

Abstract
Kawaski disease (KD) is an acute, self-limited vasculitis that typically occurs in young children and was first described by Japanese pediatrician Tomisaku Kawasaki in 1967. Although originally thought to be a rare condition, KD has become the most common cause of acquired heart disease in the pediatric age group in developed countries. The majority of patients with KD appear to have a benign prognosis but a subset of patients with coronary artery aneurysms are at risk for ischemic events and require lifelong treatment. In the four decades that have passed since the initial recognition of KD, the number of patients reaching adulthood has continued to grow. Adult cardiologists will be increasingly involved in the management these patients. Currently, there are no established guidelines for the evaluation and treatment of adult patients who have had KD. We review here the current literature that may be helpful to clinicians who care for adults who suffered from KD in childhood.
Keywords: aneurysm, vasculitis, myocardial infarction, myocardial flow reserve, myocarditis
Introduction
Kawasaki disease (KD) is the leading cause of acquired heart disease in children in the developed world(1), Typically, KD presents in children under the age of five years as a febrile illness with mucocutaneous changes(2). A subset of patients will develop permanent damage to the arterial wall, valve leaflets, and myocardium. The acute phase of the illness is self -limited and the diagnosis may be missed. If untreated, KD can result in coronary aneurysms in 25% of patients(3). Patients who suffer coronary artery damage may develop thrombosis or stenotic lesions associated with the aneurysms and are at risk of myocardial infarction, sudden death, and congestive heart failure(4,5) The prognosis for adults who recovered from KD without coronary aneurysms is postulated to be good, but longitudinal studies have not been performed to test this hypothesis.
In 2004, the American Heart Association issued updated guidelines for the care and management of children with KD(6). However, studies of the optimal therapy and management of the sequelae of KD in adults have not been performed. Nor have official guidelines been developed that provide direction for cardiologists as they begin to care for the growing number of young adults who suffered KD in childhood. The available data suggest that the pathophysiology of the vascular lesion in KD is unique and distinct from atherosclerosis. The following is a critical review of the literature describing the cardiovascular manifestations in young adults who suffered from KD in childhood.
Epidemiology and clinical aspects of acute KD
It is estimated that over 4,000 new cases of KD are diagnosed in the U.S. each year(7). In Japan, where the incidence is approximately 10-fold higher as compared to the U.S., more than 10,000 new cases are diagnosed each year(8). Seasonality of cases, nationwide epidemics, and the self-limited nature of the acute illness suggest an infectious trigger but no causative agent has been identified. Genetic influences on disease susceptibility and outcome have been identified and the current paradigm proposes that KD results from exposure to a common agent that triggers the syndrome only in genetically susceptible hosts(9-11).
The self-limited clinical syndrome is recognized through a constellation of clinical signs that include fever for at least 4 days associated with rash, conjunctival injection, erythema of the lips and oropharynx, edema of the hands and feet, erythema of the palms and soles, and, in the convalescent phase, periungual desquamation(6). Up to 25% of untreated children will develop permanent damage to the coronary arteries with inflammatory cell infiltration of the arterial wall, destruction of the internal elastic lamina, necrosis of smooth muscle cells, myointimal proliferation, and subsequent aneurysm formation (3,12). Aneurysms of systemic, extraparenchymal muscular arteries also occur in a subset of patients with coronary aneurysms(13). The proximal coronary arteries can be readily imaged in infants and children using transthoracic echocardiography that permits reliable and reproducible measurement of the internal diameter of the proximal right and left anterior descending coronary arteries (RCA and LAD) and the expression of these measurements as standard deviation units (Z score) normalized for body surface area (BSA)(14-16).
Administration of a single dose of intravenous immunoglobulin (IVIG) in conjunction with aspirin within the first ten days after fever onset reduces the incidence of aneurysms from 25% to 3-5%(17,18). The AHA guidelines have divided these patients into five groups based on coronary artery Z scores and morphology of the coronary artery lesions(6)(Table). Approximately 30% of IVIG-treated children with KD will develop transient dilatation of the coronary arteries (Z score ≥ 2.5 for the RCA or LAD, AHA Risk level II)(16,19). Another 5-10% will develop coronary artery aneurysms, which in some cases can be attributed to delayed diagnosis and treatment. There are no data regarding the number of young adults in the U.S. who suffered from KD in childhood. If we estimate 4,000 KD patients/year in the U.S. beginning in 1986 when IVIG treatment was first recommended, assume an average age of onset of 2 years, a rate of 30% for coronary artery dilatation, and 5% for aneurysms, then there are currently 24,000 young adults (≥ 18 yrs.) who have recovered from KD and approximately 8,400 young adults who are classified as AHA Risk level II or greater(7). The number of adults classified as Risk Level II or greater will grow by an estimated 1,400 individuals each year. These numbers are clearly underestimates because many KD patients were older than 2 years at the time of disease onset and many clinical cases were never diagnosed. Whatever the real figures are, there is clearly a growing population of young adults with potentially important coronary artery disease following KD in childhood and adult cardiologists must be prepared to care for them.
Cardiovascular sequelae of KD in adults
Only in Japan has an attempt been made to systematically collect mortality data on patients with KD. Over a 10-year period from 1982-1992, a cohort of 6,576 Japanese patients was created and the seventh report on the status of the cohort was recently published (20). As of 2004, there were 3,326 adult subjects in the cohort aged 20-34 years with an average observation period of approximately 17 years. Standardized mortality ratios (SMR) were calculated for subsets in the cohort based on sex, coronary artery sequelae, and timing of death after KD. After the acute phase, the SMR was elevated only for males with known cardiovascular sequelae (expected deaths: 3.9, observed deaths: 10; SMR 2.55, 95% CI 1.23-4.70). The cause of death in these 10 males was listed as coronary artery insufficiency (2), acute myocardial infarction (3), sudden death (1), congestive heart failure (1), influenza pneumonia (1), and suicide (2) with deaths occurring between 11 months to 18 years after onset of KD. Unfortunately, only mortality data are available on the cohort and no information is available on the clinical status of these subjects.
Late complications of KD may include both residual damage from the acute vasculitis as well as the myocarditis(21). In the only longitudinal angiographic study of KD, Kato et al. described the natural history of the vascular lesions in 594 Japanese subjects 10-12 years after onset of KD (3)(Figure 1). This study was performed before the routine use of IVIG to treat acute KD. Long-term complications included stenosis, myocardial infarction, and death. Other series have reported both symptomatic and asymptomatic coronary artery occlusion in regions of previous aneurysms(22,23), coronary artery stenosis(24), coronary artery calcification(25), diastolic dysfunction(26), and sudden death(27). One study of 562 Japanese KD patients with known coronary artery lesions documented the appearance of new aneurysms 2-19 years after disease onset in 15 patients (3%)(28). KD patients with aneurysms at least 6 mm in maximal diameter had a greater than 50% chance of developing a clinically significant stenotic lesion during a mean follow-up period of 8 years(24). Most of these series are from Japan and none report longitudinal outcome in KD patients who were treated with IVIG during the acute illness. Based on the accumulating evidence, it is likely that patients with known aneurysms during the acute phase of KD will have some cardiovascular morbidity as young adults. The fate of IVIG-treated children who had no lesions detected by echocardiography as a result of the acute vasculitis is unknown (Figure 2A and B).
Figure 1. Sequential angiographic evaluation over a 10-21year-period of Japanese patients with KD who developed coronary artery aneurysms (Adapted from Kato et al., Ref. 12).
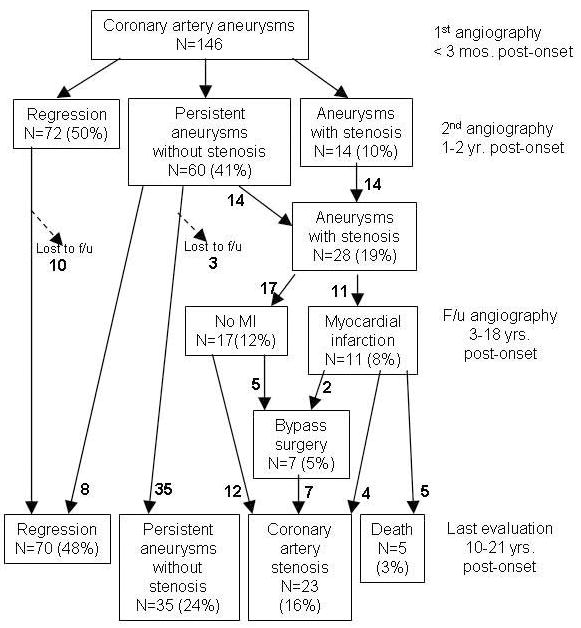
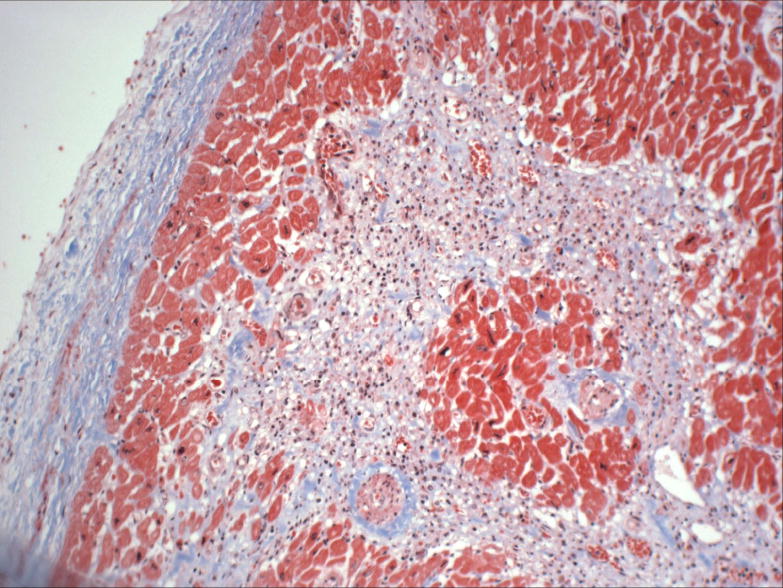
Figure 2. KD Histology.
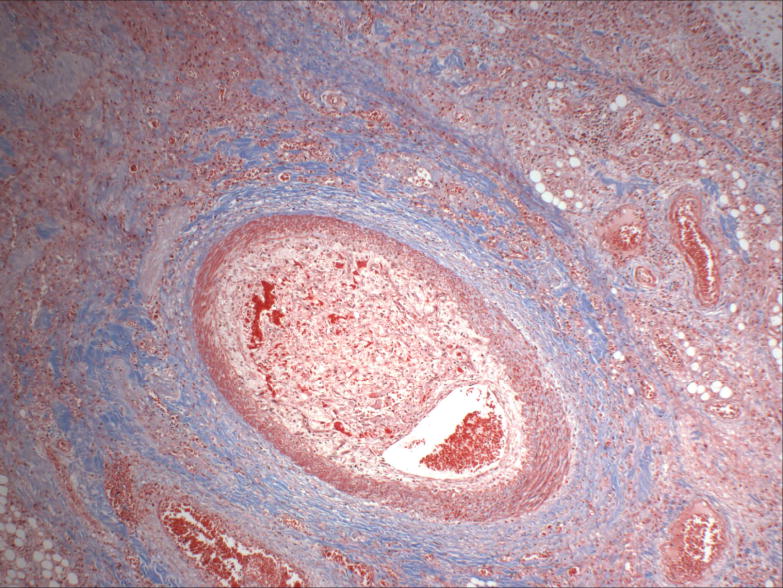
Autopsy findings in a 19 year-old man who developed severe cardiomyopathy 17 years after Kawasaki disease at age 2 years treated with intravenous immunoglobulin. Echocardiography during the acute and convalescent phase showed normal internal dimensions of the coronary arteries. A. Masson trichrome stain of a branch of the right coronary artery showing late organization of a thrombus. Original maginification x40. B. Masson trichrome stain of left ventricle showing endocardial fibrosis with an organizing subendocardial microinfarct. Original magnification x100. Photos courtesy of Dr. Henry F. Krous, Director of Pathology Research, Rady Children’s Hospital, San Diego, CA.
During acute KD, approximately 2% of patients will develop valvulitis followed by scarring of the valve leaflets, most commonly in the mitral valve, leading to valvular incompetence and the need for valve replacement in a subset of patients(29-31). Another manifestation of the cardiovascular damage following acute KD is the progressive dilatation of the aortic root(32). In a longitudinal study of 100 children with KD, the BSA-adjusted aortic root dimension was significantly larger when compared to control subjects. Mild aortic valve regurgitation was noted at the one-year visit in 4% of KD patients(32,33).
Focus on the coronary aneurysms has diverted attention from other potential cardiovascular complications of KD. Diffuse myocarditis followed by myocardial fibrosis may lead to systolic or diastolic dysfunction in a subset of KD patients(34-36). During acute KD, tissue Doppler interrogation of left ventricular inflow velocities has revealed abnormal relaxation patterns and was associated with elevated levels of brain natriuretic peptide(35). Decreased ventricular contractility and abnormal relaxation may be the consequences of antecedent myocardial inflammation and late-onset ventricular arrhythmias and congestive heart failure have been observed(21,37).
Missed KD presenting in adulthood
In 1992, Kato and co-workers in Japan published the results of a questionnaire survey sent to adult cardiologists that asked about adult patients with angiographically proven coronary artery disease that could reasonably be attributed to antecedent KD(38). The survey identified 130 patients age 20-63 years: 21 adults had ischemic heart disease definitely (n=2) or possibly (n=19) attributed to antecedent KD and 109 adults had coronary artery aneurysms with no clear history of clinical KD in childhood. Of the 21 patients with a high likelihood of antecedent KD, 3 had died of ischemic complications and 18 were alive with serious cardiovascular sequelae including mitral regurgitation requiring valve replacement, arrhythmias, dilated cardiomyopathy, and congestive heart failure. The authors concluded that all 130 patients likely had KD as the cause of their vascular damage and that adult cardiologists should be aware of these patients in their clinical practice. No subsequent survey from Japan or elsewhere has been performed to estimate the numbers of adult patients under the care of a cardiologist for the sequelae of KD.
Young adults with no known previous cardiovascular history may present with angina, myocardial infarction, ischemia-induced arrhythmia, or sudden death(39). Characteristics of the coronary arteries that should prompt questioning about antecedent KD include proximal aneurysms with or without calcification followed by an angiographically normal distal segment. Young adults in Japan have presented with ventricular tachycardia in the setting of left heart failure decades after missed KD(37). Investigation of these patients revealed the classic calcified aneurysms of KD. Thus, the acute vasculitis and myocarditis associated with KD may lead to a complex set of cardiovascular problems later in life.
Pathology
Although the term “atherosclerosis” has been loosely applied to the progressive vascular lesion following KD, evidence suggests that this is a misnomer. While many autopsy reports of individuals who died late after KD describe calcified aneurysms, myointimal proliferation, and organizing thrombus in the coronary arteries with recanalization, there is scant mention of lipid-laden macrophages and cholesterol crystals, the hallmarks of established atherosclerosis(40,41). There is ample histological evidence to support the concept that coronary arteries that develop aneurysms as a result of the intense inflammatory process during acute KD have very abnormal architecture despite normalization of the lumen and angiographic evidence of “healing”(42,43). The typical lesions are discrete regions of myointimal proliferation associated with disrupted internal elastic lamina and medial smooth muscle cell necrosis with replacement by fibrosis and calcification. Suzuki et al. examined 7 subjects at autopsy who died 3 to 12 years following acute KD(44). Active remodeling of the aneurysms with intimal proliferation and neoangiogenesis was evident in all cases. None of the subjects had coronary artery lesions consistent with atherosclerosis. Takahashi et al. described a series of 6 subjects with arterial lesions who died from either sudden death (5 subjects) or sepsis (1 subject) at least 15 years following acute KD(45). Only one of the six subjects had pathology consistent with atherosclerosis. No clinical details were provided in this report, so it is unknown if this 39 year-old subject with typical atherosclerotic lesions had cardiovascular risk factors superimposed on his antecedent KD. The extent to which KD is a cardiovascular risk factor for the future development of atherosclerosis is unknown.
Another controversial issue is the pathology of arteries in IVIG-treated individuals whose echocardiograms showed no evidence of structural damage to the coronary artery wall. The scant autopsy data available on the histological changes in children and young adults who have died late after KD appear as case reports, many of them in the forensic literature(39). In an autopsy study of a child who died from unrelated causes 13 months after recovery from KD with normal echocardiograms, the intima of the coronary artery was thickened, the internal elastic lamina was disrupted, and smooth muscle cells were seen infiltrating into the intima(46). Further autopsy studies of incidental deaths in subjects with antecedent KD and normal echocardiograms will be necessary to determine how often KD leads to pathologic changes in coronary arteries with no dilatation noted during the acute phase of the illness. A prospective registry of KD cases would allow tracking of deaths and correlation of the histopathology with echocardiographic assessment during the acute illness.
Pathologic changes in the myocardium as a result of injury during the acute inflammatory phase have also been reported. Three series from Japan reported endomyocardial biopsies at various timepoints after the acute illness(47-49). In the study by Yonesaka et al. hypertrophy, degeneration of myocytes, and fibrosis were noted in the majority of biopsies obtained at least 3 years after KD in 38 subjects, and their presence was more frequent in subjects who had suffered coronary artery aneurysms during the acute phase(48). Yutani et al. found myocardial abnormalities including lymphocyte and plasma cell infiltration, myocardial fibrosis, and disarray of myocardial fibers in every biopsy from the 201 KD subjects in their study(47,50). Changes were most pronounced in patients studied four or more years after disease onset and the investigators raised the question of progression of myocardial pathology over time.
Some autopsy reports of adults late after KD describe cardiomyocyte drop out and diffuse fibrosis not in the watershed distribution of the epicardial coronary arteries(51-53)(Figure 2B). Increasing numbers of deaths that are attributed to left ventricular dysfunction and presumed ventricular arrhythmias are being reported in young adults from Japan with antecedent KD(27). Whether the diffuse fibrosis is a consequence of ischemic injury from microinfarcts or inflammatory cardiomyocyte injury or both is unknown.
Endothelial cell dysfunction and arterial wall injury
In addition to causing coronary artery aneurysms and stenoses, KD also has been shown to have deleterious effects on coronary artery function years after the acute presentation. Arterial function has been assessed in multiple studies evaluating myocardial and coronary flow reserve with angiography(54-57), invasive flow measurements(58-60), positron emission tomography(61-63), and transthoracic Doppler ultrasound of the coronary arteries(64). Abnormalities have been observed in endothelial-mediated as well as endothelial-independent coronary artery vasodilatation. In patients with persistent coronary artery aneurysms, coronary artery function has repeatedly been shown to be impaired compared to controls(56,57,59-61,64). Coronary flow reserve is also abnormal in patients with a history of transiently dilated coronary arteries (54-57,60-62), and in patients with evidence of inducible ischemia but angiographically normal-appearing coronary arteries (58,59). Even in patients with a history of KD without antecedent coronary artery dilatation or ischemia, impaired coronary flow reserve has been observed(54,60,61,63,64), although conflicting studies showed no difference from normal controls(55-57). Thus, the damage to coronary arteries appears to extend beyond that which is observed angiographically.
Studies of systemic vascular function via flow-mediated dilatation of the brachial artery have yielded conflicting results. Dhillon et al. demonstrated abnormal brachial artery reactivity in 20 male subjects in the U.K. age 11-19 years who were studied 5-17 years post-onset of KD, irrespective of whether they had developed aneurysms during the acute phase(65). In studies of Japanese subjects of approximately the same age and interval from disease onset, only patients with previous aneurysms had abnormal flow-mediated dilatation(66,67). Finally, a recent study of 52 Canadian KD subjects concluded that there was no evidence of long-term endothelial cell dysfunction late after KD(68). It is unclear whether these conflicting results are best explained by methodological issues or genetic differences of the populations studied. Metabolic abnormalities manifested as abnormal lipid profiles with persistently low HDL may also contribute to endothelial cell dysfunction(69,70).
Carotid intimal medial thickness (IMT) measured non-invasively by ultrasound is used as a surrogate marker of coronary atherosclerosis and has been correlated with the risk of stroke and MI in adults with atherosclerosis(71). Several small studies have demonstrated increased carotid IMT in patients who have recovered from KD, but the significance of this observation is unclear(66,72-74). Patients with remodeled coronary aneurysms have even greater carotid IMT than those without aneurysms. However, no study to date has correlated clinical outcomes with IMT findings in KD patients. There is no evidence that increased carotid IMT in KD patients implies atherosclerosis and the prognostic significance of this measurement is unknown.
Identifying the adult with possible antecedent KD
The adult cardiologist should be sufficiently familiar with the signs and symptoms of acute KD to allow questioning of the patient or parent about an antecedent KD-compatible illness that was not diagnosed. Features of the illness that are frequently recalled by patients and parents are the prolonged fever, rash, “bloodshot” eyes in the acute phase, and peeling of the fingers and toes in the convalescent phase. Common misdiagnoses for KD include viral syndrome, measles, scarlet fever, allergic reaction to antibiotics, and Stevens Johnson syndrome(4). Because the etiology remains unknown, there is no specific diagnostic test that can be used to make a retrospective diagnosis.
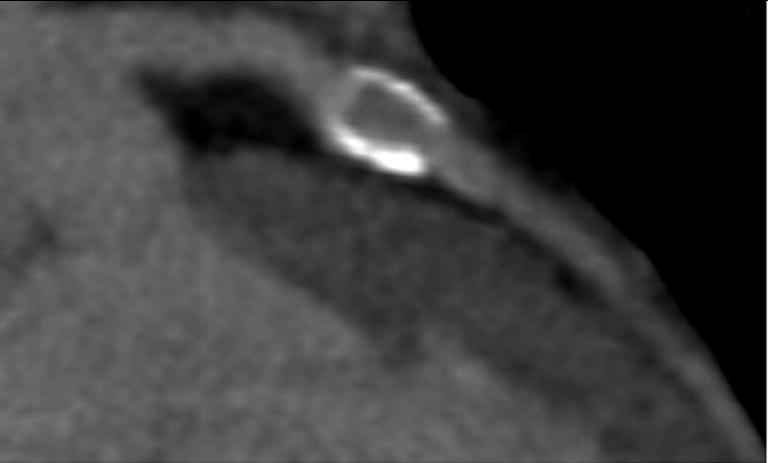
Imaging studies may be helpful in identifying patients with antecedent KD (LOE IIa, C). Calcification of the arterial wall in regions where former aneurysms have remodeled are hallmarks of KD and may even be apparent on chest radiograph(41,75). In a study of Japanese young adults 20 years following acute KD, 94% of those with aneurysms at least 6 mm in internal diameter during the subacute phase of the illness had calcification seen by electron beam computed tomography (CT) (76). Arterial wall calcification can be also be imaged by multislice CT angiography (Figure 3). Coronary calcium scores are elevated in a subset of KD subjects with antecedent vascular injury(77). Suspicion of antecedent KD should be high in the young adult with coronary artery calcification and a low risk profile for atherosclerosis.
Figure 3. Calcification of coronary artery.
Multislice computed tomography angiogram showing extensive calcification of a left anterior descending coronary artery aneurysm in a 12 year-old boy 7 years after acute KD.
Differentiation of atherosclerotic aneurysms from KD may be aided by angiography (LOE IIb, C). Whereas atherosclerosis tends to involve the arterial wall diffusely, KD results in focal abnormalities only at the site of previous aneurysms. Vessels proximal and distal to the lesion appear healthy with a smooth luminal surface and normal diameter (Figure 4). Remodeled aneurysms of KD may be more difficult to recognize and intravascular ultrasound (IVUS) may be useful to detect the thickened arterial wall of the aneurysm(78,79).
Figure 4. Right coronary artery occlusion.
Angiogram of occluded right coronary artery (RCA) aneurysm in a 33 year-old man who suffered a KD-compatible illness at age 6 years (diagnosed as non-specific viral illness) and was asymptomatic until his myocardial infarction. A. Injection of the occluded RCA B. RCA after percutaneous transluminal coronary angioplasty with re-established distal flow. Note smooth appearance of distal branches of the RCA C. Patent RCA aneurysm one month after PTCA, aspirin, and warfarin therapy maintaining an INR of 2-2.5.
Magnetic resonance (MR) imaging is emerging as the modality of choice for imaging structural damage late after KD (LOE IIa, C). Repeated imaging is possible without concerns for radiation exposure. Myocardial inflammation using T2-weighted images as well as myocardial scarring and fibrosis can be detected as late gadolinium enhancement(80-82). At the present time, gadolinium MR angiography is not as sensitive as CT angiography or cardiac catheterization for the detection of coronary artery stenosis (80)
Management of the adult with antecedent KD
The optimal management of adults with antecedent KD can only be established through systematic study of this patient population with the creation of regional or national registries to record patient histories and outcomes and generate hypotheses regarding their care that could be tested in appropriately powered clinical studies. One challenge of studies designed to collect cardiovascular outcome data will be to differentiate the effects of antecedent KD from the effects of traditional cardiovascular risk factors, which will accumulate as this population ages. For now, the management of these patients must be guided by common sense and an appreciation of the uncertainty about the cardiovascular outcomes in adults who suffered KD in childhood. The Japanese Circulation Society published guidelines based on the opinion of experts in Japan in 2003 for the management and treatment of adults who had KD in childhood (Table 2)(83). The guidelines state that cardiovascular symptoms in KD patients only begin to appear two decades after the onset of the acute disease, so only now are patients beginning to present with sequelae.
Table 2.
Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease as outlined by the Japanese Circulation Society (adapted from (83))
| Patient risk level | Recommendation |
|---|---|
| AHA risk level 1 and 2 | Consider non-invasive testing every 3-4 yrs.* No medical therapy |
| AHA risk level 3, 4, 5 without symptoms | Evaluate every 4-6 mos. with non-invasive testing and angiography every 2-3 years. Treat with low-dose aspirin. |
| AHA risk level 3, 4, 5 with symptoms | Evaluate every 3-4 mos. with non-invasive testing and angiography as needed. Treat with low-dose aspirin; other medications as dictated by the cardiovascular status. |
Non-invasive testing: Exercise testing, nuclear imaging studies, Holter monitor, transesophageal echocardiogram, magnetic resonance angiography, computed tomography angiogram
As with all clinical practice, the admonishment of primum non nocere must be heeded. Subjecting otherwise healthy, asymptomatic individuals to frequent testing may have undesirable psychological consequences. At the same time, ignoring a past history of KD may lead to missed opportunities for intervention in a subset of these patients. A rational approach to these patients might include standard testing for cardiovascular risk assessment as well as specific testing to detect sub-clinical ischemia, valvular dysfunction, and myocardial fibrosis caused by antecedent KD. Testing might include a lipid profile, high sensitivity C-reactive protein (CRP) level, electrocardiogram (ECG), two-dimensional (2D) transthoracic echocardiogram, and stress echocardiogram (LOE IIb, C). Because arterial calcification is a feature of KD vascular lesions, a single, baseline coronary artery calcium score by CT may be informative, particularly for patients whose initial evaluation by echocardiogram in childhood was technically inadequate or for whom the results are unknown(77) (LOE IIb, C). MR imaging can detect small myocardial scars and fibrosis that cannot be detected by other modalities and thus cardiac MRI may also be useful in the baseline evaluation of this patient population (LOE IIb, C). Non-invasive assessments of endothelial cell function such as brachial artery flow-mediated dilatation and structural assessments such as carotid IMT remain research tools at this time with uncertain prognostic significance. Follow-up evaluations every 3 to 5 years are currently recommended for KD patients during childhood and continuing this periodic re-assessment into adulthood seems prudent given the lack of information about the long-term consequences of KD(6). No medication is currently recommended for this patient population.
Adults with persistent or regressed aneurysms should be followed at regular intervals with functional and structural cardiovascular studies to determine the need for interventions (LOE IIa, B). When considering CT, cardiac catheterization, or nuclear medicine studies, consideration should be given to the young age of these adults and the need for life-long, repeated assessments when weighing the risks versus the benefits of the radiation exposure. While repeated MR imaging is without known risk, CT angiography provides a better assessment of coronary artery stenosis and calcification. Future improvements in software and cardiac cycle gaiting techniques will likely reduce the radiation exposure.
Optimal pharmacologic therapy of adult patients with persistent or regressed aneurysms has not been established. The AHA guidelines advocate the use of aspirin as an antiplatelet agent (3-5 mg/kg/day) in children with small to moderate aneurysms (< 8 mm)(Table 1)(6). Ticlopidine or clopidogrel are also added to aspirin therapy at some centers (LOE IIb, C). The current AHA guidelines suggest discontinuation of anti-platelet therapy when the aneurysm regresses (LOE IIa, C)(Table). HMG-CoA reductase inhibitors, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers may all mobilize endothelial progenitor cells and promote vascular wall remodeling although there are no data to support their use in the setting of KD(84,85).
Table 1.
American Heart Association risk stratification for Kawasaki disease (Adapted from ref. 6)
| Risk Level | Pharmacological Therapy | Follow-Up and Diagnostic Testing | Invasive Testing |
|---|---|---|---|
| I (no coronary artery changes at any stage of illness) | None beyond 1st 6–8 weeks | Cardiovascular risk assessment, counseling at 5-y intervals | None recommended |
| II (transient coronary artery ectasia disappears within 1st 6–8 weeks) | None beyond 1st 6–8 weeks | Cardiovascular risk assessment, counseling at 3- to 5-y intervals | None recommended |
| III (1 small–medium coronary artery aneurysm/major coronary artery) | Low-dose aspirin (3–5 mg/kg aspirin/d), at least until aneurysm regression documented | Annual cardiology follow-up with echocardiogram +ECG, combined with cardiovascular risk assessment, counseling; biennial stress test/evaluation of myocardial perfusion scan | Angiography, if noninvasive test suggests ischemia |
| IV (≥1 large or giant coronary artery aneurysm, or multiple or complex aneurysms in same coronary artery, without obstruction) | Long-term antiplatelet therapy and warfarin (target INR 2.0–2.5) or low-molecular-weight heparin (target: antifactor Xa level 0.5–1.0 U/mL) should be combined in giant aneurysms | Biannual follow-up with echocardiogram + ECG; annual stress test/evaluation of myocardial perfusion scan | 1st angiography at 6–12 mo or sooner if clinically indicated; repeated angiography if noninvasive test, clinical, or laboratory findings suggest ischemia; elective repeat angiography under some circumstances (see text) |
| V (coronary artery obstruction) | Long-term low-dose aspirin; warfarin or low-molecular-weight heparin if giant aneurysm persists; consider use of ß-blockers to reduce myocardial O2 consumption | Biannual follow-up with echocardiogram and ECG; annual stress test/evaluation of myocardial perfusion scan | Angiography recommended to address therapeutic options |
For KD patients with persistent aneurysms, treatment regimens should be tailored based on the size of the aneurysm and flow characteristics. In patients with giant aneurysms (≥8 mm) in which blood flow is sluggish and risk for thrombosis is high, systemic anticoagulation with warfarin with an INR between 2.0-2.5 has been associated with improved survival in small series of KD patients from Canada and Japan (LOE IIa, B) (86,87). There are no data to inform the management of adult patients with large aneurysms, but continuation of systemic anticoagulation seems reasonable. Addition of aspirin for platelet inhibition should also be considered (LOE IIa, C).
Based on available data, pregnancy in KD patients with persistent aneurysms is not associated with increased risk(88-90). A nationwide survey in Japan reported the outcome of 46 deliveries in 30 KD patients(91). Two-thirds of the deliveries were vaginal. Mothers with persistent giant aneurysms were given subcutaneous low-molecular weight heparin and low-dose aspirin during the pregnancy. There were no cardiac complications and the authors concluded that the mode of delivery should be dictated by obstetrical considerations and that coronary artery aneurysms alone were not an indication for Caesarean section (LOE IIb, B).
Percutaneous catheter interventions may be necessary if narrowing of the vessel lumen leads to signs or symptoms of ischemia (LOE B, IIa). The Japanese have developed consensus guidelines for the use of these procedures in childhood(92). Percutaneous transluminal angioplasty (PTCA) has been complicated by the need for very high balloon pressures in highly calcified lesions leading to neoaneurysm formation(93). There is limited experience with revascularization procedures using covered or drug-eluting stents in this patient population(94,95). Rotational atherectomy is the interventional procedure of choice for heavily calcified, stenotic lesions which are not amenable to PTCA, although current experience is limited (LOE IIa,C) (96).
Surgical approaches using both venous and arterial grafts have been used in this patient population (LOE IIa, B). In a survey of 156 KD patients older than 12 years treated with internal thoracic artery grafts, the patency rate at 15 years was 91%(97). Use of arterial grafts in patients with large growth potential resulted in a much higher rate of graft patency over time as compared to venous grafts. Surgical intervention in young adults with aneurysms following KD has been reported(98). Surgical risks and graft survival did not differ from those of patients undergoing similar procedures for ischemia due to atherosclerotic disease.
Cardiac transplantation has been successfully performed for KD patients with end-stage cardiomyopathy, severe ventricular arrhythmias, and inoperable multivessel stenotic coronary artery disease(99). There has been no recurrence of KD or coronary artery aneurysms in the transplanted hearts and all morbidity and mortality in this cohort have been related to rejection and complications of immunosuppression.
Conclusion
In the coming years, growing numbers of patients with cardiovascular complications after KD will present to internists and adult cardiologists for care. The vascular lesions in these patients differ from atherosclerosis and may include coronary artery aneurysms, calcification, and stenosis. These patients may also present with valvular incompetence due to scarring of the leaflets or progressive aortic root dilatation and myocardial lesions including diffuse fibrosis or focal scarring in regions of myocardial ischemia or infarct. The inflammatory insult associated with acute KD has the potential to affect all components of the cardiovascular system. Systematic study of adults with a history of KD in childhood is needed to define the natural history of this enigmatic disease.
Acknowledgments
The authors wish to thank Dr. Hiroko Shike for helpful discussion, Drs. Jeffrey Fraser and Henry F. Krous for assistance with the figures, and Dr. Chisato Shimizu for translation of the Japanese guidelines.
This work supported in part by a grant from the National Institutes of Health, Heart, Lung, Blood Institute to JCB (RO1-HL69413)
Abbreviations
- KD
Kawasaki disease
- INR
International normal ratio
- IVIG
Intravenous immunoglobulin
- RCA
Right coronary artery
- LAD
Left anterior descending coronary artery
- BSA
Body surface area
- AHA
American Heart Association
- SMR
Standardized mortality ratio
- LOE
Level of evidence
- CT
Computed tomography
- MRI
Magnetic resonance imaging
- CRP
C-reactive protein
- ECG
Electrocardiogram
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimersthat apply to the journal pertain.
References
- 1.Taubert KA, Rowley AH, Shulman ST. Nationwide survey of Kawasaki disease and acute rheumatic fever. J Pediatr. 1991;119:279–82. doi: 10.1016/s0022-3476(05)80742-5. [DOI] [PubMed] [Google Scholar]
- 2.Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974;54:271–6. [PubMed] [Google Scholar]
- 3.Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Kawasaki disease. A 10- to 21-year follow-up study of 594 patients. Circulation. 1996;94:1379–85. doi: 10.1161/01.cir.94.6.1379. [DOI] [PubMed] [Google Scholar]
- 4.Burns JC, Glode MP. Kawasaki syndrome. Lancet. 2004;364:533–44. doi: 10.1016/S0140-6736(04)16814-1. [DOI] [PubMed] [Google Scholar]
- 5.Senzaki H. Long-term outcome of Kawasaki disease. Circulation. 2008;118:2763–72. doi: 10.1161/CIRCULATIONAHA.107.749515. [DOI] [PubMed] [Google Scholar]
- 6.Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–71. doi: 10.1161/01.CIR.0000145143.19711.78. [DOI] [PubMed] [Google Scholar]
- 7.Holman RC, Curns AT, Belay ED, Steiner CA, Schonberger LB. Kawasaki syndrome hospitalizations in the United States, 1997 and 2000. Pediatrics. 2003;112:495–501. doi: 10.1542/peds.112.3.495. [DOI] [PubMed] [Google Scholar]
- 8.Nakamura Y, Yashiro M, Uehara R, Oki I, Kayaba K, Yanagawa H. Increasing incidence of Kawasaki disease in Japan: nationwide survey. Pediatr Int. 2008;50:287–90. doi: 10.1111/j.1442-200X.2008.02572.x. [DOI] [PubMed] [Google Scholar]
- 9.Rowley AH, Baker SC, Orenstein JM, Shulman ST. Searching for the cause of Kawasaki disease--cytoplasmic inclusion bodies provide new insight. Nat Rev Microbiol. 2008;6:394–401. doi: 10.1038/nrmicro1853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Onouchi Y, Gunji T, Burns JC, et al. ITPKC functional polymorphism associated with Kawasaki disease susceptibility and formation of coronary artery aneurysms. Nat Genet. 2008;40:35–42. doi: 10.1038/ng.2007.59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dergun M, Kao A, Hauger SB, Newburger JW, Burns JC. Familial occurrence of Kawasaki syndrome in North America. Arch Pediatr Adolesc Med. 2005;159:876–81. doi: 10.1001/archpedi.159.9.876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brown TJ, Crawford SE, Cornwall ML, Garcia F, Shulman ST, Rowley AH. CD8 T lymphocytes and macrophages infiltrate coronary artery aneurysms in acute Kawasaki disease. J Infect Dis. 2001;184:940–3. doi: 10.1086/323155. [DOI] [PubMed] [Google Scholar]
- 13.Amano S, Hazama F, Hamashima Y. Pathology of Kawasaki disease: II. Distribution and incidence of the vascular lesions. Jpn Circ J. 1979;43:741–8. doi: 10.1253/jcj.43.741. [DOI] [PubMed] [Google Scholar]
- 14.Chung KJ, Brandt L, Fulton DR, Kreidberg MB. Cardiac and coronary arterial involvement in infants and children from New England with mucocutaneous lymph node syndrome (Kawasaki disease). Angiocardiographic-echocardiographic correlations. Am J Cardiol. 1982;50:136–42. doi: 10.1016/0002-9149(82)90019-4. [DOI] [PubMed] [Google Scholar]
- 15.Capannari TE, Daniels SR, Meyer RA, Schwartz DC, Kaplan S. Sensitivity, specificity and predictive value of two-dimensional echocardiography in detecting coronary artery aneurysms in patients with Kawasaki disease. J Am Coll Cardiol. 1986;7:355–60. doi: 10.1016/s0735-1097(86)80505-8. [DOI] [PubMed] [Google Scholar]
- 16.de Zorzi A, Colan SD, Gauvreau K, Baker AL, Sundel RP, Newburger JW. Coronary artery dimensions may be misclassified as normal in Kawasaki disease. J Pediatr. 1998;133:254–8. doi: 10.1016/s0022-3476(98)70229-x. [DOI] [PubMed] [Google Scholar]
- 17.Newburger JW, Takahashi M, Burns JC, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med. 1986;315:341–7. doi: 10.1056/NEJM198608073150601. [DOI] [PubMed] [Google Scholar]
- 18.Newburger JW, Takahashi M, Beiser AS, et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N Engl J Med. 1991;324:1633–9. doi: 10.1056/NEJM199106063242305. [DOI] [PubMed] [Google Scholar]
- 19.McCrindle BW, Li JS, Minich LL, et al. Coronary artery involvement in children with Kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation. 2007;116:174–9. doi: 10.1161/CIRCULATIONAHA.107.690875. [DOI] [PubMed] [Google Scholar]
- 20.Nakamura Y, Aso E, Yashiro M, et al. Mortality among persons with a history of Kawasaki disease in Japan. Circ J. 2008;72:134–138. doi: 10.1253/circj.72.134. [DOI] [PubMed] [Google Scholar]
- 21.Tsuda E, Matsuo M, Naito H, Noguchi T, Nonogi H, Echigo S. Clinical features in adults with coronary arterial lesions caused by presumed Kawasaki disease. Cardiol Young. 2007;17:84–9. doi: 10.1017/S1047951107000169. [DOI] [PubMed] [Google Scholar]
- 22.Tatara K, Kusakawa S, Itoh K, et al. Long-term prognosis of Kawasaki disease patients with coronary artery obstruction. Heart Vessels. 1989;5:47–51. doi: 10.1007/BF02058358. [DOI] [PubMed] [Google Scholar]
- 23.Shiraishi I, Onouchi Z, Hayano T, Hamaoka K, Kiyosawa N. Asymptomatic myocardial infarction in Kawasaki disease: long-term prognosis. Pediatr Cardiol. 1991;12:78–82. doi: 10.1007/BF02238407. [DOI] [PubMed] [Google Scholar]
- 24.Tsuda E, Kamiya T, Ono Y, Kimura K, Kurosaki K, Echigo S. Incidence of stenotic lesions predicted by acute phase changes in coronary arterial diameter during Kawasaki disease. Pediatr Cardiol. 2005;26:73–9. doi: 10.1007/s00246-004-0698-1. [DOI] [PubMed] [Google Scholar]
- 25.Muneuchi J, Joo K, Morihana E, Mizushima A. Detectable Silent Calcification in a Regressed Coronary Artery Aneurysm of a Young Adult with a History of Kawasaki Disease. Pediatr Cardiol. 2007 doi: 10.1007/s00246-007-9062-6. [DOI] [PubMed] [Google Scholar]
- 26.Arnold R, Goebel B, Ulmer HE, Gorenflo M, Poerner TC. An exercise tissue Doppler and strain rate imaging study of diastolic myocardial dysfunction after Kawasaki syndrome in childhood. Cardiol Young. 2007;17:478–86. doi: 10.1017/S1047951107000959. [DOI] [PubMed] [Google Scholar]
- 27.Tsuda E, Arakaki Y, Shimizu T, et al. Changes in causes of sudden deaths by decade in patients with coronary arterial lesions due to Kawasaki disease. Cardiol Young. 2005;15:481–8. doi: 10.1017/S1047951105001344. [DOI] [PubMed] [Google Scholar]
- 28.Tsuda E, Kamiya T, Ono Y, Kimura K, Echigo S. Dilated coronary arterial lesions in the late period after Kawasaki disease. Heart. 2005;91:177–82. doi: 10.1136/hrt.2003.025338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Akagi T, Kato H, Inoue O, Sato N, Imamura K. Valvular heart disease in Kawasaki syndrome: incidence and natural history. Am Heart J. 1990;120:366–72. doi: 10.1016/0002-8703(90)90081-8. [DOI] [PubMed] [Google Scholar]
- 30.Nakamura Y, Yashiro M, Uehara R, Oki I, Watanabe M, Yanagawa H. Epidemiologic Features of Kawasaki Disease in Japan: Results from the Nationwide Survey in 2005-2006. J Epidemiol. 2008 doi: 10.2188/jea.JE2008001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Imakita M, Sasaki Y, Misugi K, Miyazawa Y, Hyodo Y. Kawasaki disease complicated with mitral insufficiency. Autopsy findings with special reference to valvular lesion. Acta Pathol Jpn. 1984;34:605–16. doi: 10.1111/j.1440-1827.1984.tb07588.x. [DOI] [PubMed] [Google Scholar]
- 32.Ravekes WJ, Colan SD, Gauvreau K, et al. Aortic root dilation in Kawasaki disease. Am J Cardiol. 2001;87:919–22. doi: 10.1016/s0002-9149(00)01541-1. [DOI] [PubMed] [Google Scholar]
- 33.Nakano H, Nojima K, Saito A, Ueda K. High incidence of aortic regurgitation following Kawasaki disease. J Pediatr. 1985;107:59–63. doi: 10.1016/s0022-3476(85)80615-6. [DOI] [PubMed] [Google Scholar]
- 34.Nagasawa H, Arakaki Y, Yamada O, Nakajima T, Kamiya T. Longitudinal observations of left ventricular end-diastolic dimension in children using echocardiography. Pediatr Cardiol. 1996;17:169–74. doi: 10.1007/BF02505207. [DOI] [PubMed] [Google Scholar]
- 35.Kurotobi S, Kawakami N, Shimizu K, et al. Brain Natriuretic Peptide as a Hormonal Marker of Ventricular Diastolic Dysfunction in Children with Kawasaki Disease. Pediatr Cardiol. 2005 doi: 10.1007/s00246-004-0812-4. [DOI] [PubMed] [Google Scholar]
- 36.Takeuchi D, Saji T, Takatsuki S, Fujiwara M. Abnormal tissue doppler images are associated with elevated plasma brain natriuretic peptide and increased oxidative stress in acute Kawasaki disease. Circ J. 2007;71:357–62. doi: 10.1253/circj.71.357. [DOI] [PubMed] [Google Scholar]
- 37.Yagi S, Tsuda E, Shimizu W, et al. Two adults requiring implantable defibrillators because of ventricular tachycardia and left ventricular dysfunction caused by presumed Kawasaki disease. Circ J. 2005;69:870–4. doi: 10.1253/circj.69.870. [DOI] [PubMed] [Google Scholar]
- 38.Kato H, Inoue O, Kawasaki T, Fujiwara H, Watanabe T, Toshima H. Adult coronary artery disease probably due to childhood Kawasaki disease. Lancet. 1992;340:1127–9. doi: 10.1016/0140-6736(92)93152-d. [DOI] [PubMed] [Google Scholar]
- 39.Burns JC, Shike H, Gordon JB, Malhotra A, Schoenwetter M, Kawasaki T. Sequelae of Kawasaki disease in adolescents and young adults. J Am Coll Cardiol. 1996;28:253–7. doi: 10.1016/0735-1097(96)00099-x. [DOI] [PubMed] [Google Scholar]
- 40.Fujiwara H, Fujiwara T, Kao TC, Ohshio G, Hamashima Y. Pathology of Kawasaki disease in the healed stage. Relationships between typical and atypical cases of Kawasaki disease. Acta Pathol Jpn. 1986;36:857–67. doi: 10.1111/j.1440-1827.1986.tb03119.x. [DOI] [PubMed] [Google Scholar]
- 41.Muneuchi J, Joo K, Morihana E, Mizushima A. Detectable silent calcification in a regressed coronary artery aneurysm of a young adult with a history of kawasaki disease. Pediatr Cardiol. 2008;29:195–7. doi: 10.1007/s00246-007-9062-6. [DOI] [PubMed] [Google Scholar]
- 42.Amano S, Hazama F, Hamashima Y. Pathology of Kawasaki disease: I. Pathology and morphogenesis of the vascular changes. Jpn Circ J. 1979;43:633–43. doi: 10.1253/jcj.43.633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tsuda E, Kamiya T, Kimura K, Ono Y, Echigo S. Coronary artery dilatation exceeding 4.0 mm during acute Kawasaki disease predicts a high probability of subsequent late intima-medial thickening. Pediatr Cardiol. 2002;23:9–14. doi: 10.1007/s00246-001-0004-4. [DOI] [PubMed] [Google Scholar]
- 44.Suzuki A, Miyagawa-Tomita S, Komatsu K, et al. Active remodeling of the coronary arterial lesions in the late phase of Kawasaki disease: immunohistochemical study. Circulation. 2000;101:2935–41. doi: 10.1161/01.cir.101.25.2935. [DOI] [PubMed] [Google Scholar]
- 45.Takahashi K, Oharaseki T, Naoe S. Pathological study of postcoronary arteritis in adolescents and young adults: with reference to the relationship between sequelae of Kawasaki disease and atherosclerosis. Pediatr Cardiol. 2001;22:138–42. doi: 10.1007/s002460010180. [DOI] [PubMed] [Google Scholar]
- 46.Suzuki A, Miyagawa-Tomita S, Komatsu K, et al. Immunohistochemical study of apparently intact coronary artery in a child after Kawasaki disease. Pediatr Int. 2004;46:590–6. doi: 10.1111/j.1442-200x.2004.01943.x. [DOI] [PubMed] [Google Scholar]
- 47.Yutani C, Okano K, Kamiya T, et al. Histopathological study on right endomyocardial biopsy of Kawasaki disease. Br Heart J. 1980;43:589–92. doi: 10.1136/hrt.43.5.589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yonesaka S, Takahashi T, Matubara T, et al. Histopathological study on Kawasaki disease with special reference to the relation between the myocardial sequelae and regional wall motion abnormalities of the left ventricle. Jpn Circ J. 1992;56:352–8. doi: 10.1253/jcj.56.352. [DOI] [PubMed] [Google Scholar]
- 49.Haneda N, Mori C. Histopathologic and coronary angiographic assessment of effectiveness of aspirin or aspirin-and-gammaglobulin in Kawasaki disease. Acta Paediatr Jpn. 1993;35:294–7. doi: 10.1111/j.1442-200x.1993.tb03056.x. [DOI] [PubMed] [Google Scholar]
- 50.Yutani C, Go S, Kamiya T, et al. Cardiac biopsy of Kawasaki disease. Arch Pathol Lab Med. 1981;105:470–3. [PubMed] [Google Scholar]
- 51.Sakai Y, Takayanagi K, Inoue T, et al. Coronary artery aneurysms and congestive heart failure--possible long-term course of Kawasaki disease in an adult--a case report. Angiology. 1988;39:625–30. doi: 10.1177/000331978803900711. [DOI] [PubMed] [Google Scholar]
- 52.Kristensen IB, Kristensen BO. Sudden death caused by thrombosed coronary artery aneurysm. Two unusual cases of Kawasaki disease. Int J Legal Med. 1994;106:277–80. doi: 10.1007/BF01225421. [DOI] [PubMed] [Google Scholar]
- 53.Rozin L, Koehler SA, Shakir A, Ladham S, Wecht CH. Kawasaki disease: a review of pathologic features of stage IV disease and two cases of sudden death among asymptotic young adults. Am J Forensic Med Pathol. 2003;24:45–50. doi: 10.1097/01.PAF.0000051518.85512.FD. [DOI] [PubMed] [Google Scholar]
- 54.Suzuki A, Yamagishi M, Kimura K, et al. Functional behavior and morphology of the coronary artery wall in patients with Kawasaki disease assessed by intravascular ultrasound. J Am Coll Cardiol. 1996;27:291–6. doi: 10.1016/0735-1097(95)00447-5. [DOI] [PubMed] [Google Scholar]
- 55.Iemura M, Ishii M, Sugimura T, Akagi T, Kato H. Long term consequences of regressed coronary aneurysms after Kawasaki disease: vascular wall morphology and function. Heart. 2000;83:307–11. doi: 10.1136/heart.83.3.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Sugimura T, Kato H, Inoue O, Takagi J, Fukuda T, Sato N. Vasodilatory response of the coronary arteries after Kawasaki disease: evaluation by intracoronary injection of isosorbide dinitrate. J Pediatr. 1992;121:684–8. doi: 10.1016/s0022-3476(05)81893-1. [DOI] [PubMed] [Google Scholar]
- 57.Yamakawa R, Ishii M, Sugimura T, et al. Coronary endothelial dysfunction after Kawasaki disease: evaluation by intracoronary injection of acetylcholine. J Am Coll Cardiol. 1998;31:1074–80. doi: 10.1016/s0735-1097(98)00033-3. [DOI] [PubMed] [Google Scholar]
- 58.Hamaoka K, Onouchi Z, Ohmochi Y. Coronary flow reserve in children with Kawasaki disease without angiographic evidence of coronary stenosis. Am J Cardiol. 1992;69:691–2. doi: 10.1016/0002-9149(92)90167-w. [DOI] [PubMed] [Google Scholar]
- 59.Hamaoka K, Onouchi Z, Kamiya Y, Sakata K. Evaluation of coronary flow velocity dynamics and flow reserve in patients with Kawasaki disease by means of a Doppler guide wire. J Am Coll Cardiol. 1998;31:833–40. doi: 10.1016/s0735-1097(98)00019-9. [DOI] [PubMed] [Google Scholar]
- 60.Mitani Y, Okuda Y, Shimpo H, et al. Impaired endothelial function in epicardial coronary arteries after Kawasaki disease. Circulation. 1997;96:454–61. [PubMed] [Google Scholar]
- 61.Furuyama H, Odagawa Y, Katoh C, et al. Altered myocardial flow reserve and endothelial function late after Kawasaki disease. J Pediatr. 2003;142:149–54. doi: 10.1067/mpd.2003.46. [DOI] [PubMed] [Google Scholar]
- 62.Hauser M, Bengel F, Kuehn A, et al. Myocardial blood flow and coronary flow reserve in children with “normal” epicardial coronary arteries after the onset of Kawasaki disease assessed by positron emission tomography. Pediatr Cardiol. 2004;25:108–12. doi: 10.1007/s00246-003-0472-9. [DOI] [PubMed] [Google Scholar]
- 63.Muzik O, Paridon SM, Singh TP, Morrow WR, Dayanikli F, Di Carli MF. Quantification of myocardial blood flow and flow reserve in children with a history of Kawasaki disease and normal coronary arteries using positron emission tomography. J Am Coll Cardiol. 1996;28:757–62. doi: 10.1016/0735-1097(96)00199-4. [DOI] [PubMed] [Google Scholar]
- 64.Cicala S, Galderisi M, Grieco M, et al. Transthoracic echo-Doppler assessment of coronary microvascular function late after Kawasaki disease. Pediatr Cardiol. 2008;29:321–7. doi: 10.1007/s00246-007-9030-1. [DOI] [PubMed] [Google Scholar]
- 65.Dhillon R, Clarkson P, Donald AE, et al. Endothelial dysfunction late after Kawasaki disease. Circulation. 1996;94:2103–6. doi: 10.1161/01.cir.94.9.2103. [DOI] [PubMed] [Google Scholar]
- 66.Ikemoto Y, Ogino H, Teraguchi M, Kobayashi Y. Evaluation of preclinical atherosclerosis by flow-mediated dilatation of the brachial artery and carotid artery analysis in patients with a history of Kawasaki disease. Pediatr Cardiol. 2005;26:782–6. doi: 10.1007/s00246-005-0921-8. [DOI] [PubMed] [Google Scholar]
- 67.Kadono T, Sugiyama H, Hoshiai M, et al. Endothelial Function Evaluated by Flow-Mediated Dilatation in Pediatric Vascular Disease. Pediatr Cardiol. 2005 doi: 10.1007/s00246-004-0755-9. [DOI] [PubMed] [Google Scholar]
- 68.McCrindle BW, McIntyre S, Kim C, Lin T, Adeli K. Are patients after Kawasaki disease at increased risk for accelerated atherosclerosis? J Pediatr. 2007;151:244–8. 248 e1. doi: 10.1016/j.jpeds.2007.03.056. [DOI] [PubMed] [Google Scholar]
- 69.Newburger JW, Burns JC, Beiser AS, Loscalzo J. Altered lipid profile after Kawasaki syndrome. Circulation. 1991;84:625–31. doi: 10.1161/01.cir.84.2.625. [DOI] [PubMed] [Google Scholar]
- 70.Chiang AN, Hwang B, Shaw GC, et al. Changes in plasma levels of lipids and lipoprotein composition in patients with Kawasaki disease. Clin Chim Acta. 1997;260:15–26. doi: 10.1016/s0009-8981(96)06502-3. [DOI] [PubMed] [Google Scholar]
- 71.de Groot E, Hovingh GK, Wiegman A, et al. Measurement of arterial wall thickness as a surrogate marker for atherosclerosis. Circulation. 2004;109:III33–8. doi: 10.1161/01.CIR.0000131516.65699.ba. [DOI] [PubMed] [Google Scholar]
- 72.Noto N, Okada T, Yamasuge M, et al. Noninvasive assessment of the early progression of atherosclerosis in adolescents with Kawasaki disease and coronary artery lesions. Pediatrics. 2001;107:1095–9. doi: 10.1542/peds.107.5.1095. [DOI] [PubMed] [Google Scholar]
- 73.Cheung YF, Wong SJ, Ho MH. Relationship between carotid intima-media thickness and arterial stiffness in children after Kawasaki disease. Arch Dis Child. 2007;92:43–7. doi: 10.1136/adc.2006.096628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Dalla Pozza R, Bechtold S, Urschel S, Kozlik-Feldmann R, Netz H. Subclinical atherosclerosis, but normal autonomic function after Kawasaki disease. J Pediatr. 2007;151:239–43. doi: 10.1016/j.jpeds.2007.03.057. [DOI] [PubMed] [Google Scholar]
- 75.Ino T, Shimazaki S, Akimoto K, et al. Coronary artery calcification in Kawasaki disease. Pediatr Radiol. 1990;20:520–3. doi: 10.1007/BF02011380. [DOI] [PubMed] [Google Scholar]
- 76.Kaichi S, Tsuda E, Fujita H, et al. Acute coronary artery dilation due to Kawasaki disease and subsequent late calcification as detected by electron beam computed tomography. Pediatr Cardiol. 2008;29:568–73. doi: 10.1007/s00246-007-9144-5. [DOI] [PubMed] [Google Scholar]
- 77.Dadlani GH, Gingell RL, Orie JD, et al. Coronary artery calcifications in the long-term follow-up of Kawasaki disease. Am Heart J. 2005;150:1016. doi: 10.1016/j.ahj.2005.07.025. [DOI] [PubMed] [Google Scholar]
- 78.Terashima M, Awano K, Honda Y, et al. Images in cardiovascular medicine. “Arteries within the artery” after Kawasaki disease: a lotus root appearance by intravascular ultrasound. Circulation. 2002;106:887. doi: 10.1161/01.cir.0000030708.86783.92. [DOI] [PubMed] [Google Scholar]
- 79.Ishii M, Ueno T, Ikeda H, et al. Sequential follow-up results of catheter intervention for coronary artery lesions after Kawasaki disease: quantitative coronary artery angiography and intravascular ultrasound imaging study. Circulation. 2002;105:3004–10. doi: 10.1161/01.cir.0000019733.56553.d8. [DOI] [PubMed] [Google Scholar]
- 80.Arnold R, Ley S, Ley-Zaporozhan J, et al. Visualization of coronary arteries in patients after childhood Kawasaki syndrome: value of multidetector CT and MR imaging in comparison to conventional coronary catheterization. Pediatr Radiol. 2007;37:998–1006. doi: 10.1007/s00247-007-0566-2. [DOI] [PubMed] [Google Scholar]
- 81.Suzuki A, Takemura A, Inaba R, Sonobe T, Tsuchiya K, Korenaga T. Magnetic resonance coronary angiography to evaluate coronary arterial lesions in patients with Kawasaki disease. Cardiol Young. 2006;16:563–71. doi: 10.1017/S1047951106001168. [DOI] [PubMed] [Google Scholar]
- 82.Takemura A, Suzuki A, Inaba R, et al. Utility of coronary MR angiography in children with Kawasaki disease. AJR Am J Roentgenol. 2007;188:W534–9. doi: 10.2214/AJR.05.1414. [DOI] [PubMed] [Google Scholar]
- 83.Japanese Circulation S. Guidelines for the diagnosis and management of cardiovascular sequelae in Kawasaki disease. Circ J. 2003;67:1111–1174. [Google Scholar]
- 84.Min TQ, Zhu CJ, Xiang WX, Hui ZJ, Peng SY. Improvement in endothelial progenitor cells from peripheral blood by ramipril therapy in patients with stable coronary artery disease. Cardiovasc Drugs Ther. 2004;18:203–9. doi: 10.1023/B:CARD.0000033641.33503.bd. [DOI] [PubMed] [Google Scholar]
- 85.Bahlmann FH, de Groot K, Mueller O, Hertel B, Haller H, Fliser D. Stimulation of endothelial progenitor cells: a new putative therapeutic effect of angiotensin II receptor antagonists. Hypertension. 2005;45:526–9. doi: 10.1161/01.HYP.0000159191.98140.89. [DOI] [PubMed] [Google Scholar]
- 86.Sugahara Y, Ishii M, Muta H, Iemura M, Matsuishi T, Kato H. Warfarin therapy for giant aneurysm prevents myocardial infarction in Kawasaki disease. Pediatr Cardiol. 2008;29:398–401. doi: 10.1007/s00246-007-9132-9. [DOI] [PubMed] [Google Scholar]
- 87.Levy DM, Silverman ED, Massicotte MP, McCrindle BW, Yeung RS. Longterm outcomes in patients with giant aneurysms secondary to Kawasaki disease. J Rheumatol. 2005;32:928–34. [PubMed] [Google Scholar]
- 88.Arakawa K, Akita T, Nishizawa K, et al. Anticoagulant therapy during successful pregnancy and delivery in a Kawasaki disease patient with coronary aneurysm--a case report. Jpn Circ J. 1997;61:197–200. doi: 10.1253/jcj.61.197. [DOI] [PubMed] [Google Scholar]
- 89.Hayakawa H, Katoh T. Successful pregnancy after coronary artery bypass grafting for Kawasaki disease. Acta Paediatr Jpn. 1998;40:275–7. doi: 10.1111/j.1442-200x.1998.tb01927.x. [DOI] [PubMed] [Google Scholar]
- 90.Shear R, Leduc L. Successful pregnancy following Kawasaki disease. Obstet Gynecol. 1999;94:841. doi: 10.1016/s0029-7844(99)00348-8. [DOI] [PubMed] [Google Scholar]
- 91.Tsuda E, Kawamata K, Neki R, Echigo S, Chiba Y. Nationwide survey of pregnancy and delivery in patients with coronary arterial lesions caused by Kawasaki disease in Japan. Cardiol Young. 2006;16:173–8. doi: 10.1017/S1047951106000126. [DOI] [PubMed] [Google Scholar]
- 92.Ishii M, Ueno T, Akagi T, et al. Guidelines for catheter intervention in coronary artery lesion in Kawasaki disease. Pediatr Int. 2001;43:558–62. doi: 10.1046/j.1442-200x.2001.01464.x. [DOI] [PubMed] [Google Scholar]
- 93.Akagi T. Interventions in Kawasaki Disease. Pediatr Cardiol. 2005 doi: 10.1007/s00246-004-0964-2. [DOI] [PubMed] [Google Scholar]
- 94.Kwon HS, Md, Shin JI, Md, Choi JY, Md, Sul JH, Md, Jang YS., Md Polytetrafluoroethylene-covered stent deployment in the setting of Kawasaki disease. Catheter Cardiovasc Interv. 2007;69:1075–6. doi: 10.1002/ccd.21002. author reply 1077. [DOI] [PubMed] [Google Scholar]
- 95.Waki K, Baba K. Transcatheter polytetrafluoroethylene-covered stent implantation in a giant coronary artery aneurysm of a child with Kawasaki disease--a potential novel treatment. Catheter Cardiovasc Interv. 2006;68:74–7. doi: 10.1002/ccd.20808. [DOI] [PubMed] [Google Scholar]
- 96.Peters TF, Parikh SR, Pinkerton CA. Rotational ablation and stent placement for severe calcific coronary artery stenosis after Kawasaki disease. Catheter Cardiovasc Interv. 2002;56:549–52. doi: 10.1002/ccd.10226. [DOI] [PubMed] [Google Scholar]
- 97.Tsuda E, Kitamura S. National survey of coronary artery bypass grafting for coronary stenosis caused by Kawasaki disease in Japan. Circulation. 2004;110:II61–6. doi: 10.1161/01.CIR.0000138194.61225.10. [DOI] [PubMed] [Google Scholar]
- 98.Kitamura A, Mukohara N, Ozaki N, Yoshida M, Shida T. Two adult cases of coronary artery aneurysms secondary to kawasaki disease. Thorac Cardiovasc Surg. 2008;56:57–9. doi: 10.1055/s-2007-965056. [DOI] [PubMed] [Google Scholar]
- 99.Checchia PA, Pahl E, Shaddy RE, Shulman ST. Cardiac transplantation for Kawasaki disease. Pediatrics. 1997;100:695–9. doi: 10.1542/peds.100.4.695. [DOI] [PubMed] [Google Scholar]