

Abstract
Anhedonia (lack of reactivity to pleasurable stimuli) and a negatively skewed view of the future are important components of depression that could affect economic decisions in depressed individuals. Delay discounting paradigms might be useful for probing putative affective and cognitive underpinnings of such decisions. As a first step to evaluate whether difficulties experiencing pleasure might affect delay discounting, 36 undergraduate students with varying levels of anhedonia performed a delay discounting task in which they made choices between a small immediate and larger future monetary reward. Increasing levels of anhedonia (Snaith-Hamilton Pleasure Scale) were negatively associated with delay discounting rate, indicating that anhedonic individuals tended to choose the larger, albeit delayed reward. These correlations remained after controlling for variables previously linked to delay discounting (working memory capacity and impulsivity) and pessimistic future-directed thinking. The current findings provide preliminary evidence indicating that anhedonic individuals make less myopic decisions about their future, possibly due to their decreased responsiveness to immediate rewards.
Keywords: Delay discounting, Anhedonia, Impulsivity, Working memory, Depression, Future-directed thinking
1. Introduction
Major Depressive Disorder (MDD) is a common and debilitating psychiatric disorder, with a lifetime prevalence of 16.2% in the United States (Kessler et al., 2003). MDD is characterized by persistent sad mood and difficulty experiencing pleasure (anhedonia), accompanied by several associated symptoms, including weight loss or gain, sleep disturbances, and difficulty concentrating, among others. An important feature of depressive thinking is a negative view of the future (Beck, Rush, Shaw, & Emery, 1979), which can manifest as a lack of positive expectations (MacLeod & Salaminiou, 2001).
A sound measure of future-oriented thinking regarding positive experiences (e.g., receiving rewards) is the delay discounting paradigm. Delay discounting refers to the reduction in the present value of a future reward as the delay for obtaining the reward increases (Richards, Zhang, Mitchell & de Wit, 1999). Delay discounting is usually measured by presenting individuals with a hypothetical or real choice between two rewarding options available at different times (e.g., “Would you prefer $10 now or $15 in a week?”). Individuals have different discount rates (i.e., some value future rewards less than others), and delay discounting shows substantial stability over time (1-year test-retest stability: 0.71; Kirby, 2009). Prior research suggests that delay discounting represents an important individual difference variable that could shape decision making in a host of contexts (e.g., decisions about diets, relationships and spending).
It is not clear whether delay discounting rate might be affected by depression or elevated anhedonic symptoms, and if so, in which way. One hypothesis is that, because of their generally bleak view of the future (Beck et al., 1979), depressed individuals will discount delayed rewards at a higher rate than healthy controls. This relationship might reflect mood incongruence: difficulty forming mental representations of positive future experiences might result from the discrepancy between these representations and current low mood in depression (Schacter, Addis, & Buckner, 2007). In other words, reflecting on current depressed mood could lead individuals to expect similarly negative future events (pessimistic future-directed thinking), possibly leading to a preference for immediately available rewards, and thus more “short-sighted” (myopic) decisions in delay discounting paradigms.
The contrasting hypothesis is that, relative to healthy controls, depressed individuals will show reduced delay discounting due to current anhedonia, evident in their reduced positive affect and behavioral responsiveness to immediately available pleasurable stimuli (e.g., Berenbaum & Oltmanns, 1992). In other words, because immediate rewards tend to elicit weaker levels of pleasure in depressed individuals relative to healthy subjects, they might be deemed less preferable than objectively greater delayed rewards, leading to more “far-sighted” decisions.
A small number of studies have explored the relationship between delay discounting and depression. In one recent study, ex-smokers endorsing a history of depressive symptoms exhibited greater discounting rates than ex-smokers without such history (Yoon et al., 2007). In another report, relative to healthy participants, medicated subjects with MDD discounted delayed outcomes less when probed about the distant future, whereas they showed a larger discount rate of rewards in the near future (Takahashi et al., 2008). These findings were interpreted within the framework of increased impulsivity in depression, which might manifest itself in impulsive and risky (including self-harm) behavior (Sinclair, Crane, Hawton & Williams, 2006).
Prior studies of delay discounting in depression are characterized by three important limitations. First, these studies have not considered the possible influence of other variables known to modulate delay discounting, including impulsivity and working memory capacity. Impulsive behavior (e.g., in the context of substance abuse) has been strongly associated with higher discount rates (for review, see Reynolds, 2006). Similarly, discount rates are higher in individuals with poor working memory and in healthy subjects under high working memory load (Bobova, Finn, Rickert & Lucas, 2009; Shamosh et al., 2008; Hinson, Jameson, & Whitney, 2003), likely due to a diminished ability to consider the most rational decision and resorting to “gut” decisions by choosing the immediate (yet smaller) reward. In light of the role of impulsivity (Takahashi et al., 2008) and diminished working memory capacity (Austin et al., 2001) in depression, it appears critical to consider individual differences in these variables when examining links between depression/anhedonia and discount rate.
Second, depression is a highly heterogeneous condition, and it is conceivable that distinct constellations of symptoms may impact delay discounting in different ways, leading to inconsistencies in the literature. Third, although studies in currently depressed participants are clearly very important, the study of individuals experiencing current MDD does not allow researchers to differentiate whether abnormal delay discounting behavior might represent a vulnerability to depression, or rather a consequence of current symptoms. In light of these key conceptual challenges, consensus is emerging about the need to consider intermediate phenotypes (“endophenotypes”) that might be more proximally related to disease vulnerabilities (Gottesman & Gould, 2003; Insel & Cuthbert, 2009). Because of its relative stability over time (Shankman et al., 2010), clinical and biological plausibility (e.g., American Psychiatric Association, 2000; Pizzagalli et al., 2009), and substantial heritability (Bogdan and Pizzagalli, 2009; Dworkin & Saczynski, 1984), anhedonia has emerged as one of the most promising endophenotypes of depression (Hasler, Drevets, Manji, & Charney, 2004), warranting investigations of its putative effects on delay discounting.
As a first step to address these limitations, the present study examined the relationship between anhedonic symptoms, as measured by the Snaith-Hamilton Pleasure Scale (Snaith et al., 1995), and delay discounting rate in a student sample without any history of MDD while controlling for individual differences in impulsivity and working memory. We tested the two contrasting hypotheses developed above: relative to participants reporting normal hedonic tone, those reporting elevated levels of anhedonic symptoms: (1) will discount delayed rewards at a higher rate, possibly due to difficulties forming mental representations of positive future experiences; vs. (2) will discount delayed rewards at a lower rate, possibly due to reduced responsiveness to immediate rewards. Critically, we reasoned that evidence for the second hypothesis could be bolstered by showing that links between anhedonic symptoms and delay discounting rates remained after controlling for pessimistic future-directed thinking, which was assessed by means of the Future Events Task (Miranda & Mennin, 2007).
2. Method
2.1 Participants
Thirty-nine participants, recruited from the Harvard University Department of Psychology study pool, completed the study after providing informed written consent. All were English-speaking and right-handed. They were paid $10/hour, and were told that they would have the opportunity to win more money during one of the computerized tasks. Three participants were excluded from analyses; two were current cigarette smokers, while one fulfilled criteria for marijuana abuse. These subjects were excluded due to the well-established link between drug abuse and high delay discounting rate (Reynolds, 2006). The remaining thirty-six subjects (mean age: 26.3 years, S.D.: 7.5, range: 19-50; 20 females; 6 African-American, 19 Caucasian, 11 Asian) reported no current or past depression and no current psychopathology, as assessed by the Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998). The study was approved by the Committee on the Use of Human Subjects at Harvard University.
2.2. Procedure
2.2.1. Delay discounting task
The delay discounting task used here is a computerized question-based measure that can be used to study choice behavior (Richards et al., 1999). Participants were presented with a series of questions asking about their preferences between $10 to be received after one of the delays (1, 2, 30, 180 and 365 days) or a smaller amount (e.g., $2) to be received immediately. For each trial, they were instructed to click on the reward they preferred. Time to choose was unlimited, and after each response, participants were asked, “Are you sure about your response?” If they indicated uncertainty, they were permitted to go back to make a different choice; if they were sure, the program continued to the next question. For each delay, the smaller amount was increased or decreased in value (± $0.50) based on previous responses until an indifference value was reached. An indifference value is defined as the smallest amount of money chosen to be received immediately instead of waiting the specified delay in order to receive the $10 standard. The task automatically terminated once an indifference value was calculated for each delay. To increase the saliency and relevance of their choices, participants were told at the outset that one of their responses would be randomly selected and that they would receive the amount they chose at the delay specified. That is, if they chose the immediate reward on the randomly selected trial, they would receive the money as additional compensation after the session; conversely, if they chose the larger, delayed reward, they would receive the money by mail after the delay specified. After completing the delay discounting task, participants were asked to rate their certainties for receiving the delayed rewards (e.g. “If you had chosen the money delayed by 365 days, were you sure you would actually get that money if it was the randomly selected answer? How sure were you that you would get the money in 365 days if you chose it?”; Richards et al., 1999).
2.2.2. Automated Operation Span Task
The Automated Operation Span task (Unsworth, Heitz, Schrock, & Engle, 2005) was used to assess working memory capacity. In this task, participants are asked to recall a sequence of letters, while solving simple math operations. In each trial, participants first saw a math operation (e.g., (1*2) + 1 = ?). Once they thought that they knew the answer, they clicked the mouse to advance to the next screen. They then saw a number (e.g., “3”) and were required to respond if the number was the correct solution by clicking on “True” or “False” on the screen. Following this, participants saw a letter, which was presented for 800 ms. After the presentation of 3-7 pairs of math problems and letters, the participants saw a list of letters and were asked to indicate by mouse click the order of the letters in the last set. They were then provided with feedback, which included how many letters they recalled correctly in that set, and what cumulative percentage of the math problems were answered accurately. If participants took more time to solve the math than their average time (as determined during a practice section before the task) plus 2.5 SD, the program automatically advanced. This served to prevent participants from rehearsing the letters while solving the math operations. Participants were instructed to maintain their math accuracy above 85% in order to ensure that they were attempting to both solve the math operations and remember the letters. Performance on this task has been found to provide a reliable measure of working memory capacity (Unsworth et al., 2005). Higher scores indicate better working memory capacity. In total, the task included 75 operations and 75 letters. As in prior studies (e.g., Unsworth et al., 2005), the Operation Span score was the main variable of interest and reflected the sum of all perfectly recalled sets. If, for example, a participant correctly recalled four letters in a set size of 4, five letters in a set size of 5, and one letter in a set size of 6, his or her Operation Span score was 9 (4 + 5 + 0).
2.2.3. Self-report questionnaires
Self-report questionnaires administered after the experiment included the Future Events Task (Miranda & Mennin, 2007), Beck Depression Inventory-II (BDI-II; Steer et al., 1996), Snaith-Hamilton Pleasure Scale (SHPS; Snaith et al., 1995), and Barratt Impulsiveness Scale Version 11 (BIS-11; Patton, Stanford & Barratt, 1995). In the Future Events Task, participants were presented with a list of 34 future events, half of which were positive and half negative. For each item, they were asked to (1) answer the question, “Is this likely to happen to you some time in the future?” by circling yes or no, and (2) indicate how certain they were of each response by using a 5-point Likert scale (1: Not at all certain; 5: As certain as one can be). Participants were assigned a score of “1” for each item scored “as certain as one can be” about a pessimistic expectation (i.e., being certain that a negative event would happen or a positive event would not happen to them), and assigned a score of “0” otherwise. The total score indicates level of depressive predictive certainty, with higher scores indicating more pessimistic future-thinking (Miranda & Mennin, 2007).
The BDI-II is a reliable and well-validated instrument used to assess symptoms of depression (Beck et al., 1996). For each of the 21 items, individuals are asked to choose statements that indicate how they have been feeling in the past two weeks. These items reflect symptoms such as sadness, loss of pleasure, and changes in energy, sleep, and appetite. The SHPS is a well-validated, 14-item instrument used to assess anhedonia. Participants are asked to rate whether they agree, strongly agree, disagree, or strongly disagree that they would enjoy various experiences that are generally considered pleasurable (e.g. “I would find pleasure in my hobbies and past-times”). Following recent recommendation (Franken, Rassin & Murris, 2007), an ordinal (rather than the original dichotomous) scoring was used. Specifically, items answered with “strongly agree” were coded as “1”, while a “strongly disagree” response was assigned a score of “4.” Therefore, scores on the SHPS can range from 14 to 56, with higher scores corresponding to higher levels of anhedonia. The SHPS has satisfactory test-retest validity in healthy participants over an interval of three weeks (intraclass correlation coefficient between test and retest: r = .70, p < .001; Franken, Rassin & Murris, 2007). The BIS-11 provides a measure of real-world impulsivity (e.g. “I charge more than I earn”) and has been found to possess satisfactory reliability and validity (e.g., Patton et al., 1995).
2.2.4. Mini International Neuropsychiatric Interview (MINI)
The MINI is a short structured diagnostic interview for DSM-IV and ICD-10 psychiatric disorders with satisfactory reliability and validity (Sheehan et al., 1998). The MINI interview was administered in the same session, following the experimental portion.
2.3. Data Reduction and Analyses
For each participant, the indifference values obtained in the delay discounting task were used to estimate a delay discount rate, measured by the variable k. Prior research indicates that delay discounting of reward value can be described by a hyperbolic discount function (e.g., Richards et al., 1999):
| (Equation 1) |
where A is the amount of the reward, D is the delay to reward, and k is a free parameter. This equation was fit to the five delay indifference points for each person using LoggerPro 3.5 (Vernier Software & Technology; Beaverton, OR), which determined the best fitting values for k. Larger values of k indicate more marked devaluation of reinforcer value by delay, or higher discount rate (Richards et al., 1999).
Due to prior evidence of a relationship between inconsistency in intertemporal choice and depression (Takahashi et al., 2008), we also fitted the q-exponential function to each subjects’ data to determine estimates of q (inconsistency) and kq (impulsivity) using R statistical language (www.r-project.org). This function is based on Tsallis’ statistics, and was computed as:
| (Equation 2) |
where A is the amount of the reward at D = 0, D is the delay to reward, kq is a parameter of impulsivity at delay D=0, and expq () is the q-exponential function (Cajueiro, 2006; Takahashi, 2007; Takahashi et al., 2007).2
The goodness-of-fit was evaluated using the second-order Akaike Information Criterion (AICc), which was used to correct for small sample size. Smaller AICc indicates better fit. The AICc values for the hyperbolic discount function, q-exponential function, and exponential function were 15.66, 29.85 and 42.44, respectively. Hence, we concluded that the hyperbolic function was the best choice of discounting model for this particular data set; accordingly, main analyses focused on k values. Before analyses, the distribution of k values was normalized using a log10 transformation.
To examine the relationship between anhedonic symptoms and delay discounting rate, a Pearson correlation was performed between SHPS scores and k values. Next, a hierarchical regression was performed to examine whether SHPS scores predicted delay discounting rate when controlling for variance associated with working memory capacity (as assessed by the Operation Span scores), impulsivity (as assessed by the total BIS-11 scores), and certainty ratings about the delivery of delayed reward (as assessed by the post-task questionnaire). For a more stringent test of the study hypotheses, a second hierarchical regression was run to evaluate whether SHPS scores would predict delay discounting rate after entering pessimistic future-directed thinking (as assessed by the Future Events Task) in the first step, and impulsivity, working memory capacity, and certainty regarding the delivery of delayed reward in the second step of the model. Finally, in secondary analyses, Pearson correlations between delay discounting rate and (1) post-task ratings of certainty regarding the delivery of a reward at various delays; and (2) depressive predictive certainty (as assessed by the Future Events Task) were run. All analyses were performed using SPSS, Version 16.0.
3. Results
3.1 Primary Analyses
One participant’s delay discounting rate data were lost due to experimenter error. Gender did not affect delay discounting (t(34) = -0.86, p > 0.39) or anhedonia (t(34) = 0.68, p>0.49), thus this variable was not further considered in the analyses. Table 1 summarizes descriptive statistics and inter-correlations among the variables. Of primary relevance to the study hypotheses, k values were significantly and negatively correlated with SHPS scores (SHPS range: 14-30; r = -0.42; p < 0.015; Fig. 1). Accordingly, increasing anhedonic symptoms were associated with smaller discounting rate of future rewards, suggesting that participants reporting relatively greater anhedonic symptomatology were more likely to choose a larger, delayed reward over an immediate smaller reward.1 Pessimistic future-thinking in the Future Events Task was weakly related to k value (r = -0.30, p = 0.08). In contrast to prior studies (e.g., Reynolds, 2006; Bobova et al., 2009), no correlations emerged between delay discounting and impulsivity score (r = -0.12, p > 0.51) or working memory capacity (r = -0.20, p > 0.25).
Table 1.
Descriptive statistics (mean and SD) and correlation matrix of the variables of interest
| Mean | SD | BIS-11 | WM | FET | k value | |
|---|---|---|---|---|---|---|
| SHPS | 21.57 | 4.08 | r = -0.23 | r = 0.16 | r = 0.21 | r = -0.42 |
| p = 0.19 | p = 0.36 | p = 0.23 | p < .015 | |||
| BIS-11 | 70.17 | 9.33 | 1 | r = 0.26 | r = -.13 | r = -0.12 |
| p = 0.13 | p = 0.44 | p = 0.51 | ||||
| WM | 49.78 | 15.33 | 1 | r = -.05 | r = -0.20 | |
| p = 0.77 | p = 0.25 | |||||
| FET | 1.42 | 1.78 | 1 | r = -.30 | ||
| p = 0.08 | ||||||
| k value | -2.04 | 0.82 | 1 |
Notes: SHPS: Snaith-Hamilton Pleasure Scale (Snaith et al., 1995); BIS-11: Barratt Impulsiveness Scale, version 11 (Patton et al., 1995); WM: working memory capacity (as assessed by the Operation Span task; Unsworth et al., 2005); FET: Future Events Task; k value: discount rate. Higher scores on the SHPS and BIS-11 indicate higher levels of anhedonia and impulsivity, respectively. Higher WM scores indicate better working memory capacity. Higher FET scores indicate more elevated depressive predictive certainty. Higher (less negative) k values indicate preference for smaller immediate rewards over later, larger ones.
Fig. 1.
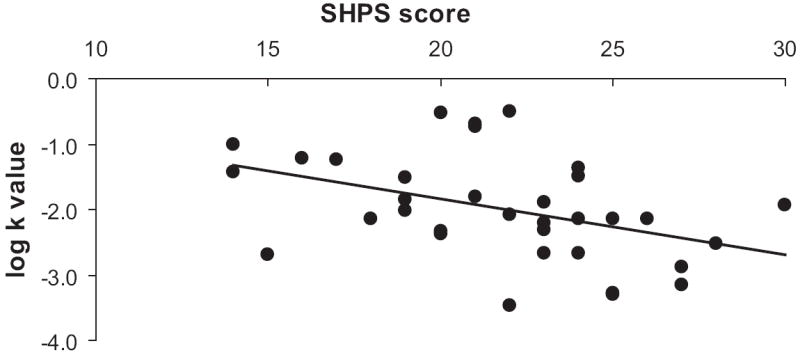
Pearson correlation and scatterplot of delay discounting rate and SHPS scores (r = -0.42; p < 0.015).
A hierarchical regression analysis indicated that SHPS scores predicted delay discounting rates even after controlling for individual differences in impulsivity, working memory capacity, and certainty regarding the delivery of delayed reward [ΔR2 = 0.16, F(1, 29) = 6.71, p < 0.015]. Moreover, SHPS scores remained significant predictors of discounting rates even when entering pessimistic future-directed thinking in the first step of the hierarchical regression model, and impulsivity, working memory capacity, and certainty regarding the delivery of delayed reward in the second step [ΔR2 = 0.11, F (1, 28) = 5.26, p < 0.03].
3.2 Control Analyses
In order to disentangle the effect of general depressive symptoms, as measured by the BDI-II, from the effect of anhedonia on delay discounting rate, a hierarchical regression analysis was performed. Findings revealed that SHPS scores continued to predict delay discounting rate even when BDI-II scores were entered with impulsivity, working memory capacity and certainty regarding the delivery of delayed reward in the first step of the model [ΔR2 = 0.13, F (1, 28) = 1.11, p < 0.02].
Analyses considering the q-exponential function based on Tsallis’ statistics to estimate q (inconsistency) and kq (impulsivity) revealed no relationship between either of these variables and SHPS score (q: r = -0.39; p > 0.07; kq: r = 0.12; p > 0.57). Finally, there was no relation between either of these parameters and working memory, impulsivity and future-directed thinking.
4. Discussion
The results of the present study indicate that relatively decreased capacity for experiencing pleasure is associated with a lower discount rate for future rewards. Thus, when participants reporting anhedonic symptoms in their daily life faced a choice between a small, immediate reward and a larger, future reward, they were more likely to take the larger reward in the future, despite the delay, demonstrating more far-sighted decisions. Interestingly, anhedonic symptoms predicted delay discounting rates even when controlling for individual differences in variables previously associated with discounting behavior, including working memory capacity and impulsivity (Hinson et al., 2003; Reynolds, 2006; Bobova et al., 2009), general depressive symptoms (as assessed by the BDI-II), and pessimistic future-directed thinking (as assessed by the Future Events Task).
In light of this pattern, we speculate that the current finding of an inverse relation between anhedonic symptoms and delay discounting rate might be explained by blunted responses to immediate rewards and positive cues characteristic of individuals with anhedonia and/or depression (e.g., Berenbaum & Oltmanns, 1992; Wacker, Dillon, & Pizzagalli, 2009). Of note, neuroimaging studies of delay discounting have shown that activation in ventral striatal regions (e.g., the nucleus accumbens) is associated with a preference for immediate over delayed rewards (e.g., Hariri et al., 2006). The nucleus accumbens plays a key role in coding the incentive properties of stimuli and has been found to be hypoactive in both non-clinical samples with elevated anhedonic symptoms (Wacker et al., 2009) and unmedicated MDD samples (e.g., Pizzagalli et al., 2009). Collectively, these findings raise the possibility that weaker hedonic responses to immediately available rewards might contribute to a lower delay discounting rate in anhedonic individuals.
In spite of these convergent findings, the neurobiological basis of delay discounting remains largely unknown (but see Schweighofer et al., 2008 for initial evidence indicating that acutely lowered serotonin levels lead to steeper delayed discounting, likely due to more impulsive behavior). Anhedonia has been associated with a hypoactive dopaminergic system (Hasler et al., 2008; Heinz et al., 1994; Tremblay et al., 2002), and it is possible that reduced dopamine transmission might diminish the saliency of immediate rewards (Berridge, 2007), biasing anhedonic individuals towards larger, delayed rewards. Although entirely speculative at this stage, it is interesting to note that individuals with disorders characterized by an excess of mesolimbic dopamine, such as schizophrenia, are characterized by higher-than-normal discount rates (Heerey, Robinson, McMahon & Gold, 2007). Moreover, delay discounting rate has been inversely associated with salivary cortisol levels, indicating that individuals with high cortisol levels made more far-sighted decisions (Takahashi, 2004). Critically, anhedonic subjects are characterized by dysfunctional stress regulation (Putnam et al., 2008; Soliman et al., 2008), which might make them more vulnerable to the deleterious effects of stressful events (Meehl, 1975). Collectively, these findings suggest that it will be important in future studies to investigate the role of stress in delay discounting, and whether discounting rate factors into the progression from dysregulated stress response to major depression.
The present results could also be interpreted within the framework of recent findings emerging from the affective forecasting literature. For example, in a recent series of studies, Kassam, Gilbert, Boston & Wilson (2008) described the construct of future anhedonia, or the belief that hedonic states will be less intense in the future than the present. According to this conceptualization, because of the temporal distance between the self and the future reward, it may be difficult to mentally represent the emotion that would follow receipt of the future reward. In individuals who have difficulty experiencing pleasure in the present (i.e., anhedonic subjects), hedonic responses to current rewards are, by definition, blunted. It is possible, then, that only the magnitudes of the rewards might factor into the choices of anhedonic individuals. As a consequence, they are more likely than healthy controls to make the more far-sighted decision and choose the larger, albeit delayed reward. Interestingly, emerging evidence from behavioral economics indicates that far-sighted vs. myopic decisions can have different affective sequelae within specific contexts. Kivetz and Keinan (2006), for example, reported that myopic choices are often followed by less regret than more far-sighted choices are (e.g., participants who chose work over pleasure later expressed more regret over their choice than participants who made the opposite decision). Because depression is often marked by overwhelming feelings of regret, it will be important to investigate whether abnormalities in reward-related decision making might increase risk for depression through the emergence of regret and other negative emotions.
It is worth noting that in the current delay discounting task, the probability that any particular reward in any trial would actually be received was small. Therefore, a preference for later, larger rewards should not be interpreted as evidence of an optimistic outlook toward the future. Rather than contradicting previous findings of pessimistic future-directed thinking in depression, these results support the assertion that reduced hedonic capacity may be responsible for the inability to find future positive experiences pleasurable (MacLeod & Salaminiou, 2001). Accordingly, both cognitive and affective components likely play a key role in the emergence and maintenance of a negative view toward the future in depression.
The sample used in this study can be seen as both a strength and a limitation. Utilizing a psychiatrically healthy student sample allowed us to (1) investigate the effect of anhedonia on delay discounting without the possible confounding effects of other symptoms associated with major depression, and (2) identify hedonic abnormalities that might represent a vulnerability for, rather than consequence of, depression. Interestingly, anhedonia was a significant predictor of delay discounting rate even after controlling for general depressive symptoms, highlighting the specificity of this relationship. The clear limitation is that possible inferences to major depression are premature. Importantly, we cannot discern whether the current individuals with elevated anhedonic symptoms but no current or past depression represent a “resilient” group or rather a group with increased risk for future depression (particularly since this young group was still within the vulnerability period for depression).
Several other limitations of the present study deserve mention. First, the sample size was relatively modest, and low statistical power might explain null findings concerning relations between delay discounting, on one side, and working memory capacity and impulsivity, on the other side. Null findings with respect to working memory capacity are unexpected, but while working memory load has been shown to affect discount rate in healthy participants (Hinson et al., 2003), another factor (i.e., intelligence) has been found to mediate the relationship between working memory capability and discounting rate (Shamosh et al., 2008). Unfortunately, intelligence was not assessed in the current study. Negative findings regarding impulsivity are only partially surprising, particularly when seen within the framework of prior reports. While some studies have shown a link between self-report and behavioral measures of impulsivity, others have found very weak relationships (Reynolds, Ortengren, Richards & de Wit, 2006). It is possible that delay discounting paradigms and self-report questionnaires measure different constructs; in self-report measures, participants must recognize and report on their own behavioral tendencies in various contexts, and these self-perceptions may not always accurately reflect their behavior. In contrast, performance on behavioral tasks is less sensitive to biased self-perceptions (Reynolds et al., 2006). It is interesting to note, however, that the present link between anhedonic symptoms and delay discounting remained after controlling for individual differences in working memory capacity and impulsivity, highlighting promising specificity.
Second, although the relation between anhedonic symptoms and delay discounting remained even after controlling for pessimistic future-directed thinking, providing suggestive evidence that the current findings might be explained by reduced responsiveness to immediate rewards, conclusive statements about mechanisms behind the affect-discounting relationship are premature. Neuroimaging approaches contrasting reward-related encoding and retrieval processes might be useful for pinpointing mechanisms contributing to the present findings.
Finally, we hypothesized that performance in the Future Events Task, a questionnaire that assesses individuals’ expectations about the future, would be related to delay discounting rate, but only a statistical trend emerged (possibly due to limited statistical power). The trending inverse correlation indicates that individuals with more pessimistic expectations about the future were characterized by reduced discounting of future reward, in line with the primary findings. Critically, anhedonic symptoms predicted discounting rates above and beyond pessimistic future-directed thinking, consistent with the assumption of reduced hedonic responsiveness to immediate rewards.
In conclusion, the current findings indicate that individuals reporting loss of pleasure in their daily life make more economically far-sighted choices about their future, possibly due to their decreased responsiveness to immediate rewards. These preliminary findings are consistent with the assumption that affective components play an important role in economic decisions in depression, and warrant future studies in clinical samples.
Acknowledgments
This study was supported by the Harvard College Research Program and by the Mind/Brain/Behavior Mary Gordon Roberts Fellowship awarded to KML and by an NIMH grant (R01 MH068376) awarded to DAP. The authors would like to thank Dr. Harriet de Wit for providing the computerized delay discounting task used in the current study, and Dr. Daniel G. Dillon for thoughtful comments on an early version of this manuscript.
Footnotes
A similar correlation emerged when considering total BDI scores (Pearson r = -0.45; p < 0.007). Although the range for BDI scores was 0 to 19, the mean BDI score was low (4.78, SD = 5.11), and the distribution was skewed toward the left, which is not surprising given the nonclinical nature of the sample. A non-parametric Spearman Rank’s correlation confirmed a significant relation between BDI scores and delay discount rates (rho = -0.38, p = 0.025). In light of the overall low BDI scores, main analyses focused on anhedonic symptoms, as assessed by the SHPS.
Note that Equation 2 is equivalent to the simple hyperbolic discount function [Equation 1 = V(D) = A/(1 + kD)] when q = 0. Critically, in the current dataset, the q-exponential function could not be fitted in 10 participants due to an infinity value. In light of these results and the AICc values indicating that the hyperbolic function best fitted the current dataset, findings emerging from the q-exponential function were not further interpreted and should be interpreted with caution.
Disclosures Dr. Pizzagalli has received research support from GlaxoSmithKline and Merck & Co. for studies unrelated to this article, consulting fees from ANT North America Inc. (Advanced Neuro Technology) and AstraZeneca, and honoraria from AstraZeneca.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. American Psychiatric Press; Washington, DC: 2000. text revision. [Google Scholar]
- Austin MP, Mitchell P, Goodwin GM. Cognitive deficits in depression: possible implications for functional neuropathology. British Journal of Psychiatry. 2001;178:200–206. doi: 10.1192/bjp.178.3.200. [DOI] [PubMed] [Google Scholar]
- Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy for Depression. New York: Guilford Press; 1979. [Google Scholar]
- BeckA T, Steer RA, Brown GK. Beck Depression Inventory Manual. 2. San Antonio, Texas: The Psychological Corporation; 1996. [Google Scholar]
- Berenbaum H, Oltmanns TF. Emotional experience and expression in schizophrenia and depression. Journal of Abnormal Psychology. 1992;101:37–44. doi: 10.1037//0021-843x.101.1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berridge KC. The debate over dopamine’s role in reward: the case for incentive salience. Psychopharmacology. 2007;191:391–431. doi: 10.1007/s00213-006-0578-x. [DOI] [PubMed] [Google Scholar]
- Bobova L, Finn PR, Rickert ME, Lucas J. Disinhibitory psychopathology and delay discounting in alcohol dependence: personality and cognitive correlates. Experimental and Clinical Psychopharmacology. 2009;17:51–61. doi: 10.1037/a0014503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bogdan R, Pizzagalli DA. The heritability of hedonic capacity and perceived stress: A twin study evaluation of candidate depressive phenotypes. Psychological Medicine. 2009;39:211–218. doi: 10.1017/S0033291708003619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cajueiro DO. A note on the relevance of the q-exponential function in the context of intertemporal choices. Physica A. 2006;364:385–388. [Google Scholar]
- Dworkin RH, Saczynski K. Individual differences in hedonic capacity. Journal of Personality Assessment. 1984;48:620–626. doi: 10.1207/s15327752jpa4806_8. [DOI] [PubMed] [Google Scholar]
- Franken IH, Rassin E, Muris P. The assessment of anhedonia in clinical and non- clinical populations: further validation of the Snaith-Hamilton Pleasure Scale (SHAPS) Journal of Affective Disorders. 2007;99:83–89. doi: 10.1016/j.jad.2006.08.020. [DOI] [PubMed] [Google Scholar]
- Gottesman II, Gould TD. The endophenotype concept in psychiatry: etymology and strategic intentions. American Journal of Psychiatry. 2003;160:636–645. doi: 10.1176/appi.ajp.160.4.636. [DOI] [PubMed] [Google Scholar]
- Hasler G, Drevets WC, Manji HK, Charney DS. Discovering endophenotypes for major depression. Neuropsychopharmacology. 2004;29:1765–81. doi: 10.1038/sj.npp.1300506. [DOI] [PubMed] [Google Scholar]
- Hasler G, Fromm S, Carlson PJ, Luckenbaugh DA, Waldeck T, Geraci M, Roiser JP, Neumeister A, Meyers N, Charney DS, Drevets WC. Neural response to catecholamine depletion in unmedicated subjects with major depressive disorder in remission and healthy subjects. Archives of General Psychiatry. 2008;65:521–31. doi: 10.1001/archpsyc.65.5.521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hariri AR, Brown SM, Williamson DE, Flory JD, de Wit H, Manuck SB. Preference for immediate over delayed rewards is associated with magnitude of ventral striatal activity. Journal of Neuroscience. 2006;26:13213–13217. doi: 10.1523/JNEUROSCI.3446-06.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heerey EA, Robinson BM, McMahon RP, Gold JM. Delay discounting in schizophrenia. Cognitive Neuropsychiatry. 2007;12:213–221. doi: 10.1080/13546800601005900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heinz A, Schmidt LG, Reischies FM. Anhedonia in schizophrenic, depressed, or alcohol-dependent patients--neurobiological correlates. Pharmacopsychiatry. 1994;27(Suppl 1):7–10. doi: 10.1055/s-2007-1014317. [DOI] [PubMed] [Google Scholar]
- Hinson JM, Jameson TL, Whitney P. Impulsive decision making and working memory. Journal of Experimental Psychology: Learning, Memory & Cognition. 2003;29:298–306. doi: 10.1037/0278-7393.29.2.298. [DOI] [PubMed] [Google Scholar]
- Insel TR, Cuthbert BN. Endophenotypes: bridging genomic complexity and disorder heterogeneity. Biological Psychiatry. 2009;66:988–989. doi: 10.1016/j.biopsych.2009.10.008. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) Journal of the American Medical Association. 2003;289:3095–3105. doi: 10.1001/jama.289.23.3095. [DOI] [PubMed] [Google Scholar]
- Kirby KN. One-year temporal stability of delay-discount rates. Psychonomic Bulletin & Review. 2009;16:457–462. doi: 10.3758/PBR.16.3.457. [DOI] [PubMed] [Google Scholar]
- Kivetz R, Keinan A. Repenting hyperopia: an analysis of self-control regrets. Journal of Consumer Research. 2006;33:273–282. [Google Scholar]
- Macleod AK, Salaminiou E. Reduced positive future-thinking in depression: cognitive and affective factors. Cognition and Emotion. 2001;15:99–107. [Google Scholar]
- Miranda R, Mennin DS. Depression, Generalized Anxiety Disorder, and certainty in pessimistic predictions about the future. Cognitive Therapy & Research. 2007;31:71–82. [Google Scholar]
- Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. Journal of Clinical Psychology. 1995;51:768–774. doi: 10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Pizzagalli DA, Holmes AJ, Dillon DG, Goetz EL, Birk JL, Bogdan R, et al. Reduced caudate and nucleus accumbens response to rewards in unmedicated individuals with Major Depressive Disorder. American Journal of Psychiatry. 2009;166:702–710. doi: 10.1176/appi.ajp.2008.08081201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Putnam KA, Pizzagalli DA, Gooding DC, Kalin NH, Davidson RJ. Neural activity and diurnal variation of cortisol: evidence from brain electrical tomography analysis and relevance to anhedonia. Psychophysiology. 2008;45:886–895. doi: 10.1111/j.1469-8986.2008.00697.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reynolds B. A review of delay-discounting research with humans: relations to drug use and gambling. Behavioral Pharmacology. 2006;17:651–657. doi: 10.1097/FBP.0b013e3280115f99. [DOI] [PubMed] [Google Scholar]
- Reynolds B, Ortengren A, Richards JB, de Wit H. Dimensions of impulsive behavior: personality and behavioral measures. Personality and Individual Differences. 2006;40:305–315. [Google Scholar]
- Richards JB, Zhang L, Mitchell SH, de Wit H. Delay or probability discounting in a model of impulsive behavior: Effect of alcohol. Journal of the Experimental Analysis of Behavior. 1999;71:121–143. doi: 10.1901/jeab.1999.71-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schacter DL, Addis DR, Buckner RL. Remembering the past to imagine the future: the prospective brain. Nature Reviews Neuroscience. 2007;8:657–661. doi: 10.1038/nrn2213. [DOI] [PubMed] [Google Scholar]
- Schweighofer N, Bertin M, Shishida K, Okamoto Y, Tanaka SC, Yamawaki S, Doya K. Low-serotonin levels increase delayed reward discounting in humans. Journal of Neuroscience. 2008;28:4528–32. doi: 10.1523/JNEUROSCI.4982-07.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shamosh NA, DeYoung CG, Green AE, Reis DL, Johnson MR, Conway AR, et al. Individual differences in delay discounting: relation to intelligence, working memory, and anterior prefrontal cortex. Psychological Science. 2008;19:904–911. doi: 10.1111/j.1467-9280.2008.02175.x. [DOI] [PubMed] [Google Scholar]
- Shankman SA, Nelson BD, Harrow M, Faull RJ. Does physical anhedonia play a role in depression? A 20-year longitudinal study. Affective Disorders. 2010;120:170–176. doi: 10.1016/j.jad.2009.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry. 1998;59(Suppl 20):22–33. [PubMed] [Google Scholar]
- Sinclair J, Crane C, Hawton K, Williams JM. The role of autobiographical memory specificity in deliberate self-harm: correlates and consequences. Journal of Affective Disorders. 2006;102:11–18. doi: 10.1016/j.jad.2006.12.006. [DOI] [PubMed] [Google Scholar]
- Snaith RP, Hamilton M, Morley S, Humayan A, Hargreaves D, Trigwell P. A scale for the assessment of hedonic tone: The Snaith-Hamilton Pleasure Scale. British Journal of Psychiatry. 1995;167:99–103. doi: 10.1192/bjp.167.1.99. [DOI] [PubMed] [Google Scholar]
- Soliman A, O’Driscoll GA, Pruessner J, Holahan AL, Boileau I, Gagnon D, Dagher A. Stress-induced dopamine release in humans at risk of psychosis: a [11C]raclopride PET study. Neuropsychopharmacology. 2008;33:2033–41. doi: 10.1038/sj.npp.1301597. [DOI] [PubMed] [Google Scholar]
- Swann AC, Bjork JM, Moeller FG, Dougherty DM. Two models of personality traits: relationship to personality traits and psychopathology. Biological Psychiatry. 2002;51:988–994. doi: 10.1016/s0006-3223(01)01357-9. [DOI] [PubMed] [Google Scholar]
- Takahashi T. Cortisol levels and time-discounting of monetary gain in humans. Neuroreport. 2004;15:2145–2147. doi: 10.1097/00001756-200409150-00029. [DOI] [PubMed] [Google Scholar]
- Takahashi T. A comparison of intertemporal choices for oneself versus someone else based on Tsallis’ statistics. Physica A. 2007;385:637–644. [Google Scholar]
- Takahashi T, Oono H, Inoue T, Boku S, Kako Y, Kitaichi Y, et al. Depressive patients are more impulsive and inconsistent in intertemporal choice behavior for monetary gain and loss than healthy subjects--an analysis based on Tsallis’ statistics. Neuro Endocrinology Letters. 2008;29:351–358. [PubMed] [Google Scholar]
- Takahashi T, Oono H, Radford MH. Empirical estimation of consistency parameter in intertemporal choice based on Tsallis’ statistics. Physica A. 2007;381:338–342. [Google Scholar]
- Tremblay LK, Naranjo CA, Cardenas L, Herrmann N, Busto UE. Probing brain reward system function in major depressive disorder: altered response to dextroamphetamine. Archives of General Psychiatry. 2002;59:409–416. doi: 10.1001/archpsyc.59.5.409. [DOI] [PubMed] [Google Scholar]
- Unsworth N, Heitz RP, Schrock JC, Engle RW. An automated version of the operation span task. Behavior Research Methods. 2005;37:498–505. doi: 10.3758/bf03192720. [DOI] [PubMed] [Google Scholar]
- Wacker J, Dillon DG, Pizzagalli DA. The role of the nucleus accumbens and rostral anterior cingulate cortex in anhedonia: integration of resting EEG, fMRI, and volumetric techniques. Neuroimage. 2009;46:327–337. doi: 10.1016/j.neuroimage.2009.01.058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yoon JH, Higgins ST, Heil SH, Sugarbaker RJ, Thomas CS, Badger GJ. Delay discounting predicts postpartum relapse to cigarette smoking among pregnant women. Experimental and Clinical Psychopharmacology. 2007;15:176–186. doi: 10.1037/1064-1297.15.2.186. [DOI] [PubMed] [Google Scholar]