

Abstract
This cross-sectional study explored associations among (a) age of sexual debut, (b) drug abuse, and (c) sexual risk behaviors among an urban community based sample of 158 predominantly immigrant, Latina adults. Time in the United States and having a mother who used drugs during the participants' childhood or adolescence were significantly related to age of sexual debut. In turn, younger ages of sexual debut were associated with drug abuse and more sexual risk behaviors (greater number of sexual partners, more frequent alcohol and drug use before or during sex, greater levels of intoxication from alcohol or drugs during sex). Implications for HIV/AIDS and drug abuse clinical services and future research with U.S. Latina populations are discussed.
Keywords: Sexual debut, immigrant, Latina, Hispanic, HIV risk, drug abuse
U.S. Latinas are affected disproportionately by HIV/AIDS. The rate of existing AIDS cases among Latinas is six times higher than the corresponding rate among non- Latina, White women (CDC, 2007). Engagement in sexual activity at an early age is a potential contributor to this disparity. Latino adolescents report a high prevalence rate of sexual intercourse (CDC, 2008). Such early sexual activity increases an individual's chance of exposure to HIV (Dolcini et al., 1993).
This study uses retrospective responses from adult Latinas to determine if age of sexual debut is related to (a) length of time in the U.S. and (b) having a mother who abused drugs during one's youth. Latinas who report longer lengths of time in the U.S. are hypothesized to indicate earlier sexual debut. Latinas with drug abusing mothers also are hypothesized to report younger ages of sexual debut. Age of sexual debut is expected to be associated with adult drug abuse and HIV sexual risk behaviors. Latinas who report younger ages of sexual debut are hypothesized to (a) be drug abusers as adults, (b) report more sexual partners, (c) report more use of substances before sex, and (d) indicate more intoxication from alcohol or drugs before sex. The remainder of this section introduces epidemiological and sociocultural literature that informs the hypotheses of this study.
Correlates of Sexual Debut
Latino cultural norms, such as gender inequality and power imbalance within romantic relationships, influence the onset of sexual activity (Gilliam, Berlin, Kozloski, Hernandez, & Grundy, 2007). Latina immigrant youth often struggle with balancing cultural norms (e.g., forbidding premarital sex) with conflicting sexual expectations espoused by U.S. born peers (Raffaelli & Ontai, 2001). The cultural expectation to be submissive is theorized to impair healthy sexual decision-making (Weeks, Schensul, Williams, Singer, & Grier, 1995). Other cultural factors, such as nativity and acculturation, impact sexual initiation and risk among Latinas (Afable-Munsuz & Brindis, 2006). Highly acculturated Latina youth are more likely to be sexually active at an early age and engage in sexual risk behaviors (Gilliam et al., 2007). Decreases in familism (a cultural value that emphasizes interdependence among family members for support, emotional connectedness, familial honor, loyalty, and solidarity; Muñoz-Laboy, 2008) due to acculturation is theorized to lead to higher levels of sexual activity among acculturated Latinas (Afable-Munsuz & Brindis, 2006). Given the influence of these cultural dynamics, we examined associations between length of time lived in the U.S. (as a proxy for acculturation) and age of sexual debut.
Several theories attempt to explain intergenerational transmission of health risk behaviors (Wilder & Watt, 2002). Social learning theory suggests that when parents model problem behaviors, their children adopt similar behaviors (Lau, Quadrel, & Hartman, 1990). Social development theory (Catalano & Hawkins, 1996) emphasizes the importance of a close relationship with a healthy (e.g., non-drug using) parent to facilitate healthy child development. Given the implications of such theories, mothers who abused drugs during their daughters' lifetime were expected to model health risk behaviors in the presence of their daughters, and experience more relationship problems with their daughters, leading to daughters' early sexual debut.
Consequences of Early Sexual Debut
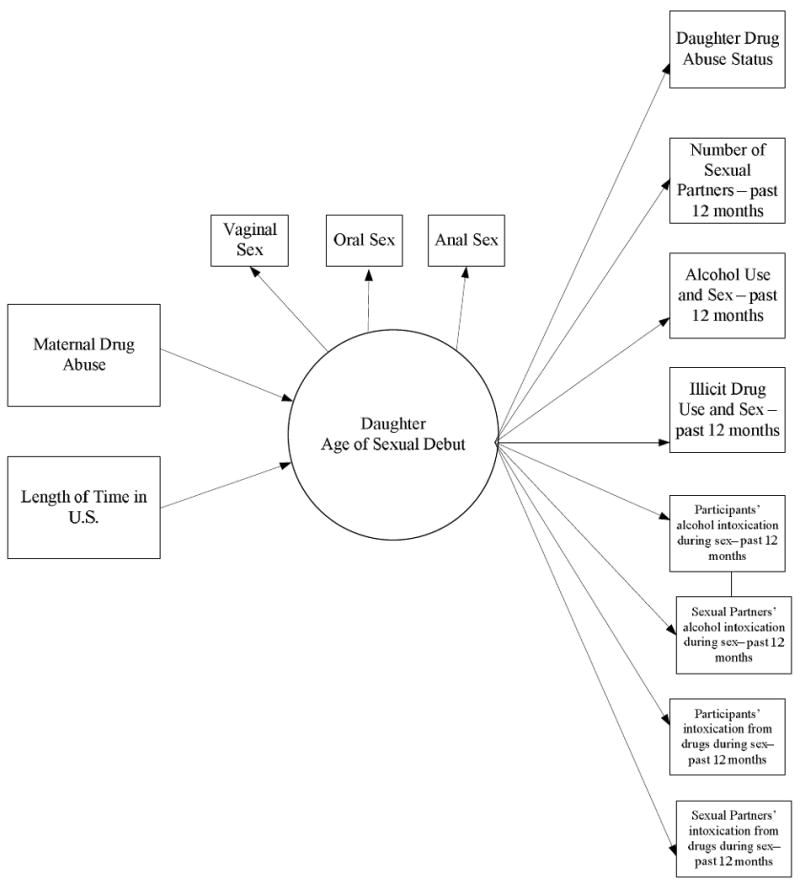
Early sexual debut has been associated with drug use and sexual risk behaviors, including number of sexual partners and sexual activity under the influence of substances (Sandfort, Orr, Hirsch, & Santelli, 2008). The extent to which these relationships continue into adulthood among U.S. Latinas has been sparsely studied. Furthermore, syndemic theory, which to describes the intertwined nature health crises in marginalized communities (e.g., substance abuse, violence, and AIDS), posits that interconnections between drug use, HIV and poverty, interact to lower the overall health profiles of ethnic minorities in the U.S. (Singer, 1996). Thus, this study not only examines correlates of age of sexual debut, but also accounts for interconnections between age of sexual debut and adult drug abuse and sexual risk (See Figure 1).
Figure 1. Conceptual model.
Methods
Participants and Procedures
The study was approved by the Institutional Review Board at a southeastern university in the U.S. Participants were 158 Latina mother-daughter dyads (total N = 316 participants) living in an urban area (Miami, Florida). Assessments were conducted in Spanish (65%) or English (35%) by eleven trained female interviewers.
The mean age of daughters was 27.21 years (SD = 9.21). The mean age of mothers was 52.30 years (SD = 9.87). Most mothers were born outside of the U.S. (84.2%, n = 133). Most mothers emigrated to the U.S. from Cuba (n = 49, 31%) and 18.4 % from Colombia (n = 29). Approximately half (46%) of daughters (n = 72) were born in the U.S. About 15% of daughters (n = 24) were born in Cuba, and 9.5% of daughters (n = 15) were born in Colombia. Remaining participants were born in other Central and South American countries.
Fifty-nine mothers (37.3%) and 91 daughters (57.6%) were categorized as drug abusers. Drug abusers were identified by extent of alcohol and/or drug use during six months prior to assessment. Alcohol abusers were defined in terms of at least one heavy drinking episode per month– at least 4-5 glasses of wine, 3-4 cans/bottles of beer, or 3-4 four-ounce drinks of hard liquor per occasion – during the 12 months prior to assessment (adapted from Naimi et al., 2003). Drug abusers reported at least 3 days per week of marijuana use, 2 days a week of cocaine use, 1 or more occasions of heroin use per week, and/or at least 3 ecstasy use occasions per month during the 12 months prior to assessment. Abuse of prescribed medication occurred when participants took medicine without medical authorization, or in larger amounts than prescribed, or for longer than prescribed, during the 12 months prior to assessment (adapted from Turner et al., 2001).
On average, drug abusing mothers gave birth to daughters at 23.29 years (SD = 5.95). All drug abusing mothers started using alcohol sometime before their daughters were born. Approximately 36% of drug abusing mothers started using drugs before the birth of their daughters. The other 64% started using drugs after the birth of their daughters but before their daughters' 18th birthday, indicating drug use during their daughters' youth.
Measures
Demographics Variables and Time in U.S.
Items asked participants age (How old are you?) and nativity (Where were you born?). Percent of life in the U.S. was calculated by dividing number of years the participant lived in the U.S. by their age at time of assessment.
Alcohol Use
Items from the Health and Daily Living Form (HDL; Billings, Cronkite, & Moos, 1983) assessed participant alcohol use and, in part, determined drug abuse status. HDL indices have yielded evidence of concurrent and predictive validity (Moos, Schutte, Brennan, & Moos, 2005). See Table 1 for items and response formats for all study measures.
Table 1. Measures, Items, and Item Response Formats for Study Constructs.
| Construct | Measure | Items | Item Response Format |
|---|---|---|---|
| Alcohol Use | Healthy Daily Living Form |
|
Frequency of Use |
| |||
| Beer Quantity Responses | |||
| |||
| Hard Liquor Quantity Responses | |||
| |||
| Wine Quantity Responses | |||
| |||
| Drug Use | Drug Use Frequency measure | How often did you use the following drugs or medications during the past 12 months?: sedatives, hypnotics or tranquilizers; cannabis; stimulants; heroin; opioids; cocaine; PCP; hallucinogens; inhalants; others |
|
| Maternal Age of Alcohol and Drug Use Onset | Life Course and Health Research Center Survey | When I mention the following substances, please indicate the age when you first started using that substance: alcohol, sedatives, hypnotics or tranquilizers; cannabis; stimulants; heroin; opioids; cocaine; PCP; hallucinogens; inhalants; others | n/a |
| Age of Sexual Debut | Life Course and Health Research Center Survey |
|
n/a |
| Number of Sexual Partners | Life Course and Health Research Center Survey | Thinking back over the past 12 months, with how many different people, including men and women, have you had sex (vaginal, anal or oral) even if only one time? | n/a |
| Substance Use Before or During Sex | Life Course and Health Research Center Survey |
|
|
| Participant and Sexual Partners Intoxication During Sex | Life Course and Health Research Center Survey |
|
|
Drug Use
The Drug Use Frequency measure (DUF; O'Farrell, Fals-Stewart, & Murphy, 2003) assessed the frequency of drug use and, in part, determined drug abuse status. DUF scores correlate with collateral reports of drug use frequency and with the Timeline Follow-Back, indicating evidence of concurrent validity (O'Farrell et al., 2003).
Maternal Age of Alcohol and Drug Use Onset
Questions asking ages of onset of substance use were taken from a health risk behavior survey (Life Course and Health Research Center, 1997). No psychometric properties are available for these survey items.
Age of Sexual Debut and Number of Sexual Partners
Questions asking ages of debut of (a) vaginal sex, (b) oral sex, and (c) anal sex; and number of sexual partners during the past year were taken from the same survey (Life Course and Health Research Center, 1997).
Substance Use Before or During Sex
Items from the same survey (Life Course and Health Research Center, 1997) assessed the frequency of substance use before or during sex.
Participant and Sexual Partners Intoxication During Sex
Items from the same survey (Life Course and Health Research Center, 1997) also assessed intoxication during sex.
Results
Preliminary Analyses
One hundred and three (65.2%) daughters reported using alcohol before sex, and 54 (34.2%) used drugs before sex during the past year. Fifty-one daughters (32.3%) stated they were affected by alcohol during sex, while 24 (15.2%) were affected by illicit drugs during sex during the past year. Fifty daughters (31.6%) reported that their sexual partners were affected by alcohol during sex, while 25 (15.8%) indicated that their partners were intoxicated by drugs during sex.
A bivariate correlation matrix, including means and standard deviations, is presented in Table 2. Ages of oral, anal, and vaginal sex debut were positively correlated. More time in the U.S. was linked to younger ages of vaginal and oral sex debut, and maternal drug abuse. Maternal drug use was related to younger ages of vaginal and oral sex debut and more time in the U.S. More frequent alcohol use before sex was related to a younger age of debut of oral sex and maternal drug use. More frequent drug use before sex was related to (a) younger ages of debut of vaginal and oral sex, (b) more alcohol use before sex, (c) more time in the U.S., and (d) maternal drug use.
Table 2. Correlations, Means, and Standard Deviations among Daughter Variables.
| Variable | N | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age of Debut – Vaginal Sex (years) | 151 | 16.38 | 2.74 | 1.00 | ||||||||||||
| 2. Age of Debut – Oral Sex (years) | 138 | 17.96 | 4.13 | .64** | 1.00 | |||||||||||
| 3. Age of Debut – Anal Sex (years) | 60 | 22.07 | 7.05 | .38** | .46** | 1.00 | ||||||||||
| 4. Length of Life in U.S. (%) | 158 | 64.87 | 36.79 | -.36** | -.40** | -.24 | 1.00 | |||||||||
| 5. Maternal Drug Abuse Statusa | 158 | 0.37 | 0.48 | -.33** | -.38** | -.24 | .20* | 1.00 | ||||||||
| 6. Alcohol Use Before or During Sex – past 12 monthsb | 144 | 2.15 | 1.12 | -.16 | -.24** | -.01 | .08 | .19* | 1.00 | |||||||
| 7. Illicit Drug Use Before or During Sex – past 12 monthsb | 143 | 1.66 | 1.22 | -.31** | -.34** | -.21 | .21* | .27** | .41** | 1.00 | ||||||
| 8. Participants' average level of alcohol intoxication – past 12 monthsc | 144 | 1.37 | 0.57 | -.08 | -.22* | -.16 | .19* | .19* | .51** | .18* | 1.00 | |||||
| 9. Sexual partners' average level of alcohol intoxication– past 12 monthsc | 144 | 1.38 | 0.60 | -.03 | -.18* | -.03 | .23** | .12 | .44* | .23** | .56** | 1.00 | ||||
| 10. Participants' average level of intoxication from drugs– past 12 months | 143 | 1.17 | 0.42 | -.30** | -.32** | -.29* | .17* | .12 | .30** | .65** | .27** | .12 | 1.00 | |||
| 11. Sexual partners' average level of intoxication from drugs – past 12 months | 143 | 1.20 | 0.50 | -.23** | -.24** | -.14 | .15 | .16* | .33** | .62** | .27** | .38** | .64** | 1.00 | ||
| 12. Number of Sexual Partners – past 12 months | 154 | 1.43 | 1.18 | -.21* | -.33** | -.20 | .08 | .15 | .08 | .20* | .16* | .20* | .18* | .07 | 1.00 | |
| 13. Daughters' Drug Use Statusd | 158 | 0.58 | 0.50 | -.36** | -.35** | -.36** | .20* | .16* | .31** | .40** | .29** | .22** | .23** | .19* | .18* | 1.00 |
p < .05,
p < .01.
0 = non-abusing mother, 1 = abusing mother;
1 = never, 2 = rarely, 3 = sometimes, 4 = usually, 5 = always;
1 = not at all, 2 = somewhat, or 3 = very strongly;
0= non-abuser, 1 = abuser
As expected, more alcohol intoxication before sex was related to more frequent alcohol use before sex among participants. More alcohol intoxication before sex also was related to (a) younger age of oral sex debut (b) more time in the U.S., (c) maternal drug use, and (d) more drug use before sex. Sexual partners' level of alcohol intoxication before sex was positively related to participants' alcohol use before sex and participants' level of alcohol intoxication before sex too. Higher levels of alcohol intoxication before sex among sexual partners' also was related to (a) younger age of oral sex debut, (b) more time in the U.S., and (c) more drug use before sex among participants.
Level of intoxication from drug use before sex was positively related to frequency of drug use before sex. Level of intoxication also was positively related to (a) younger ages of vaginal, oral, and anal sex debut; (b) more time in the U.S.; (c) more frequent alcohol use before sex; and (d) higher levels of alcohol intoxication before sex. Similarly, sexual partners' level of intoxication from drug use before sex was positively related to participants' drug use before sex and participants' level of intoxication from drug use before sex. Higher levels of intoxication from drug use before sex among sexual partners' also was related to (a) participants' younger ages of vaginal and oral sex debut, (b) maternal drug abuse, (c) more participants' alcohol use before sex, and (d) greater participants' and partners' alcohol intoxication before sex.
More sexual partners was related to (a) younger ages of debut of vaginal and oral sex, (b) more drug use before sex, (c) participants' level of intoxication from drugs and alcohol before sex, and (d) sexual partners' level of alcohol intoxication before sex.
Participants' adult drug abuse status was related to (a) younger ages of vaginal, oral, and anal sexual debut, (b) more time in the U.S., (c) maternal drug abuse, (d) more frequent drug and alcohol use before sex, (e) higher level of intoxication from drug and alcohol use before sex, and (f) more sexual partners.
Age of Sexual Debut Measurement Model
A latent construct (age of sexual debut) was hypothesized to consist of 3 observed measures: ages of debut of (a) vaginal, (b) oral, and (c) anal sex. A latent construct was preferred over separate analyses of age of onset for each type of sexual behavior because the ages of debut were correlated, and we were interested in a parsimonious analytic model.
A confirmatory factor analysis (CFA) was conducted to test if indicators adequately represented the latent construct. We evaluated the measurement model (and the overall SEM – see Figure 1) using the comparative fit index (CFI), for which values above .90 reflect adequate fit (Kline, 2005) and values above .95 represent excellent fit (Tomarken & Waller, 2005); and the root mean square error of approximation (RMSEA). Values below .08 represent adequate fit (Quintana & Maxwell, 1999) and values below .05 represent excellent fit (Hancock & Freeman, 2001). Because three indicators were included in the measurement model, it was just-identified. Fit statistics are not available for such models. Factor loadings suggested that three indicators loaded strongly onto the latent construct (β estimates ranging from .47 to .88). Seventy-seven percent was variability in age of sexual debut was explained by age of debut of oral sex. Fifty-two percent was explained by age of debut of vaginal sex. Twenty-two percent was explained by age of debut of anal sex.
Structural Equation Model
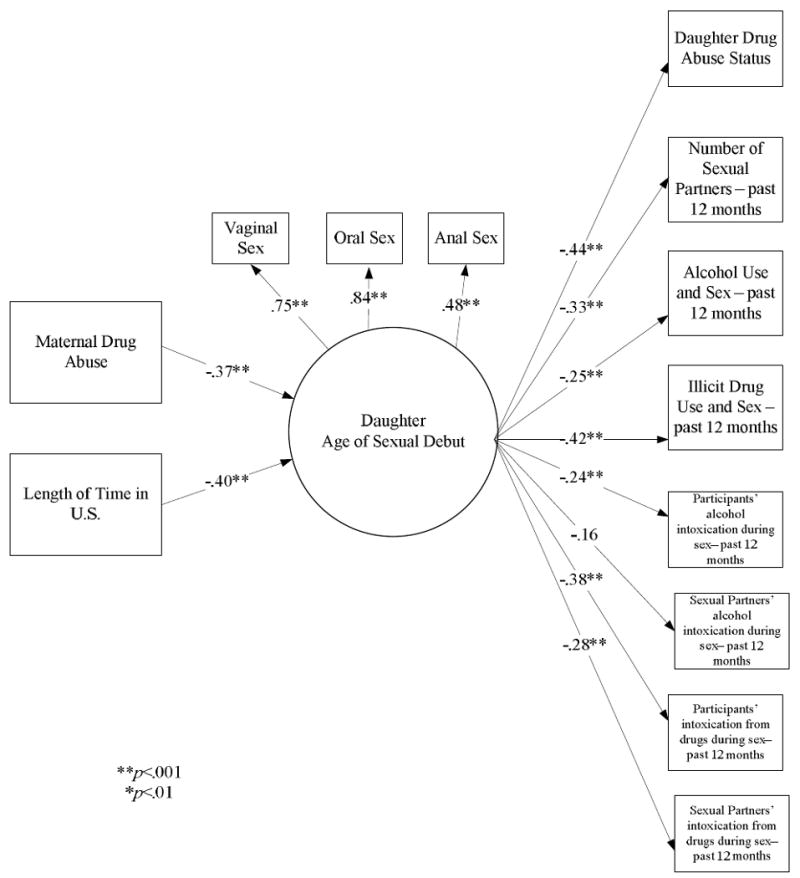
The SEM model (displayed in Figure 2) demonstrated adequate model fit, χ2 (36, N = 158) = 35.14, p = .51; CFI = 1.00; RMSEA < .001.
Figure 2. Structural equation model results.
Correlates of Age of Sexual Debut
Maternal drug abuse and time in the U.S. were both associated with daughters' age of sexual debut. Participants whose mothers were current drug abusers (and also had used drugs during the participants' youth) reported younger ages of sexual debut. Participants who spent more time in the U.S. also reported younger ages of sexual debut.
Sequelae of Age of Sexual Debut in Adulthood
Participants who reported younger ages of sexual debut were more often classified a drug abuser at the time of the study. Participants with younger ages of sexual debut also indicated (a) more sexual partners, (b) more alcohol and drug use before sex, and (c) higher levels of intoxication from alcohol and drug use before sex. Participants with younger ages of sexual debut also indicated that their sexual partners had higher levels of intoxication from drug use before sex.
Relationships between HIV/AIDS Risk Behaviors and Drug Abuse
Participant classification as a drug abuser was related to more alcohol (r = .37, p < .01) and drug use (r = .17, p < .05) before sex. Drug abuse status also was related to more alcohol intoxication before sex by participants (r = .21, p < .01) and their sexual partners (r = .17, p < .05). Participants who reported more alcohol use before sex also indicated (a) more drug use before sex (r = .35, p < .05), (b) more alcohol intoxication before sex for them (r = .49, p < .01) and their sexual partners (r = .43, p < .05), as well as (c) more intoxication from drug use before sex for them (r = .23, p < .01) and their sexual partners (r = .28, p < .01). Participants who reported more drug use before sex also indicated (a) more alcohol intoxication before sex by their sexual partners (r = .19, p < .05), as well as (b) more intoxication from drug use before sex for them (r = .58, p < .01) and their sexual partners (r = .56, p < .01). Higher levels of alcohol intoxication before sex among participants was related to more intoxication from drug use before sex for them (r = .20, p < .01) and their sexual partners (r = .22, p < .01). Likewise, more intoxication from drug use before sex among participants also was related to more intoxication from alcohol (r = .35, p < .01) and drug use before sex (r = .60, p < .01) by their sexual partners.
Discussion
Drug use among Latina mothers during their daughters' youth appears to be a salient risk factor for younger sexual debut and the likelihood that their daughters will become drug abusers as adults. In turn, daughters with younger ages of sexual debut abused more substances and engaged in more sexual risk behaviors. These findings illustrate the need for clinical efforts to address maternal drug abuse among Latinas and its potential harmful effects on their daughters' development. In addition, the chronicity of maternal drug use in the current sample suggests that drug use may have been a lifelong and untreated problem for many mothers. More culturally syntonic drug abuse interventions (e.g., involving family members, addressing cultural values) appear to be needed to better engage drug abusing Latinas (Bernal, 2006).
More time spent in the U.S. was associated with younger age of sexual debut. Although we were not able to determine whether foreign born daughters' first sexual activity occurred in the U.S. or in their countries of origin, such findings in a predominantly immigrant, Latina sample suggests that acculturation may predispose U.S. Latinas to initiate sex at earlier ages. Daughters who spent more of their lives in the U.S. also were classified as an adult drug abuser more often. Furthermore, they (a) tended to have drug abusing mothers; (b) reported more use of drugs before sex; and (c) had higher levels of intoxication from substances before sex. These findings reflect the nativity health paradox or the link between less time in the U.S. and better overall health behaviors despite comparatively low socioeconomic status and stress among Latino immigrants (Turner, Lloyd, & Taylor, 2006).
These findings should be interpreted in light of several limitations. Additional research should determine if findings differ depending on the context of first sexual experience; such as whether or not sex was consensual (Sandfort et al., 2008). Second, some Latino subgroups were not well represented. The sample was representative of Latinas living in Miami-Dade County, but not the United States. Finally, correlates of sexual debut may differ depending on geographic locale (Guo et al., 2005), and results may not generalize to Latinas living in rural areas of the United States.
Age of sexual debut appears to serve as a long term predictor of adult drug abuse and sexual risk behaviors. Researchers and interventionists need to consider early age of sexual debut among Latinas as a marker of risk for health compromising behaviors. Such efforts should consider mechanisms through which sexual initiation affects Latinas' health behaviors later in life. Much work remains to identify individual and contextual processes influencing early sexual activity among this growing segment of the U.S. population. Prevention efforts should focus on Latinas who are likely to initiate sexual activities in early adolescence, and disrupting the continuity of drug use and sexual risk taking between adolescence and adulthood.
Acknowledgments
This study was supported by award number P20MD002288 from the National Center for Minority and Health Disparity and award number R24DA014260 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center on Minority Health and Health Disparities, the National Institute on Drug Abuse, or the National Institutes of Health.
References
- Afable-Munsuz A, Brindis CD. Acculturation and the sexual and reproductive health of Latino youth in the United States: A literature review. Perspectives on Sexual and Reproductive Health. 2006;38:208–219. doi: 10.1363/psrh.38.208.06. [DOI] [PubMed] [Google Scholar]
- Bernal G. Intervention development and cultural adaptation research with diverse families. Family Process. 2006;45:143–151. doi: 10.1111/j.1545-5300.2006.00087.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Billings AG, Cronkite RC, Moos RH. Social-environmental factors in unipolar depression: Comparisons of depressed patients and nondepressed controls. Journal of Abnormal Psychology. 1983;92:119–133. doi: 10.1037//0021-843x.92.2.119. [DOI] [PubMed] [Google Scholar]
- Catalano RF, Hawkins JD. The social development model: A theory of antisocial behavior. In: Hawkins JD, editor. Delinquency & Crime: Current Theories. New York: Cambridge University Press; 1996. pp. 149–197. [Google Scholar]
- Centers for Disease Control & Prevention. Youth risk behavior surveillance-United States, 2007. Morbidity and Mortality Weekly Report 2008. 2008;57(SS-4):1–31. [PubMed] [Google Scholar]
- Centers for Disease Control & Prevention. HIV/AIDS Surveillance Report, Vol 17, Revised Edition. Atlanta: U.S. Department of Health and Human Services; 2007. [Google Scholar]
- Dolcini MM, Catania JA, Coates TJ, Stall R, Hudes ES, Gagnon JH, Pollack LM. Demographic characteristics of heterosexuals with multiple partners: the National AIDS Behavioral Surveys. Family Planning Perspectives. 1993;25:208–214. [PubMed] [Google Scholar]
- Gilliam ML, Berlin A, Kozloski M, Hernandez M, Grundy M. Interpersonal and personal factors influencing sexual debut among Mexican-American young women in the United States. Journal of Adolescent Health. 2007;41:495–503. doi: 10.1016/j.jadohealth.2007.05.009. [DOI] [PubMed] [Google Scholar]
- Guo S, Stanton B, Cottrell L, Clemens RL, Li X, Harris C, Marshall S, Gibson C. Substance use among rural adolescent virgins as a predictor of sexual initiation. Journal of Adolescent Health. 2005;37:252–255. doi: 10.1016/j.jadohealth.2004.11.124. [DOI] [PubMed] [Google Scholar]
- Hancock GR, Freeman MJ. Power and sample size for the root mean square error of approximation test of not close fit in structural equation modeling. Educational and Psychological Measurement. 2001;61:741–758. [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 2nd. New York: Guilford Press; 2005. [Google Scholar]
- Lau RR, Quadrel MJ, Hartman KA. Development and change of young adults' preventive health beliefs and behavior: Influence from parents and peers. Journal of Health and Social Behavior. 1990;31:240–259. [PubMed] [Google Scholar]
- Life Course and Health Research Center. Transitions: A study of stress and well being in young adulthood Wave I questionnaire. Florida International University; Miami, FL: 1997. Title of project: Drug Use Trajectories—Ethnic/Racial Comparisons. NIDA Grant Number DA10772. Retrieved on August 26, 2002 (available at http://www.fiu.edu/∼lchrc/pdfs/w2instrument.pdf) [Google Scholar]
- Moos RH, Schutte KK, Brennan PL, Moos BS. The interplay between life stressors and depressive symptoms among older adults. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 2005;60:P199–P206. doi: 10.1093/geronb/60.4.p199. [DOI] [PubMed] [Google Scholar]
- Muñoz-Laboy MA. Familism and sexual regulation among bisexual Latino men. Archives of Sexual Behavior. 2008;37:773–782. doi: 10.1007/s10508-008-9360-y. [DOI] [PubMed] [Google Scholar]
- Naimi TS, Brewer RD, Mokdad AH, Denny C, Serdula M, Marks JS. Binge drinking among US adults. Journal of the American Medical Association. 2003;289:70–75. doi: 10.1001/jama.289.1.70. [DOI] [PubMed] [Google Scholar]
- O'Farrell TJ, Fals-Stewart W, Murphy M. Concurrent validity of a brief self-report drug use frequency measure. Addictive Behaviors. 2003;28:327–337. doi: 10.1016/s0306-4603(01)00226-x. [DOI] [PubMed] [Google Scholar]
- Quintana SM, Maxwell SE. Implications of recent developments in structural equations modeling for counseling psychology. The Counseling Psychologist. 1999;27:485–527. [Google Scholar]
- Raffaelli M, Ontai LL. ‘She's 16 years old and there's boys calling over to the house’: An exploratory study of sexual socialization in Latino families. Culture, Health & Sexuality. 2001;3:295–310. [Google Scholar]
- Sandfort TG, Orr M, Hirsch JS, Santelli J. Long-term health correlates of timing of sexual debut: results from a national US study. American Journal of Public Health. 2008;98:155–161. doi: 10.2105/AJPH.2006.097444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singer M. A dose of drugs, a touch of violence and case of AIDS: Conceptualizing the SAVA syndemic. Free Inquiry in Creative Sociology. 1996;24:99–110. [Google Scholar]
- Tomarken A, Waller NG. Structural equation modeling as a data-analytic framework for clinical science: Strengths, limitations, and misconceptions. Annual Review of Clinical Psychology. 2005;1:31–65. doi: 10.1146/annurev.clinpsy.1.102803.144239. [DOI] [PubMed] [Google Scholar]
- Turner BJ, Fleishman JA, Wenger N, London AS, Burnam MA, Shapiro MF, Bing EG, Stein MD, Longshore D, Bozzette SA. Effects of drug abuse and mental disorders on use and type of antiretroviral therapy in HIV-infected persons. Journal of General Internal Medicine. 2001;16:625–633. doi: 10.1046/j.1525-1497.2001.016009625.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner RJ, Lloyd DA, Taylor J. Stress burden, drug dependence and the nativity paradox among U.S. Hispanics. Drug and Alcohol Dependence. 2006;83:79–89. doi: 10.1016/j.drugalcdep.2005.11.003. [DOI] [PubMed] [Google Scholar]
- Weeks MR, Schensul JJ, Williams SS, Singer M, Grier M. AIDS prevention for African-American and Latina women: Building culturally and gender-appropriate intervention. AIDS Education and Prevention. 1995;7:251–264. [PubMed] [Google Scholar]
- Wilder EI, Watt TT. Risky parental behavior and adolescent sexual activity at first coitus. The Milbank Quarterly. 2002;80:481–524. doi: 10.1111/1468-0009.00020. [DOI] [PMC free article] [PubMed] [Google Scholar]