

SUMMARY
Data from the 1997–2004 Surveys of Prevalent HIV Infections Diagnosed were analysed by three geographical areas of residence and treatment to describe the heterogeneous growth of the HIV epidemic in England and provide projections to 2007. Between 1997 and 2004, the number of diagnosed HIV-infected adults resident in England increased by 163% (14 223 to 37 459). Within the ‘London environs’ the increase was 360% (742 to 3411), within the rest of England 219% (4417 to 14 088) and within London 120% (9064 to 19 960). By 2004, the London environs had the largest proportion of infections acquired through heterosexual sex (and in particular women) and the most recently diagnosed population. Projections indicate over half of diagnosed HIV-infected adults will live outside London by 2007. The epidemiology of diagnosed HIV infection within the London environs is likely to be a predictor of future trends in England overall.
INTRODUCTION
Established in 1995, the annual cross-sectional Survey of Prevalent HIV Infections Diagnosed (SOPHID) provides a residence-based measure of individuals with diagnosed HIV infection [1–3]. The survey aims to include every individual in England, Wales and Northern Ireland with diagnosed HIV infection who has attended for HIV-related care at National Health Service (NHS) sites of treatment within a calendar year.
Historically London has been the focus of HIV in the United Kingdom and although London continues to have the largest numbers of resident and treated individuals, recent increases in prevalence have been proportionally greater outside the capital [1]. Analyses of the 1997–2003 SOPHID data [1] found the four strategic health authorities with the largest observed increases in the number of adults seen for HIV-related care or treatment, were outside London (Bedfordshire and Hertfordshire; Essex; Leicestershire, Northamptonshire and Rutland; Thames Valley) [1]. Of these, three bordered London (Bedfordshire and Hertfordshire; Essex; Thames Valley). Much of the increase in the number of adults seen for HIV-related care in the United Kingdom since 1997 is a result of continuing new diagnoses of HIV, particularly among those migrating from countries with high HIV prevalence, and the impact of highly active antiretroviral therapy, which has substantially reduced HIV-related mortality [4, 5].
To inform the planning and financing of HIV services in England, we investigate the heterogeneous growth of the HIV epidemic by focusing on the changes in the epidemiology of diagnosed HIV infection between 1997 and 2004 within the health authorities in close proximity to London [the London environs (LE)] and comparing these to London and the Rest of England (RoE). We also investigate what implications current and future trends of diagnosed HIV infection in the LE may have for the other areas.
METHODS
The Survey of Prevalent HIV Infections Diagnosed (SOPHID) was established in 1995 as an annual cross-sectional survey of all individuals accessing HIV-related treatment and care services in England, Wales and Northern Ireland. The SOPHID database is held at the Health Protection Agency's Centre for Infections and strict attention to confidentiality is maintained at every stage of data collection, analysis and storage.
Eight consecutive annual cross-sectional SOPHID surveys (1997–2004) each providing a ‘census’ of individuals with diagnosed HIV in England were used for these analyses. Methods of data collection, de-duplication and dissemination have been described elsewhere [1–3]. This study was restricted to adults aged ⩾15 years. The following variables from SOPHID were included in these descriptive analyses: area of residence, area of treatment, probable route of infection, sex and ethnicity. Where an individual was reported by more than one site to an annual survey, they were assigned to the site at which they were last seen in the calendar year, and the place of residence is as reported by that site.
Information on the time of diagnosis and the world region where HIV infection occurred were available by linking SOPHID data to the national surveillance database for new diagnoses of HIV [6, 7]. Record linkage was based on soundex code [3], date of birth and sex. World region of infection is only presented for adults infected through heterosexual sex as this information is not investigated further for other groups (warranted because the majority of adults infected through sex between men (SBM) probably acquire their infection within the United Kingdom whereas the majority of adults infected through heterosexual sex probably acquire their infection outside the United Kingdom [6]).
Increases in numbers of adult residents with diagnosed HIV infection between 1997 and 2004 were ranked by strategic health authority of residence. Based on the rank order of these increases three geographical areas were defined for analyses using 2001 health authorities: London, LE and RoE. The LE area was defined as the eight health authorities (2001 definition) bordering London (Buckinghamshire, Hertfordshire, North Essex, South Essex, West Kent, East Surrey, West Surrey and Berkshire) and Bedfordshire, which was included due to its proximity and links to London [1]. London was defined as for the current London government office region (2005 definition). RoE was defined as all other parts of England. Health authority boundaries provide more geographical definition than larger strategic health authorities (introduced in April 2002). Retrospective allocation of pre-2002 surveys to the 2002 NHS administrative boundaries of primary care trusts was not technically possible.
Results are presented by area of residence unless stated otherwise. Prevalence is shown per 100 000 population, based on the Office of National Statistics (ONS) mid-2001 resident population estimates (aged ⩾15 years). Children were excluded as no soundex code is reported for these records and additional information could not be attributed from the new diagnoses database. Descriptive analyses of epidemiological variables concentrate on differences between the three areas of residence.
Data by probable route of infection and residence were extrapolated to provide an estimate of the number of adults with diagnosed HIV infection for the years 2005–2007. To reflect current trends, projections were based on 2001–2004 SOPHID data. A number of model diagnostic and fitting techniques were applied to the 2001–2004 data to find a model that yielded a good fit. The negative binomial model, previously used to provide extrapolation estimates [2], was shown to no longer adequately fit the data. A linear regression model was found to be the most appropriate to model the temporal trend for each of the exposure by residence groups. stata 8.2 was used for statistical analysis (Stata Corp., College Station, TX, USA).
RESULTS
Area of residence and area of HIV treatment or care
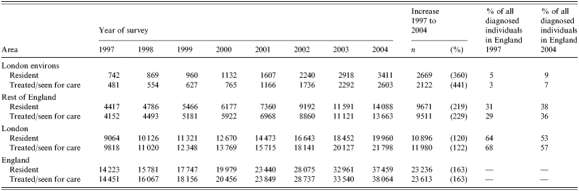
Between 1997 and 2004, both the number of diagnosed HIV-infected adults resident in England and those receiving HIV-related treatment or care in England increased by 163% (14 223 to 37 459 and 14 451 to 38 064 respectively). These increases varied greatly across the three study areas (Table 1). In England in 2004, the rate of diagnosed HIV-infected adults per 100 000 adult population was 92, in LE it was 62, in RoE 48 and in London 335.
Table 1.
Adults with diagnosed HIV infection by area of residence and area seen for HIV-related treatment or care, 1997–2004
Area of treatment and care in relation to area of residence
In 2004, 68% (2322/3411) of adults resident in LE also received their care within LE compared to 54% (401/742) in 1997. The proportion of adults both resident and treated in RoE increased slightly from 91% (4029/4417) in 1997 to 94% (10 812/11 591) in 2004 whereas in London the proportion was over 99% for all years [1997 (9020/9064), 2004 (19 786/19 960)].
Of the 32% (1089) LE residents receiving care elsewhere in 2004, 86% (933) were treated in London and 14% (156) in RoE. A higher proportion of LE residents infected through SBM received their care elsewhere (49%, 398/817) than LE residents infected through heterosexual sex (25%, 609/2459). Of the 6% (779) RoE residents receiving care elsewhere in 2004, 82% (736/899) were treated in London, 17% (150) in LE and 1% (13) in Wales or Northern Ireland.
Sex, ethnicity and probable route of infection
While the number of men doubled between 1997 and 2004, the number of women increased almost five times such that the male:female ratio decreased in all areas, particularly in LE where in 2004 there was near parity (LE 4·1:1 to 1·1:1, RoE 6·1:1 to 2·1:1, London 4·2:1 to 2·2:1) (Table 2). In all three geographical areas, the largest proportional increases were seen in the number of individuals of black-African ethnicity. This rise was largest in LE, increasing from 9% of all resident diagnosed adults (69/729) in 1997 to 57% (1935/3371) in 2004 (Table 2).
Table 2.
Adults with diagnosed HIV infection by area of residence, sex, ethnicity, year of UK diagnosis and route and country of infection, 1997 and 2004
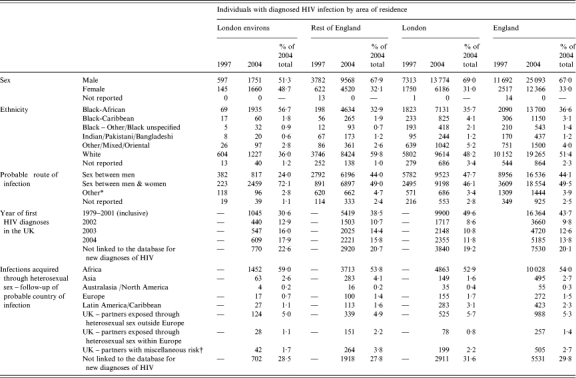
Includes injecting drug use, mother-to-child transmission (>14 years of age) and blood/blood products.
Includes partners exposed through heterosexual sex in an unknown country, and partners exposed within or outside the UK through injecting drug use, blood/blood products, and sex between men.
Within LE the number of resident adults who acquired their infection through heterosexual sex (either within or outside the United Kingdom) outnumbered those reported as having acquired their infection through SBM (either within or outside the United Kingdom) in 2000. In RoE this epidemiological shift took place in 2004 whereas SBM remained the most probable route of infection reported in London in 2004 (Table 2).
In 2004, black-African women infected through heterosexual sex accounted for the highest proportion of residents within LE with diagnosed HIV infection (39%, 1322/3411), followed by white men infected through SBM (22%, 736). Within RoE and London, the two largest groups in 2004 were white men infected through SBM [42% (5851/14 088) and 39% (7818/19 960) respectively] and black-African females infected through heterosexual sex [21% (2960) and 22% (4479) respectively].
Year of HIV diagnoses in the United Kingdom and probable country of infection
Across the three study areas approximately the same proportion of adults reported to SOPHID in 2004 were found to have a linked record in the national surveillance database for new diagnoses of HIV (Table 2). Of adults reported as resident within LE in 2004 and who had a linked record, 60·4% (1596/2641) were shown to have been diagnosed with HIV infection in the United Kingdom in 2002, 2003 or 2004 (Table 2). Of adults reported as resident within LE in 2004 who acquired their infection through heterosexual sex and had a linked record, 82·6% (1452/1757) acquired their infection in Africa (Table 2). Within RoE the figures were 51·5% (5749/11 168) and 74·6% (3713/4979) respectively and within London 38·8% (6220/16 120) and 77·4% (4863/6287) respectively.
Projected estimates of diagnosed HIV infection for 2005–2007
The linear regression model predicted an increase of 55% (3372 to 5243) between 2004 and 2007 in the overall number of diagnosed adults resident within LE (Table 3). In RoE it predicted an increase of 46% (13 755 to 20 134) and within London an increase of 28% (19 407 to 24 781). The model predicted that by 2007 over half of diagnosed HIV-infected adults will live outside London.
Table 3.
Adults with diagnosed HIV infection by area of residence and probable route of infection – observed data 2001–2004 and estimates using a linear regression model 2001–2007
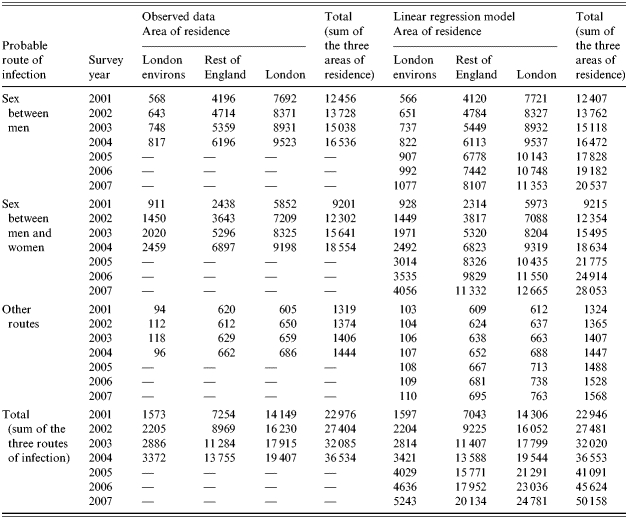
In all three areas the estimated increases are strongly influenced by new diagnoses in adults infected through heterosexual sex. Within London it was predicted that the number of adults infected through heterosexual sex would exceed, for the first time, those infected through SBM in and after 2005 (Table 3). This epidemiological shift was observed within LE in 2000 and RoE in 2004. Within all three areas it is estimated that numbers of adults infected through SBM will gradually increase between 2004 and 2007 whereas, numbers infected through other (non-sexual) routes remain constant (Table 3).
DISCUSSION
Increase in number of diagnosed HIV infections
The large increase in numbers of adults living with diagnosed HIV infection in England between 1997 and 2004 is, in part, due to the success of anti-retroviral drugs in reducing mortality rates [4]. However, a stronger influence than reduced mortality on the figures is the large increase that has been seen in new HIV diagnoses, particularly since 2000–2001 [8]. A number of factors would appear to contribute to this increase including an increase in the uptake of voluntary confidential HIV testing, the continued transmission of HIV within the United Kingdom [particularly amongst men who have sex with men (MSM)], the increased diagnosis of infections acquired through heterosexual contact in countries with a high HIV prevalence and the introduction of the universal offer and recommendation of antenatal screening for HIV in 1999.
During the study period the largest increase in numbers of diagnosed individuals was in London. Proportionally, however, infections increased at a faster pace outside London and in particular within LE where the proportional increase of diagnosed infections was three times that seen within London and almost double that seen within RoE.
Overall new diagnoses in England among heterosexual men and women exceeded those in MSM in 1999 [9]. Whereas LE and RoE have already seen the prevalent number of diagnosed adults infected through heterosexual sex exceed the number of adults infected through SBM, the linear regression model predicts that this epidemiological shift will not take place within London until 2005 (observed data not available until late 2006).
In 1999, when new diagnoses of heterosexually acquired infections exceeded those acquired through SBM, 61% of the population in England seen for HIV-related treatment or care were infected through SBM compared to half in LE. This reflects that the epidemiology of diagnosed HIV infection within LE is shaped to a greater extent than elsewhere by more recently diagnosed infections. Also reflecting this is that only within LE has the number of HIV-infected black-African women exceeded that of all white adults (2002), and only within LE has the ratio of male:female adults (including all ethnicities and routes of infection) almost reached parity.
Service providers
The number of individuals receiving HIV-related care at services within LE has increased because of the growth in the resident diagnosed population and the increase in the proportion of the current resident population seeking care locally. Interestingly, the data show a difference by probable route of infection between those LE residents receiving care locally and those receiving care in the capital, with a large proportion of those infected through SBM receiving HIV care in London.
These differences may be explained by: MSM having greater social ties with the capital; current treatment facilities locally not meeting the needs of certain groups; disparities in awareness of availability and open access of services; socioeconomic disparities. Further analyses are necessary to understand patterns of use of HIV-related services. However, it is inevitable that the increase in diagnosed HIV infections observed and predicted for LE will not only have implications for service providers within LE but also those within London.
Limitations of this study
It is estimated that ∼34% of adults aged between 15 and 59 years living with HIV infection in the United Kingdom are unaware of their status [10]. Therefore, the results presented reflect not the total number of adults living with HIV in England but the number resident within England aware of their HIV infection and accessing NHS sites of treatment for HIV-related care within a calendar year [1–3]. It is also worth noting that probable route of infection may not necessarily reflect an individual's risk of onward transmission of HIV infection and this should be considered when using SOPHID data to inform HIV prevention strategies.
With the three study areas being large there is obviously considerable heterogeneity within each area in terms of the rate of increase in numbers of diagnosed HIV infections and in the epidemiology of the resident populations, particularly for RoE [1]. However, extrapolations for these areas are likely to be more reliable than for smaller geographies.
The extrapolated estimates for 2005–2007, using a linear regression model, assume that current observed trends continue [2]. The model is particularly sensitive to changes in the pattern of in-migration of HIV-infected people from countries with a high prevalence of HIV to the United Kingdom (the majority of individuals resident in LE and reported as having been infected through heterosexual sex were probably infected in Africa) and changes in number of deaths among individuals with diagnosed HIV infection. However, a negative binomial model applied to the 1997–2001 SOPHID data accurately predicted the 2003 totals for LE (estimate 2918, observed 2918) and London (estimate 18 742, observed 18 452), although it underestimated the total for RoE (estimate 10 526, observed 11 591) [2].
Neither SOPHID nor the national database for new diagnoses of HIV collect information on an individual's residency status or reasons for migration within the United Kingdom. Therefore, it was not possible to comment on whether the National Asylum Support Service guidelines on dispersal [11] (as informed by section 97 of the Immigration and Asylum Act 1999) possibly explain some of the trends presented in this paper.
Implications
Of the three study areas the trends seen within LE most closely follow those seen in new diagnoses in the United Kingdom as a whole [6]. If current trends continue it is probable that the diagnosed population resident within RoE will, in the next couple of years, present a similar epidemiology to that currently seen within LE. The increase in number of diagnosed HIV infections among heterosexual men and women from countries with a high HIV prevalence reinforces the need for sustained prevention activities within these communities to minimize the risk of ongoing transmission of HIV within the United Kingdom.
The increases described have serious implications for the planning and financing of HIV/AIDS services and the appropriate targeting of prevention programmes in the three study areas. As stated in the Department of Health's national strategy for sexual health and HIV, local services should meet the needs of different populations [12]. Data presented in this study highlight the need for local HIV/AIDS services to be responsive to rapid increases and changes to the epidemiology and treatment access patterns of their diagnosed prevalent HIV-infected population.
CONCLUSIONS
Between 1997 and 2004, the number of adults living with diagnosed HIV infection increased in all three study areas. However, the proportional increase of diagnosed adults resident within LE was three times that seen within London and nearly double that seen within RoE.
In 2004, of the three study areas, LE had the largest proportion of infections acquired through heterosexual sex, the largest proportional increase in numbers of diagnosed adults of black-African ethnicity, the most recently diagnosed population and the highest proportion of individuals receiving HIV-related care outside their area of residence.
While LE and RoE have already seen numbers of adults infected through heterosexual sex exceed those acquired through SBM the linear regression model predicts that this epidemiological shift will take place within London in 2005.
London continues to have the largest number of resident and treated adults with diagnosed HIV infection, however, using a linear regression model projections based on current figures show that over half of diagnosed HIV-infected adults will live outside London by 2007.
Based on current trends it is probable that the diagnosed population resident within RoE will, in the next couple of years, present a similar epidemiology to that currently seen within LE.
ACKNOWLEDGEMENTS
We thank the SOPHID advisory group, facilitators and data providers across England, Wales and Northern Ireland, for their continuing help and support with the survey. The National SOPHID survey was funded by the Department of Health. The London SOPHID survey was funded by the NHS London Specialised Commissioning Group.
DECLARATION OF INTEREST
None.
REFERENCES
- 1.Rice B et al. The changing epidemiology of prevalent diagnosed HIV infections in England, Wales and Northern Ireland 1997 to 2003. Sexually Transmitted Infections. 2005;81:223–229. doi: 10.1136/sti.2004.012070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rice B et al. Prevalent diagnosed HIV in England, Wales & Northern Ireland – adjusted totals 1996 to 2001 and extrapolations to 2004. AIDS. 2004;18:927–932. doi: 10.1097/00002030-200404090-00010. [DOI] [PubMed] [Google Scholar]
- 3.McHenry A et al. National assessment of prevalent diagnosed HIV infections. Communicable Disease and Public Health. 2000;3:277–281. [PubMed] [Google Scholar]
- 4.Communicable Disease Surveillance Centre (Department of HIV & STI) and Scottish Centre for Infection and Environmental Health. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm Quarterly Surveillance Tables No. 65. 04/4 Table 2 ( ). Accessed 31 January 2005.
- 5.Communicable Disease Surveillance Centre (Department of HIV & STI) and Scottish Centre for Infection and Environmental Health. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm Quarterly Surveillance Tables No. 65. 04/4 Table 7a ( ). Accessed 31 January 2005.
- 6.Communicable Disease Surveillance Centre (Department of HIV & STI) and Scottish Centre for Infection and Environmental Health. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm Quarterly Surveillance Tables No. 65. 04/4 ( ). Accessed 31 January 2005.
- 7.Sinka K et al. Impact of the HIV epidemic in sub-Saharan Africa on the pattern of HIV in the UK. AIDS. 2003;17:1683–1690. doi: 10.1097/00002030-200307250-00013. [DOI] [PubMed] [Google Scholar]
- 8.Communicable Disease Surveillance Centre (Department of HIV & STI) and Scottish Centre for Infection and Environmental Health. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm Quarterly Surveillance Tables No. 65. 04/4 Table 3a ( ). Accessed 31 January 2005.
- 9.Communicable Disease Surveillance Centre (Department of HIV & STI) and Scottish Centre for Infection and Environmental Health. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm. http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/hiv/epidemiology/hars_tables.htm Quarterly Surveillance Tables No. 65. 04/4 Table 6a ( ). Accessed 31 January 2005.
- 10.The UK Collaborative Group for HIV and STI Surveillance London: Health Protection Agency Centre for Infections; 2005. . Mapping the Issues – HIV and other Sexually Transmitted Infections in the United Kingdom: , November 2005 ( ). Accessed 19 May 2006. [Google Scholar]
- 11.National Asylum Support Service 2004. http://www.asylumsupport.info/bulletin31.htm. http://www.asylumsupport.info/bulletin31.htm . NASS Policy Bulletin 31 – Dispersal guidelines, ). Accessed 19 May 2006.
- 12.Department of Health. 2001. The national strategy for sexual health and HIV, . Crown Copyright.