

Abstract
Removal of intramedullary nails often is relegated to younger surgeons but may be difficult and challenging. We describe difficulties with removal of an incarcerated expandable femoral nail and a new technique for retrograde mobilization of an intramedullary nail through a small infrapatellar incision. No special device was necessary for successful implant removal.
Level of Evidence: Level V, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Introduction
Intramedullary nailing is considered by many to be the gold standard for treating closed femoral shaft fractures in adult patients [18, 19]. Removal of an intramedullary nail may be performed for painful prominent hardware [18, 19], implant failure, infection, nonunion, or in some centers as a routine procedure [7]. The difficulty of this procedure is underestimated and we suspect sometimes relegated to younger surgeons. However, in some situations, it may be difficult and challenging even for experienced orthopaedic surgeons.
Intact intramedullary nails usually are removed using threaded extraction devices provided by the manufacturer. These devices may fail as a result of several factors such as destruction of the proximal nail threads, blocking of the proximal nail by bony ingrowth, or breakage of the threaded connection from the extraction bolt [23].
We describe a technique for removal of an incarcerated expandable intramedullary femoral nail. We are unaware of previous reports of this complication of an expandable nail and of this new technique for nail removal.
Case Report
A 21-year-old man sustained a closed fracture of the right femoral shaft after high-energy trauma (motorcycle accident) (Fig. 1). He underwent closed, antegrade nailing of his right femur with a 12-mm cannulated nail. Fifteen months after the initial trauma, radiographs in two planes revealed a hypertrophic nonunion of the right femur and shortening of 30 mm (Fig. 2). A two-staged procedure was planned: treatment of the nonunion first and lengthening in a second procedure. The nonunion was treated by implant removal, intramedullary reaming of the shaft as much as 17 mm, and insertion of an intramedullary expandable nail (length 400 mm, reduced diameter 12 mm, expanded diameter 19 mm) (Fixion nail; Disco-Tech, Tel Aviv, Israel) (Fig. 3). The expandable nail offers the advantages of improved load-sharing and rotational control without the need for interlocking screws and is recommended for tibial and femoral nonunions to decrease the use of autogenous bone graft [21].
Fig. 1A–B.

A 21-year-old man had a right femoral shaft fracture in a motorcycle accident. (A) An AP radiograph shows a displaced mid-shaft comminuted fracture. (B) The lateral radiograph shows a mid-shaft fracture without distal extension.
Fig. 2A–B.

(A) Anteroposterior and (B) lateral views show the posttraumatic hypertrophic nonunion of the femoral shaft 15 months after trauma.
Fig. 3A–D.

(A) Anteroposterior and (B) lateral radiographs are shown after intramedullary reaming and implantation of an expandable nail. (C) Anteroposterior and (D) lateral radiographs show consolidation 9 months after surgery.
After uneventful union (Fig. 3C–D), we proceeded with removal of the Fixion nail and insertion of an intramedullary skeletal kinetic distractor (ISKD) nail to address the femoral shortening by intramedullary lengthening. In the lateral position, the end cap of the nail was removed. The nail then was deflated according to the manufacturer’s instructions. The extraction device was inserted into the proximal end of the nail until it was tightened in the nail. Several attempts were made to extract the nail with the slotted hammer over the extraction device. However, the connection screw of the extraction device broke after several strokes. The nail still was jammed in the intramedullary canal.
We decided to mobilize the nail through a small incision through the knee. With the knee flexed 40°, a 3-cm long incision was made in the midline of the patellar tendon. Under fluoroscopic guidance, a 3-mm guide pin was inserted in the center of the knee 10 mm anterior to Blumensaat’s line. The pin was pushed forward to the distal end of the nail (Fig. 4A). The reamer of a distal femoral nail (DFN; Synthes, Umkirch, Germany) was used to open the distal femoral medullary canal (Fig. 4B). An extraction rod was inserted and firmly seated against the distal part of the nail. After a few slight hammer blows, the distal tip of the nail was deformed and the nail was mobilized and removed through its original insertion point (Fig. 4C–E). After removal of the expandable nail, an osteotomy for femoral lengthening was performed and the ISKD nail was inserted without any problems (Fig. 5).
Fig. 4A–E.

(A) A 3-mm guide wire approaches the distal part of the expansion nail. (B) Consequently, the reamer approaches the distal tip of the nail. (C) Placing of the extraction rod on the tip of the expansion nail and mobilization of the jammed nail by retrograde hits are shown. (D) Retrograde removal of the nail from the knee with slight hammer blows on an extraction rod is shown. (E) The distal tip of the nail is shown after removal.
Fig. 5A–B.
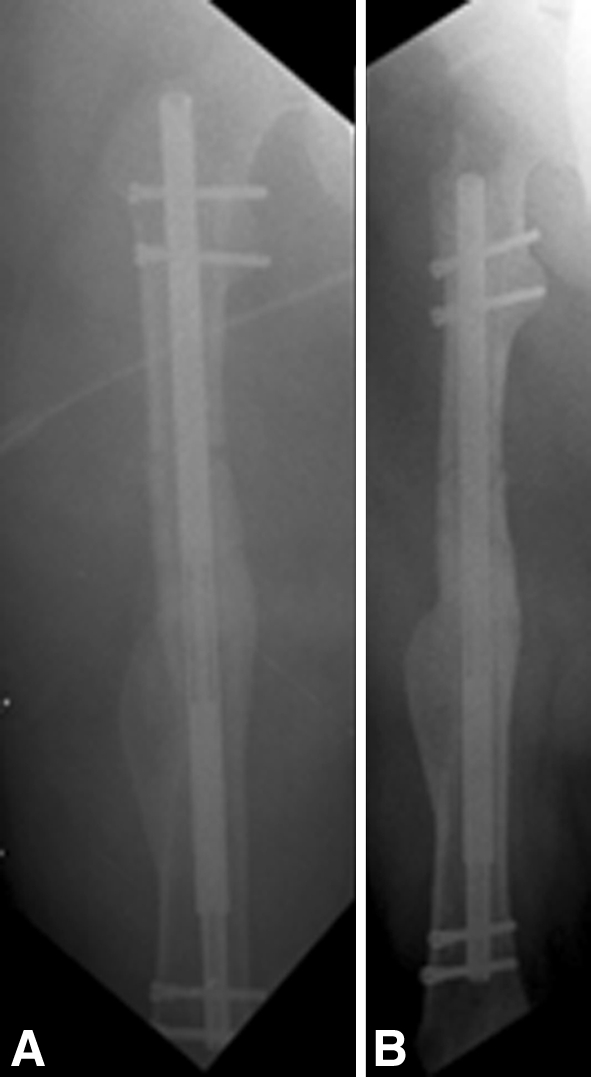
(A) Anteroposterior and (B) lateral postoperative radiographs are shown after insertion of the intramedullary skeletal kinetic distractor nail.
Discussion
Many techniques have been described for removal of broken intramedullary nails [1, 2, 5, 6, 9–13, 15, 16, 22]. However, few reports describe techniques for removal of jammed unbroken femoral nails [4, 23, 24], and articles describing complications [3, 15, 20] do not mention the problem of a jammed expandable nail. To the best of our knowledge, the technique of retrograde mobilization through a small-incision arthrotomy has not been described before.
The technique we describe is simple, minimally invasive, and can be used for different nail types. Moreover, no specialized or custom-made devices are needed and it can be performed with equipment available in most orthopaedic operating rooms. The disadvantage of our technique is the intraarticular working channel.
For removing intact jammed nails, universal extraction tools may be used [24]. However, they often are not available, especially when difficult nail removal is not anticipated. As in our case, these devices still may fail to remove implants [4]. Their use was precluded in our case owing to blockage of the proximal opening of the nail by the broken connection screw of the extraction bolt. Georgiadis et al. [4] described one technique for removal jammed nails after failure of a proximal extraction device. In that case, a high-speed drill with a carbide metal cutting bit was used to create a slot in the proximal end of the nail, allowing for attachment of a hook for subsequent removal. Their technique, however, requires large soft tissue dissection to expose the proximal part of the nail. Another technique for removing a jammed intramedullary nail using olive-tipped multiple guide wires was described by Weinrauch and Blakemore [23]. Guide wires were passed through the proximal nail opening into the proximal locking screw holes. With the use of multigrip pliers, they were extracted with the nail. Their technique also requires access to the inner section of the nail, which was obstructed in our case. Additional techniques for removing broken intramedullary nails include using hooks [1], a Hohmann retractor through a working channel in the lateral femoral cortex similar to a shoehorn (called the push-out technique) [11], or Ender nails [13], which must be placed beyond the distal tip of a broken nail and then hooked through the locking holes of the nail [16]. Other techniques use sigmoidoscopy forceps [12], distally impacted multiple guide wires [14, 17], or custom-made devices [6]. All these techniques were described for removal of the distal fragment of a broken nail, and none could be used in our situation with a jammed intact intramedullary nail.
The method we describe for removal of the femoral nail is easy and requires only a reamer to open the femoral canal through the knee through a small incision. Furthermore, this procedure may be applicable to many types of nails and is a reasonable alternative to nonexpandable, antegrade femoral nails that are incarcerated in a similar manner. This technique’s disadvantage is the need to open the knee where the entrance in the intercondylar region must be large enough to pass the extraction rod without causing distal femur fractures [8].
Acknowledgments
We thank Paula Coyle (St Richard’s Hospital, Chichester, United Kingdom) for assistance in editing this paper.
Footnotes
Each author certifies that he has no commercial associations (eg, consultancies, stock ownership, equity interest, etc) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that all investigations were conducted in conformity with ethical principles of research.
This work was performed at the Medical School Hannover, Hannover, Germany.
References
- 1.Acharya M, Alani A, Almedghio S. The fish hook technique of extracting broken intramedullary nails. Acta Orthop Belg. 2008;74:686–688. [PubMed] [Google Scholar]
- 2.Balcarek P, Burchhardt H, Sturmer KM. [Minimally invasive removal of a broken femoral nail] [in German] Unfallchirurg. 2005;108:419–422. doi: 10.1007/s00113-004-0871-2. [DOI] [PubMed] [Google Scholar]
- 3.Fortis AP, Dimas A, Lamprakis AA. Expandable nailing system for tibial shaft fractures. Injury. 2008;39:940–946. doi: 10.1016/j.injury.2008.01.022. [DOI] [PubMed] [Google Scholar]
- 4.Georgiadis GM, Heck BE, Ebraheim NA. Technique for removal of intramedullary nails when there is failure of the proximal extraction device: a report of three cases. J Orthop Trauma. 1997;11:130–132. doi: 10.1097/00005131-199702000-00012. [DOI] [PubMed] [Google Scholar]
- 5.Giannoudis PV, Matthews SJ, Smith RM. Removal of the retained fragment of broken solid nails by the intra-medullary route. Injury. 2001;32:407–410. doi: 10.1016/S0020-1383(00)00236-9. [DOI] [PubMed] [Google Scholar]
- 6.Gosling T, Allami M, Koenemann B, Hankemeier S, Krettek C. Minimally invasive exchange tibial nailing for a broken solid nail: case report and description of a new technique. J Orthop Trauma. 2005;19:744–747. doi: 10.1097/01.bot.0000161540.24280.34. [DOI] [PubMed] [Google Scholar]
- 7.Gosling T, Hufner T, Hankemeier S, Zelle BA, Muller-Heine A, Krettek C. Femoral nail removal should be restricted in asymptomatic patients. Clin Orthop Relat Res. 2004;423:222–226. doi: 10.1097/01.blo.0000130208.90879.67. [DOI] [PubMed] [Google Scholar]
- 8.Grimme K, Gosling T, Pape HC, Schandelmaier P, Krettek C. [Fracture of the medial femoral condyle as a complication of retrograde femoral nail removal] [in German] Unfallchirurg. 2004;107:532–536. doi: 10.1007/s00113-004-0760-8. [DOI] [PubMed] [Google Scholar]
- 9.Hankemeier S, Pape HC, Gosling T, Hufner T, Richter M, Krettek C. Improved comfort in lower limb lengthening with the intramedullary skeletal kinetic distractor: principles and preliminary clinical experiences. Arch Orthop Trauma Surg. 2004;124:129–133. doi: 10.1007/s00402-003-0625-6. [DOI] [PubMed] [Google Scholar]
- 10.Khan FA. Retrieval of a broken intramedullary femoral nail. Injury. 1992;23:129–130. doi: 10.1016/0020-1383(92)90049-X. [DOI] [PubMed] [Google Scholar]
- 11.Krettek C, Schandelmaier P, Tscherne H. Removal of a broken solid femoral nail: a simple push-out technique. A case report. J Bone Joint Surg Am. 1997;79:247–251. doi: 10.1302/0301-620X.79B1.6910. [DOI] [PubMed] [Google Scholar]
- 12.Maheshwari R, Tadross TS. Extracting broken intramedullary femoral nails. Orthopedics. 2006;29:880–881. doi: 10.3928/01477447-20061001-06. [DOI] [PubMed] [Google Scholar]
- 13.Maini L, Singh J, Agarwal P, Gautum VK, Dhal AK. Removal of broken Kuntscher’s nail: an innovative close technique. J Trauma. 2005;59:1518–1520. doi: 10.1097/01.ta.0000198352.05833.88. [DOI] [PubMed] [Google Scholar]
- 14.Middleton RG, McNab IS, Hashemi-Nejad A, Noordeen MH. Multiple guide wire technique for removal of the short distal fragment of a fractured intramedullary nail. Injury. 1995;26:531–532. doi: 10.1016/0020-1383(95)00103-G. [DOI] [PubMed] [Google Scholar]
- 15.Ozturk H, Unsaldi T, Ozdemur Z, Bulut O, Korkmaz M, Demirel H. Extreme complications of Fixion nail in treatment of long bones fractures. Arch Orthop Trauma Surg. 2008;128:301–306. doi: 10.1007/s00402-007-0458-9. [DOI] [PubMed] [Google Scholar]
- 16.Park SY, Yang KH, Yoo JH. Removal of a broken intramedullary nail with a narrow hollow. J Orthop Trauma. 2006;20:492–494. doi: 10.1097/00005131-200608000-00007. [DOI] [PubMed] [Google Scholar]
- 17.Riansuwan K, Carter C, Nercessian O. Removal of broken long gamma nail: a modified guide wires technique. J Trauma. 2008;64:517–519. doi: 10.1097/TA.0b013e3181469e0f. [DOI] [PubMed] [Google Scholar]
- 18.Ricci WM, Gallagher B, Haidukewych GJ. Intramedullary nailing of femoral shaft fractures: current concepts. J Am Acad Orthop Surg. 2009;17:296–305. doi: 10.5435/00124635-200905000-00004. [DOI] [PubMed] [Google Scholar]
- 19.Rudloff MI, Smith WR. Intramedullary nailing of the femur: current concepts concerning reaming. J Orthop Trauma. 2009;23(5 suppl):S12–S17. doi: 10.1097/BOT.0b013e31819f258a. [DOI] [PubMed] [Google Scholar]
- 20.Smith WR, Ziran B, Agudelo JF, Morgan SJ, Lahti Z, Vanderheiden T, Williams A. Expandable intramedullary nailing for tibial and femoral fractures: a preliminary analysis of perioperative complications. J Orthop Trauma. 2006;20:310–314. doi: 10.1097/00005131-200605000-00002. [DOI] [PubMed] [Google Scholar]
- 21.Steinberg EL, Keynan O, Sternheim A, Drexler M, Luger E. Treatment of diaphyseal nonunion of the femur and tibia using an expandable nailing system. Injury. 2009;40:309–314. doi: 10.1016/j.injury.2008.07.029. [DOI] [PubMed] [Google Scholar]
- 22.Steinberg EL, Luger E, Menahem A, Helfet DL. Removal of a broken distal closed section intramedullary nail: report of a case using a simple method. J Orthop Trauma. 2004;18:233–235. doi: 10.1097/00005131-200404000-00007. [DOI] [PubMed] [Google Scholar]
- 23.Weinrauch PC, Blakemore M. Extraction of intramedullary nails by proximal stacked wire technique. J Orthop Trauma. 2007;21:663–664. doi: 10.1097/BOT.0b013e3181583b34. [DOI] [PubMed] [Google Scholar]
- 24.Wood GW., 2nd Safe, rapid, and effortless femoral nail removal using a new third-generation universal femoral nail extraction tool. J Orthop Sci. 2006;11:626–627. doi: 10.1007/s00776-006-1062-5. [DOI] [PMC free article] [PubMed] [Google Scholar]