

Abstract
Objective
To compare differences in degree of bother in black and white women with urinary incontinence (UI).
Study Design
A population-based study was conducted in black and white women in Michigan. Participants completed an interview and the Incontinence Impact Questionnaire short form (IIQ-7). Statistical analysis included 2-way ANOVA for post-hoc comparisons of IIQ-7 scores between races at different frequencies, amounts, and types of UI.
Results
Black women with moderate UI had significantly higher IIQ-7 scores than white women (31.4 ± 3.5 vs. 23.7 ± 1.9, p=.03). Overall, black women with urge incontinence had higher scores than white women (30.5 ± 4.0 vs. 21.0 ± 3.0, p=.05). After adjusting for severity, black women with urge and mixed incontinence tended to be more bothered (p=.06).
Conclusion
With moderate UI (not mild or severe), black women are more bothered than white women. At this discriminatory level of UI severity, racial differences are important, as they may dictate care-seeking.
Keywords: urinary incontinence, bother, race
Introduction
Urinary incontinence (UI) is a common problem affecting many women, and has a peak incidence between the ages of 45 and 55 years.1 The prevalence and risk factors associated with UI have been extensively studied in Caucasian women, 2,3 and more recently, studies looking at racial differences in incontinence patterns have been published. 4-7 The EPI study (Establishing the Prevalence of Incontinence) was conducted primarily to evaluate racial differences in incontinence8 and found that the prevalence of UI was significantly lower in black women than white women (14.6% vs. 33.1%), and that a larger proportion of black women complained of pure urge incontinence compared to white women. Conversely, more white women reported symptoms of pure stress incontinence.
It is well known that UI has a significant impact on quality of life.9-11 However, little is known about the impact of UI or degree of bother in different races and how this may impact care-seeking behavior. The aim of this study was to examine differences in degree of bother in women with UI in a sample of black and white community-dwelling women in the EPI study. Specifically, we were interested in examining the impact of and racial differences in frequency of UI episodes, amount of urine loss, and type of UI in black and white women.
Materials and Methods
As previously described8, the EPI study was conducted at the University of Michigan with the primary purpose of examining differences between black and white women in UI prevalence, frequency, quantity, type and risk factors. Briefly, this study included community-dwelling black and white women aged 35 to 64 years. Using purchased telephone records from geographical areas of known racial composition within southeastern Michigan, trained female telephone interviewers called the households to screen for eligible participants. Women in this age group, who self-identified as black or white race and who had not been pregnant in the last 12 months, were identified and deemed eligible for a 20 minute interview to assess their demographics and overall health and lifestyle factors. Overall, 1,922 black and 892 white women completed the telephone survey. The study was approved by the university’s institutional review board (IRBMED# 2000-0824). Black women were deliberately oversampled.
As part of this survey, the 580 (black, 282 and white 298) women who reported at least 12 episodes of incontinence in the last 12 months were further queried about their urine loss. Frequency of UI episodes per month (<1, 1-4, 5-24 and 25-90) and type of incontinence (mixed, stress, urge, below threshold) were determined based on a 10-item questionnaire (modified Medical Epidemiologic and Social Aspects of Aging; MESA questionnaire)12 assessing how often and during which activities/situations this urine loss occurred as previously described8. Incontinence “below threshold” denoted women who did not reach a threshold of “often” on any of the 10 questions. Women were also asked to quantify amount of urine loss as (1) few drops, (2) wet underwear or pad, (3) soak outer clothes, or (4) drip onto floor.
To assess bother, women completed the Incontinence Impact Questionnaire short form (IIQ-7), which is a more global, life-impact assessment instrument, specific to UI.13 The IIQ-7 is a 7 item questionnaire scored on a 0-3 Likert scale with scores ranging from 0 to 100. Higher scores indicate greater degree of bother. In order to assess severity of symptoms, a modified Sandvik scale14 was calculated. This severity index is a product of a four-category frequency variable (0, 1-4, 5-24, ≥ 25 episodes of leakage per month in the last 12 months) and a two-category quantity variable (few drops vs. all greater quantities). Because women reporting “0” as their frequency of leakage inherently cannot report a quantity of leakage, this produced 6 possibilities for a variable coded 1, 2, 3, 4, 6, 8. This range was then collapsed into three categorical variables of UI severity including mild (1,2), moderate (3,4), and severe (6,8).
All statistical analyses were performed using SAS version 9.1.3 (SAS Institute, Inc., Cary, North Carolina). Data reflect values weighted to represent the population from which the sample was taken as detailed in our previously published analysis.8 Statistical analysis included 2-way analysis of variance (ANOVA) for post-hoc comparisons of IIQ-7 scores between the two races at different levels of frequency, amount and type of UI. On bivariate analysis, significant correlations between IIQ scores and education, self-reported health, BMI and alcohol use were found. All multivariate models were adjusted for these significant covariates.
Results
The characteristics of the study population are shown in Table 1. Overall, black women had a higher mean BMI, more vaginal deliveries, and less Cesarean section deliveries than white women. Black women also reported completing fewer years of higher education and overall poorer self-rated health. More black women had hysterectomies and hypertension while fewer reported currently drinking alcohol (Table 1).
Table 1.
Demographics, health history, lifestyle and obstetric/gynecologic characteristics of study sample
| Black (n=282) | White (n=298) | P* | |
|---|---|---|---|
| Age (years) | 50.5 ± 7.3 | 51.4 ± 7.9 | 0.170 |
| BMI (kg/m2) | 33.0 ± 7.5 | 30.8 ± 8.2 | 0.001 |
| Years of education | <0.001 | ||
| < 12 | 11 (3.9) | 14 (4.7) | |
| 12 | 70 (24.8) | 71 (23.8) | |
| 13-15 | 132 (46.8) | 76 (25.5) | |
| ≥ 16 | 69 (24.5) | 137 (46.0) | |
| Household income | 0.922 | ||
| < $35K | 76 (27.0) | 76 (25.5) | |
| $35K- $70K | 72 (25.5) | 72 (24.2) | |
| >$70K | 108 (38.3) | 116 (38.9) | |
| Not reported | 26 (9.2) | 34 (11.4) | |
| Self-rated health | <0.001 | ||
| Excellent | 18 (6.4) | 34 (11.4) | |
| Very good | 54 (19.2) | 98 (32.9) | |
| Good | 105 (37.2) | 103 (34.6) | |
| Fair | 79 (28.0) | 50 (16.8) | |
| Poor | 26 (9.2) | 13 (4.4) | |
| Hypertension | 144 (51.1) | 96 (32.2) | <0.001 |
| Hysterectomy | 98 (34.8) | 70 (23.5) | 0.003 |
| Surgery for fallen uterus, bladder, or bowel | 20 (7.1) | 26 (8.7) | 0.456 |
| Surgery for urinary incontinence | 9 (3.2) | 16 (5.4) | 0.197 |
| # Vaginal births | 0.002 | ||
| 0 | 63 (22.3) | 81 (27.2) | |
| 1 or 2 | 113 (40.1) | 120 (40.3) | |
| 3 or more | 105 (37.2) | 94 (31.5) | |
| Not reported | 1 (0.4) | 3 (1.0) | |
| # C-section deliveries | 0.011 | ||
| 0 | 215 (76.2) | 255 (85.6) | |
| 1 or 2 | 52 (18.4) | 27 (9.1) | |
| 3 or more | 9 (3.2) | 6 (2.0) | |
| Not reported | 6 (2.1) | 10 (3.3) | |
| Currently smoke cigarettes | 76 (27.0) | 71 (23.8) | 0.467 |
| Currently drink alcoholic beverages | 120 (42.6) | 158 (53.0) | 0.012 |
Values reported as mean ± standard deviation or n (%)
Chi-square p value for categorical and t-test p-value used for differences in means among black and white women
To examine potential confounding effects, those characteristics that were significantly different between the races were then incorporated into a multivariate regression analysis with IIQ-7 score as the primary outcome. Education, BMI, self-rated health and alcohol use were all significantly associated with bother as assessed by the IIQ-7 (p<0.001). Thus, all models were adjusted for these four covariates to adjust for confounding.
IIQ-7 scores were then compared between the two races across various levels of UI frequency and quantity of urine loss. Among black women, incontinence frequency and mean IIQ-7 score were directly related; as frequency increased, bother did as well. This was true for white women at frequencies greater than 1 time (Table 2). Similarly, in both black and white women, mean IIQ-7 scores increased as quantity of urine loss increased (until the group that reported “drip onto the floor”) (Table 2). In this group of women, scores decreased across both races. This was likely a reflection of the small number of women in this group (n=9 for both black and white women). However, for each level of frequency and amount, no racial differences were observed in mean IIQ-7 scores (p>0.05).
Table 2.
IIQ-7 scores among black and white women based on UI frequency (episodes per month) and amount of urine loss in the last 12 months (adjusted for education, BMI, self-reported health, alcohol use)
| IIQ-7 score | P | ||
|---|---|---|---|
| Black Women | White Women | ||
| Incontinence Frequency Level* | |||
| <1† | 13.5 ± 10.9 (n=9) | 38.2 ± 8.0 (n=5) | 0.07 |
| 1-4 | 26.2 ± 3.5 (n=93) | 22.7 ± 2.1 (n=96) | 0.36 |
| 5-24 | 33.1 ± 3.5 (n=91) | 28.6 ± 2.0 (n=99) | 0.23 |
| 25-90 | 38.3 ± 4.0 (n=73) | 33.6 ± 2.0 (n=81) | 0.28 |
| Amount of incontinence‡ | |||
| Few drops | 26.0 ± 3.4 (n=104) | 22.7 ± 1.8 (n=149) | 0.34 |
| Wet underwear/pad | 31.2 ± 2.9 (n=140) | 30.1 ± 1.9 (n=111) | 0.75 |
| Soak outer clothes | 50.3 ± 6.4 (n=27) | 41.1 ± 3.2 (n=25) | 0.19 |
| Drip onto floor | 38.6 ± 10.4 (n=9) | 31.2 ± 6.1 (n=9) | 0.54 |
Mean ± standard error reported
Information on frequency was provided by 547 women
There were 14 women who reported leaking ≥12 times/year, but did not leak at least once a month because their leakage was episodic or seasonal.
Information on quantity was provided by 574 total women
Overall, there was a strong positive correlation between mean IIQ-7 scores and modified Sandvik scores for both black and white women (correlation coefficient r=0.31, p<0.0001). When IIQ-7 scores among black and white women with minimal, moderate and severe UI, black women had significantly higher mean IIQ-7 scores at moderate severities (p=0.03) (Table 3).
Table 3.
Correlation of IIQ-7 and modified Sandvik scores among black and white women (adjusted for education, BMI, self-reported health, alcohol use)
| IIQ-7 Score | P | ||
|---|---|---|---|
| Black Women | White Women | ||
| Modified Sandvik Score | |||
| Minimal | 19.9 ± 4.3 (n=58) | 22.6 ± 2.4 (n=67) | 0.56 |
| Moderate | 31.4 ± 3.5 (n=96) | 23.7 ± 1.9 (n=118) | 0.03 |
| Severe | 36.7 ± 3.0 (n=126) | 34.9 ± 1.8 (n=109) | 0.60 |
Mean ± standard error reported
Degree of bother among both races was then examined by type of incontinence (below threshold, mixed, stress, and urge). Overall, women with mixed incontinence (irrespective of race) were bothered the most by their UI, after adjusting for education, BMI, self-reported health and alcohol use (Figures 1 and 2). Black women with urge incontinence were more bothered than their white counterparts after adjusting for these covariates (Figure 1). However, when adjusting for the above covariates as well as for severity, black women with both urge and mixed incontinence seemed to be more bothered by their UI than white women. Even though the standard errors do not overlap in this comparison, this difference was not statistically significant at this sample size (p=0.06, Figure 2).
Figure 1.
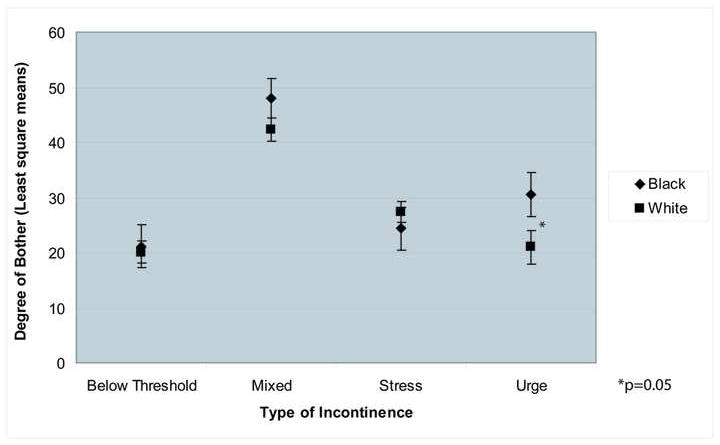
Degree of bother among black and white women based on type of incontinence (adjusted for education, BMI, self-reported health, alcohol use)
Figure 2.
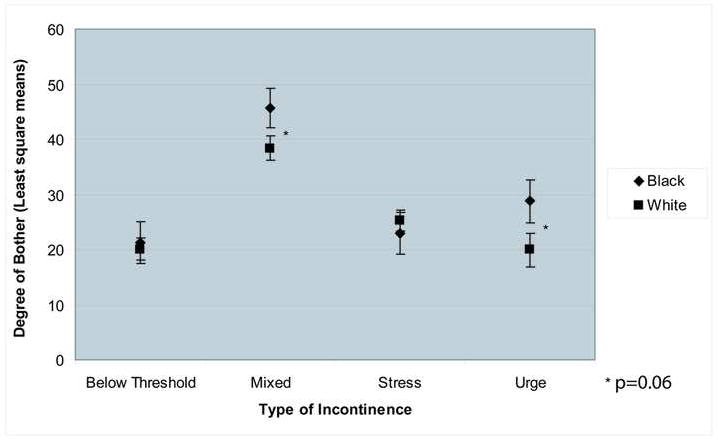
Degree of bother among black and white women based on type of incontinence (adjusted for all covariates as well as severity)
Comment
In this study of community-dwelling black and white women, we found that racial differences in bother due to urinary incontinence (UI) do not exist at the extremes of the incontinence severity spectrum. Black and white women were equally bothered at mild and severe levels of leakage. This is not surprising, as women with very little incontinence are not likely to be very bothered, and those with severe incontinence are all likely to be very bothered. One would assume that few women with rare incontinence would seek treatment and that most women with severe leakage would consult medical care. The women with moderate leakage may or may not seek treatment, depending upon their degree of bother or impact at this level of leakage. It was in this group that we found that black women reported higher degree of bother compared to the white women.
It is known that, in women with overactive bladder symptoms (in primarily white populations), those that report bother tended to seek treatment.7,15 Thus, it becomes important to determine why black women may not be seeking care for their UI. In controlling for other socioeconomic variables as well as severity of UI in this study, our findings suggest that true racial differences in bother exist. Studies have addressed treatment-seeking behavior for UI in more homogenous patient populations.16, 2,17 However, in the future, ultimately determining how patients’ perception of bother influences health-care seeking among racially diverse women will be important, especially in determining whether there are barriers to care, a lack of understanding about the condition and possible treatments, and whether health-care providers are not inquiring about UI symptoms in black women.
As other studies have shown,5 when frequency and quantity of urine leakage increase, bother increased in all of the women in our sample. However, our study extends the published literature, as we were able to look at differences among the two races not only with varying UI frequency and amount, but also with type of leakage in a sample that was 48.6% black. In this racially-diverse study, our results are similar to some and contrary to other studies. In 2004, Bogner et al. reported that African Americans with UI were more likely to experience general, psychological distress than those without UI in a population-based survey of 747 individuals.18 Interestingly, the whites with UI were no more likely to report distress than those without UI. However, information regarding frequency, amount of leakage and type of leakage was not collected in this study, nor was distress specifically related to UI. On the other hand, others have reported no association of race on UI.19 In a study of 654 racially diverse women (6.7% of whom were non-Hispanic black), UI severity (measured by number of leakage episodes during a 3-day voiding diary) and bother (measured with the Urogenital Distress Inventory) did not vary based on race.20
Several possibilities as to why black women with moderate UI in this study were more bothered than white women exist. First, it has been reported that lower socioeconomic status affects racial differences in UI knowledge, more so than race/ethnicity. Kubik et al. created a socioeconomic score (using the occupation of the main household earner and education level of respondent), which was weighted differently for white and minority respondents.21 In our study, household income did not differ between black and white women; however, occupational information was not collected. Similarly, while we did control for the differing educational levels among races, it is possible that we did not account for true socioeconomic status. If socioeconomic status reflects UI knowledge, lack of understanding symptoms associated with UI may lead to worse bother. Secondly, poor self-reported health is known to be associated with more severe UI.22 In our study, black women overall had lower self-reported health; this was adjusted for in our models. It is possible however, that patients’ perceptions about their health were not adequately captured and may have influenced their degree of bother.
In this study, mixed incontinence was the most bothersome type of UI for all women compared to other types of UI. This is consistent with previous studies23, 24, suggesting that the additive effect of both stress and urge symptoms impacts quality of life more than pure urge or pure stress symptoms. Furthermore, it has been reported that the prevalence of urge and mixed incontinence is higher in black compared to white women.8, 25-27 In the primary EPI study, we did find that a larger proportion of black women reported symptoms of pure urge incontinence compared to white women.8 And, in this current study, urge incontinence was significantly more bothersome to black women than white women. In a similar study, Coyne et al. specifically examined the impact of stress, urge and mixed UI on quality of life and found that individuals with urge and mixed incontinence reported significantly worse quality of life than those with pure stress incontinence.28 This study was conducted in an 85% Caucasian population. Our study furthers these results in a diverse cohort of women. When we controlled for severity of incontinence, black women with urge and mixed incontinence still seemed to be more bothered, though the difference was no longer statistically significant. This trend may have maintained its significance in a larger sample of women.
Several important factors must be considered when interpreting the results of this study. First, this arm of the study was based on self-reported incontinence and questionnaire data rather than on voiding diaries. Recall bias is inherent in the study design. Also, this population was recruited from southeastern Michigan, and may not be generalizable to other more urban populations where different socioeconomic circumstances may affect bother. Finally, our population was limited to black and white women. In the future it would be prudent to examine racial effects in other populations of women such as Asian-Americans and Latinas.
Our findings of racial differences in bother secondary to UI should lead us to consider the impact of these differences and how they affect health-seeking behaviors. Despite the lower prevalence of UI among black women, the findings in this study suggest that the disease burden is equal or more bothersome in black women. Screening for incontinence should be routine for all women regardless of race, and efforts are needed to educate women on the prevalence of urinary incontinence and possible treatments.
Footnotes
To be presented at 35th Annual Scientific Meeting of the Society of Gynecologic Surgeons, New Orleans, Louisiana, March 2009.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Reprints will not be available.
References
- 1.Hannestad YS, Rortveit G, Sandvik H, Hunskaar S Norwegian EPINCONT study. Epidemiology of Incontinence in the County of Nord-Trondelag. A community-based epidemiological survey of female urinary incontinence: The norwegian EPINCONT study. epidemiology of incontinence in the county of nord-trondelag. J Clin Epidemiol. 2000;53(11):1150–7. doi: 10.1016/s0895-4356(00)00232-8. [DOI] [PubMed] [Google Scholar]
- 2.Melville JL, Katon W, Delaney K, Newton K. Urinary incontinence in US women: A population-based study. Arch Intern Med. 2005;165(5):537–42. doi: 10.1001/archinte.165.5.537. [DOI] [PubMed] [Google Scholar]
- 3.Whitcomb EL, Lukacz ES, Lawrence JM, Nager CW, Luber KM. Prevalence and degree of bother from pelvic floor disorders in obese women. Int Urogynecol J Pelvic Floor Dysfunct. 2008 Nov 11; doi: 10.1007/s00192-008-0765-x. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Thom DH, van den Eeden SK, Ragins AI, Wassel-Fyr C, Vittinghof E, Subak LL, et al. Differences in prevalence of urinary incontinence by race/ethnicity. J Urol. 2006;175(1):259–64. doi: 10.1016/S0022-5347(05)00039-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tennstedt SL, Fitzgerald MP, Nager CW, Xu Y, Zimmern P, Kraus S, et al. Quality of life in women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(5):543–9. doi: 10.1007/s00192-006-0188-5. [DOI] [PubMed] [Google Scholar]
- 6.Goode PS, Burgio KL, Redden DT, Markland A, Richter HE, Sawyer P, et al. Population based study of incidence and predictors of urinary incontinence in black and white older adults. J Urol. 2008;179(4):1449–54. doi: 10.1016/j.juro.2007.11.069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sampselle CM, Harlow SD, Skurnick J, Brubaker L, Bondarenko I. Urinary incontinence predictors and life impact in ethnically diverse perimenopausal women. Obstet Gynecol. 2002;100(6):1230–8. doi: 10.1016/s0029-7844(02)02241-x. [DOI] [PubMed] [Google Scholar]
- 8.Fenner DE, Trowbridge ER, Patel DA, Fultz NH, Miller JM, Howard D, et al. Establishing the prevalence of incontinence study: Racial differences in women’s patterns of urinary incontinence. J Urol. 2008;179(4):1455–60. doi: 10.1016/j.juro.2007.11.051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wyman JF, Harkins SW, Choi SC, Taylor JR, Fantl JA. Psychosocial impact of urinary incontinence in women. Obstet Gynecol. 1987;70(3 Pt 1):378–81. [PubMed] [Google Scholar]
- 10.Hunskaar S, Vinsnes A. The quality of life in women with urinary incontinence as measured by the sickness impact profile. J Am Geriatr Soc. 1991;39(4):378–82. doi: 10.1111/j.1532-5415.1991.tb02903.x. [DOI] [PubMed] [Google Scholar]
- 11.Fultz NH, Burgio K, Diokno AC, Kinchen KS, Obenchain R, Bump RC. Burden of stress urinary incontinence for community-dwelling women. Am J Obstet Gynecol. 2003;189(5):1275–82. doi: 10.1067/s0002-9378(03)00598-2. [DOI] [PubMed] [Google Scholar]
- 12.Herzog AR, Diokno AC, Brown MB, Normolle DP, Brock BM. Two-year incidence, remission, and change patterns of urinary incontinence in noninstitutionalized older adults. J Gerontol. 1990;45(2):M67–74. doi: 10.1093/geronj/45.2.m67. [DOI] [PubMed] [Google Scholar]
- 13.Uebersax JS, Wyman JF, Shumaker SA, McClish DK, Fantl JA. Short forms to assess life quality and symptom distress for urinary incontinence in women: The incontinence impact questionnaire and the urogenital distress inventory. continence program for women research group. Neurourol Urodyn. 1995;14(2):131–9. doi: 10.1002/nau.1930140206. [DOI] [PubMed] [Google Scholar]
- 14.Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. J Epidemiol Community Health. 1993;47(6):497–9. doi: 10.1136/jech.47.6.497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Irwin DE, Milsom I, Kopp Z, Abrams P EPIC Study Group. Symptom bother and health care-seeking behavior among individuals with overactive bladder. Eur Urol. 2008;53(5):1029–37. doi: 10.1016/j.eururo.2008.01.027. [DOI] [PubMed] [Google Scholar]
- 16.Kinchen KS, Burgio K, Diokno AC, Fultz NH, Bump R, Obenchain R. Factors associated with women’s decisions to seek treatment for urinary incontinence. J Women’s Health (Larchmt) 2003;12(7):687–98. doi: 10.1089/154099903322404339. [DOI] [PubMed] [Google Scholar]
- 17.Hannestad YS, Rortveit G, Hunskaar S. Help-seeking and associated factors in female urinary incontinence. The Norwegian EPINCONT Study. Epidemiology of Incontinence in the County of Nord-Trøndelag. Scand J Prim Health Care. 2002;20(2):102–7. [PubMed] [Google Scholar]
- 18.Bogner HR. Urinary incontinence and psychological distress in community-dwelling older african americans and whites. J Am Geriatr Soc. 2004;52(11):1870–4. doi: 10.1111/j.1532-5415.2004.52509.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ragins AI, Shan J, Thom DH, Subak LL, Brown JS, Van Den Eeden SK. Effects of urinary incontinence, comorbidity and race on quality of life outcomes in women. J Urol. 2008;179(2):651–55. doi: 10.1016/j.juro.2007.09.074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kraus SR, Markland A, Chai TC, Stoddard A, FitzGerald MP, Leng W, et al. Race and ethnicity do not contribute to differences in preoperative urinary incontinence severity or symptom bother in women who undergo stress incontinence surgery. Am J Obstet Gynecol. 2007;197(1):92.e1–92.e6. doi: 10.1016/j.ajog.2007.03.072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kubik K, Blackwell L, Heit M. Does socioeconomic status explain racial differences in urinary incontinence knowledge? Am J Obstet Gynecol. 2004;191(1):188–93. doi: 10.1016/j.ajog.2004.03.084. [DOI] [PubMed] [Google Scholar]
- 22.Johnson TM, 2nd, Kincade JE, Bernard SL, Busby-Whitehead J, Hertz-Picciotto I, DeFriese GH. The association of urinary incontinence with poor self-rated health. J Am Geriatr Soc. 1998;46(6):693–9. doi: 10.1111/j.1532-5415.1998.tb03802.x. [DOI] [PubMed] [Google Scholar]
- 23.Dooley Y, Lowenstein L, Kenton K, Fitzgerald M, Brubaker L. Mixed incontinence is more bothersome than pure incontinence subtypes. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(10):1359–62. doi: 10.1007/s00192-008-0637-4. [DOI] [PubMed] [Google Scholar]
- 24.van der Vaart CH, de Leeuw JR, Roovers JP, Heintz AP. The effect of urinary incontinence and overactive bladder symptoms on quality of life in young women. BJU Int. 2002;90(6):544–9. doi: 10.1046/j.1464-410x.2002.02963.x. [DOI] [PubMed] [Google Scholar]
- 25.Waetjen LE, Liao S, Johnson WO, Sampselle CM, Sternfield B, Harlow SD, et al. Factors associated with prevalent and incident urinary incontinence in a cohort of midlife women: A longitudinal analysis of data: Study of women’s health across the nation. Am J Epidemiol. 2007;165(3):309–18. doi: 10.1093/aje/kwk018. [DOI] [PubMed] [Google Scholar]
- 26.Bump RC. Racial comparisons and contrasts in urinary incontinence and pelvic organ prolapse. Obstet Gynecol. 1993;81(3):421–5. [PubMed] [Google Scholar]
- 27.Duong TH, Korn AP. A comparison of urinary incontinence among african american, asian, hispanic, and white women. Am J Obstet Gynecol. 2001;184(6):1083–6. doi: 10.1067/mob.2001.115221. [DOI] [PubMed] [Google Scholar]
- 28.Coyne KS, Zhou Z, Thompson C, Versi E. The impact on health-related quality of life of stress, urge and mixed urinary incontinence. BJU Int. 2003;92(7):731–5. doi: 10.1046/j.1464-410x.2003.04463.x. [DOI] [PubMed] [Google Scholar]