little is known about the effects of alcohol or marijuana use on psychosocial maturity, there is a lack of guiding theory or data to choose appropriate time lags for these models. However, because our participants were interviewed every six months and because effects of adolescent marijuana use on cognitive outcomes have been reported to linger for one to three months after abstinence (Jacobus et al., 2009), we adopted a six-month interval for the cross-lagged effects. To facilitate model convergence (Bollen & Curran, 2004), the cross-lag paths were constrained to be equal. All participants (N=1,170) were included in these models and they had good fit for both alcohol and marijuana use variables (see Table 1).
Higher initial alcohol use was associated with significantly lower initial levels of psychosocial maturity (r = −.25, p < .05). However, the slope of alcohol use was not associated with the slope of psychosocial maturity (r = −.10, n.s). When examining lagged effects, higher alcohol use predicted a significant decline in psychosocial maturity six months later (β =−.03, p < .05), but not vice versa – i.e., psychosocial maturity did not predict change in alcohol use.
Higher initial levels of marijuana use were associated with lower initial psychosocial maturity (r =−.17, p < .05). Moreover, the slope of marijuana use was inversely associated with the slope of psychosocial maturity (r =−.52, p < .01), such that greater age-related increases in marijuana use were associated with smaller age-related increases in maturity. Examination of lagged effects revealed that higher marijuana use was associated with decreased psychosocial maturity six months later (β =−.05, p < .001) and, conversely, higher psychosocial maturity was associated with lower marijuana use six months later (β =−.06, p < .01). In sum, these results showed that: (1) initial substance use was associated with lower initial psychosocial maturity, (2) the rate at which adolescents develop psychosocial maturity was independent of the rate of change in alcohol use but was negatively associated with the rate of change in marijuana use, (3) both higher alcohol and higher marijuana use were associated with time-specific decreases in maturity six months later (above and beyond the boys’ average level of maturity), and (4) higher psychosocial maturity was associated with time-specific decreases in marijuana use six months later (above and beyond the boys’ average level of marijuana use).
Group-Based Modeling of Substance Use
Both theory and previous research have suggested that there is substantial heterogeneity in trajectories of substance use, such that an overall, aggregate depiction of the relation between age and substance use does not present an appropriate characterization (e.g., Windle & Wiesner, 2004). Accordingly, the final set of analyses tested for the presence of qualitatively different developmental trajectories of substance use, while also allowing for within-trajectory group variability in growth parameters (e.g., intercepts and slopes), with a general growth mixture model (GGMM) for zero-inflated censored data (Kreuter & Muthen, 2008).3 Specifically, in our models we examined quadratic trajectories of substance use over age and tested, within the GGM model, whether youths following different substance use trajectories significantly differed in their intercepts and slopes of psychosocial maturity. All models were tested with Mplus 4.2 (Muthen & Muthen, 2004). Variance in alcohol and marijuana use that was associated with time spent in supervised settings was partialled out with OLS regressions prior to GMM modeling. Missing data on supervised time meant that the alcohol and marijuana use scores of some participants could not be adjusted for supervised time in these OLS regressions. Thus, 903 participants were included in the GMM modeling. Once again, the antisocial risk variable and ethnicity were controlled for in models testing the association between the substance use trajectories and psychosocial maturity. Because of the preponderance of zeros in the data (i.e., when youths did not used alcohol or marijuana within a given time period), we used models for censored zero-inflated data. For both alcohol and marijuana use, a quadratic model was tested. The optimal number of classes was guided by the Bayesian Information Criterion (BIC) and the p value for the Lo-Mendel-Rubin likelihood ratio test (LRT; Lo, Mendel, & Rubin, 2001). Optimization for the GMM models is carried out in two stages. By default, during the first stage, ten random sets of starting values are generated and ten iterations are carried out for each value. Second, two values (of the original ten) with the highest ending log likelihoods are selected and are used as starting values in the final stage optimizations (Muthen & Muthen, 2004). To avoid local maxima, we carried out a more thorough investigation by using up to 500 starting values (depending on replicability of results), 20 initial stage iterations, and up to 50 starting values for the final stage optimizations. For all models, the solution was not accepted until the best log likelihood was replicated across several starting values.
Based on the BIC and LRT (Table 2), 4-group models were selected for both alcohol and marijuana use. The four trajectories of alcohol use (Figure 2) were Adolescence-Limited (12%), Low (38%), Decreasing (14%), and Increasing (36%). The average posterior probabilities were .70 for Adolescence-Limited, .66 for Low, .68 for Decreasing, and .72 for Increasing groups. Nagin (2005) suggested that posterior probabilities >.70 are indicative of good placement of individuals into groups. Thus, our results both suggest adequate probability of an individual being assigned to the group to which their behavior most resembled, and also some variability within each group. This reinforces our choice of growth mixture modeling, which estimates variability in growth parameters, rather than latent class growth analysis, which does not.
Table 2.
Fit Statistics for Growth Mixture Models of Alcohol and Marijuana Use
| Models | Log Likelihood | # of Parameters | BIC | LRT |
|---|---|---|---|---|
| Alcohol Use (N=903) | ||||
| 2 groups | −5,236.4 | 24 | 10,636.1 | .000 |
| 3 groups | −5,156.9 | 29 | 10,511.3 | .016 |
| 4 groups | −5,131.8 | 34 | 10,494.9 | .003 |
| 5 groups | −5,101.5 | 39 | 10,468.5 | .075 |
| Marijuana Use (N=903) | ||||
| 2 groups | −6,080.9 | 23 | 12,318.2 | .000 |
| 3 groups | −6,032.5 | 28 | 12,255.6 | .000 |
| 4 groups | −5,768.6 | 33 | 11,652.3 | .000 |
| 5 groups | −6,019.0 | 38 | 12,296.6 | .080 |
BIC = Bayesian Information Criterion; LRT = Lo-Mendell-Rubin Likelihood Ratio Test for N-1 vs. N number of groups (a significant value indicates preference for a model with more groups
Figure 2.

Trajectories of Predicted Alcohol Use Adjusted for Supervised Time (N = 903)
The four trajectories of marijuana use (Figure 3) were Decreasing (26%), Low (38%), Increasing (31%), and Late Adolescent Onset (5%). The average posterior probabilities were .76 for Decreasing, .66 for Low, .78 for Increasing, and .65 for Late Adolescent Onset groups, again indicating adequate capability of the model to place individuals into groups.
Figure 3.

Trajectories of Predicted Marijuana Use Adjusted for Supervised Time (N = 903)
Trajectories of psychosocial maturity were compared across the alcohol and marijuana use groups by testing the differences among the psychosocial maturity intercept and slope across the latent substance use groups. The model for alcohol use controlled for the effects of antisocial risk on the psychosocial maturity intercept and slope, as well as for ethnic differences in the psychosocial maturity intercepts. The model for marijuana use controlled for the effects of antisocial risk and ethnicity on the psychosocial maturity intercept and slope.4
As Figure 4 indicates, youths on the decreasing alcohol use trajectory evinced low psychosocial maturity at age 15 but became significantly more mature as they got older (b = .91, SE = .45, p =.05) and were the only group that showed a significant increase in maturity. Youths on the low alcohol use trajectory evinced low psychosocial maturity at age 15 and did not significantly grow in psychosocial maturity as they got older (b=.07, SE = .17, n.s.). Youths on the increasing alcohol use trajectory evinced high levels of psychosocial maturity at age 15 but significantly declined in maturity as they got older (b=−.26, SE = .10, p < .05). Youths on the adolescence-limited trajectory evinced high psychosocial maturity at age 15 and did not significantly change in psychosocial maturity over age (b =−.04, SE =.25, n.s.).
Figure 4.

Trajectories of Psychosocial Maturity by Alcohol Use Groups (N = 903)
To test whether maturity trajectories significantly varied across the alcohol groups, we compared a model in which intercepts and slopes of psychosocial maturity were constrained to be equal across the alcohol groups to a model in which the intercepts and slopes were allowed to vary. There was significantly better model fit when intercepts and slopes were allowed to vary across the alcohol use groups (Δχ2 [3] = 29.22, p <.001 for intercepts and Δχ2 [3] = 19.13, p <.001 for slopes), suggesting that trajectories of psychosocial maturity varied across the alcohol groups. Tests of all pairwise comparisons among the alcohol groups indicated that maturity intercepts for the adolescence-limited and increasing groups were significantly higher than intercepts for the low and decreasing groups (Δχ2 [1]= 25.13, p <.001). The decreasing alcohol group showed the steepest increase in psychosocial maturity (Δχ2 [1] = 12.79, p <.001) and the increasing alcohol group showed the least steep increase in psychosocial maturity (Δχ2 [1] = 16.35, p < .001), and in fact, showed a decrease.
For marijuana use, as shown in Figure 5, youths on the decreasing trajectory evinced low psychosocial maturity at age 15 but significantly increased in maturity with age (b = .47, SE = .16, p < .01). Similar to the case for alcohol use, youth who decreased marijuana use were the only group that showed a significant increase in maturity. Youths on the increasing marijuana use trajectory evinced low psychosocial maturity at age 15, but did not significantly change with age (b=−.07, SE = .09, n.s.). Youths on the low marijuana use trajectory evinced high psychosocial maturity at age 15 and did not significantly change with age (b = .01, SE = .11, n.s.. Youths on the late adolescent onset marijuana use trajectory also evinced high psychosocial maturity at age 15 but declined significantly over age (b =−.32, SE = .16, p < .05).
Figure 5.

Trajectories of Psychosocial Maturity by Marijuana Use Groups (N = 903)
To test whether trajectories of psychosocial maturity varied across the marijuana groups we compared a model that constrained intercepts and slopes of psychosocial maturity to be equal across the marijuana groups to a model that allowed the intercepts and slopes to vary. There was significantly worse model fit in the constrained model (Δχ2 [3] = 9.64, p <.05 for intercepts and Δχ2 [3] = 18.06, p <.001 for slopes) suggesting that intercepts and slopes of psychosocial maturity significantly varied across the marijuana groups. Tests of all pairwise comparisons indicated that maturity intercepts for the late adolescent onset and low marijuana use groups were significantly higher than were maturity intercepts for the increasing and decreasing marijuana use groups (Δχ2 [1] = 9.33, p <.01). Those on the decreasing marijuana use trajectory showed the steepest growth in psychosocial maturity (Δχ2 [1]= 15.91, p <.001) and those on the late adolescent onset marijuana use trajectories showed the least (Δχ2 [1] = 5.07, p <.05).
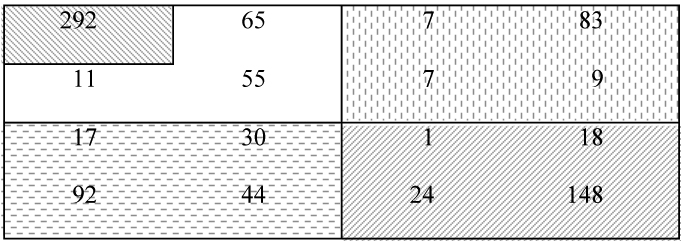
These analyses tested separate contributions of alcohol and marijuana use trajectories and did not take into account their joint contribution. Thus, the final analyses created substance use groups by assigning individuals to the alcohol and marijuana use groups (based on their posterior probabilities) and cross-tabulating these groups (see Table 3). To create groups of reasonable sample size, we defined a “Low” use group (combining low stable alcohol and marijuana use); an “Elevated Alcohol-Decreasing or Low Marijuana” group (combining low stable or decreasing marijuana use with increasing or adolescent-limited alcohol use) an “Elevated Marijuana-Decreasing or Low Alcohol” group (combining decreasing or low stable alcohol use with increasing or late adolescent onset marijuana use), an “Increasing group” (combining late adolescent onset or increasing marijuana use with adolescence-limited or increasing alcohol use), and a “Decreasing” group (decreasing marijuana use and decreasing or low stable alcohol use).
Table 3.
| Marijuana Use Groups |
||||
|---|---|---|---|---|
| Low-Stable | Decreasing | Late Adolescent Onset |
Increasing | |
| Alcohol use groups | ||||
| Low-Stable |
|
|||
| Decreasing | ||||
| Adolescence-limited | ||||
| Increasing | ||||
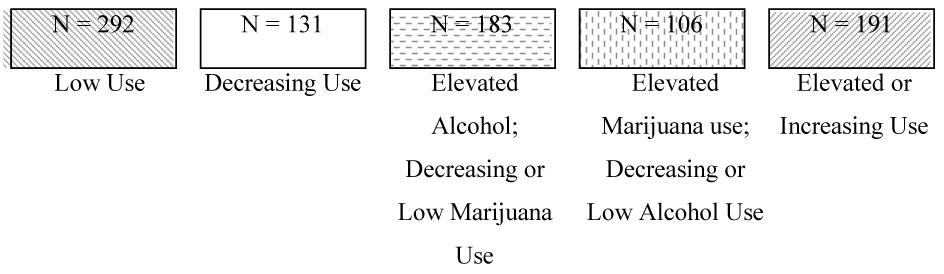 | ||||
We then compared these groups on their intercepts and slopes of psychosocial maturity (controlling for the effects of ethnicity on the psychosocial maturity intercept, and of antisocial risk on psychosocial maturity intercept and slope). Adolescents in the five combined groups followed different trajectories of psychosocial maturity (Figure 6). There were no significant differences in intercepts (Δχ2 [4] = 4.31, n.s.), but there were significant differences in slopes (Δχ2 [4]= 18.99, p < .001). Psychosocial maturity slopes for boys in the “low,” “decreasing,” and “elevated alcohol, decreasing or low marijuana” groups were significantly higher than those for boys in the “elevated marijuana, decreasing or low alcohol” and “increasing” groups (Δχ2 [1]= 16.35, p < .001). The last two groups were also characterized by a significant decline in psychosocial maturity, whereas only the “decreasing use” group showed a significant increase in maturity (Figure 6). Differences among slopes of all other groups were not significant.
Figure 6.

Trajectories of Psychosocial Maturity by Substance Use Groups (N = 903)
Discussion
The current study examined the relation between adolescent alcohol and marijuana use and developmental growth in psychosocial maturity from ages 15 to 21 within a sample of male juvenile offenders. Given the nature of the sample, it was first important to examine age-related changes in substance use and maturity considered separately. Our findings showed that, overall, alcohol and marijuana use still showed the significant increases that were expected during these ages and that are found in more general population samples (e.g., Chen & Kandel, 1995). In contrast, there was no significant overall increase in psychosocial maturity, suggesting that, as an overall group, adolescents in this sample were not experiencing age-typical increases in maturity. This overall lack of growth in maturity might reflect the characteristics of a male offender sample and/or might suggest that factors correlated with boys’ juvenile offending might act to suppress age-typical growth in maturity. For example, these boys may be embedded in family and peer environments as well as the environments of correctional facilities that may suppress growth in maturity (Steinberg, Chung, & Little, 2004). It is also possible that different age-related patterns of growth would be found for girls or for individual components of maturity, which may not all follow the same timing of growth (Steinberg et al., 2008, 2009). However, even though there was no significant overall growth in psychosocial maturity in the sample as a whole, there was significant individual variation in growth, so that the relation between adolescent substance use and growth in maturity could be tested.
Consistent with previous research on heterogeneity in developmental trajectories of substance use, we identified distinct patterns of age-related changes in alcohol and marijuana use that varied in levels of use, ages of increase and decline, and the extent of change. Comparing our trajectory solutions to previous studies is difficult, not only because studies vary in the ages and demographic characteristics of the samples, but also because variations in the number and timing of assessments and operational definitions of substance use produce different findings (Jackson & Sher, 2005; 2006). Common across most studies of adolescents, and also present in the current data are stable low-level alcohol and marijuana users as well as those who increase their use with age (e.g., Hill et al., 2000; Guo et al., 2002; Ellickson et al., 2004; Tucker et al., 2005; Windle & Wiesner, 2004). These previous studies have also found an early onset group that uses at high levels and either maintains their use or decreases over time (analogous to our decreasing group). Perhaps our most unusual group was the developmentally limited drinkers. Although this pattern is common in epidemiological data (Masten et al., 2008), it is unusual to observe declines at ages as young as those in the current study (age 18). Of course, the substance use trajectories identified in the current study are influenced not only by the demographic characteristics of the sample (ethnically diverse, males, ages 15–21), but by the sanctions and interventions that juvenile offenders receive, making comparison to previous studies tentative.
The central question of the study was whether higher levels of adolescent alcohol and marijuana use were associated with a lowered rate of growth in maturity. We tested this question in multiple ways—asking whether past six-month use at one age point could predict lowered maturity six months later; and whether longer-term patterns of alcohol and marijuana use over age could predict the rate of growth in maturity. As our ALT models revealed, six-month periods of elevated alcohol or marijuana use prospectively predicted a lowered level of maturity six months later. Importantly, in an ALT modeling framework, these time-specific effects are tested above and beyond a boy’s expected trajectory of maturity, so they indicate that maturity was decreased below a boy’s expected level in the six-month period after his substance use was elevated.
Moreover, longer-term patterns of alcohol and marijuana use were also associated with changes in maturity. Specifically, elevated or increasing adolescent substance use was actually associated with significant declines in maturity over these ages. Conversely, decreases in alcohol and marijuana use were associated with significant increases in psychosocial maturity. Although directionality (and causality) cannot be established from these analyses, the combination of the short-term prospective prediction and these longer-term relations between substance use and maturity suggest that there is some temporal precedence such that substance use predicts maturity. These findings suggest some cause for concern in that elevated and prolonged adolescent substance use is associated with decreased growth in psychosocial maturity. Multiple mechanisms could underlie this relation including avoidance of the developmentally-appropriate challenges needed for the development of maturity and/or substance use effects on the developing adolescent brain. Both of these mechanisms suggest that preventive interventions to delay substance use until after sufficient neurobiological maturation or sufficient experience with developmental tasks could have potential benefit for the development of psychosocial maturity (Odgers et al., 2008).
At the same time, however, the fact that declines in alcohol and marijuana use were associated with growth in maturity suggests a cause for optimism in that reduced psychosocial maturity is not necessarily permanent. Similar findings have been reported from longitudinal studies that have predicted outcomes at a single adult time point (rather than predicting age-related changes in an outcome variable, as we did in the current study). For example, Jessor, Donovan and Costa (1991) found that adolescent “problem behavior” (including alcohol use) that persisted into adulthood predicted negative adult developmental outcomes such as low job prestige and job satisfaction, but adolescent problem behavior that remitted by adulthood was not associated with negative adult outcomes. Other long-term studies of offender trajectories points to similar substantive conclusions (Piquero et al, in press). Given the high prevalence of adolescent substance use and substance use disorders among juvenile offenders (Chassin, 2008), even though prevention of substance use may not be a realistic goal, substance use treatment may be beneficial for growth in psychosocial maturity.
It is also noteworthy that these results were obtained above and beyond the effects of ethnicity, of time spent in supervised correctional settings, and of antisocial history. Thus, although “third variable” effects cannot be definitively ruled out and not all possible confounding variables were tested, our substantive results remain even after controlling for some of the most obvious potential confounds. Significant relations between increasing maturity and decreasing alcohol and marijuana use might also be due to a common response bias, such that boys who wish to present themselves more positively over age, report more socially desirable responses on both substance use and psychosocial maturity items. However, this explanation is unlikely given the significant prospective effect of substance use on maturity six months later.
Our findings also suggest that it is important to consider the use of multiple substances. That is, although low levels and decreases in both alcohol and marijuana use were associated with growth in maturity in separate analyses, our combined analyses suggested that marijuana use was particularly meaningful. Specifically, those who decreased their marijuana use (despite elevated alcohol use) showed significant growth in psychosocial maturity. A recent review of the literature on substance use and adolescent brain development (Squeglia et al., 2009) similarly suggests that there may be different impacts from different forms of substance use on cognitive functioning (e.g., tests of memory, attention, and learning) and suggests that co-occurring use be considered in future research.
Although our findings suggest that elevated levels of adolescent substance use are associated with suppressed age-typical growth in psychosocial maturity, there are important questions that were not addressed by our study, as well as limitations that should be considered. First, our data do not speak to the mechanisms that underlie the effects of adolescent alcohol and marijuana use on psychosocial maturity. As noted earlier, there may be multiple underlying mechanisms, including the effects of adolescent substance use on the development of neurobiological systems governing reward sensitivity and self-regulation and the effects of adolescent substance use on individuals’ level of engagement with developmental challenges that is necessary for the development of coping skills and self-regulatory abilities. Identifying these mechanisms is an important future goal. Second, our study did not test whether there are specific thresholds of consumption (in terms of specific levels of quantity, frequency or duration of use) at which deleterious effects are triggered. Shedler and Block (1990) suggest that total abstinence from adolescent substance use is associated with maladjustment, and that low levels of experimental substance use are actually beneficial (although more recent data have not replicated this finding (Milich et al., 2000; Tucker et al., 2006). In any case, in terms of clinical implications, it would be important to know what levels and durations of use create risk for negative outcomes. Finally, our results were obtained in a sample of male serious juvenile offenders, and it is unknown whether similar findings would obtain in a study of female offenders or in general population samples.
In short, the current study asked whether adolescent alcohol and marijuana use were associated with suppressed age-typical development in psychosocial maturity. We used multiple methods to test these relations, and we tested effects of substance use above and beyond time spent in supervised settings, ethnicity, and initial antisociality. Overall, there was no significant growth in maturity among these adolescent offenders, but there was significant variation in growth. Moreover, alcohol and marijuana use at one age point prospectively predicted lower maturity six months later. Longer-term patterns of increasing substance use were associated with declines in maturity (particularly for marijuana use) whereas longer-term patterns of decreasing use were associated with significant increases in maturity. Thus, our results suggest that continuity is not set in stone, and there exist important prospects for change that can re-orient paths away from negative outcomes—even among serious juvenile offenders.
Acknowledgments
This project was supported by funds from the following: Office of Juvenile Justice and Delinquency Prevention, National Institute of Justice, John D. and Catherine T. MacArthur Foundation, William T. Grant Foundation, Robert Wood Johnson Foundation, William Penn Foundation, Center for Disease Control, National Institute on Drug Abuse (R01DA019697), Pennsylvania Commission on Crime and Delinquency, and the Arizona Governor’s Justice Commission. We are grateful for their support. The content of this paper, however, is solely the responsibility of the authors and does not necessarily represent the official views of these agencies. Dr. Modecki’s contributions were supported by the National Institute of Mental Health Training Grant T32 MH018387.
Footnotes
Publisher's Disclaimer: The following manuscript is the final accepted manuscript. It has not been subjected to the final copyediting, fact-checking, and proofreading required for formal publication. It is not the definitive, publisher-authenticated version. The American Psychological Association and its Council of Editors disclaim any responsibility or liabilities for errors or omissions of this manuscript version, any version derived from this manuscript by NIH, or other third parties. The published version is available at www.apa.org/journals/adb
Other potentially important covariates were measured in the data set. To evaluate the possibility of including other covariates, we predicted maturity intercept and slope from baseline measures of family functioning (parental knowledge of adolescent’s activities, parental monitoring, parental hostility, and parental warmth). However, although these variables predicted maturity intercept, they did not significantly predict maturity slope. Baseline depression scores in this sample had a restricted range and thus were not useful as a covariate. Thus, because antisociality, race/ethnicity, and time spent in supervised facilities were closely associated with substance use and particularly relevant for an offender sample, we selected these for inclusion as covariates.
The Full Pathways sample also contained 184 female participants. However, because we did not cap the percentage of drug offenders at 15% for females and because of the small number of females, the current analyses are restricted to male participants.
Based on our growth curve modeling results, marijuana use did not have significant variability in its growth parameters, making it unclear whether there would be heterogeneity in forms of growth. However, because there were significant ethnic differences in both intercept and slope of marijuana use, we proceeded to test for heterogeneity in trajectories of marijuana use.
The marijuana trajectory group models included an additional control for ethnicity on maturity slope because our earlier analyses showed a significant effect of ethnicity on marijuana use slope. Thus, we wished to separate the portion of the association between the marijuana use trajectory groups and maturity slope that was due to ethnic differences in age-related changes in marijuana use.
References
- Albert D, Steinberg L, Woolard J, Banich M, Cauffman E, Graham S. Age differences in strategic planning as indexed by the Tower of London task. 2009 doi: 10.1111/j.1467-8624.2011.01613.x. Manuscript under review. [DOI] [PubMed] [Google Scholar]
- Barrera M, Castro F, Biglan A. Ethnicity, substance use and development: Exemplars for exploring group differences and similarities. Development and Psychopathology. 1999;11:805–822. doi: 10.1017/s0954579499002333. [DOI] [PubMed] [Google Scholar]
- Baumrind D, Moselle KA. A developmental perspective on adolescent drug abuse. Advances in Alcohol & Substance Abuse. 1985;4(3–4):41–67. doi: 10.1300/J251v04n03_03. [DOI] [PubMed] [Google Scholar]
- Bollen KA, Curran PJ. Autoregressive latent trajectory (ALT) models: A synthesis of two traditions. Sociological Methods Research. 2004;32:336–383. [Google Scholar]
- Brook JS, Brook DW, Arencibia-Mireles O, Richter L, Whiteman M. Risk factors for adolescent marijuana use across cultures and across time. Journal of Genetic Psychology. 2001;162(3):357–374. doi: 10.1080/00221320109597489. [DOI] [PubMed] [Google Scholar]
- Brown S, Tapert SF. Adolescence and the trajectory of alcohol use: Basic to clinical studies. Annals of the New York Academy of Sciences. 2004;1021(1):234–244. doi: 10.1196/annals.1308.028. [DOI] [PubMed] [Google Scholar]
- Brown S, McGue M, Maggs J, Schulenberg J, Hingson R, Swartzwelder S, Martin C, Chung T, Taper S, Sher K, Winters C, Lowman C, Murphy S. A developmental perspective on alcohol and youths 16 to 20 years of age. Pediatrics. 2008;121 Suppl. 4:S290–S310. doi: 10.1542/peds.2007-2243D. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cauffman E, Shulman E, Steinberg L, Claus E, Banich M, Graham S, Woolard J. Age differences in affective decision making as indexed by performance on the Iowa Gambling Task. Developmental Psychology. doi: 10.1037/a0016128. (in press). [DOI] [PubMed] [Google Scholar]
- Cauffman E, Steinberg L. (Im)maturity of judgment in adolescence: Why adolescents may be less culpable than adults. Behavioral Sciences & the Law. 2000;18(6):741–760. doi: 10.1002/bsl.416. [DOI] [PubMed] [Google Scholar]
- Cauffman E, Woolard J. The Future Outlook Inventory. Instrument developed for the MacArthur Juvenile Competence Study. Unpublished measure available from the first author. Irvine: Department of Psychology and Social Behavior, University of California; 1999. [Google Scholar]
- Chambers RA, Taylor JR, Potenza MN. Developmental neurocircuitry of motivation in adolescence: A critical period of addiction vulnerability. American Journal of Psychiatry. 2003;160:1041–1052. doi: 10.1176/appi.ajp.160.6.1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chassin L. Juvenile justice and substance use. The Futures of Children. 2008;18(2):165–185. doi: 10.1353/foc.0.0017. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pitts SC, DeLucia C. The relation of adolescent substance use to young adult autonomy, positive activity involvement, and perceived competence. Development and Psychopathology. 1999;11:915–932. doi: 10.1017/s0954579499002382. [DOI] [PubMed] [Google Scholar]
- Chen K, Kandel DB. The natural history of drug use from adolescence to the midhirties in a general population sample. American Journal of Public Health. 1995;85:41–47. doi: 10.2105/ajph.85.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark DB, Thatcher DL, Tapert SF. Alcohol, psychological dysregulation, and adolescent brain development. Alcoholism: Clinical and Experimental Research. 2008;32(3):375–385. doi: 10.1111/j.1530-0277.2007.00601.x. [DOI] [PubMed] [Google Scholar]
- Colder CR, Chassin LC. Affectivity and impulsivity: Temperament risk for adolescent alcohol involvement. Psychology of Addictive Behaviors. 1997;11(2):83–97. [Google Scholar]
- Colder CR, Stice E. A longitudinal study of the interactive effects of impulsivity and anger on adolescent problem behavior. Journal of Youth and Adolescence. 1998;27(3):255–274. [Google Scholar]
- Cooper ML, Agocha VB, Sheldon MS. A motivational perspective on risky behaviors: The role of personality and affect regulatory processes. Journal of Personality. 2000;68(6):1059–1088. doi: 10.1111/1467-6494.00126. [DOI] [PubMed] [Google Scholar]
- Ellickson P, Martino S, Collins R. Marijuana use from adolescence to young adulthood: Multiple developmental trajectories and their associated outcomes. Health Psychology. 2004;23:299–307. doi: 10.1037/0278-6133.23.3.299. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Swain-Campbell N. Cannabis use and psychosocial adjustment in adolescence and young adulthood. Addiction. 2002;97(9):1123–1135. doi: 10.1046/j.1360-0443.2002.00103.x. [DOI] [PubMed] [Google Scholar]
- Giancola PR, Martin CS, Tarter RE. Executive cognitive and aggressive behavior in preadolescent boys at high risk for substance abuse/dependence. Journal of Studies on Alcohol. 1996;57:352–259. doi: 10.15288/jsa.1996.57.352. [DOI] [PubMed] [Google Scholar]
- Goudriaan AE, Grekin ER, Sher KJ. Decision making and binge drinking: A longitudinal study. Alcoholism, Clinical and Experimental Research. 2007;31(6):928–938. doi: 10.1111/j.1530-0277.2007.00378.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenberger E, Knerr C, Knerr B, Brown JB. Measuring psychosocial maturity: A status report. Johns Hopkins University Center for Social Organization of Schools; 1974. [Google Scholar]
- Greenberger E, Sorensen AB. Toward a concept of psychosocial maturity. Journal of Youth and Adolescence. 1974;3(4):329–358. doi: 10.1007/BF02214746. [DOI] [PubMed] [Google Scholar]
- Grisso T, Steinberg L, Woolard J, Cauffman E, Scott E, Graham S, et al. Juveniles’ competence to stand trial: A comparison of adolescents’ and adults’ capacities as trial defendants. Law and Human Behavior. 2003;27(4):333–363. doi: 10.1023/a:1024065015717. [DOI] [PubMed] [Google Scholar]
- Guo J, Chung I, Hill KG, Hawkins JD, Catalano RF, Abbott RD. Developmental relationships between adolescent substance use and risky sexual behavior in young adulthood. Journal of Adolescent Health. 2002;31:354–362. doi: 10.1016/s1054-139x(02)00402-0. [DOI] [PubMed] [Google Scholar]
- Hill KG, White HR, Chung I, Hawkins JD, Catalano RF. Early adult outcomes of adolescent binge drinking: Person- and variable-centered analyses of binge drinking trajectories. Alcoholism: Clinical and Experimental Research. 2000;24(6):892–901. [PMC free article] [PubMed] [Google Scholar]
- Horvath LS, Milich R, Lynam D, Leukefeld C, Clayton R. Sensation seeking and substance use: A cross-lagged panel design. Individual Differences Research. 2004;2(3):175–183. [Google Scholar]
- Huizinga D, Esbensen F, Weiher A. Are there multiple paths to delinquency? Journal of Criminal Law and Criminology. 1991;82:83–118. [Google Scholar]
- Jackson K, Sher K. Similarities and differences of longitudinal phenotypes across alternate indices of alcohol involvement: A methodological comparison of trajectory approaches. Psychology of Addictive Behaviors. 2005;19:339–351. doi: 10.1037/0893-164X.19.4.339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson K, Sher K. Comparison of longitudinal phenotypes based on number and timing of assessments: A systematic comparison of trajectory approaches ii. Psychology of Addictive Behaviors. 2006;20:373–384. doi: 10.1037/0893-164X.20.4.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobus J, Bava S, Cohen-Zion M, Mahmood O, Tapert S. Functional consequences of marijuana use in adolescents. Pharmacology, Biochemistry, and Behavior. 2009;92:559–565. doi: 10.1016/j.pbb.2009.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor R, Donovan JE, Costa F. Beyond Adolescence: Problem Behavior and Young Adult Development. New York: Cambridge University Press; 1991. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Demographic subgroup trends for various licit and illicit drugs, 1975–2007 (Monitoring the Future Occasional Paper No. 69) [Online] Ann Arbor, MI: Institute for Social Research; 2008. Available: http://www.monitoringthefuture.org/ [Google Scholar]
- King KM, Meehan BT, Trim RS, Chassin L. Marker or mediator? The effects of adolescent substance use on young adult educational attainment. Addiction. 2006;101:1730–1740. doi: 10.1111/j.1360-0443.2006.01507.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kreuter F, Muthén B. Analyzing criminal trajectory profiles: Bridging multilevel and group-based approaches using growth mixture modeling. Journal of Quantitative Criminology. 2008;24:1–31. [Google Scholar]
- Li F, Duncan T, Hops H. Examining developmental trajectories in adolescent alcohol use using piecewise growth mixture modeling analysis. Journal of Studies on Alcohol. 2001;62:199–210. doi: 10.15288/jsa.2001.62.199. [DOI] [PubMed] [Google Scholar]
- Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- Loeber R, Burke J, Pardini D. Development and etiology of disruptive and delinquent behavior. Annual Review of Clinical Psychology. 2009;5:291–310. doi: 10.1146/annurev.clinpsy.032408.153631. [DOI] [PubMed] [Google Scholar]
- Masten A, Faden V, Zucker R, Spear L. Underage drinking: A developmental framework. Pediatrics. 2008;121 Suppl. 4:S235–S251. doi: 10.1542/peds.2007-2243A. [DOI] [PubMed] [Google Scholar]
- Mauricio A, Little M, Chassin L, Knight G, Piquero A, Losoya S, Vargas-Chanes D. Juvenile offenders’ alcohol and marijuana trajectories: Risk and protective actor effects in the context of time in a supervised facility. Journal of Youth and Adolescence. 2009;38:269–286. doi: 10.1007/s10964-008-9324-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McEwen B. Understanding the potency of stressful early life experiences on brain and body function. Metabolism. 2008;57 Supp. 2:S11–S15. doi: 10.1016/j.metabol.2008.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Medina K, McQueeny T, Nagel B, Hanson K, Schweinsburg A, Tapert S. Prefrontal cortex volumes in adolescents with alcohol use disorders: Unique gender effects. Alcoholism: Clinical and Experimental Research. 2008;32:386–394. doi: 10.1111/j.1530-0277.2007.00602.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milich R, Lynam D, Zimmerman R, Logan T, Martin C, Luekefeld C, Portis C, Miller J, Clayton R. Differences in young adult psychopathology among drug abstainers, experimenters, and frequent users. Journal of Substance Abuse. 2000;11:69–88. doi: 10.1016/s0899-3289(99)00021-8. [DOI] [PubMed] [Google Scholar]
- Modecki KL. Addressing gaps in the maturity of judgment literature: Age differences and delinquency. Law and Human Behavior. 2008;32(1):78–91. doi: 10.1007/s10979-007-9087-7. [DOI] [PubMed] [Google Scholar]
- Monahan K, Steinberg L, Cauffman E, Mulvey E. Trajectories of antisocial behavior and psychosocial maturity from adolescence to young adulthood. Developmental Psychology. doi: 10.1037/a0015862. (in press). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moss HB. Special section: Alcohol and adolescent brain development. Alcoholism: Clinical and Experimental Research. 2008;32(3):427–429. doi: 10.1111/j.1530-0277.2007.00606.x. [DOI] [PubMed] [Google Scholar]
- Mulvey EP, Steinberg L, Fagan J, Cauffman E, Piquero A, Chassin L, Knight G, Brame R, Schubert C, Hecker T, Losoya S. Theory and research on desistance from antisocial activity among serious juvenile offenders. Youth, Violence, and Juvenile Justice. 2004:213–236. doi: 10.1177/1541204004265864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulvey EP, Schubert CA, Chung HL. Service use after court involvement in a sample of serious adolescent offenders. Children and Youth Services Review. 2007;29(4):518–544. doi: 10.1016/j.childyouth.2006.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthen LK, Muthen BO. Mplus: The comprehensive modeling program for applied researchers. User’s guide. 3rd ed. Los Angeles: Muthen & Muthen; 2004. [Google Scholar]
- Nagin D. Group-based modeling of development. Cambridge, MA: Harvard University Press; 2005. [Google Scholar]
- Newcomb MD, Bentler PM. Impact of adolescent drug use and social support on problems of young adults: A longitudinal study. Journal of Abnormal Psychology. 1988;97:64–75. doi: 10.1037//0021-843x.97.1.64. [DOI] [PubMed] [Google Scholar]
- Odgers CL, Caspi A, Nagin DS, Piquero AR, Slutske WS, Milne B, Dickson N, Poulton R, Moffitt TE. Is it important to prevent early exposure to drugs and alcohol among adolescents?”. Psychological Science. 2008;19:1037–1044. doi: 10.1111/j.1467-9280.2008.02196.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedersen W. Mental health, sensation seeking and drug use patterns: a longitudinal study. British Journal of Addiction. 1991;86:195–204. doi: 10.1111/j.1360-0443.1991.tb01769.x. [DOI] [PubMed] [Google Scholar]
- Piquero A, Blumstein A, Brame R, Haapanen R, Mulvey E, Nagin D. Assessing the impact of exposure time and incapacitation on longitudinal trajectories of criminal offending. Journal of Adolescent Research. 2001;16:54–74. [Google Scholar]
- Piquero A, Farrington D, Nagin D, Moffitt TE. Trajectories of offending and their relation to life failure in late middle age: Findings from the Cambridge Study in Delinquent Development. Journal of Research in Crime and Delinquency. (in press). [Google Scholar]
- Potenza MN. To do or not to do? The complexities of addiction, motivation, self-control and impulsivity. American Journal of Psychiatry. 2007;164:4–6. doi: 10.1176/ajp.2007.164.1.4. [DOI] [PubMed] [Google Scholar]
- Schubert C, Mulvey E, Steinberg L, Cauffman E, Losoya S, Hecker T, Chassin L, Knight G. Operational lessons from the pathways to desistance project. Journal of Youth Violence and Juvenile Justice. 2004;2:237–255. doi: 10.1177/1541204004265875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulenberg J, Merline A, Johnston L, O’Malley P, Bachman J, Laetz V. Trajectories of marijuana use during the transition to adulthood: The Big Picture Based on national panel data. Journal of Drug Issues. 2005;35:255–279. doi: 10.1177/002204260503500203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulenberg J, O’Malley P, Bachman J, Wadsworth K, Johnston L. Getting drunk and growing up: Trajectories of frequent binge drinking during the transition to young adulthood. Journal of Studies on Alcohol. 1996;57:289–304. doi: 10.15288/jsa.1996.57.289. [DOI] [PubMed] [Google Scholar]
- Shedler J, Block J. Adolescent drug use and psychological health: A longitudinal inquiry. American Psychologist. 1990;45:612–630. doi: 10.1037//0003-066x.45.5.612. [DOI] [PubMed] [Google Scholar]
- Sowell E, Jernigan T. Further MRI evidence of late brain maturation: Limbic volume increase and changing asymmetries during childhood and adolescence. Developmental Neuropsychology. 1998;14:599–617. [Google Scholar]
- Spear LP. The adolescent brain and age-related behavioral manifestations. Neuroscience and Biobehavioral Reviews. 2000a;24:417–463. doi: 10.1016/s0149-7634(00)00014-2. [DOI] [PubMed] [Google Scholar]
- Spear LP. Neurobehavioral changes in adolescence. Current Directions in Psychological Science. 2000b;9(4):111–114. [Google Scholar]
- Squeglia L, Jacobus J, Tapert S. The influence of substance use on adolescent brain development. Clinical EEG and Neuroscience. 2009;40:31–38. doi: 10.1177/155005940904000110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L, Albert D, Cauffman E, Banich M, Graham S, Woolard J. Age differences in sensation seeking and impulsivity as indexed by behavior and self-report: Evidence for a dual systems model. Developmental Psychology. 2008;44:1764–1778. doi: 10.1037/a0012955. [DOI] [PubMed] [Google Scholar]
- Steinberg L, Cauffman E. Maturity of judgment in adolescence: psychosocial factors in adolescent decision making. Law and Human Behavior. 1996;20(3):249–272. [Google Scholar]
- Steinberg L, Cauffman E, Woolard J, Graham S, Banich M. Are adolescents less mature than adults? Minors’ access to abortion, the juvenile death penalty, and the alleged APA “flip-flop.”. American Psychologist. doi: 10.1037/a0014763. (in press). [DOI] [PubMed] [Google Scholar]
- Steinberg L, Chung H, Little M. Reentry of young offenders from the justice system: A developmental perspective. Youth Violence and Juvenile Justice. 2004;1:21–38. doi: 10.1177/1541204003260045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L, Graham V, O’Brien L, Woolard J, Cauffman E, Banich M. Age differences in future orientation and delay discounting. Child Development. 2009;80:28–44. doi: 10.1111/j.1467-8624.2008.01244.x. [DOI] [PubMed] [Google Scholar]
- Steinberg L, Monahan K. Age differences in resistance to peer influence. Developmental Psychology. 2007;43:1531–1543. doi: 10.1037/0012-1649.43.6.1531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tapert S, Granholm E, Leedy N, Brown S. Substance use and withdrawal: Neuropsychological functioning over 8 years in youth. Journal of the International Neuropsychological Society. 2002;8:873–883. doi: 10.1017/s1355617702870011. [DOI] [PubMed] [Google Scholar]
- Tapert SF, Schweinsburg AD, Drummond SPA, Paulus MP, Brown SA, Yang TT, Frank LR. Functional MRI of inhibitory processing in abstinent adolescent marijuana users. Psychopharmacology. 2007;194:173–183. doi: 10.1007/s00213-007-0823-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teicher M, Tomoda A, Andersen S. Neurobiological consequences of early stress and childhood maltreatment: Are results from human and animal studies comparable? Annals of the New York Academy of Sciences. 2006;1071:313–323. doi: 10.1196/annals.1364.024. [DOI] [PubMed] [Google Scholar]
- Trim RS, Meehan BT, King KM, Chassin L. The relation between adolescent substance use and young adult internalizing symptoms: Findings from a high-risk longitudinal sample. Psychology of Addictive Behaviors. 2007;21(1):97–107. doi: 10.1037/0893-164X.21.1.97. [DOI] [PubMed] [Google Scholar]
- Tucker J, Ellickson P, Collins R, Klein D. Are drug experimenters better adjusted than abstainers and users?: A longitudinal study of adolescent marijuana use. Journal of Adolescent Health. 2006;39:488–494. doi: 10.1016/j.jadohealth.2006.03.012. [DOI] [PubMed] [Google Scholar]
- Tucker JS, Ellickson PL, Orlando M, Martino SC, Klein DJ. Substance use trajectories from early adolescence to emerging adulthood: A comparison of smoking, binge drinking, and marijuana use. Journal of Drug Issues. 2005;35:307–332. [Google Scholar]
- Volkow ND, Fowler JS, Wang GJ. The addicted human brain viewed in the light of imaging studies: brain circuits and treatment strategies. Neuropharmacology. 2003;47:3–13. doi: 10.1016/j.neuropharm.2004.07.019. [DOI] [PubMed] [Google Scholar]
- Volkow N, Li T-K. The neuroscience of addiction. Nature Neuroscience. 2005;8(11):1429–1430. doi: 10.1038/nn1105-1429. [DOI] [PubMed] [Google Scholar]
- Wanner B, Viatro F, Carbonneau R, Tremblay R. Cross-lagged links among gambling, substance use, and delinquency from midadolescence to young adulthood: Additive and moderating effects of common risk factors. Psychology of Addictive Behaviors. 2009;23:91–104. doi: 10.1037/a0013182. [DOI] [PubMed] [Google Scholar]
- Weinberger DA, Schwartz GE. Distress and restraint as superordinate dimensions of self-reported adjustment: A typological perspective. Journal of Personality. 1990;58(2):381–417. doi: 10.1111/j.1467-6494.1990.tb00235.x. [DOI] [PubMed] [Google Scholar]
- White HR. The drug use-delinquency connection in adolescence. In: Weisheit R, editor. Drugs, crime and the criminal justice system. Cincinnati, Ohio: Anderson; 1990. pp. 215–256. [Google Scholar]
- White HR, Bates ME, Labouvie EW. Adult outcomes of adolescent drug use: A comparison of process-oriented and incremental analyses. In: Jessor R, editor. New perspectives on adolescent risk behavior. Cambridge, England: Cambridge University Press; 1998. pp. 150–181. [Google Scholar]
- Wills TA, Vaccaro D, McNamara G, Hirky AE. Escalated substance use: a longitudinal grouping analysis from early to middle adolescence. Journal of Abnormal Psychology. 1996;105(2):166–180. doi: 10.1037//0021-843x.105.2.166. [DOI] [PubMed] [Google Scholar]
- Windle M, Wiesner M. Trajectories of marijuana use from adolescence to young adulthood.: predictors and outcomes. Development and Psychopathology. 2004;16:1007–1027. doi: 10.1017/s0954579404040118. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Washington DC: American Psychiatric Press; Composite International Diagnostic Interview (CIDI) researcher’s manual. 1997