

SUMMARY
The study was designed to determine the contribution of standardized scored inspections implemented during the Athens 2004 Pre-Olympic and Olympic period, in assessing the presence of Legionella spp. in water sites. Inspection grading scores of 477 water supply systems, 127 cooling towers and 134 decorative fountains were associated with the corresponding microbiological test results of 2514 samples for Legionella spp. Nine violations of water supply systems and nine of cooling towers significantly associated with positive microbiological test results, and four violations of water supply systems and one of cooling towers were among those designated as ‘critical’ water safety hazards in the inspection reports. The study documents a strong correlation [water supply systems (RR 1·92), cooling towers (RR 1·94)] between unsatisfactory inspection scoring results and Legionella-positive microbiological test results (in excess of 10 000 c.f.u./l) and suggests the utility of inspection scoring systems in predicting Legionella proliferation of water systems and in preventing Legionnaires' disease.
INTRODUCTION
Legionnaires' disease (LD) is a serious pneumonia infection caused by inhaling the bacteria Legionella pneumophila or other Legionella spp. Water supply systems, cooling towers and decorative fountains have been linked to outbreaks of LD [1–8]. In recent years, the European Union has experienced several large outbreaks of LD [9–11]. In July 2001 the world's largest community outbreak of LD occurred in Spain [12]. In the United States, the estimated incidence of LD was 13 000 per year [13, 14]. It is estimated that <5% of cases may eventually be reported to public health authorities through passive surveillance [15]. Cases associated with travel are known to comprise up to 50% of national reports of the disease in some countries [16]. In addition, an annual rise in the number of cases, clusters and linked cases associated with a visit to a hotel or other tourist accommodation has been identified by the European surveillance scheme for Travel Associated Legionnaires' Disease [17]. This number has risen from <100 per year in 1987 to >600 in 2004 [18]. More than half of the cases are reported from European countries with warm climates with summer being the peak months for onset of Legionella infection [19].
LD prevention was identified as an objective for the Athens 2004 Organizing Committee of the Olympic and Paraolympic Games. Special regulations and procedures for the prevention of LD were enacted in previous Olympic Games [20]. To this end, standardized inspections and microbiological sample testing were conducted at water sites before and during the Athens 2004 Games.
More than 1500 hotels were used to accommodate athletes and tourists during the Games. About 3 500 000 spectators and 15 000 athletes consumed tap water from hotels or Olympic venues during the same period. A large number of people congregated in areas of the Olympic cities where water-cooling systems with cooling towers and evaporative condensers and decorative fountains were located. This exposure increased the potential for the spread of waterborne illnesses.
This study combines inspection scores of water supply systems (of hotels, and Olympic venues), cooling towers and decorative fountains with water microbiological test results (MTRs) from samples collected from the above sites. The study was designed to evaluate the scoring system implemented in the inspection programme for the Olympic Games and to determine the contribution of standardized scored inspections in the assessment of the presence of Legionella spp. in water systems.
METHODS
Environmental health inspection system
In 2001, the Hellenic Ministry of Health established the Olympic Planning Unit at the National School of Public Health, which was responsible for devising a plan for the Environmental Health Surveillance concerning a number of targets of Public Health importance including LD prevention. Water supply systems of hotels and Olympic venues, cooling towers and decorative fountains were registered, inspected and microbiologically tested, in Athens and the other four Olympic cities (Thessaloniki, Patra, Volos and Iraklio), from June 2002 to July 2004.
Standardized inspection reports
Environmental health inspections were performed using standardized reports, developed by the Olympic Planning Unit. The items included in the reports were based on requirements of national and European legislation, World Health Organization guidelines and the International Standardization Organization (ISO).
The inspection reports included ‘critical’ and ‘non-critical’ items. Critical items were violations ‘which are more likely to contribute to food or water contamination, illness, or environmental degradation and represent substantial public health hazards and [are] most likely associated with potential foodborne or waterborne disease transmission’ [21]. The water supply system standardized inspection report included 42 scored items, 11 of which were designated as ‘critical’. The items were classified into seven categories: construction – maintenance; cleaning – disinfection; cold-water distribution system; hot-water distribution system; system protection cross-connections – backflow; record keeping; and on-site manually conducted tests. The cooling tower standardized inspection report included 39 scored items, six of which were designated as ‘critical’. The inspection items were classified into six categories: construction; operation; cleaning – disinfection; personnel; record keeping; and on-site manually conducted tests. The decorative fountain standardized inspection report included 17 scored items concerning operation, cleaning – disinfection and on-site manually conducted tests, three of which were designated as ‘critical’. Data available for each standardized inspection report included: name of establishment, unique code, inspection identification code, county, date of inspection, overall score, specific violations cited, inspectors and time spent on inspection.
Scoring system and quantitative assessment
In each standardized inspection report, a standard number of scored items were included. The items were negatively scored from −1 to −3 points. Three negative points represented critical items. The non-critical items were scored either with −1 or −2 points according to their importance and severity of the violation. The final scoring of each item was decided after the pre-testing of the standardized inspection reports during the first test event in 2002. For the standardized inspection report of water supply systems, the total negative score was calculated and classified qualitatively in the following three categories (A) satisfactory result (0 to −7 points, <10% of the total negative score, no critical violation), (B) relatively satisfactory result (–8 to −14 points, 11–20% of the total negative score, or a critical violation), and (C) unsatisfactory result (more than −14 points, >20% of the total negative score). For the standardized inspection report of cooling towers the classification was as follows: (A) 0 to −6 points, (B) −7 to −11 points, and (C) more than −11 points. For the standardized inspection report of decorative fountains the classification was: (A) 0 to −2 points, (B) −3 to −5 points, and (C) more than −5 points. The classified categories were standardized and printed in each inspection report. During inspection, all negative points from deficiencies were identified, calculated and the overall negative score was assigned to one of the three categories described above. In this study, satisfactory grading results were considered as those assigned grade ‘A’, with grades ‘B’ and ‘C’ representing unsatisfactory grading results.
Sample collection
Water supply system
At least four water samples were drawn from the furthest outlet from the hot-water storage heater. The first sample was collected from hot water discharging from the shower head immediately after it was turned on and the second sample after 60 s flow time. The third sample was collected from cold water discharging from the shower head immediately after it was turned on and the fourth sample after 2 min flow time. When the water supply system comprised more than one ring, four water samples were drawn from the shower heads on each ring.
Cooling tower
One sample was collected from the water returning to the cooling tower in addition to a sample from the cooling tower pond, as far away from the fresh water inlet as possible.
Decorative fountain
One sample was collected from each decorative fountain pond. Samples were taken in sterile 0·5-l glass bottles and temperature, pH and free chlorine were measured. To neutralize residual free chlorine, sodium thiosulphate was added in sterile bottles for bacteriological analysis. Acid-preserved glass bottles were used for chemical determinations. Collection bottles were returned to the laboratory immediately after sampling for bacteriological and chemical–physical examination. Samples which were not examined within 24 h, were kept at refrigerator temperature as recommended by ISO 11731 [22].
Microbiological analysis methods
Water samples collected from water supply systems, cooling towers and decorative fountains were tested for Legionella spp. using methods in accordance with ISO 11731 and for aerobic count at 37°C for a minimum of 48 h incubation using the pour-plate method according to ISO 6222 [22, 23]. All tests were performed at the Legionella Reference Laboratory of the National School of Public Health.
To detect Legionella spp., 0·2-l water samples were concentrated by membrane filtration (0·45-μm pore-sized polyamide filter, Millipore, MA, USA; and white hydrophilic mixed cellulose ester membrane, Pall Life Sciences, Michigan, MI, USA). The filter membrane was resuspended in 10 ml Ringer's solution and vortex-mixed for 2 min. To reduce contamination by other microorganisms, 2 ml of this suspension was heat-treated (50°C for 30 min in a water bath). Two aliquots of 0·1 ml of the original and concentrated specimens (heat-treated and untreated, 1:10 diluted and undiluted) were each spread on duplicate plates of GVPC selective medium (bioMérieux, Marcy l'Etoile, France; Biolife, Milan, Italy). The plates were incubated at 37°C in a humidified environment for at least 10 days and read from day 4 with the aid of a plate microscope. Suspected colonies with a mottled surface or an iridescent and faceted cut-glass appearance were counted from each sampling. Three colonies of each kind of suspected colonies on a GVPC plate were subcultured on buffered charcoal yeast extract (BCYE) agar (with cysteine) (bioMérieux; Biolife) and nutrient agar (cysteine-free) media (LAB M, Bury, Lancashire, UK) for >2 days. Only colonies that failed to grow on nutrient agar but grew on BCYE were subsequently identified by an agglutination test (Legionella Latex test, Oxoid, Basingstoke, Hants). This test allows identification of L. pneumophila serogroup 1 and serogroups 2–14 and detection of seven Legionella spp. (other than L. pneumophila), which have been implicated in human disease: L. longbeachae, L. bozemanii 1 and 2, L. dumoffii, L. gormanii, L. jordanis, L. micdadei, L. anisa. The results were expressed as colony-forming units per litre (c.f.u./l), after counting the GVPC plate with the highest number of confirmed colonies and taking into account the sample dilution factor. The detection lower limit of the procedure was 500 c.f.u./l. Before and during the research period, the reference laboratory participated in an external quality-control scheme for Legionella detection in water (Quality Management Ltd, Bury, Lancashire, UK), through a periodic distribution of water samples seeded with unknown Legionella spp. and concentration. The total microbial counts at 37°C for 48 h were obtained twice by the pour-plate method on yeast extract agar (LAB M).
MTRs' quantitative assessment
The criteria used to interpret the results of the bacteriological examination of various sampling points were those used by the European Working Group for Legionella Infection (EWGLI). Test results were considered Legionella positive if the bacteria count was >10 000 c.f.u./l in at least one sample or >1000 but <10 000 c.f.u./l in more than two samples collected from water supply systems. The MTRs of samples collected from cooling towers or decorative fountains were considered Legionella positive if the bacteria count was >10 000 c.f.u./l in one sample, or the Legionella bacteria count was >1000 c.f.u./l but <10 000 c.f.u./l in at least one sample and the aerobic count was >100 000 c.f.u./ml [19].
Standardized inspections and samplings
From June 2002 to July 2004, 196 inspectors conducted registrations by using standardized data collection forms, inspections and samplings of 997 water supply systems of 887 hotels and 140 Olympic venues, 208 cooling towers, and 540 decorative fountains in all five Olympic cities. Analysis included samplings and the first inspections of water sites conducted the same day in the specific establishment. Inspections and samplings which were not conducted on the same day in the specific establishment were excluded from the analysis. Re-inspection scores and MTRs from water samples collected after taking corrective action were not included in the analysis.
Data analysis
Separate sets of three databases each were developed to record the establishments (registry database), the inspection standardized reports and results, and the MTRs. A unique code was used for each establishment to relate the inspection and MTR. Data were analysed with Epi-Info 2000 (CDC, Atlanta, GA, USA) and SPSS for Windows Release 11.0.1 software (SPSS Inc, Chicago, IL, USA) by correlation analysis, t test, one-way analysis of variance (ANOVA), and by χ2 test. Relative risk (RR) and 95% confidence interval (CI) were calculated to assess the risk of unsatisfactory standardized inspection scores of water sites to produce Legionella-positive test results. The receiver-operating-characteristic (ROC) curve was used to identify statistical cut-off points. Results were considered statistically significant when the P value was <0·05.
RESULTS
A total of 477 standardized inspections of water supply systems of hotels and Olympic venues, 127 cooling towers and 134 decorative fountains carried out together with water samplings (2514 water samples), fulfilled the criteria to be included in this study. Environmental health inspection scores and violations were correlated to the water MTRs of the water sites. The mean scores of water supply systems and cooling towers with positive MTRs were significantly higher than the mean scores of inspections with negative MTRs (Table 1). Moreover, the risk of a positive MTR was higher when unsatisfactory inspection grading results were recorded for water supply systems (RR 1·92, 95% CI 1·0–3·4, P<0·01; Table 2) and cooling towers (RR 1·94, 95% CI 0·7–5·2, P=0·1; Table 2). There was no significant association between unsatisfactory inspection grading results of decorative fountains and positive MTRs (Table 2).
Table 1.
Mean inspection scores in association with Legionella spp. microbiological test results
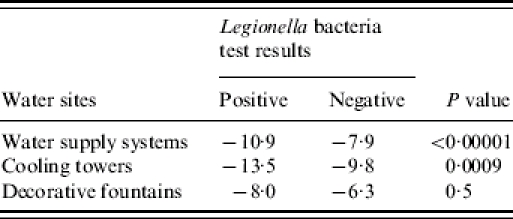
Table 2.
Association between inspection scores and positive microbiological test results for Legionella spp.
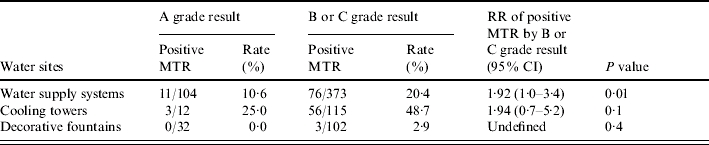
MTR, Microbiological test result; RR, relative risk; CI, confidence interval.
During inspections of water supply systems nine violations were significantly associated with positive MTRs (Table 3), four of these were designated as ‘critical’ water safety hazards in the standardized inspection report (Table 3). For the cooling towers, nine violations were significantly associated with a positive MTR and one was designated as ‘critical’ in the standardized inspection report (Table 4).
Table 3.
Violations associated with positive microbiological test results for Legionella spp. in water supply systems
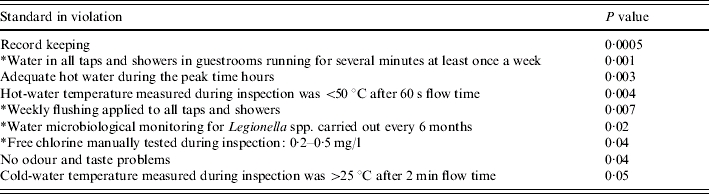
Designated as a critical item in the inspection report.
Table 4.
Violations associated with positive microbiological test results for Legionella spp. in cooling towers
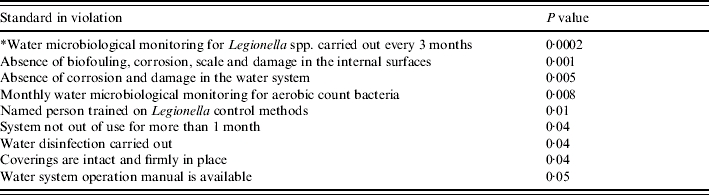
Designated as a critical item in the inspection report.
The area under the ROC curve derived from the association between environmental health inspection scores and water MTRs of water supply systems was estimated at 0·62 (95% CI 0·56–0·69; Fig. 1). The ROC curve identified −15·5 as the ideal negative score (cut-off point), with a sensitivity of 26·4% (95% CI 17·6–37·0) and a specificity of 91·8% (95% CI 88·6–94·3) for positive MTRs. The positive predictive value was 41·8% (95% CI 28·7–55·9) and the negative predictive value 84·8% (95% CI 81–88). Good correlation was also found with the negative scoring system and positive MTRs for cooling towers. For this analysis the area under the ROC curve was 0·67 (95% CI 0·58–0·77; Fig. 2). The ideal negative score was estimated at −19·5 with a sensitivity of 18·6% (95% CI 9·7–30·9) and a specificity of 89·7% (95% CI 79·9–95·8). The positive predictive value was 61·1% (95% CI 35·7–82·7) and negative predictive value was 56·0% (95% CI 46·1–65·5).
Fig. 1.

Receiver-operator-characteristic curve for inspection scores of water supply systems according to microbiological test results for Legionella spp. [area under the curve (AUC)=62%]. Diagonal segments are produced by ties.
Fig. 2.

Receiver-operator-characteristic curve for inspection scores of cooling towers according to microbiological test results for Legionella spp. [area under the curve (AUC)=67%]. Diagonal segments are produced by ties.
No cases of LD case were linked to the water sites inspected during the 2-year period before or during the Olympic period.
Discussion
The data presented here show that there was a clear correlation between unsatisfactory inspection grading results of water supply systems and cooling towers and positive MTRs for Legionella spp. In addition, unsatisfactory inspection scoring results appear to predict water contamination of Legionella spp. concentrations in excess of 104 c.f.u./l. Together this suggests that the standardized inspection reports and the scoring system were appropriately designed and fit for the intended purpose.
However, no link was established between unsatisfactory inspection scoring results of decorative fountains and positive MTRs. Although 76% of the total 134 decorative fountain inspections were unsatisfactory, only three (2·2%) were positive for Legionella spp. These failed samples were from fountains located inside the hotels. Further studies are necessary to examine factors such as sunlight that might influence the proliferation of Legionella in fountains located outside buildings.
The ROC analysis showed −15·5 as the cut-off point for an unsatisfactory score for water supply systems albeit with a relatively low sensitivity, but high specificity. It may be possible to increase sensitivity by separating the inspection report into two sections, one dealing with water safety and faecal contamination and the other specifically on Legionella contamination. The ROC cut-off point of −19·0 for cooling towers did not correspond with the unsatisfactory score (−11 points) in the inspection report of cooling towers. This suggests that some adjustment to the scoring system is warranted. To this end, specific items significantly associated with positive microbiology results should be scored as critical (−3 points) and the unsatisfactory score in the inspection report for cooling towers should be −19 points.
The results of this study suggest that combined analysis of environmental inspections and water microbiological quality data can be used to identify the most important causes of, and control measures for, water contamination [24]. Four of the nine violations significantly associated with a positive MTR of water supply systems were successfully scored as critical and so was one of the nine violations observed for cooling towers. We recommend that violations significantly associated with a positive MTR, but not considered as critical in the inspection reports, should be scored as critical items in subsequent revisions of the standardized inspection reports.
According to World Health Organization Guidelines, regulatory or other appropriate authorities may provide guidance on the development and application of Water Safety Plans for drinking-water systems of large buildings, cooling towers and evaporative condensers of air-conditioning devices [24]. Risk factors significantly associated with Legionella-positive results, could be considered as requirements for the Water Safety Plans.
Scheduled microbiological monitoring for legionellae remains controversial because the presence of the organisms is not necessarily evidence of the potential for causing disease [25]. The Centers for Disease Control and Prevention recommend aggressive disinfection measures for cleaning and maintaining devices known to transmit legionellae, but does not recommend regular scheduled microbiological assays for the bacteria [26]. EWGLI recommends monitoring for Legionella at a prescribed frequency according to the risk assessment findings. However, a negative microbiological result is no guarantee that Legionella bacteria are not present. Conversely, a positive result may not indicate a failure of controls, as Legionella are present in almost all natural water sources [19]. The increased laboratory cost and the long duration of Legionella detection are additional disadvantages. Thus, the development of a predictive system based on the application of standardized inspections, will warn that a hazardous situation is imminent and will enable timely and cost-effective correction of the situation by informing of the need for risk management decisions.
During an outbreak investigation, confirmation of the epidemiological hypothesis includes microbiological analysis of human and environmental samples and sanitary inspection. Even when it is possible to carry out testing of microbial quality the results are not instantly available. Moreover, recovery of pathogens from water is often unsuccessful, even when a water system is strongly associated with an outbreak [27]. The most common causes of failure to detect an implicated pathogen are the time between contamination and subsequent infection and the time that the outbreak is detected and the investigation commenced; or the common practice of implementing preventative super-disinfection [25]. Thus, the immediate assessment of contamination risk may be based on other indicators such as the results of standardized inspections which can allow control measures to be immediately instigated. In this study the fact that no cases of LD were linked to the water sites inspected during the study period does not necessarily imply that the inspection system was the only control measure that contributed to the prevention of the disease. Further research should directly evaluate the scoring system in relation to LD cases and outbreaks.
We have shown the utility of inspection scoring systems in predicting Legionella proliferation in water systems and in preventing LD and suggest that prevention planning and implementation strategies of policy-makers and regulators should include standardized scored inspections of water sites.
Acknowledgements
We extend thanks to all environmental health inspectors of Olympic cities, the Ministry of Health for the financial support and the staff of the National School of Public Health. We also thank Professor Athina Mavridou, Dr Vasili D. Daniilides, Mrs L. Georgiadou, and Mr George Panagako.
DECLARATION OF INTEREST
None.
References
- 1.Stout JE et al. Potable water as a cause of sporadic cases of community-acquired legionnaires' disease. New England Journal of Medicine. 1992;326:151–155. doi: 10.1056/NEJM199201163260302. [DOI] [PubMed] [Google Scholar]
- 2.Sabria M, Yu VL. Hospital-acquired legionellosis: solutions for a preventable infection. Lancet Infectious Diseases. 2002;2:368–373. doi: 10.1016/s1473-3099(02)00291-8. [DOI] [PubMed] [Google Scholar]
- 3.Anaissie EJ, Penzak-Scott R, Dignani MC. The hospital water supply as a source of nosocomial infections: a plea for action. Archives of Internal Medicine. 2002;162:1483–1492. doi: 10.1001/archinte.162.13.1483. [DOI] [PubMed] [Google Scholar]
- 4.Fisher-Hoch SP et al. Investigation and control of an outbreak of legionnaires' disease in a district general hospital. Lancet. 1981;1:932–936. doi: 10.1016/s0140-6736(81)91626-3. [DOI] [PubMed] [Google Scholar]
- 5.Stout JE et al. Ubiquitousness of Legionella pneumophila in the water supply of a hospital with endemic Legionnaires' disease. New England Journal of Medicine. 1982;306:466–468. doi: 10.1056/NEJM198202253060807. [DOI] [PubMed] [Google Scholar]
- 6.Bartlett CL, Bibby LF. Epidemic legionellosis in England and Wales 1979–1982. Zentralblatt für Bakteriologie, Mikrobiologie und Hygiene. 1983;255:64–70. [PubMed] [Google Scholar]
- 7.Garcia-Fulgueiras A et al. Legionnaires' disease outbreak in Murcia, Spain. Emerging Infectious Diseases. 2003;9:915–921. doi: 10.3201/eid0908.030337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hlady WG et al. Outbreak of Legionnaire's disease linked to a decorative fountain by molecular epidemiology. American Journal of Epidemiology. 1993;138:555–562. doi: 10.1093/oxfordjournals.aje.a116895. [DOI] [PubMed] [Google Scholar]
- 9.Den Boer JW et al. A large outbreak of legionnaires' disease at a flower show, the Netherlands, 1999. Emerging Infectious Disease. 2002;8:37–43. doi: 10.3201/eid0801.010176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Institut de Veille Sanitaire, Saint-Maurice, France. Outbreak of legionnaires' disease cases in northern France, November 2003 – January 2004: update, 14 January. http://www.eurosurveillance.org/ew/2004/040115.asp Eurosurveillance Weekly. 2004;8 [Google Scholar]
- 11.Joseph C. New outbreak of legionnaires' disease in the United Kingdom. British Medical Journal. 2002;325:347–348. doi: 10.1136/bmj.325.7360.347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Community outbreak of Legionnaires' disease in Murcia, Spain 2001. http://www.eurosurv.org/2001/010712.htm p. 010712.http://www.eurosurv.org/2001/010712.htm . Eurosurveillance Weekly .
- 13.Ford TE. Microbiological safety of drinking water: United States and global perspectives. Environmental Health Perspectives. 1999;107:191–206. doi: 10.1289/ehp.99107s1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Breiman RF, Butler JC. Legionnaires' disease: clinical, epidemiological, and public health perspectives. Seminars in Respiratory Infections. 1998;13:84–89. [PubMed] [Google Scholar]
- 15.Marston BJ et al. Incidence of community-acquired pneumonia requiring hospitalisation – results of a population-based active surveillance study in Ohio Archives in Internal Medicine. 1997;157:1709–1718. . The Community-Based Pneumonia Incidence Study Group. [PubMed] [Google Scholar]
- 16.Joseph CA et al. Legionnaires' disease in residents of England and Wales: 1998. Communicable Disease and Public Health. 1999;2:280–284. [PubMed] [Google Scholar]
- 17.Ricketts K, Joseph C. Travel associated legionnaires' disease in Europe: 2003. Eurosurveillance. 2004;9:5–6. doi: 10.2807/esm.09.10.00480-en. [DOI] [PubMed] [Google Scholar]
- 18.Ricketts K, McNaught B, Joseph CA. Travel associated legionnaires' disease in Europe 2004. Eurosurveillance. doi: 10.2807/esm.11.04.00617-en. (in press). [DOI] [PubMed] [Google Scholar]
- 19.European Surveillance Scheme for Travel Associated Legionnaires' Disease and European Working Group for Legionella Infections (EWGLI) . European Guidelines for control and prevention of travel associated Legionnaires' disease, January 2005.
- 20.Banwell K. Environmental health preparation for the Sydney 2000 Olympic and Paraolympic Games. New South Wales Public Health Bulletin. 2000;11:147–148. doi: 10.1071/nb00067. [DOI] [PubMed] [Google Scholar]
- 21.U.S. Department of Health and Human Services Washington: Public Health Service, Food and Drug Administration; 2001. . 2001 Food code. [Google Scholar]
- 22.ISO 1998 1998. . ISO 11731. Water Quality – detection and enumeration of Legionella. Part 1,
- 23.ISO 1999 1999. . ISO 6222. Water Quality – Enumeration of culturable micro-organisms – colony count by inoculation in a nutrient agar culture medium,
- 24.WHO 3rd edn Vol. 1 Geneva: World Health Organization; 2004. . Guidelines for drinking water quality, , vol. . Recommendations. [Google Scholar]
- 25.Joly JR, Barbaree JM, Breiman RF, Dufour AP. Legionella: current status and emerging perspectives. Washington DC: American Society for Microbiology Press; 1993. Monitoring for the presence of Legionella: where, when, and how; pp. 211–216. : pp. [Google Scholar]
- 26.Hoge CW, Breiman RF. Advances in the epidemiology and control of Legionella infections. Epidemiology Reviews. 1991;13:329–340. doi: 10.1093/oxfordjournals.epirev.a036076. [DOI] [PubMed] [Google Scholar]
- 27.WHO and the Organisation for Economic Co-operation. Assessing Microbial Safety of Drinking Water. Improving Approaches and Methods. London: World Health Organization and the Organisation for Economic Co-operation; 2003. [Google Scholar]