

SUMMARY
We estimated the number of deaths in France for the year 2000 in HIV-infected adults using three sources. The sources were (1) the ‘Mortalité 2000’ survey (M2000): 964 deaths were documented by 185 hospital wards involved in HIV management; (2) 1288 death certificates with a mention of HIV infection (INSERM-CepiDc) and (3) the French hospital database on HIV infection (FHDH) identified 654 deaths. The capture–recapture method was used with log-linear modelling. Overall 1559 deaths were observed. Estimation of the number of deaths in France was 1699 (95% CI 1671–1727). The completeness of M2000, CepiDc and FHDH were 55%, 76% and 38% respectively. Diversification of diseases and of causes of death in HIV-infected adults may explain: (1) the diversification of physicians involved in their management and incomplete coverage of M2000 and FHDH, and (2) why HIV infection was not mentioned in all death certificates.
INTRODUCTION
Causes of death have changed in HIV-infected adults since the dramatic decline in AIDS-related mortality due to highly active antiretroviral therapy (HAART) [1, 2]. Since mortality remains higher in HIV-infected persons than in the general population [3, 4], a description of the distribution of causes of death may provide a means of identifying priorities in the management of HIV infection and associated comorbidities. Several sources are available in France for identifying deaths in HIV-infected persons. First, surveillance systems on HIV and AIDS record deaths after occurrence of AIDS. None of the other following sources alone allow for a valid estimation of the number of deaths in HIV-infected persons. Identification through death certificates involves a selection of certificates which mention HIV infection. Due to the increasing diversification of the causes of death, this source may omit non-HIV-related deaths. Cohort studies do not include the whole HIV-infected population, and do not currently use standardized determination of the causes of death. Finally, a specific survey, called ‘Mortalité 2000’, was planned in France in 2000 to describe the distribution of the causes of death in HIV-infected adults [5]. The participating physicians were those identified as currently involved in the management of HIV infection.
Using the capture–recapture method, the number of cases can be estimated according to several sources when complete census is not available and when random sampling is not easily applicable [6–8]. This method is based on cross-match between several databases in order to identify common cases. The availability of at least three sources makes it possible to verify hypotheses of the capture–recapture method.
The objective of this analysis was to estimate the number of deaths in France in 2000 in HIV-infected adults according to three sources representing different modes of collection of deaths in HIV-infected adults: the national death certificates database (CepiDc), the French hospital database on HIV infection (FHDH), a cohort of HIV-infected patients followed in hospitals, and the ‘Mortalité 2000’ survey (M2000). The completeness of each source was assessed.
METHODS
Data sources
Three sources of data were used, all approved by the French commission on informatics and liberties. First, the M2000 aimed at describing the distribution of the underlying cause of death in HIV-infected adults based on a standardized questionnaire [5]. All hospital wards known to be involved in the management of HIV infection in France were contacted. Physicians who agreed to participate were asked to report all deaths in HIV-infected adults (⩾18 years) quarterly in 2000.
Second, death certificates for adults in 2000 with any mention of HIV infection were selected by the Epidemiological Center for Medical Causes of Death (INSERM-CepiDc).
Third, deaths of adults in 2000 were identified in FHDH, a cohort concerning HIV-infected patients followed in 29 HIV Information and Care Centers (CISIH) [9].
Cross-matches
The three databases were matched 2×2 using the following variables: gender, date of birth and date of death for M2000 and CepiDc; gender, month and year of birth, date of death and transmission group for M2000 and FHDH; and gender, month and year of birth and date of death for CepiDc and FHDH. A first step retained exact cross-matches. Further steps accepted one or two differences after checking place of birth and place of death, when available. For these cross-matches accepting differences among matching variables, the causes of death had to be informative (other than unknown or an immediate cause of death) and belong to the same category of the International Classification of Diseases – 10th revision (ICD-10).
Capture–recapture method
The capture–recapture method was used to estimate the total number of cases according to the three sources of data. It is based on the following hypotheses [6, 7, 10]: cases must be true cases with common definition between sources; the population must be closed and the period and geographical areas must be the same between sources; the matching between sources must be accurate; the probability for each case to be identified must be the same within one source (homogeneity of capture); and identification by one source does not have to depend on identification by another (independence). Possible heterogeneity and dependence can be tested and taken into account using a log-linear model when more than two sources are available.
First, estimates of the total number of deaths were calculated for each pair of sources using unbiased formulae of Chapman [11] and Seber [12]. Dependence between sources comparing pairwise estimates can thus be detected [13], a lower estimate as compared to the others leading to suspected dependence between the sources of the concerned pair.
Second, the total number of deaths was estimated by log-linear modelling including all 2×2 interactions between the three sources, in order to take into account dependence between sources or heterogeneity of capture [6]. Statistical Analysis System software 8.2 proc genmod was used (SAS Institute, Cary, NC, USA). A first step identified potential interaction between sources (dependence) and a second step stratified the analysis by gender and age in order to identify possible heterogeneity of capture. Age was considered in two classes: above or below 50 years. The choice of the final model was based on the Akaike Information Criterion [AIC=G2−2(d.f.)] and on the Bayesian Information Criterion [BIC=G2−(log Nobs/2π)(d.f.)] where G2 is the deviance, d.f. the number of degrees of freedom and Nobs the number of observed cases [7]. The 95% confidence intervals (95% CI) were based on variance.
Deaths from Metropolitan France (excluding oversea areas) were stratified according to the place of death in two groups: Paris region (Ile-de-France) and other regions. The completeness of a source was defined as the number of deaths identified by this source divided by estimate of the total number of deaths.
In the death certificates' source, the underlying cause of death was determined by CepiDc according to ICD-10 rules [14]. In M2000, the underlying cause of death was determined using a coding adapted from the ICD-10 rules for specific concerns in HIV infection [5]. The underlying cause of death was not available in the FHDH source. The distribution of the underlying cause of death was described from the point of view of both M2000 and CepiDc, according to identification by other sources. Characteristics of patients were described according to the source and compared using χ2 and Kruskal–Wallis tests.
RESULTS
Cross-matches
In 2000, 964 deaths were identified in HIV-infected adults in M2000, 1288 in CepiDc and 654 in FHDH. Pairwise matching retained 538, 451 and 276 exact cross-matches and accepted 717, 571 and 486 cross-matches between M2000–CepiDc, M2000–FHDH and CepiDc–FHDH respectively. Overall, 427 cases were common to all three sources and 1559 cases were identified by one source at least (Fig.).
Fig.

Number of deaths of HIV-infected adults in France in 2000, cross-matches between three sources of data: Mortalité 2000 survey (M2000), death certificates (CepiDc) and French Hospital Database on HIV infection (FHDH).
Capture–recapture estimates
According to the two-source capture–recapture analysis, the estimate of the total number of deaths for the M2000–FHDH pair was about 1·6 times smaller (1104, 95% CI 1083–1125) than for the M2000–CepiDc (1731, 95% CI 1689–1774) and the CepiDc–FHDH (1733, 95% CI 1671–1794) pairs, leading us to suspect dependence between the two sources: M2000 and FHDH.
Log-linear modelling using the three sources selected the model with an estimate of the number of deaths given by the three sources and an interaction M2000*FHDH, confirming the dependence between M2000 and FHDH. Among the four models with the lowest values of both AIC and BIC, this model had the lowest number of parameters. At this step estimation of the number of deaths was 1738 (95% CI 1711–1770).
Overall 1534 (98%) observations among the 1559 identified by at least one source had gender and age documented. Heterogeneity of capture was identified according to gender and age (Table 1, model 4). Finally the estimated number of deaths in France was 1699 (95% CI 1671–1727). The completeness of M2000, CepiDc and FHDH was, therefore, 55% (95% CI 54–56), 76% (95% CI 74–77) and 38% (95% CI 37–39) respectively (Table 2).
Table 1.
Log-linear models and estimates of the number of deaths in HIV-infected adults in France in 2000, stratified by gender (SEXE) and age (AGE50) and in Metropolitan France (excluding overseas areas) stratified by gender, age and region of death (REG2)
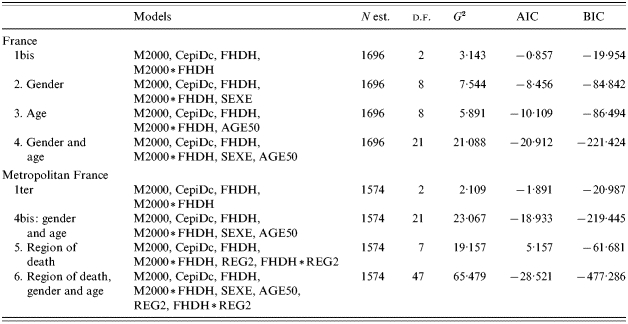
M2000, Mortalité 2000 survey; FHDH, French Hospital Database on HIV infection; CepiDc, Centre d'Epidémiologie sur les Causes de décès [Epidemiological Centre for Medical Causes of Death]; d.f., degrees of freedom; G2, deviance; AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion.
Table 2.
Estimates of the number of deaths in HIV-infected adults in France in 2000 according to age and gender, and completeness of the three sources of data
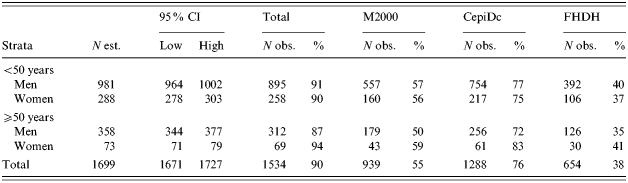
M2000, Mortalité 2000 survey; FHDH, French Hospital Database on HIV infection; CepiDc, Centre d'Epidémiologie sur les Causes de décès [Epidemiological Centre for Medical Causes of Death]; 95% CI, variance-based 95% confidence interval.
Considering deaths that occurred in Metropolitan France (excluding oversea areas), 1433 cases with documented gender and age were recorded. Heterogeneity of capture was identified according to the region of death, and an interaction was identified between FHDH and the region. The final model took into account heterogeneity of capture according to gender, age and region of death (Table 1, model 6). In Metropolitan France, the estimated number of deaths was 1574 (95% CI 1548–1599) and the completeness of M2000, CepiDc and FHDH was 54% (95% CI 53–55), 78% (95% CI 77–80) and 36% (95% CI 35–36) respectively (Table 3). In FHDH, the completeness was higher in men aged <50 years who had died in the Paris region, and in M2000 the completeness was lower in men and women aged >50 years who had died in the Paris region (Table 3).
Table 3.
Estimates of the number of deaths in HIV-infected adults in Metropolitan France (excluding overseas areas) in 2000 according to region of death, age and gender, and completeness of the three sources of data
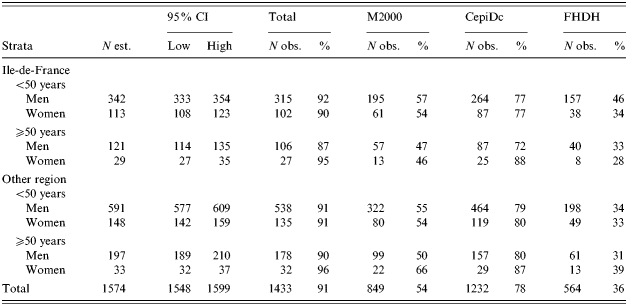
Ile-de-France, Paris region; M2000, Mortalité 2000 survey; FHDH, French Hospital Database on HIV infection; CepiDc, Centre d'Epidémiologie sur les Causes de décès [Epidemiological Centre for Medical Causes of Death]; 95% CI, variance-based 95% confidence interval.
Characteristics of patients according to the source
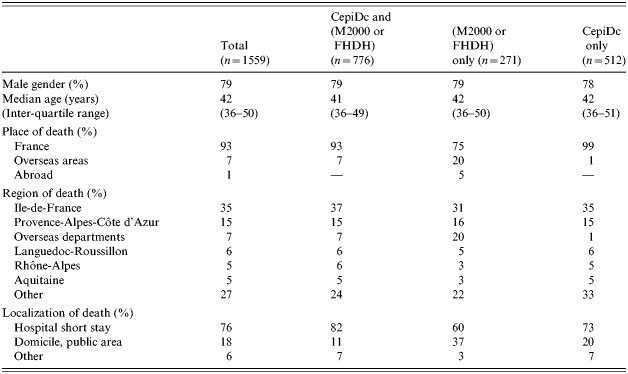
Because of the dependence between FHDH and M2000, the comparisons of patient characteristics were carried out according to the following grouping: (1) common cases to CepiDc and (M2000 or FHDH), (2) (M2000 or FHDH) without CepiDc, (3) CepiDc only (Table 4). Age and gender did not differ according to the sources. Cases identified by M2000 or FHDH had died more frequently in overseas areas or abroad and more frequently at home (37%) compared to those identified by CepiDc only (20%) and by both sources (11%).
Table 4.
Characteristics of HIV-infected persons dying in France in 2000 according to the source ofidentification
In a sample of 215 death certificates among the 570 not identified by M2000, the speciality of the certifying physician was unknown for 26%. Among the 160 cases for whom it was documented, 86% did not belong to the specialities that were contacted for participation in M2000, i.e. infectious diseases and internal medicine.
Causes of death according to the source
From the M2000 source, the underlying cause of death was AIDS-related in 55, 50, 35 and 25% of cases identified by (1) three sources, (2) M2000 and CepiDc, (3) M2000 and FHDH and (4) M2000 only. From the CepiDc source, the underlying cause of death was HIV-related in 87, 81, 93 and 78% and AIDS-related in 44, 39, 39 and 31% of cases identified by (1) three sources, (2) CepiDc and M2000, (3) CepiDc and FHDH and (4) CepiDc only. Overall AIDS-related deaths were less frequent among cases identified by only one source.
DISCUSSION
Using log-linear modelling and three sources, we estimated the number of deaths in HIV-infected adults in 2000 in France as 1699 (95% CI 1671–1727). Considering only Metropolitan France, the estimation was 1574 (95% CI 1548–1599). Overall, the completeness was 55% (95% CI 54–56) for M2000, 76% (95% CI 74–77) for Cepi-DC and 38% (95% CI 37–39) for FHDH.
We acknowledge several limitations to our analysis when considering the hypotheses of the capture–recapture method [6, 7, 10]. The definition of case is in our opinion straightforward, because we sought to identify deaths from all causes and because diagnosis of HIV infection in France is based on Western blot testing.
Closed population
The population cannot be considered as closed since some HIV-infected persons may have migrated between France and other countries. Nevertheless, as in most epidemiological studies, we considered that the size of the population of HIV-infected adults was constant within the period of study [8].
Accuracy of matching
Because no complete identifier was available for patients, cross-match was performed according to a set of characteristics and accepted some differences. For that reason we can assume that there are both false-positive matches and false-negative matches. Concerning matches that accept potential differences in dates, verification of other available variables made them acceptable. When these verifications could not be made, the correspondence between the two records was not accepted. For this reason we assume that the most likely are false-negative matches resulting in an underestimation of the number of cross-matches, overestimating the total number of deaths and underestimating the completeness.
Independence between sources
We identified dependence between M2000 and FHDH. Indeed, most of the physicians who participated in M2000 were involved in the management of HIV infection in hospital wards participating in FHDH. This dependence has been taken into account in the log-linear model. On the contrary, we did not identify dependence between mention of HIV infection on the death certificate and participation in both M2000 and FHDH.
Homogeneity of capture
We identified heterogeneity of capture according to age, gender and region of death. In M2000 and FHDH, lower completeness in persons >50 years may indicate that older patients are followed by various physicians, not only those specializing in the management of HIV infection. This especially seems to occur in the Paris region.
Completeness
Overall 45% of the estimated number of deaths has not been identified by M2000. According to analysis of a sample of death certificates, the majority of certificates concerning these non-identified cases were filled in by physicians not identified by the M2000 protocol as being currently involved in the management of HIV infection. The diversification of diseases in HIV-infected adults has widened the number of physicians and specialities involved in their management. In a future survey, one might extend the speciality of participants in order to increase the number of identified cases. Nevertheless, this choice can result in greater difficulties in obtaining exhaustive participation and standardized collection of data.
Although death certificates collect information on all deaths in France, the identification of HIV-infected people was not complete. The implementation of electronic certification may resolve this problem in the future, allowing more precise data on HIV infection to be collected from certification during a specific period.
The completeness of FHDH was lower than for M2000, as was expected by the participating hospital wards. This is lower than the completeness of FHDH for AIDS cases that was estimated at 48% for 1990–1993 [9]. This may be explained by either a lower completeness of death notification in FHDH in the HAART period compared to the pre-HAART period because of a diversification of involved physicians, or by a lower notification of deaths in FHDH compared to AIDS cases. This will be explored by matching lost-to-follow-up patients in FHDH and deaths in the two other sources. Lack of correct determination of the underlying cause of death means that the distribution of the causes in this database cannot be described. Further standardization of data collection on deaths to be implemented will make it possible to evaluate the role of this database in the surveillance of the causes of death in HIV-infected adults in France.
Cause of death according to the source
From the CepiDc source, the ICD-10 rules led to classification of the underlying cause of death as HIV-related in a majority of cases when HIV infection was mentioned in the certificate. For this reason the comparison of distribution of the causes of death in cases identified only by the death certificate and in cases identified by both the death certificate and another source does not lead to straightforward conclusions. Proportions of cases related to HIV/AIDS are quite similar in these groups and the proportion of AIDS-related deaths is lower in cases identified only by the death certificate. One reason may be that AIDS is most frequent in cases followed by physicians specializing in HIV infection, or that the AIDS diagnosis is stated more frequently, and that in cases followed elsewhere, HIV infection is involved but the diagnosis is less precise.
From the M2000 source, the proportion of AIDS-related deaths was lower in cases not identified by a death certificate, and this corresponds to cases in which the mention of HIV infection was not recorded on the death certificate.
These differences in the distribution of the causes of death may suggest heterogeneity of capture according to the cause of death. Nevertheless, differences in the coding of the cause of death between sources and unavailability of the underlying cause of death in one source did not allow us to stratify our analysis according to this information.
Characteristics according to the source
We did not stratify the analysis according to the place of death defined as hospital, home or public area because of lack of this information in one source. However, people who died at home were less likely to be identified by both M2000 and CepiDc, and were more likely to be identified either by M2000, or by CepiDc. Different interpretations of this phenomenon may be possible: (1) cases deceased at home may have been more frequently reported by a physician not specializing in HIV infection, and have been identified by death certificate alone; (2) cases identified only by M2000 died more frequently of non-AIDS defining causes, and more frequently at home; (3) documentation of deaths occurring at home may have been less complete in M2000 making cross-matching impossible.
Specific interest of each source
In order to identify deaths occurring in HIV-infected adults in the HAART period, death certificates had the best completeness but they underestimated non-HIV-related deaths. Hospital databases may be representative of deaths occurring among patients currently followed in hospital. The completeness of M2000 was between the two other sources. Specific surveys like M2000 can reach high level of standardization of data collection and they can be adapted to specific concerns related to the pathology studied, like HIV infection in the HAART period.
CONCLUSION
Using a capture–recapture method, we estimated that a total of 1699 deaths occurred in France in 2000 among HIV-infected adults, leading to an 1·9% annual mortality rate (95% CI 1·0–3·3) according to estimation of prevalence of HIV infection in France at the end of 2000 [15]. None of the three sources studied is complete and the interest of a source in identifying deaths in HIV-infected persons will depend on research objectives. Regular estimations of the number of deaths in HIV-infected persons according to several sources are needed since treatment strategies are changing and pathologies are diversifying in this population. This will contribute to an evaluation both of the completeness of surveillance systems that may change and of the completeness of specific surveys like the M2000.
ACKNOWLEDGEMENTS
Thanks are due to the following groups: The Epidemiological Center for Medical Causes of Death (INSERM-CepiDc), The Mortalité 2000 Study Group, and the Clinical Epidemiology Group of the FHDH. Members of the groups are listed at: http://www.isped.u-bordeaux2.fr/FIXED/M2K/capture_death_estimation_acknowledgement.pdf
DECLARATION OF INTEREST
None.
REFERENCES
- 1.CASCADE Collaboration. Survival after introduction of HAART in people with known duration of HIV-1 infection. Lancet. 2000;355:1158–1159. [PubMed] [Google Scholar]
- 2.Mocroft A et al. Changes in the cause of death among HIV positive subjects across Europe: results from the EuroSIDA study. AIDS. 2002;16:1663–1671. doi: 10.1097/00002030-200208160-00012. [DOI] [PubMed] [Google Scholar]
- 3.Keiser O et al. All cause mortality in the Swiss HIV cohort study from 1990 to 2001 in comparison with the Swiss population. AIDS. 2004;18:1835–1843. doi: 10.1097/00002030-200409030-00013. [DOI] [PubMed] [Google Scholar]
- 4.Lewden C et al. The APROCO Study Group. Mortality in a cohort of HIV-infected adults started on a protease inhibitor-containing therapy – standardization to the general population. Journal of Acquired Immune Deficiency Syndrome. 2001;26:480–482. doi: 10.1097/00126334-200104150-00013. [DOI] [PubMed] [Google Scholar]
- 5.Lewden C et al. Causes of death among HIV-infected adults in the era of potent antiretroviral therapy: emerging role of hepatitis and cancers, persistent role of AIDS. International Journal of Epidemiology. 2005;34:121–130. doi: 10.1093/ije/dyh307. [DOI] [PubMed] [Google Scholar]
- 6.International Working Group for Disease Monitoring and Forecasting. Capture–recapture and multiple-record systems estimation I: history and theoretical development. International Working Group for Disease Monitoring and Forecasting. American Journal of Epidemiology. 1995;142:1047–1058. [PubMed] [Google Scholar]
- 7.Hook EB, Regal RR. Capture–recapture methods in epidemiology: methods and limitations. Epidemiological Review. 1995;17:243–264. doi: 10.1093/oxfordjournals.epirev.a036192. [DOI] [PubMed] [Google Scholar]
- 8.Chao A et al. The applications of capture–recapture models to epidemiological data. Statistics in Medicine. 2001;20:3123–3157. doi: 10.1002/sim.996. [DOI] [PubMed] [Google Scholar]
- 9.Bernillon P et al. Record-linkage between two anonymous databases for a capture–recapture estimation of underreporting of AIDS cases: France 1990–1993. The Clinical Epidemiology Group from Centres d'Information et de Soins de l'Immunodeficience Humaine. International Journal of Epidemiology. 2000;29:168–174. doi: 10.1093/ije/29.1.168. [DOI] [PubMed] [Google Scholar]
- 10.Hook EB, Regal RR. Recommendations for presentation and evaluation of capture–recapture estimates in epidemiology. Journal of Clinical Epidemiology. 1999;52:917–926. doi: 10.1016/s0895-4356(99)00060-8. [DOI] [PubMed] [Google Scholar]
- 11.Chapman D. Some properties of the hypergeometric distribution with application to he zoological sample censuses. University of California Public Statistics. 1951;1:1060–1067. [Google Scholar]
- 12.Seber G. The effect of trap response on tag recapture estimates. Biometrics. 1970;26:12–22. [Google Scholar]
- 13.Wittes JT, Colton T, Sidel VW. Capture–recapture methods for assessing the completeness of case ascertainment when using multiple information sources. Journal of Chronic Diseases. 1974;27:25–36. doi: 10.1016/0021-9681(74)90005-8. [DOI] [PubMed] [Google Scholar]
- 14.WHO. International Classification of Diseases (Tenth Revision) Geneva: World Health Organization; 1993. [Google Scholar]
- 15.Desenclos J et al. Prevalence of HIV seropositivity in France [in French] Bulletin Epidémiologique Hebdomaire. 2005;11:41–44. [Google Scholar]