

Abstract
This study investigated the role of family conflict resolution as a mediator of the relationship between ethnicity and psychological distress in dementia caregivers. The sample was composed of the families of 182 caregivers who participated in REACH (Resources for Enhancing Alzheimer’s Caregiver Health). The sample consisted of 84 Cuban American and 98 non-Hispanic White American families. Mediation analyses revealed that both income and conflict resolution partially mediated the relationship between ethnicity and caregiver psychological distress. Specifically, Cuban American families were less likely than non-Hispanic White families to reach a resolution to their disagreements, which may have rendered the caregiver at greater risk for psychological distress. These results suggest that Cuban American caregivers may benefit from interventions that improve the family’s ability to resolve conflicts.
Keywords: caregivers, conflict, Cuban, dementia, family, Hispanic
The untoward consequences of caring for a family member with dementia are well documented in the research literature. Caregivers face elevated stress and are more likely to experience emotional distress (Ory, Yee, Tennstedt, & Schulz, 2000; Schulz, Visitainer, & Williamson, 1990) relative to comparable noncaregivers. Because some dementia caregivers fare better than others (Zarit, Johansson, & Jarrott, 1998), researchers have sought to identify factors that predict the emotional toll of caregiving. One demographic factor linked to caregiver distress is ethnicity. There is evidence to suggest that Hispanic American caregivers may be more vulnerable to depression than non-Hispanic Americans (see Dilworth-Anderson, Williams, & Gibson, 2002; Harwood et al., 1998; Janevic & Connell, 2001).
While ethnicity and caregiver distress appear to be linked, the mechanisms that drive this ethnic difference are unknown. Identifying the underlying factors that render one ethnic group of caregivers particularly vulnerable to distress may allow clinical scientists to customize caregiver interventions to address these risk factors. In this study we test one such possible mediator of the link between caregiver ethnicity and psychological distress: family conflict resolution.
The theoretical framework that guides the current study is structural family theory (Minuchin, 1974), which views the family as an organism regulated by “structures,” which are defined as repetitive patterns of interaction. According to structural theory, problematic structures are the root cause of symptoms in individual family members. Structures influence the manner in which family members interact across multiple dimensions, including how they manage everyday problems and disagreements. While conflicts are natural and inevitable in all families, the inability to resolve conflict can have a negative impact on the emotional functioning of vulnerable family members, such as dementia caregivers.
Family conflict resolution has been implicated in mental health outcomes in dementia caregiver families. Fisher and Lieberman (1996) examined various dimensions of family functioning, including conflict avoidance, which they defined as the degree to which the expression of conflict was avoided or ignored in the family Using interviewer ratings, they found that conflict avoidance predicted subsequent anxiety and depression among the children of dementia patients.
There is an intimate interplay between family process and ethnicity, and evidence for ethnic differences in how families deal with medically related conflicts. Fisher et al. (2000) employed observational methods to investigate conflict resolution among Hispanic and White non-Hispanic American couples in which one partner had Type 2 diabetes. Couples were asked to spend 10 minutes discussing and reaching a resolution about a problem related to diabetes and its management that had been previously identified as highly salient for both partners. Ratings of the videotaped discussions revealed that the Hispanic American couples were more emotionally close, less hostile toward each other, less avoidant, had more off-task behavior, and had less dominant patients than their non-Hispanic counterparts. However, this study did not link these differences to individual-level outcomes and thus did not test for any mediating effects of ethnicity on individual outcomes.
The current study builds upon our prior research, which found that the manner in which caregiver families managed and resolved conflicts was associated with caregiver depressive symptoms and anxiety (Mitrani, Feaster, McCabe, Czaja, & Szapocznik, 2005). In this study we took a closer look at our earlier findings to investigate the role of conflict resolution in the relationship between ethnicity and caregiver emotional distress. In conducting this study, we hoped to address the important challenge for family intervention science of investigating the interplay between ethnicity, family functioning, and individual outcomes. More specifically, we aimed to gather information that will facilitate the development of culturally appropriate intervention strategies for dementia caregivers.
Method
Participants
The sample included the families of 182 caregivers (84 Cuban American and 98 non-Hispanic White American) of persons with Alzheimer’s disease or a related dementia who participated in the Miami site of REACH (Resources for Enhancing Alzheimer’s Caregiver Health; Eisdorfer et al., 2003). REACH tested 15 interventions to alleviate caregiver distress (9 active and 6 control group conditions) at six sites (Birmingham, Boston, Memphis, Miami, Palo Alto, and Philadelphia) and assessed at four time points (baseline, 6, 12, and 18 months) using common outcome measures (Schulz et al., 2003). The interventions consisted of psychosocial/educational services, behavioral interventions, environmental modifications, and technology interventions. The Miami site tested a family-based intervention and the family intervention enhanced by technology. Caregivers were recruited through medical providers, social service agencies, and mass media announcements.
The inclusion/exclusion criteria for REACH are described elsewhere (Wisniewski et al., 2003). Briefly, caregivers were required to live with the patient and provide care for a minimum of 4 hours per day for at least 6 months. At the Miami site, at least one other family member, besides the care recipient, had to agree to participate. Family members included household members and anyone else who the caregiver considered to be family (including fictive kin). See Table 1 for a description of the caregivers (CG), care recipients (CR), and their families.
TABLE 1.
Sample Descriptions With ANOVA and χ2 Results for Differences by Ethnicity
| ANOVA | Cuban Americans |
White Non-Hispanic |
Total |
df | F | |||
|---|---|---|---|---|---|---|---|---|
| N | M (SD) | N | M (SD) | N | M (SD) | |||
| CG age | 82 | 67.93 (10.99) | 93 | 70.20 (11.60) | 175 | 69.13 (11.34) | 1, 173 | 1.70 |
| CR age | 66 | 78.68 (6.58) | 66 | 80.02 (7.72) | 132 | 79.35 (7.18) | 1, 130 | 1.14 |
| Years caring | 82 | 3.93 (2.91) | 93 | 3.51 (3.22) | 175 | 3.70 (3.08) | 1, 173 | 0.81 |
| CG years of education | 82 | 9.15 (4.27) | 82 | 12.64 (2.52) | 175 | 10.98 (3.88) | 1, 170 | 43.65*** |
| CG depression | 82 | 19.02 (11.38) | 88 | 16.02 (11.22) | 170 | 17.46 (11.36) | 1, 168 | 2.99 |
| CG anxiety | 81 | 24.06 (6.93) | 87 | 21.95 (7.53) | 168 | 22.69 (7.30) | 1, 166 | 3.55 |
| CG distress | 81 | .37 (1.82) | 87 | .27 (1.94) | 168 | .07 (1.90) | 1, 166 | 4.26* |
| CR MMSE | 83 | 13.59 (7.60) | 93 | 14.48 (8.35) | 176 | 14.80 (8.00) | 1, 141 | 0.43 |
| CR ADLs | 83 | 2.92 (2.41) | 93 | 2.46 (2.18) | 176 | 2.68 (2.29) | 1, 174 | 1.83 |
| CR IADLs | 82 | 8.05 (4.99) | 91 | 7.54 (5.01) | 173 | 7.78 (4.99) | 1, 171 | 0.45 |
| Conflict resolution | 98 | 2.42 (1.37) | 84 | 3.32 (1.38) | 182 | 2.91 (1.44) | 1, 178 | 19.03*** |
| Chi-square | df | χ2 | ||||||
| CG gender | 1 | 0.23 | ||||||
| Female | N = 65 | N = 60 | N = 125 | |||||
| Male | N = 28 | N = 22 | N = 175 | |||||
| CR gender | 1 | 1.75 | ||||||
| Female | N = 47 | N = 44 | N = 91 | |||||
| Male | N = 35 | N = 49 | N = 84 | |||||
| Relationship to patient | 9 | 6.01 | ||||||
| Wife | N = 32 | N = 43 | N = 75 | |||||
| Husband | N = 18 | N = 26 | N = 44 | |||||
| Daughter | N = 23 | N = 18 | N = 41 | |||||
| Other relative | N = 7 | N = 5 | N = 12 | |||||
| Income | 3 | 29.82*** | ||||||
| Less than $5,000 to $14,999 | N = 32 | N = 7 | N = 39 | |||||
| $15,000–$29,999 | N = 2S | N = 26 | N = 54 | |||||
| $30,000–$49,999 | N = 11 | N = 28 | N = 39 | |||||
| $50,000 and up | N = 10 | N = 11 | N = 25 | |||||
| N = 81 | N = S6 | N = 167 | ||||||
Note. ADL = limitations in activities of daily living; IADL = limitations in instrumental activities of daily living; MMSE = Mini Mental Status Exam Score; CR = care recipient; CG = caregiver.
p<.05.
p<.001.
Measures
The core battery of measures for the REACH study is described in Wisniewski et al. (2003). The Structural Family Systems Ratings–Dementia Caregiver (SFSR-DC) was administered only at the Miami site. All self-report measures were translated and back translated into Spanish using the method recommended by Kurtines and Szapocznik (1995). The SFSR and the primary outcome and predictor measures chosen for the present study are described below.
Care recipient functioning was measured using the Mini-Mental State Exam (MMSE; Folstein, Folstein, & McHugh, 1975), Activities of Daily Living Scale (Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963), and Instrumental Activities of Daily Living Scale (Lawton & Brody, 1969). The 11-item CG/CR Sociodemographic Information Form provided information on ethnicity/race, place of birth, marital status, educational attainment, where education was completed, income, number of people living in the home, whether the CG moved in with CR to provide care, and employment.
Caregiver Depression was measured using the Center for Epidemiologic Studies Distress Scale (CES-D; Radloff, 1977), a 20-item self-report of depressive symptoms. The instrument asks about the frequency of depressive symptoms within the last week (four-point scale). This study used the overall CES-D score, which is the sum of all items. The instrument has relatively high internal reliability and predictive validity (Baker, Velli, Friedman, & Wiley, 1995). A score of 16 or above has been identified as discriminating between groups with clinically relevant and nonrelevant depressive symptoms (Radloff & Teri, 1986). In the current sample, 49.4% of caregivers scored above the clinical cutoff. Cronbach’s alpha in the current sample was 0.86.
Caregiver Anxiety was measured using the State Anxiety Inventory (SAI; Spielberger, 1979), which consists of 10 items comprising the state anxiety subscale of Spielberger’s State-Trait Personality Inventory (STAI; Spielberger, Gorsuch, Lushene, Vagg, & Jacobs, 1983). In the SAI, respondents are asked how much they agreed with statements such as “I feel nervous” (four-point scale). Four of the items are scaled negatively. The SAI was modified for REACH by changing the duration of time being from “right now” to “during the past week.” Cronbach’s alpha for this scale in the current sample was 0.87.
Caregiver Distress was measured using a composite of the two indicators of depression and anxiety. In this sample, the Pearson correlation between depression and anxiety was 0.76. Because of the high level of multicollinearity, we calculated a composite distress index by summing the standardized depression and anxiety scores. We utilized the z-score transformation before summing so that both variables would have a common scale.
Conflict Resolution was assessed using the conflict resolution subscale of the Structural Family Systems Ratings-Dementia Caregiver (SFSR-DC; Mitrani et al., 2005), an adaptation of the Structural Family Systems Ratings (SFSR; Szapocznik et al., 1991). The SFSR-DC is an observational measure that uses a standardized procedure, the Wiltwick Family Tasks (Minuchin, Rosman, & Baker, 1978), for eliciting family interaction on three activities (planning a menu, stating likes and dislikes about each other, and discussing a recent family argument). The current study uses a subsample from the SFSR-DC validation study (Mitrani et al., 2005). The 182 families in the current study included 147 families whose first SFSR-DC was conducted at baseline and 35 whose first SFSR-DC was at a later time point. These latter families were enrolled in the study since baseline but had missing baseline SFSR-DC’s because of unavailability of the CR, poor videotape quality, or breaches in administration of the family tasks.
The SFSR-DC was rated by a trained rater and the first author, who observed and coded videotapes of the family performing these tasks. Rater training consisted of the two raters reviewing the coding manual, rating five tapes together, and rating five tapes independently followed by meetings to reconcile discrepancies. Calibration between raters continued throughout the study. In this study, as in the validation study of the SFSR-DC, interrater reliability calculated with an intraclass correlation on the conflict resolution subscale was 0.80 (Mitrani et al., 2005). Internal consistency is not calculated for this subscale because items represent mutually exclusive categories.
The SFSR-DC yields scores on six subscales: disengagement of the care recipient, enmeshment/cohesion, identified patienthood, expressed anger, expressed positive affect, and conflict resolution. The range of scores on each subscale is from 1 (highly problematic) to 5 (highly adaptive). The six subscale scores are summed to determine the total score. The total SFSR-DC score has been found to be related to caregiver distress, anxiety, and subjective burden. The measure has been provisionally cross-validated and showed invariance across Cuban American and White, non-Hispanic American subsamples (Mitrani et al., 2005). The current study examined only the conflict resolution scale of the SFSR-DC as a mediator.
With the conflict resolution scale, raters first assess the manner in which the family manages specific differences of opinions, or conflicts, during a task. Each difference of opinion that occurs during either of two tasks (planning a menu and discussing a family argument) is assigned to one of five categories. The lowest category is denial (acting as though a conflict or problem does not exist), followed by avoidance (the conflict or problem emerges but is “swept under the rug”), next is diffusion (moving on to another conflict or problem without resolving the previous one), then emergence (discussion of the conflict or problem) without reaching a resolution, and the highest level is emergence with resolution, which is rated when the family expresses a disagreement and is able to agree on a conclusion or when they succeed in performing the overall task as instructed. Additionally, the rater assigns each of the three tasks to a category based on overall resolution of the task.
After viewing the tasks, the rater counts the number of single conflicts assigned to each category and ratings of overall tasks. The count of each of the five categories is summed to form a weighted conflict score, with the total number of denials having a weight of 0, the total number of avoidances a weight of 1, diffusions a weight of 2, emergences without resolution a weight of 3, and emergences with resolution a weight of 5. The ratio of the weighted conflict score to the total count of conflicts observed in each task is the conflict resolution score. Families are then assigned to one of the five categories to describe their total conflict resolution across all three tasks. Thus, the conflict resolution score is not influenced by how many disagreements the family has but merely how they tend to manage disagreements and overall tasks.
In addition to the conflict resolution rating, which represents an average of the 1 to 5 ordinal scale and thus gives an overall sense of the family’s success in managing conflict, it is possible to examine the relative frequency of each category of conflict resolution for a particular family or group of families. While this manner of reviewing the ratings is not used for scoring of the SFSR, it can yield information that is clinically distinct from the overall rating. For example, two families can each receive a conflict resolution score of 3 yet have very different styles of managing conflict. One family can get a conflict resolution score of 3 by receiving an equal number of denials (scored as l’s) and emergences with resolution (scored as 5’s), and having no other ratings; another family could get a conflict resolution score of 3 by receiving ratings that consist purely of diffusions (scored as 3’s). More typically, families have a smattering of different types of resolutions, but may favor one type over another.
Data were analyzed at the family level with 182 independent observations, one for each participating family. Although eligibility for the parent study required that three individuals (a third family member in addition to the CG and CR) were willing to participate, family tasks for videotape ratings were administered even if only two individuals (the CG and CR) were present. Thirty-six families had only two individuals, the CG and CR. The average number of participants in the family tasks was 3.04 (SD = 0.73). At the individual level, family members other than the CG and CR who participated were daughters (n = 47), sons (n = 33), husbands (n = 22), sisters (n = 15), daughters-in-law (n = 11), brothers (n = 10), sisters-in-law (n = 8), other extended family (n = 28), friends/neighbors (n = 11), and hired aides (n = 3).
Results
Testing Group Differences
We first examined whether there were significant differences between the two ethnic groups on our predictor (conflict resolution) and outcome (distress) variables, as well as on a variety of demographic variables. Although our focus was on conflict resolution, we examined differences between ethnic groups on the demographic variables in order to provide some degree of statistical control for alternative explanations for the difference in distress. The results of the one-way ANOVAs and chi-squares are presented in Table 1. As these comparisons were designed to decide whether to include variables in the mediation model, we used the less conservative strategy of not using a Bonferroni correction. In comparison to the White non-Hispanic American caregivers, Cuban American caregivers were more distressed, and their families had lower conflict resolution scores. The Cuban American caregivers were also less educated and had lower incomes. The ethnic groups did not differ on caregiver age or gender, relationship between the caregiver and care recipient, care recipient activities of daily living, instrumental activities of daily living or mini-mental score, or number of participants in the family tasks.
Examining the Prevalence of Conflict Resolution Categories
We examined differences between ethnic groups in the number of each of the five categories of conflict resolution (i.e., denial, avoidance, diffusion, emergence without resolution, emergence with resolution) based on single differences of opinion. For both ethnic groups, denial was the most prevalent manner in which they managed conflict; diffusion was second; emergence with resolution was third; emergence without resolution was fourth; and avoidance was the least frequently used. Independent samples t-tests showed that the Cuban American group used more denial, t (180) = −3.69, p < .001, than White, non-Hispanics, while White, non-Hispanics used more avoidance, t (180) = 1.97, p < .05, and more emergence with resolution, t (180) = 3.73, p < .001, than did the Cuban Americans. These results are summarized in Table 2.
TABLE 2.
Means and Standard Deviations of Each Conflict Resolution Category Rating Across Three Tasks by Ethnic Group
| Cuban Americans |
White, Non-Hispanic |
||||
|---|---|---|---|---|---|
| Conflict Resolution Category | M | SD | M | SD | t |
| Denial | 3.77 | 2.36 | 2.60 | 1.93 | −3.69*** |
| Avoidance | 0.93 | 1.03 | 1.28 | 1.34 | 1.97* |
| Diffusion | 2.10 | 2.16 | 2.41 | 2.13 | 0.98 |
| Emergence without resolution | 1.13 | 1.24 | .96 | 1.10 | −0.98 |
| Emergence with resolution | 1.24 | 1.44 | 2.12 | 1.71 | 3.73*** |
| N = 84 | N = 98 | ||||
p<.05.
p<.01.
p<.001.
Testing Mediation
Mediation was tested using the bias-corrected bootstrap method (MacKinnon, Lockwood, & Williams, 2004). The statistical package used was Mplus Version 3.12 (Muthén & Muthén, 2004), which allows modeling with ordered categorical observed variables (both conflict resolution and income are measured as ordered categorical variables). This is achieved by estimating the probability of observing the categories (a nonlinear function) using a robust, weighted, least-squares estimator. Mplus also uses full information maximum likelihood estimation to account for missing data. The bias-corrected bootstrap method forms standard error estimates based on the empirical distribution of the model estimates by resampling and corrects for bias in the central tendency of the estimate. MacKinnon et al. (2004) state that this method produces more accurate confidence intervals for the test of mediation with higher power than other methods. The coefficient and p-statistic associated with the product of the paths to and from the proposed mediating variable were estimated, and a 95% confidence interval (CI) was constructed around the product of the paths. The absence of zero in the confidence interval indicates a significant mediation effect.
We first tested an overall model, presented in Figure 1, which tested whether conflict resolution and two demographic variables that were significantly different between the ethnic groups—years of education and income level-mediated the relationship between ethnicity and caregiver distress. Consistent with the results presented in Table 1, significant paths were found between ethnicity and all three proposed mediators. After including the proposed mediators, the path from ethnicity to caregiver distress was reduced to nonsignificance (β = 0.16, B = 0.60, SEB = 0.29, p < .05 to = −0.06, B = −0.22, SEB = 0.40, ns). Significant paths were found that indicated mean differences between the ethnic groups in years of education (β = −0.45, B = −3.50, SEB = 0.56, p < .0001), conflict resolution (β = −0.32, B = −0.67, SEB = 0.16, p < .0001), and income level (β = −0.41, B = −0.91, SEB = 0.18, p < .0001). Significant paths were found between income level and caregiver distress (β = −0.25, B = −0.43, SEB = 0.15, p < .01) and between conflict resolution and caregiver distress (B = −0.23, B = −0.42, SEB = 0.15, p < .01). The path between years of education and caregiver distress was not significant (β = −0.09, B = −0.22, SEB = 0.04, ns). The product of the paths from ethnicity to conflict resolution and from conflict resolution to caregiver distress was significant (β = 0.07, B = 0.28, SEB = 0.12, p < .05, 95% CI(B) = 0.07, 0.60). In addition, the product of the paths from ethnicity to income level and from income level to caregiver distress was significant (β = 0.10, B = 0.39, SEB = 0.15, p < .01, 95% CI(B) = 0.12, 0.74). Therefore, both income and conflict resolution partially mediated the relationship between ethnicity and caregiver distress, controlling for the other variables in the model.
Figure 1.
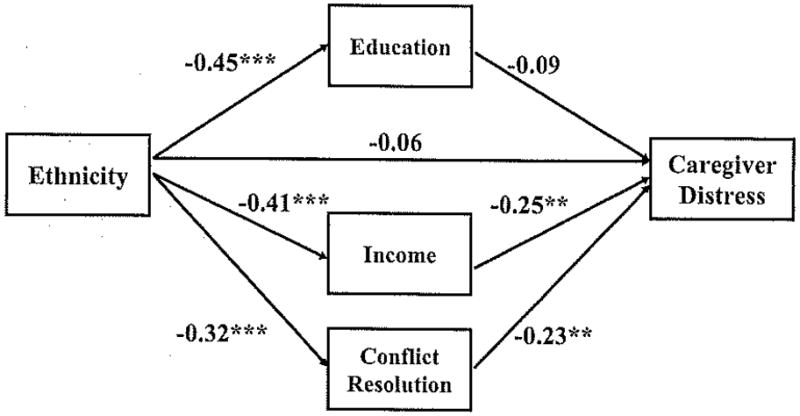
Path model of conflict resolution, level of income, and years of education mediating the relationship between ethnic group and caregiver distress (standardized solution; N = 182).
Note. RMSEA = 0.00; Chi-square and CFI not defined for analysis with categorical variables.
**p < .01. ***p < .001.
We followed up on these findings by testing whether any or all of the five conflict resolution categories mediated the relationship between ethnicity and caregiver distress. This model is presented in Figure 2. The same analysis strategy as in the overall model was used. Consistent with the results from Table 2, significant paths were found between ethnicity and three of the five proposed mediators. These significant paths indicated mean differences between ethnic groups in the total denials (β = 0.27, B = 1.17, SEB = 0.31, p < .001), total avoidances (β = −0.14, B = −0.35, SEB = 0.16, p < .05), and total emergences with resolution (β = −0.27, B = −0.88, SEB = 0.23, p < .001) for each ethnic group. The path between emergence with resolution and caregiver distress was significant (β = −0.19, B = −0.22, SEB = 0.10, p < .05). No other paths to caregiver distress were significantly different from zero. After including the five conflict resolution categories, the path from ethnicity to caregiver distress was reduced to nonsignificance (β = 0.08, B = −0.29, SEB = 0.33, ns). The product of the paths from ethnicity to emergence with resolution and from emergence with resolution to caregiver distress was significant (β = 0.05, B = 0.20, SEB = 0.11, p < 0.05, 95% CI(B) = 0.03, 0.46). Therefore, emergence with resolution mediated the relationship between ethnicity and caregiver distress.
Figure 2.
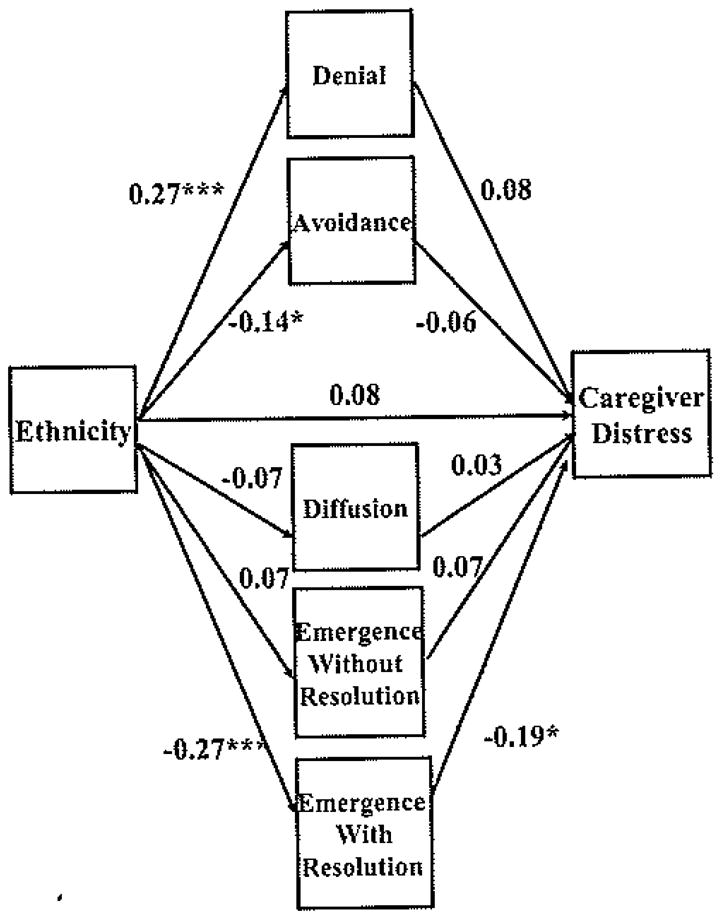
Path model of five styles of conflict resolution mediating the relationship between ethnic group and caregiver distress (standardized solution; N= 182).
Note. Chi-square = 1.107, df = 4, p < .89; CFI = 1.00; RMSEA = .000. Correlated errors not shown.
*p < .05. ***p < .001.
Assessing Potential Confounding Variables
We assessed if the addition of 35 postbaseline cases to the 147 baseline cases was acceptable. First, we tested whether the path models held across the two groups of cases (baseline and postbaseline) using multiple group path analysis. This procedure compares the relative fit of a model that constrains the two groups to have the same paths to an alternative model where the two groups are allowed to have different paths. There was not a statistically significantly difference in fit between the two alternative models for either the overall mediation model (χ2 [df = 9] = 13.03, ns) or the mediation model by conflict resolution category (χ2 df = 9] = 15.74, ns). The absence of significant differences between the two alternative models suggested that differences in the overall pattern of paths between cases drawn from baseline and postbaseline were unlikely.
Next, we tested for a significant influence of intervention assignment on caregiver distress and conflict resolution after adding the postbaseline cases. Two dummy-coded variables representing comparisons of each of the two active interventions to the control group were added to the overall mediation model. Neither the effect of the family intervention (β = −0.02, ns) nor the effect of the technology-enhanced family intervention (β = −0.11, ns) on caregiver distress were significantly different from the control group. Likewise neither the effect of the family intervention (β = 0.01, ns) nor the effect of the technology-enhanced family intervention (β = −0.03, ns) on conflict resolution were significantly different from the control group. The absence of statistically significant intervention effects indicated that the addition of postbaseline cases was unlikely to confound the results of the mediation analyses with intervention effects.
Discussion
One of the important challenges for family intervention science is to develop a better understanding of the interplay between ethnicity, family functioning, and individual outcomes. Understanding the mechanisms that underlie the vulnerability of a particular group of caregivers is valuable for guiding the development of culturally specific interventions aimed at preventing and alleviating caregiver distress. This study followed up on an earlier finding that the manner in which families address conflict is a significant factor in predicting caregiver distress (Mitrani et al., 2005). Using an observation-based measure of family conflict resolution, the current study found some differences in how Cuban American and White non-Hispanic American caregiver families managed conflict While for both ethnic groups the most common manner of addressing conflict was denial—that is, acting as if a problem or disagreement does not exist—the Cuban American families used denial significantly more often than the White, non-Hispanic families. Also, mirroring research findings with a different health-related population (Fisher et al., 2000), the Cuban American families used less conflict avoidance, on average, than their non-Hispanic, White counterparts. However, while these ethnic differences are interesting from an anthropological perspective, neither denial nor conflict avoidance were associated with caregiver distress, which indicates that these differences may not be clinically relevant.
The more important finding from a treatment development perspective is the potentially protective impact of successfully resolving family conflict. The Cuban American families in our sample were less likely than the White, non-Hispanic American families to reach resolution on disagreements, and this, in rum, may render Cuban American caregivers more at risk for emotional distress. This effect was found even when controlling for some other significant factors that differentiated the two ethnic groups, such as education and income, and may be an underlying mechanism driving the elevated levels of distress among Cuban American caregivers. The findings of this study suggest that interventions that help families successfully resolve their disagreements might help to alleviate or prevent caregiver distress, and may be particularly indicated among Cuban American caregivers. Such an intervention has to be addressed in a culturally sensitive and congruent manner, with an understanding of the intrapersonal and interpersonal barriers to confronting conflict, particularly in late-life families.
Limitations
Limitations in this study warrant caution in interpreting results. First, the definition of “family” in the parent study was left to the discretion of the caregiver, and our sample includes only those family members who chose to attend after being invited by the caregiver. Therefore the sample may be overrepresented by family members who have positive relationships with the caregiver. The complexity of defining who constitutes a family unit and the difficulty of recruiting all members of a family represent inherent difficulties in conducting family research. These issues are particularly complex in late-life families because of developmental transitions associated with age, such as relocations that make it difficult to include geographically distant but nevertheless influential family members, the recent losses of significant family members to death or disability, and the importance of recently formed informal kinship networks that may include neighbors and hired aides.
A further limitation associated with family definition and recruitment is that 35 families consisted of only the caregiver and care recipient. While we could not conduct our mediation analyses with such a small subsample, interrater reliability of the conflict resolution subscale was satisfactory (kappa = 0.82; n = 13, from the entire sample in the parent study).
Finally, it is important to state that while this study may be generalizable to other Cuban American caregiver families, it should not be assumed that other Hispanic subgroups would have similar patterns of conflict resolution.
Directions for Future Research
The ultimate aim of this study was to provide information that could assist family clinicians in developing culturally informed family interventions for dementia caregivers. Treatment development efforts aimed at helping Cuban American caregiver families resolve conflict and problems are needed, followed by controlled efficacy studies. As for more basic research, it would be helpful to examine whether the content of conflicts (i.e., whether the disagreements are about a caregiving issue) is relevant to ethnicity-related differences in conflict resolution and the role of conflict resolution in caregiver distress.
In addition to conflict resolution, income was also a significant mediator of the difference in emotional distress between the two ethnic groups. Seventy-four percent of the Cuban American caregivers had annual incomes below $30,000, as compared to 38% of the White, non-Hispanic Americans. Low income and its associated conditions, such as reduced availability of respite and other services, are significant social stressors confronted by ethnic minority elders. The results of this study indicate that low-income Cuban American caregivers are at especially high risk for distress, regardless of family functioning. The current sample size precludes examining an interaction effect; however, the possibility that the confluence of Cuban American ethnicity and low income may have more than an additive (negative) effect on psychological distress of caregivers is worthy of investigation.
The present study tested a simple mediation model within a cross-sectional framework. Investigating whether the model holds longitudinally is warranted. Further research is needed to determine if family-based interventions that successfully address conflict resolution will reduce the distress experienced by dementia caregivers.
Acknowledgments
This study was supported by a mentored scientist development grant from the National Institute on Aging (K01AG00977) to Victoria Mitrani, and a grant from the National Institute on Aging and National Institute on Nursing Research (VO1AG13292) to Carl Eisdorfer. We express our gratitude to Sara Czaja, Carl Eisdorfer, Jose Szapocznik, Monica Zarate, and the families who participated in this study.
Contributor Information
Victoria B. Mitrani, University of Miami School of Nursing and Health Studies.
Ellen L. Vaughan, University of Miami School of Education.
Brian E. McCabe, University of Miami School of Education.
Daniel J. Feaster, Florida International University Stempel School of Public Health.
References
- Baker FM, Velli SA, Friedman J, Wiley C. Screening tests for depression in older Black versus White patients. American Journal of Geriatric Psychiatry. 1995;3:43–51. doi: 10.1097/00019442-199524310-00006. [DOI] [PubMed] [Google Scholar]
- Dilworth-Anderson P, Williams IC, Gibson BE. Issues of race, ethnicity, and culture in caregiving research: A 20-year review (1980–2000) The Gerontologist. 2002;42:237–272. doi: 10.1093/geront/42.2.237. [DOI] [PubMed] [Google Scholar]
- Eisdorfer C, Czaja SJ, Loewenstein DA, Rubert MP, Arguelles S, Mitrani VB, et al. The effect of a family therapy and technology-based intervention on caregiver depression. The Gerontologist. 2003;43:521–531. doi: 10.1093/geront/43.4.521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher L, Gudmundsdotter M, Gilliss C, Skaff M, Mullan J, Kanter R, et al. Resolving disease management problems in White, non-Hispanic-American and Latino couples with type 2 diabetes: The effects of ethnicity and patient gender. Family Process. 2000;39:403–416. doi: 10.1111/j.1545-5300.2000.39402.x. [DOI] [PubMed] [Google Scholar]
- Fisher L, Lieberman MA. The effects of family context on adult offspring of patients with Alzheimer’s disease: A longitudinal study. Journal of Family Psychology. 1996;10:180–191. [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: A practical method for grading the cognitive state of patients for the clinician. journal of Psychiatric Research. 1975;12:189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Harwood DG, Barker WW, Cantillon M, Loewenstein DA, Ownby RL, Duara R. Depressive symptomatology in first-degree family caregivers of Alzheimer’s disease patients: A cross-ethnic comparison. Alzheimer’s Disease and Associated Disorders. 1998;12:340–346. doi: 10.1097/00002093-199812000-00015. [DOI] [PubMed] [Google Scholar]
- Janevic MR, Connell CM. Racial, ethnic, and cultural differences in the dementia caregiving experience: Recent findings. The Gerontologist. 2001;41:334–347. doi: 10.1093/geront/41.3.334. [DOI] [PubMed] [Google Scholar]
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: The index of ADL, a standardized measure of biological and psychosocial function. Journal of the American Medical Association. 1963;185:914–919. doi: 10.1001/jama.1963.03060120024016. [DOI] [PubMed] [Google Scholar]
- Kurtines WM, Szapocznik J. Cultural competence in assessing Hispanic youths and families: Challenges in the assessment of treatment needs and treatment evaluation for Hispanic drug abusing adolescents. In: Rahdert E, Czechowicz D, editors. Adolescent drug abuse: Clinical assessment and therapeutic interventions. (NIDAResearch Monograph No. 156, NIH Publication No. 95-3908) Bethesda, Maryland: NIDA; 1995. pp. 172–189. [PubMed] [Google Scholar]
- Lawton MP, Brady EM. Assessment of older people: Self-maintaining instrumental activities of daily living. The Gerontologist. 1969;9:179–186. [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the produce and resampling methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minuchin S. Families and family therapy. Cambridge, MA: Harvard University Press; 1974. [Google Scholar]
- Minuchin S, Rosman BL, Baker L. Psychosomatic families: Anorexia nervosa in context. Cambridge, MA: Harvard University Press; 1978. [Google Scholar]
- Mitrani VB, Feaster DJ, McCabe BE, Czaja SI, Szapocznik J. Adapting the Structural Family Systems Rating to assess the patterns of interaction in families of dementia caregivers. The Gerontologist. 2005;46:97–105. doi: 10.1093/geront/45.4.445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 3. Los Angeles, CA: Muthén & Muthén; 2004. [Google Scholar]
- Ory MG, Yee JL, Tennstedt SL, Schulz R. The extent and impact of dementia care: Unique challenges experienced by family caregivers. In: Schulz R, editor. Handbook of dementia caregiving: Evidence-based interventions for family caregivers. New York: Springer Publishing; 2000. [Google Scholar]
- Radloff L. The Center for Epidemiological Studies Depression Scale: A self-report depression scale for research in the general population. Applied Psychological Measurements. 1977;3:385–401. [Google Scholar]
- Radloff LS, Teri L. Use of the Center for Epidemiological Studies-Depression Scale with older adults. Clinical Gerontologist. 1986;5(1–2):119–136. [Google Scholar]
- Schulz R, Burgio L, Burns R, Eisdorfer C, Gallagher-Thompson D, Gitlin LN, et al. Resources for Enhancing Alzheimer’s Caregiver Health (REACH): Overview, site-specific outcomes, and future directions. The Gerontologist. 2003;43:514–520. doi: 10.1093/geront/43.4.514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulz R, Visitainer P, Williamson GM. Psychiatric and physical morbidity effects of caregiving. Journal of Gerontology. 1990;45:181–191. doi: 10.1093/geronj/45.5.p181. [DOI] [PubMed] [Google Scholar]
- Spielberger CD. Preliminary manual for the State-Trait Personality Inventory (STPI) Tampa: University of South Florida; 1979. [Google Scholar]
- Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. State Trait Anxiety Inventory for adults manual. Palo Alto, CA: Consulting Psychologists Press; 1983. [Google Scholar]
- Szapocznik J, Rio AT, Hervis OE, Mitrani VB, Kurtines WM, Faraci AM. Assessing change in family functioning as a result of treatment: The Structural Family Systems Rating Scale (SFSR) Journal of Marital and Family Therapy. 1991;17(3):295–310. [Google Scholar]
- Wisniewski S, Belle S, Coon D, Marcus S, Ory M, Burgio L, et al. The Resources for Enhancing Alzheimer’s Caregiver Health (REACH): Project design and baseline characteristics. Psychology and Aging. 2003;18:375–384. doi: 10.1037/0882-7974.18.3.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zarit SH, Johansson L, Jarrott SE. Family caregiving: Stress, social programs, and clinical interventions. In: Nordhus IH, VandenBos GR, Berg S, Fromholt P, editors. Clinical geropsychology. Washington, DC: American Psychological Association; 1998. pp. 345–360. [Google Scholar]