

Abstract
The aim of this study was to examine the influence of maternal-child relationship quality during toddlerhood on early childhood physiological regulation. A community sample of 447 children (215 males) was recruited at age two for participation in the study using the Child Behavior Checklist (Achenbach, 1992). Mothers and children were observed across several interactions in the laboratory at age two and mothers completed the Parenting Stress Index (Abidin, 1995). Relationship quality was assessed using laboratory measures of hostility, positive guidance, and stress related to the quality of the relationship as reported by mothers. Cardiac vagal regulation at age five was assessed across six challenge tasks, three in which the child and mother worked together and three in which the child worked independently, and was indexed by the magnitude of vagal withdrawal (decrease in respiratory sinus arrhythmia, RSA) to challenge. Results indicated that children displayed greater cardiac vagal regulation and heart rate acceleration during collaborative tasks versus independent tasks. In addition, maternal-child relationship quality predicted the degree of vagal regulation in children at age five, even after controlling for early and concurrent level of behavior problems as well as two year cardiac vagal regulation. Children with poorer quality relationships displayed significantly poorer vagal regulation and lower heart rate acceleration (p <.01). These findings are discussed in terms of the implications of environmental factors for the acquisition of fundamental self-regulatory skills.
Keywords: RSA, vagal regulation, maternal-child relationship, physiological regulation, toddlerhood, children, maternal behavior, parenting stress, emotion
Toddlerhood
Recent work in both developmental and clinical psychology has noted that self-regulation skills are critical to adaptive functioning across a range of domains (Baumeister & Vohs, 2004; Calkins & Fox, 2002; Keenan, 2000; Shaw, Keenan, Vondra, Delliquadri, & Giovannelli, 1997). The ability to exercise self-control over emotions, cognitions, and behavior develops over the first several years of life and has particular importance for the development of appropriate and adaptive social behavior and academic achievement during the school years (Calkins, in press; Calkins & Keane, 2004; Eisenberg, Smith, Sadovsky, & Spinrad, 2004; Howse, Calkins, Keane, Anastopoulos & Shelton, 2003; Rothbart & Sheese, 2007). Research in the area of early self-regulation has focused on both intrinsic (child) and extrinsic (familial) contributors to both normative development and individual differences in a range of regulatory skills and abilities, from the physiological to the behavioral (Fox & Calkins, 2003).
With respect to child characteristics that may contribute to the development of self-regulation, temperamental and biological substrates of self-regulation have been the focus of considerable theoretical (Beauchaine, 2001; Calkins, 1994; Davidson, Fox & Kalin, 2007; Fox, 1994; Lewis, 2005) and empirical work (Blair, 2003; Calkins & Dedmon, 2000; Calkins & Keane, 2004). Theories of self-regulation that focus on underlying biological components assume that maturation of different biological support systems lays the foundation for increasingly sophisticated emotional, cognitive, and behavioral regulation that is observed across childhood. More specifically, recent psychophysiological research highlights the role of the autonomic nervous system in regulating many biobehavioral processes. The autonomic nervous system functions as a complex system of afferent and efferent feedback pathways that are integrated with other neurophysiological and neuroanatomical processes, reciprocally linking cardiac activity with central nervous system processes (Chambers & Allen, 2007). Pathways of the parasympathetic nervous system, in particular, are implicated in these processes and, consequently, they play a key role in the regulation of state, motor activity, emotion, and cognition (Porges, 2003). Specifically, the myelinated vagus nerve, originating in the brainstem nucleus ambiguus, provides input to the sinoatrial node of the heart, producing dynamic changes in cardiac activity that allow the organism to transition between sustaining metabolic processes and generating more complex responses to environmental events (Porges, 2007). This central-peripheral neural feedback loop is functional relatively early in development (Porges, 2007), though there is good evidence that individual differences in the integrity of these processes are a consequence of both organic characteristics and postnatal experiences (Calkins & Hill, 2007).
Parasympathetic influences on heart rate can be easily quantified in young humans by measuring heart rate variability. Variability in heart rate that occurs at the frequency of spontaneous respiration (respiratory sinus arrhythmia, RSA) can be measured non-invasively and is considered a good estimate of the parasympathetic influence on heart rate variability via the vagus nerve. Porges and colleagues developed a method that measures the amplitude and period of the oscillations associated with inhalation and exhalation, referred to as vagal tone (Vna; Porges, 1985, 1991, 1996; Porges & Byrne, 1992). Of particular interest to researchers studying self-regulation, though, has been measurement of vagal regulation of the heart when the organism is challenged. Such regulation is indexed by a decrease in RSA or vagal tone (vagal withdrawal) during situations where coping or emotional and behavioral regulation is required (Porges, 2003; 2007). Vagal regulation in the form of decreases in RSA is often described as the functioning of “the vagal brake” because a decrease, or withdrawal, of vagal input to the heart has the effect of stimulating increases in heart rate. During demanding tasks, such a response reflects physiological processes that allow the child to shift focus from internal homeostatic demands to demands that require internal processing or the generation of coping strategies to control affective or behavioral arousal. Thus, vagal withdrawal is thought to be a physiological strategy that results in greater cardiac output in the form of HR acceleration, and that supports behaviors indicative of active coping (Calkins, Graziano, & Keane, 2007; El-Sheikh & Whitson, 2006; Porges, 1991; 1996; Propper & Moore, 2006; Wilson & Gottman, 1996).
Considerable research suggests that cardiac vagal withdrawal is linked to a range of behavioral processes that are regulatory in nature and that are observable quite early in development. Greater vagal withdrawal during challenging situations is related to better state regulation, greater self-soothing and more attentional control in infancy (DeGangi, DiPietro, Greenspan, & Porges, 1991; Huffman et al., 1998), fewer behavior problems and more appropriate emotion regulation in preschool (Calkins, 1997; Calkins & Dedmon, 2000; Calkins & Keane, 2004; Porges, Doussard-Roosevelt, Portales, & Greenspan, 1996), and effortful control of attention and sustained attention in school-age children (Calkins et al., 2007; Suess, Porges, & Plude, 1994). Moreover, recent research comparing the magnitude of RSA response to different types of challenges indicates that children display significantly greater decreases in RSA when provided with parental support during a task than when confronted with a challenge independent of support (Calkins & Keane, 2004), and that the magnitude of this response is an individual difference that is moderately stable across early development and that predicts a range of indicators of adaptive functioning (Calkins & Keane, 2004; El-Sheikh, 2005). The extension of these research findings is that while vagal withdrawal may be related to complex responses involving the regulation of attention, emotion, and behavior, a deficiency in this ability may be related to early adjustment problems, particularly problems characterized by a lack of behavioral and emotional regulation (Calkins & Dedmon, 2000; Calkins et al., 2007; Doussard-Roosevelt, Montgomery, & Porges, 2003; Porges, 1996;). Moreover, because of its importance in the regulation of emotion and behavior, both of which show considerable growth during the preschool period (Bronson, 2000), the predictors of individual differences in physiological regulation are of both theoretical and empirical significance.
Previous work has shown that cardiac functioning is affected by both sympathetic and parasympathetic processes (Calkins et al., 2007; Lahey, Hart, Pliska, Applegate, & McBurnett, 1993; Raine, 1996). Given that HR is influenced both sympathetically and parasympathetically, it would be important to examine these effects independently. For example, some studies have suggested that underarousal of the autonomic nervous system as reflected by low heart rate (HR) in particular may be a core characteristic of adolescents and adults with regulation difficulties (Lahey et al., 1993; Raine, Venable, & Williams, 1990; Raine, 1996). In addition, Wilson and Gottman (1996) hypothesized that excessive heart rate reactivity may interfere with the effective allocation of attentional abilities to meet task demands. Resting measures of cardiac activity and response measures (e.g., RSA suppression) have also been shown to be related in children (Calkins, 1997; Suess et al., 1994). Consequently, the current study sought to measure children's regulation capabilities via a reduction in general levels of arousal (indexed by HR) and through better implementation of regulatory processes stemming from the parasympathetic nervous system (i.e., RSA withdrawal).
In addition to the influence of child characteristics on emerging self-regulation, recent conceptual work and empirical research suggests that caregiver behavior may affect the development of behavioral self-regulation skills (Calkins, 2004; Crockenberg & Leerkes, 2004), as well as the functioning of numerous biological regulatory and stress systems (Calkins & Hill, 2007; Gunnar, 2006; Propper & Moore, 2006). During infancy, successful regulation largely depends on caregiver support and flexible responding (Kopp, 1982; Calkins & Fox, 2002; Sroufe, 2000). To the extent that a caregiver can appropriately read infant signals and respond in ways that minimize distress, or alternatively, motivate positive interaction, the infant will integrate such experiences into the emerging behavioral repertoire of self-regulatory skills. In addition, deviations from supportive caregiving may contribute to patterns of self-regulation that undermine the development of appropriate skills and abilities needed for later developmental challenges (Cassidy, 1994). During toddlerhood, the range of self-regulatory skills of the child is expected to increase, and the caregiver's supportive versus non-supportive role in this process is also an important predictor of positive outcomes (Calkins, 2007).
Although most of the emphasis in the empirical literature on the development of self-regulation has been on the effects of caregiver behavior on behavioral manifestations of such regulation, caregivers may also influence children's functioning at a biological level (Calkins & Hill, 2007; Propper & Moore, 2006). Importantly, evidence from animal models suggests that caregiving affects infants' biological and behavioral systems of regulation through the environment the caregiver provides rather than through shared inherited traits. For example, Meeney and colleagues have shown that high levels of maternal licking/grooming and arched backed nursing in rats affects the neurological systems associated with the stress response, a process that has a long-term influence on stress-related illness, certain cognitive functions, and physiological functions (Caldji et al., 1998; Champagne & Meaney, 2001; Francis et al., 1999). Furthermore, cross-fostering studies demonstrate convincingly that these maternal behaviors are transmitted behaviorally through the nursing mother and not through the biological mother, indicating that early caregiving is a crucial factor in early development and may affect the organism's level of emotional reactivity even when they reach adulthood (Calatayud, Coubard, & Belzung, 2004; Champagne & Meaney, 2001).
This psychobiological influence on emerging regulation is important as children who have characteristically low thresholds for arousal, or who have difficulty managing that physiological arousal, are at a disadvantage because emergent behavioral self-regulation strategies are dependent on the basic control of physiological processes that support behavioral strategies (Porges, 2003). To the extent that caregivers can provide the support for such physiological control early in development, children should be more successful at using attentional and behavioral strategies to control emotion, behavior, and cognitive processes. A small number of studies have examined the effects of maternal behavior on child vagal regulation in particular. In general, these studies, most of which are cross-sectional, find that mothers who are sensitive and engage in more responsive parenting have children with better vagal regulation, and that maternal intrusiveness and restrictive parenting undermines such regulation (Calkins, Smith, & Gill, 1998; Haley & Stansbury, 2003; Kennedy, Rubin, Hastings, & Maisel, 2004; Moore & Calkins, 2004; Porter, 2003). For example, several studies indicate that mother infant co-regulated communication patterns and more responsive parenting is positively related to good vagal regulation, and maternal intrusiveness and restrictive parenting is negatively related to such regulation (Calkins et al., 1998; Haley & Stansbury, 2003; Kennedy, Porter, 2003; Kennedy et al., 2004). And, infants who share more mutual affect regulation with their mothers (dyads that demonstrated more matched affect and synchrony of affective states) were more effective in their physiological regulation across a stress-inducing still-face paradigm (Moore & Calkins, 2004). Little research, however, has explored the longer term effects of maternal behavior during the toddler period when important developments in the regulation of affect and behavior are emerging.
One final issue that has yet to be addressed systematically in any study is the degree to which children's physiological regulation is influenced by the presence of a supportive caregiver versus the degree to which such parenting effects generalize to contexts in which the child must regulate independently. It may be that positive maternal-child relationships in toddlerhood facilitate the acquisition of vagal regulation (Calkins et al., 1998), but that this effect is most pronounced in contexts in which the child is engaged in a collaborative activity with the mother versus engaged in a solitary task (Calkins & Keane, 2004). Or, it may be that a relationship that is not facilitative or harmonious results in dysregulated physiological functioning when the mother is present and that exposure to this type of interaction, over time, compromises the integrity of the physiological system that must support well-regulated behavior when the child is challenged to function independently. While prior work has shown that on average, children display greater physiological regulation in the presence of a caregiver, such functioning may vary depending on the degree of support the child is accustomed to receiving from the caregiver.
The broad goal of the current study was to examine the role of mother-child relationship quality on the development of physiological regulation in young children. We examined this predictor from the toddler period, as this is a period of rapid growth in self-regulatory abilities (Kopp, 1982), to the early childhood period, when physiological regulation has been demonstrated to support more sophisticated emotional and cognitive self-regulation skills (Calkins & Keane, 2004). Prior research indicates that there are concurrent relations between externalizing spectrum behavior problems and physiological regulation across childhood (Calkins, 1997; Calkins et al., 2007; El-Sheikh, Harger, & Whitson, 2001) and between maternal positive and negative behavior and vagal regulation (Calkins et al., 1998). In this study we examined whether the quality of the maternal-child relationship during toddlerhood (indexed by maternal behavior characterized by low hostility, high positive affect and responsiveness, and low stress attributed to the maternal-child relationship) would affect physiological regulation at age 5, beyond the effects of prior and current levels of behavioral functioning. The current study also controlled for early physiological regulation to ensure that the effects of the maternal-child relationship on the development of physiological regulation are above and beyond the effects of prior regulation skills. Based on prior work in the temperament (Crockenberg & Leerkes, 2006) and stress/maltreatment literature (Gunnar & Donzella, 2002) which suggests that the effects of maternal behavior on children's development are most notable when conditions are aversive or very favorable, we expected that the effects of the maternal-child relationship on physiological regulation would be most readily seen in children experiencing either very low or very high levels of such a relationship. Finally, we examined whether the effect of relationship quality would vary depending on the context of the regulation (i.e., whether the child was faced with a challenge alone versus when in a situation with maternal support), with greater physiological regulation hypothesized to occur in the context of maternal support.
Methods
Participants
The current sample used data from three cohorts of children who were part of an ongoing longitudinal study. The 2-year and 5-year laboratory assessments were the focus of the current study. The goal for recruitment was to obtain a sample of children who were at risk for developing future externalizing behavior problems and who were representative of the surrounding community in terms of race and socioeconomic status (SES). All cohorts were recruited through child day care centers, the County Health Department, and the local Women, Infants, and Children (WIC) program. Potential participants for cohorts 1 and 2 were recruited at 2-years of age (cohort 1: 1994-1996 and cohort 2: 2000-2001) and screened using the Child Behavior Checklist (CBCL 2-3; Achenbach, 1992) completed by the mother to over-sample for externalizing behavior problems. Children were identified as being at risk for future externalizing behaviors if they received an externalizing T-score of 60 or above. Efforts were made to obtain approximately equal numbers of males and females. A total of 307 children were selected for Cohorts 1 and 2. Cohort 3 was initially recruited when infants were 6-months of age (in 1998) for their level of frustration based on laboratory observation and parent report and followed through the toddler period (See Calkins, Dedmon, Gill, Lomax, & Johnson, 2002, for more information). Children whose mother's completed the CBCL at 2-years of age were included in the current study (n = 140). Of the entire sample (N = 447; 215 males), 37% of the children were identified as being at risk for future externalizing problems. There were no significant demographic differences between cohorts with regard to gender, χ2 (2, N = 447) = .63, p = .73, minority status, χ2 (2, N = 447) = 1.13, p = .57, or 2-year SES, F (2, 444) = .53, p = .59. Cohort 3 had a significantly lower average 2-year externalizing T-score (M = 50.36) compared to cohorts 1 and 2 (M = 54.49), t (445) = -4.32, p = .01.
Of the 447 original screened participants from the three cohorts, 6 were dropped because they did not participate in any 2-year data collection. At 5 years of age 365 families participated. Families lost to attrition included those who could not be located, who moved out of the area, who declined participation, and who did not respond to phone and letter requests to participate. There were no significant differences between families who did and did not participate in the 5-year assessment in terms of gender, χ2 (1, N = 447) = .76, p = .38, minority status, χ2 (1, N = 447) = .17, p = .68, 2-year socioeconomic status, t (424) = 1.93, p = .06), and 2-year externalizing T-score (t (445) = -1.73, p = .09). Sixty-seven percent were European American, 27% were African American, 4% were biracial, and 2% were Hispanic. At age 2, the children were primarily from intact families (81%), 84% of the mothers had at least some college or higher education, and families were economically diverse with Hollingshead (1975) scores ranging from 14 to 66 (M = 39.63).
Procedures
Laboratory assessments
When children were 2 ½ years old, they were asked to come to the laboratory with their mothers for a 2-hour assessment examining children's regulatory functioning during various tasks and mother-child interactions. All interactions and tasks were videotaped through a one-way mirror. Three mother-child interaction tasks were examined from this assessment. These tasks included a teaching task, in which mothers were asked to teach their children to complete a shape puzzle (4 min for cohorts 1 and 2; 3 min for cohort 3); a free-play task, in which mothers and their children were asked to play as they normally would at home with a Sesame Street toy farm set (4 min); and a compliance task, in which mothers were asked to tell their children to clean up the toys from the free-play task (2 min). Mothers were also asked to complete several questionnaires during this visit as well as during the 5-year visit.
Cardiac measures were derived during the same laboratory assessment when children were 2 ½ years old and then again at 5 ½ years old. First, the experimenter placed three disposable pediatric electrodes in an inverted triangle pattern on the child's chest while the mother was seated at a table next to the mother. The electrodes were connected to a preamplifier, the output of which was transmitted to a vagal tone monitor (VTM-I, Delta Biometrics, Inc, Bethesda, MD) for R-wave detection. The vagal tone monitor displayed ongoing heart rate (HR) and computed and displayed an estimate of respiratory sinus arrhythmia (RSA; vagal tone) every 30 seconds. A data file containing the interbeat intervals (IBIs) for the entire period of collection was transferred to a laptop computer for later artifact editing (resulting from child movement) and analysis. The onset and end of each challenge episode was marked on the computer file of the IBI data through the use of an electronic signal controlled by the experimenter. While connected to the HR collection equipment, the child was observed during a multiepisode sequence derived from the Laboratory Temperament Assessment Battery (LAB-TAB; Goldsmith & Rothbart, 1993) and methods used in prior work (Calkins, 1997; Calkins & Keane, 2004; Kochanska, Murray & Coy, 1997).
Both the two year and five year assessment started with a baseline episode, consisting of a 5-minute segment of the videotape “Spot,” a short story about a puppy exploring a neighborhood. Although this episode was not a true baseline measure as the child's attention was engaged in an external stimulus, it was able to keep the child sitting quietly and displaying little affect. Given the age of the children, such a stimulus was necessary to keep the child seated at the table and to limit movement artifact in the HR data. Following the baseline episode, the child was observed in several situations designed to elicit physiological stress and coping. These tasks were standardized and the order of administration remained the same for each child. Given that the children are engaging in repeated regulatory challenges, it was necessary to separate each challenge episode from the subsequent episode by a very brief (2-3 min) period during which the child was free to interact with the mother while the experimenter gathered materials for the next episode. This break period ensured that children's physiological regulation during the tasks were not a result of fatigue and lessened the chance of a task order effect. Additionally, this break was necessary because the children's tolerance for the heart rate collection (and in particular, remaining seated for collection) was often low. This break was not considered to be an additional resting measure of cardiac activity with which to contrast the subsequent challenge episode given that the child was almost always engaged with the mother or was moving around (or both). Moreover, there was some concern that there would be carry-over effects from the episode to the break that would call into question the validity of using the break to derive resting measures. For these reasons, only the initial baseline measure was considered for analyses involving contrasts with the challenge episodes.
For the 2-year assessment, the challenge tasks included a positive task (2 minutes), in which the experimenter and the child blew bubbles together; a fear task (2 minutes), in which the experimenter tried to get the child to play with a toy spider; a teaching task (4 minutes), in which mothers were asked to help their children complete a simple puzzle; an empathy task (2 minutes), in which the child hears a tape of a crying child; and a frustration task (2 minutes), in which the child is given a container with cookies in it that cannot be opened. A subsample of children also completed an attention task (2 minutes), in which they were asked to watch a powerpoint presentation slide show, and a building task (5 minutes), in which they were asked to take turns while building a tower with the examiner.
For the 5-year assessment and of interest to the present study are the mother-child collaborative tasks (COL) and the independent challenge tasks (IN) which have been shown to yield variability in vagal suppression (Calkins & Dedmon, 2000; Stifter & Corey, 2001). The order of administration of these tasks was as follows: The first task was a 6-minute effortful control task (IN) designed to assess the child's ability to slow down gross and fine motor activity. The child was asked to draw some shapes (circles and stars) between boundary lines at varying speeds (regular, slow, and fast). Next, children completed a series of collaborative tasks including a teaching task (COL), in which mothers were asked to teach their children to make a toy puppet (6 min); an easy puzzle task (COL), in which mothers were asked to help their children complete a simple puzzle (2 min); and a difficult puzzle task (COL), in which mothers were asked to help their children complete a more difficult puzzle (4 min). Following these collaborative tasks, children completed a 4-minute effortful control task (IN) similar to a Stroop task. The child was presented with large pictures representing large shapes (e.g., animals, geometric figures). Within the larger pictures, smaller shapes were depicted. In half of the trials the small shapes were consistent with the large shape (e.g., a large cat was made up of identical smaller cats), and in the other half the shapes were inconsistent (e.g. large circle made up of small squares). The child was asked to identify only the smaller shapes in the pictures presented and were instructed to answer as fast as they could. The last episode was a 3-minute attentional persistence task (IN), during which the child was asked to sort a large number of beads by color and place them in a container (LAB-TAB; Goldsmith & Rothbart, 1993).
Measures
2-year Maternal Behavior
Global codes of positive maternal behavior and hostility were adapted from the Early Parenting Coding System (Winslow, Shaw, Bruns, & Kiebler, 1995). Behaviors coded included warmth/positive affect (displaying positive affect and warmth toward the child), sensitivity/responsiveness (promptly and appropriately responding to the child's bids to her), and hostility (emotional expressions of anger toward the child). Each behavior was coded once for each episode on a 4-point scale (1 = low to 4 = high). Four coders trained on 10% of the videotaped sessions and independently coded another 10% for reliability. The adjusted Kappas for global codes were all above .70. In addition to these global codes, maternal statements were also coded for Child oriented goals, statements in which the mother attempted to maintain or encourage the child's ongoing behavior and activities. The duration of episodes varied across dyad, so the sum of child-oriented statements was standardized for each participant by dividing the total number of statements by the total time of the episode and multiplying this value by the expected time of the episode (teaching: 4 minutes, freeplay: 4 minutes, cleanup: 2 minutes). Coding of child oriented goals has been used in previous research to predict childhood functioning (Smith, Calkins, Keane, Anastopoulos, & Shelton, 2004). Finally, behaviors indicative of directiveness and mother-oriented goals were also coded, but these measures have been found in prior work to be correlated with both positive and negative maternal behavior (Smith et al., 2004), so they were not included in these analyses.
The child-oriented goals and the global codes were each averaged across episodes. A maternal positive behavior composite was created by standardizing and summing the average child-oriented goals, global warmth/positive affect score, and global sensitivity/responsiveness score (Cronbach's α = .82). In addition to the maternal positive behavior composite, the global code for maternal hostility was examined as an index of relationship quality. However, due to the low occurrence of maternal hostility, we chose to examine this variable as a categorical variable that indicated whether or not hostility was observed.
2-year Parenting Stress
During the 2-year assessment mothers reported on their parenting stress by completing the Parenting Stress Index/Short Form (PSI; Abidin, 1995). The PSI contains 36 items rated on a 1 (strongly disagree) to 5 (strongly agree) scale. Total Parenting Stress is comprised of items assessing parental distress, stress related to parent-child interactions, and stress related to the child's behavior. The Parent-Child Dysfunctional Interaction subscale was the focus of the current study. This subscale includes 12 items assessing stress associated with parent-child interactions. Test-retest reliability for the Parent-Child Dysfunctional Interaction subscale over a 6-month period was found to be .68 (Abidin, 1995). Cronbach's alpha for the current study was .78.
2-year and 5-year Child Behavior Problems
Mother-reported, 2-year and 5-year externalizing and internalizing behavior measured by the Child Behavior Checklist (CBCL 2-3; Achenbach, 1992 and CBCL 4-18; Achenbach, 1991) were used as control variables. The minor subscales of aggression and delinquency comprise the overall Externalizing subscale and include items such as “argues a lot,” “gets in many fights,” and “destroys his/her own things.” The Internalizing subscale includes the minor subscales of anxious/depressed behavior, withdrawn behavior, and somatic complaints (e.g., “shy or timid,” “too fearful or anxious,” “overtired”). Each item was rated on a 3-point scale. The CBCL 2-3 and 4-18 have been found to be valid and reliable (Achenbach, 1991; Achenbach & Rescorla, 2001). For the CBCL 2-3, one week-test reliability was found to be .84 for the Externalizing subscale and .87 for the Internalizing subscale (Achenbach, 1992). For the CBCL: 4-18, one-week test-retest reliability was .93 for the Externalizing subscale and .89 for the Internalizing subscale (Achenbach, 1991). Cronbach's alphas for all items on the Externalizing and Internalizing subscales in the current study ranged from α = .85 to α = .90, respectively.
2-year and 5-year Cardiac Measures
Two types of physiological measures were derived from the laboratory assessments. These were: cardiac vagal regulation measures (RSA and RSA change), and heart period measures (HP and HP change). To generate measures of cardiac activity to derive measures of resting RSA (baseline vagal tone) and RSA suppression (baseline vagal tone - challenge vagal tone = vagal regulation), the interbeat interval (IBI) files were edited and analyzed using MXEDIT software (Delta Biometrics, Bethesda, MD). Editing the files consisted of scanning the data for outlier points relative to adjacent data and replacing those points by dividing them or summing them so that they would be consistent with the surrounding data. Data files that required editing of more than 5% of the data were not included in the analyses.
Estimates of RSA were calculated using Porges' (1985) method to analyze the IBI data. This method applies an algorithm to the sequential heart period data. The algorithm uses a moving 21-point polynomial to detrend periodicities in heart period (HP) slower than RSA. A band-pass filter then extracts the variance of HP within the frequency band of spontaneous respiration in young children, 0.24-1.04 Hz. Although lower frequency bands may be studied, research with young children has consistently examined this band and identified associations to child functioning (Huffman, et al., 1998; Porges et al., 1996; Stifter & Fox, 1990). The estimate of RSA was derived by calculating the natural log of this variance and is reported in units of ln(msec)2. Heart period and RSA was calculated every 30 seconds for the 5 minute baseline period and all other challenge episodes greater than 3 minutes in length. The mean estimate of HP and RSA of the 30 sec epochs within each episode was used in subsequent analyses. If the standard deviation across the epochs was greater than 1.00 for RSA (indicating a high degree of variability over the course of the episode and calling into question the validity of the mean RSA value), that episode was excluded from subsequent analyses (n = 5). Children with excluded RSA episodes due to a high degree of variability did not differ in terms of demographic variables compared to children with complete RSA data. Descriptive statistics for RSA and HP for the baseline and challenge episodes are reported in Tables 1 and 2.
Table 1. Descriptive statistics for 2-year RSA, RSA change, HP, and HP change variables.
| M | SD | Min | Max | N | |
|---|---|---|---|---|---|
| 2-year RSA | |||||
| Baseline RSA | 5.45 | 1.28 | 1.10 | 8.79 | 352 |
| Positive RSA | 4.98 | 1.18 | .48 | 8.93 | 328 |
| Fear RSA | 4.89 | 1.15 | 1.67 | 8.18 | 338 |
| Teaching RSA | 4.64 | 1.14 | 1.49 | 8.11 | 344 |
| Empathy RSA | 5.07 | 1.18 | 2.14 | 8.30 | 341 |
| Frustration RSA | 4.89 | 1.16 | 1.45 | 8.57 | 336 |
| Attention RSA | 4.98 | .98 | 2.42 | 7.82 | 83 |
| Block Tower RSA | 4.62 | 1.06 | 1.59 | 7.61 | 70 |
| 2-year RSA change | |||||
| Positive RSA | .49 | .77 | -2.14 | 3.22 | 320 |
| Fear RSA | .57 | .81 | -2.08 | 4.01 | 332 |
| Teaching RSA | .83 | .75 | -1.19 | 3.03 | 337 |
| Empathy RSA | .39 | .76 | -2.57 | 2.88 | 336 |
| Frustration RSA | .60 | .75 | -1.92 | 3.10 | 329 |
| Attention RSA | .28 | .53 | -.82 | 1.59 | 82 |
| Block Tower RSA | .62 | .73 | -.97 | 3.08 | 67 |
| 2-year HP | |||||
| Baseline HP | 547.24 | 52.33 | 373.57 | 721.18 | 352 |
| Positive HP | 519.53 | 45.39 | 406.08 | 652.86 | 328 |
| Fear HP | 517.43 | 47.01 | 353.18 | 684.20 | 338 |
| Teaching HP | 517.26 | 44.04 | 393.13 | 691.96 | 343 |
| Empathy HP | 527.96 | 46.51 | 389.19 | 723.65 | 341 |
| Frustration HP | 516.96 | 46.78 | 359.92 | 694.20 | 336 |
| Attention HP | 531.36 | 43.41 | 403.02 | 650.94 | 83 |
| Block Tower HP | 514.21 | 37.79 | 400.57 | 595.79 | 70 |
| 2-year HP change | |||||
| Positive HP | 27.45 | 31.87 | -116.51 | 163.52 | 320 |
| Fear HP | 30.16 | 32.01 | -110.84 | 190.56 | 332 |
| Teaching HP | 30.43 | 25.49 | -50.82 | 124.28 | 336 |
| Empathy HP | 19.56 | 28.05 | -98.87 | 124.04 | 336 |
| Frustration HP | 31.32 | 29.03 | -87.83 | 120.50 | 329 |
| Attention HP | 15.93 | 21.61 | -34.04 | 62.90 | 82 |
| Block Tower HP | 33.91 | 23.68 | -8.79 | 102.13 | 67 |
RSA= respiratory sinus arrhythmia, HP = heart period
a Positive change scores indicate a decrease in RSA or HP from baseline to task (i.e., RSA or HP suppression)
Table 2. Descriptive statistics for 5-year RSA, RSA change, HP, and HP change.
| M | SD | Min | Max | N | |
|---|---|---|---|---|---|
| 5-year RSA | |||||
| Baseline RSA | 6.08 | 1.15 | 3.28 | 9.42 | 296 |
| Teaching RSA (COL) | 5.51 | 1.08 | 2.89 | 8.51 | 290 |
| Easy Puzzle RSA (COL) | 5.48 | 1.15 | 2.68 | 8.90 | 288 |
| Difficult Puzzle RSA (COL) | 5.49 | 1.10 | 2.34 | 9.00 | 293 |
| Effortful Control #1 RSA (IN) | 6.09 | 1.13 | 3.09 | 9.09 | 293 |
| Effortful Control #2 RSA (IN) | 5.87 | 1.18 | 3.01 | 8.80 | 291 |
| Attentional Persistence RSA (IN) | 5.57 | 1.13 | 2.72 | 8.85 | 288 |
| 5-year RSA change | |||||
| Teaching Task (COL) | .56 a | .69 | -2.88 | 3.10 | 290 |
| Easy Puzzle (COL) | .59 | .78 | -2.51 | 3.26 | 288 |
| Difficult Puzzle (COL) | .59 | .73 | -3.17 | 3.23 | 292 |
| Effortful Control #1 (IN) | -.02 | .55 | -2.88 | 2.05 | 293 |
| Effortful Control #2 (IN) | .20 | .77 | -3.47 | 3.34 | 290 |
| Attentional Persistence (IN) | .49 | .78 | -3.02 | 3.24 | 287 |
| 5-year HP | |||||
| Baseline HP | 642.82 | 70.88 | 501.90 | 913.56 | 296 |
| Teaching HP (COL) | 589.61 | 57.96 | 478.39 | 822.43 | 290 |
| Easy Puzzle HP (COL) | 598.83 | 60.18 | 477.67 | 849.77 | 288 |
| Difficult Puzzle HP (COL) | 595.78 | 60.23 | 465.30 | 838.35 | 293 |
| Effortful Control #1 HP (IN) | 626.62 | 66.94 | 487.45 | 893.86 | 293 |
| Effortful Control #2 HP (IN) | 621.83 | 64.46 | 489.89 | 862.02 | 291 |
| Attentional Persistence HP (IN) | 595.75 | 59.75 | 473.35 | 798.23 | 288 |
| 5-year HP change | |||||
| Teaching HP (COL) | 53.70 | 29.80 | -14.59 | 198.63 | 290 |
| Easy Puzzle HP (COL) | 43.63 | 33.17 | -38.42 | 171.38 | 288 |
| Difficult Puzzle HP (COL) | 46.41 | 31.37 | -23.88 | 189.41 | 292 |
| Effortful Control #1 HP (IN) | 15.95 | 25.00 | -53.60 | 133.82 | 293 |
| Effortful Control #2 HP (IN) | 20.04 | 35.07 | -75.39 | 176.32 | 290 |
| Attentional Persistence HP (IN) | 46.05 | 35.93 | -54.30 | 195.11 | 287 |
RSA= respiratory sinus arrhythmia, HP = heart period, COL = collaborative tasks, IN = independent tasks,
a Positive change scores indicate a decrease in RSA or HP from baseline to task (i.e., RSA or HP suppression)
As the table indicates, the data files of several children were not included in some of the analyses. Several situations led to missing data across the laboratory tasks. A few children would not allow the experimenter to apply the HR electrodes. In other situations, the HR data collection equipment failed. A third explanation for missing data was that the child pulled on, or touched, the HR leads at the beginning of the collection procedure, which caused excessive movement artifact affecting greater than 5% of the data in the HR file, thus not allowing appropriate editing. A comparison of children with missing HR data from those without missing data revealed that these children did not differ in terms of demographic variables.
Vagal regulation scores indexed by change scores were computed for each challenge episode by subtracting the challenge episode RSA from the baseline RSA. These change scores are also reported in Tables 1 and 2. Consistent with previous research methodology (Blair & Peters, 2003; Calkins & Keane, 2004; Porges et al., 1996), positive change scores indicate a decrease in RSA from baseline to task (i.e., RSA suppression or vagal withdrawal). Because initial or baseline levels of RSA are predictive of change scores of RSA, these initial levels were covaried. Likewise, HP change scores were calculated by subtracting the challenge episode HP from baseline HP. Initial levels of HP were covaried due to their correlation with HP change scores. It is also important to note that an examination of Tables 1 and 2 demonstrate that a task order effect was not present as children's RSA suppression varied from task to task.
Results
Preliminary Analysis
Descriptive statistics
Descriptive statistics for the study variables are presented in Tables 1, 2, and 3. Preliminary analyses examined whether there were any relations between sex, race, maternal education, or SES and the 2- and 5-year physiological measures of baseline and task RSA and HP as well as 2- and 5-year behavior problems. There were no significant sex, race, or SES differences in the 2- or 5-year physiological and behavioral measures.
Table 3. Descriptive statistics for behavioral measures.
| M | SD | Min | Max | N | |
|---|---|---|---|---|---|
| 2-year Maternal Hostility (L) | .11 | .31 | 0 | 1.00 | 428 |
| 2-year Maternal Positive Behavior Composite (L) | .00 | 2.57 | -7.94 | 5.14 | 428 |
| 2-year Parent-Child Dysfunctional Interaction (P) | 20.23 | 6.08 | 12 | 46 | 418 |
| 2-year Externalizing T-Score (P) | 53.15 | 9.79 | 30 | 91 | 447 |
| 2-year Internalizing T-Score (P) | 48.96 | 9.94 | 30 | 90 | 447 |
| 5-year Externalizing T-Score (P) | 51.70 | 10.28 | 30 | 79 | 341 |
| 5-year Internalizing T-Score (P) | 47.29 | 9.81 | 33 | 82 | 341 |
(L) = laboratory measure, (P) = parent questionnaire measure
Maternal-child relationship quality
The current study used three indicator variables—maternal hostility, maternal positive behavior, and stress due to parent-child dysfunctional interaction—to generate a maternal-child relationship quality variable. The three indicator variables were standardized via Z scores with the negative indicators (i.e., maternal hostility and stress due to parent-child dysfunctional interaction) being reversed scored. These standardized scores were then averaged and re-standardized to create a single measure of maternal-child relationship quality with higher scores indicating a positive maternal-child relationship quality. Given the current study's hypotheses that the effects of the maternal-child relationship on physiological regulation would be most readily seen for children experiencing either very low or very high levels of such relationship, a quartile split was conducted and follow up analyses compared children who were in upper 25th percentile in their maternal-child relationship quality score, referred to as the High Maternal-Child Relationship Quality group (n = 107), to children falling below the 25th percentile, referred to as the Low Maternal-Child Relationship Quality group (n = 107). It is important to point out that the physiological regulation data was not available on every child. Thus, despite using all available data, the sample size varied across analyses due to the multiple measures being used.
Next, follow up analyses were conducted to determine whether children in the Low versus High Maternal-Child Relationship Quality groups differed in terms of demographic variables. Children in the High Maternal-Child Relationship Quality group were more likely to come from higher SES families, F(1, 203) = 24.19, p<.001; M = 42.30, SD = 10.40, and had mothers with higher levels of education, F(1, 204) = 34.62, p<.001; M = 3.75, SD = .90, compared to children in the Low Maternal-Child Relationship Quality group (M = 34.81, SD = 11.38 and M = 2.95, SD = 1.06, respectively). Due to such relations, SES and maternal education were covaried in our main analyses. Lastly, chi-square analyses were conducted to determine whether the distribution of maternal-child relationship groups differed based on children's sex or race. No differences were found in regards to sex. Thus, boys and girls had a relatively equal chance of being in the low or high maternal-child relationship quality group. We did find a significant difference in the distribution of maternal-child relationship groups based on children's racial groups, χ2 (1, N= 214) = 33.39, p < .001. Due to the low number of children classified as biracial or Hispanic, these analyses compared children who were Caucasian versus Minority. Examination of the observed versus expected frequencies indicated that Caucasian children were more likely to be classified in the high maternal-child relationship quality group, χ2 (1, N= 87) = 6.32, p < .05 and less likely to be classified in the low maternal-child relationship quality group than expected by chance χ2 (1, N= 46) = 6.32, p < .05. Minority children, however, were more likely to be classified in the low maternal-child relationship quality profile than expected by chance, χ2 (2, N= 61) = 6.32, p < .05, and were less likely to be classified in the high maternal-child relationship quality profile than expected by chance, χ2 (1, N= 20) = 6.32, p < .05. Due to these findings, race was covaried in our main analyses.
Maternal-Child Relationship Quality Groups and differences in RSA change
To investigate whether the maternal-child relationship quality groups predicted children's vagal regulation, a repeated measures ANOVA was conducted using the general linear model. The dependent variables were RSA change scores (i.e., vagal regulation) across the 6 laboratory tasks. Because initial or baseline levels of RSA are predictive of change scores of RSA, these initial levels were covaried. The context of such regulation (collaborative vs. independent) was also examined as a within-subjects factor. The maternal-child relationship groups were the between subjects variables. To ensure that children's vagal regulation was not due to earlier or concurrent behavior problems, 2-year and 5-year externalizing and internalizing problems were also entered as covariates. Race, SES, and maternal education levels were also covaried due to our earlier findings. Lastly, because we were interested in whether early maternal-child relationship exerts an effect on children's physiological regulation development, it was important to control for earlier levels of physiological regulation that may predict later regulation. Thus, children's 2-year baseline RSA as well as their average levels of 2-year vagal regulation (i.e., RSA change scores) were covaried. It is important to note that children's average levels of 2-year vagal regulation scores were used due to the fact that the laboratory tasks during the 2-year and 5-year assessments differed. There were not any statistically significant differences between children's RSA suppression across the 2-year laboratory tasks indicating that using a mean level of RSA suppression would be an appropriate way to control for early regulation. In addition, the formation of the mother-child relationship quality groups did not seem to be influenced by children's early physiological regulation as they were not statistically related.
In terms of the effects of the covariates, 2-year baseline RSA and 2-year average RSA change scores significantly predicted change scores of RSA at 5 years, F (1, 87) = 4.37, p < .05, partial eta-squared = .05 and F (1, 87) = 8.17, p < .01, partial eta-squared = .09, respectively. Thus, higher baseline levels of RSA and higher average change scores of RSA (i.e., vagal suppression or regulation) at 2 years were associated with greater levels of RSA suppression at 5 years. Baseline RSA at 5 years was also a significant predictor of change scores of RSA at 5 years, F (1, 87) = 23.04, p < .001, partial eta-squared = .21. This indicates that higher baseline levels of RSA at 5 years were associated with greater levels of RSA suppression at 5 years. Concurrent 5-year externalizing problems were also predictive of children's RSA suppression, F (1, 87) = 6.70, p < .05, partial eta-squared = .07. Specifically, children displaying higher levels of 5-year externalizing problems had lower levels of RSA suppression at 5 years. None of the other covariates (race, maternal education, SES, 2-year externalizing and internalizing problems, and concurrent 5-year internalizing problems) were significantly associated with RSA suppression.
This analysis also revealed a main effect of the context (collaborative vs. independent) on children's RSA suppression, F(1, 87) = 83.62, p<.001, partial eta-squared = .49. As seen in Figure 1, children displayed significantly greater levels of RSA suppression during collaborative tasks (estimated marginal M = .571, SE = .055) than during independent challenge tasks (estimated marginal M = .240, SE = .048). There was also a significant main effect of maternal-child relationship profiles, F (1, 87) = 5.72, p < .05, partial eta-squared = .06, on the measures of RSA change. Specifically, children in the Low Maternal-Child Relationship Quality group had significantly lower RSA suppression across all the laboratory tasks (estimated marginal M = .258 SE = .077) compared to children in the High Maternal-Child Relationship Quality group (estimated marginal M = .553, SE = .080). Lastly, the interaction effect between context and maternal-relationship quality on children's RSA suppression was not significant. This null finding indicates that children displayed significantly greater levels of RSA suppression during collaborative tasks than during independent challenge tasks, regardless of whether they were in the High or Low Maternal-Child Relationship Quality group.
Figure 1.
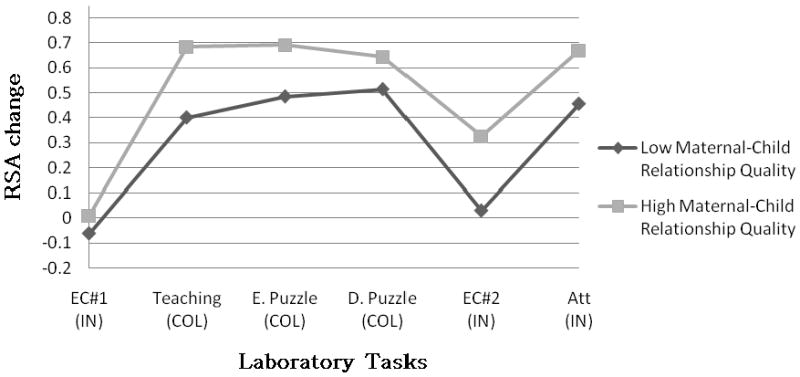
RSA change scores for maternal-child relationship quality groups. RSA = respiratory sinus arrhythmia; positive change scores indicate greater decrease from baseline to task or vagal suppression. EC#1 = effortful control task 1, E. Puzzle = easy puzzle, D. Puzzle = difficult puzzle, EC#2 = effortful control task 2, Att = attention task. (IN) = independent tasks, (COL) = collaborative tasks.
Maternal-Child Relationship Quality Profiles and differences in HP change
To investigate whether the maternal-child relationship quality profiles predicted children's HP change, a repeated measures ANOVA was conducted using the general linear model. The dependent variables were HP change scores across the 6 laboratory tasks. Because initial or baseline levels of HP are predictive of change scores of HP, these initial levels were covaried. The context of such HR acceleration (collaborative vs. independent) was also examined as a within-subjects factor. The maternal-child relationship groups were the between subjects variables. Once again, to ensure that children's HP change was not due to earlier or concurrent behavior problems, 2-year and 5-year externalizing and internalizing problems were also entered as covariates. Race, SES, and maternal education levels were also covaried due to our earlier findings. Lastly, we controlled for earlier levels of HP (2-year baseline HP and 2-year HP change) that may predict later cardiac functioning.
In terms of the effects of the covariates, 5-year baseline HP significantly predicted change scores of HP at 5-years, F (1, 88) = 76.11, p < .001, partial eta-squared = .46. Thus, higher baseline levels of HP at 5 years was associated with greater levels of HP suppression (i.e., heart rate acceleration) at 5-years. Early HP suppression at 2 years was also a significant predictor of change scores of HP at 5 years, F (1, 88) = 7.22, p < .01, partial eta-squared = .08. This indicates that higher levels of HP suppression at 2 years was associated with greater levels of heart rate acceleration at 5 years. None of the other covariates (race, maternal education, SES, 2-year and 5-year externalizing and internalizing problems, and 2-year baseline HP) were significantly associated with HP change at 5 years.
Similar to the RSA suppression findings, this analysis also revealed a main effect of the context (collaborative vs. independent) on children's HP suppression, F(1, 88) = 146.42, p<.001, partial eta-squared = .63. Children displayed significantly greater levels of heart rate acceleration during collaborative tasks (estimated marginal M = 49.38, SE = 2.29) than on independent challenge tasks (estimated marginal M = 29.99, SE = 2.21). Finally, there was a significant main effect for maternal-child relationship groups, F (1, 88) = 9.70, p < .01, partial eta-squared = .10, on the measures of HP change. Specifically, children in the Low Maternal-Child Relationship Quality group had significantly lower heart rate acceleration across all the laboratory tasks (estimated M = 31.39 SE = 3.35) compared to children in the High Maternal-Child Relationship Quality profile (estimated M = 47.99, SE = 3.44).
Prior work (Calkins et al., 2007) has noted the importance of determining whether group differences in heart rate is a function of general levels of arousal in the autonomic nervous system or a function of differences in regulatory processes stemming from the parasympathetic nervous system (i.e., RSA withdrawal). Thus, to examine whether the HP change difference that was observed among the two maternal-child relationship quality groups was a function of the group difference in RSA withdrawal that was observed, a repeated measures ANOVA was conducted once again while controlling for RSA suppression as well as the other previously significant covariates (5-year baseline HP, 2-year HP suppression). This analyses revealed a significant effect of RSA suppression on HP suppression, F (1, 100) = 45.17, p<.001, partial eta-squared =.31. This indicates that higher levels of RSA suppression are associated with higher levels of heart rate acceleration. However, after controlling for the effects of RSA suppression, the maternal-child relationship quality groups no longer differed in terms of HP change, F(1,100) = 1.98, p>.05.
Discussion
The aim of this study was to examine mother-child relationship quality as one potential longitudinal predictor of children's physiological regulation, as indexed by vagal withdrawal to challenge. Prior research indicates that vagal withdrawal under conditions of emotional, cognitive, and behavioral challenge is an indicator of the degree of child coping and is related to other dimensions of child functioning (Calkins & Keane, 2004; El-Sheikh, 2005). Our rationale for examining maternal-child relationship quality as one predictor of such functioning was predicated on considerable prior work demonstrating the effects of caregiving on behavioral indices of self-regulation in humans (Calkins, 2004; Crockenberg & Leerkes, 2004) and on animal work demonstrating the multiple levels of influence of early caregiving (Polan & Hofer, 1999). We also examined whether the context of self-regulation, collaborative versus independent, would affect children's ability to engage in physiological regulation. We explored these issues in a large community sample of young children, some of whom were at elevated risk for externalizing behavior problems (Hill et al., 2006).
To generate an index of the quality of the relationship between mother and child during toddlerhood, we assessed that relationship using several types of interactions observed in the laboratory (maternal hostility and maternal positive behaviors) and by maternal report of the level of stress mothers indicated they experienced as a function of their perceived relationship with their children. Lower SES scores characterized the low quality relationship group. This finding is consistent with previous research indicating that less educated mothers are less likely to engage in parental behaviors characterized by warmth and responsivity (Klebanov, Brooks-Gunn, & Duncan, 1994) and are more likely to use greater control when interacting with their children (Sullivan & McGrath, 1999). Moreover, less educated mothers have been found to use less effective emotion regulation strategies in interacting with their children (Martini, Root, & Jenkins, 2004; Raviv, Kessenich, & Morrison, 2004; Sullivan & McGrath, 1999). Thus, the linkage between SES and poor relationship quality is to be expected in a community sample of children and mothers; the likely direction of effects is from low social and educational resources to lower quality interactions with children.
To address the effects of relationship quality on children's physiological functioning, we utilized a battery of tasks designed to challenge the child emotionally and behaviorally. Prior research has demonstrated that such tasks typically elicit a withdrawal of vagal influence to the heart that indicates the engagement of attention and that facilitates active coping (Calkins, 1997, El-Sheikh & Whitson, 2006). Prior work also suggests that children's behavioral functioning is supported by this physiological response and that children with poor physiological regulation, or lower levels of vagal withdrawal, display difficulty in managing emotions and behavior adaptively (Calkins & Dedmon, 2000; Calkins & Keane, 2004).
Two questions were of interest in examining these data. First, is the prior quality of the relationship predictive of the level of physiological regulation the child displays, above and beyond the effects of early and concurrent behavioral functioning as well as early physiological functioning? And, second, does this physiological response vary as a function of the presence of the caregiver, or does it generalize to situations in which the caregiver is absent? This issue is important because generalizability suggests that children's physiological response is not simply supported by the actual presence of the caregiver; the caregiver affects the child's functioning outside the dyad as well. Generalization, then, suggests a greater degree of impairment that will likely undermine functioning across a range of tasks and in a variety of situations.
Our findings revealed a main effect for maternal-child relationship quality such that children from dyads with greater levels of dysfunction displayed less physiological regulation to challenge than did children from low levels of dysfunction. Dyads in which mothers displayed greater hostility, less positive and responsive behavior, and that mothers characterized as stressful, displayed less vagal regulation and lower heart rate acceleration across all six challenge tasks. It is important to point out that after controlling for vagal regulation (i.e., RSA suppression) the maternal-child relationship quality groups no longer differed in terms of heart rate acceleration (i.e., HP change). This result has important theoretical implications as it indicates that the caregiver relationship does not simply affect children's general levels of arousal as indicated by HP change but rather more complex regulatory mechanisms stemming from the parasympathetic nervous system (i.e., RSA suppression). Moreover, the specification of the parasympathetic nervous system as the mechanism by which the caretaker relationship affects cardiac functioning is especially important given the current body of literature which clearly demonstrates that HR is multiply determined by sympathetic, parasympathetic, homeostatic and hormonal processes.
These findings also supported our hypothesis that supportive, warm relationships facilitate the acquisition of self-regulation skills at the biological level. There is a rich literature documenting the effects of parenting on children's behavior. Here we see evidence that these relationships have important effects at the physiological level that are observable across time. Our finding is particularly strong given that such effect was seen even after accounting for children's early physiological regulation abilities as well as early and concurrent behavioral difficulties. The possible mechanism of these effects is unclear, however. Whether children in dysfunctional relationships experience these relationships as disruptive to their own regulation because of less physical contact and soothing, or through a lack of positive engagement and modeling is unclear. Animal work (Polan & Hofer, 1999) suggests that caregiver behavior may translate regulatory skills through touch. Human work suggests that behavioral synchrony between caregiver and child has an effect as well (Feldman, 2006). More research is needed to understand the specific behaviors that affect physiological regulation in the context of parent-child interactions.
The current study also found that concurrent externalizing problems were related to lower physiological regulation across both collaborative and independent tasks. This finding is consistent with previous empirical (Calkins et al., 2007) and theoretical work (Keenan & Shaw, 2003) suggesting that children experiencing externalizing symptoms have significant difficulties regulating their emotions. It is also important to note that toddler's early physiological regulation abilities were a strong predictor of childhood physiological regulation. This finding is consistent with previous work demonstrating a modest degree of stability in physiological regulation across toddlerhood to age 4 (Calkins & Keane, 2004). Although cross-age comparisons are difficult to make on physiological regulation measures as they are confounded with the different task and task demands at each age, our findings illustrate that early physiological regulation abilities continue to exert a strong influence in subsequent regulation abilities through early childhood. It will be important for future research to examine developmental trajectories of physiological regulation. This type of research would enable the field to determine what factors distinguish children whose physiological regulation abilities increase over time from children whose physiological regulation abilities stay stable overtime as well as the consequences of such different trajectories.
The effect of context (collaborative versus independent) on physiological regulation was also observed. Specifically, children displayed higher levels of vagal withdrawal (i.e. suppression) and greater heart rate acceleration during tasks in which they were engaged with their mothers compared to when working independently. This effect was consistent across different levels of maternal-child relationship quality. Thus, it appears that children's physiological regulation is facilitated by a mere presence of their caretaker, regardless of the level of their relationship. This is not surprising given that the caretaker is an important and early source of assistance in helping children's regulate their emotions (Fox & Calkins, 2003; Kopp, 1989; Rothbart et al., 1992). This finding is also consistent with prior work in the toddlerhood period (Calkins & Keane, 2004) and expands the literature by documenting that even at 5.5 years of age, children rely heavily on their caretakers for regulation support. As children get older and develop other regulatory skills, the caretaker should theoretically play less of a role in facilitating their regulation. We may find that children with a history of high quality relationships with their caretakers are better able to shift their regulation abilities to independent contexts while children from poor relationships may be less equipped to regulate on their own. These findings underscore the need to facilitate positive parenting in toddlerhood and early childhood during which time physiological and behavioral skills necessary for independent and well-regulated behavior are emerging. Intervention and prevention programs aimed at such skills must acknowledge the important role of caregiver behavior in supporting and undermining biological processes that support such skills.
An important question unaddressed in this study is whether maternal-child relationship problems during toddlerhood are a function of child or maternal problems. That is, it is possible that the relationship effects observed in this study are a function of manifestations of child behavioral difficulties that are observable early and that affect parents' experiences and behaviors with their offspring. Recent work suggests that toddler behavior that is aversive, problematic, and normative affects caregiver's experience of stress in both the short (Calkins, 2002) and the long term (Williford, Calkins & Keane, 2007). It is possible that fundamental problems in physiological regulation lead to patterns of unpredictable, unmanageable, and difficult behavior that stresses the emerging parent-child relationship. Under conditions that exacerbate such stress, such as those that accompany social and economic challenge, normative child behavioral difficulties may lead to negative, hostile, and non-supportive parenting that undermines the acquisition of basic regulatory skills of the sort that are integral to adaptive functioning during early childhood.
This study has several limitations that must be acknowledged. First, the data were collected in very brief laboratory sessions. Questions about whether such brief observation periods allow for adequate characterization of children's responding and maternal behavior are unanswered. Second, children are influenced by the behaviors of caregivers other than mothers. Data on fathers may help illuminate the precise kinds of behaviors that affect children's biological functioning. Third, one important indicator of the quality of the mother-child relationship, security of attachment, was not assessed in this study. Patterns of mother-child attachment may or may not map onto the kinds of interactions and indices of relationship qualities that were observed in this study (Matas, Arend, & Sroufe, 1978). Finally, the effects of prior relationship quality observed in this study were relatively modest. However, it is important to note that these significant effects emerged even after controlling for early measures of physiological and behavioral functioning as well as concurrent levels of baseline vagal tone and behavioral measures of child functioning. Lingering questions remain about the extent to which these differing patterns of physiological functioning influence subsequent functioning, and the extent to which these may be influenced by numerous environmental factors.
Acknowledgments
This research was supported by National Institute of Mental Health awards (MH 55625 and MH 55584) to the first author and an NIMH award (MH 58144) to the first and fourth authors. The authors would like to thank Laura Lomax, Rachel Naas, Cynthia Smith, David Topor, Rachael Reavis, Caitlin Stone, and Michelle Wilkinson for their help in participant recruitment, data collection, and coding. The authors also thank the RIGHT Track families, who generously gave their time to participate in the study.
References
- Abidin RR. Manual for the parenting stress index. Odessa, FL: Psychological Assessment Resources; 1995. [Google Scholar]
- Achenbach TM. Integrative guide for the 1991 CBCL/4-18, YSR & TRF profiles. Burlington, VT: University of Vermont Department of Psychiatry; 1991. [Google Scholar]
- Achenbach TM. Manual for the child behavior checklist/2-3 & 1992 profile. Burlington, VT: University of VT Department of Psychiatry; 1992. [Google Scholar]
- Achenbach TM, Rescorla LA. Manual for the ASEBA school-Age forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families; 2001. [Google Scholar]
- Beauchaine T. Vagal tone, development, and Gray's motivational theory: Toward an integrated model of autonomic nervous system functioning in psychopathology. Development and Psychopathology. 2001;13:183–214. doi: 10.1017/s0954579401002012. [DOI] [PubMed] [Google Scholar]
- Baumeister RF, Vohs KD. Handbook of self-regulation: Research, theory, and application. New York: The Guilford Press; 2004. [Google Scholar]
- Blair C. Behavioral inhibition and behavioral activation in young children: Relations with self-regulation and adaptation to preschool children attending Head Start. Developmental Psychobiology. 2003;42:301–311. doi: 10.1002/dev.10103. [DOI] [PubMed] [Google Scholar]
- Blair C, Peters R. Physiological and neurocognitive correlates of adaptive behavior in preschool among children in Head Start. Developmental Neuropsychology. 2003;24:479–497. doi: 10.1207/S15326942DN2401_04. [DOI] [PubMed] [Google Scholar]
- Bronson MB. Self-regulation in early childhood: Nature and Nurture. New York, NY: The Guilford Press; 2000. [Google Scholar]
- Calatayud F, Coubard S, Belzung C. Emotional reactivity may not be inherited but influenced by parents. Physiological Behavior. 2004;80:465–474. doi: 10.1016/j.physbeh.2003.10.001. [DOI] [PubMed] [Google Scholar]
- Caldji C, Tannenbaum B, Sharma S, Francis D, Plotsky PM, Meaney MJ. Maternal care during infancy regulates the development of neural systems mediating the expression of fearfulness in the rat. Neurobiology. 1998;9:5335–5340. doi: 10.1073/pnas.95.9.5335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calkins SD. Origins and outcomes of individual differences in emotional regulation. Fox NA, editor. Emotion regulation: Behavioral and biological considerations, Monographs of the Society for Research in Child Development (Nos. 2-3, Serial No. 240) 1994:53–72. [PubMed] [Google Scholar]
- Calkins SD. Cardiac vagal tone indices of temperamental reactivity and behavioral regulation in young children. Developmental Psychobiology. 1997;31:125–135. doi: 10.1002/(sici)1098-2302(199709)31:2<125::aid-dev5>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- Calkins SD. Early attachment processes and the development of emotional self-regulation. In: Baumeister R, Vohs K, editors. Handbook of self-regulation: Research, theory, and applications. New York: The Guilford Press; 2004. pp. 324–339. [Google Scholar]
- Calkins SD. The Emergence of Self-regulation: Biological and Behavioral Control Mechanisms Supporting Toddler Competencies. In: Brownell C, Kopp C, editors. Socioemotional Development in the Toddler Years. New York: The Guilford Press; 2007. pp. 261–284. [Google Scholar]
- Calkins SD. Regulatory competence and early disruptive behavior problems: The role of physiological regulation. In: Olson S, Sameroff A, editors. Regulatory processes in the development of behavior problems: Biological, behavioral, and social-ecological interactions. Cambridge: University Press; in press. [Google Scholar]
- Calkins SD, Dedmon SE. Physiological and behavioral regulation in two-year-old children with aggressive/destructive behavior problems. Journal of Abnormal Child Psychology. 2000;28:103–118. doi: 10.1023/a:1005112912906. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Dedmon S, Gill K, Lomax L, Johnson L. Frustration in infancy: Implications for emotion regulation, physiological processes, and temperament. Infancy. 2002;3:175–198. doi: 10.1207/S15327078IN0302_4. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Fox NA. Self-regulatory processes in early personality development: A multilevel approach to the study of childhood social withdrawal and aggression. Development and Psychopathology. 2002;14:477–498. doi: 10.1017/s095457940200305x. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Graziano PA, Keane SP. Cardiac vagal regulation differentiates among children at risk for behavior problems. Biological Psychology. 2007;74:144–153. doi: 10.1016/j.biopsycho.2006.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calkins SD, Hill AL. Caregiver influences on emerging emotion regulation: Biological and environmental transactions in early development. In: Gross J, editor. Handbook of emotion regulation. New York: The Guilford Press; 2007. pp. 229–248. [Google Scholar]
- Calkins SD, Keane SP. Cardiac vagal regulation across the preschool period: Stability, continuity, and implications for childhood adjustment. Developmental Psychobiology. 2004;45:101–112. doi: 10.1002/dev.20020. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Smith CL, Gill KL. Maternal interactive style across contexts: Relations to emotional, behavioral, and physiological regulation during toddlerhood. Social Development. 1998;7:350–369. [Google Scholar]
- Cassidy J. Emotion regulation: influences of attachment relationships. Monographs of the Society of Research in Child Development. 1994;59:228–249. [PubMed] [Google Scholar]
- Chambers A, Allen J. Cardiac vagal control, emotion, psychopathology, and health. Biological Psychology. 2007;74:113–115. doi: 10.1016/j.biopsycho.2006.09.004. [DOI] [PubMed] [Google Scholar]
- Champagne F, Meaney MJ. Like mother, like daughter: Evidence for non-genetic transmission of parental behavior and stress responsivity. Progressive Brain Research. 2001;133:287–302. doi: 10.1016/s0079-6123(01)33022-4. [DOI] [PubMed] [Google Scholar]
- Crockenberg S, Leerkes E. Infant and maternal behaviors regulate infant reactivity to novelty at 6 months. Developmental Psychology. 2004;40:1123–1132. doi: 10.1037/0012-1649.40.6.1123. [DOI] [PubMed] [Google Scholar]
- Crockenberg S, Leerkes E. Infant and maternal behavior moderate reactivity to novelty to predict anxious behavior at 2.5 years. Development and Psychopathology. 2006;18:17–34. doi: 10.1017/S0954579406060020. [DOI] [PubMed] [Google Scholar]
- Davidson R, Fox A, Kalin N. Neural bases of emotion regulation in nonhuman primates and humans. In: Gross J, editor. Handbook of emotion regulation. New York: The Guilford Press; 2007. pp. 47–68. [Google Scholar]
- Dayton CM. Latent class scaling analysis Quantitative Applications in the Social Sciences. Thousand Oaks, CA: Sage Publications; 1998. (126). [Google Scholar]
- DeGangi G, DiPietro J, Greenspan S, Porges SW. Psychophysiological characteristics of the regulatory disordered infant. Infant Behavior and Development. 1991;14:37–50. [Google Scholar]
- Doussard-Roosevelt J, Montgomery L, Porges S. Short-term stability of physiological measures in kindergarten children: Respiratory sinus arrhythmia, heart period, and cortisol. Developmental Psychobiology. 2003;43:230–242. doi: 10.1002/dev.10136. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Smith C, Sadovsky A, Spinrad T. Effortful control: Relations with emotion regulation, adjustment, and socialization in childhood. In: Baumeister R, Vohs K, editors. Handbook of self-regulation: Research, theory, and applications. New York: The Guilford Press; 2004. pp. 259–282. [Google Scholar]
- El-Sheik M. Stability of respiratory sinus arrhythmia in children and young adolescents. Developmental Psychobiology. 2005;46:307–317. doi: 10.1002/dev.20036. [DOI] [PubMed] [Google Scholar]
- El-Sheik M, Whitson S. Longitudinal relations between marital conflict and child adjustment: Vagal regulation as a protective factor. Journal of Family Psychology. 2006;20:30–39. doi: 10.1037/0893-3200.20.1.30. [DOI] [PubMed] [Google Scholar]
- Everitt B, Hand DJ. Finite mixture distributions. New York: Chapman & Hall; 1981. [Google Scholar]
- Feldman R. From biological rhythms to social rhythms: Physiological precursors of mother-infant synchrony. Developmental Psychology. 2006;42:175–188. doi: 10.1037/0012-1649.42.1.175. [DOI] [PubMed] [Google Scholar]
- Fox NA. Dynamic cerebral processes underlying emotion regulation. Fox NA, editor. Emotion regulation: Behavioral and biological considerations, Monographs of the Society for Research in Child Development (Nos. 2-3, Serial No. 240) 1994:152–166. [PubMed] [Google Scholar]
- Fox N, Calkins SD. The development of self-control of emotion: Intrinsic and extrinsic influences. Motivation and Emotion. 2003;23:7–26. [Google Scholar]
- Francis DD, Caldji C, Champagne F, Plotsky PM, Meaney MJ. The role of cortcotropin-releasing factor-norepinephrine systems in mediating the effects of early experience on the development of behavioral and endocrine responses to stress. Biological Psychiatry. 1999;46:1153–1166. doi: 10.1016/s0006-3223(99)00237-1. [DOI] [PubMed] [Google Scholar]
- Gilliom M, Shaw DS. Codevelopment of externalizing and internalizing problems in early childhood. Development and Psychopathology. 2004;16:313–333. doi: 10.1017/s0954579404044530. [DOI] [PubMed] [Google Scholar]
- Goldsmith HH, Rothbart MK. The laboratory temperament assessment battery (LAB-TAB) University of Wisconsin; 1993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gunnar MR. Social regulation of stress in early child development. In: McCartney K, Phillips D, editors. Blackwell handbook of early childhood development. Blackwell Publishing; 2006. pp. 106–125. [Google Scholar]
- Gunnar MR, Donzella B. Social regulation of the cortisol levels in early human development. Psychoneuroendocrinology. 2002;27:199–220. doi: 10.1016/s0306-4530(01)00045-2. [DOI] [PubMed] [Google Scholar]
- Haley D, Stansbury K. Infant stress and parent responsiveness: Regulation of physiology and behavior during still-face and reunion. Child Development. 2003;74:1534–1546. doi: 10.1111/1467-8624.00621. [DOI] [PubMed] [Google Scholar]
- Hill AL, Degnan KA, Calkins SD. Profiles of externalizing behavior problems for boys and girls across preschool: The roles of emotion regulation and inattention. Developmental Psychology. 2006;42:913–928. doi: 10.1037/0012-1649.42.5.913. [DOI] [PubMed] [Google Scholar]
- Hipp JR, Bauer DJ. Local solutions in the estimation of growth mixture models. Psychological Methods. 2006;11:36–53. doi: 10.1037/1082-989X.11.1.36. [DOI] [PubMed] [Google Scholar]
- Hollingshead AB. Four Factor Index of Social Status. Yale University; 1975. [Google Scholar]
- Howse RB, Calkins SD, Keane SP, Anastopoulos AD, Shelton TL. Regulatory contributors to children's kindergarten achievement. Early Education and Development. 2003;14:101–119. [Google Scholar]
- Huffman LC, Bryan Y, del Carmen R, Pederson F, Doussard-Roosevelt J, Porges S. Infant temperament and cardiac vagal tone: Assessments at twelve weeks of age. Child Development. 1998;69:624–635. [PubMed] [Google Scholar]
- Keenan K. Emotion dysregulation as a risk factor for child psychopathology. Clinical Psychology: Science and Practice. 2000;7:418–434. [Google Scholar]
- Keenan K, Shaw DS. Exploring the etiology of antisocial behavior in the first years of life. In: Lahey BB, Moffitt TE, Caspi A, editors. Causes of conduct disorder and juvenile delinquency. The Guilford Press; New York: 2003. pp. 153–181. [Google Scholar]
- Kennedy AE, Rubin K, Hastings P, Maisel B. Longitudinal relations between child vagal tone and parenting behavior: 2 to 4 years. Developmental Psychobiology. 2004;45:10–21. doi: 10.1002/dev.20013. [DOI] [PubMed] [Google Scholar]
- Klebanov P, Brooks-Gunn J, Duncan G. Does neighborhood and family poverty affect mothers' parenting, mental health, and social support? Journal of Marriage and the Family. 1994;56:441–455. [Google Scholar]
- Kochanska G, Murray K, Coy KC. Inhibitory control as a contributor to conscience in childhood: From toddler to early school age. Child Development. 1997;68:264–277. [PubMed] [Google Scholar]
- Kopp C. Antecedents of self-regulation: A developmental perspective. Developmental Psychology. 1982;18:199–214. [Google Scholar]
- Lahey B, Hart E, Pliska S, Applegate B, McBurnett R. Neurophysiological correlates of conduct disorder: a rationale and review of research. Journal of Clinical Child Psychology. 1993;22:141–153. [Google Scholar]
- Lewis MD. Self-organizing individual differences in brain development. Developmental Review. 2005;25:252–277. [Google Scholar]
- Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- Martini T, Root C, Jenkins J. Low and middle income mothers' regulation of negative emotion: Effects of children's temperament and situational emotional responses. Social Development. 2004;13:515–530. [Google Scholar]
- Matas L, Arend R, Sroufe A. Continuity of adaptation in the second year: The relationship between quality of attachment and later competence. Child Development. 1978;49:547–556. [Google Scholar]
- McCutcheon AC. Latent class analysis. Beverly Hills: Sage Publications; 1987. [Google Scholar]
- Moore G, Calkins SD. Infants' vagal regulation in the still-face paradigm is related to dyadic coordination of mother-infant interaction. Developmental Psychology. 2004;40:1068–1080. doi: 10.1037/0012-1649.40.6.1068. [DOI] [PubMed] [Google Scholar]
- Muthén B. Latent variable analysis: Growth mixture modeling and related techniques for longitudinal data. In: Kaplan D, editor. Handbook of quantitative methodology for the social sciences. Newbury Park, CA: Sage Publications; 2004. pp. 345–368. [Google Scholar]
- Muthén L, Muthén B. Mplus 4.1 user's guide. Los Angeles: Author; 2006. [Google Scholar]
- Polan, Hofer . Psychobiological origins of infant attachment and separation responses. In: Cassidy J, Shaver PR, editors. Handbook of attachment: Theory, research, and clinical applications. New York: Guilford Press; 1999. pp. 162–180. [Google Scholar]
- Porges SW. Method and apparatus for evaluating rhythmic oscillations in aperiodic physiological response systems. United States patent no. 4520944 1985
- Porges SW. Vagal tone: An autonomic mediator of affect. In: Garber J, Dodge KA, editors. The development of emotional regulation and dysregulation. Cambridge: Cambridge University Press; 1991. pp. 111–128. [Google Scholar]
- Porges SW. Physiological regulation in high-risk infants: A model for assessment and potential intervention. Development and Psychopathology. 1996;8:43–58. [Google Scholar]
- Porges SW. The polyvagal theory: Phylogenetic substrates of a social nervous system. International Journal of Psychophysiology. 2001;42:123–146. doi: 10.1016/s0167-8760(01)00162-3. [DOI] [PubMed] [Google Scholar]
- Porges SW. The polyvagal theory: Phylogenetic contributions to social behavior. Physiology and Behavior. 2003;79:503–513. doi: 10.1016/s0031-9384(03)00156-2. [DOI] [PubMed] [Google Scholar]
- Porges SW. The polyvagal perspective. Biological Psychology. 2007;74:116–143. doi: 10.1016/j.biopsycho.2006.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porges SW, Byrne EA. Research methods for measurement of heart rate and respiration. Biological Psychology. 1992;34:93–130. doi: 10.1016/0301-0511(92)90012-j. [DOI] [PubMed] [Google Scholar]
- Porges SW, Doussard-Roosevelt J, Portales L, Greenspan SI. Infant regulation of the vagal “brake” predicts child behavior problems: A psychobiological model of social behavior. Developmental Psychobiology. 1996;29:697–712. doi: 10.1002/(SICI)1098-2302(199612)29:8<697::AID-DEV5>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- Porter C. Coregulation in mother-infant dyads: links to infants' cardiac vagal tone. Psychological Reports. 2003;92:307–319. doi: 10.2466/pr0.2003.92.1.307. [DOI] [PubMed] [Google Scholar]
- Propper C, Moore G. The influence of parenting on infant emotionality: A multi-level psychobiological perspective. Developmental Review. 2006;26:427–460. [Google Scholar]
- Raine A. Autonomic nervous system activity and violence. In: Stoff DM, Cairns RB, editors. Aggression and Violence. Erlbaum; Hillsdale, NJ: 1996. pp. 145–168. [Google Scholar]
- Raine A, Venable P, Williams M. Relationship between CNS and ANS measures of arousal at age 15 and criminality at age 24. Archives of General Psychiatry. 1990;47:1003–007. doi: 10.1001/archpsyc.1990.01810230019003. [DOI] [PubMed] [Google Scholar]
- Raviv T, Kessenich M, Morrison F. A mediational model of the association between socioeconomic status and three-year-old language abilities: the role of parenting factors. Early Childhood Research Quarterly. 2004;19:528–547. [Google Scholar]
- Rothbart M, Sheese B. Temperament and emotion regulation. In: Gross J, editor. Handbook of emotion regulation. New York: The Guilford Press; 2007. pp. 331–350. [Google Scholar]
- Schafer JL, Graham JW. Missing Data: Our view of the state of the art. Psychological Methods. 2002;7:147–177. [PubMed] [Google Scholar]
- Shaw DS, Keenan K, Vondra J, Delliquadri E, Giovanelli J. Antecedents of preschool children's internalizing problems: A longitudinal study of low-income families. Journal of the American Academy of Child and Adolescent Psychiatry. 1997;36:1760–1767. [PubMed] [Google Scholar]
- Smith C, Calkins S, Keane SP, Anastopoulos A, Shelton T. Predicting stability and change in toddler behavior problems: Contributions of maternal behavior and child sex. Developmental Psychology. 2004;40:29–42. doi: 10.1037/0012-1649.40.1.29. [DOI] [PubMed] [Google Scholar]
- Sroufe L. Early relationships and the development of children. Infant Mental Health Journal. 2000;21:67–74. [Google Scholar]
- Stifter C, Corey J. Vagal regulation and observed social behavior in infancy. Social Development. 2001;10:189–201. [Google Scholar]
- Stifter CA, Fox NA. Infant reactivity: Physiological correlates of newborn and 5-month temperament. Developmental Psychology. 1990;26:582–588. [Google Scholar]
- Suess PE, Porges SW, Plude DJ. Cardiac vagal tone and sustained attention in school-age children. Psychophysiology. 1994;31:17–22. doi: 10.1111/j.1469-8986.1994.tb01020.x. [DOI] [PubMed] [Google Scholar]
- Sullivan M, McGrath M. Proximal and distal correlates of maternal control style. Western Journal of Nursing Research. 1999;21:313–334. doi: 10.1177/01939459922043901. [DOI] [PubMed] [Google Scholar]
- Williford A, Calkins S, Keane S. Predicting change in parenting stress across early childhood: child and maternal factors. Journal of Abnormal Child Psychology. 2007;35:251–263. doi: 10.1007/s10802-006-9082-3. [DOI] [PubMed] [Google Scholar]
- Wilson B, Gottman J. Attention--the shuttle between emotion and cognition: Risk, Resiliency, and physiological bases. In: Hetherington E, Blechman E, editors. Stress, coping and resiliency in children and families. Mahwah, N.J.: Lawrence Erlbaum Associates; 1996. [Google Scholar]
- Winslow EB, Shaw DS, Bruns H, Kiebler K. Parenting as a mediator of child behavior problems and maternal stress, support, and adjustment. Paper presented at the biennial meeting of the Society for Research in Child Development; Indianapolis, IN. 1995. [Google Scholar]