

Abstract
Study Design
Observational cohort design.
Objective
To quantify the frequencies and magnitudes of neck motion during daily activities in healthy subjects.
Summary of Background Data
Previous studies have measured the maximum excursions during re-created ADLs in lab settings, but there is a lack of information available on frequencies and excursions of neck motion with ADLs in non-artificial settings.
Methods
Ten healthy young adults were fitted with a portable motion measurement device that recorded movement about each primary axis. Participants were instructed to wear the unit continuously over a 5-day period and record their daily activities with corresponding times. After the collection period, subjects' activity logs were analyzed and data were partitioned into five categories which provided the most primary representation of ADLs: athletics, work, travel, sleep, and miscellaneous. Each category was further divided into increasingly specific activities (e.g. running and walking). Frequency of motions within 5° increments was determined and an hourly rate was calculated for each activity. Median motion about each axis for each activity was also determined.
Results
The total number of movements per hour for all axes, regardless of amplitude, was highest during athletic activity and lowest during sleeping. The majority of movements (92% of athletic activity, 90% of work) required less than 25° of lateral bending, while greater range of movement requirements were observed for flexion-extension and axial rotation. The median range of motion along all axes was highest for athletic activity and lowest for sleeping.
Conclusions
The results of this study provide a baseline of the frequency and magnitude of neck motion during normal ADLs for the specified population. These findings can assist physicians and physical therapists in determining the extent of disability and identifying activities that will likely be problematic for patients with limited cervical motion.
Keywords: cervical spine, cervical range of motion, activities of daily living, continuous motion monitoring
Introduction
Limited cervical range of motion (CROM) as a result of various disorders can be a major obstacle to the satisfactory performance of activities of daily living (ADLs). A recent study by Cagnie et al. (2007) found reduced CROM in patients with chronic whiplash and idiopathic neck pain.1 Following cervical laminoplasty, CROM decreases,2 resulting in limited ADL performance3 similar to that following cervical fusion procedures.4 Patients suffering from cervical myelopathy have a significantly lower average CROM than healthy individuals5 and are often characterized by an inability to satisfactorily perform ADLs such as ascending stairs or walking with a normal gait pattern.2 To properly assess and treat such conditions, baseline measurements of neck range of motion during specific activities are required.
Previous studies have measured the maximum cervical excursions during re-created ADLs in lab settings, but there is a lack of information available on frequencies of motion with true ADLs performed over a period of days. Bennett et al.6 recorded the active CROM during each of 13 functional tasks; however, most tasks that required interaction with the environment, such as crossing the street and backing up a car, were simulated. Further, the equipment used to measure CROM was not conducive to use outside of a laboratory setting, and therefore motion of the cervical spine could only be characterized by active or end ROM.6
The ability to measure and define activities performed in an unrestricted environment, in a manner which does not result in a reactive effect to monitoring, is a unique prospect.7 Vast improvements have been made in the use of inclinometers,8 gyroscopes,9 and accelerometers10 to enable a portable, objective assessment of movement and physical activity. The system used in this study was constructed with the explicit purpose of measuring neck motion in vivo over extended periods of time.11 Defining the frequency and magnitude of CROM will aid in the assessment of movement avoidance in various patient populations, the design and implementation of artificial disks, the creation and utilization of therapeutic methods, and the assessment of outcomes from these interventions. Thus, the purpose of this study was to quantify the frequencies and magnitudes of neck motion during non-artificial daily activities in healthy subjects.
Methods
Subjects
Ten healthy young adults (6 males, 4 females; age, 22.1 ± 1.1 yrs; height, 177.7 ± 10.2 cm; and mass, 73.4 ± 13.9 kg) with no prior spine injury or pathology were recruited to participate in this study. Each subject gave informed consent according to a protocol approved by the University of Wisconsin Health Science Institutional Review Boards.
Procedure
To record neck motion over the 5-day period, subjects were fit with the Wisconsin Analysis of Spine Motion Performance (WASP) system, consisting of a portable data logger (MiniSun LLC, Fresno, CA) and two sensor arrays (Figure 1). Each array is comprised of two inclinometers that record angular displacements during flexion-extension (FE) and lateral bending (LB), with a gyroscope measuring angular velocities during axial rotation (AR) (Figure 1). Each sensor array weighs 2 g with the data logger weighing 59 g and measuring 7.0 × 5.4 × 1.7 cm in size. All data are recorded (8 Hz) with a timestamp to the data logger's on-board flash memory for later downloading to a personal computer for analysis. The accuracy of the WASP unit was validated against a materials testing system and optical motion capture system, which revealed it to be reliable and valid for flexion-extension and lateral bending movements of greater than 3°.11 While the initial validation indicated axial rotation to be reliable within 10°, correction of the analysis software has resulted in the detection of axial rotation to be consistent with the other two axes.12
Figure 1.

Subject wearing the WASP unit. Data sensors attached with medical adhesive to the mastoid process and the intersection of the 7th rib and the mid-axillary line on the left side of the body.
The sensor arrays were securely positioned on the mastoid process and the intersection of the 7th rib and the mid-axillary line on the left side of the body using a medical adhesive (Medical Spirit Gum 2100, Kryolan, Berlin, Germany), while the data logger was attached to the subject's beltline (Figure 1). The unit was calibrated prior to initial collection and prior to each new period of data collection to determine the three axes of motion with respect to current sensor position. Participants were instructed to wear the unit continuously throughout a 5 day period (at least one of which was a weekend day) but were told to remove the sensors and data logger before showering, swimming, participating in a contact sport, or performing any other activity which could have damaged the unit. Subjects were given standardized instructions to record their daily activities with corresponding start and end times in a provided journal. Once every 24 hour period, an investigator met with the subject to download data, recalibrate the unit for the start of the next collection period and address any questions. If the subject removed the unit or the sensors became loose in the middle of the 24 hour period, the subject was instructed to reattach the sensors as close as possible to their initial position.
Data Processing
Following the 5 day collection period, the data were imported into a commercial software package (Actview, MiniSun LLC, Fresno, CA) and visually examined. Regions of data when the sensors were detached while the data logger was still recording were removed. Neck motion along each primary axis was defined as the difference between the respective sensor axes located on the mastoid and thorax. Data from each axis were processed using custom algorithms (Matlab®, The Mathworks, Inc, Natick, MA) to identify motion peaks, defined as the point when the signal slope changes sign and the magnitude of the motion is above a threshold of 3°. This threshold was based on prior validation testing of the WASP system. 11
Subjects' activity logs were analyzed and data were partitioned into five primary categories based on the nature and distribution of activities reported: athletics, work, travel, sleep, and miscellaneous (Table 1). Each category was further divided into increasingly specific activities. The athletics category was composed of running, lifting weights, and light activity. The travel category was divided into periods of walking, biking, and driving. The miscellaneous category represented the majority of subjects' daily activities which were performed when not sleeping or working. Due to the variety of activities included in this category, each miscellaneous activity was further classified into one of three groups: high (shopping/errands), medium (cooking/eating) and low (watching television/relaxing) activity. A minimum of three subjects or five separate occurrences reported were required for a subcategory analysis. Some miscellaneous activities recorded were only performed by one or two subjects (playing cards/games) and thus were not analyzed as a subcategory but are still included in the larger miscellaneous category, resulting in the total hours of the subcategories not summing to the total hours of the primary categories.
Table 1.
Primary activity categories representing all day-to-day activity.
| Traveling | The subject is walking, biking, driving, or in some other way traveling to a location |
| Sleeping | The subject is asleep or laying down with the intent of falling asleep |
| Working / Class | The subject is at work or at class or is working on job or school work |
| Specified working out/athletics | The subject is participating in a sport or voluntarily exercising |
| Miscellaneous | The subject is doing/completing many various tasks or activities; includes cooking/eating, cleaning, using computer/video games/watching television, relaxing, reading, hanging out with friends, practicing hygiene upkeep, or performing many other common daily activities |
| Sensors Off | The IDEEA unit is still collecting data, but the subject is not currently wearing one or both of the sensors. Usually the subject is showering or participating in an activity that requires removal of the IDEEA unit; occasionally the sensors fall off and the subject does not immediately reattach them. |
Statistical Analysis
To characterize the frequency and magnitude of neck motion during each activity, motion magnitudes between consecutive peaks were calculated, with the frequency of motions within 5° increments determined. The number of movements per hour for each activity category was calculated by dividing the total number of peaks within each increment by the total time a subject performed the activity. The median magnitude of motion for each activity category was calculated. Activity log data were also divided based on the day of the week the unit was worn, with the average number of movements per hour calculated for each day. All calculations were repeated for each axis of motion.
Results
Compliance
One subject failed to turn in an activity log and as a result was excluded from all analyses. The amount of time the subjects actively wore the WASP system ranged from 69.5 to 117.5 hrs, while 5.0 to 39.0 hrs per subject were classified as “sensors off” (Figure 2). Approximately 3.6% of total recorded time was lost due to errors that occurred during data transfer from the data logger to the personal computer, incorrect placement of the sensors, or the data logger prematurely ending the recording.
Figure 2.
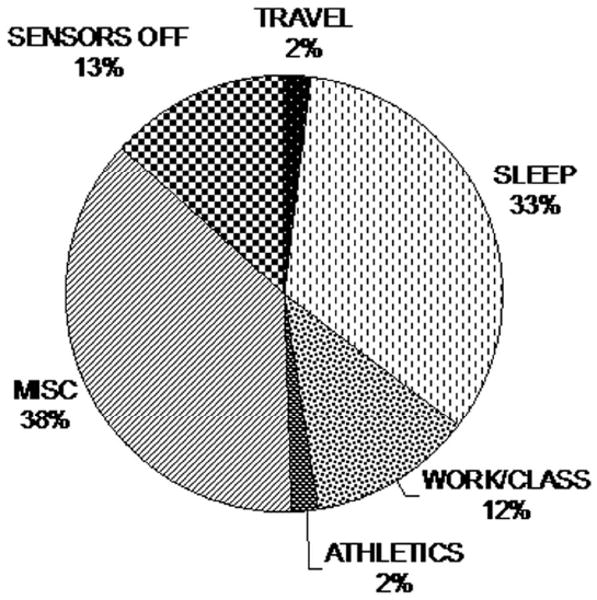
Combined total of recorded daily activities from all subjects, partitioned into primary activity categories. See Table 1 for categorical definitions. Data from subject 6 has been excluded due to incomplete activity log.
Frequency of Motion
The total number of movements per hour for all axes, regardless of amplitude, was highest during athletic activity and lowest during sleeping (Table 2). The total number of movements per hour during athletic activity was 2 to 3 times that of work, depending on the axis of motion. Similarly, the number of movements per hour during sleep was considerably less (5.7 to 7.9%) in comparison to work. The majority of these movements (92% of athletic activity, 90% of work) required less than 25° of LB, while greater range of movement requirements were observed for FE and AR (Figure 3). Only 4.3%, 1.1%, and 5.5% of FE, LB, and AR movements, respectively, exceeded 50°. Periods of running and walking produced an increased occurrence of motions beyond 25° on the FE axis. During running, only 42% of cycles were less than 25° compared to 68% for AR and 93% for LB. The average number of movements per hour across all subjects was highest on Mondays and Wednesdays and lowest on the weekends, along all axes (Table 3).
Table 2.
Mean (SD) number of movements per hour among all subjects for each of the five primary activity categories.
| FLEXION-EXTENSION | LATERAL BENDING | AXIAL ROTATION | |
|---|---|---|---|
| ATHLETICS | 8485.9 (7543.4) | 4623.6 (4742.6) | 3418.0 (2610.0) |
| Running | 14312.9 (8618.4) | 8563.9 (5367.4) | 5367.2 (3254.0) |
| Lifting Weights | 5056.8 (1559.3) | 2116.1 (454.5) | 2205.5 (536.4) |
| Light Intensity | 4032.0 (723.9) | 1847.5 (221.0) | 2009.8 (166.0) |
| TRAVEL | 6112.0 (5120.6) | 2339.9 (1852.8) | 2176.1 (1521.1) |
| Biking | 9134.9 (3245.9) | 2975.7 (1537.4) | 2650.7 (1105.7) |
| Driving | 3097.4 (2843.5) | 1397.8 (834.3) | 1408.0 (860.6) |
| Walking | 10405.8 (4379.0) | 4166.9 (2220.2) | 3734.4 (1770.2) |
| WORK | 3312.1 (1648.5) | 1516.1 (590.4) | 1642.9 (504.2) |
| MISCELLANEOUS | 3015.5 (2102.9) | 1334.7 (882.6) | 1422.3 (793.2) |
| High | 4139.6 (1925.2) | 1830.0 (966.5) | 1846.4 (758.8) |
| Shopping/Errands | 4201.9 (1150.0) | 1768.1 (628.2) | 1935.7 (579.4) |
| Getting Dressed/Ready | 4167.7 (1822.4) | 1849.5 (1179.3) | (1878.5 (894.2) |
| Out With Friends | 3993.4 (2454.1) | 1874.3 (844.5) | 1653.8 (595.9) |
| Medium | 2883.0 (1847.6) | 1308.4 (733.5) | 1424.5 (694.7) |
| Cooking/Eating | 3493.3 (1751.5) | 1625.3 (692.8) | 1736.8 (647.5) |
| Undefined | 2572.8 (1679.0) | 1174.5 (608.3) | 1299.4 (606.8) |
| Multi-Categorical | 3115.2 (1972.8) | 1374.5 (899.1) | 1476.3 (821.6) |
| Low | 1378.4 (1243.0) | 620.3 (506.1) | 711.5 (514.9) |
| Reading/Studying | 1582.6 (1667.2) | 503.8 (548.1) | 588.8 (576.1) |
| TV/Movie/Relaxing | 1307.7 (1056.6) | 660.7 (491.1) | 754.0 (494.1) |
| SLEEPING | 243.9 (208.3) | 87.1 (79.3) | 128.9 (83.0) |
Figure 3.

The average number of movements per hours of the cervical spine for a) flexion-extension, b) lateral bending and c) axial rotation. Less than 6% of the movements exceeded 50°. Error bars represent +1 SD.
Table 3.
Mean (SD) number of movements per hour among all subjects for each day of the week.
| FLEXION-EXTENSION | LATERAL BENDING | AXIAL ROTATION | |
|---|---|---|---|
| MONDAY | 2221.6 | 1021.5 | 1069.5 |
| TUESDAY | 2129.5 | 912.1 | 1060 |
| WEDNESDAY | 2305.8 | 1011.5 | 1097.5 |
| THURSDAY | 1784.9 | 803.5 | 879.7 |
| FRIDAY | 1968.1 | 846.8 | 914.3 |
| SAT & SUN | 1657.2 | 770.6 | 823.5 |
Median Motion
The median range of motion along all axes was highest for athletic activity and lowest for sleeping along the AR and FE axes (Table 4). While subjects were awake, the specific activity that produced the lowest median range of motion was driving, with 8, 9 and 10° of movement for LB, FE, and AR, respectively.
Table 4.
Median range of motion interval (degrees) among all subjects for primary and secondary activities.
| FLEXION / EXTENSION | LATERAL BENDING | AXIAL ROTATION | TOTAL HOURS OF DATA COLLECTION | TOTAL # OF SUBJECTS | |
|---|---|---|---|---|---|
| ATHLETICS | 18 | 12 | 16 | 19.4 | 8 |
| Running | 27 | 13 | 19 | 3.1 | 4 |
| Lifting Weights | 15 | 10 | 15 | 5.7 | 3 |
| Light Intensity | 14 | 11 | 13 | 5.3 | 3 |
| TRAVEL | 12 | 10 | 12 | 23.2 | 8 |
| Biking | 13 | 12 | 15 | 4.5 | 2 |
| Driving | 9 | 8 | 10 | 16.0 | 7 |
| Walking | 19 | 9 | 12 | 1.7 | 4 |
| WORK | 13 | 10 | 14 | 116.5 | 8 |
| MISCELLANEOUS | 13 | 10 | 13 | 358.8 | 9 |
| High | 14 | 10 | 13 | 92.7 | 9 |
| Shopping/Errands | 13 | 9 | 14 | 23.0 | 8 |
| Getting Dressed/Ready | 14 | 10 | 14 | 18.6 | 8 |
| Out With Friends | 16 | 10 | 12 | 31.3 | 5 |
| Medium | 13 | 10 | 13 | 195.3 | 9 |
| Cooking/Eating | 14 | 11 | 14 | 17.7 | 6 |
| Undefined | 13 | 10 | 12 | 107.5 | 8 |
| Multi-Categorical | 13 | 10 | 13 | 60.6 | 8 |
| Low | 10 | 10 | 11 | 70.8 | 9 |
| Reading/Studying | 10 | 9 | 10 | 17.7 | 4 |
| TV/Movie/Relaxing | 12 | 10 | 12 | 53.1 | 8 |
| SLEEPING | 9 | 10 | 8 | 320.3 | 9 |
Discussion
The results of this study show greater total cervical motion for higher intensity activities and less total cervical motion for lower intensity activities across all three axes. Each axis had the greatest amount of motion for athletic activity, followed by travel, work, miscellaneous, and sleeping. The majority of movements required less than 25° of motion, while a small percentage of movements (< 6%) were greater than 50°. The median range of motion interval was also higher for greater intensity activities and lower for less intense activities. Although athletic activity represented the highest median CROM and sleeping resulted in the lowest, the medium intensity activities such as work, travel, and most miscellaneous categories were quite similar in terms of median excursion.
Previous information available on CROM during daily activities was restricted to laboratory-based measurements during simulated activities. Our findings include a complete analysis of average neck motion over an extended period of time, both in frequency of movement and magnitude per excursion, throughout a wide range of ADLs. Although the standard clinical measure of CROM is maximum active range of motion, the fact that so few movements occur beyond 50° suggests that frequency and total motion may be useful information for the health care provider.
Recent studies have attempted to use neck motion magnitudes to characterize a variety of disorders involving neck pain. Dall'Alba et al. (2001) found that post-whiplash patients have significantly decreased ROM in all primary movements, while Johnston et al. (2008) showed that female office workers with neck pain have demonstrated reduced AR range.13, 14 Although reduced CROM is representative of these disorders, it is unclear if or how the reduced ROM is actually inhibiting the patient's daily activities. A more functional measurement could be to compare activity-related frequencies and total excursion to a set of age-matched healthy subjects.
When CROM is lost due to injury, age, or other conditions, it is typically characterized as a loss at end range of motion. For example, subaxial CROM due to aging decreases at a rate of roughly 5° every 10 years.15 Due to the fact that such a small percentage of motion occurs at magnitudes large enough to require full CROM, loss of end range of motion may not be the primary factor in reduced performance of ADLs. Thus, a more complete analysis of these patients in terms of total excursion and movement frequencies might provide a better characterization of disability.
An unexpected finding of this study was that periods of running and walking produced an increased occurrence of motions beyond 25° on the FE axis. Subsequent laboratory testing involving synchronous recording of cervical motion during running from the WASP system and an optical motion capture system revealed the WASP unit to consistently record a greater frequency and magnitude of motion specific to the FE axis. As this finding did not appear in any other activity or movement category, we are confident that it is the result of either excess motion of the rib sensor (through arm or skin movement), or a jarring effect of forceful foot-to-ground impacts (more pronounced with running). Thus, the FE motions reported during running should be interpreted with caution.
The average frequency of cervical motion between the days of the week (Table 4) indicates that the subject population was less active on the weekends than the weekdays. This may be due to the fact that the majority of the data collections (8 out of 10) were taken during the summer months of May through August, when most college-aged individuals are working or enjoying recreational activities, not sitting in class on the weekdays. Thus, the subject population and time of the year likely influenced the between-day differences in motion.10
The need to remove the sensors and data logger before participating in activities that could damage the unit (e.g. most contact sports, swimming) likely resulted in an under-representation of the amount of time spent being physically active, as these periods were categorized as “sensors off.” In general, it appears that both the athletics category and the travel category times were less than the amount of time the subjects actually spent performing these activities. The travel category was likely under-reported because subjects did not necessarily think of driving or walking to the store as traveling. Most subjects recorded longer excursions, but few recorded walks, bikes or drives of 15 minutes or less.
The use of activity logs have shown that subjects are able to produce an accurate record of daily activities when given proper instructions.16 A limitation of the current study was that subjects were not given very strict guidelines regarding the activity logs. The less accurate logs made it difficult to identify the corresponding WASP data, resulting in these data being either classified as undefined or multi-categorical, or being excluded from the analysis. Fortunately, only 3.6% of the total data were omitted in this way with most activity logs providing sufficient detail.
Quantifying CROM frequency and magnitude may enable researchers and clinicians to better characterize mechanisms of, and compensations to, injury. For example, the presence of neck pain in office workers has been related to prolonged posture and repetitive movements.17 The use of frequency data and continuous motion monitoring could aid researchers in exploring these relationships by identifying specific positions and volume of repetitive movements. In addition, individuals with visual or vestibular dysfunctions have been found to adopt compensatory head postures with limited neck motion.18 Continuous motion monitoring could be used to determine the extent of movement avoidance and compensatory strategies used by these individuals to complete ADLs.
Conclusion
The results of this study provide a baseline of the frequency and magnitude of neck motion during normal ADLs for healthy young adults. These findings can assist physicians and physical therapists in determining the extent of the disability and identifying activities that will likely be problematic for patients with limited cervical motion. Additional research should focus on exploring the associations between various disorders and CROM, and developing a more functional characterization of the disability.
Key Points.
The objective of this study was to quantify the frequencies and magnitudes of neck motion during inartificial daily activities in healthy subjects
Greater total cervical motion for higher intensity activities were observed across all three axes with less total cervical motion for lower intensity activities
The majority of movements (92% of athletic activity, 90% of work) required less than 25° of lateral bending, while greater range of movement requirements were observed for flexion-extension and axial rotation. Less than 6% of movements exceeded 50°
These data can be used to develop a more functional characterization of disability, explore the associations between disorders affecting cervical range of motion and limitation of ADLs, and determine appropriate movement goals
Acknowledgments
We gratefully acknowledge the contributions of Faiz I. Syed and Huayong Hu to the data analysis.
Sources of Support: This study was funded by a research grant from Medtronic.
References
- 1.Cagnie B, Cools A, De Loose V, et al. Reliability and normative database of the Zebris cervical range-of-motion system in healthy controls with preliminary validation in a group of patients with neck pain. J Manipulative Physiol Ther. 2007;30:450–5. doi: 10.1016/j.jmpt.2007.05.003. [DOI] [PubMed] [Google Scholar]
- 2.Kang SH, Rhim SC, Roh SW, et al. Postlaminoplasty cervical range of motion: early results. J Neurosurg Spine. 2007;6:386–90. doi: 10.3171/spi.2007.6.5.386. [DOI] [PubMed] [Google Scholar]
- 3.Takeuchi K, Yokoyama T, Ono A, et al. Limitations of activities of daily living accompanying reduced neck mobility after cervical laminoplasty. Arch Orthop Trauma Surg. 2007;127:475–80. doi: 10.1007/s00402-007-0372-1. [DOI] [PubMed] [Google Scholar]
- 4.Ratliff JK, Cooper PR. Cervical laminoplasty: a critical review. J Neurosurg. 2003;98:230–8. doi: 10.3171/spi.2003.98.3.0230. [DOI] [PubMed] [Google Scholar]
- 5.Holmes A, Wang C, Han ZH, et al. The range and nature of flexion-extension motion in the cervical spine. Spine. 1994;19:2505–10. doi: 10.1097/00007632-199411001-00003. [DOI] [PubMed] [Google Scholar]
- 6.Bennett SE, Schenk RJ, Simmons ED. Active range of motion utilized in the cervical spine to perform daily functional tasks. J Spinal Disord Tech. 2002;15:307–11. doi: 10.1097/00024720-200208000-00008. [DOI] [PubMed] [Google Scholar]
- 7.Behrens TK, Dinger MK. Motion sensor reactivity in physically active young adults. Res Q Exerc Sport. 2007;78:1–8. doi: 10.1080/02701367.2007.10762229. [DOI] [PubMed] [Google Scholar]
- 8.Lanningham-Foster LM, Jensen TB, McCrady SK, et al. Laboratory measurement of posture allocation and physical activity in children. Med Sci Sports Exerc. 2005;37:1800–5. doi: 10.1249/01.mss.0000175050.03506.bf. [DOI] [PubMed] [Google Scholar]
- 9.Mayagoitia RE, Nene AV, Veltink PH. Accelerometer and rate gyroscope measurement of kinematics: an inexpensive alternative to optical motion analysis systems. J Biomech. 2002;35:537–42. doi: 10.1016/s0021-9290(01)00231-7. [DOI] [PubMed] [Google Scholar]
- 10.Trost SG, McIver KL, Pate RR. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sports Exerc. 2005;37:S531–43. doi: 10.1249/01.mss.0000185657.86065.98. [DOI] [PubMed] [Google Scholar]
- 11.Syed FI, Oza AL, Vanderby R, et al. A method to measure cervical spine motion over extended periods of time. Spine. 2007;32:2092–8. doi: 10.1097/BRS.0b013e318145a93a. [DOI] [PubMed] [Google Scholar]
- 12.Sterling AC, Cobian DG, Anderson PC, et al. Annual Frequency and Magnitude of Neck Motion in Healthy Individuals. Spine. doi: 10.1097/BRS.0b013e31817e7019. in press. [DOI] [PubMed] [Google Scholar]
- 13.Dall'Alba PT, Sterling MM, Treleaven JM, et al. Cervical range of motion discriminates between asymptomatic persons and those with whiplash. Spine. 2001;26:2090–4. doi: 10.1097/00007632-200110010-00009. [DOI] [PubMed] [Google Scholar]
- 14.Johnston V, Jull G, Souvlis T, et al. Neck movement and muscle activity characteristics in female office workers with neck pain. Spine. 2008;33:555–63. doi: 10.1097/BRS.0b013e3181657d0d. [DOI] [PubMed] [Google Scholar]
- 15.Simpson AK, Biswas D, Emerson JW, et al. Quantifying the effects of age, gender, degeneration, and adjacent level degeneration on cervical spine range of motion using multivariate analyses. Spine. 2008;33:183–6. doi: 10.1097/BRS.0b013e31816044e8. [DOI] [PubMed] [Google Scholar]
- 16.Wickel EE, Welk GJ, Eisenmann JC. Concurrent validation of the Bouchard Diary with an accelerometry-based monitor. Med Sci Sports Exerc. 2006;38:373–9. doi: 10.1249/01.mss.0000183344.46077.bb. [DOI] [PubMed] [Google Scholar]
- 17.Cagnie B, Danneels L, Van Tiggelen D, et al. Individual and work related risk factors for neck pain among office workers: a cross sectional study. Eur Spine J. 2007;16:679–86. doi: 10.1007/s00586-006-0269-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Morris B, Smith V, Elphick J, et al. Compensatory head posture and neck problems: is there an association? A cohort study of nystagmus patients. Eye. 2008 doi: 10.1038/sj.eye.6703087. [DOI] [PubMed] [Google Scholar]