

Abstract
Objective
To assess whether change in endoscopy score correlates with change in health-related quality of life (HRQOL) following endoscopic sinus surgery (ESS) for chronic rhinosinusitis (CRS).
Setting
Tertiary rhinology clinic
Patients
One hundred two adult patients, with and without nasal polyposis, who elected to undergo ESS and were followed for 12 ± 2 months postoperatively.
Intervention
Patient characteristics and Lund-Mackay computed tomography scores were recorded preoperatively. Lund-Kennedy endoscopy scores and 2 HRQoL surveys, the Rhinosinusitis Disability Index (RSDI) and Chronic Sinusitis Survey (CSS), were examined before and after surgery.
Main Outcome Measures
Postoperative changes in endoscopy score and HRQOL were examined using bivariate and multivariate analyses.
Results
Statistically significant improvements were found in endoscopy score (p<0.001) and for all total and subscale HRQoL measures (p<0.001). After controlling for baseline status and comorbid factors, improvement in endoscopy score significantly correlated with 12 month improvement on the total RSDI (p=0.01), the physical (p=0.01) and functional (p=0.02) subscales of the RSDI, and the symptom subscale of the CSS (p=0.003), but could explain only 25.5–36.6% of the linear variation for these HRQOL improvements.
Conclusions
For most patients, endoscopy scores and disease specific HRQOL significantly improved after endoscopic sinus surgery. Changes in endoscopy scores explain a portion of the improvement in HRQOL. For patients with CRS, improvements in disease specific HRQoL outcomes are complex, multidimensional constructs that cannot be entirely explained by surgical changes measured by endoscopic examination.
Keywords: Endoscopic sinus surgery, endoscopy, outcomes, quality-of-life, chronic sinusitis
INTRODUCTION
Relationships between objective measures of chronic rhinosinusitis (CRS) and health-related quality of life (HRQOL) remain elusive for patients electing endoscopic sinus surgery (ESS). There is evidence that a patients’ subjective symptomatic experience correlates with improved HRQOL following sinus surgery.1,2 However, a patients’ symptomatic experience has been shown, at best, to be weakly associated with objective findings such as computed tomography (CT) results.3,4 In fact, most of the literature shows that CT imaging does not correlate well with patient symptoms or HRQOL.5–8
Sinonasal endoscopy is used to gather critical information about mucosal inflammation before and after therapeutic intervention and is often used to direct ongoing therapy for CRS, however there has been limited investigation into the association between endoscopy results and HRQOL. Weak to moderate correlations have been reported between improvement in sinonasal symptoms and postoperative endoscopic examination results in patients after ESS.9,10 In contrast, patient response on the Chronic Sinusitis Survey (CSS), a validated HRQOL instrument, was not significantly correlated with endoscopic examination scores at any specific time after surgery.10 There has also been a reported lack of correlation between endoscopy score and a patient’s mean self-rated symptom score or Rhinosinusitis Disability Index (RSDI) total score in a nonsurgical group.11 Similarly, previous work from our group showed that preoperative endoscopy scores are not associated with changes in the CSS or RSDI after sinus surgery.12 The preceding literature is limited because relationships between endoscopy scores and HRQOL have been examined in a cross sectional fashion at various, discrete time intervals. To our knowledge, associations between postoperative changes in endoscopy scores and measures of improvement in postoperative HRQoL have not been examined in a population with chronic sinus disease. Investigating trends of postoperative improvement in endoscopy score as a proxy measure of improvement in mucosal inflammation could help to better understand whether improvements in endoscopic examination results coincide with and potentially predict improvements in disease specific HRQOL after sinus surgery.
The aim of this study was to investigate the relationship between change in endoscopy score and change in disease specific HRQOL following ESS for CRS. We hypothesized that postoperative improvement in endoscopy scores significantly correlates with improvement in HRQOL following surgical intervention.
METHODS
STUDY POPULATION and DATA MANAGEMENT
An institutional review board provided approval for consent/authorization forms and all research protocols. Subjects were identified from a tertiary rhinology clinic. Detailed study protocols and methods have been reported elsewhere.12,13 Eligible subjects consisted of adult patients referred to a rhinology specialist (T.L.S) with a primary diagnosis of CRS and whose condition was refractory to medical management. Patient diagnoses followed guidelines established by the Rhinosinusitis Task Force and endorsed by the American Academy of Otolaryngology – Head and Neck Surgery.14 Endoscopic sinus surgery was elected as the next treatment option. For patients meeting the inclusion criteria and agreeing to participate, one of us (T.L.S.) performed a thorough history and medical record review. Data collection included age, sex, race, preoperative CT findings, and sinus disease cofactors such as asthma, acetylsalicylic intolerance, nasal polyps, tobacco use, allergy, depression, and history of previous sinus surgery.
Patients returning for postoperative appointments 12 ± 2 months later were included in this analysis. Data were collected, compiled, and manually scored after each clinic visit. All responses were deidentified, transcribed, and securely stored in a database (Microsoft FoxPro for Windows; Microsoft Corp., Redmond, Washington).
OBJECTIVE MEASURES
Blinded to all HRQOL scores for the study duration, a single otolaryngologist (T.L.S.) performed preoperative bilateral assessments of the paranasal sinuses by reviewing CT scans in the coronal plane and conducting sinonasal endoscopy with the use of 2.7mm to 4.0mm diameter rigid endoscopes. Endoscopy procedures were repeated at the 12 month (± 2 months) postoperative appointments. Computed tomography and endoscopy were quantified using the Lund-MacKay (score range: 0–24) and Lund-Kennedy (score range: 0–20) scoring systems, respectively.15,16 The Lund-Mackay CT scoring system quantifies the severity of image opacification in the maxillary, ethmoidal, sphenoidal, ostiomeatal complex, and frontal sinus regions. The Lund-Kennedy endoscopy scoring system grades visual pathologic states within the nose and paranasal sinuses including: polyps, discharge, edema, scarring, and crusting.
QUALITY-OF-LIFE EVALUATIONS
A trained research coordinator aided subjects in completing two HRQoL surveys: the RSDI and the CSS. Patients were asked to complete each HRQoL instrument at both of the preoperative and postoperative clinic visits. The RSDI contains 30 questions (score range: 0–120) and consists of three subscales that measure disease-specific patient status in the physical, functional, and emotional domains.17 The physical subscale contains 11 questions (score range: 0–44), the functional subscale contains 9 questions (score range: 0–36), and the emotional subscale contains 10 questions (score range: 0–40). Lower RSDI total and subscale scores represent a lower impact of sinus disease. The CSS is a six-item HRQoL monitor used to measure sinusitis-specific symptom and medication use during the preceding 8-week period.18 The aggregate and subscale scores each range from 0 to 100 with lower scores representing a greater impact of sinus disease.
The outcome of interest was the improvement in HRQoL as measured by the total and subscale scores of the RSDI and CSS (postoperative score minus preoperative score). Improvement in the mucosal inflammatory process was operationalized as the difference in endoscopic examination score (postoperative score minus preoperative score).
STATISTICAL ANALYSIS
All analysis was performed using SPSS statistical software (version 16.0; SPSS Inc., Chicago, IL). Descriptive statistics (means, standard deviations, frequencies, and correlation coefficients) were calculated for all measures. Paired t-tests were used to test for significant improvement in endoscopy score and HRQOL between the preoperative and 12 month follow-up examinations. Because the subset of patients with nasal polyposis represents an extreme type of the inflammatory disease process within CRS, Spearman bivariate correlations were examined to determine potential differences in bivariate correlations for patients with and without polyps. Simple linear regression was then used to assess preliminary associations between change in endoscopy score and each HRQOL outcome.
Multivariate linear regression was used to control for and identify other significant cofactors. Preliminary multivariable models included change in endoscopy score as the independent variable of interest, age and preoperative CT score as continuous variables, and candidate variables with univariate significance (p ≤ 0.25). Potential confounders were identified by introducing each cofactor into a regression model that included the endoscopic change variable. A cofactor producing at least a ± 10% difference in the association between change in endoscopic score and change in outcome was considered a significant confounder.19 All multiplicative interactions were examined and remained in the model when marginally significant (p ≤ 0.10). Final models included adjustment for baseline HRQoL measures. All variables for the final seven individual models were selected using forward selection and backwards elimination processes based on p=0.10 and p=0.15 alpha levels, respectively, in a manual stepwise procedure. Residual patterning and diagnostic analyses were used to confirm assumptions of linearity and model accuracy. The adjusted coefficient of multiple determination (R2) was used to compare the percentage of variability explained by each model. Crude and adjusted effect estimates (β), standard errors, and 95% confidence intervals (CIs) are reported and p ≤ 0.10 was considered clinically significant for all analyses.
RESULTS
Of the 192 open cohort patients identified at baseline, data were prospectively collected and evaluated for 102 patients (52.8%) returning for normal scheduled follow-up, approximately 12 (± 2) months after surgery. Patient characteristics and the prevalence of each CRS cofactor are presented in Table 1.
Table 1.
Characteristics and comorbid factors in 102 Patients with CRS
| Mean ± SD | No. (%) | |
|---|---|---|
| Characteristics | ||
| Age | 46.7 ± 12.3 | |
| Follow-up (months) | 13.2 ± 2.3 | |
| Sex | ||
| Male | 36 (35.3) | |
| Female | 66 (64.7) | |
| CRS Cofactors | ||
| ASA Intolerance | 15 (14.7) | |
| Asthma | 48 (47.1) | |
| Sinonasal polyps | 36 (35.3) | |
| Current smoker | 9 (8.8) | |
| Allergy | 39 (38.2) | |
| Depression | 23 (22.5) | |
| Previous sinus surgery | 70 (68.6) | |
| Preoperative CT | 11.3 ± 7.2 |
Abreviations: CRS, chronic rhinosinusitis; SD, standard deviation; ASA, acetylsalicylic acid; CT, computed tomography.
Patients experienced a statistically significant mean reduction in inflammatory disease characteristics of the sinonasal mucosa, as measured by endoscopy (p<0.001) and improvement in all disease-specific HRQOL domains (all p<0.001; Table 2) approximately 1 year after surgery.
Table 2.
Mean Postoperative Changes in Endoscopy and HRQOL Outcome Measures in 102 Patients with CRS
| Preoperative Mean ± SD |
Postoperative Mean ± SD |
Change Mean ± SD |
(95% CI) | |
|---|---|---|---|---|
| Endoscopy score | 7.9 ± 4.8 | 5.1 ± 4.5 | −2.8 ± 4.6 | (−3.6, −1.9) |
| HRQoL outcomes | ||||
| RSDI physical subscale | 19.2 ± 7.9 | 12.4 ± 8.3 | −6.9 ± 8.4 | (−8,6, −5.2) |
| RSDI functional subscale | 16.6 ± 7.5 | 9.1 ± 7.4 | −7.6 ± 7.3 | (−9.1, −6.1) |
| RSDI emotional subscale | 14.8 ± 8.0 | 8.7 ± 7.9 | −6.1 ± 7.3 | (−7.5, −4.6) |
| RSDI total | 50.7 ± 20.7 | 30.2 ± 21.6 | −20.5 ± 20.0 | (−24.6, −16.6) |
| CSS symptom subscale | 27.8 ± 26.1 | 59.6 ± 27.8 | 31.9 ± 31.4 | (26.0, 38.4) |
| CSS medication subscale | 39.0 ± 25.2 | 55.1 ± 24.8 | 16.2 ± 31.4 | (9.7, 22.1) |
| CSS total | 33.4 ± 19.2 | 57.4 ± 20.7 | 24.0 ± 21.5 | (19.8, 28.3) |
Abbreviations: SD,standard deviation;
CI, confidence interval for change scores; RSDI, Rhinosinusitis Disability Index; CSS, Chronic Sinusitis Survey. Significant (p<0.001) postoperative improvements in endoscopy score and outcome measures were found 12+-2 months after endoscopic sinus surgery. p≤0.10 was considered statistically significant.
BIVARIATE CORRELATIONS FOR TOTAL COHORT
Moderate correlations were found between baseline HRQoL status and improvements for all HRQoL outcomes (r = −0.64 to −0.44, p<0.001). Patients reporting the worst preoperative status were associated with the greatest mean postoperative improvement in HRQoL 12 months after surgery.
Before adjusting for significant cofactors, change in endoscopy score significantly correlated with improvement on the RSDI total score (p=0.051), the RSDI physical subscale score (p=0.058), the RSDI functional subscale score (p=0.06), and the CSS symptom score (p=0.052; Figures 1,2,3, and 4). Change in endoscopy score was not found to significantly correlate with the RSDI emotional subscale score (r = 0.130; p=0.20), the CSS medication score (r = 0.159; p=0.11), or the total CSS (r = −0.025; p=0.81).
Figure 1.
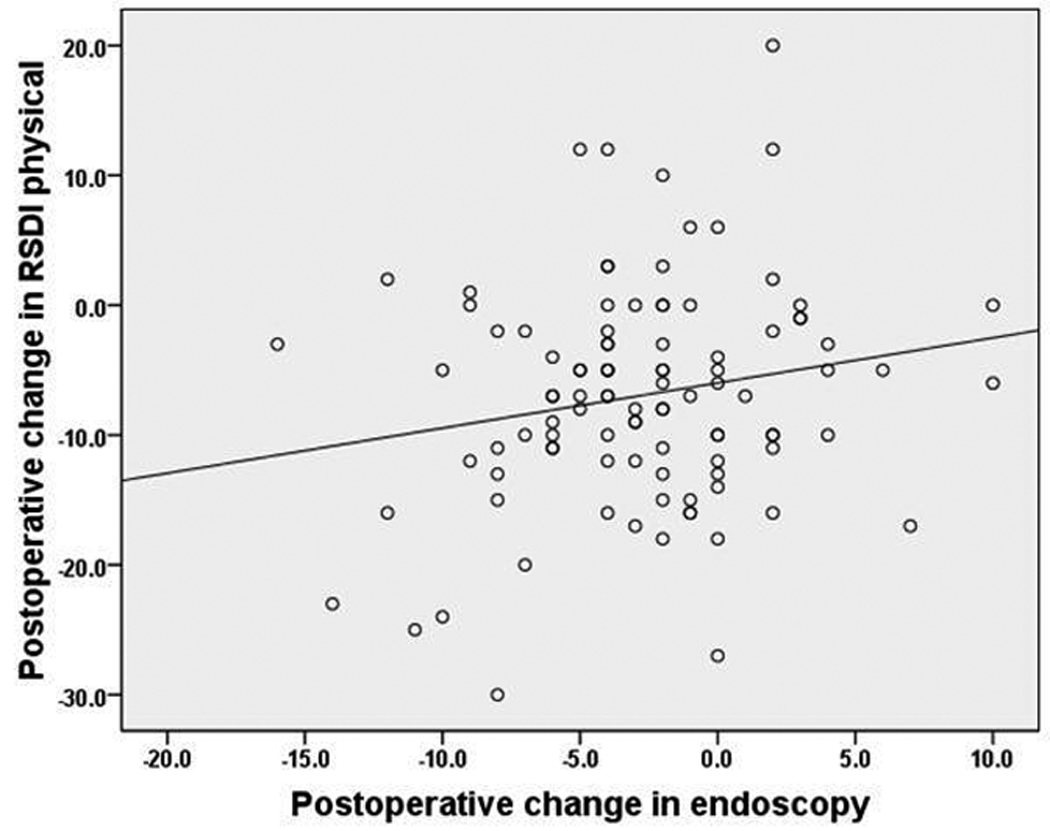
Bivariate correlation between postoperative changes in the Rhinosinusitis Disability Index (RSDI) physical subscale and postoperative changes in endoscopy score (n=102). Pearson’s r = 0.190, p=0.058.
Figure 2.
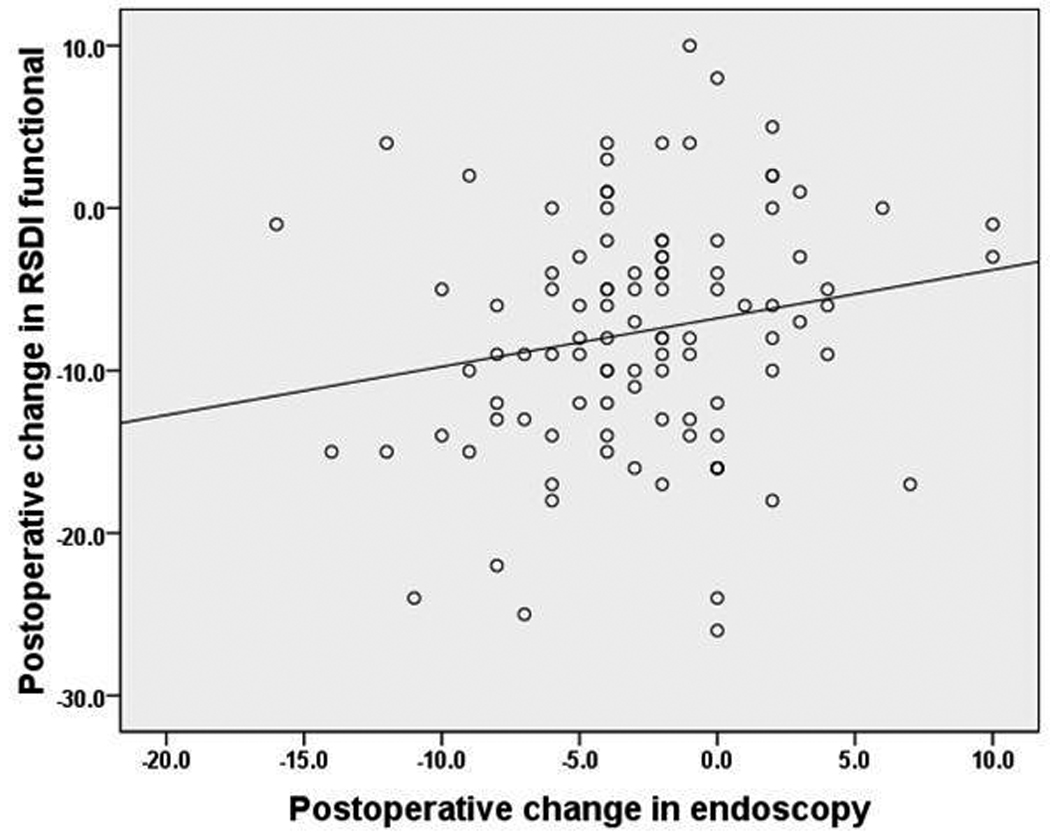
Bivariate correlation between postoperative changes in the Rhinosinusitis Disability Index (RSDI) functional subscale and postoperative changes in endoscopy score (n=102). Pearson’s r = 0.187,p=0.061.
Figure 3.
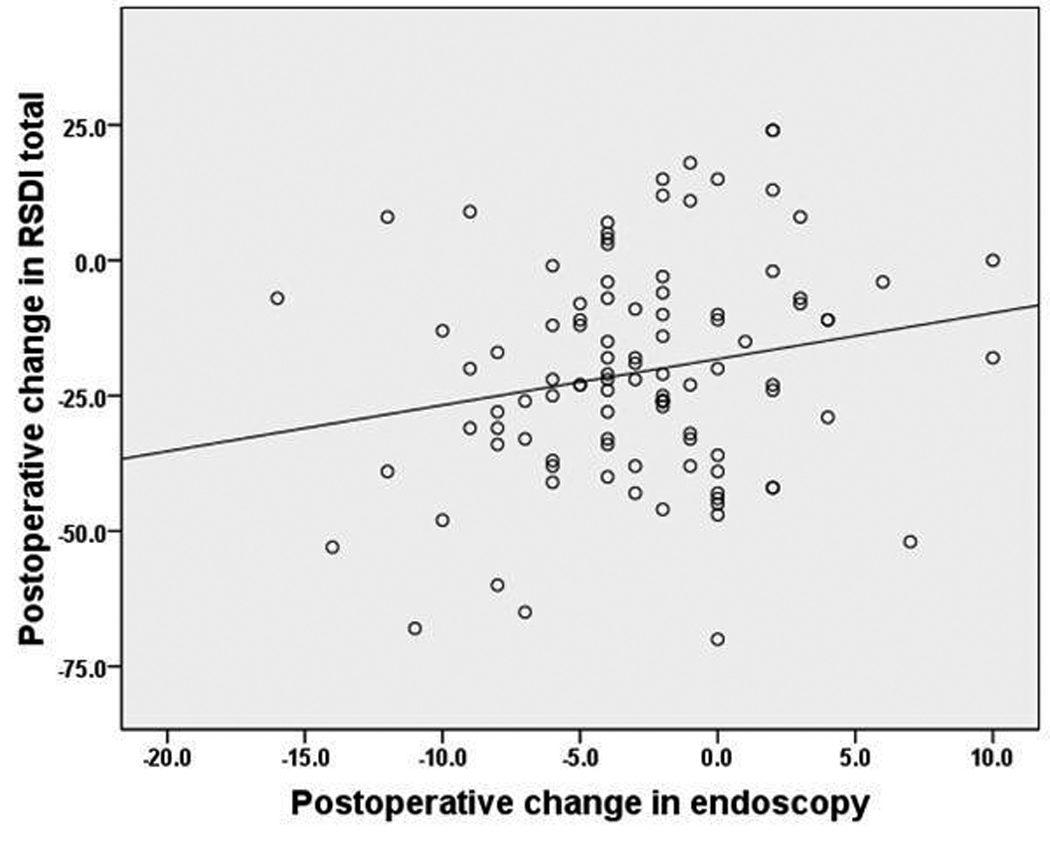
Bivariate correlations between postoperative changes in total Rhinosinusitis Disability Index (RSDI) total scores and postoperative changes in endoscopy score (n=102). Pearson’s r = 0.195, p=0.051.
Figure 4.
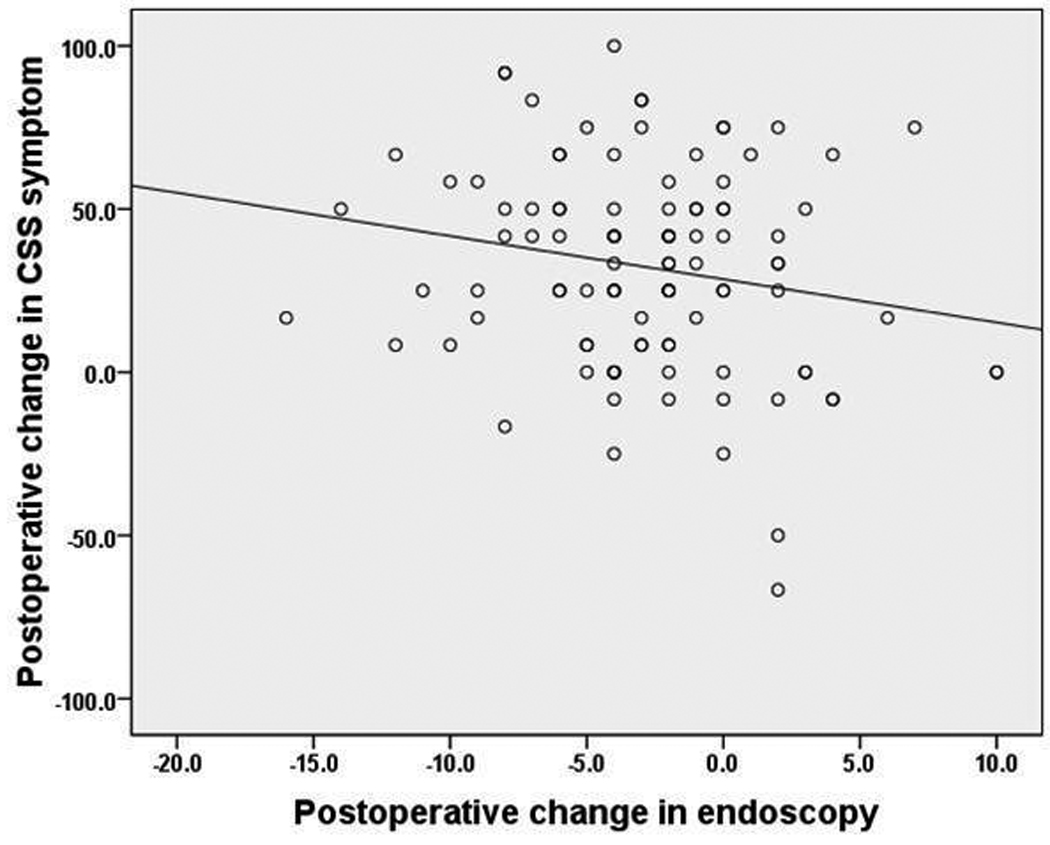
Bivariate correlations between postoperative changes in Chronic Sinusitis Survey (CSS) symptom subscale and postoperative changes in endoscopy score (n=102). Pearson’s r = 0.194,p=0.052.
BIVARIATE CORRELATIONS FOR POLYPS VS. NO POLYPS
For the 36 subjects with polyps, significant differences in bivariate correlations were found when compared with patients without polyps (Figure 5 and Figure 6). Correlations between improvement in endoscopy score and improvements on the RSDI physical subscale increased (r = 0.347; p = 0.04), as did correlations between improvement in endoscopy and improvements on the RSDI functional subscale score (r = 0.388; p=0.02), the RSDI total score (r = 0.367; p = 0.03), and the CSS symptom subscale score (r = −0.361; p = 0.03). Correlation between endoscopy score changes and improvement in the CSS medication subscale score became significant (r = 0.395; p = 0.02) for subjects with nasal polyps.. There were no significant correlations between improvement in endoscopy score and any HRQOL outcome for the 66 patients without polyps (all r < 0.125; p ≥ 0.32).
Figure 5.
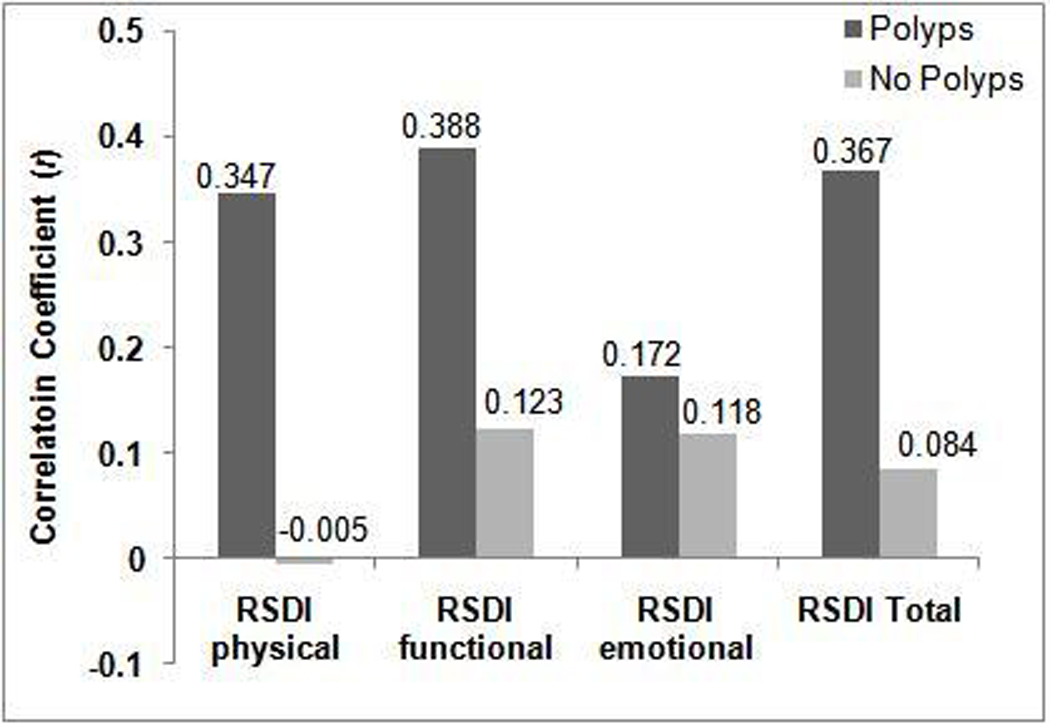
Comparisons of bivariate correlations between postoperative changes in endoscopy score and Rhinosinusitis Disability Index (RSDI) subscale and total scores for patients with and without nasal polyposis.
Figure 6.
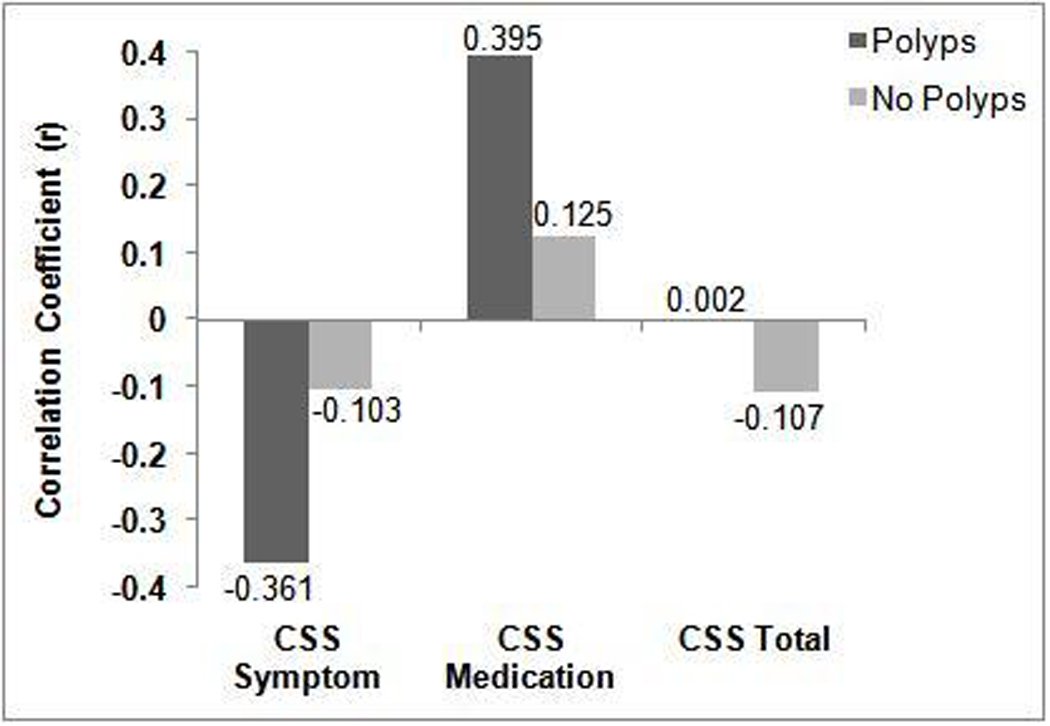
Comparison of bivariate correlations between postoperative changes in endoscopy score and Chronic Sinusitis Survey (CSS) subscale and total scores for patients with and without nasal polyposis.
MULTIVARIATE LINEAR REGRESSION MODELING
After controlling for sex, ASA intolerance, baseline HRQOL, and polyp status, improvement in endoscopy scores significantly correlated with postoperative improvement on the RSDI total score (p = 0.01), and the RSDI physical (p = 0.01) and functional (p = 0.02) subscales scores. Postoperative improvement in endoscopy score also significantly correlated with improvement in the CSS symptom subscale score (p = 0.003). No evidence of covariate interaction or confounding was identified with any final model and no significant outliers were discovered.
Results of multivariate modeling found that the effect estimate (β), or amount of improvement, in HRQoL that can be explained by improvements in the endoscopy score was relatively minimal (Table 3). For example, with a single point improvement in endoscopy score, RSDI total scores would be expected to improve by 1.03 units (95% CI: 0.23, 1.83 units). After adjusting for other significant cofactors, the mean observed 3.0 unit improvement in endoscopy score would equate to a 3.0 (2.5%) unit improvement on the RSDI total score. The amount of variability explained by each significant model was between 25.5% and 36.6%.
Table 3.
Crude and Adjusted Effect Estimates for Postoperative Changes in Lund-Kennedy Endoscopy Scores on HRQoL Outcomes in 102 Patients with CRS
| Outcome measures: | β±SE | Adjusted β±SE | (95% CI) | p-value | R2 |
|---|---|---|---|---|---|
| RSDI physical change | 0.35 ± 0.18 | 0.41 ± 0.16 | (0.09, 0.72) | 0.01 | 0.346 |
| RSDI functional change | 0.30 ± 0.16 | 0.31 ± 0.14 | (0.04, 0.58) | 0.02 | 0.302 |
| RSDI emotional change | 0.21 ± 0.16 | 0.20 ± 0.14 | (−0.07, 0.48) | 0.15 | 0.242 |
| RSDI total change | 0.85 ± 0.43 | 1.03 ± 0.40 | (0.23, 1.83) | 0.01 | 0.255 |
| CSS symptom change | −1.32 ± 0.67 | −1.77 ± 0.56 | (−2.92, −0.62) | 0.003 | 0.366 |
| CSS medication change | 1.09 ± 0.68 | 0.63 ± 0.56 | (−0.49, 1.74) | 0.27 | 0.266 |
| CSS total change | −0.12 ± 0.47 | −0.45 ± 0.43 | (−1.30, 0.41) | 0.30 | 0.246 |
Abbreviations: HRQoL, health-related quality of life; SE, mean standard error.; CI, confidence interval; RSDI, Rhinosinusitis Disability Index; CSS,Chronic Sinusitis Survey.
Effect estimates (β) for postoperative changes in endoscopy scores. Adjusted models included baseline HRQoL and significant covariate risk factors. p≤0.10 was considered statistically significant.
COMMENT
This investigation examined the association between 12 month postoperative changes in endoscopy score and disease-specific HRQoL in 102 patients undergoing ESS for CRS. Postoperative improvement in endoscopy score significantly correlated with improvement in the physical and functional subscale scores and total score of the RSDI, as well as the symptom subscale score of the CSS. Interpretation of statistical findings, however, demands prudence because the correlations estimates were relatively weak and multivariate models were able to explain only 25.5% – 36.6% of the total final model variance for these four significant outcomes. There is no criterion standard for interpreting R2 in regression modeling for this patient group; however these percentages suggest that better predictive models may be obtainable by using other independent predictors of HRQoL.20
Although surgical and therapeutic reduction of polyps, discharge, edema, and crusting significantly improves a patient’s inflammatory process and corresponding endoscopy score, these improvements can explain only a small percentage of the association with patient-based HRQoL and sinonasal symptom burden. These results are somewhat surprising because we intuitively expected that reducing mucosal inflammation, infection, and obstruction in the sinuses would explain a greater degree of improvement in those HRQoL domains. One plausible explanation is that disease-specific HRQoL is a complex, multidimensional construct that cannot be measured by endoscopic exam alone in this population.
Very few previous studies have addressed consistent correlations between measures of endoscopic examination and survey responses in patients undergoing sinus surgery. For patients with nasal polyps, Wright and Agrawal reported moderate correlations (r < 0.500) between Lund-Kennedy endoscopy scores and scores on the Sinus Symptom Questionnaire at 2 weeks and 1, 3, and 6-months after ESS using a cross-sectional analysis at specific time intervals.10 Analogous to our study, they failed to uncover significant correlations between endoscopy scores and CSS total scores at the 3-month (r < 0.050) and 6-month (r < 0.100) postoperative follow-up visits, but did report a weak correlation between changes in Lund-Kennedy endoscopy scores and improvement in CSS total scores between the 3- and 6-month follow-up (r = −0.300; p < 0.001).
Toros et al.21 reported finding significant correlations between endoscopy score and total patient reported symptom (on a visual analog scale: 0–10cm) preoperatively (r = 0.479; p < 0.001) and 12 months postoperatively (r = 0.628; p < 0.001) in 86 patients with and without polyps. Likewise, Giger et al. 9 reported that the percentage of subjective symptom improvement correlated significantly (r = −0.600; p < 0.001) with postoperative endoscopy findings in the ethmoidal cavities of 77 patients with CRS who did not have nasal polyposis. Although the studies are similar, they used patient-reported symptom severity measures as clinical outcomes of interest in smaller populations with varied regard for nasal polyposis. However, they did not assess postoperative trends with the use of validated, disease-specific HRQOL survey instruments. In addition, Birch et al.11 reported finding a lack of correlation between endoscopy scores and self-related symptom scores or RSDI total scores in a nonsurgical population of 53 patients with CRS but without regard for polyp status. Although that study used a disease-specific HRQOL outcome measure, the study was limited to a cross sectional analysis of a smaller, non-surgical population.
Endoscopic sinus surgery with postoperative medical management is not uniformly successful for decreasing the chronic inflammatory process in all patients. That fact is responsible for the high prevalence (approximately 68%) of prior surgery reported in this investigation and accounts for the 19 cohort patients (18.6%) who had worse postoperative endoscopy scores. A total of 15 (14.7%) and 13 (12.7%) patients also reported worse postoperative total scores on the RSDI and CSS, respectively. We believe these findings to be representative of our larger clinical population and the removal of these patients for this analysis did not significantly change the linear associations between improvements in endoscopy score and HRQOL outcomes in the total population.
Thirty-six patients with nasal polyposis were found to have stronger correlations between changes in endoscopy score and HRQOL. The removal of polyps and reduction of sinonasal edema, which are associated with ESS, are objectively measured by the Lund-Kennedy scoring system (improvement range: 4–8 units). We surmise that improvements in HRQoL may be related to a patient’s perception of changes in nasal obstruction, improved ventilation and olfaction, and reduced facial pressure. For patients with polyps, we found moderate, positive correlation between changes in endoscopy score and the CSS medication subscale score, indicating that medication usage moderately increased as endoscopy scores improved. The CSS medication subscale is sensitive to the use of prescribed topical nasal corticosteroid sprays and there is a higher likelihood that patients with nasal polyps will be prescribed long-term topical nasal corticosteroid sprays to control future inflammatory symptoms.
Defining the relevant and minimal clinically important differences in HRQoL can be challenging for patients with sinusitis.22 For instance, Gliklich and Metson23 defined an indication of “clinical improvement” on the CSS total score as an improvement of 8 points, or a 4-week (of 8-week [50%]) change in duration of symptom or medication usage. To define a similar degree of improvement, using a similar effect estimate of 0.5, the RSDI total score would require a 12 point change. Other investigations have defined clinically meaningful improvement as an effect estimate greater than or equal to half a standard deviation in the preoperative score of each HRQOL outcome.24,25 For example, applying this definition to our study population, a clinically meaningful improvement would be defined as at least 10.4 units (20.7 divided by 2) for RSDI total scores or 2.4 units (4.8 divided by 2) for endoscopy scores (Table 2). To use either of these definitions would lead us to conclude that improvements in HRQOL that are attributable to improvements in endoscopy, were statistically significant but less clinically relevant according to multivariate modeling (Table 3).
There are caveats to be considered with this study. First, there was a 47.2% loss to follow-up for all patients enrolled at baseline. We believe that this is representative of a tertiary clinical population with CRS and often is attributable to changes in insurance coverage, long distance travel, and unwillingness to participate. We found no meaningful differences in patient characteristics or prevalence of CRS comorbidity between patients with and without 12 month follow-up that would reasonably explain this attrition rate. Secondly, the lack of correlations between improvement in endoscopy score and HRQOL outcomes are confined to the 12 ± 2 month postoperative period and should not be generalized to follow-up times outside that range. In addition, correlation studies are inherently limited and cannot infer a direct cause-and-effect relationship. There is consistency of statistically significant effect across different, complementary measures of disease-specific HRQOL outcomes. However, because HRQOL subscales strongly correlate with total scores and because of a subsequent increased likelihood of making a Type I error owing to these clinical or biological patterns, correcting for multiple comparisons should be considered when examining a similar number of HRQOL outcomes simultaneously. Despite these considerations, our investigation adds to the dearth of literature regarding the associations between sinonasal endoscopy score and postoperative improvements in disease specific HRQOL outcomes.
In conclusion, strong associations between independent predictors and various outcome measures of CRS remain elusive. This investigation determined that significant postsurgical improvement in endoscopy score correlates with significant improvement in disease-specific HRQOL domains for patients electing ESS, with stronger correlations found in the subset of patients presenting with nasal polyposis. However, postoperative improvement in sinonasal characteristics can explain only a relatively small contribution to average HRQOL improvement after ESS. Although endoscopy score is a critical and reliable measure of postoperative treatment effect, this investigation allows for the provision and dissemination of more accurate information during patient consultation and prognosis after ESS.
ACKNOWLEDGEMENTS
This research was made possible by a grant from the NIH/NIDCD #R01 DC005805 and support from the Master of Public Health graduate program within the Department of Public Health and Preventive Medicine at Oregon Health & Science University. Oregon Health & Science University provided non-financial assistance for this investigation through administrative support, access to office and clinical space, as well as protected research time for all investigators. Dr. Timothy L. Smith (PI) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. We would also like to thank Lindsay Wyant, PA, for her clinical assistance and consultation during this process.
Footnotes
Public clinical trial registration (http://www.clinicaltrials.gov) ID: NCT00799097.
Jess Mace and Timothy L. Smith were both partially funded by grant support from the NIH/NIDCD. Timothy L. Smith is also a consultant for Sinexus, Inc., Palo Alto, Ca., which provided no financial support for this investigation. There are no potential conflicts of financial interest for any other coauthor.
REFERENCES
- 1.Giger R, Landis BN, Zheng C, et al. Objective and subjective evaluation of endoscopic nasal surgery outcomes. Am J Rhinol. 2003;17(6):327–333. [PubMed] [Google Scholar]
- 2.Damm M, Quante G, Jungehuelsing M, Stennert E. Impact of functional endoscopic sinus surgery on symptoms and quality of life in chronic rhinosinusitis. Laryngoscope. 2002;112:310–315. doi: 10.1097/00005537-200202000-00020. [DOI] [PubMed] [Google Scholar]
- 3.Wabnitz D, Nair S, Wormald PJ. Correlation between preoperative symptom scores, quality-of-life questionnaires, and staging with computed tomography in patients with chronic rhinosinusitis. Am J Rhinol. 2005;19(1):91–96. [PubMed] [Google Scholar]
- 4.Bhattacharyya N. A comparison of symptom scores and radiographic staging systems in chronic rhinosinusitis. Am J Rhinol. 2005;19(2):175–179. [PubMed] [Google Scholar]
- 5.Bhattacharyya N. Radiographic stage fails to predict symptom outcomes after endoscopic sinus surgery for chronic rhinosinusitis. Laryngoscope. 2006;116(1):18–22. doi: 10.1097/01.mlg.0000192284.22703.04. [DOI] [PubMed] [Google Scholar]
- 6.Basu S, Georgalas C, Kumar BN, Desai S. Correlation between symptoms and radiologic findings in patients with chronic rhinosinusitis: an evaluation study using the Sinonasal Assessment Questionnaire and Lund-Mackay grading system. Eur Arch Otorhinolaryngol. 2005;262:751–754. doi: 10.1007/s00405-004-0891-0. [DOI] [PubMed] [Google Scholar]
- 7.Hwang PH, Irwin SB, Griest SE, Caro JE, Nesbit GM. Radiologic correlates of symptom-based diagnostic criteria for chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2003;128:489–496. doi: 10.1016/S0194-59980223295-7. [DOI] [PubMed] [Google Scholar]
- 8.Bhattacharyya T, Piccirillo J, Wippold JF. Relationship between patient-based descriptions of sinusitis and paranasal sinus computed tomographic findings. Arch Otolaryngol Head Neck Surg. 1997;123:1189–1192. doi: 10.1001/archotol.1997.01900110039006. [DOI] [PubMed] [Google Scholar]
- 9.Giger R, Dulguerov P, Quinodoz D, et al. Chronic panrhinosinusitis without nasal polyps: Long-term outcome after functional endoscopic sinus surgery. Otolaryngol Head Neck Surg. 2004;131:534–541. doi: 10.1016/j.otohns.2004.03.030. [DOI] [PubMed] [Google Scholar]
- 10.Wright ED, Agrawal S. Impact of perioperative systemic steroids on surgical outcomes in patients with chronic rhinosinusitis with polyposis: Evaluation with the novel perioperative sinus endoscopy (POSE) scoring system. Laryngoscope. 2007;117(11 Pt 2) Suppl 115:1–28. doi: 10.1097/MLG.0b013e31814842f8. [DOI] [PubMed] [Google Scholar]
- 11.Birch DS, Saleh HA, Wodehouse T, et al. Assessing the quality of life for patients with chronic rhinosinusitis using the “Rhinosinusitis Disability Index”. Rhinology. 2001;39(4):191–196. [PubMed] [Google Scholar]
- 12.Smith TL, Mendolia-Loffredo S, Loehrl TA, Sparapani R, Laud PW, Nattinger AB. Predictive factors and outcomes in endoscopic sinus surgery for chronic rhinosinusitis. Laryngoscope. 2005;115:1–7. doi: 10.1097/01.mlg.0000182825.82910.80. [DOI] [PubMed] [Google Scholar]
- 13.Mace J, Michael YL, Carlson NE, Litvack JR, Smith TL. Effects of depression on quality of life improvement after endoscopic sinus surgery. Laryngoscope. 2008;118(3):528–534. doi: 10.1097/MLG.0b013e31815d74bb. [DOI] [PubMed] [Google Scholar]
- 14.Benninger MS, Ferguson BJ, Hadley JA, et al. Adult chronic rhinosinusitis: Definitions, diagnostics, epidemiology, and pathophysiology. Otolaryngol Head Neck Surg. 2003;129 Suppl:S1–S32. doi: 10.1016/s0194-5998(03)01397-4. [DOI] [PubMed] [Google Scholar]
- 15.Lund VJ, Mackay IS. Staging in rhinosinusitis. Rhinology. 1993;107:183–184. [PubMed] [Google Scholar]
- 16.Lund VJ, Kennedy DW. Quantification for staging sinusitis. Ann Otol Rhinol Laryngol. 1995;167:17–21. [PubMed] [Google Scholar]
- 17.Benninger MS, Senior BA. The development of the rhinosinusitis disability index. Otolaryngol Head Neck Surg. 1997;123:1175–1179. doi: 10.1001/archotol.1997.01900110025004. [DOI] [PubMed] [Google Scholar]
- 18.Gliklich RE, Metson R. Techniques for outcomes research in chronic sinusitis. Laryngoscope. 1995;105:387–390. doi: 10.1288/00005537-199504000-00010. [DOI] [PubMed] [Google Scholar]
- 19.Greenland S. The effect of misclassification in the presence of covariates. Am J Epidemiol. 1980;112:564–569. doi: 10.1093/oxfordjournals.aje.a113025. [DOI] [PubMed] [Google Scholar]
- 20.Chen H, Katz PP, Eisner MD, et al. Health-related quality of life in adult rhinitis: the role of perceived control of disease. J Allergy Clin Immunol. 2004;114(4):845–850. doi: 10.1016/j.jaci.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 21.Toros SZ, Bolukbasi S, Naiboglu B, et al. Comparative outcomes of endoscopic sinus surgery in patients with chronic sinusitis and nasal polyps. Eur Arch Otorhinolaryngol. 2007;264:1003–1008. doi: 10.1007/s00405-007-0301-5. [DOI] [PubMed] [Google Scholar]
- 22.Meltzer EO, Hamilos DL, Hadley JA, et al. Rhinosinusitis: Establishing definitions for clinical research and patient care. J Allergy Clin Immunol. 2004;114(6 Suppl):S155–S212. doi: 10.1016/j.jaci.2004.09.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gliklich RE, Metson R. Effect of sinus surgery on quality of life. Otolaryngol Head Neck Surg. 1997;117:12–17. doi: 10.1016/S0194-59989770199-2. [DOI] [PubMed] [Google Scholar]
- 24.Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care. 2003;41(5):582–592. doi: 10.1097/01.MLR.0000062554.74615.4C. [DOI] [PubMed] [Google Scholar]
- 25.Robinson JL, Griest S, James KE, Smith TL. Impact of aspirin intolerance on outcomes of sinus surgery. Laryngoscope. 2007;117(5):825–830. doi: 10.1097/MLG.0b013e3180333121. [DOI] [PubMed] [Google Scholar]