

Abstract
We coached a parent to conduct functional analysis and functional communication training (FCT) procedures in her home to reduce the destructive behavior displayed by her 2-year-old son. Descriptive assessment information and functional analysis results suggested that destructive behavior was maintained by escape from demands. After conducting a series of baseline probes, the parent implemented an FCT program to teach her son to comply with designated task requests and to mand for a break to play. Results showed that destructive behavior decreased and manding and independent task completion increased during FCT. Positive intervention outcomes were maintained for 1 year. Results are discussed with respect to developing an FCT program that is both efficient and acceptable for parents to implement in their homes.
Descriptors: Destructive behavior, functional analysis, functional communication training, parent training, preschoolers
During the last 2 decades, the use of functional communication training (FCT) for individuals who display problem behavior has been the focus of numerous investigations (see Tiger, Hanley, & Bruzek, 2008, for a recent review). FCT is a differential reinforcement procedure that teaches an individual to emit an appropriate communicative response (mand) as an alternative to engaging in problem behavior to acquire the same class of reinforcement (Carr & Durand, 1985). The first step in developing an FCT program is to conduct a functional analysis to identify the reinforcers for the individual's problem behavior (Iwata, Dorsey, Slifer, Bauman, & Richman, 1982/1994). The next step is to match the FCT procedure with the results of the functional analysis such that reinforcement is provided for manding and problem behavior is placed on extinction (Fisher et al., 1993; Wacker et al., 1990). As discussed by Tiger et al., the topography of manding selected for reinforcement should be based on considerations of the relative response effort required for the individual to acquire and emit the mand (Horner & Day, 1991; Winborn, Wacker, Richman, Asmus, & Geier, 2002), and the ability of others to recognize the mand (Durand & Carr, 1992).
The effectiveness of FCT in reducing problem behavior displayed by individuals with developmental disabilities has been demonstrated in a number of investigations (Day, Horner, & O'Neil, 1994; Durand & Carr, 1991; Durand, 1999; Fisher, Kuhn, & Thompson, 1998; Kelley, Lerman, & Van Camp, 2002). With respect to conducting FCT in home settings with parents, reductions in problem behavior following FCT have been shown to be durable over time (Derby et al., 1997; Wacker et al., 1998) and associated with generalized effects across settings, persons, and tasks (Berg, Wacker, Harding, Ganzer, & Barretto, 2007; Wacker et al., 2005). Wacker et al. (2005) evaluated the effects of FCT with 12 children who received FCT at home with their parents across different contexts (i.e., different care providers, tasks, and settings). All participants were 6 years of age or younger, were diagnosed with developmental disabilities, and displayed destructive behavior. Following a functional analysis, investigators conducted pre-treatment probes across a selection of tasks (e.g., tooth brushing, dressing, academic tasks), people (e.g., parents, relatives, teachers), and settings (e.g., home, relatives' homes, school). Treatment with FCT was then implemented with a designated person, task, and setting (e.g., mother, picking up toys, home). After destructive behavior decreased, the probes were repeated across the untrained conditions to evaluate generalized changes in problem behavior. Results showed an average reduction in destructive behavior of 93% for the initial FCT treatment, 81% across persons, 90% across settings, and 73% across tasks when compared to pre-treatment levels.
Since 1992, our research team at The University of Iowa Center for Disabilities and Development has conducted a series of research projects funded by the National Institute of Child Health and Human Development of the National Institutes of Health (Wacker & Berg, 1992; Wacker, Berg, & Harding, 1996, 2000, 2004). These projects have focused on conducting functional analyses and FCT with young children (6 years or younger) with developmental disabilities who displayed severe problem behavior such as aggression, self-injury, and property destruction. During the course of these projects, research team members, referred to as “consultants,” scheduled weekly to monthly visits to 101 participants' homes in Iowa communities. The parents in these projects served as therapists during in-home assessment and intervention procedures that were monitored for up to 3 years. Consultants provided instruction to parents, prescriptive feedback, and systematic progress evaluation. All of the direct assessment and intervention procedures were recorded on videotape for subsequent data collection and analysis. Functional analyses, completed with 95 of the children in these projects, showed that social reinforcement (e.g., parent attention, escape from parent demands) maintained destructive behavior for 85% of the children. An evaluation of intervention outcomes showed that 75% of the children who received FCT displayed a 90% or greater reduction in destructive behavior from baseline levels (Wacker, Berg, Harding, & Lee, 2008).
In this article, we provide a detailed case example of the procedures used in these projects. The purposes of this article are to (a) describe the assessment procedures and their contributions to FCT development, (b) describe the FCT program, and (c) suggest practical considerations for conducting assessment and FCT procedures with young children when working with parents in their homes.
Method
Participant and Setting
Andy was referred to our project by a school psychologist from a community-based early intervention team. Andy was 2 years and 6 months old and lived with his parents in an apartment. He was diagnosed with developmental delays and Peter's Anomaly, a genetic syndrome that resulted in blindness in his right eye. His language consisted primarily of single words, such as “no,” “please,” and “bye,” which he used independently. Although Andy could repeat words, the words “play” and “work” (which were included as mands during assessment and treatment) were not part of his usual vocabulary. At the time of his enrollment in the project, he was receiving in-home speech therapy once per week. Destructive behavior consisted of aggression toward his parents (e.g., hitting, scratching, pulling hair, head butting), property destruction (e.g., ripping books, throwing toys), and noncompliance during many activities of daily living. Andy's problem behavior also limited his parents' ability to take him into the community for activities such as shopping or visits to relatives' homes. Andy's mother, Sharon, did not work outside the home and had no previous experience or training with behavioral assessment or intervention techniques.
During the course of Andy's participation in the project, a consultant made weekly to monthly 1-hr visits to the family's apartment over a 14-month period. Andy's mother served as the therapist during all assessment and treatment procedures with coaching from the consultant. All procedures were conducted in Andy's bedroom, which contained his toys, a large chair, and a bed. During FCT, a small desk and chair were added to the bedroom furnishings. All procedures were videotaped for data collection and analysis at the Center for Disabilities and Development at The University of Iowa.
Data Collection and Response Definitions
Consultants collected data on child behavior using 6-s partial-interval recording. Aggression was defined as any behavior that could result in tissue damage to another person (e.g., hitting, kicking). Self-injury was defined as any behavior that could result in tissue damage to the person performing the behavior (e.g., head banging, hand biting). Property destruction was defined as any behavior that could result in damage to objects in the environment (e.g., throwing toys). For the purposes of this investigation, intervals of aggression, self-injury, and property destruction were combined and labeled as destructive behavior. Independent manding was defined as a request for reinforcement in the absence of a specific adult prompt. Manding included vocal communication, manual signing, or touching a word/picture card (“play”) that was attached to a microswitch. The microswitch was programmed to play a recorded message when touched (e.g., “Play, please”). Independent manding was further categorized as target manding and other manding. Target manding was defined as saying, signing, or touching the “play” word/picture card. Other manding was defined as saying or signing a response indicating that the child did not want to engage in a designated work task. Other manding typically consisted of Andy saying, “No,” and, in one session, “All done.” However, he rarely displayed other manding during baseline or FCT sessions. Toy engagement was defined as direct physical contact with a toy.
During work tasks, we measured Andy's task completion using event recording. In this procedure, the data collectors recorded each task that Andy was required to complete (e.g., “Put the red block on the blue block”). Each task was then coded as (a) completed independently (i.e., without physical assistance), (b) not completed, or (c) completed with physical assistance.
Data were collected during home visits two to three times per month for 9 months. Although we tried to schedule regular weekly visits, there were interruptions due to family illness, holidays, and hazardous driving conditions during the winter. Monthly probes were conducted for the final 3 months. During home visits, the consultant typically videotaped three to five 5-min assessment or FCT sessions. Thus, our videotaped probes sampled Andy's training and progress on a regular basis.
Interobserver Agreement
Two trained data collectors independently scored the occurrence of child behavior and task completion. Interobserver agreement on the occurrence of child behavior was calculated based on exact interval-by-interval comparisons in which the number of agreements was divided by the number of agreements plus disagreements and multiplied by 100. Interobserver agreement for child behavior was assessed for 30% of each session across all procedures and ranged from 90% to 100% (M = 96%). Interobserver agreement on the occurrence of independent task completion was calculated by dividing the number of agreements by the number of agreements plus disagreements and multiplying by 100. Interobserver agreement for task completion was assessed for 30% of each session and was 100%.
Treatment Acceptability
At the beginning of treatment and at the end of Andy's participation in the project, parent satisfaction with the intervention program was evaluated by asking Andy's mother to complete the Treatment Acceptability Rating Form-Revised (TARF-R; Reimers & Wacker, 1988). The TARF-R is a 10-item survey that asks respondents questions regarding treatment acceptability, effectiveness, and negative side effects. Respondents answer questions by selecting a Likert-type scale rating. For example, with respect to the question, “How acceptable do you find the treatment to be regarding your concerns about your child?” respondents can choose a rating of (1) Not at all acceptable to (7) Very acceptable.
Procedure and Experimental Design
Andy's assessment and intervention were conducted in four phases (see Table 1). During Phase 1, Andy's mother completed descriptive and indirect assessments to provide the consultant with general information regarding Andy's behavior and to develop hypotheses about routine events that occasioned problem behavior. She also conducted a preference assessment within a multielement design to identify preferred and non-preferred toys. In Phase 2, Andy's mother conducted a functional analysis using a multielement design to identify reinforcers that maintained Andy's destructive behavior. During Phase 3, his mother conducted a series of demand probes that provided a baseline of destructive behavior. During Phase 4, the consultant taught Andy's mother to implement an FCT program to teach Andy to complete task requests and to mand appropriately to gain reinforcement. FCT was evaluated within a reversal design (ABABABAB) in which we returned to the baseline demand probes (A) three times to demonstrate experimental control.
Table 1.
Assessment and Intervention Procedures
| Phase | Procedure | Purpose |
| 1 | Daily behavior record Interview Preference assessment Behavior Rating Scale | Develop hypotheses regarding events that occasion and maintain destructive behavior; identify preferred toys. |
| 2 | Functional analysis | Identify reinforcers for destructive behavior. |
| 3 | Baseline (extinction) demand probes | Evaluate baseline levels of behavior during target demand condition. |
| 4 | Functional communication training | Teach child to perform adaptive behavior (completing work tasks, manding) to gain reinforcement. |
Phase 1: Descriptive and Indirect Assessments
Assessments conducted in the first phase helped us to establish a working relationship with Sharon in addition to helping us develop hypotheses about Andy's behavior. The first step was to ask Sharon to complete a daily behavior record for 7 days. Sharon used this record to record the time of day and frequency of destructive behavior based on the scatterplot described by Touchette, MacDonald, and Langer (1985). She also recorded the activities that were involved when Andy displayed destructive behavior (antecedent), the type of problem behavior that he displayed (behavior), and how she responded to the behavior (consequence) based on the antecedent-behavior-consequence (ABC) assessment described by Bijou, Peterson, and Ault (1968). The descriptive assessment provided the consultants with data on events associated with Andy's destructive behavior and Sharon's current response to the behavior. During our initial contacts with families, it is common for parents to state that the child's destructive behavior occurs “all the time” without an obvious reason. However, a review of daily behavior records sometimes reveals a pattern showing that destructive behavior was associated with a particular time of day, activity, or event. These findings are presented to the parent as possible explanations for the behavior.
The next step in this phase was to ask Sharon to create a list of toys and to rate these toys with respect to Andy's preference. The objective was to create a preliminary selection of toys that might serve as reinforcers for appropriate behavior and tasks that might serve as nonpreferred activities during our assessment. To confirm that we had identified highly preferred and less preferred toys, Sharon conducted a series of free play conditions in which Andy was allowed to play with a selection of toys identified as both preferred and nonpreferred (Windsor, Piche, & Locke, 1994) while she provided noncontingent attention. The consultant used 6-s partial-interval recording to determine the percentage of intervals during which Andy engaged with each toy during each 5-min session.
The final procedure was to ask Sharon to complete the Behavior Rating Scale that we developed for our in-home investigations with preschool-aged children (Wacker, Berg, & Harding, 1996). The purpose of this scale was to obtain additional information on the severity of the child's behavior across multiple activities in the home and community. This form provides a list of 27 activities of daily living (e.g., mealtimes, brushing teeth), communication efforts (e.g., asking for assistance), social behavior (e.g., playing cooperatively with peers), and community-based activities (e.g., going shopping, going to someone else's home). Sharon was asked to rate the degree of problem behavior (e.g., major behavior problems, minor behavior problems, or no behavior problems) that Andy displayed during each of these activities. Sharon completed this scale again at the end of her participation in the study so that we could evaluate the potential generalization of treatment effects.
The overall results of these assessments provided general information on Andy's current skills and toy preferences, how he responded to different situations throughout the day, and the occurrence of major problem behavior across activities and settings. However, the assessment procedures did not clearly identify the functions of his destructive behavior. Thus, the consultant next asked Sharon to conduct a functional analysis.
Phase 2: Functional Analysis
The functional analysis was based on the procedures described by Iwata et al. (1982/1994). Conditions were counterbalanced and conducted during four visits over the course of 5 weeks. All sessions were 5 min. Given that Andy had a high activity level, his bedroom was chosen as the assessment setting. The bedroom had only one door, so it could be easily blocked if Andy tried to leave the room. The room was large enough for play activities and was well organized (e.g., all toys were on shelves) so that we could maintain control over toys. Using Andy's bedroom as an assessment setting also avoided potential damage to expensive items (e.g., television) or objects that were valuable to Andy's parents.
Before beginning the functional analysis, we explained that we would be conducting different conditions during each visit (i.e., “mixing them up”) so that we could observe situations in which Andy did well (e.g., free play) and situations in which he displayed problem behavior (e.g., demands). We also explained that by conducting a functional analysis, we could determine if Andy's problem behavior was related to obtaining a specific social outcome, such as gaining attention or escaping from demands. Thus, the results of the functional analysis could provide information that would inform the development of an individualized training program.
Prior to beginning each session, the consultant described the purpose of the condition and how Sharon should respond to Andy's behavior. We explained that we would cue her when it was time to provide reinforcement and that we would let her know when the reinforcement period had elapsed via a timer on our camcorder. In the case of the demand condition, the consultant also demonstrated how to deliver prompts using a three-step prompt sequence (see further description below).
During the free-play condition, Andy had access to his preferred toys, and his mother provided non-contingent attention. We asked Sharon to do her best to make the play time enjoyable for Andy and to provide continuous attention. We also stressed that Sharon should avoid directing Andy's play so that the free play condition did not inadvertently become a demand condition. Thus, we tried to eliminate any social motivation to engage in problem behavior. We asked Sharon to ignore minor problem behavior if it occurred and to block destructive behavior in a neutral fashion. By neutral, we meant blocking the behavior without discussion.
During the attention condition, Sharon told Andy, “I'm going to read. You play with your toys.” She then read a magazine and ignored Andy. If Andy engaged in destructive behavior, she provided him with 20 s of attention in the form of reprimands (e.g., “Don't do that!”). During the tangible condition, Sharon initially allowed Andy to play with his preferred toy. After a brief period, Sharon took away his preferred toy (electronic game) and told him, “We're going to play with blocks now” (a less preferred toy). If Andy engaged in destructive behavior, Sharon returned his preferred toy for 20 s. During the demand condition, Sharon put away all of Andy's toys except for the plastic blocks. At 30-s intervals, Sharon told Andy, “It's time to work,” and directed him to sit on the floor with her. Using a three-step prompting procedure, she instructed him to stack a plastic block. The first step was a verbal directive (“Andy, put the red block on the green block”). The second step was modeling the directive. During the third step, Sharon used hand-over-hand physical guidance to assist Andy in completing the task. If Andy engaged in destructive behavior at any time during these prompts, Sharon discontinued her instructions and removed the task materials without commenting on Andy's behavior, and Andy received a 20-s break from the work task. During the break, Andy was allowed to move around the room and interact with his mother, but he was not allowed access to toys. After 20 s, Andy was again directed to work.
Phase 3: Baseline Demand Probes
Before Sharon implemented FCT, we wanted to observe how Andy responded when she did not allow him to escape from work tasks by engaging in destructive behavior (i.e., under extinction conditions). We selected demands for our baseline because noncompliance was a major behavior concern for Sharon, and the results of the functional analysis showed that escape from demands was a primary maintaining variable for destructive behavior. As she did during the demand condition of the functional analysis, Sharon told Andy, “Time to work,” and directed him to attend to the same task (stacking blocks) on the floor. During each baseline session, Sharon gave Andy instructions to complete a specific task (“Andy, put the red block on the blue block”). The presentation of a specific task constituted one trial. Sharon presented a series of six to nine tasks (M = 7) during each 5-min baseline session. Thus, Andy was asked to stack six to nine blocks during each of the four baseline demand sessions. If Andy performed the task, Sharon praised him. If Andy did not perform the task within 30 s, the trial for that task request ended, the task was scored as “not completed,” and Sharon presented a new task (“Put the yellow block on the green block”). The microswitch and “play” picture/word card were not present during the initial baseline demand condition or during any repeated baseline sessions. Sharon was instructed to ignore vocal manding and mild problem behavior and to block destructive behavior in a neutral fashion.
Phase 4: Functional Communication Training
After Sharon completed the assessment procedures, the consultant reviewed the results with Sharon. The descriptive assessment provided information suggesting that demands during Andy's daily routine were associated with destructive behavior. The preference assessment identified preferred toys that could be used as reinforcers and less preferred toys that could be used as training tasks. The functional analysis demonstrated that destructive behavior was maintained by escape from demands. Finally, the baseline probes showed that destructive behavior persisted under brief periods of extinction. This information was used to develop an FCT program that was based on behavioral function and included age-appropriate activities in Andy's normal environment.
The FCT program contained multiple implementation components. Our objectives were to make the procedures easy for Sharon and to enable Andy to obtain reinforcement efficiently. As a first step, we structured the environment so that visual cues for desired behaviors (going to work, task completion, manding) were as clear as possible. We next conducted an initial training session with Sharon and encouraged her to begin practicing the FCT program throughout the week. During weekly visits, the consultant provided feedback to Sharon while videotaping FCT sessions, shared graphic representations of Andy's performance, and answered Sharon's questions. An outline of the activities we conducted during a typical visit is provided in Table 2.
Table 2.
Guidelines for Training Parents During Home Visits
|
Visual cues.
A “work area” was created in the bedroom by bringing in a small desk and chair that were already present in the home. All task demands were presented when Andy was seated at the desk; thus, it served as a visual prompt that work was required. The desk and chair arrangement also enabled Sharon to manage Andy physically if he became noncompliant and attempted to escape from the work task. In contrast, the floor and bed served as a “play area” where Andy had access to his preferred toys during work breaks.
We chose “play” as a mand that Andy could use to request a break from work tasks. We created a “play” picture/word card from BoardMaker™. The card was attached to the touch plate of a BIGmack™ microswitch. The microswitch was programmed to play the recorded message, “Play, please,” when touched. We also provided Sharon with a “work” picture/word card. Sharon used this card to signal Andy that it was “time to work” and placed the card on his desk during work tasks.
Parent training.
We provided Sharon with step-by-step written instructions on how to conduct the FCT program. Sharon then watched a videotaped recording that showed a mother conducting assessment and FCT procedures with her young son. The family in the tape had previously participated in our in-home project and had given us consent to share their experience with other families and professionals. Our goal was for Sharon to have realistic expectations regarding how Andy might respond to the FCT program. The tape showed the child displaying destructive behavior during assessment procedures and early FCT sessions. Thus, it provided a realistic example of how another child behaved and how his mother responded to the behavior. It also showed the child's progress as he learned to follow his mother's instructions and to communicate appropriately during FCT.
After reviewing the FCT program with Sharon, the consultant modeled each step with Andy. Sharon then implemented the program while receiving prompts and feedback from the consultant. We asked Sharon to practice the FCT program for 10 to 15 min on a daily basis. We recommended practicing at a time that was convenient for her and relatively free from interruptions so that she could give Andy her full attention. The consultant visited on a weekly basis to videotape Sharon conducting FCT sessions with Andy. These visits enabled the consultant to provide feedback on Sharon's treatment implementation and to share updated graphic data that illustrated Andy's progress.
FCT procedure.
At the beginning of each 5-min session, Sharon involved Andy in a play activity with his preferred toys. The purpose of this step was to set the occasion for toys and parent attention to function as reinforcement for appropriate behavior. We wanted to increase Andy's motivation to complete his work and to mand so that he could return to playing with his toys.
After a few minutes of play, Sharon showed Andy the work card and told him, “Time to work. Please sit at your desk.” This step can be challenging because children often resist going to their work area early in treatment, and the parent may have to use physical guidance to direct the child to the seat. If this occurs, we tell the parent to remind the child, “Work first, then play.” The parent then uses simple language (“Stand, please,” “Walk, please,” “Sit, please”) for each step to be completed and provides physical assistance as needed to guide the child to the seat. Each time the child performs one of these actions appropriately, the parent provides praise (e.g., “Thank you. Good walking!”).
After Andy was seated, Sharon presented his work task. The initial objective was for Andy to stack one block as instructed (e.g., “Put the blue block on the yellow block.”) and then mand for a break. Although Andy was capable of stacking more than one block at a time, we wanted to make this task easy to perform at the beginning and provide a high amount and quality of reinforcement (praise, break from work, toys) for appropriate behavior. During the initial treatment sessions (FCT [2]), Andy was required to stack a total of two blocks (one block per trial) and earned two opportunities to mand for a break. Over time, we increased the amount of work that Andy was required to complete before he had an opportunity to mand for a break. Eventually, his task requirements were increased to stacking four blocks (two blocks per trial) and eight blocks (four blocks per trial) during each session. Thus, as task requirements increased, Andy still had the opportunity to complete his work and to mand for a break twice during each training session.
Sharon modeled the task while giving instructions and then told Andy, “Now you do it.” If Andy completed the task independently (without physical assistance) and displayed appropriate behavior, he received praise. Sharon then presented the microswitch and asked Andy if he wanted to do more work or play. Initially, Sharon told Andy that if he wanted to play, he needed to “Say ‘play’ or touch the switch.” This specific instruction was faded over time as Andy learned to say, “play,” and touch the switch independently. If Andy said “work,” she gave him another block to stack and again provided him with an opportunity to take a play break. If Andy refused to mand or engaged in problem behavior, his opportunity to take a break ended, and he was given another block to stack. If Andy said, “play,” touched the microswitch, or emitted any other appropriate communication indicating he wanted to discontinue work and engage in a different activity (e.g., “Done”), the “work” card and blocks were removed from the desk and he received a 1-min play break. For the mand to be reinforced, it had to be performed in an appropriate fashion. For example, if Andy hit the micro- switch forcefully, his mother said, “Too hard. Touch it nicely.” Sharon used physical guidance to demonstrate the appropriate way to touch the microswitch and then gave Andy another opportunity to mand. Similarly, Andy was corrected if he yelled the word “play” (e.g., “That's too loud. Say it nicely please.”) If destructive behavior occurred concurrently with manding, Sharon identified the behavior (“No hitting. Back to work.”), and Andy was required to complete another task and mand again. Thus, each trial was composed of a two-step chain: Completing the required task independently produced the card/microswitch, and manding appropriately produced a break with toys and attention.
During Andy's break, he was allowed to play with his preferred toys. Sharon tried to make his break enjoyable. She typically ignored or redirected mild problem behavior during the break. However, if he became too rough and engaged in destructive behavior, she ended his break and required him to return to his desk for another work task.
Reversal to baseline condition.
After FCT was initiated, we returned to the baseline condition three times. The first reversal was conducted after 1 month (following 9 FCT sessions). The second reversal was conducted after 2 months (following an additional 13 FCT sessions). The third and final reversal was conducted after 7 months (following an additional 15 FCT sessions). We conducted three baseline sessions during each visit and did not evaluate FCT until the following visit. Before we conducted the baseline conditions, we told Sharon that we wanted to observe Andy's behavior during demands when FCT was not in place. We explained that if Andy's behavior worsened during the baseline sessions but improved when FCT was implemented again, this would demonstrate that her efforts in conducting the training program were responsible for the changes in Andy's behavior. These results would also indicate the extent to which Andy still needed the structure of the FCT program to complete the designated task.
Results
Descriptive Assessment and Preference Assessment
One week after our initial visit to the home, we reviewed the daily behavior records that Sharon completed. Sharon recorded 37 incidents of problem behavior over 7 days. Of these 37 incidents, 21 (57%) were associated with antecedent events that we interpreted as demand conditions, such as meals, getting dressed, diaper changing, and medical procedures. The remaining antecedent events were associated with play activities (30%) or activities in the community (13%), such as “visiting Grandma.” Table 3 shows three examples from Sharon's records and a possible hypothesis for the function of Andy's behavior during each incident. Overall, Andy received varied consequences for problem behavior. Sometimes Sharon ignored problem behavior, and sometimes she provided possible positive and negative reinforcers. Thus, the function of his behavior remained unclear.
Table 3.
Examples From Parent's Daily Behavior Record and Our Hypotheses About Function
| Antecedent | Behavior | Consequence | Hypothesis |
| Dressing him | Pulled my hair | Told him “No.” Tried to distract him with a toy. Continued to dress him. | Escape |
| He was playing in his room. | Got toy phone and started swinging it around, hitting furniture and door | I took the phone away. He got mad and started hitting, so I put him in high chair. | Tangible |
| He was playing in his room. | Started banging his door | Ignored it. He eventually stopped. | Attention |
Results of the preference assessment are displayed in Figure 1. Andy's engagement with the electronic game averaged 41% across sessions, whereas wooden blocks, books, and plastic blocks averaged 27%, less than 1%, and 0%, respectively. These results showed that the electronic game was a highly preferred toy. The least preferred toys were books and interlocking plastic blocks.
Figure 1.
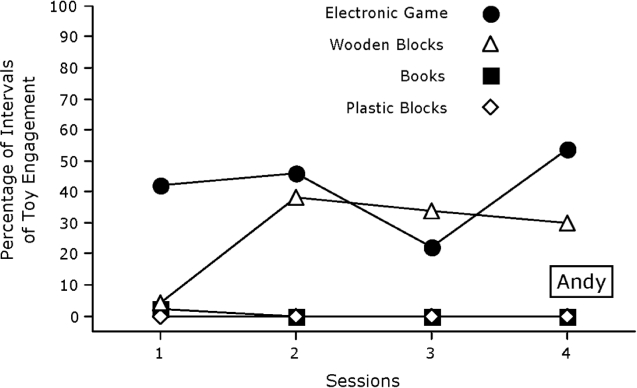
Percentage of intervals of toy engagement during the preference assessment.
Functional Analysis
The results of Andy's functional analysis are shown in Figure 2. The percentage of intervals of destructive behavior in the demand condition was consistently elevated across all three sessions and averaged 27%. In comparison, destructive behavior during the attention, tangible, and free play conditions averaged 6%, 5%, and 3%, respectively. These results suggested that there was a functional relation between escape from demands and the occurrence of destructive behavior. During the demand condition, Andy avoided completing tasks by engaging in aggression (e.g., pushing, hitting, scratching) and throwing the task materials. Andy's behavior during the demand condition was similar to his mother's reports of noncompliance and destructive behavior during various activities throughout the day.
Figure 2.
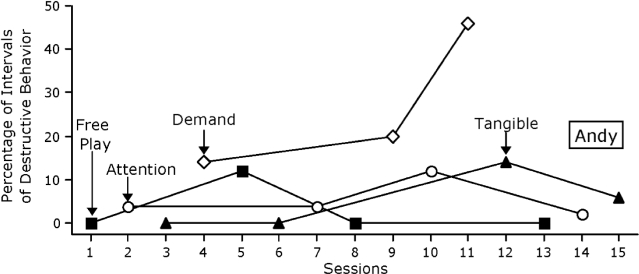
Percentage of intervals of destructive behavior during the functional analysis.
The results of the functional analysis demonstrated that Andy's destructive behavior was maintained by social reinforcement in the form of escape from demands. Equally important, serving as the therapist during the functional analysis was an educational experience for Andy's mother. Sharon was able to experience in a direct and systematic fashion how her behavior affected Andy's behavior. For example, she could see how quickly Andy calmed down when he was allowed to escape from a demand. The graphic representation of the functional analysis further illustrated that Andy's destructive behavior was related to escape from demands. Sharon was now convinced that allowing Andy to escape by engaging in destructive behavior would make his behavior worse over time. She was also concerned that she would have even more difficulty controlling him as he became bigger and stronger.
Functional Communication Training
Figure 3 shows the results of Andy's treatment with FCT during a 12-month period. The top panel shows the percentage of intervals of destructive behavior during baseline probes and FCT conditions. The middle panel shows the percentage of intervals of independent target manding and other manding, and the bottom panel shows the percentage of independent task completion. During the initial baseline probes (sessions 1 to 4), Andy displayed destructive behavior during all four sessions (M = 23%). He did not display manding, and his independent task completion was low for three of the four sessions. When FCT was first implemented (sessions 5 and 6), Andy continued to display destructive behavior. However, within 1 week, his behavior had improved substantially (session 7). His destructive behavior remained at low levels, he manded independently for breaks by saying, “play,” and/or by touching the microswitch, and he completed all of his work independently. Given his improved performance, we increased the amount of work he was required to complete from stacking two blocks per session to stacking four blocks during session 12. This increase in demands did not have a negative effect on Andy's performance.
Figure 3.
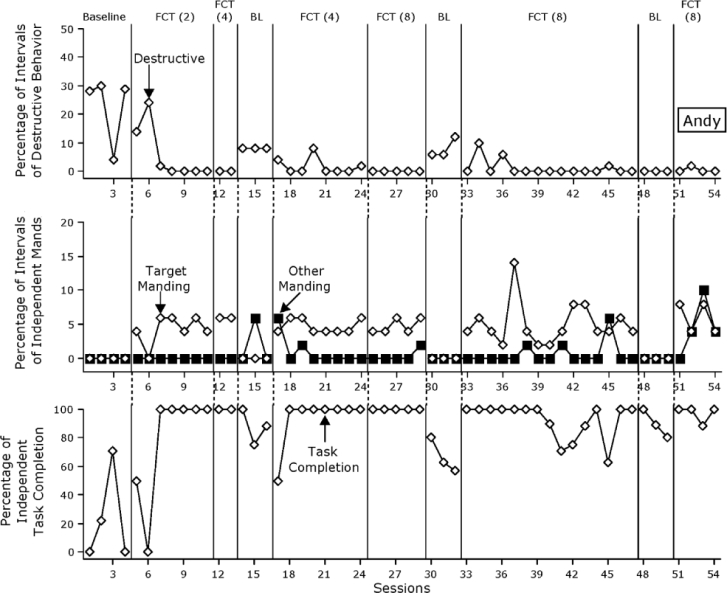
Percentage of intervals of destructive behavior (top panel) and independent target manding and other manding (middle panel) and percentage of independent task completion (bottom panel) during functional communication training and baseline conditions. BL = baseline, FCT = functional communication training.
After 1 month, we repeated our baseline probes (sessions 14 to16). The purpose of returning to the baseline condition was to demonstrate that Andy's improved behavior was due to the FCT program rather than to another factor. During the baseline probes, Andy's destructive behavior increased and manding decreased. He also displayed a slight decrease in independent task completion. These results suggested that improvements in Andy's behavior during the work task were related to the FCT program. To confirm this hypothesis, we returned to the FCT program during session 17. Andy's destructive behavior decreased and his task completion increased within a few sessions.
Given Andy's success with stacking four blocks per training session, we increased the amount of work to eight blocks during session 25 (FCT [8]), 2 months after implementing FCT. This was greater than the average amount of work that we presented during the baseline sessions (M = 7), but Andy continued to do well. This was an important goal. Within 2 months, Andy had gone from high levels of destructive behavior, no manding, and limited task completion to low levels of destructive behavior, consistent manding, and 100% task completion across multiple sessions. We continued to visit Andy's home and collect data to evaluate whether his response to the FCT program would continue over time.
During sessions 30 to 32, we again returned to the baseline condition after 2 months of FCT. Removing the FCT program resulted in an increase in destructive behavior and a decrease in manding and independent task completion. When we returned to FCT (session 33), manding and task completion improved immediately, and destructive behavior decreased within a few sessions. This extension to our reversal design (ABABAB) provided additional evidence that changes in Andy's behavior were due to FCT. However, Andy's behavior was not always perfect. As indicated in the bottom panel (e.g., sessions 41 to 45), Andy sometimes resisted doing his work independently, and his mother needed to provide hand-over-hand assistance.
During sessions 48 to 50, we again returned to the baseline condition. At this point, we had been evaluating Andy's response to FCT for 7 months. During these baseline probes, we saw a change in some of Andy's behavior compared to previous returns to baseline. Andy displayed no destructive behavior and his independent task completion remained relatively high (80% or higher). Consistent with previous baseline probes, Andy did not emit any target mands. Thus, it appeared that destructive behavior had now been replaced with independent task completion.
We continued to evaluate Andy's behavior during FCT within our reversal design (ABABABAB). Sessions 51 to 54 were conducted during visits that were 4 to 6 weeks apart. Andy continued to display zero to near-zero levels of destructive behavior, appropriate manding, and high levels of independent task completion. These data provided some evidence that his continued performance was not related to the frequency of visits from the consultant.
Behavior Rating Scale
Results of the initial Behavior Rating Scale showed that Sharon identified 8 activities in which major behavior problems occurred and 13 activities in which minor behavior problems occurred. Andy did not have exposure to six activities (e.g., going to church). Major problem behaviors were associated with picking up toys, getting dressed and undressed, brushing teeth, working with adults, going to someone else's home, and asking for items or assistance appropriately. Results of the Behavior Rating Scale that Sharon completed at the end of the investigation showed only one activity that was associated with major problem behaviors (entertains self when alone). All activities that were rated as being associated with major problem behavior before treatment were rated as being associated with minor problem behavior or no problem behavior at the end of treatment.
Treatment Acceptability
One week after implementing FCT, we asked Sharon to complete the TARF-R (Reimers & Wacker, 1988). With respect to the question, “How acceptable do you find the treatment to be regarding your concerns about your child?” Sharon chose a rating of 6 (7 = Very acceptable). With regard to “How effective is this treatment likely to be for your child?” Sharon's rating on this question was also 6 (7 = Very effective). Thus, the intervention approach was rated as acceptable and effective. After conducting our final FCT probe, we asked Sharon to complete the TARF-R a second time. Sharon again rated the questions on treatment acceptability and effectiveness as 6. Thus, Sharon continued to rate FCT as an acceptable and effective approach to treating Andy's behavior problems.
Conclusions and Guidelines for Practitioners
This case example provided a description of the procedures that we used during in-home assessment and intervention procedures with a young child. The functional analysis showed that the child's destructive behavior appeared to be related to escape from parent demands. Based on this result, the parent was taught to implement an FCT program to teach her child to follow directions and to mand for a break. Results showed that destructive behavior decreased during FCT, whereas appropriate communication and task completion increased. These results were durable over time. Similar outcomes have been reported with many young children (Wacker et al., 1998; Wacker et al., 2005), demonstrating that parents can be effective therapists with coaching from behavioral consultants.
The results of this study suggested a number of guidelines for conducting FCT procedures in home settings (see Table 4). Although we found the descriptive assessment to be a helpful step in gathering information regarding Andy's behavior across different activities, there were some limitations to this procedure. The data from the descriptive assessment indicated a correlation between the presentation of demands during Andy's daily routine and his problem behavior, but the consequences that maintained his problem behavior were not clear. Thus, one suggestion for practitioners is to use the descriptive assessment information to formulate hypotheses that can be tested directly via a functional analysis (Mace & Lalli, 1991).
Table 4.
Guidelines for Conducting FCT in Home Settings
|
Conducting a functional analysis often provides a more definitive demonstration of the consequences that are maintaining the child's problem behavior. In this case example, the functional analysis enabled Sharon to experience directly how her behavior affected Andy's behavior. As suggested by the descriptive assessment, results of the functional analysis showed that Andy's destructive behavior was primarily related to escape from demands. Demand situations were not the only time that Andy engaged in problem behavior, but the frequency and severity of his behavior during demands made this context his mother's first choice for intervention.
When the function of the child's behavior has been determined, it is important to develop an FCT program that “matches” this function (Iwata et al., 1994). It is also critical to design a program that is relatively easy to implement and acceptable to the parent. During Andy's FCT program, we focused our intervention probes on his performance of a simple target task (stacking blocks). The results of our baseline assessment demonstrated that this type of demand occasioned destructive behavior. Stacking blocks, per se, was not selected for its value as an educational outcome. It was a task that Andy could do but did not want to do. The same could be said of other tasks and activities that were part of his regular routine at home. An advantage of stacking blocks as a work task in this case was that it represented a relatively simple, discrete task that could be easily presented and measured. Our objective was to provide a specific FCT program based directly on assessment results that Sharon could implement successfully.
Although the extended evaluation of Andy's behavior during FCT was limited to demands with a specified task, Sharon reported improved behavior across settings and tasks in the Behavior Rating Scale. This outcome was consistent with the generalization obtained in our previous studies (e.g., Wacker et al., 2005). However, we did not directly observe this improved behavior, as the focus of the current research project was the evaluation of long-term maintenance (Wacker, Berg, & Harding, 2004). We do not assume that generalization will occur. We recommend that practitioners collect baseline data on behavior in two to three additional settings or situations prior to beginning FCT. When FCT is completed in the training setting, practitioners should probe these additional settings or situations to determine if generalization has occurred. If additional FCT programs are needed, practitioners and care providers may observe substantially reduced training time in these additional settings or situations (Stokes & Baer, 1977).
The use of response chaining is another consideration with respect to developing an FCT program for behavior maintained by escape (Lalli, Casey, & Kates, 1995). At the beginning of FCT, Andy was required to do very little work (one task) during each trial before gaining the opportunity to mand for a break. In this respect, Andy was able to gain a considerable amount of reinforcement initially for very little effort. However, most caregivers or teachers will have higher expectations for the amount of work to be completed. Similar to Lalli et al., we gradually increased the amount of work that Andy was required to complete independently before he earned the opportunity to request a break.
Conducting reversals to baseline enabled Sharon to observe how making changes in the way that she structured Andy's environment, presented tasks, and responded to Andy influenced both his destructive and appropriate behavior throughout treatment. These results appeared to improve Sharon's confidence in how she managed Andy's behavior. After conducting FCT, Sharon learned to provide instructions and deliver consequences in a clear and consistent fashion (e.g., “If you pick up your toys, you may watch a video.”). Sharon also incorporated picture schedules into Andy's daily routine.
Although Andy showed initial improvement during FCT, his destructive behavior reoccurred from time to time during the course of our visits. This matched Sharon's reports that he had “good days and bad days” when she worked with him during the week. Consultants should reassure parents that such day-to-day variability in responding is not uncommon and may not represent a failure on their part. However, variability in child behavior may, in some cases, indicate how accurately the parent is implementing intervention components. One limitation of the current study is that we did not conduct an analysis of treatment integrity when the consultant was not present. Future investigations might have parents videotape their training sessions when the consultant is absent to evaluate treatment integrity.
With regard to manding, Andy learned to say, “play,” and to touch the card/microswitch as an appropriate means of obtaining a break from his work task during FCT sessions. It is notable that Andy did not emit the target mand, “play,” vocally during repeated baseline sessions when the card/microswitch and scheduled reinforcement for completing a work task was not available. One hypothesis is that manding for a break from work tasks came under stimulus control of the presence of the card/microswitch. We did not code the occurrence of vocal manding and touching the card/microswitch as separate manding topographies. However, research has suggested that children may develop preferences for a specific topography of manding when multiple manding topographies are reinforced during FCT (Harding et al., 2009).
Our goal in this article was to provide an example of the assessment and treatment procedures that we have used with many parents in home settings. On a practical level, we acknowledge that many practitioners may not have the resources to conduct the extended analyses and the detailed data collection procedures that we have described. However, even relatively modest data collection techniques and brief analyses may reveal important relations that inform treatment strategies and validate treatment effects.
Parents vary substantially in their experience and educational backgrounds. Some parents are able to perform procedures quickly and with good integrity with relatively little explanation, demonstration, or prescriptive feedback. Other parents may require repeated instruction and support. Ultimately, we believe that involving parents directly as collaborators in the assessment and treatment process is a productive approach to improving their understanding of their children's behavior, enhancing their skill as therapists, and promoting the acceptability of intervention recommendations.
Footnotes
This investigation was supported by Grant R01 HD029402 from the National Institute of Child Health and Human Development of the National Institutes of health.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Child Health and Human Development or the National Institutes of Health. The authors express their appreciation to the family who participated in this investigation and to Agnes DeRaad for her assistance with manuscript preparation.
Danielle Dolezal is now at the Kennedy Krieger Institute at Johns Hopkins University.
Contributor Information
Jay W Harding, The University of Iowa
David P Wacker, The University of Iowa
Wendy K Berg, The University of Iowa
John F Lee, The University of Iowa
Danielle Dolezal, The University of Iowa
References
- Berg W. K, Wacker D. P, Harding J. W, Ganzer J, Barretto A. An evaluation of multiple dependent variables across distinct classes of antecedent stimuli pre and post functional communication training. Journal of Early and Intensive Behavioral Intervention. 2007;34(4)(1):305–333. [Google Scholar]
- Bijou S. W, Peterson R. F, Ault M. H. A method to integrate descriptive and experimental field studies at the level of data and empirical concepts. Journal of Applied Behavior Analysis. 1968;1:175–191. doi: 10.1901/jaba.1968.1-175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr E. G, Durand V. M. Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis. 1985;18:111–126. doi: 10.1901/jaba.1985.18-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Day H. M, Horner R. H, O'Neill R. E. Multiple functions of problem behaviors: Assessment and intervention. Journal of Applied Behavior Analysis. 1994;27:279–289. doi: 10.1901/jaba.1994.27-279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Derby K. M, Wacker D. P, Berg W, DeRaad A, Ulrich S, Asmus J, et al. The long-term effects of functional communication training in home settings. Journal of Applied Behavior Analysis. 1997;30:507–531. doi: 10.1901/jaba.1997.30-507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durand V. M. Functional communication training using assistive devices: Recruiting natural communities of reinforcement. Journal of Applied Behavior Analysis. 1999;32:247–267. doi: 10.1901/jaba.1999.32-247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durand V. M, Carr E. G. Functional communication training to reduce challenging behavior: Maintenance and application in new settings. Journal of Applied Behavior Analysis. 1991;24:251–264. doi: 10.1901/jaba.1991.24-251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durand V. M, Carr E. G. An analysis of maintenance following functional communication training. Journal of Applied Behavior Analysis. 1992;25:777–794. doi: 10.1901/jaba.1992.25-777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher W. W, Kuhn D. E, Thompson R. H. Establishing discriminative control of responding using functional and alternative reinforcers during functional communication training. Journal of Applied Behavior Analysis. 1998;31:543–560. doi: 10.1901/jaba.1998.31-543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher W. W, Piazza C. C, Cataldo M, Harrell R, Jefferson G, Conner R. Functional communication training with and without extinction and punishment. Journal of Applied Behavior Analysis. 1993;26:23–26. doi: 10.1901/jaba.1993.26-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harding J. W, Wacker D. P, Berg W. K, Winborn-Kemmerer L, Lee J. F, Ibrahimovic M. Analysis of multiple manding topographies during functional communication training. Education and Treatment of Children. 2009;32:21–36. doi: 10.1353/etc.0.0045. NIHMSID # 95534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horner R. H, Day H. M. The effects of response efficiencies on functionally equivalent competing behaviors. Journal of Applied Behavior Analysis. 1991;24:719–732. doi: 10.1901/jaba.1991.24-719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwata B. A, Dorsey M. F, Slifer K. J, Bauman K. E, Richman G. S. Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis. 1994;27:197–209. doi: 10.1901/jaba.1994.27-197. (Reprinted from Analysis and Intervention in Developmental Disabilities, 2, 3–20, 1982) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iwata B. A, Pace G. M, Dorsey M. F, Zarcone J. R, Vollmer T. R, Smith R. G, et al. The functions of self-injurious behavior: An experimental-epidemiological analysis. Journal of Applied Behavior Analysis. 1994;27:215–240. doi: 10.1901/jaba.1994.27-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelley M. E, Lerman D. C, Van Camp C. M. The effects of competing reinforcement schedules on the acquisition of functional communication. Journal of Applied Behavior Analysis. 2002;35:59–63. doi: 10.1901/jaba.2002.35-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lalli J. S, Casey S, Kates K. Reducing escape behavior and increasing task completion with functional communication training, extinction, and response chaining. Journal of Applied Behavior Analysis. 1995;28:261–268. doi: 10.1901/jaba.1995.28-261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mace F. C, Lalli J. S. Linking descriptive and experimental analyses in the treatment of bizarre speech. Journal of Applied Behavior Analysis. 1991;24:553–562. doi: 10.1901/jaba.1991.24-553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reimers T, Wacker D. Parents' ratings of the acceptability of behavioral treatment recommendations made in an outpatient clinic: A preliminary analysis of the influence of treatment effectiveness. Behavioral Disorders. 1988;14:7–15. [Google Scholar]
- Stokes T. F, Baer D. M. An implicit technology of generalization. Journal of Applied Behavior Analysis. 1977;10:349–367. doi: 10.1901/jaba.1977.10-349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tiger J. H, Hanley G. P, Bruzek J. Functional communication training: A review and practical guide. Behavior Analysis in Practice. 2008;1:16–23. doi: 10.1007/BF03391716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Touchette P. E, MacDonald R. F, Langer S. N. A scatterplot for identifying stimulus control of problem behavior. Journal of Applied Behavior Analysis. 1985;18:343–351. doi: 10.1901/jaba.1985.18-343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wacker D. P, Berg W. K. Inducing reciprocal parent/child interactions. Rockville, MD: Department of Health and Human Services, National Institute of Child and Human Development; 1992. [Google Scholar]
- Wacker D. P, Berg W. K, Harding J. W. Promoting stimulus generalization with young children. Rockville, MD: Department of Health and Human Services, National Institute of Child and Human Development; 1996. [Google Scholar]
- Wacker D. P, Berg W. K, Harding J. W. Functional communication training augmented with choices. Rockville, MD: Department of Health and Human Services, National Institute of Child and Human Development; 2000. [Google Scholar]
- Wacker D. P, Berg W. K, Harding J. W. Maintenance effects of functional communication training. Rockville, MD: Department of Health and Human Services, National Institute of Child and Human Development; 2004. [Google Scholar]
- Wacker D. P, Berg W. K, Harding J. W, Barretto A, Rankin B, Ganzer J. Treatment effectiveness, stimulus generalization, and parent acceptability of functional communication training. Educational Psychology. 2005;25:231–254. [Google Scholar]
- Wacker D. P, Berg W. K, Harding J. W, Derby K. M, Asmus J. M, Healy A. Evaluation and long-term treatment of aberrant behavior displayed by young children with disabilities. Journal of Developmental and Behavioral Pediatrics. 1998;19:26–32. doi: 10.1097/00004703-199808000-00004. [DOI] [PubMed] [Google Scholar]
- Wacker D. P, Berg W. K, Harding J. W, Lee J. F. An evaluation of behavioral persistence following long-term treatment of destructive behavior with functional communication training. 2008, December. Invited presentation for the Maryland Association for Behavior Analysis, Baltimore, MD.
- Wacker D. P, Steege M. W, Northup J, Sasso G, Berg W, Reimers T, et al. A component analysis of functional communication training across three topographies of severe behavior problems. Journal of Applied Behavior Analysis. 1990;23:417–429. doi: 10.1901/jaba.1990.23-417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winborn L, Wacker D. P, Richman D. M, Asmus J, Geier D. Assessment of mand selection for functional communication training packages. Journal of Applied Behavior Analysis. 2002;35:295–298. doi: 10.1901/jaba.2002.35-295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Windsor J, Piché L. M, Locke P. A. Preference testing: A comparison of two presentation methods. Research in Developmental Disabilities. 1994;15:439–455. doi: 10.1016/0891-4222(94)90028-0. [DOI] [PubMed] [Google Scholar]